")
Back to Journals » International Journal of General Medicine » Volume 15
Change in Diagnosis of Benign Paroxysmal Positional Vertigo During COVID-19 Pandemic
Authors Lee DH, Shin JE, Jung T, Kim CH
Received 21 June 2022
Accepted for publication 31 August 2022
Published 5 September 2022 Volume 2022:15 Pages 7029—7037
DOI https://doi.org/10.2147/IJGM.S378822
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Dong-Han Lee, Jung Eun Shin, Taesik Jung, Chang-Hee Kim
Department of Otorhinolaryngology-Head and Neck Surgery, Konkuk University Medical Center, Research Institute of Medical Science, Konkuk University School of Medicine, Seoul, Republic of Korea
Correspondence: Chang-Hee Kim, Department of Otorhinolaryngology-Head and Neck Surgery, Konkuk University Medical Center, Konkuk University School of Medicine, 120-1 Neungdong-ro (Hwayang-dong), Gwangjin-gu, Seoul, 05030, Republic of Korea, Tel +82-2-2030-7666, Fax +82-2-2030-5299, Email [email protected]
Purpose: The present study investigated the impact of coronavirus disease 2019 (COVID-19) pandemic on benign paroxysmal positional vertigo (BPPV).
Patients and Methods: The medical records of BPPV patients who were evaluated in the outpatient department (OPD) and emergency room (ER) during (435 patients) and before (517 patients) the COVID-19 pandemic were retrospectively reviewed. Dix-Hallpike and supine head-roll tests were used to classify the subtype of BPPV as posterior semicircular canal (PSCC), geotropic lateral semicircular canal (geotropic LSCC), or apogeotropic lateral semicircular canal (apogeotropic LSCC) BPPV.
Results: More patients with PSCC BPPV were diagnosed at the OPD compared with those who were diagnosed at the ER both before and during the COVID-19 pandemic; however, more patients with LSCC BPPV were diagnosed at the ER compared with those who were diagnosed at the OPD during the same periods. The mean time interval between vertigo onset and initial evaluation was remarkably longer during the pandemic in patients with PSCC BPPV.
Conclusion: This study demonstrated that the incidences of BPPV subtypes according to hospital visit type were not significantly different before and during the COVID-19 pandemic. Because hospital visits were delayed in patients with PSCC BPPV during the COVID-19 pandemic, telemedicine or e-health could be suitable alternatives to face-to-face medical care for these patients.
Keywords: benign paroxysmal positional vertigo, COVID-19, emergency room, outpatient department, healthcare use behavior, hospital visit type
Introduction
Benign paroxysmal positional vertigo (BPPV) is characterized by sudden onset of vertigo elicited by change of head position. BPPV is the most common cause of vertigo, with an idiopathic etiology in the majority of cases. Idiopathic BPPV can be defined when the etiology of BPPV is unrecognizable, and common conditions, which can be associated with secondary BPPV, include head trauma, vestibular neuritis, Meniere’s disease, sudden sensorineural hearing loss and postsurgical. BPPV most commonly involves the posterior semicircular canal (PSCC), followed by the lateral semicircular canal (LSCC); however, several recent studies have shown that LSCC BPPV might be more common than reported previously.1–4 Because spontaneous remission often occurs in BPPV,5–7 the time interval from onset of vertigo to initial evaluation should be considered when estimating the true incidence of BPPV subtypes. Additionally, patient-perceived subjective vertigo may vary among individuals with BPPV, which can thus affect hospital use behavior. Furthermore, patient referral systems may keep patients with BPPV waiting pending the results of initial evaluations at the OPD clinics of tertiary hospitals. We have recently reported that the incidence of BPPV subtypes differs according to the type of hospital visit, ie, whether the patient is evaluated at the outpatient department (OPD) vs emergency room (ER).8
The coronavirus disease 2019 (COVID-19) pandemic has markedly impacted patient and provider lifestyles, including patterns of healthcare system use. During the severe crisis period, only emergency and oncology services were active in the tertiary referral medical center, as was the case in many other hospitals. Because dizzy patients may be concerned that hospitals are high-risk environments for COVID-19 infection, the pattern of hospital visit behavior in these patients may be different from that prior to the pandemic. We hypothesized that COVID-19 pandemic affected the medical healthcare use behavior in patients with BPPV, eliciting the change in the diagnosis of BPPV. This study aimed to investigate the impact of COVID-19 on the incidence of BPPV subtypes by hospital visit type (OPD vs ER) in a single tertiary university hospital. We also compared the duration between symptom onset and the initial professional evaluation in different subtypes of BPPV.
Patients and Methods
The medical records of patients who presented with BPPV to the hospital’s OPD and ER during and before the COVID-19 pandemic were retrospectively reviewed. A total of 517 patients diagnosed with idiopathic BPPV between March 2018 and December 2019 (before the COVID-19 pandemic) and a total of 435 patients diagnosed with idiopathic BPPV between March 2020 and December 2021 (during the COVID-19 pandemic) were included in this study. Neurological examinations were performed in each patient, and brain magnetic resonance imaging (MRI) was performed in patients with additional neurological abnormalities, and in those with severe imbalance, ataxia, and isolated vertigo with ocular movements suggesting central disorders such as gaze-evoked nystagmus, vertical or pure torsional spontaneous nystagmus, skew deviation or perverted head-shaking nystagmus. Nystagmus was examined using a video-oculography system in all BPPV patients at OPD and ER.
This study included only typical BPPV, including canalolithiasis-type PSCC BPPV, geotropic LSCC BPPV, and apogeotropic LSCC BPPV, and BPPV was diagnosed according to the clinical practice guidelines of the American Academy of Otorhinolaryngology-Head and Neck Surgery and Barany Society.9,10 PSCC BPPV was diagnosed when upbeat-torsional nystagmus was provoked by the Dix–Hallpike test. Geotropic LSCC BPPV was diagnosed when positional geotropic nystagmus lasting less than 1 min was induced by a head-roll test. Geotropic nystagmus was defined when the right-beating nystagmus was observed upon right head-rolling and the left-beating nystagmus was observed upon left head-rolling. Apogeotropic LSCC BPPV was diagnosed when positional apogeotropic nystagmus lasting longer than 1 min was provoked by the head-roll test. Apogeotropic nystagmus was defined when the left-beating nystagmus was observed upon right head-rolling and the right-beating nystagmus was observed upon left head-rolling.
Patients with superior semicircular canal (SSCC) BPPV, multicanal BPPV, recurrent BPPV, or central positional nystagmus were excluded from this study. To include cases of idiopathic BPPV, patients with suspected secondary BPPV, such as those with a current or recent history of inner ear disease, were excluded. Patients with post-traumatic BPPV or post-surgery conditions were excluded. Patients diagnosed with BPPV during severe medical illnesses, such as those undergoing chemotherapy or hemodialysis, were also excluded. Ninety-eight patients with apogeotropic LSCC BPPV underwent diffusion-weighted brain MRIs in the ER, all of which revealed no acute brain lesions. Routine contrast-enhanced brain MRIs, which were conducted on only two OPD patients with apogeotropic LSCC BPPV, demonstrated no abnormal findings.
SPSS version 24.0 (IBM SPSS, Armonk, NY, USA) was used for statistical analyses. The chi-square test or Fisher’s exact test was used for categorical variables, and Student’s t-test or Mann–Whitney U-test was used for continuous variables. We conducted Shapiro–Wilk test to examine if the samples are from a normally distributed population before performing Student’s t-test, and Mann–Whitney U-test was used in cases that the data tested are not assumed to be normally distributed. To assess the homogeneity of variances, Levene’s test of Equality of Variances was used in Student’s t-test. For categorical variables, Fisher’s exact test was used instead of chi-square test when more than 20% of cells have expected frequencies <5. A p value <0.05 was considered significant. This study was approved by the local institutional review board of Konkuk University Medical Center (No. 2022-04-042). Informed consents were exempted from all participants; this study is a retrospective study using only medical records. The study was conducted according to the guidelines of the Declaration of Helsinki for studies on human subjects.
Results
A total of 517 and 435 patients were diagnosed with idiopathic BPPV before (March 2018 and December 2019) and during (March 2020 and December 2021) the COVID-19 pandemic period, respectively. The patients’ mean age was 54.6 ± 12.9 years (range, 20–83 years) before the COVID-19 pandemic and 55.2 ± 17.2 years (range, 14–84 years) during the pandemic; however, these findings were not significantly different (p = 0.156, Student’s t-test). The male-to-female ratios were 141 (27%): 376 (73%) before the COVID-19 pandemic, and 129 (30%): 306 (70%) during the pandemic; these findings were also not significantly different (p = 0.417, chi-square test). The right-to-left ratio of the involved side was 253:264 before the COVID-19 pandemic and 216:219 during the pandemic, which was not significantly different (p = 0.825, chi-square test). Thirty-eight percent of BPPV patients (199/517) was diagnosed at the OPD before the COVID-19 pandemic, and 39.3% of BPPV patients (171/435) were diagnosed at the OPD during the pandemic; the proportion of patients with BPPV evaluated at the OPD was not significantly different between the two periods (p = 0.741, chi-square test).
Of the 517 BPPV patients before the COVID-19 pandemic, 198 (38%) were diagnosed with PSCC BPPV, 102 (20%) with geotropic LSCC BPPV, and 217 (42%) with apogeotropic LSCC BPPV (Table 1). Among the 198 patients with PSCC BPPV, more patients were diagnosed at the OPD (106/198 [54%]) than at the ER (92/198 [46%]) (Table 1). However, more patients were diagnosed at the ER than OPD in geotropic LSCC BPPV (76/102 [75%] at ER vs 26/102 [25%] at OPD) and apogeotropic LSCC BPPV (150/217 [69%] at ER vs 67/217 [31%] at OPD) (Table 1). Compared with PSCC BPPV, significantly higher proportions of patients were diagnosed at the ER in geotropic LSCC BPPV and apogeotropic LSCC BPPV (Figure 1). The mean time interval from vertigo onset to diagnosis was significantly longer in patients with PSCC BPPV (7.58 ± 16.13 days; range, 0–120 days) than in those with geotropic LSCC BPPV (2.05 ± 6.17 days; range, 0–52 days) or apogeotropic LSCC BPPV (3.32 ± 11.31 days; range, 0–120 days) (Table 1, Figure 2). Irrespective of BPPV subtype, the mean time interval between vertigo onset and diagnosis was remarkably longer in BPPV patients diagnosed at the OPD than those who were diagnosed at the ER (Table 1, Figure 3).
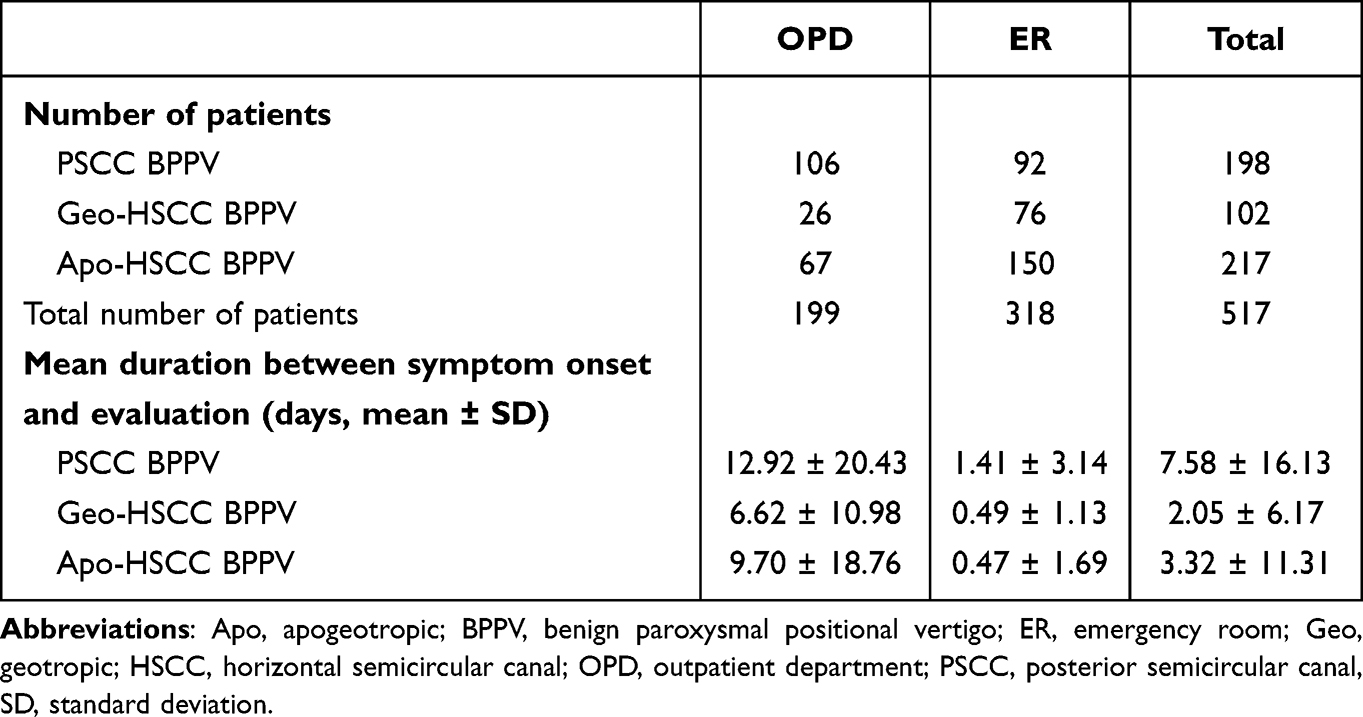 |
Table 1 Number of Patients and Mean Duration Between Symptom Onset and Evaluation According to BPPV Subtype During the Period Before COVID-19 Pandemic (Mar. 2018 ~ Dec. 2019) |
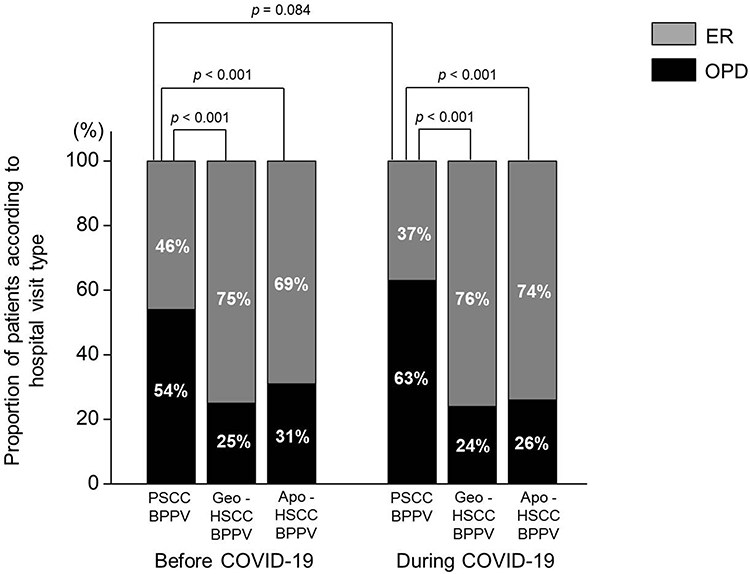 |
Figure 1 Proportion of patients (%) with PSCC BPPV, geotropic LSCC BPPV, and apogeotropic LSCC BPPV by hospital visit type before and during the COVID-19 pandemic. Significantly higher proportions of geotropic LSCC BPPV (p < 0.001, chi-square test) and ageotropic LSCC BPPV (p < 0.001, chi-square test) patients were diagnosed in the ER compared with those with PSCC BPPV in both before and during the COVID-19 pandemic. The proportion of patients who were diagnosed at the ER was not significantly different from those diagnosed at the OPD in PSCC BPPV (p = 0.084, chi-square test). Abbreviations: Apo, apogeotropic; BPPV, benign paroxysmal positional vertigo; COVID-19, coronavirus disease 2019; ER, emergency room; Geo, geotropic; LSCC, lateral semicircular canal; OPD, outpatient department; PSCC, posterior semicircular canal. |
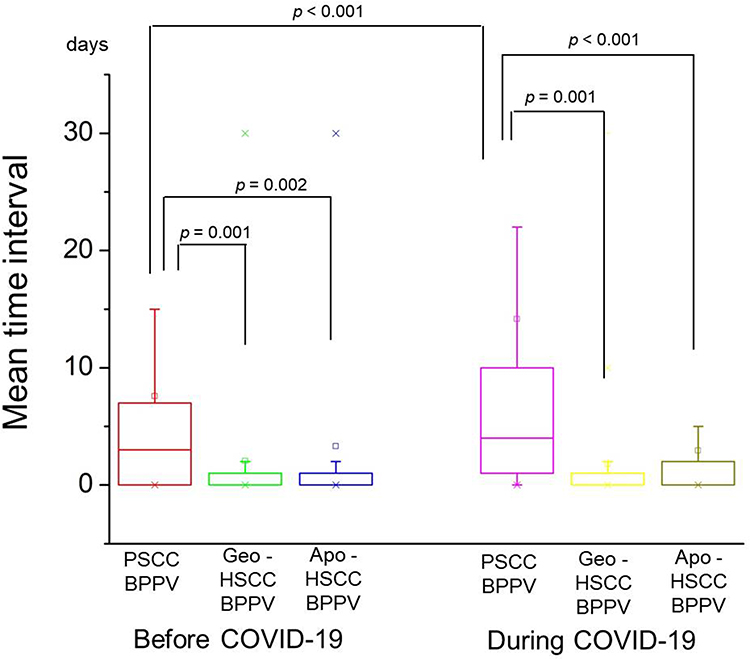 |
Figure 2 Mean time interval between symptom onset and clinical evaluation by BPPV subtype before and during the COVID-19 pandemic. Before COVID-19 pandemic, the mean time interval was significantly longer in patients with PSCC BPPV (7.58 ± 16.13 days) than in those with geotropic LSCC BPPV (2.05 ± 6.17 days, p = 0.001, Mann–Whitney U-test) or apogeotropic LSCC BPPV (3.32 ± 11.31 days, p = 0.002, Mann–Whitney U-test). During COVID-19 pandemic, the mean time interval was significantly longer in patients with PSCC BPPV (14.22 ± 39.00 days) than in those with geotropic LSCC BPPV (1.48 ± 2.33 days, p = 0.001, Mann–Whitney U-test) or apogeotropic LSCC BPPV (2.94 ± 8.05 days, p < 0.001, Mann–Whitney U-test). The mean time interval was remarkably longer during the COVID-19 pandemic than before the COVID-19 pandemic in PSCC BPPV (p < 0.001, Mann–Whitney U-test). Abbreviations: Apo, apogeotropic; BPPV, benign paroxysmal positional vertigo; COVID-19, coronavirus disease 2019; Geo, geotropic; LSCC, lateral semicircular canal; PSCC, posterior semicircular canal. |
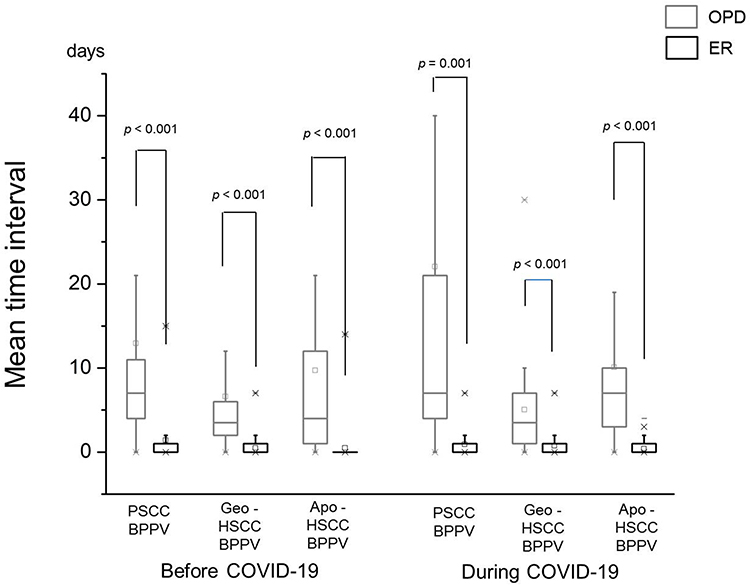 |
Figure 3 Differences in mean time intervals between symptom onset and clinical evaluation according to BPPV subtype by hospital visit type before and during the COVID-19 pandemic. Before the COVID-19 pandemic, the mean time interval for patients who were assessed at the OPD vs the ER was 12.92 ± 20.43 days vs 1.41 ± 3.14 days for PSCC BPPV (p < 0.001, Mann–Whitney U-test), 6.62 ± 10.98 days vs 0.49 ± 1.13 days for geotropic-LSCC BPPV (p < 0.001, Mann–Whitney U-test), and 9.70 ± 18.76 days vs 0.47 ± 1.69 days for apogeotropic-LSCC BPPV (p < 0.001, Mann–Whitney U-test), respectively. During the COVID-19 pandemic, the mean time interval for the patients who were diagnosed at the OPD vs ER was 22.26 ± 47.68 days vs 0.90 ± 1.46 days for PSCC BPPV (p = 0.001, Mann–Whitney U-test), 4.10 ± 2.98 days vs 0.70 ± 1.37 days for geotropic LSCC BPPV (p < 0.001, Mann–Whitney U-test), and 10.07 ± 13.39 days vs 0.39 ± 0.66 days for apogeotropic LSCC BPPV (p < 0.001, Mann–Whitney U-test), respectively. Abbreviations: Apo, apogeotropic; BPPV, benign paroxysmal positional vertigo; COVID-19, coronavirus disease 2019; ER, emergency room; Geo, geotropic; LSCC, lateral semicircular canal; OPD, outpatient department; PSCC, posterior semicircular canal. |
Of the 435 BPPV patients during the COVID-19 pandemic, 163 (37%) were diagnosed with PSCC BPPV, 116 (27%) with geotropic LSCC BPPV, and 156 (36%) with apogeotropic LSCC BPPV (Table 2). The BPPV subtype distribution according to hospital visit type was similar before and during the COVID-19 pandemic. Among the 163 patients with PSCC BPPV, more patients were diagnosed at the OPD (102/163 [63%]) than at the ER (61/163 [37%]) (Table 2). However, more patients were diagnosed at the ER than at the OPD in geotropic LSCC BPPV (88/116 [76%] vs 28/116 [24%]) and apogeotropic LSCC BPPV (115/156 [74%] vs 41/156 [26%]) (Table 2). Significantly higher proportions of patients were diagnosed at the ER in geotropic LSCC BPPV and apogeotropic LSCC BPPV compared with PSCC BPPV (Figure 1). The mean time interval was significantly longer for PSCC BPPV (14.22 ± 39.00 days; range, 0–365 days) than for geotropic LSCC BPPV (1.48 ± 2.33 days; range, 0–30 days) or apogeotropic LSCC BPPV (2.94 ± 8.05 days; range, 0–60 days) (Table 2, Figure 2). Irrespective of BPPV subtype, the mean time interval was significantly longer in patients diagnosed at the OPD than the ER (Table 2, Figure 3).
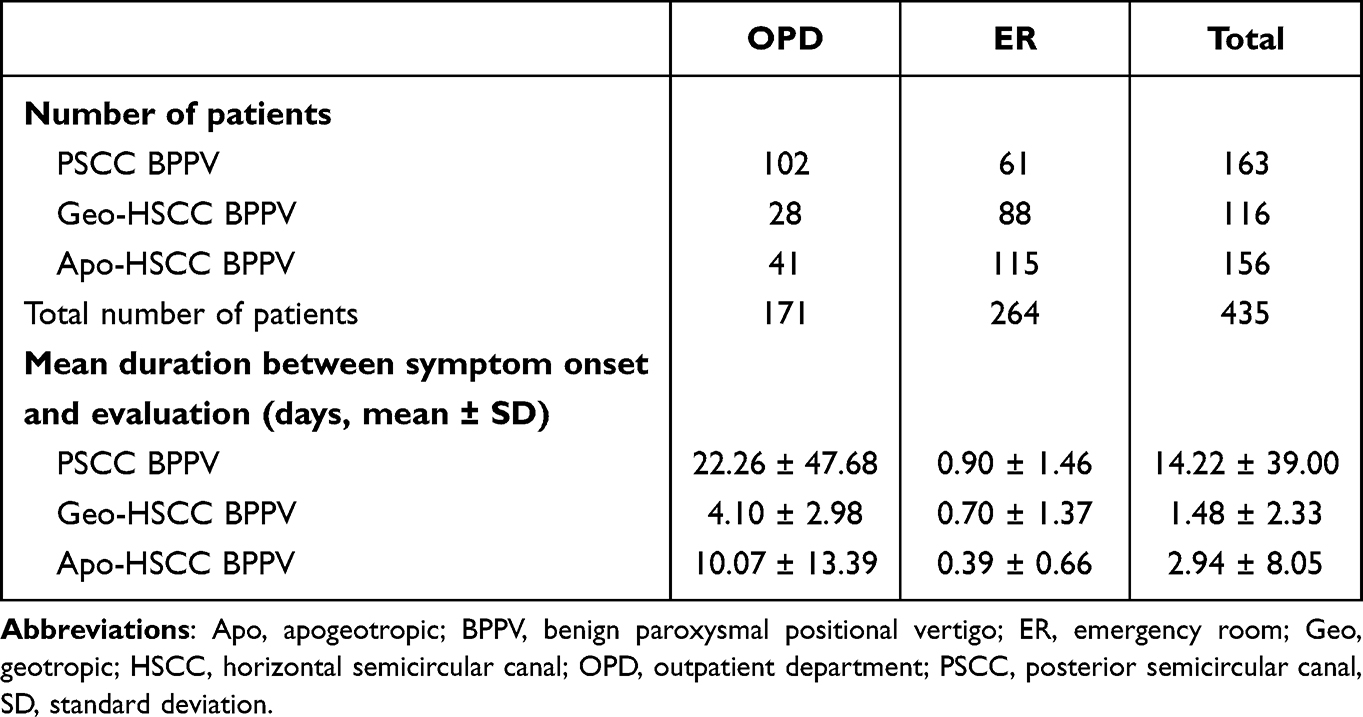 |
Table 2 Number of Patients and Mean Duration Between Symptom Onset and Evaluation According to BPPV Subtype During the Period of COVID-19 Pandemic (Mar. 2020 ~ Dec. 2021) |
We then compared the incidence of BPPV subtypes and symptom duration prior to hospital visits between the periods before and during the COVID-19 pandemic. Irrespective of BPPV subtype, the proportion of patients who were evaluated at the ER was not significantly different from those evaluated at the OPD in geotropic LSCC BPPV (p = 0.370, chi-square test), apogeotropic LSCC BPPV (p = 0.335, chi-square test), and PSCC BPPV (p = 0.084, chi-square test, Figure 1). However, while the mean time interval from vertigo onset to diagnosis was also not significantly different before and during the COVID-19 pandemic in geotropic LSCC BPPV (p = 0.309, Mann–Whitney U-test) and apogeotropic LSCC BPPV (p = 0.367, Mann–Whitney U-test), in the case of PSCC BPPV, the mean time interval was remarkably longer during the COVID-19 pandemic than before the COVID-19 pandemic (p < 0.001, Mann–Whitney U-test, Figure 2). We then investigated the actual change in the proportion of BPPV patients during the COVID-19 pandemic. The numbers of patients who visited our ENT OPD or those who were evaluated by ENT specialists at the ER during COVID-19 pandemic (16,835 OPD patients, 1980 ER patients) and before the pandemic (22,149 OPD patients, 3059 ER patients) was calculated. The proportion of BPPV patients at the OPD was 0.90% (199 of 22,149) before the COVID-19 pandemic and 1.02% (171/16,835), which was not significantly different (p = 0.237, chi-square test). However, the proportion of BPPV patients at the ER was 10.40% (318 of 3059) before the COVID-19 pandemic and 13.3% (264/1980), which show significant difference (p < 0.001, chi-square test) (Table 3).
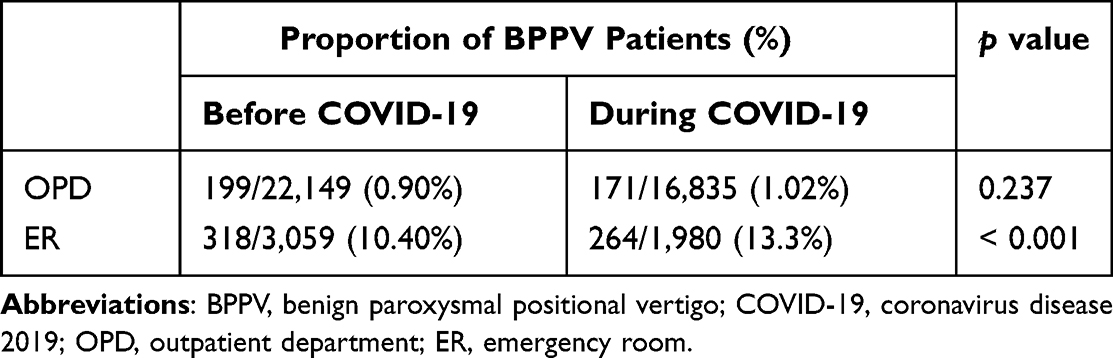 |
Table 3 Change in the Proportion of BPPV Patients Before and During COVID-19 Pandemic |
Discussion
In the present study, we compared the incidence of BPPV subtypes and the mean time interval from vertigo onset to initial evaluation in patients with BPPV before and during the COVID-19 pandemic. The results demonstrated that although the incidence of BPPV subtypes according to hospital visit type was not significantly different before and during the COVID-19 pandemic, the mean time interval between vertigo onset and initial evaluation in patients with PSCC BPPV became significantly longer during the COVID-19 pandemic.
Several previous studies have investigated the impact of the COVID-19 pandemic on the hospital visit behavior of patients with dizziness, with controversial results. Ueda et al investigated the impact of the COVID-19 pandemic on OPD follow-up cancellations by dizziness/vertigo patients in a university hospital and found that while most of the patients who cancelled during the COVID-19 pandemic had BPPV, patients with Meniere’s disease had the least number of cancellations during the COVID-19 pandemic.11 Li et al compared the demographic characteristics and etiological distribution of dizziness/vertigo patients in the OPD during and before the COVID-19 pandemic and demonstrated that although the absolute number of dizziness/vertigo patients decreased 40.4% during the COVID-19 pandemic, the proportion of BPPV diagnoses in dizziness/vertigo patients increased from 30.7% to 35%.12 Waissbluth et al reported that a high proportion of consultations for vertigo were observed, although overall number of medical consultations dropped significantly due to preventive lockdown during COVID-19 pandemic; furthermore, the number of consultations for BPPV increased 183% during COVID-19 pandemic compared with pre-pandemic levels.13 Parrino et al reported that there were no differences in the absolute number of acute audio-vestibular disorders during the COVID-19 pandemic compared with previous periods, and sudden hearing loss during the pandemic seemed worse in terms of hearing threshold, and with a higher incidence of associated vestibular involvement.14 Di Mauro et al evaluated 33 patients with acute vertigo after COVID-19 vaccination, and BPPV was diagnosed in 9 (27%) of 33 patients.15 Other studies have suggested the COVID-19 infection as a cause of BPPV.16,17 Due to the limited access to medical care provider during the COVID-19 pandemic, telemedicine for diagnosis and treatment of BPPV was proposed as a good alternative.18–20
To our knowledge, this study is the first to examine the impact of COVID-19 on the incidence of BPPV subtypes by hospital visit (OPD vs ER), and the mean time interval between vertigo onset and primary evaluation. Our data demonstrated that the total number of BPPV patients who were diagnosed in the ER and OPD decreased by 15.9% (517 to 435) during the COVID-19 pandemic compared with pre-pandemic levels. Age and sex distributions were not significantly different between the two time periods. Remarkably, the proportion of BPPV patients diagnosed at the OPD was significantly higher for PSCC BPPV than for LSCC BPPV during both periods (Figure 1). So why are patients with LSCC BPPV being diagnosed more commonly in the ER than in the PSCC BPPV? It has been reported that patient-perceived severity of vertigo is more intense with LSCC BPPV than with PSCC BPPV, leading to increased treatment urgency among patients with LSCC BPPV.21,22 In addition, spontaneous resolution of LSCC BPPV occurs more quickly and easily in than with PSCC BPPV;5–7 as a result, PSCC BPPV patients with longer symptom durations may be more likely to seek treatment at the OPD. Finally, under Korea’s healthcare delivery system, before being evaluated at the OPD of a tertiary referral center, patients with BPPV must usually wait for several days after undergoing an initial evaluation by a primary care physician.
Another interesting finding of our research was that LSCC BPPV was a more common subtype than PSCC BPPV prior to and during the pandemic (Tables 1 and 2), which was inconsistent with most previous studies that reported a higher incidence of PSCC BPPV.9,10,23 However, if we estimate the incidence of BPPV subtypes in patients who were diagnosed at the OPD, PSCC BPPV was the most common subtype, which is consistent with previous study findings. Furthermore, considering that many patients with PSCC BPPV might have been diagnosed at a primary health care clinic without being referred to a tertiary referral center, the actual incidence of PSCC BPPV is probably higher than that estimated in the present study. On the other hand, we suspect that the incidence of LSCC BPPV might also have been underestimated because spontaneous remission of this subtype is more likely, and, consequently, the natural course of LSCC BPPV is shorter.5–7 In the present study, we demonstrated that PSCC BPPV is more commonly diagnosed in the OPD setting than LSCC BPPV, and that LSCC BPPV is more common than PSCC BPPV in the ER setting. Indeed, although it is known that PSCC is the most common subtype of BPPV,9,24 the diagnosis appeared to have been made at the OPD in most studies that reported higher incidences of PSCC BPPV.25–29 Further studies are needed to clarify the true incidence of BPPV subtypes.
It is noteworthy that the mean time interval from onset of PSCC BPPV symptoms to hospital evaluation was significantly longer during the COVID-19 pandemic than it was before the pandemic, whereas the interval was not significantly in cases of geotropic and apogeotropic LSCC BPPV. This finding may be explained by the fact that LSCC BPPV patients had more severe symptoms and thus visited the hospital earlier despite treatment limitations during the COVID-19 pandemic, whereas the pandemic delayed hospital visits for patients with PSCC BPPV whose symptoms were less severe and more tolerable. Another interesting finding was that although the proportion of BPPV patients was not changed significantly between during and before the COVID-19 at the OPD, the proportion of BPPV patients significantly increased during COVID-19 pandemic at the ER.
This study has two primary limitations intrinsic to an incidence study. First, because this study was conducted at a single tertiary referral center, it is difficult to generalize our results to other facilities and populations. Second, because patients with atypical BPPV including SSCC BPPV, posttraumatic BPPV, multiple canal BPPV, and secondary BPPV were excluded from the study, the incidence in the present study may not represent all BPPV populations.
Conclusions
The present study demonstrated that no differences were observed in the incidence of BPPV subtypes by hospital visit type (OPD vs ER) during the COVID-19 pandemic when compared with pre-pandemic levels. In patients with PSCC BPPV, the mean interval between vertigo onset and the first evaluation was remarkably longer during the pandemic period. Telemedicine or e-medicine may be considered to improve hospital accessibility in similar circumstances, in order to minimize delays in clinical evaluation and treatment.
Abbreviations
COVID-19, coronavirus disease 2019; ER, Emergency room; OPD, outpatient department; BPPV, benign paroxysmal positional vertigo; PSCC, posterior semicircular canal; LSCC, lateral semicircular canal; SSCC, superior semicircular canal.
Funding
This paper was supported by Konkuk University in 2022.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Kong TH, Song MH, Shim DB. Recurrence rate and risk factors of recurrence in benign paroxysmal positional vertigo: a single-center long-term prospective study with a large cohort. Ear Hear. 2021;43(1):234–241.
2. Nahm H, Han K, Shin JE, Kim CH. Benign paroxysmal positional vertigo in the elderly: a single-center experience. Otol Neurotol. 2019;40:1359–1362. doi:10.1097/MAO.0000000000002385
3. Chung KW, Park KN, Ko MH, et al. Incidence of horizontal canal benign paroxysmal positional vertigo as a function of the duration of symptoms. Otol Neurotol. 2009;30:202–205. doi:10.1097/MAO.0b013e31818f57da
4. Choi S, Choi HR, Nahm H, Han K, Shin JE, Kim CH. Utility of the bow and lean test in predicting subtype of benign paroxysmal positional vertigo. Laryngoscope. 2018;128:2600–2604. doi:10.1002/lary.27142
5. Shim DB, Ko KM, Lee JH, Park HJ, Song MH. Natural history of horizontal canal benign paroxysmal positional vertigo is truly short. J Neurol. 2015;262:74–80. doi:10.1007/s00415-014-7519-0
6. Imai T, Ito M, Takeda N, et al. Natural course of the remission of vertigo in patients with benign paroxysmal positional vertigo. Neurology. 2005;64:920–921. doi:10.1212/01.WNL.0000152890.00170.DA
7. Imai T, Takeda N, Ito M, Inohara H. Natural course of positional vertigo in patients with apogeotropic variant of horizontal canal benign paroxysmal positional vertigo. Auris Nasus Larynx. 2011;38:2–5. doi:10.1016/j.anl.2010.05.011
8. Kim CH, Jeong H, Shin J, Locke R, Kontorinis G. Incidence of idiopathic benign paroxysmal positional vertigo subtype by hospital visit type: experience of a single tertiary referral center. J Laryngol Otol. 2022;1–4. doi:10.1017/S0022215122000299
9. Bhattacharyya N, Gubbels SP, Schwartz SR, et al. Clinical practice guideline: benign paroxysmal positional vertigo (update). Otolaryngol Head Neck Surg. 2017;156:S1–s47. doi:10.1177/0194599816689667
10. von Brevern M, Bertholon P, Brandt T, et al. Benign paroxysmal positional vertigo: diagnostic criteria. J Vestib Res. 2015;25:105–117. doi:10.3233/VES-150553
11. Ueda K, Ota I, Yamanaka T, Kitahara T. The impact of the COVID-19 pandemic on follow-ups for vertigo/dizziness outpatients. Ear Nose Throat J. 2021;100:163s–168s. doi:10.1177/0145561320980186
12. Li C, Guo D, Ma X, Liu S, Liu M, Zhou L. The impact of coronavirus disease 2019 epidemic on dizziness/vertigo outpatients in a neurological clinic in China. Front Neurol. 2021;12:663173. doi:10.3389/fneur.2021.663173
13. Waissbluth S, García-Huidobro F, Araya-Céspedes M. The impact of COVID-19 preventive lockdowns on the prevalence of benign paroxysmal positional vertigo. Medwave. 2021;21:e8174. doi:10.5867/medwave.2021.03.8174
14. Parrino D, Frosolini A, Toninato D, Matarazzo A, Marioni G, de Filippis C. Sudden hearing loss and vestibular disorders during and before COVID-19 pandemic: an audiology tertiary referral centre experience. Am J Otolaryngol. 2022;43:103241. doi:10.1016/j.amjoto.2021.103241
15. Di Mauro P, La Mantia I, Cocuzza S, et al. Acute vertigo after COVID-19 vaccination: case series and literature review. Front Med. 2021;8:790931. doi:10.3389/fmed.2021.790931
16. Maslovara S, Košec A, Yaman H. Post-COVID-19 benign paroxysmal positional vertigo. Case Rep Med. 2021;2021:9967555. doi:10.1155/2021/9967555
17. Picciotti PM, Passali GC, Sergi B, De Corso E. Benign paroxysmal positional vertigo (BPPV) in COVID-19. Audiol Res. 2021;11:418–422. doi:10.3390/audiolres11030039
18. Bashir K, Yousuf A, Rauf L, Dewji M, Elmoheen A. Curing Benign Paroxysmal Positional Vertigo (BPPV) through telehealth: a case series. Cureus. 2021;13:e16363. doi:10.7759/cureus.16363
19. Harrell RG, Schubert MC, Oxborough S, Whitney SL. Vestibular rehabilitation telehealth during the SAEA-CoV-2 (COVID-19) pandemic. Front Neurol. 2021;12:781482. doi:10.3389/fneur.2021.781482
20. Barreto RG, Yacovino DA, Teixeira LJ, Freitas MM. Teleconsultation and teletreatment protocol to diagnose and manage patients with Benign Paroxysmal Positional Vertigo (BPPV) during the COVID-19 pandemic. Int Archiv Otorhinolaryngol. 2021;25:e141–e149. doi:10.1055/s-0040-1722252
21. Martens C, Goplen FK, Aasen T, Nordfalk KF, Nordahl SHG. Dizziness handicap and clinical characteristics of posterior and lateral canal BPPV. Eur Arch Otorhinolaryngol. 2019;276:2181–2189. doi:10.1007/s00405-019-05459-9
22. Kim MJ, Kim KS, Joo YH, Park SY, Han GC. The dizziness handicap inventory and its relationship with vestibular diseases. J Int Adv Otol. 2012;8:69–77.
23. Cakir BO, Ercan I, Cakir ZA, Civelek S, Sayin I, Turgut S. What is the true incidence of horizontal semicircular canal benign paroxysmal positional vertigo? Otolaryngol Head Neck Surg. 2006;134:451–454. doi:10.1016/j.otohns.2005.07.045
24. Parnes LS, Agrawal SK, Atlas J. Diagnosis and management of benign paroxysmal positional vertigo (BPPV). Cmaj. 2003;169:681–693.
25. Marciano E, Marcelli V. Postural restrictions in labyrintholithiasis. Eur Arch Otorhinolaryngol. 2002;259:262–265. doi:10.1007/s00405-001-0445-7
26. Wolf JS, Boyev KP, Manokey BJ, Mattox DE. Success of the modified Epley maneuver in treating benign paroxysmal positional vertigo. Laryngoscope. 1999;109:900–903. doi:10.1097/00005537-199906000-00011
27. Katsarkas A. Benign paroxysmal positional vertigo (BPPV): idiopathic versus post-traumatic. Acta Otolaryngol. 1999;119:745–749. doi:10.1080/00016489950180360
28. Korres S, Balatsouras DG, Kaberos A, Economou C, Kandiloros D, Ferekidis E. Occurrence of semicircular canal involvement in benign paroxysmal positional vertigo. Otol Neurotol. 2002;23:926–932. doi:10.1097/00129492-200211000-00019
29. Honrubia V, Baloh RW, Harris MR, Jacobson KM. Paroxysmal positional vertigo syndrome. Am J Otol. 1999;20:465–470.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.