")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Changes in Depression Among Adolescents: A Multiple-Group Latent Profile Transition Analysis
Authors Li G, Liu J, Wen H, Shen Q
Received 19 September 2022
Accepted for publication 6 January 2023
Published 8 February 2023 Volume 2023:16 Pages 319—332
DOI https://doi.org/10.2147/PRBM.S390116
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Guangming Li,1,2 Juan Liu,2 Haiying Wen,3 Qiyun Shen4
1Key Laboratory of Brain, Cognition and Education Sciences, Ministry of Education, South China Normal University, Guangzhou, 510631, People’s Republic of China; 2School of Psychology, Center for Studies of Psychological Application, and Guangdong Key Laboratory of Mental Health and Cognitive Science, South China Normal University, Guangzhou, 510631, People’s Republic of China; 3Department of Fashion Design, Guangdong Province Technician College of Light Industry, Guangzhou, 510315, People’s Republic of China; 4Zhongshan Polytechnic, Zhongshan, 528404, People’s Republic of China
Correspondence: Guangming Li, Email [email protected]
Background: Depression of adolescents is an important public health problem. Persistent depression will become a huge hidden danger of individual mental health development. It is important to study the change mechanism of adolescents’ depression.
Methods: A total of 563 males and 739 females aged 11– 19 years reported their depression. 1302 adolescents participated in a short-term 6-month longitudinal study. They were contacted every three months for two follow-up tests (T2 and T3). Participants completed internet addiction test, self-rating anxiety scale and self-rating depression scale. Multiple-group latent profile transition analysis (MLPTA) was used to identify meaningful subgroups and transitions between groups across time. Covariates (anxiety and internet addiction) were used to analyze the influencing factors.
Results: The results showed that: (1) There are three categories of adolescents’ depression, namely no-depression group, low-depression-mountain group and low-depression-hill group. (2) The depression of the subjects showed a trend of improvement, but the proportion of low-depression-mountain group is relatively high at three time points (0.44, 0.59, and 0.30). (3) The transition probability between the low-depression-mountain group and the no-depression group is large, which suggests the low-depression-mountain group can easily convert into the no-depression group, but the transition probability from low-depression-hill group to other groups is relatively low and stable, which suggests the low-depression-hill group is not easily converted into the no-depression group. (4) Both anxiety and internet addiction affect the development of adolescents’ depression across three time points. Anxiety played a significant role in affecting female adolescents’ depression, while internet addiction played a significant role in affecting male adolescents’ depression.
Conclusion: This study demonstrated a transition pattern in adolescents’ depression. We should pay more attention to the low-depression-mountain group and try to do their mental health well. Adolescents’ Depression changes rapidly with anxiety and internet addiction for different genders, which suggests that some interventions are needed.
Keywords: adolescents, depression, multiple-group latent profile transition analysis, anxiety, internet addiction
Introduction
Adolescence is not only a period of individual physiological and psychological development, but also a period when the probability of individual emotional disorders and problem behaviors increases greatly.1,2 It is also a critical period to understand the pathological source and occurrence process of emotional disorders. Depression likely runs an entire clinical spectrum from mild to severe. There are genetic and neurobiological studies lending support to the notion that these conditions are not discrete categories but rather, have common biological underpinnings and may form at least part of a continuum or affective disorder spectrum.3 A survey of epidemic prevalence showed that up to 21.4% of the global population suffers from depressive symptoms that meet clinical diagnostic criteria.4 With depression projected to be the leading cause of death and disability worldwide by 2030, it has become a pressing public mental health issue. Studies have shown that individuals have a higher risk of depression in adolescence than in other periods.5,6 The prevalence of depression in children is less than 1%, while the rate is more than 4–5% in middle and late adolescence.7 At the same time, depression, as a typical internalization problem, usually does not pose a direct threat or harm to others like externalization problems such as attack and aggression, and it is not easy to be detected by parents, teachers, and researchers. For a long time, researchers have paid more attention to clinical depression symptoms. However, sub-clinical depression in children and adolescents is largely unexplored. Although early depressive symptoms in adolescents do not necessarily lead to depression in adulthood, many adult patients attribute depressive disorders to childhood or adolescent experiences when the cause is retrospective.8 Therefore, understanding the characteristics of the occurrence and development of depression during adolescence is particularly necessary for the maintenance of the mental health of adolescents.
Adolescents’ depression is influenced by many factors such as anxiety and internet addiction etc. Among them, anxiety and depression are highly comorbid.9,10 Due to the high correlation between anxiety and depression and their high co-occurrence in clinical samples, there are also differences in the order of occurrence and influence of individual anxiety and depression. Some longitudinal studies have shown that anxiety symptoms will appear before depressive symptoms. Children’s previous high levels of anxiety can significantly predict the increase in their depression levels over time. Most depressed adolescents have experienced anxiety disorders before their depressive symptoms occur.11 However, some researchers proposed different views. Moffitt et al12 found in a follow-up study that in some cases of depression, anxiety occurs before or at the same time of the occurrence of depression. Moreover, with the rapid development and popularization of the internet, internet addiction has also become an important factor that affects adolescents’ mood and even leads to depression. However, it is unclear whether internet addiction is the cause of depression or whether depression precedes the development of internet addiction. According to the social migration hypothesis, the substitution of online social communication for offline social interaction may lead to depression. Some studies have found that internet addiction can predict subsequent depression.13,14 However, Bryant and Zillmann15,16 proposed the emotion enhancement hypothesis, which assumes that individuals use media based on their emotions. To relieve stress, people who are depressed are more likely than others to participate in leisure activities, including watching TV, surfing the internet, and playing online games. Therefore, the relationship between depression and internet addiction is worthy of in-depth study.
There are gender differences in adolescents’ depression. Some cross-sectional and longitudinal studies have shown that there is no significant gender difference between childhood and adolescents’ depression.17–21 However, most studies have found that there are significant gender differences in the early depression of adolescents. Before puberty, boys had a higher level of depression than girls, and after puberty, the result was reversed.22 And some researchers have shown that women generally show more depressive symptoms than men, and this gender difference is more pronounced for adolescence.23 The results of the study on depressive symptoms of middle school students show that boys’ depression levels are generally higher than girls in terms of age and grade, and girls gradually show more depressive symptoms than boys in the later stages of childhood, and become more pronounced in adolescence. Another study pointed out that throughout adolescence, girls showed more obvious depressive moods and symptoms than boys.24,25
Previous longitudinal studies on adolescents’ depression mostly used growth curves to describe the development trajectory of individuals, such as the latent growth curve model, latent category growth curve model, and growth mixed model to study the development trend of adolescents’ depression trajectories throughout the measurement time point. The existing studies have examined and confirmed the heterogeneous trajectories of the development of depression in adolescents.2,20,21,26–31 These researchers have repeatedly found three depression-related development trajectories concerning the development and changes of depression in adolescents. The initial levels are low, medium, and high. However, there is still disagreement with the specific development patterns of these three trajectories, namely whether they will continue to rise, continue or decline over time. Latent transition analysis (LTA) is an individual-centered longitudinal data analysis method. It is a latent class analysis based on the longitudinal extension of a latent Markov model. It is applicable to analyze data where both explicit variables and latent variables are categorical. The LTA can divide the subjects into different latent categories according to the answer, and then explore the development and changes of the subjects’ categories over time.32 When the explicit variables are continuous data, it is more suitable to use latent profile analysis (LPA) to explain the association between continuous explicit indicators through the category of latent variables.33 Correspondingly, the LTA has also been extended to latent profile transition analysis (LPTA), which can simultaneously estimate latent classes at multiple time points and their development trends between time points.34 Previous studies have also confirmed that the LPTA can be used in longitudinal studies.34–36 Therefore, it is very meaningful to explore the development law of adolescents’ depression over time through the LPTA. If the LPTA is used to do a multiple-group analysis (eg, female and male), it is called as multiple-group latent profile transition analysis (MLPTA).37
At present, the researches on adolescents’ depression have achieved some results, but there are also some shortcomings: (1) Most studies focus on horizontal research, mainly discussing the current situation and influencing factors of teenagers’ depression, but few studies explore the development of adolescents’ depression from the perspective of longitudinal analysis.1,9,10 Relatively little attention has been paid to the heterogeneity of individual development. (2) For some longitudinal studies, the LPTA was used, but these studies did not examine the effects of groups, such as the effects of different genders.34,36 In fact, it is very important to examine the group effect. Most studies did not implement the MLPTA in the true sense because the effects of grouping were considered, which was insufficient. (3) Most studies did not explore the covariates of adolescents’ depression or the influencing factors of adolescents’ depression.38 In a sense, the interference effects of some influencing factors of adolescents’ depression cannot be ignored, and they are conducive to analyzing the main causes of adolescents’ depression. (4) Most researchers use the total score of the scale to classify the subjects, ignoring the performance of the subjects on various items.38,39 This classification method does not mine the information in depth, so we should further explore whether there are individuals or sub groups with different depression performance patterns.
The purpose of this paper is to analyze the latent classes, transition pattern and influencing factors of adolescents’ depression through MLPTA. This study explores the tendency of adolescents’ depression using the MLPTA to address three purposes: (1) Identifying the different latent classes of adolescents’ depression and their transition pattern; (2) Identifying the similarities and differences of the types and transition pattern of adolescents’ depression in male and female adolescents; (3) Exploring whether anxiety and internet addiction will affect the types and changes of depression in male and female adolescents.
Methods
Participants
Participants were a sample of Chinese adolescents (N = 1405, 52.0% females) between 11 and 19 years of age (M = 14.90; SD = 1.83) from three middle schools (17 classes) in an urban school district in South China. Of these, 1302 adolescents (92.7%; 563 males and 739 females) provided complete data at both Time 2 and Time 3. In this study, a total of 1302 middle school students were selected. Different classes had different students, and each class had about 60 students. They were contacted every three months for two follow-up tests (T2 and T3).
There is a certain degree of loss during the test. The reasons for the loss of subjects are as follows: (1) Absence of class on the day of the test; (2) Individual academic transfer or suspension; (3) The test is completed casually, and there are obvious overfills, omissions, and fill less. In this study, the data of all subjects participating in the three studies were taken as the research samples, with a total of 1302 people. During the three administrations (T1: the first administration; T2: the second administration; T3: the third administration). We conducted a series of missing analyses and the results showed that, at baseline (T1), adolescents who had complete data were more likely than those who had missing data to be females, χ2(1) = 12.021, p < 0.001, and to report a higher level of depression, t = −2.471, p = 0.016. There were no differences in gender for adolescents’ depression (t = 1.154, p = 0.248). Table 1 shows the detailed information of the participants.
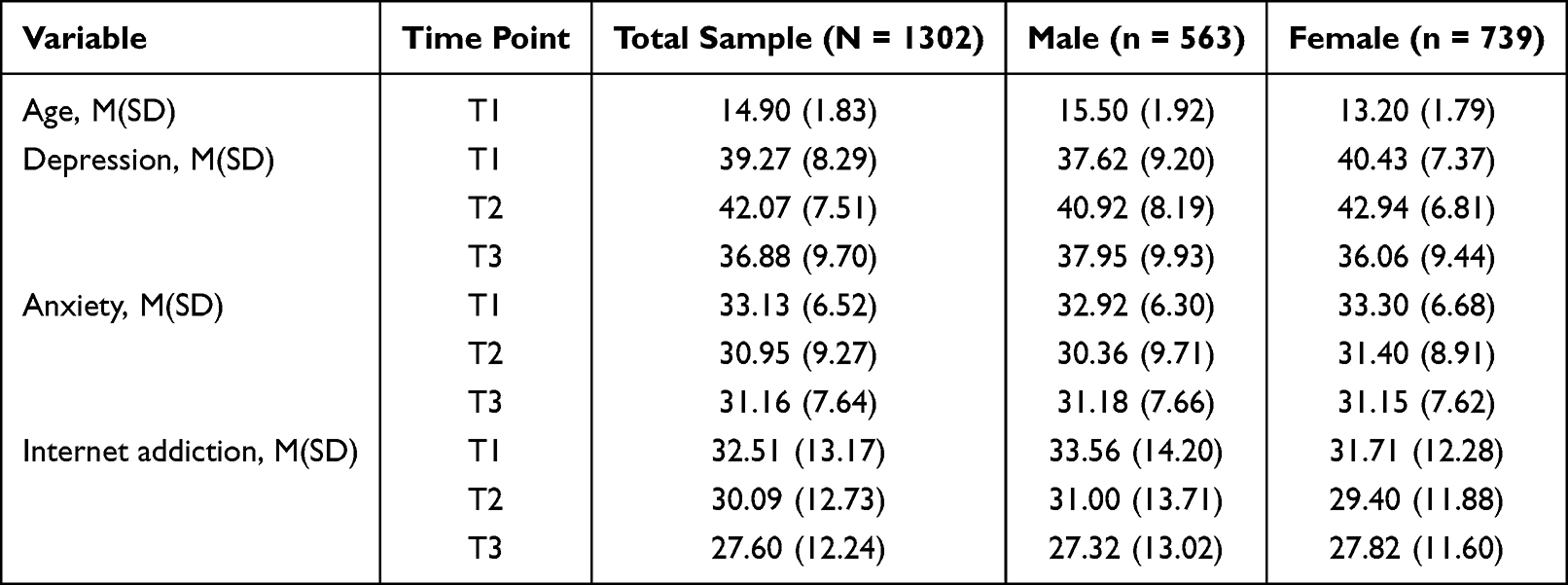 |
Table 1 Sample Characteristics |
Procedure
Students from a middle school were selected to participate in the test. All students completed the questionnaire in the classroom. The test was conducted every 3 months, and a total of three tests were conducted. We randomly selected three middle schools in urban areas in southern China, and then randomly chose 17 classes from these three middle schools. Different students were nested in different classes. Data were collected using paper/pencil tests in classrooms every three months for a total study span of six months. Each participant had a unique ID, and the same ID was used at all three waves. No participants changed classes or schools during these six months. The measurement sites were provided by the Academic Affairs Offices of the three middle schools. Researchers were trained before they administered the survey. Both schools and parents agreed the assessment.
The informed consent was obtained from all participants and their parents. All participants were voluntary and adequately informed of the aims, methods, sources of funding, any possible conflicts of interest, institutional affiliations of the researcher, the anticipated benefits and potential risks of the study etc. This study involving human subjects conformed to generally accepted scientific principles and was approved by the South China Normal University (SCNU) research ethics board (Institutional Review Board) who approved the experiments, including any relevant details and confirmed that all experiments were performed in accordance with relevant guidelines and regulations.
Measures
Self-Rating Depression Scale
Depression was measured using Zung’s Self-rating Depression Scale (SDS).40 SDS had 20 items (eg, “I feel down-hearted and blue.”), all of them rated on 4-point scales (1 = no or very little time; 2 = a small amount of time; 3 = a considerable amount of time; 4 = most or all of the time). Depression degree index (DDI) was derived by dividing the sum of the scores on the 20 items by the maximum possible score of 80 and expressed as a decimal. A score lower than 0.50 was recoded as “no depression”, 0.50–0.59 recoded as “minor to mild depression”, and 0.60–0.69 as “moderate to severe depression”, and higher than 0.69 recoded as “severe depression”.41 The Cronbach’s alpha coefficients of the depression scale were 0.795 at T1, 0.824 at T2, and 0.845 at T3.
Anxiety Self-Rating Scale
Anxiety was assessed using the Self-rating Anxiety Scale (SAS).42 SAS had 20 items (eg, I feel more nervous and anxious than usual), all of them rated on 4-point scales, ranging from “a little of the time” to “most of the time”. Items were reversely coded whenever necessary. The Cronbach’s alpha coefficients of the anxiety scale were 0.762 at T1, 0.779 at T2, and 0.744 at T3.
Adolescent Internet Addiction Scale
The 20-item Adolescent Internet Addiction Scale39 was used to evaluate the internet addiction status of the participants. The items were measured on a 5-point scale (1= rarely, 2= occasionally, 3= sometimes, 4= often, and 5= always). We took the sum of all these items, and higher scores indicated more serious degrees of internet addiction. It was considered to be internet addicted when the summed score was higher than 50. The Cronbach’s alpha coefficients of the scale were 0.871 at T1, 0.885 at T2, and 0.906 at T3.
Data Analyses
The MLPTA was conducted in Mplus 8.3 using maximum likelihood estimation with robust standard errors.37 Specifically, LPA was used performed to examine the complex patterns in adolescents’ depression over time. The optimal number of profiles was selected based on the following indices: Akaike Information Index (AIC), Bayesian Information Index (BIC), sample-corrected BIC (aBIC), entropy (Entropy), Lo-Mendell-Rubin likelihood ratio test (LMR-LRT), and Bootstrap-based likelihood ratio test (BLRT). Smaller values of AIC, BIC, and aBIC indicate better model fit. Entropy evaluates the classification quality of the model, and a value larger than 0.80 indicates that the classification accuracy rate exceeds 90%. LMR-LRT and BLRT (p < 0.05) indicates that the model of k categories is better than the model of k-1 categories. Based on the results of LPA, we examined the changes (ie, transition) in adolescents’ depression using MLPTA. We then examined the impact of anxiety and internet addiction on the latent state and transition probability using the R3STEP approaches with multinomial logistic regression modeling. The R3STEP approaches were implemented through the AUXILIARY command, which was used to analyze the role of latent variable influencing factors.43 We also considered the gender differences in these models.
Results
Common Method Deviation Test
We also conducted a series of unrotated principal component factor analysis on adolescents’ depression using Harman’s single factor test method.44 The results showed that there were 3 common factors with characteristic roots greater than 1 at T1, and 22.62% of the variance was explained by the first factor; at T2, there were 4 common factors with characteristic roots greater than 1, and 24.28% of the variance was explained by the first factor; at T3, there were 3 common factors with characteristic roots greater than 1, and 28.02% of the variance was explained by the first factor. If the explanatory power of a factor of the unrotated principal component factor analysis is larger than 40%, there would be a common method deviation.45 Therefore, we did not observe an obvious common method deviation in this study.
Invariance Test
Model fitting results of invariance test of three tests of adolescents’ depression are presented in Table 2.
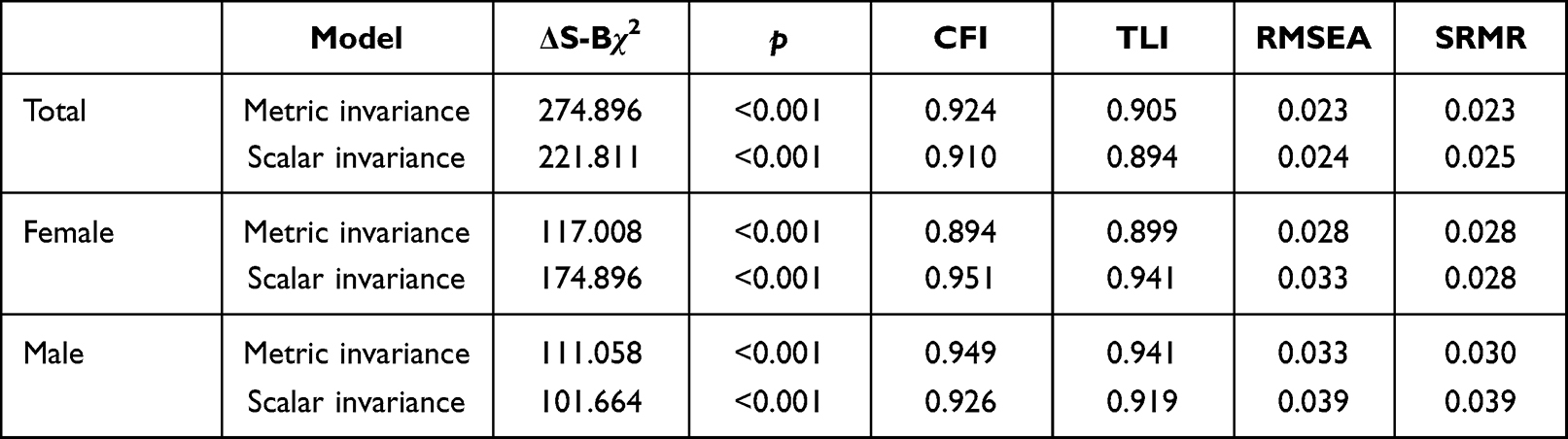 |
Table 2 Model Fitting Results of Invariance of Three Tests of Adolescents’ Depression |
According to Table 2, for all adolescents’ depression, metric invariance (ΔS-Bχ2 = 274.896, p<0.001, CFI = 0.924, TLI =0.905, RMSEA = 0.023, SRMR =0.023) and scalar invariance (ΔS-Bχ2 = 221.811, p<0.001, CFI = 0.910, TLI =0.894, RMSEA = 0.024, SRMR = 0.025), which fitting indicators of longitudinal invariance test were good for all sample.46 For female adolescents’ depression, metric invariance (ΔS-Bχ2 = 117.008, p<0.001, CFI = 0.894, TLI = 0.899, RMSEA = 0.028, SRMR = 0.028) and scalar invariance (ΔS-Bχ2 = 174.896, p<0.001, CFI = 0.951, TLI = 0.941, RMSEA = 0.033, SRMR = 0.028), which fitting indicators of longitudinal invariance test were good for female sample. For male adolescents’ depression, metric invariance (ΔS-Bχ2 = 111.058, p<0.001, CFI = 0.949, TLI = 0.941, RMSEA = 0.033, SRMR = 0.030) and scalar invariance (ΔS-Bχ2 = 101.664, p<0.001, CFI = 0.926, TLI = 0.919, RMSEA = 0.039, SRMR = 0.039), which fitting indicators of longitudinal invariance test were good for female sample.
To sum up, all adolescents’ depression, female adolescents’ depression, and male adolescents’ depression meet the longitudinal invariance test cross 3 time measurement, which indicates that this batch of data can be used for the MLPTA.
The Results of Total Sample
The LPA Results of Total Sample
We conducted LPA to examine one to five profile solutions to identify participants’ profile membership in depression. Fit indices are presented in Table 3.
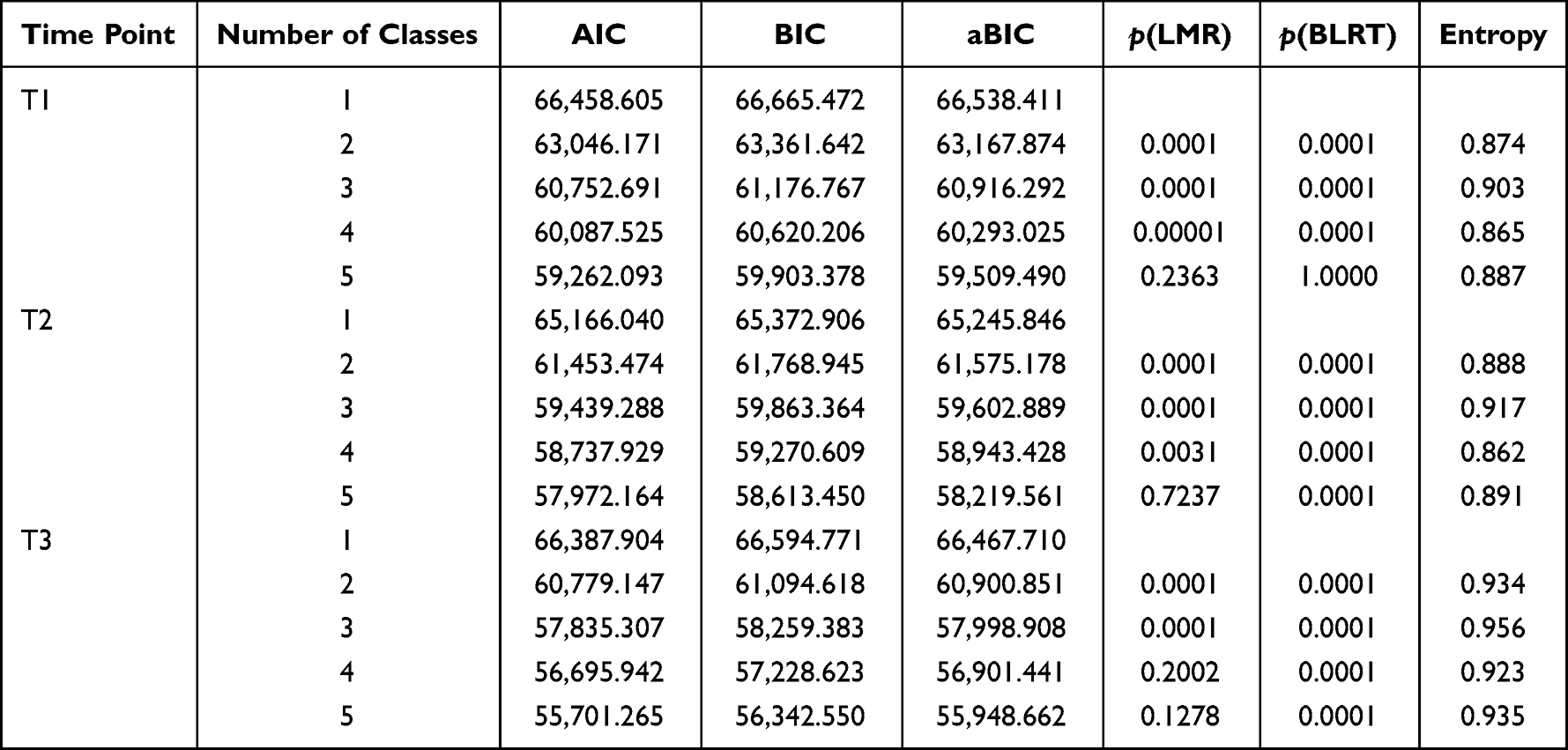 |
Table 3 Fitting Indicators of the Latent Profile Model of the Total Sample |
According to Table 3, at T1, the values of AIC, BIC, and aBIC decreased with the increase of the number of categories, and decreases became marginal when the profile number reached three. The entropy value of the 3-class model was highest (0.903), indicating a high level of classification precision. Similar solution patterns were observed at T2 and T3. We selected a 3-class solution as the best model. The distributions of the mean scores for the three profiles at three time points are displayed in Figures 1–3.
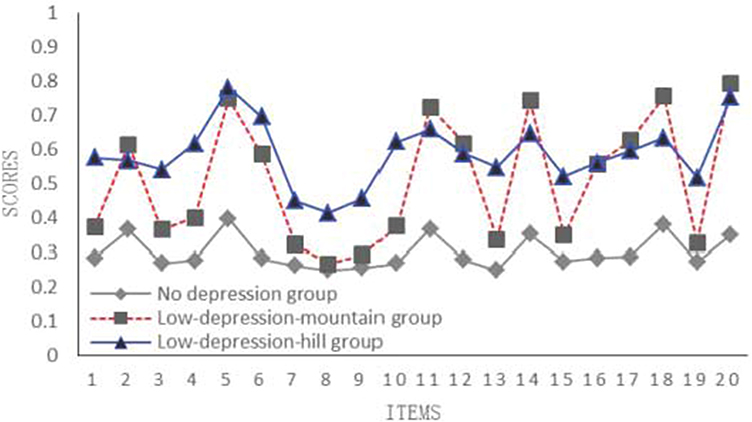 |
Figure 1 The average scores of 20 items of adolescents’ depression at T1 (n =1302). |
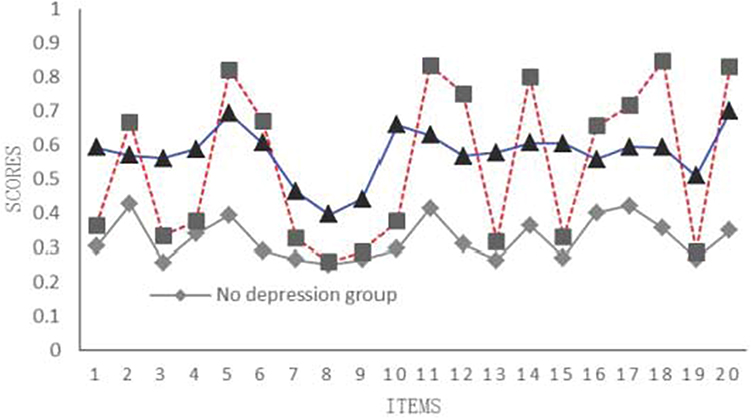 |
Figure 2 The average scores of 20 items of adolescents’ depression at T2 (n =1302). |
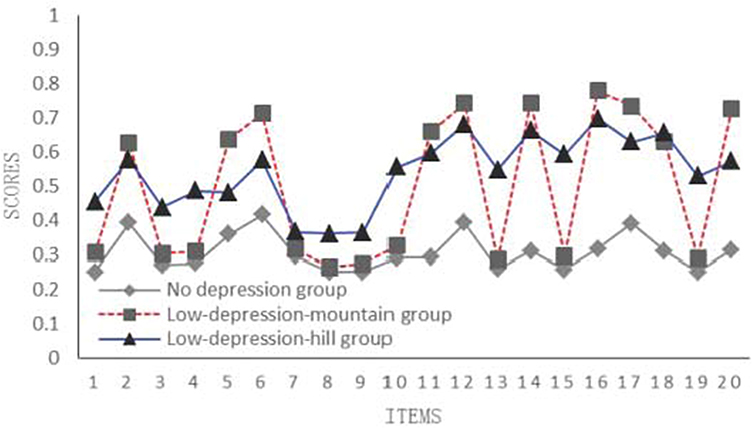 |
Figure 3 The average scores of 20 items of adolescents’ depression at T3 (n =1302). |
Specifically, at T1, some students followed low depression pattern, and the average scores on most items were close to 1, whose DDI was lower than 0.50, and were identified as “no-depression group” (DDI was 0.35 ± 0.07) (profile 1). Some students received high scores on some items, but low scores on other items, and were identified as “low-depression-mountain group” (DDI was 0.54 ± 0.09) (profile 2). The rest of the students were identified as “low-depression-hill group” (DDI was 0.54 ± 0.06) (profile 3). Like at T1, the similar patterns were observed at T2 and T3. At T2, the DDI of class 1 was 0.35 ± 0.07, the DDI of class 2 was 0.55 ± 0.09, and the DDI of class 3 was 0.55 ± 0.05. At T3, the DDI of class 1 was 0.37 ± 0.07, the DDI of class 2 was 0.54 ± 0.09, and the DDI of class 3 was 0.55 ± 0.06. Thus, we used the same labels for three profiles at T2 and T3.
The MLPTA Results of Total Sample
Table 4 shows the latent class probabilities at three time points. The latent class probability of “no-depression group” showed a downward trend at T2 (from 0.260 to 0.140) and then a significant increase at T3 (from 0.140 to 0.560). The latent class probability of “low-depression-mountain group” increased at T2 and then decreased at T3, whereas the latent class probability of “low-depression-hill group” decreased at both T2 and T3 (from 0.300 to 0.140).
 |
Table 4 Latent Class Probabilities of the Total Sample at Three Time Points |
The MLPTA allowed us to examine the changes in profile membership at three consecutive time points and to analyze the development direction and stability of adolescents’ depression. There were two transition matrices for data tracking at three-time points, namely time point 1–2 and time point 2–3. The results are shown in Table 5.
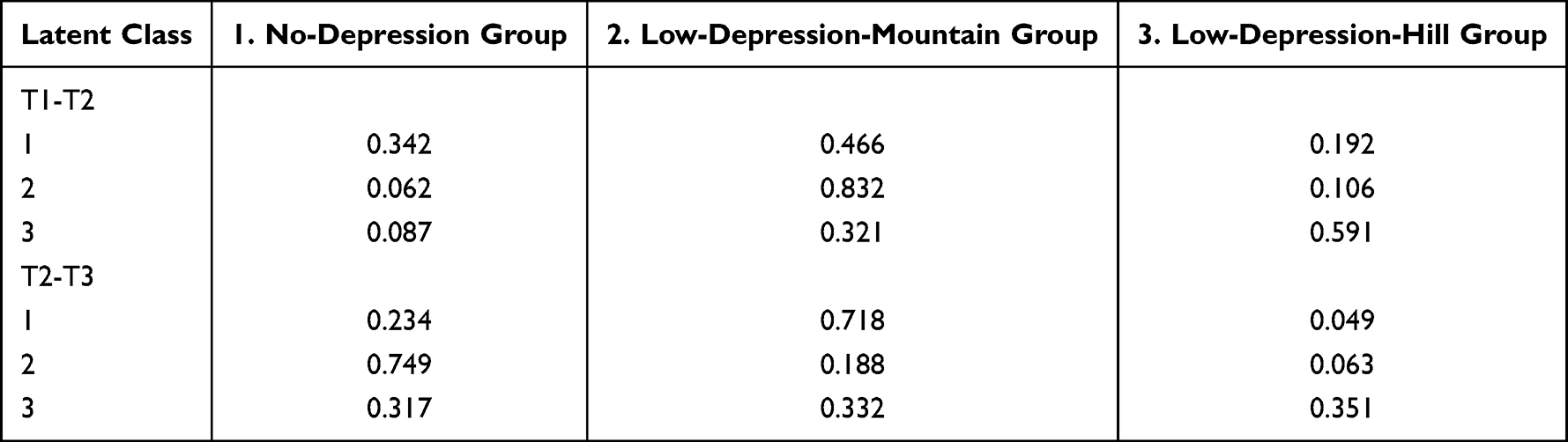 |
Table 5 The Latent Transition Probability Matrix of the Total Sample at Three Time Points |
According to Table 5, at time point 1–2, class 2 adolescents (“low-depression-mountain group”) showed greatest stability, with a 0.832 probability of remaining in the same class. Approximately 59.1% adolescents remained in class 3 (“low-depression-hill group”), but 32.1% adolescents transitioned to class 2. Class 1 (“no-depression group”) showed lowest stability, with only a 0.342 probability of remaining in the same class, a 0.466 probability of transition to class 2, and a 0.192 probability of transition to class 3.
At time point 2–3, the stability of three classes was moderate. The probability of class 1 remaining in the same class was only 0.234, and the probability of transiting to class 2 was 0.718. The probability of class 2 remaining in the same class was only 0.188, and the probability of transiting to class 1 was 0.749. The probability of class 3 remaining in the same class was 0.351, and the probability of transiting to class 2 was 0.332, the probability of transiting to class 1 was 0.317.
The Results of Influencing Factors of Adolescents’ Depression
The Influencing Factors of the Latent Class Probabilities of the Female and Male Group
The influencing factors of the latent class probabilities of the female group and male group shown in Table 6.
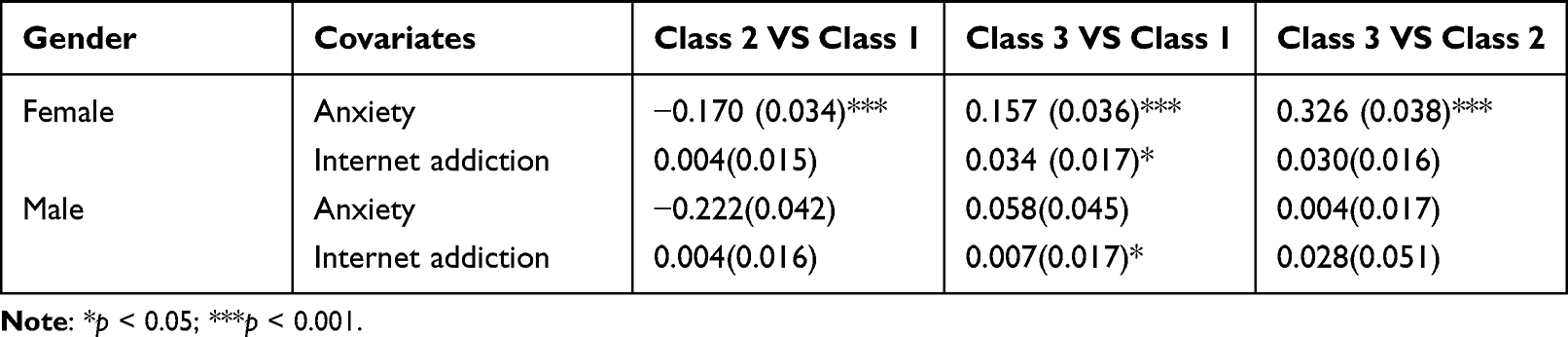 |
Table 6 The Influence of Covariates on the Latent Class Probabilities at T1 |
According to Table 6, in female group, the higher the degree of an individual anxiety is, the greater the probability of belonging to a group with a higher level of depression is. As for the factor of internet addiction, the higher the degree of an individual’s internet addiction, the greater the probability of belonging to the “low-depression-hill group” (class 3) compared to the “no-depression group” (class 1) (b = 0.034, p < 0.05).
In male group, anxiety does not affect the class membership of male group. Individuals with a deeper degree of internet addiction are more likely to belong to the “low-depression-hill group” (class 3) than the “no-depression group” (class 1) (b = 0.007, p < 0.05).
The Influencing Factors of the Latent Transition Probabilities for the Female and Male Group
The odds ratio (OR) of latent transition probabilities as a function of anxiety is shown in Table 7.
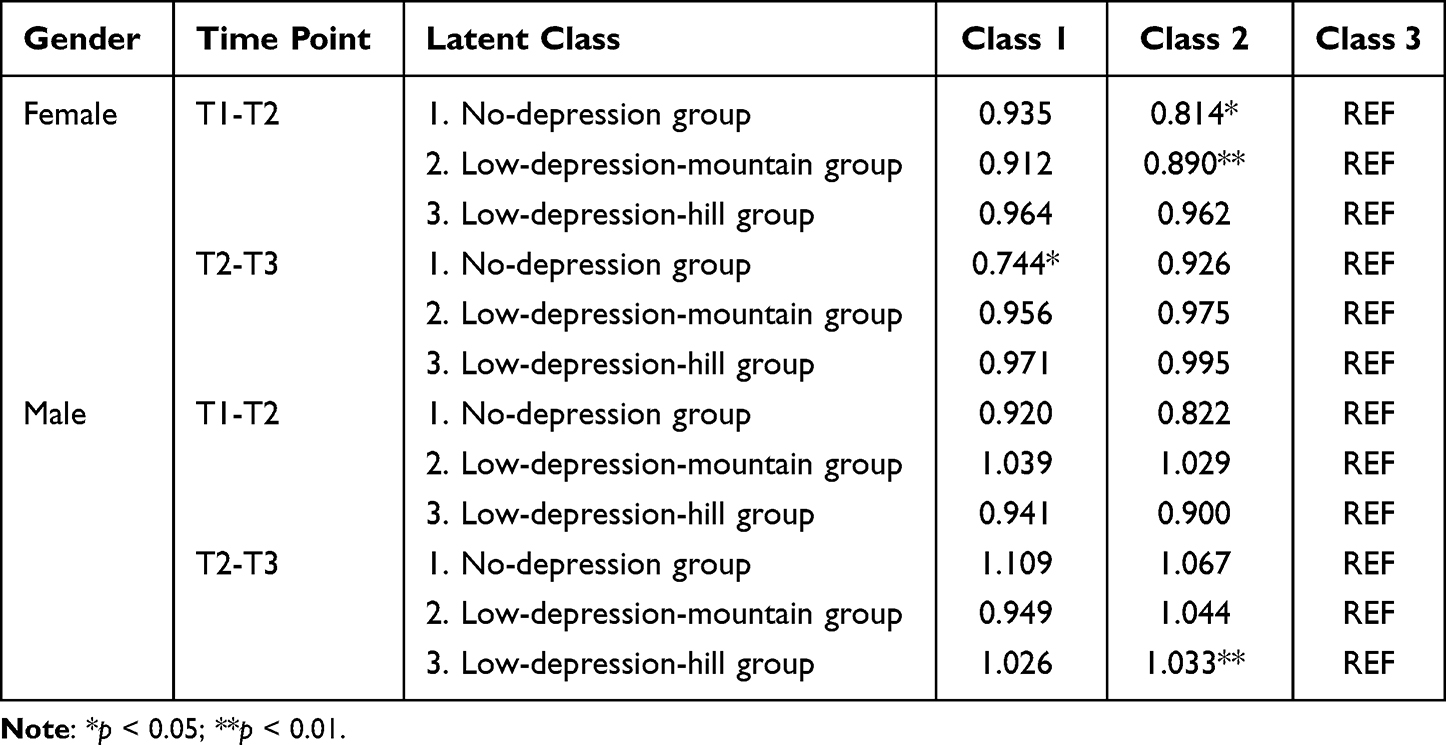 |
Table 7 The OR of Latent Transition Probabilities as a Function of Anxiety |
According to Table 7, in female group, as the degree of anxiety increases, individuals in the “no-depression group” (class 1) at time point 1 have a lower probability of transitioning to the “low-depression-mountain group” (class 2) than the “low-depression-hill group” (class 3) (OR = 0.814); individuals in the “low-depression-mountain group” (class 2) are also less likely to switch to their own group than the “low-depression-hill group”(class 3) (OR = 0.890). At time point 2, individuals in the “no-depression group”(class 1) have a lower probability of transitioning to their own group than the “low-depression-hill group”(class 3) (OR = 0.744). That is, the higher the degree of anxiety, the easier it is to change to the “low-depression-hill group”(class 3).
In male group, under the influence of anxiety level, individuals in the “low-depression-hill group” at time point 2 are more likely to switch to the “low-depression-mountain group” (OR = 1.033). But overall, anxiety has little effect on the transition of depression in male adolescents.
The OR of latent transition probabilities as a function of internet addiction is shown in Table 8.
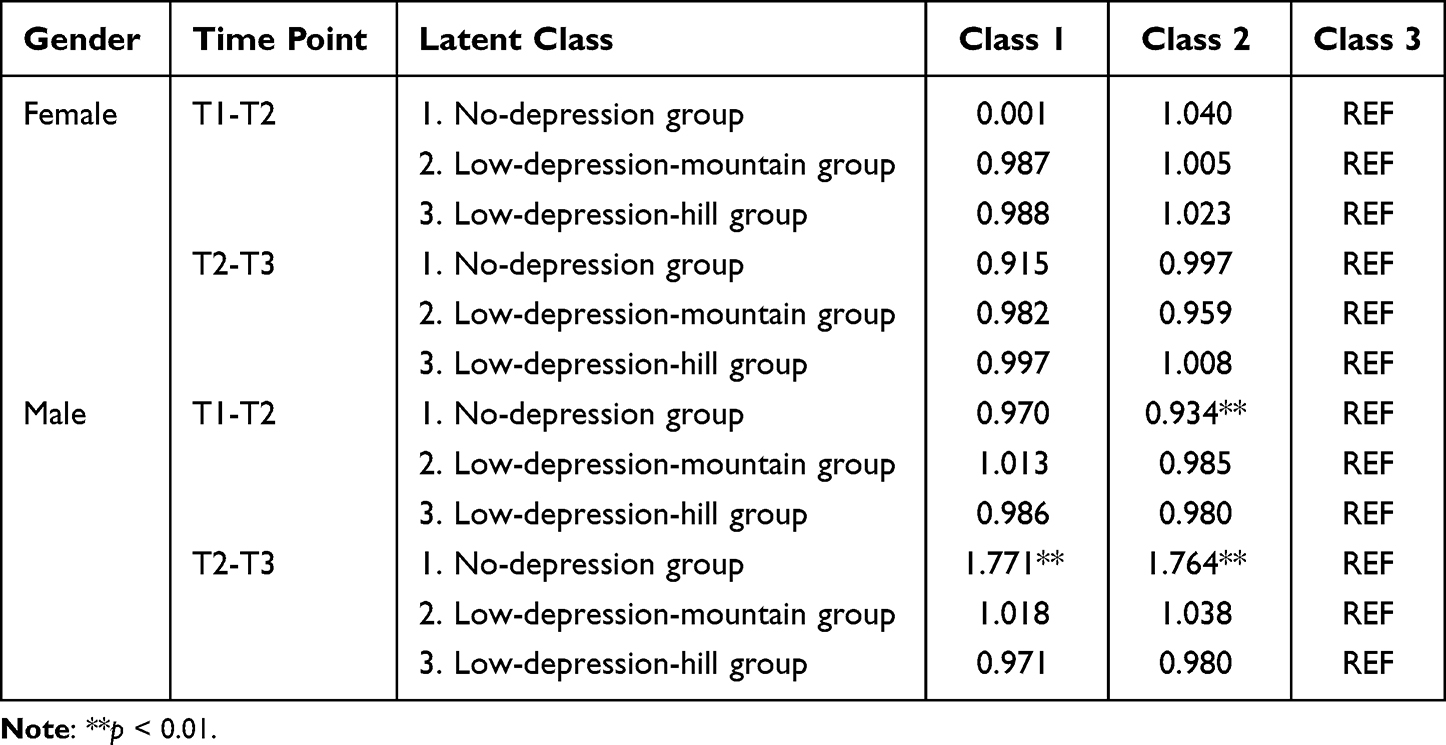 |
Table 8 The OR of Latent Transition Probabilities as a Function of Internet Addiction |
According to Table 8, in female group, the level of internet addiction does not affect the depression transition of female adolescents. In male group, under the influence of internet addiction, individuals in the “no-depression group” (class 1) at time point 1, compared to the “low-depression-hill group”(class 3), have a lower probability of switching to the “low-depression-mountain group”(class 2) (OR = 0.934). At time point 2, individuals in the “no-depression group”(class 1) will have an increased probability of staying in their own class and transferring to the “low-depression-mountain group”(class 2) (OR = 1.771, OR = 1.764). Overall, the influence of internet addiction on the transition of male adolescents’ depression classes is not stable.
Discussions
The Latent Classes of Adolescents’ Depression
In terms of the number of classes, this study uses a latent profile model to classify three consistent classes for the total sample and the two subsamples of male and female adolescents at three-time points and named them as the “no-depression group”, “low-depression-mountain group” and “low-depression-hill group” according to the scores and patterns. The number of classes we extracted is in line with the results of some previous researches conducted among children,47 adults48 and the elderly.49,50 However, previous research identified the high depressive symptom group or the severe depression group, in this study, the group with the most severe depressive symptoms was “low-depression-mountain group”. This may be because previous studies mainly used latent class models, while this study used latent profile models to classify adolescents’ depression levels in more detail. At the same time, there are other differences in the use of scales and the age of participants.
In terms of the proportion of depression classes at the initial time point, whether it is the total sample or the two subsamples, the “low-depression-mountain group” has always had a high proportion (overall: 44%; female: 46%; male: 44%). This may because adolescence is a critical period of individual’s physical and psychological development, the adolescents’ self-cognition and external cognition are more prone to fluctuate, and their psychological state is not particularly stable,51 so some groups are always in the susceptible state of psychological crisis. In previous studies, this part of the group will also be named the transition group or the susceptible group, which is a group that is worthy of attention. If the correct guidance and sufficient care are not given, it is very likely to change to a higher depression group. The proportions of the “no-depression group” and “low-depression-hill group” of male adolescents were 31% and 25%, respectively, which were lower than the proportions of female adolescents, which were 22% and 32%, respectively. This shows that the initial level of depression in the male group is lower than that of the female, which is consistent with the results of previous studies.22
The Changing Patterns of Adolescents’ Depression
As for the changing trend of adolescents’ depression, the results of the total sample showed that the “low-depression-mountain group” had always maintained a proportion of more than 30%, showing greater stability. The proportion of the “no-depression group” increased, and the proportion of the “low-depression-hill group” decreased. This indicated that the depression of subjects had been relieved over the 6 months. Although adolescents face pressure from academics, family, interpersonal communication, etc., adolescence is also an important period for improving self-efficacy. Adolescents with high levels of emotional regulation have the ability to effectively regulate negative emotions, even if they face setback.52,53
In terms of specific changing trend, both of the “no-depression group” and the “low-depression-mountain group” have undergone a significant change to the other group at time 2–3. In the “low-depression-hill group”, a part of the proportion remained stable in its own group. According to Beck’s cognitive model of depression, the root cause of depressive symptoms lies in the individual’s stable irrational cognitive schema.54 As long as the schema is not broken or reconstructed, it will continue to interact negatively with life and perpetuate the depressive state. Therefore, relevant workers should pay more attention to this group, and strengthen the identification and intervention of it.
In the two subsamples, in the “no-depression group”, the proportion of female adolescents increased more than that of male adolescents (female: 22%-62%; male: 31–49%); for the “low-depression-hill group”, female adolescents had a greater decline than male adolescents (female: 25%-10%; male: 32–16%). It shows that although the initial depression status of male adolescents is better than that of females, female adolescents show better resilience and regulation ability. Previous studies have shown that throughout adolescence, female adolescents report higher levels of depression than male adolescents.24 At the same time, although females are more prone to suffer from depression, they will show better mental resilience to regulate their emotions due to their mental maturity.55 In the “low-depression-mountain group”, the risk of females is on a downward trend, while the risk of male adolescents remained even, which shows that male adolescents have a greater risk of depression during adolescence.
The Influence of Anxiety and Internet Addiction on Adolescents’ Depression
As for the influence of anxiety and internet addiction on adolescents’ depression, anxiety is an obvious risk factor for depression in female adolescents. The level of depression will increase as the degree of anxiety deepens. And the higher the degree of anxiety, female adolescents are more likely to change to higher depression. The effect of anxiety on the depression level of male adolescents is not obvious. In the sample of this study, female adolescents have higher average anxiety than male adolescents. At the same time, it has been found in previous studies that female adolescents are generally more anxious than male adolescents.56 Anxiety and depression are often two factors of comorbidity. Generally speaking, the higher the degree of anxiety is, the higher the degree of depression is. The results of this study are consistent with previous studies.9,10
For male and female adolescents, their depression levels will increase with the degree of internet addiction, which indicates that internet addiction is a risk factor for adolescents’ mental health. With the development of time, internet addiction only has an impact on the depressive transition of male adolescents, and it may shift to a higher degree of depression under the influence of internet addiction. Male adolescents are more likely to be depressed because they are addicted to the internet.57 This is because, in the study of internet addiction, scholars have used cross-sectional and longitudinal studies to find that there are gender differences in internet addiction among adolescents. And male adolescents are more likely to become addicted to the internet than female adolescents. This may because of cultural differences; male adolescents are reluctant to talk to others when facing psychological conflicts and confusion and choose more self-resolving methods. The internet is more likely to become a way for male adolescents to resolve conflicts and confusions.58 And internet addiction will affect the development of adolescents’ physical and mental health, even cause harm to their study life and interpersonal communication. Therefore, male adolescents with higher levels of internet addiction are more likely to fall into depression.
Therefore, anxiety and internet addiction are both susceptible factors for depression in adolescents. Adolescents should strengthen their recognition and regulation of negative emotions. However, for the differences between male adolescents and female adolescents, educators should take corresponding measures. For female adolescents, they should pay more attention to their emotional performance, and provide timely psychological counseling to relieve anxiety. And attention should also be paid to the internet addiction that male adolescents may exhibit. A variety of psycho-behavioral therapies can be integrated to intervene in high internet addicts promptly, and clinical drug treatment should be used when it is necessary.
In the study, 1302 adolescents participated in a short-term 6-month longitudinal study with a total of three tests. Participants completed self-rating depression scale, self-rating anxiety scale and internet addiction test. The MLPTA is used. A latent profile analysis was conducted on adolescents’ depression items. According to the model fitting indicators, a latent profile model with the optimal latent class number was selected. The model fitting indicators mainly use the information evaluation indicator AIC, BIC, aBIC, p (LMR), p (BLMR), and entropy. Based on the optimal number of latent classes, the three time points’ items were simultaneously included in a latent transition model to analysis. Anxiety and depression were taken as covariates and included in latent transition model respectively. Multivariate logistic regression was used to explore the influence of covariates on transition probability.
The innovation of this study is to use the method of MLPTA to explore the development trend and influencing factors of adolescents’ depression from the perspective of longitudinal research. Firstly, compared with similar longitudinal studies, the focus has shifted from the overall trend to the heterogeneous development of sub groups, and more attention has been paid to the transition pattern of different latent categories of adolescents’ depression. Secondly, a new longitudinal data analysis method, namely MLPTA, is adopted, and the observed explicit indicators are expanded from category variables to continuous variables. This method can be widely used in the longitudinal research of continuous data. Last but not least, the research results show that there are three latent categories of adolescents’ depression, namely no-depression group, low-depression-mountain group and low-depression-hill group. Without any intervention, the proportion of people in low-depression-mountain group has strong stability. Nonetheless, the low-depression-mountain group is more likely to be transformed into the no-depression group, and no-depression group is more likely to be transformed into the low-depression-mountain group. Therefore, it is necessary to timely intervene the low-depression-mountain group to promote adolescents’ depression development in a better direction.
Limitations
Although this study discussed the development trend and influencing factors of depression for adolescents from the perspective of longitudinal study, there are still many limitations. First of all, due to the short time interval of the survey, only a 6-month follow-up was carried out to obtain the short-term development trend of adolescent internet addiction, which affected the popularization of the research results. A short-term time span (ie, nine months in this study, with a 3-month interval between data time points) may have limited the capacity to precisely capture the developmental trajectory courses for adolescents. Secondly, the subjects of this study are middle school students, but college students are not involved. Nonetheless, in some researches about depression, many researchers classify college students as adolescents. Thirdly, due to the length of the article, the results of latent class probabilities of the total sample at three time points were not presented and compared by gender. There are other covariates that can be discussed together, such as academic burden, coping style, life satisfaction, etc. However, due to the limited space, the author did not study other factors, which can be further explored in the future. Last but not least, except for using the MLPTA method in this study, future researchers are strongly suggested to use Online Photovoice (OPV) to conduct research on the same or similar topics. The OPV was popular in some researches in recent years.59–61
Implications and Conclusions
This paper showed that there were three types of depression among adolescents, namely, no-depression group, low-depression-mountain group, and low-depression-hill group. During the 6-month measurement period, the depression of the subjects showed a trend of improvement, but the proportion of low-depression-mountain group was relatively high at three time points. The low-depression-mountain group could easily convert into the no-depression group, but the low-depression-hill group was not easily converted into the no-depression group. This shows that doing a good job in the mental health of the low-depression-mountain group is a key to prevent adolescents’ depression. The effects of covariates on adolescents’ depression showed that both anxiety and internet addiction affect the development of adolescents’ depression. Anxiety played a significant role in affecting female adolescents’ depression, while internet addiction played a significant role in affecting male adolescents’ depression. Depression changes rapidly in adolescents with some influencing factors such as anxiety and internet addiction, which suggests that tailored intervention is needed to deal with adolescents’ depression for different genders. For female adolescents, we should strengthen the identification and regulation of negative emotion. For male adolescents, we can integrate a variety of psychological behavioral therapies to prevent and intervene in their internet addiction.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported in part by Grant No. 2021A1515012516 from the Natural Science Foundation of Guangdong Province, Grant No. 2021wtscx020 from the Characteristic Innovation Project of Colleges and Universities in Guangdong Province (Philosophy and Social Science of Educational Science), and Grant No. 2018GXJK415 from the Educational Science “13th Five-Year Plan” University Scientific Research Projects of Guangdong Province.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Luo D, Tan L, Shen D, et al. Characteristics of depression, anxiety, impulsivity, and aggression among various types of drug users and factors for developing severe depression: a cross-sectional study. BMC Psychiatry. 2022;22:1–12. doi:10.1186/s12888-022-03933-z
2. Mezulis A, Salk R, Shibley-Hyde J, Priess-Groben HA, Simonson JL. Affective, biological, and cognitive predictors of depressive symptom trajectories in adolescence. J Abnorm Child Psychol. 2014;42(4):67–89. doi:10.1007/s10802-013-9812-2
3. Qin XN, Donovan YL, Kuan TC. Reimagining the spectrum of affective disorders. Bipolar Disord. 2020;22(6):638–639. doi:10.1111/bdi.12960
4. Kessler RC, Angermeyer M, Anthony JC, Graaf RD, Demyttenaere K, Gasquet I. Lifetime prevalence and age-of-onset distributions of mental disorders in the world health organization’s world mental health survey initiative. World Psychiatry. 2007;6(3):39–51.
5. Lépine JP, Briley M. The increasing burden of depression. Neuropsychiatr Dis Treat. 2011;7(1):3–7. doi:10.2147/NDT.S19617
6. Merikangas KR, He JP, Burstein M, Swanson SA, Avenevoli S, Cui L. Lifetime prevalence of mental disorders in US. adolescents: results from the national comorbidity survey replication--adolescent supplement (NCS-A). J Am Acad Child Adolesc Psychiatry. 2010;49(10):980–989.
7. Costello EJ, Debra LF, Psych AA. 10-year research update review: the epidemiology of child and adolescent psychiatric disorders: methods and public health burden. J Am Acad Child Adolesc Psychiatry. 2006;45(1):8–25. doi:10.1097/01.chi.0000184929.41423.c0
8. Mesman J, Bongers IL, Koot HM. Preschool developmental pathways to preadolescent internalizing and externalizing problems. J Child Psychol Psychiatry. 2001;42(5):679–689. doi:10.1111/1469-7610.00763
9. Risal A, Manandhar K, Linde M, Steiner TJ, Holen A. Anxiety and depression in Nepal: prevalence, comorbidity and associations. Bmc Psychiatry. 2016;16(1):1–9. doi:10.1186/s12888-016-0810-0
10. Wiethoff K, Bauer M, Baghai TC, Möller HJ, Adli M. Prevalence and treatment outcome in anxious versus no anxious depression: results from the German algorithm project. J Clin Psychiatry. 2010;71(8):1047–1054. doi:10.4088/JCP.09m05650blu
11. Cole DA, Peeke LG, Martin JM, Truglio R, Seroczynski AD. A longitudinal look at the relation between depression and anxiety in children and adolescents. J Consult Clin Psychol. 1998;66(3):451–460. doi:10.1037/0022-006X.66.3.451
12. Moffitt TE, Harrington HL, Caspi A, et al. Depression and generalized anxiety disorder: cumulative and sequential comorbidity in a birth cohort followed prospectively to age 32 years. Arch Gen Psychiatry. 2007;64(6):651–660. doi:10.1001/archpsyc.64.6.651
13. Dalbudak E, Evren C, Aldemir S, Coskun KS, Ugurlu H, Yildirim FG. Relationship of internet addiction severity with depression, anxiety, and alexithymia, temperament and character in university students. Cyberpsychol Behav Soc Netw. 2013;16(4):272–278. doi:10.1089/cyber.2012.0390
14. Park S, Hong K, Park EJ, Ha KS, Yoo HJ. The association between problematic internet use and depression, suicidal ideation and bipolar disorder symptoms in Korean adolescents. Aust N Z J Psychiatry. 2013;47(2):153–159. doi:10.1177/0004867412463613
15. Bryant J, Zillmann D. Using television to alleviate boredom and stress: selective exposure as a function of induced excavational states. J Broadcast. 1984;28(1):1–20. doi:10.1080/08838158409386511
16. Bryant J, Zillmann D. Responding to the Screen: Reception and Reaction Processes. New York, NY: Lawrence Erlbaum Associates; 1991.
17. Chen X, Liu M, Li D. Parental warmth, control, and indulgence and their relations to adjustment in Chinese children: a longitudinal study. JFP. 2000;14(3):401–419. doi:10.1037/0893-3200.14.3.401
18. Liu F. The structure of the Child Depression Scale and the characteristics of the development of children and adolescents. Psychol Devolp Educ. 1997;13(2):57–61.
19. Yang D, Wang Y, Dong Q. Depression and anxiety of junior high school students: structure and developmental characteristics. Psychol Devolp Educ. 2000;9(3):12–17.
20. Hou J, Chen Z. The developmental trajectory of adolescent depression: defining subgroups and their influencing factors. Acta Psychologica Sinica. 2016;48(8):957–968. doi:10.3724/SP.J.1041.2016.00957
21. Cao C. The effects of dopamine system genes, motherhood, and peer abuse on the trajectory of early and mid-term depression in adolescents Master’s thesis. Shanghai: East China Normal University; 2016.
22. Steinberg L. Adolescence.
23. Hankin BL, Abramson LY, Moffitt TE, Silva PA, Mcgee R, Angell KE. Development of depression from preadolescence to young adulthood: emerging gender differences in a 10-year longitudinal study. J Abnorm Psychol. 1998;107(1):128–140. doi:10.1037/0021-843X.107.1.128
24. Roza SJ, Hofstra MB, Jan V, Verhulst FC. Stable prediction of mood and anxiety disorders based on behavioral and emotional problems in childhood: a 14-year follow-up during childhood, adolescence, and young adulthood. Am J Psychiatry. 2003;160(12):2116–2121. doi:10.1176/appi.ajp.160.12.2116
25. Zahn-Waxler C, Shirtcliff EA, Marceau K. Disorders of childhood and adolescence: gender and psychopathology. Annu Rev Clin Psychol. 2008;4(1):275–303. doi:10.1146/annurev.clinpsy.3.022806.091358
26. Brendgen M, Wanner B, Morin AJS, Vitaro F. Relations with parents and with peers, temperament, and trajectories of depressed mood during early adolescence. J Abnorm Child Psychol. 2005;33(5):579–594. doi:10.1007/s10802-005-6739-2
27. Castelao CF, Kroner-Herwig B. Different trajectories of depressive symptoms in children and adolescents: predictors and differenc2017es in girls and boys. J Youth Adolesc. 2013;42(8):1169–1182. doi:10.1007/s10964-012-9858-4
28. Chaiton M, Contreras G, Brunet J, Sabiston CM, O’Loughlin J. Heterogeneity of depressive symptom trajectories through adolescence: predicting outcomes in young adulthood. J Can Acad Child Adolesc Psychiatry. 2013;22(2):96–106.
29. Dekker MC, Ferdinand RF, Lang ND, Bongers IL, Verhulst FC. Developmental trajectories of depressive symptoms from early childhood to late adolescence: gender differences and adult outcome. J Child Psychol Psychiatry. 2010;48(7):657–666. doi:10.1111/j.1469-7610.2007.01742.x
30. Duchesne S, Ratelle CF. Attachment security to mothers and fathers and the developmental trajectories of depressive symptoms in adolescence: which parent for which trajectory? J Youth Adolesc. 2014;43(4):641–654. doi:10.1007/s10964-013-0029-z
31. Sabiston CM, O’Loughlin E, Brunet J, et al. Linking depression symptom trajectories in adolescence to physical activity and team sports participation in young adults. Prev Med. 2013;56(23):95–98. doi:10.1016/j.ypmed.2012.11.013
32. Wang B, Zhang M, Zhang J, Hu J, You J, Liang Y. Analysis of potential changes in adolescents’ self-harm behavior: a longitudinal study. J Psychol Sci. 2015;38(6):90–98.
33. Wang M, Deng Q, Bi X, Ye H, Yang W. Performance of the entropy as an index of classification accuracy in latent profile analysis: a Monte Carlo simulation study. Acta Psychologica Sinica. 2017;49(11):1473–1482. doi:10.3724/SP.J.1041.2017.01473
34. Fryer H, Luke K. (latent) transitions to learning at university: a latent profile transition analysis of first-year Japanese students. Higher Educ. 2017;73(3):1–19. doi:10.1007/s10734-016-0094-9
35. Bourchtein E, Langberg JM, Owens JS, Evans SW, Perera RA. Is the positive illusory bias common in young adolescents with ADHD? A fresh look at prevalence and stability using latent profile and transition analyses. J Abnorm Child Psychol. 2017;45(6):1063–1075. doi:10.1007/s10802-016-0248-3
36. Flaig M, Simonsmeier BA, Mayer AK, Rosman T, Gorges J, Schneider M. Reprint of “Conceptual change and knowledge integration as learning processes in higher education: a latent transition analysis”. Learn Individ Differ. 2018;66:92–104. doi:10.1016/j.lindif.2018.07.001
37. Muthén LK, Muthén BO. Mplus User’s Guide.
38. Kojima R, Shinohara R, Akiyama Y, Yokomichi H, Yamagata Z. Temporal directional relationship between problematic internet use and depressive symptoms among Japanese adolescents: a random intercept, cross-lagged panel model. Addict Behav. 2021;120:1–6. doi:10.1016/j.addbeh.2021.106989
39. Young KS, De Abreu CN. Internet Addiction: A Handbook and Guide to Evaluation and Treatment. New Jersey, NJ: John Wiley & Sons; 2010.
40. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12(1):63–70. doi:10.1001/archpsyc.1965.01720310065008
41. Zhang C, Xue Y, Zhao H. Prevalence and related influencing factors of depressive symptoms among empty-nest elderly in Shanxi, China. J Affect Disord. 2019;245(14):750–756. doi:10.1016/j.jad.2018.11.045
42. Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1965;12(6):371–379. doi:10.1016/S0033-3182(71)71479-0
43. Vermunt JK. Latent class modeling with covariates: two improved three-step approaches. Polit Anal. 2010;18:450–469. doi:10.1093/pan/mpq025
44. Podsakoff PM, Mackenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879–903. doi:10.1037/0021-9010.88.5.879
45. Zhou H, Long L. The statistical test and control method of common method deviation. Adv Psychol Sci. 2004;12(6):942–950.
46. Wang M. Latent Variable Modeling Using Mplus. Chongqing university press; 2014.
47. Herman KC, Daniel C, Reinke WM, Rick O, Lori B, Elizabeth MF. Using latent profile and transition analyses to understand patterns of informant Ratings of child depressive symptoms. J Sch Psychol. 2018;69(3):84–99. doi:10.1016/j.jsp.2018.05.004
48. Liao Y, Lian R. Analysis of the potential transformation of adult depressive symptoms: a four-year follow-up study. Chin J Clin Psychol. 2020;28(3):518–522.
49. Yuan Y, Lapane KL, Rothschild AJ, Ulbricht CM. Changes in depressive symptoms and cognitive impairment in older long-stay nursing home residents in the USA: a latent transition analysis. Aging Ment Health. 2020;12(7):1–10.
50. Ni Y, Tein J, Zhang M, Yang Y, Wu G. Changes in depression among older adults in China: a latent transition analysis. J Affect Disord. 2017;13(3):353–365.
51. Yen CF, Chou WJ, Liu TL, Yang P, Hu HF. The association of internet addiction symptoms with anxiety, depression and self-esteem among adolescents with attention-deficit/hyperactivity disorder. Compr Psychiatry. 2014;55(7):1601–1608. doi:10.1016/j.comppsych.2014.05.025
52. Caprara GV, Pastorelli C, Regalia C, Scabini E, Bandura A. Impact of adolescents’ filial self-efficacy on quality of family functioning and satisfaction. J Res Adolesc. 2005;15(1):1–97. doi:10.1111/j.1532-7795.2005.00087.x
53. Dou K, Nie Y, Wang Y, Liu Y, Li J. Adolescents’ regulatory emotional self-efficacy and subjective well-being: the mediating effect of regulatory emotional style. J Psychol Sci. 2013;36(1):139–144.
54. Beck AT. Depression: Clinical, Experimental, and Theoretical Aspects. New York, NY: Harper & Row; 1967.
55. Li H. A study on the association of adolescents’ coping styles with health hazard behaviors and physical and mental sub-health Master’s Thesis. Hefei: Hebei Normal University; 2017.
56. Luo FS, Shen D, Zhang SM, Wang X, Yuan H, Li Z. Mental health status of poverty students and its influencing factors. Chin J Clin Psychol. 2009;17(3):272–274.
57. Baloglu M, Kozan HIO, Kesici S. Gender differences in and the relationships between social anxiety and problematic internet use: canonical analysis. J Med Internet Res. 2018;20(1):1–9. doi:10.2196/jmir.8947
58. Wang YM, Wang YY. A survey of gender differences in Internet addiction among college students and their online purpose. J Heilongjiang College Edu. 2015;34(9):107–108.
59. Armiya’u AY, Yildirim M, Muhammad A, Tanhan A, Young JS. Mental health facilitators and barriers during covid-19 in Nigeria. J Asian Afr Stud. 2022;002190962211113. doi:10.1177/00219096221111354
60. Doyumğaç İ, Tanhan A, Kıymaz MS. Understanding the most important facilitators and barriers for online education during COVID-19 through online photovoice methodology. Int J High Educ. 2021;10(1):166–190. doi:10.5430/ijhe.v10n1p166
61. Tanhan A, Arslan G, Yavuz KF, et al. A constructive understanding of mental health facilitators and barriers through Online Photovoice (OPV) during COVID-19. ESAM Ekonomik ve Sosyal Arastirmalar Dergisi. 2021;2(2):214–249.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.