")
Back to Journals » International Journal of General Medicine » Volume 15
Characterisation of Disease Patterns of Dermatomyositis with Different Initial Manifestations
Authors Sun Y , Li DF, Zhang YL, Liang X, Li TF
Received 4 May 2022
Accepted for publication 18 July 2022
Published 9 August 2022 Volume 2022:15 Pages 6519—6528
DOI https://doi.org/10.2147/IJGM.S372658
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Yue Sun,1 Dai-Feng Li,2 Yin-Li Zhang,1 Xu Liang,1 Tian-Fang Li1
1Department of Rheumatology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, 450000, People’s Republic of China; 2Department of Orthopaedics, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, 450000, People’s Republic of China
Correspondence: Tian-Fang Li, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, 450000, People’s Republic of China, Tel +86-15713865716, Email [email protected]
Purpose: To determine the characteristics and prognoses of dermatomyositis (DM) by comparing the difference in initial symptoms.
Patients and Methods: A retrospective analysis was performed on the patients diagnosed with DM from 1 January 2019 to 1 January 2021. Based on the firstly presented symptoms, patients were divided into five groups, namely rash group, muscle weakness group, arthritis group, respiratory symptom group and atypical symptom group. Clinical and laboratory data were recorded. All patients were followed up until 31 May 2021.
Results: In total 136 DM patients, rash (40%) was the most common initial symptom, followed by respiratory symptoms (22%), arthritis (20%), muscle weakness (10%) and atypical symptoms (8%). Rash group and atypical group had a higher positive rate of anti-TIF1γ antibodies than arthritis group and respiratory symptom group (P < 0.05). Respiratory symptom and arthritis groups had a higher positive rate of anti-Ro52 antibodies than rash and muscle weakness groups (P < 0.05). Respiratory group had a higher incidence of ILD than rash and atypical groups. The FVC and DLCO in respiratory group were significantly lower than rash group, arthritis group and atypical group (P < 0.05). The survival rate of rash group was significantly higher than muscle weakness group and arthritis group (P < 0.05).
Conclusion: DM patients with different initial manifestations had different myositis antibodies and prognoses.
Keywords: initial symptom, interstitial lung disease, ILD, rash, myositis specific antibody, MSA
Introduction
As the most common type of idiopathic inflammatory myositis (IIM), dermatomyositis (DM) is a systemic autoimmune disease characterized by skin lesions and muscle inflammation, and its incidence is approximately 1–6 per 100,000 individuals.1 The pathogenesis of DM is multifaceted with the involvement of various factors including genetic, environmental, immunological and non-immunological. Therefore, DM patients have protean clinical manifestations and different prognoses.2,3
Rash was the most common initial symptom of DM.4 Pathognomonic cutaneous lesions include heliotrope sign, Gottron's papules and Gottron's sign. Other manifestations include “V” sign, “shawl” sign, “holster” sign, nail-fold changes, scalp involvement,1 clinically psoriasiform,5 mechanic hand, panniculitis and calcinosis. To date, the following DM-specific antibodies have been found: anti-melanoma differentiation-associated protein 5 (MDA5), anti-transcription intermediary factor 1-gamma (TIF1γ), anti-nuclear matrix protein 2 (NXP2), anti-small ubiquitin-like modifier activating enzyme (SAE), and anti-chromodomain-helicase-DNA-binding proteins (Mi-2) antibodies, etc. Ulcerative lesions and panniculitis are more common in MDA5 positive patients.6,7 Typical muscle involvements manifested as symmetric and proximal muscle weakness. However, classic cutaneous and muscle involvements do not always coexist. Clinical amyopathic dermatomyositis (CADM) and clinical dermatomyositis sine dermatitis (DMSD) are two special types of DM. About 20% of DM is CADM8 and 8% is DMSD.9 The incidence of malignancy is higher compared to healthy population. Interstitial lung disease (ILD) is the most common type of pulmonary involvement and the leading cause of mortality in DM patients. Because of protean manifestations, differential diagnosis is important in the first stage of the disease. Autoimmune diseases with different initial symptoms may have different clinical features, for example, pulmonary complications were more progressive and severe in non-sicca onset than sicca onset patients in Sjogren’s patients.10 DM patients with ILD as an initial manifestation had lower incidences of heliotrope rash, chest V area rash, shawl sign and joint involvement,11 but the characteristics and prognoses of other initial symptom subgroups are not completely clear. Prompt diagnosis is a critical for successful treatment and prevention of flares.12
Materials and Methods
Materials
Patients newly diagnosed as DM were collected from 1 January 2019 to 1 January 2021. Patients with different initial symptoms were divided into these five groups: rash group, muscle weakness group, arthritis group, respiratory symptom group and atypical symptom group. Atypical symptoms were defined as those that are not commonly manifested such as rash, muscle weakness, arthritis, and respiratory symptoms. Patients who presented with two or more symptoms at the time of onset were excluded in this study in order to more clearly analyze the impact of initial symptoms on patients. All patients were followed up until 31 May 2021. The research was conducted in accordance with the ethical standards of the Declaration of Helsinki and approved by ethics committee of the First Affiliated Hospital of ZhengZhou University, and obtained informed consent of participants.
Inclusion Criteria
(1) Over 18 years old.
(2) Patients who met Bohan and Peter “definite” or “probable” diagnostic criteria,13,14 and were first diagnosed with DM.
Bohan and Peter’s criteria:
- Symmetrical weakness of the limb-girdle muscles and anterior neck flexors, progressing over weeks to months, with or without dysphagia or respiratory muscle involvement.
- Muscle-biopsy evidence of necrosis Type I and II fibers, phagocytosis, regeneration with basophilia, large vesicular sarcolemmal nuclei and prominent nucleoli, atrophy in a perifascicular distribution, variation in fiber size, and an inflammatory exudate, often perivascular.
- Elevation in serum of skeletal-muscle enzymes, particularly creatine phosphokinase and often aldolase, serum glutamate oxaloacetate and pyruvate transaminases, and lactate dehydrogenase.
- The electromyographic triad of short, small, polyphasic motor units, fibrillations, positive sharp waves and insertional irritability, and bizarre, high-frequency repetitive discharges.
- Consists of dermatologic features including a lilac discoloration of eyelids (heliotrope) with periorbital edema, a scaly, erythematous dermatitis over the dorsum of the hands (especially the metacarpophalangeal and proximal interphalangeal joints Gottron’s sign), and involvement of the knees, elbows and medial malleoli, as well as the face, neck, and upper torso.
Definite diagnostic criteria: the fifth plus any three items from the first to fourth.
Probable diagnostic criteria: the fifth plus any two items from the first to fourth.
(3) Complete basic information such as clinical features, laboratory examinations.
Exclusion Criteria
(1) Did not meet the above inclusion criteria.
(2) According to 2018 ENMC classification criteria,15 anti-synthetase syndrome (ASS) and immune-mediated necrotizing myopathy (IMNM) were excluded. Patient with anti-synthetase autoantibodies (anti-Jo1, anti-PL7, anti-EJ, anti-OJ, anti-KS, or anti-Zo autoantibodies) were considered to have anti-synthetase syndrome (ASS). Patients with anti-HMGCR or anti-SRP antibodies were considered have IMNM.
(3) Other connective tissue diseases were excluded (rheumatoid arthritis, systemic lupus erythematosus, Sjogren’s syndrome, scleroderma).
(4) Excluded other serious diseases (cardiopulmonary failure, hepatic and renal dysfunction, serious cardiovascular, cerebrovascular diseases).
Data Collection
- Clinical features: initial symptoms, muscle weakness, respiratory involvement (cough, dyspnea and cyanosis), digestive involvement (constipation, diarrhea and abdominal pain), cardiac involvement (pericarditis, myocarditis, arrhythmia), renal involvement (proteinuria, hematuria, tubular urine), arthritis, gender, age, delay in diagnosis, BMI, smoking, ILD and itch.
- Laboratory data: creatine kinase, lactate dehydrogenase, total cholesterol, triglyceride, high-density lipoprotein, low-density lipoprotein, Krebs von den Lungen-6 (KL6), ferritin and CD4/8.
- Pulmonary function tests: forced expiratory volume in 1s/forced vital capacity (FEV1/FVC), maximum mid-expiratory flow (MMEF75/25), forced vital capacity (FVC) and diffusion capacity of the lung for carbon (DLCO). The results of PFTs were shown as percentages of the predicted values of each parameter and corrected for age, gender, and height. DLCO ≥80% was defined as normal lung diffusion function. The percentage of FVC ≥80% of predicted values, and/or the percentage of FEV1 to the expected value ≥80%, and/or FEV1/FVC ≥92% were defined as normal lung function.
- Myositis antibodies: anti-RO52, anti-Mi2, anti-MDA5 and anti-TIF1γ antibodies. Anti-RO52 antibodies and anti-Mi2 antibodies were determined by luminescent immunoassay. Anti-MDA5 antibodies and anti-TIF1γ antibodies were determined by enzyme-linked immunosorbent assay.
- Follow-up: The survival conditions of all 136 patients were recorded from diagnosis to 31 May 2021 through querying outpatient and inpatient medical records and telephone return visit.
Statistical Analysis
SPSS (Version 25) and GraphPad Prism 9 were used for statistical analysis. Qualitative variables were presented as counts (n) and percentages (%) and chi-square tests or Fisher’s exact tests were used to establish statistical differences among subgroups. Normally distributed continuous variables were presented as mean ± standard deviation (SD), and non-normally distributed continuous variables presented as median (P25, P75). Kaplan–Meier survival curve was used for survival analysis among subgroups, and the survival rate was compared by Log rank test. P < 0.05 was considered statistically significant.
Results
A total of 136 cases of patients were collected according to inclusion and exclusion criteria. Tables 1–5 summarized the characteristics and study results of all 136 patients. Among them, 99 (73%) patients were female and 37 (27%) were male. Seventy-eight (57%) patients were diagnosed between the ages of 40 and 60. Seventy-two patients were recorded whether felt itch or not during the disease. Rash (n=55, 40%) was the most common first symptoms of DM, followed by respiratory symptom (n=30, 22%), arthritis (n=27, 20%), muscle weakness (n=13, 10%), and atypical symptom (n =11, 8%). Atypical symptoms included fever (n=7), diarrhea (n=2), dysphagia (n=1) and oral ulcer (n=1).
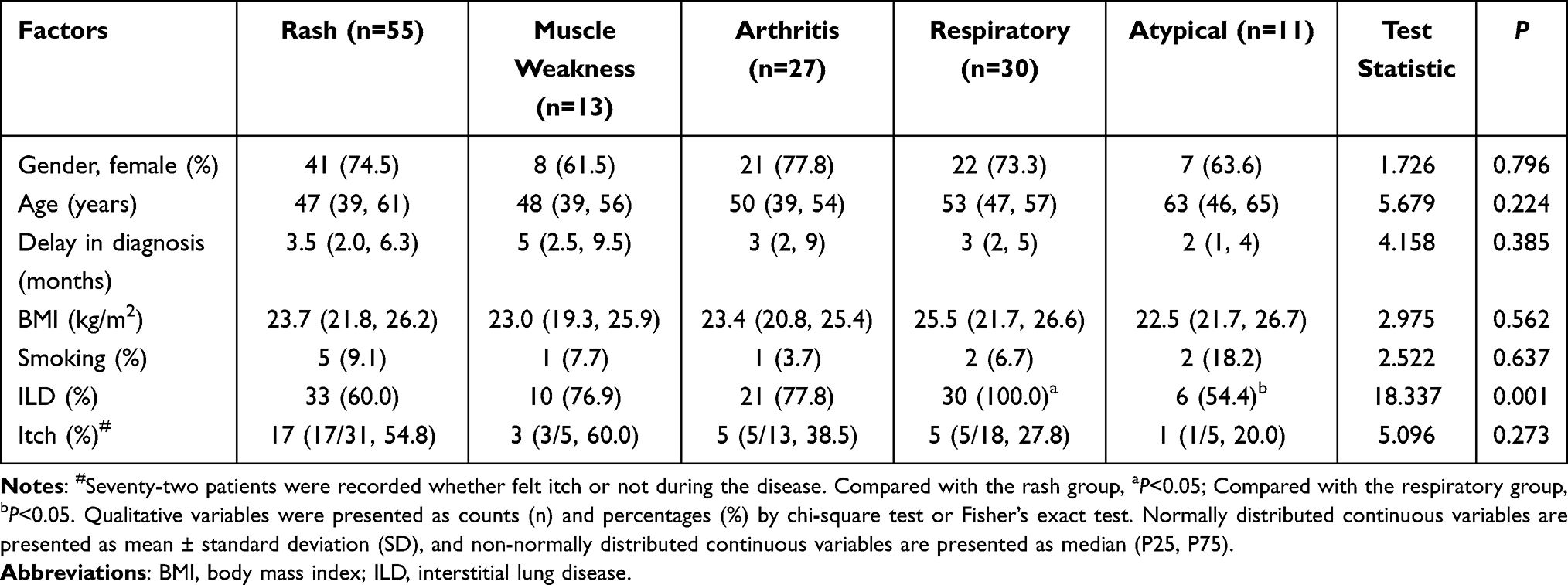 |
Table 1 General Features in Different Subgroups of DM |
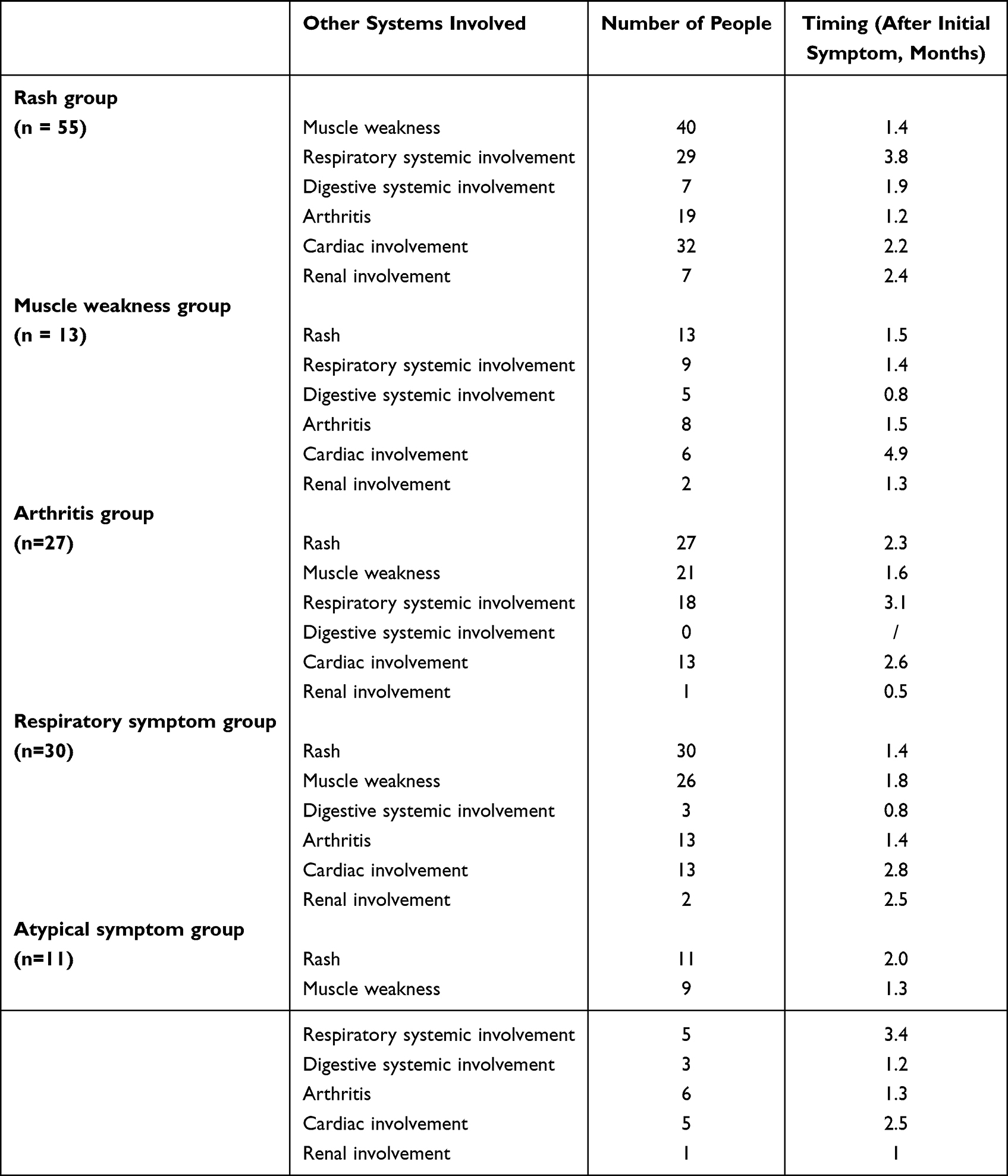 |
Table 2 Other Systems Involved in Different Subgroups of DM |
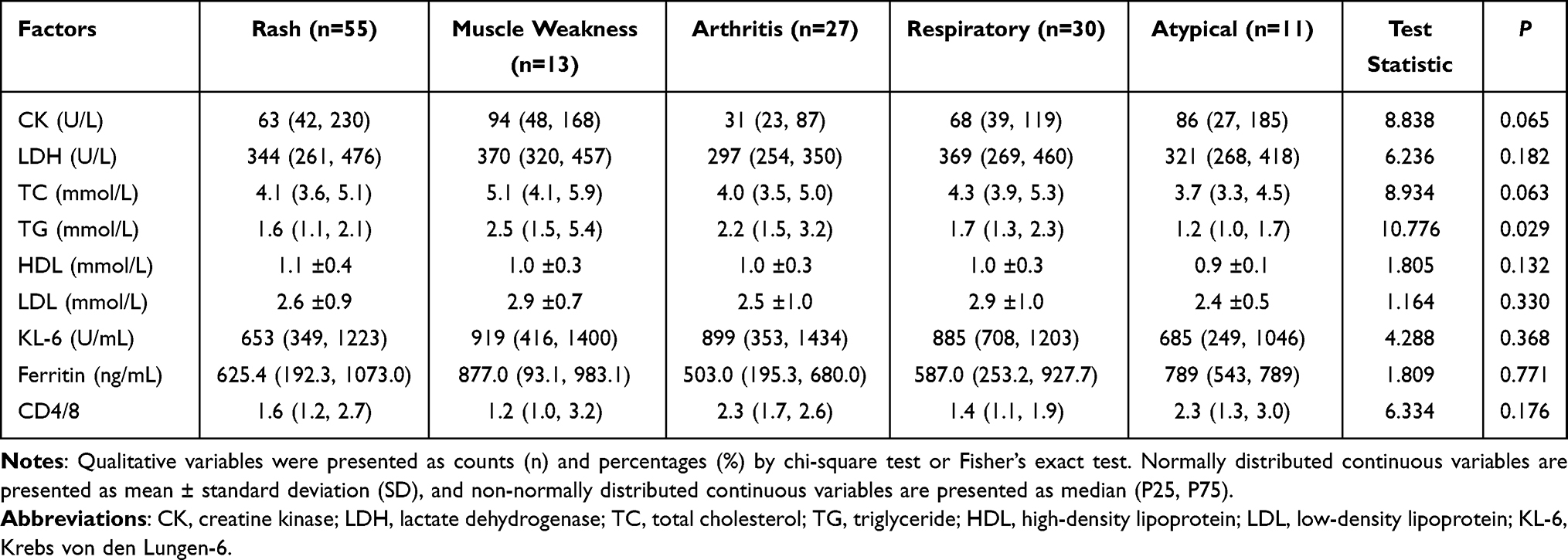 |
Table 3 Serological Indicators in Different Subgroups of DM |
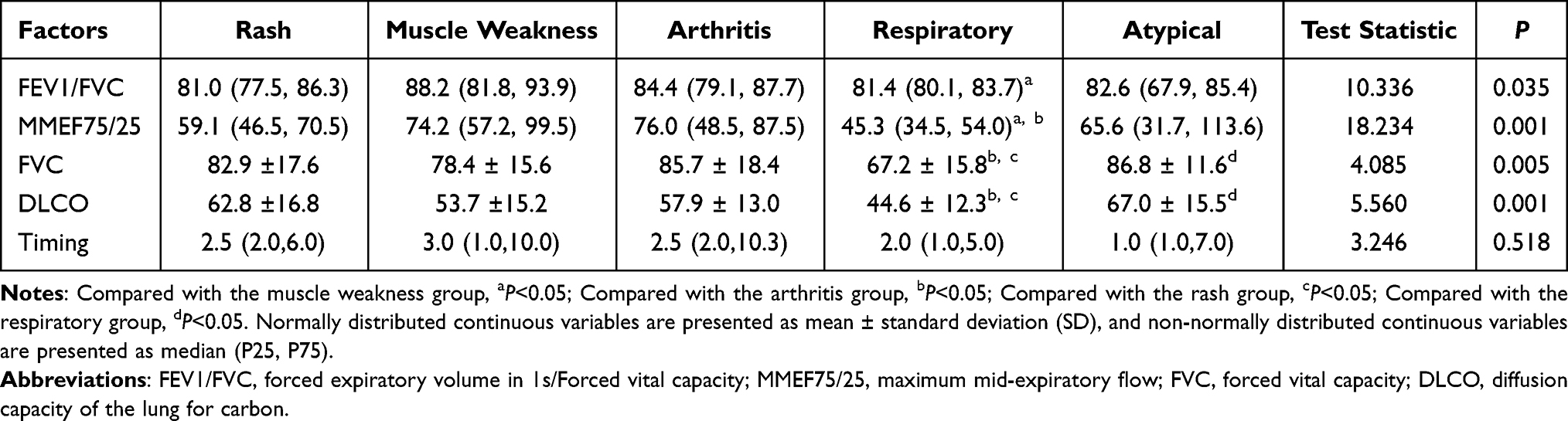 |
Table 4 PFTs in Different Subgroups of DM |
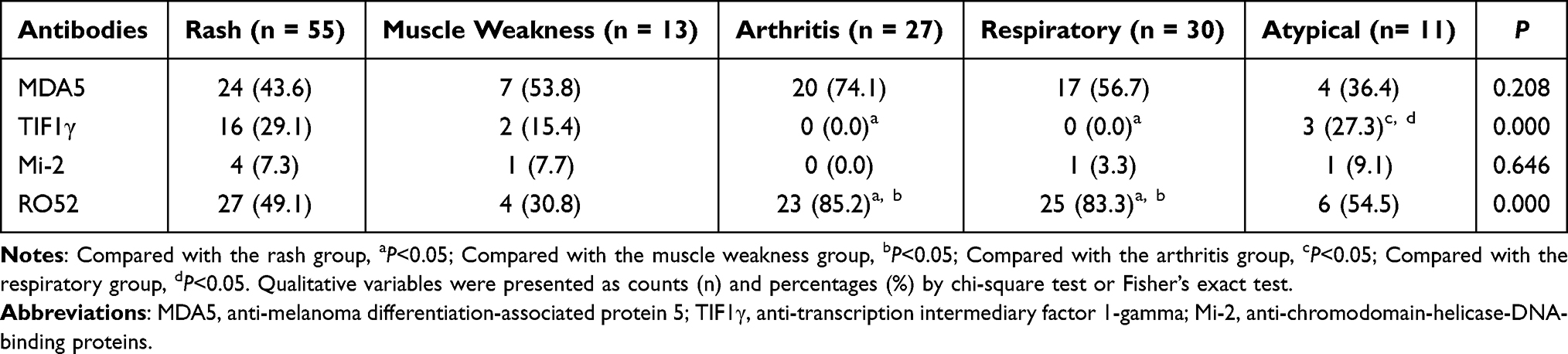 |
Table 5 Myositis Antibodies in Different Subgroups of DM |
General Features
The comparison of general features by clinical subgroups is shown in Table 1. The female-to-male ratio was about 2.7:1 in total patients, and 43% (31/72) patients experienced itchy skin during the disease. There were no significant differences in gender, age, BMI, delay in diagnosis, smoking and itch (P > 0.05). The incidence of ILD in respiratory symptom group was the higher than rash group and atypical group (100% vs 60%, 100% vs 54.4%, P < 0.05). The number of people and timing of other systems involvement in different subgroups are described in Table 2.
Serological Indicators
We examined the serological indicators in these five groups (Table 3). There were differences in the distribution of TG in the DM subgroups by Kruskal–Wallis tests (P = 0.029), but no statistic difference was found in pairwise comparison with Bonferroni’s multiple tests. The differences in other serological indicators among different subgroups had no statistical significance (P > 0.05).
Pulmonary Function Tests
Eighty patients were subjected to the PFTs in our study (Table 4). PFTs were performed at about 4 months after diagnosis, and there was no significant difference in the timing of PFTs among groups. FEV1/FVC in muscle weakness group was significantly higher than that in respiratory symptom group (88.2 (81.8, 93.9) vs 81.4 (80.1, 83.7), P < 0.05). MMEF75/25 in respiratory symptom group was significantly lower than that in muscle weakness group and arthritis group (45.3 (34.5, 54.0) vs 74.2 (57.2, 99.5), P < 0.05). FVC in respiratory symptom group was significantly lower than that in rash group, arthritis group and atypical group (67.2 ± 15.8 vs 82.9 ± 17.6, 67.2 ± 15.8 vs 78.4 ± 15.6, 67.2 ± 15.8 vs 86.8 ± 11.6, P < 0.05), and DLCO in respiratory symptom group was also significantly lower than that in rash group, arthritis group and atypical group (44.6 ± 12.3 vs 62.8 ± 16.8, 44.6 ± 12.3 vs 57.9 ± 13.0, 44.6 ± 12.3 vs 67.0 ± 15.5, P < 0.05).
Myositis Antibodies
The differences in myositis antibodies among subgroups included anti-TIF1γ and anti-RO52 antibodies (Table 5). The positive rate of anti-TIF1γ antibodies in rash group was significantly higher than that in arthritis group and respiratory symptom group (29.1% vs 0.0%, 29.1% vs 0.0%, P < 0.05). Atypical group had a higher positive rate of anti-TIF1γ antibodies than arthritis group and respiratory symptom group (27.3% vs 0.0%, 27.3% vs 0.0%, P < 0.05). The positive rate of anti-RO52 antibodies in respiratory symptom group was significantly higher than that in rash group and muscle weakness group (83.3% vs 49.1%, 83.3% vs 30.8%, P < 0.05). Arthritis group had a higher positive rate anti-RO52 antibodies than that in rash group and muscle weakness group (85.2% vs 49.1%, 85.2% vs 30.8%, P < 0.05). There were no significant differences in other myositis antibodies (P > 0.05).
Survival Analysis
All patients were followed up in our study, and 20 patients died. Of the 20 deaths, 13 were due to infection, including 11 pulmonary infections and 2 sepsis, 6 patients died of respiratory failure, and 1 patient died of cardiovascular disease. The longest follow-up time was 28 months, and the mean follow-up time was 14 months. Kaplan–Meier analysis was used to analyze survival curves among different subgroups (Figure 1). The survival rate of atypical symptom group was 100%. There were significant differences in cumulative survival rate among the five groups by Log rank test (P < 0.05). The survival rate of rash group was significantly higher than muscle weakness group and respiratory group (P = 0.008, P = 0.031), and atypical symptom group had a higher survival rate than muscle weakness group (P = 0.047).
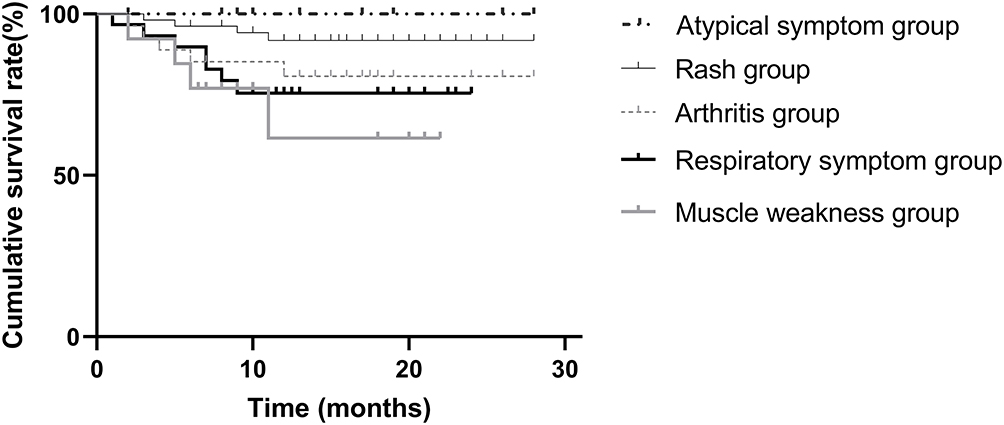 |
Figure 1 The survival curves of differences in subgroups (Kaplan–Meier analysis). There were significant differences among the five groups by Log rank test (P < 0.05). The survival rate of rash group was significantly higher than muscle weakness group and respiratory symptom group (P = 0.008, P = 0.031), and atypical symptom group had a higher survival rate than muscle weakness group (P = 0.047). |
Discussion
After dividing DM patients into rash group, muscle weakness group, arthritis group, respiratory symptom group and atypical symptom group, we demonstrate that DM patients with different initial symptoms have different characteristic features and prognoses.
General Features and Serological Indicators
In our study, no significant differences were found in demographics of different subgroups, indicating that age, gender, and BMI had no effect on the first manifestations of DM. Smoking has been reported to be associated with ILD, dysphagia, malignancy, and cardiac involvement in myositis patients.16 However, there was no significant difference in the positive rate of smoking among different subgroups. It may be due to the ethnic heterogeneity or the relatively small sample size of our study. The female-to-male ratio was about 2.7:1 for total patients, which is slightly higher than the 2:1 ratio in a previous study.17 It may be due to the regional disparity. Skin itchy appeared in 43% (31/72) patients, which is lower compared to previous studies that showed 85–90% DM patients had pruritus.18,19 The ethnic and subjective differences of patients may be responsible for such discrepancy. Rash (n=55, 40%) was the most common initial symptoms of DM. DM rash was often associated with itching and photosensitivity. The itch degree corresponds to the CDASI (Cutaneous Disease and Activity Severity Index), which can be used to assess the disease activity of patients.18 About 20% of the patients came to the hospital with arthritis as the first symptom. Arthritis in IIM is often characterized by symmetrical, non-aggressive polyarthritis, with the commonly afflicted joints as follows: the wrist, metacarpophalangeal joints, interphalangeal joints and shoulder,20 which, to some extent, similar to rheumatoid arthritis. Clinicians should take IIM into consideration when making a diagnosis of seronegative rheumatoid arthritis. About 22% patients showed respiratory symptom as the first symptom, and ILD was diagnosed after PFTs and high-resolution computed tomography (HRCT) of chest. Our results are consistent with a previous report that ILD occurred in about 20–30% of the patients before the diagnosis of myositis.21 Taking use of HRCT, the patterns of the myositis associated ILD are divided to the following types: usual interstitial pneumonia (UIP), nonspecific interstitial pneumonia (NSIP), organized pneumonia (OP), acute interstitial pneumonia (AIP), lymphocytic interstitial pneumonia (LIP).22,23 Myositis associated UIP had a better survival rate than idiopathic pulmonary fibrosis UIP.24 The incidence of ILD in respiratory symptom group was higher than rash group and atypical group. In this study, the difference of TG in subgroups was statistically significant by Kruskal–Wallis tests (P < 0.05), but no statistic difference in pairwise comparison with Bonferroni’s multiple tests probably because of the relatively small sample size.
Pulmonary Function Tests
In this retrospective study, only 80 of 136 patients were subjected to PFTs, while the remaining patients did not do it because of different reasons, for example, patients were too weak to finish such test. PFTs was conducted at the early stage of their disease, and there was no significant difference in the timing when performing PFTs among groups. Respiratory symptom group showed significantly lower levels of FVC and DLCO than those in rash group, arthritis group and atypical manifestations group. Restrictive ventilatory impairment is the typical characteristic of ILD, and the decrease of DLCO usually precedes alteration of lung volumes in PFTs. Of note, the weakness of respiratory muscles may cause abnormal PFTs. As such, both PFTs and chest HRCT are necessary to determine the cause of pulmonary involvements.
Myositis Antibodies
MSAs may help establish a diagnosis of myositis, and they are also associated with the clinical manifestations and prognosis.15,25 As only a small number of patients were tested for anti-NXP2 and anti-SAE in this retrospective study, these two antibodies were excluded from further analysis. We focused on MSAs such as anti-MDA5, anti-TIF1γ and anti-Mi2 antibodies. The positive rate of anti-TIF1γ antibodies in the rash group and atypical group was both significantly higher than arthritis group and respiratory symptom group. Previous researches also indicated that patients with positive anti-TIF1γ antibodies often present typical rash.26 All 27 patients in arthritis group had negative anti-TIF1γ and anti-Mi2 antibodies. Our data suggested the positive rate of anti-TIF1γ antibodies in arthritis group was significantly lower than rash group and atypical group, consistent with a previous study showing that patients with positive anti-TIF1γ antibodies had lower risk of arthritis.5 Anti-RO52 antibodies is the most common MAAs, and its positive rate in respiratory symptom group and arthritis group was significantly higher than that in rash group and muscle weakness group. Anti-RO52 antibodies often co-exists with anti-MDA5 antibodies, and their occurrence correlates with a more severe clinical phenotype and poorer prognosis.27 The positive rate of MSAs in this study was 70%, consistent with a previous study showing over 50% of positive rate of MSAs.28 Among the 136 patients subjected to myositis antibodies test, 6 (4.4%) had more than one MSAs, which was higher than 0.2% in a previous study,29 and was inconsistent with the mutual exclusivity of MSA. The heterogeneity of myositis and the methods used to detect the antibodies may be responsible for such a disparity.
Survival Analysis
The Kaplan–Meier survival curve showed that the cumulative survival rates of patients in different initial symptoms varied. Muscle weakness group had a lower survival rate than rash group and atypical group, and the survival rate of rash group was higher than respiratory group. In different stages of myositis, non-immune and immune system mechanisms play a key role in muscle inflammation.3,30 The different initial symptoms in DM patients may also result from different pathological mechanisms.
Our single-center study has several limitations. First, in this retrospective study, incomplete data collection may cause the loss of important indicators of DM patients. Second, the sample size was relatively small. Third, the follow-up period was short. While our study paved a new way to investigate DM, more patients and longer follow-up time may help generate more data for accurate characterization of DM.
Conclusion
The most common initial symptom in DM patients was skin rash, followed by respiratory symptom, arthritis, muscle weakness, and atypical symptom. The positive rate of anti-TIF1γ antibodies in rash and atypical symptom groups was significantly higher than arthritis and respiratory symptom groups. Respiratory symptom and arthritis groups had a significantly higher positive rate of anti-RO52 antibodies than rash and muscle weakness groups. Both PFTs and chest HRCT should be conducted for early detection of DM-ILD. The survival rate of rash group was significantly higher than muscle weakness and respiratory groups, while atypical symptom group had a higher survival rate than muscle weakness group. However, more comprehensive studies with longer follow-up periods are warranted to solidify our findings.
Data Sharing Statement
The datasets are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The research was conducted in accordance with the ethical standards of the Declaration of Helsinki and approved by ethics committee of the First Affiliated Hospital of ZhengZhou University and informed consent of participants was obtained.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No specific funding was received from any bodies in the public.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. DeWane ME, Waldman R, Lu J. Dermatomyositis: clinical features and pathogenesis. J Am Acad Dermatol. 2020;82(2):267–281. doi:10.1016/j.jaad.2019.06.1309
2. Lundberg IE. Expert perspective: management of refractory inflammatory myopathy. Arthritis Rheumatol. 2021;73(8):1394–1407. doi:10.1002/art.41762
3. Miller FW, Lamb JA, Schmidt J, Nagaraju K. Risk factors and disease mechanisms in myositis. Nat Rev Rheumatol. 2018;14(5):255–268. doi:10.1038/nrrheum.2018.48
4. Chen P, Xie J, Xiao R, Zhang G, Qiu X, Zhan Y. Clinical analysis for 108 cases of dermatomyositis. J Central South Univ Med Sci. 2019;44(10):1157–1162.
5. Fiorentino DF, Kuo K, Chung L, Zaba L, Li S, Casciola-Rosen L. Distinctive cutaneous and systemic features associated with antitranscriptional intermediary factor-1gamma antibodies in adults with dermatomyositis. J Am Acad Dermatol. 2015;72(3):449–455. doi:10.1016/j.jaad.2014.12.009
6. Charrow A, Vleugels RA. Cutaneous ulcerations in anti-MDA5 dermatomyositis. N Engl J Med. 2019;381(5):465. doi:10.1056/NEJMicm1816147
7. Hasegawa A, Shimomura Y, Kibune N, Koshio J, Umemori Y, Abe R. Panniculitis as the initial manifestation of dermatomyositis with anti-MDA5 antibody. Clin Exp Dermatol. 2017;42(5):551–553. doi:10.1111/ced.13128
8. Bendewald MJ, Wetter DA, Li X, Davis MDP. Incidence of dermatomyositis and clinically amyopathic dermatomyositis: a population-based study in Olmsted County, Minnesota. Arch Dermatol. 2010;146(1):26–30. doi:10.1001/archdermatol.2009.328
9. Inoue M, Tanboon J, Hirakawa S, et al. Association of dermatomyositis sine dermatitis with anti-nuclear matrix Protein 2 autoantibodies. JAMA Neurol. 2020;77(7):872–877. doi:10.1001/jamaneurol.2020.0673
10. Gao H, Zou YD, Zhang XW, et al. Interstitial lung disease in non-sicca onset primary Sjogren’s syndrome: a large-scale case-control study. Int J Rheum Dis. 2018;21(7):1423–1429. doi:10.1111/1756-185X.13334
11. Shen M, Gong Y, Zeng X, Zhang F, Tang F. Interstitial lung disease as an initial manifestation of dermatomyositis. Zhonghua Yi Xue Za Zhi. 2014;94(43):3402–3406.
12. Maurer B. Early symptoms of dermatomyositis and antisynthetase syndrome. Z Rheumatol. 2013;72(10):970–976. doi:10.1007/s00393-013-1196-8
13. Bohan A, Peter JB. Polymyositis and dermatomyositis (first of two parts). N Engl J Med. 1975;292(7):344–347. doi:10.1056/NEJM197502132920706
14. Bohan A, Peter JB. Polymyositis and dermatomyositis (second of two parts). N Engl J Med. 1975;292(8):403–407. doi:10.1056/NEJM197502202920807
15. Mammen AL, Allenbach Y, Stenzel W, Benveniste O. 239th ENMC International Workshop: classification of dermatomyositis, Amsterdam, the Netherlands, 14–16 December 2018. Neuromuscul Disord. 2020;30(1):70–92. doi:10.1016/j.nmd.2019.10.005
16. Lilleker JB, Vencovsky J, Wang G, et al; all EuroMyositis contributors. The EuroMyositis registry: an international collaborative tool to facilitate myositis research. Ann Rheum Dis. 2018;77(1):30–39. doi:10.1136/annrheumdis-2017-211868
17. Furst DE, Amato AA, Iorga ŞR, Gajria K, Fernandes AW. Epidemiology of adult idiopathic inflammatory myopathies in a U.S. managed care plan. Muscle Nerve. 2012;45(5):676–683. doi:10.1002/mus.23302
18. Kim HJ, Zeidi M, Bonciani D, et al. Itch in dermatomyositis: the role of increased skin interleukin-31. Br J Dermatol. 2018;179(3):669–678. doi:10.1111/bjd.16498
19. Shirani Z, Kucenic MJ, Carroll CL, et al. Pruritus in adult dermatomyositis. Clin Exp Dermatol. 2004;29(3):273–276. doi:10.1111/j.1365-2230.2004.01510.x
20. Klein M, Mann H, Vencovský J. Arthritis in idiopathic inflammatory myopathies. Curr Rheumatol Rep. 2019;21(12):70. doi:10.1007/s11926-019-0878-x
21. Barba T, Mainbourg S, Nasser M, Lega JC, Cottin V. Lung diseases in inflammatory myopathies. Semin Respir Crit Care Med. 2019;40(2):255–270. doi:10.1055/s-0039-1685187
22. Batra K, Butt Y, Gokaslan T, Burguete D, Glazer C, Torrealba JR. Pathology and radiology correlation of idiopathic interstitial pneumonias. Hum Pathol. 2018;72:1–17. doi:10.1016/j.humpath.2017.11.009
23. Lega JC, Reynaud Q, Belot A, Fabien N, Durieu I, Cottin V. Idiopathic inflammatory myopathies and the lung. Eur Respir Rev. 2015;24(137):545. doi:10.1183/16000617.00002015
24. Aggarwal R, McBurney C, Schneider F, et al. Myositis-associated usual interstitial pneumonia has a better survival than idiopathic pulmonary fibrosis. Rheumatology. 2017;56(3):384–389. doi:10.1093/rheumatology/kew426
25. Gupta L, Naveen R, Gaur P, Agarwal V, Aggarwal R. Myositis-specific and myositis-associated autoantibodies in a large Indian cohort of inflammatory myositis. Semin Arthritis Rheum. 2021;51(1):113–120. doi:10.1016/j.semarthrit.2020.10.014
26. Didona D, Juratli HA, Scarsella L, Keber U, Eming R, Hertl M. Amyopathic and anti-TIF1 gamma-positive dermatomyositis: analysis of a monocentric cohort and proposal to update diagnostic criteria. Eur J Dermatol. 2020;30(3):279–288. doi:10.1684/ejd.2020.3766
27. Xu A, Ye Y, Fu Q, et al. Prognostic values of anti-Ro52 antibodies in anti-MDA5-positive clinically amyopathic dermatomyositis associated with interstitial lung disease. Rheumatology. 2021;60(7):3343–3351. doi:10.1093/rheumatology/keaa786
28. Betteridge Z, McHugh N. Myositis-specific autoantibodies: an important tool to support diagnosis of myositis. J Intern Med. 2016;280(1):8–23. doi:10.1111/joim.12451
29. Betteridge Z, Tansley S, Shaddick G, et al; UKMyonet contributors. Frequency, mutual exclusivity and clinical associations of myositis autoantibodies in a combined European cohort of idiopathic inflammatory myopathy patients. J Autoimmun. 2019;101:48–55. doi:10.1016/j.jaut.2019.04.001
30. Ceribelli A, De Santis M, Isailovic N, Gershwin ME, Selmi C. The immune response and the pathogenesis of idiopathic inflammatory myositis: a critical review. Clin Rev Allergy Immunol. 2017;52(1):58–70. doi:10.1007/s12016-016-8527-x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.