")
Back to Journals » International Journal of General Medicine » Volume 14
Changes of Urinary Cytokines in Non-Diabetic Obese Patients After Laparoscopic Sleeve Gastrectomy
Authors Salman A , Salman M , Sarhan MD, Maurice K, Tag El-Din M, Youssef A, Ahmed R, Abouelregal T, Shaaban HE , GabAllah GMK, Omar MG
Received 19 January 2021
Accepted for publication 24 February 2021
Published 10 March 2021 Volume 2021:14 Pages 825—831
DOI https://doi.org/10.2147/IJGM.S302418
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ahmed Salman,1 Mohamed Salman,2 Mohamed D Sarhan,2 Karim Maurice,2 Mohamed Tag El-Din,3 Ahmed Youssef,1 Reham Ahmed,1 Tarek Abouelregal,1 Hossam El-Din Shaaban,4 Ghada MK GabAllah,5 Mahmoud Gouda Omar1
1Internal Medicine Department, Faculty of Medicine, Cairo University, Cairo, Egypt; 2General Surgery Department, Faculty of Medicine, Cairo University, Cairo, Egypt; 3General Surgery Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt; 4Gastroenterology Department, National Hepatology and Tropical Medicine Research Institute, Cairo, Egypt; 5Medical Biochemistry Department, Faculty of Medicine, Menoufia University, Shibin Al Kawm, Egypt
Correspondence: Ahmed Salman
Internal Medicine Department, Faculty of Medicine, Cairo University, Cairo, 11311, Egypt
Tel +20 1000468664
Email [email protected]
Introduction: Adipose tissues synthesize and secrete various proinflammatory and anti-inflammatory mediators, termed cytokines. This work aims to assess different serum and urinary cytokine levels before and 12 months after laparoscopic sleeve gastrectomy (LSG).
Patients: This prospective study was performed on 61 obese non-diabetic patients who underwent LSG. All patients were followed up postoperatively at 12 months with the assessment of arterial blood pressure, microalbuminuria, urinary and serum levels of inflammatory cytokines (macrophage migration inhibitory factor “MIF,” monocyte chemotactic protein “MCP”-1, chemokine (C-C motif) ligand 15 (CCL-15), and CCL-18), in addition to serum creatinine, total cholesterol, and C-reactive protein (CRP).
Results: Mean BMI showed decreased substantially from 44.78 ± 3.59 Kg/m2 to 34.56 ± 2.45. Systolic blood pressure decreased from 147.03 ± 16.89 mmHg to 128.82 ± 12.52 and diastolic blood pressure decreased from 90.51 ± 12.71 mmHg to 79.69 ± 10.39. At one-year of follow-up, there was statistically significant decrease of mean serum creatinine, total cholesterol, CRP, CCL-15, CCL-18, MIF/creatinine ratio, MCP-1/creatinine ratio, CCL-15/creatinine ratio, and CCL-18/creatinine ratio (P value < 0.001).
Conclusion: Improvement of systemic and renal inflammatory states after LSG may positively affect obesity-related renal disease by steering the adipokine levels towards anti-inflammatory profiles.
Keywords: laparoscopic sleeve gastrectomy, urinary cytokines
Introduction
Obesity represents a chronic low-grade inflammatory status that is mainly caused by an increase and inflammation of adipocytes. Adipose tissues synthesize and secrete various serum and urinary cytokines.1
Cytokines are glycoproteins defined as immunomodulating agents specifically in host immune responses to infection, inflammation, sepsis, cancer, and reproduction. Cytokines are produced by a broad range of cells, including immune cells as well as endothelial cells, fibroblasts, adipocytes, and various stromal cells. Cytokines include chemokines, interferons, interleukins, lymphokines, and tumor necrosis factors.2,3
Obesity is associated with multiple pathophysiologic disorders that may predispose to renal injury.4 Different adipose tissue-related serum and urinary cytokines have an intimate relation with renal and metabolic dysfunctions.5,6 Of these inflammatory cytokines, the most significant were the urinary and serum values of macrophage migration inhibitory factor (MIF),6 monocyte chemotactic protein (MCP)-1,5 chemokine (C-C motif) ligand 15 (CCL-15), and5 chemokine (C-C motif) ligand 18 (CCL-18).6,7
These cytokines are involved in the pathogenesis of obesity-related renal dysfunction that is termed obesity-related glomerulopathy (ORG). This expression points to the secondary form of focal segmental glomerulosclerosis. Proteinuria is considered the clinical landmark of obesity-related renal dysfunction, however ORG can be demonstrated at lower levels of proteinuria.4
Lifestyle changes have a limited role in severely obese patients.8,9 Bariatric operations are a well-recognized strategy for weight control among morbidly obese cases whose body mass index (BMI) exceeds 40 kg/m2 or whose BMI exceeds 35 kg/m2 with concomitant metabolic comorbidities such as elevated blood pressure or dyslipidemia.10,11
Laparoscopic sleeve gastrectomy (LSG) has been an attractive, efficient, and well-established surgical strategy in morbidly obese patients for obtaining long-term weight control with an improvement of associated metabolic disorders over the short and intermediate terms.12
From the renal perspective, bariatric surgery can have beneficial effects regarding albuminuria/proteinuria, ORG, and arterial blood pressure.13 A previous study showed the beneficial short-term impact of weight-loss operations on elevated blood pressure and kidney injury at 30 days postoperatively.14
We assumed that LSG-associated weight reduction can lead to amelioration of renal and systemic inflammatory states.
The present work aims to assess the values of different serum and urinary cytokines, microalbuminuria, glomerular filtration rate (GFR), and arterial blood pressure pre and twelve months post LSG in a cohort of obese cases.
Patients and Methods
The current prospective work included 61 obese non-diabetic cases for whom LSG was performed. Patients were enrolled from June 2015 to July 2018.
The study was approved by the ethical committee of Cairo University Hospitals (no: 0027/May 2015). (Reviewer 1) The work was performed in accordance with the rules of the declaration of Helsinki. All cases gave written informed consent before enrollment.
Cases that were eligible for study participation included motivated obese subjects whose BMI exceeded 40 Kg/m2 or 35 Kg/m2 with associated comorbidities, cases intending to adhere to regular monitoring, those in whom adequate non-surgical interventions did not succeed to attain satisfactory weight control, ranging from 18 to 60 years, and ultimately cases with no endocrine reasons for obesity.
Patients were precluded from enrollment if they have severe comorbidities hindering anesthesia, not intending to modify their lifestyle postoperatively, have psychological problems, those who underwent metabolic surgery, gestation, or lactation at enrollment for the study.
Notably, diabetic cases were excluded from the study. The exclusion was made according to American Diabetes Association criteria (those with glycated hemoglobin “HbA1C” > 6.5% or fasting blood sugar > 126 mg/dL or two-hour plasma glucose > 200 mg/dL after an oral glucose tolerance testing).
Moreover, those who did not complete the follow-up interval were excluded from the study.
Patients were selected for the operation after multidisciplinary evaluation, including different specialties such as surgery, internal medicine, anesthesia, and nutrition.
Surgical Procedure
The operation was done by the same experienced team. A sleeve was tailored around a 36F bougie 3–4 cm from the pylorus and reaching to the angle of His. The entire staple line was strengthened using continuous ligatures and examined for leakage by upper endoscopy. The gastric portion was retracted through the 15-mm trocar situated at the right upper abdomen. A suction drain was put in all cases and taken out five days postoperatively.
Case Evaluation
All cases were enrolled before the operation and reassessed postoperatively at one year. Patients were evaluated by a dedicated physician and filled a survey prepared to gather different important information such as age, sex, BMI, previous relevant history, associated comorbidities, current and past medications. All relevant data were registered during cases’ follows ups with the assistance of a specialized nurse. The serum samples were taken at 9 am after overnight fasting, centrifuged, isolated within 60 minutes of sampling, and then kept at −80 °C until assay.
Blood Pressure
Arterial blood pressure was assessed just before operation and twelve months afterwards by the same physician employing a Spot Vital Signs® device (model 42MTB-E1-M; Welch Allyn, Aston Abbotts, UK). Assessment of blood pressure was done after the patient had relaxed in a quiet room hall for a half-hour. Three evaluations were performed, and their average was registered. Cuff circumferences were selected depending on the patient arm size. All measurements were done pre sampling and compared to blood pressure measurements recorded at past follow-ups to evaluate variations.
Cure of hypertension was considered if the patient pressure decreased to lower than 140/90 mmHg without medications, while cure of obstructive sleep apnea and gastroesophageal reflux disease (GERD) was considered if the symptoms subjectively disappeared at the end of the study period.
Blood and Urine Sample Testing
Blood and urine samples were taken before the operation and 12 months afterwards. Midstream urine sample was put into sterilized tubes. Samples were centrifuged at 1600g for 10 min at 4°C, and the supernatant was kept at −80°C till subsequent assay. Biochemical (albumin and creatinine) and microbiological testing were done on urine samples. Serum samples were forwarded for biochemical testing (serum cystatin C, creatinine, albumin, total cholesterol, and C-reactive protein “CRP”). Estimated GFR (eGFR) was determined employing the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula. Urinary cytokine values were measured as a proportion to the urinary creatinine value.
Concentrations of MIF, MCP-1, CCL-15, and CCL-18 were evaluated by enzyme-linked immunosorbent assay (ELISA) based on the manufacturer’s directives (R&D Systems, Minneapolis, Minnesota, USA).
Statistical Analysis
Data were registered using the statistical package SPSS version 25. They were presented as mean, standard deviation, minimum and maximum for quantitative data and frequencies (number of cases), and relative frequencies (percentages) for categorical data. Comparisons between quantitative variables were performed using unpaired t-test while comparisons between pre and post-surgery were made applying paired t-test. For comparison between categorical variables, Chi-square test was used. Exact test was employed instead if the anticipated frequency is lower than 5. Correlations between quantitative data were made using Pearson correlation coefficient. P values lower than 0.05 were viewed as statistically significant.
Results
At first, ninety-two patients underwent baseline blood and urine samples. Thirty-one cases did not repeat blood and/or urine samples after the twelve months. Finally, the present study included 61 patients who completed the study period, of whom 36 were males. The age of the enrolled cases ranged from 34 to 60 years with a mean (SD) 47.13 (6.43).
At the start of the study, there were 35 cases with chronic obstructive pulmonary disease, 8 cases with coronary artery disease, and 14 cases with a smoking history.
Thirty-five patients were hypertensive. Twenty were on single anti-hypertensive medication, nine were on two medications, and six were on three medications. Thirty patients were on angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, eleven were on beta-blockers, nine were on calcium channel blockers, and six were on thiazides.
Mean weight decreased from 128.25 (10.47) at baseline to 99.28 (9.83) Kg after 12 months. Similarly, the initial mean BMI decreased from 44.78 (3.59) to 34.56 (2.45) Kg/m2.
Thirty-five patients were hypertensive at baseline; the number decreased to 19 after 12 months (P value 0.004). Furthermore, thirty-five patients had obstructive sleep apnea at baseline, yet the number dropped to 12 after study completion (P value 0.001). Twenty-eight patients had GERD at baseline, and only 12 had GERD after 12 months (P value 0.004).
The mean systolic blood pressure (SBP) decreased from 147.03 (16.89) to 128.82 (12.52) mmHg after one year. Also, the mean diastolic blood pressure (DBP) decreased from 90.51 (12.71) to 79.69 (10.39) mmHg.
The mean HbA1C decreased from 5.72 (0.45) to 5.26 (0.42) % at the end of the study.
There was a statistically significant decrease of mean serum levels of creatinine, total cholesterol, CRP, CCL-18, and CCL-15 at twelve months postoperatively with a concomitant increase in eGFR (P value <0.001).
Simultaneously, there were no significant changes in cystatin C, MCP-1, and MIF after the same follow-up period.
Table 1 summarizes mean serum laboratory investigations at baseline and after 12 months.
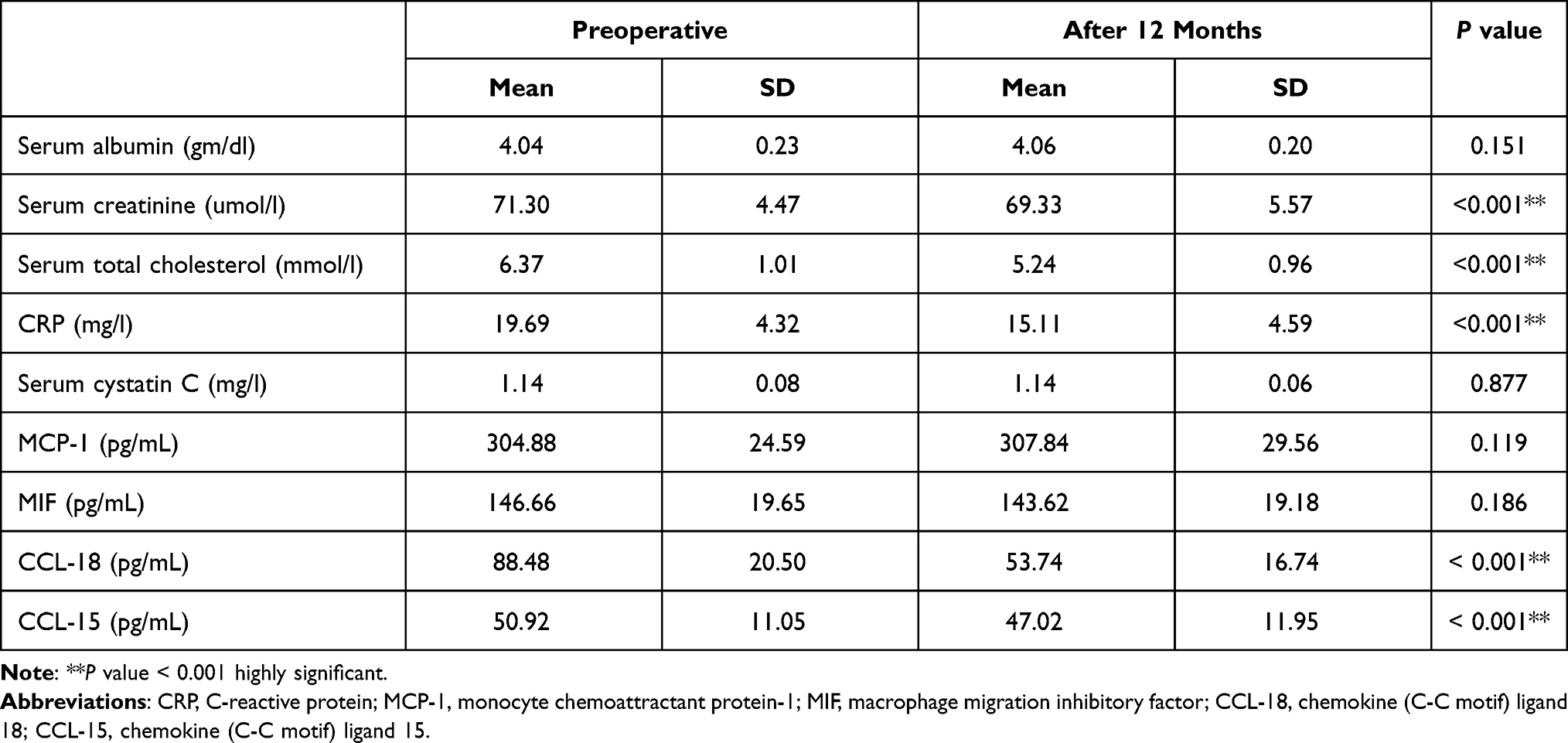 |
Table 1 Serum Laboratory Investigations at Baseline and After 12 Months |
Regarding urinary cytokines, there was a highly significant decrease of mean MIF/creatinine ratio, MCP-1/creatinine ratio, CCL-18/creatinine ratio, and CCL-15/creatinine ratio after twelve months of follow-up (P value <0.001).
Also, there was a notable decrease in microalbuminuria at the end of the study (P value 0.012).
Table 2 summarizes urinary laboratory investigations at baseline and after twelve months.
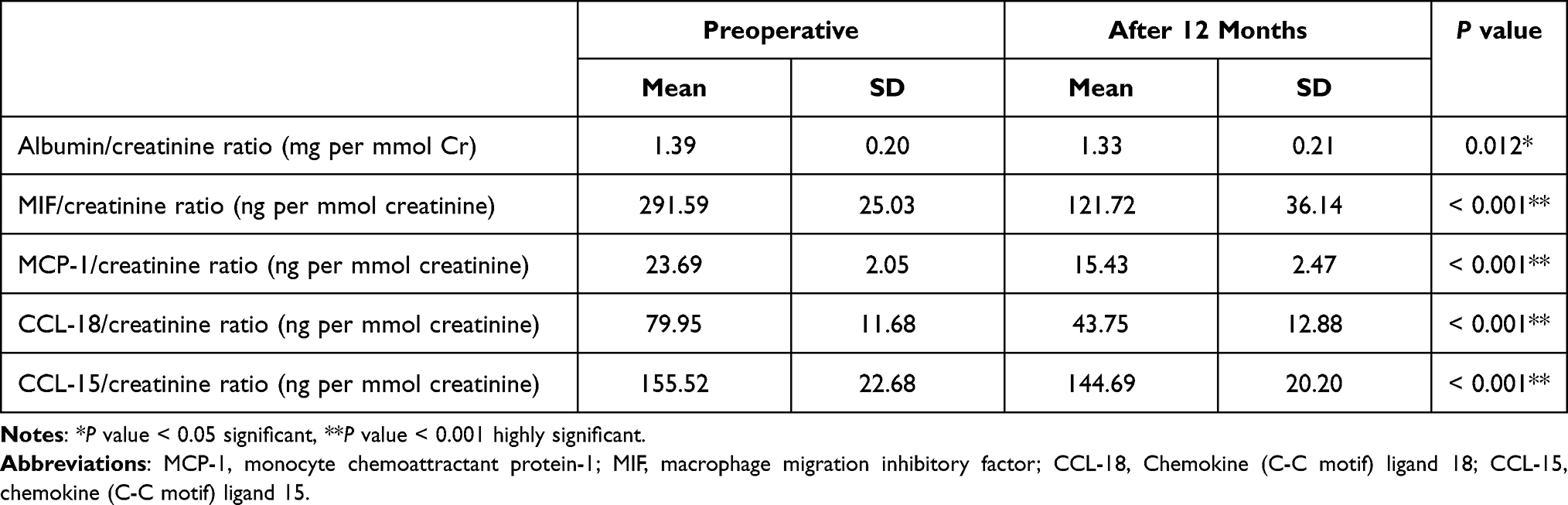 |
Table 2 Urinary Laboratory Investigations at Baseline and After 12 Months |
Discussion
Obesity is a complex chronic disease that has multifactorial aspects. Adipose tissue, the dominant character of obesity, is now identified as an active organ that has a paramount role in chronic inflammatory status.15
Inflammation is thought to have an essential role in the progression of chronic kidney disease (CKD). CKD patients usually have high circulating levels of inflammatory cytokines. So this category of patients commonly demonstrates a proinflammatory status since their early stages, which, in turn, can result in the progression of their renal disease.16
Besides, high levels of serum and urinary inflammatory cytokines accelerated renal inflammation and kidney injury in mice.17,18
The current work demonstrated that LSG resulted in a significant improvement in markers of renal inflammation. These conclusions add to the scarcely available literature on the impact of weight reduction in ameliorating the renal adipokine profile in obese non-diabetic cases.
To comprehend the worth of these conclusions, they have to be understood within the physiological and pathological roles of these cytokines.
CRP, an acute-phase reactant, is mainly synthesized in the liver.19 CRP enhances the inflammatory status resulting in pronounced systemic inflammation.20 CRP levels are linked to circulating levels of other inflammatory cytokines,21 microalbuminuria, and albuminuria.22
CCL18 is a chemokine highly expressed in the lung and in antigen-presenting cells such as M2 macrophages and dendritic cells, which can act as a chemoattractant for both lymphocytes and immature dendritic cells.23
CCL18 has been shown to have a role in chronic inflammatory conditions like atopic dermatitis, asthma, and arthritis. The accurate impact of CCL18 on pro and anti-inflammatory mechanisms still to be precisely described.24
CCL-15, a cloned chemokine, is synthesized primarily in the hepatocytes and intestinal epithelium. Moreover, this chemokine is inducible in macrophages. It plays a vital role as a chemoattractant to different cell types as monocytes/macrophages, T cells, and neutrophils. Besides, this chemokine possesses antibacterial and angiogenic effects.25
It was demonstrated that MCP-1-induced kidney damage is weakened by MCP-1 receptor knockout, decreasing glomerular fibrosis in a paradigm of unilateral ureteric blockage.26 MIF is a pleiotropic adipokine that has a role in different conditions related to immunity and systemic inflammation. It is synthesized mainly by fat cells, glomerular and tubular cells, and triggered immunocytes, such as monocytes and macrophages.14
A previous study suggested that MIF was pathogenic in acute kidney injury (AKI) mouse model in MIF wild‐type and MIF knockout mice and the plasma and urinary MIF levels correlated with the progression and regression of AKI.27
The present work revealed a substantial improvement in serum CRP, CCL-18, and CCL-15, in addition to urinary levels of CCL-18, CCL-15, MCP-1, MIF. This result agrees with the result obtained by Rojano-Rodríguez and colleagues, who demonstrated a significant decrease in CRP at six months after metabolic surgery.28
A previous study demonstrated decreased levels of urinary cytokines as well as serum CCL-18, with no changes in serum levels of MIF, CCL-15, and MCP-1 (Yet, in our analysis, there was a significant change in CCL-15 in contrast to this study).14
The development of albuminuria or proteinuria is an early clinical stigma of renal injury.29 Both albuminuria and proteinuria may antedate a decline in renal function by many years.30
After weight reduction, especially after metabolic surgery, microalbuminuria and proteinuria usually significantly decrease, and this decrease is independent of the decrease in mean arterial blood pressure.31
In agreement with these data, our analysis showed a significant reduction of albumin/creatinine ratio post LSG. We think that these changes may have a role in the potential protective impact of weight-reduction associated LSG on CKD. Moreover, the benefit of LSG is that the weight reduction is kept for a long time compared to weight-loss achieved by lifestyle changes alone.
The impact of metabolic surgery on kidney functions is not well characterized.32 Bariatric operations can prohibit kidney function deterioration by improving GFR in obese patients.33 The present research exhibited a considerable amelioration in GFR after weight-loss surgery. This coincides with recent research that showed a notable resolution of the GFR in morbidly obese patients after LSG.34
Cystatin C is a substitutional method to evaluate the alterations in the GFR as it is not influenced by the lean body mass or weight reduction,35 however, dispute encircles serum cystatin C as a decisive method of measuring kidney function in cases with near-normal function.36
Our analysis showed no significant changes in the serum level of cystatin C one year after LSG. We think that more extensive studies for more prolonged periods are needed to confirm and elucidate these results.
It is worth mentioning that the current study has some limitations. First, this work did not study whether the ameliorated inflammatory condition foreruns the decrease in arterial blood pressure or whether the improved blood pressure foreruns the ameliorated inflammatory condition. Second, the present work has a relatively short period of follow-up. In addition, removing patients who did not complete one-year follow-up may have introduced a selection bias, favoring patients who do return for follow-up (and therefore may have better weight loss and resolution of comorbidities)
Further future studies, preferably sufficiently sized controlled studies, should be performed to unify the follow-up period and technique of bariatric surgery.
In conclusion, the influence of improvement of systemic and renal inflammatory states after LSG may positively affect the obesity-related renal disease by steering the adipokine levels towards anti-inflammatory profiles.
Novelty of Study
To our knowledge, this is the first prospective work addressing urinary cytokines in obese non-diabetic patients after LSG, and according to our understanding, this may be one of the most extensive studies within this field. Diabetes can distinctly result in kidney damage, and this is the cause we excluded this category of patients as this may be a strong confounding factor. Therefore, highlighting this research field might be considered an original, valuable aspect of the present study.
Disclosure
All authors declare no conflicts of interest for this work.
References
1. Goktas Z, Moustaid-Moussa N, Shen C, Boylan M, Mo H, Wang S. Effects of bariatric surgery on adipokine-induced inflammation and insulin resistance. Front Endocrinol (Lausanne). 2013;10(4):69.
2. Kany S, Vollrath JT, Relja B. Cytokines in inflammatory disease. Int J Mol Sci. 2019;20(23):6008. doi:10.3390/ijms20236008
3. Lewko WM, Oldham RK. Cytokines. In: Oldham RK, Dillman RO, editors. Principles of Cancer Biotherapy. Dordrecht: Springer; 2009.
4. Hunley TE, Ma L, Kon V. Scope and mechanisms of obesity-related renal disease. Curr Opin Nephrol Hypertens. 2010;19(3):227–234. doi:10.1097/MNH.0b013e3283374c09
5. Tam FW, Riser BL, Meeran K, Rambow J, Pusey CD, Frankel AH. Urinary monocyte chemoattractant protein-1 (MCP-1) and connective tissue growth factor (CCN2) as prognostic markers for progression of diabetic nephropathy. Cytokines. 2009;47(1):37–42. doi:10.1016/j.cyto.2009.04.001
6. Qureshi A, Frankel AH, Tam FWK. CCL18/PARC, a novel cytokine present in urine of diabetic patients, may be involved in regulation of inflammation and fibrosis in diabetic nephropathy. Am Soc Nephrol Renal Week. 2007.
7. Bruchfeld A, Carrero JJ, Qureshi AR, et al. Elevated serum macrophage migration inhibitory factor (MIF) concentrations in chronic kidney disease (CKD) are associated with markers of oxidative stress and endothelial activation. Mol Med. 2009;15(3–4):70–75. doi:10.2119/molmed.2008.00109
8. Hell E, Miller K. Criteria for selection of patients for bariatric surgery. Zentralbl Chir. 2002;127(12):1035–1037. doi:10.1055/s-2002-36375
9. Yermilov I, McGory ML, Shekelle PW, Ko CY, Maggard MA. Appropriateness criteria for bariatric surgery: beyond the NIH guidelines. Obesity (Silver Spring). 2009;17(8):1521–1527. doi:10.1038/oby.2009.78
10. Sjöström L, Lindroos AK, Peltonen M, et al.; Obese subjects study scientific group. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351(26):2683–2693. Swedish. doi:10.1056/NEJMoa035622
11. Kulick D, Hark L, Deen D. The bariatric surgery patient: a growing role for registered dietitians. J Am Diet Assoc. 2010;110(4):593–599. doi:10.1016/j.jada.2009.12.021
12. Hoyuela C. Five-year outcomes of laparoscopic sleeve gastrectomy as a primary procedure for morbid obesity: a prospective study. World J Gastrointest Surg. 2017;9(4):109–117. doi:10.4240/wjgs.v9.i4.109
13. Ahmed MH, Byrne CD. Bariatric surgery and renal function: a precarious balance between benefit and harm. Nephrol Dial Transplant. 2010;25(10):3142–3147. doi:10.1093/ndt/gfq347
14. Bueter M, Dubb SS, Gill A, et al. Renal cytokines improve early after bariatric surgery. Br J Surg. 2010;97(12):1838–1844. doi:10.1002/bjs.7264
15. Lee H, Lee S, Choue R. Obesity, inflammation and diet. Pediatr Gastroenterol Hepatol Nutr. 2013;16(3):143–152. doi:10.5223/pghn.2013.16.3.143
16. Baracho NCDV, Silveira KD, Rocha NP, et al. Urinary cytokine profiles according to the site of blockade of the renin-angiotensin system in nephrectomized rats. J Bras Nefrol. 2017;39(2):108–118. doi:10.5935/0101-2800.20170028
17. Li J, Tang Y, Tang PMK, et al. Blocking macrophage migration inhibitory factor protects against cisplatin-induced acute kidney injury in mice. Mol Ther. 2018;26(10):2523–2532. doi:10.1016/j.ymthe.2018.07.014
18. Andres-Hernando A, Dursun B, Altmann C, et al. Cytokine production increases and cytokine clearance decreases in mice with bilateral nephrectomy. Nephrol Dial Transplant. 2012;27(12):4339–4347. doi:10.1093/ndt/gfs256
19. Eisenhardt SU, Thiele JR, Bannasch H, Stark GB, Peter K. C-reactive protein: how conformational changes influence inflammatory properties. Cell Cycle. 2009;8(23):3885–3892. doi:10.4161/cc.8.23.10068
20. Wang Z, Nakayama T. Inflammation, a link between obesity and cardiovascular disease. Mediators Inflamm. 2010;2010:535918. doi:10.1155/2010/535918
21. Kones R. Rosuvastatin, inflammation, C-reactive protein, JUPITER, and primary prevention of cardiovascular disease–a perspective. Drug Des Devel Ther. 2010;4:383–413. doi:10.2147/DDDT.S10812
22. McDonald S, Maguire G, Duarte N, Wang XL, Hoy W. C-reactive protein, cardiovascular risk, and renal disease in a remote Australian aboriginal community. Clin Sci (Lond). 2004;106(2):121–128. doi:10.1042/CS20030186
23. Schraufstatter IU, Zhao M, Khaldoyanidi SK, DiScipio RG. The chemokine CCL18 causes maturation of cultured monocytes to macrophages in the M2 spectrum. Immunology. 2012;135(4):287–298. doi:10.1111/j.1365-2567.2011.03541.x
24. Eriksson HD, Petrus P, Gao H, et al. Adipose and circulating CCL18 levels associated with metabolic risk factors in women. J Clin Endocrinol Metab. 2016;101(11):4021–4029. doi:10.1210/jc.2016-2390
25. Forssmann U, Magert HJ, Adermann K, Escher SE, Forssmann WG. Hemofiltrate CC chemokines with unique biochemical properties: HCC-1/CCL14a and HCC-2/CCL15. J Leukoc Biol. 2001;70:357–366.
26. Kitagawa K, Wada T, Furuichi K, et al. Blockade of CCR2 ameliorates progressive fibrosis in kidney. Am J Pathol. 2004;165(1):237–246. doi:10.1016/S0002-9440(10)63292-0
27. Li JH, Tang Y, Lv J, et al. Macrophage migration inhibitory factor promotes renal injury induced by ischemic-reperfusion. J Cell Mol Med. 2019;23(6):3867–3877. doi:10.1111/jcmm.14234
28. Rojano-Rodríguez ME, Valenzuela-Salazar C, Cárdenas-Lailson LE, Romero Loera LS, Torres-Olalde M, Moreno-Portillo M. C-reactive protein level in morbidly obese patients before and after bariatric surgery. Rev Gastroenterol Mex. 2014;79(2):90–95. doi:10.1016/j.rgmx.2013.11.002
29. Serra A, Granada ML, Romero R, et al. The effect of bariatric surgery on adipocytokines, renal parameters, and other cardiovascular risk factors in severe and very severe obesity: 1-year follow-up. Clin Nutr. 2006;25(3):400–408. doi:10.1016/j.clnu.2005.11.014
30. de Jong PE, Verhave JC, Pinto-Sietsma SJ, Hillege HL, PREVEND study group. Obesity and target organ damage: the kidney. Int J Obes Relat Metab Disord. 2002;26(Suppl 4):S21–4. doi:10.1038/sj.ijo.0802213
31. Ritz E. Bariatric surgery and the kidney—much benefit, but also potential harm. Clin Kidney J. 2013;6(4):368–372. doi:10.1093/ckj/sfs161
32. Holcomb CN, Goss LE, Almehmi A, Grams JM, Corey BL. Bariatric surgery is associated with renal function improvement. Surg Endosc. 2018;32(1):276–281. doi:10.1007/s00464-017-5674-y
33. Kun L, Zou J, Zhibin Y, Jianzhong D, Han X. Laparoscopic sleeve gastrectomy improves glomerular filtration rate in morbidly obese patients with impaired kidney function. J Am Coll Surg. 2017;225(4):e3.
34. Li K, Zou J, Ye Z, et al. Effects of bariatric surgery on renal function in obese patients: a systematic review and meta-analysis. PLoS One. 2016;11(10):e0163907. doi:10.1371/journal.pone.0163907
35. Friedman AN, Strother M, Quinney SK, et al. Measuring the glomerular filtration rate in obese individuals without overt kidney disease. Nephron Clin Pract. 2010;116:c224–34. doi:10.1159/000317203
36. Prigent A. Monitoring renal function and limitations of renal function tests. Semin Nucl Med. 2008;38(1):32–46. doi:10.1053/j.semnuclmed.2007.09.003
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.