")
Back to Journals » International Journal of Women's Health » Volume 14
Challenges of Perinatal Depression Care in Mexico City Health Centers
Authors Navarrete L , Lara MA, Berenzon S, Mora-Rios J
Received 19 July 2022
Accepted for publication 5 October 2022
Published 6 December 2022 Volume 2022:14 Pages 1667—1679
DOI https://doi.org/10.2147/IJWH.S381196
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Laura Navarrete,1,2 Ma Asunción Lara,1 Shoshana Berenzon,1 Jazmin Mora-Rios1
1Directorate of Epidemiological and Psychosocial Research, National Institute of Psychiatry “Ramón de la Fuente Muñiz”, Mexico City, Mexico; 2Doctorate Program in Medical, Odontology and Health Sciences of the National Autonomous, University of Mexico, Mexico City, Mexico
Correspondence: Ma Asunción Lara, Tel +52 55 4160 5170, Fax +52 55 5513 3446, Email [email protected]
Background: Perinatal depression is a common mental disorder regarded as a severe public health problem. Studies have shown that incorporating mental health care into primary health services that provide pregnancy care makes it easier for women to seek help for depressive symptoms. In this context, the following question is of interest: How prepared are primary health services in Mexico City that provide pregnancy and postpartum care to treat perinatal depression? This article seeks to explore the perceptions and knowledge of perinatal depression in health professionals and analyze the barriers to its care at primary care centers in Mexico City.
Methods: An exploratory study with a qualitative approach was conducted. Doctors, nurses, social workers who provide maternal and childcare, mental health personnel, and the directors of four centers were interviewed. Interviews were audio-recorded and transcribed for thematic analysis.
Results: Most primary care personnel are unaware of the Official Standard that recommends providing maternal mental health care during the perinatal period. There is no initiative for its incorporation into routine care. A significant barrier to its implementation is health professionals’ biased, stereotyped perception of perinatal depression, motherhood, and the role of women. Other barriers include the workload of health professionals, the division of care between professionals, and the lack of communication between the latter. Women with psychological symptoms are not referred to mental health staff in a timely manner. Social workers are in closer contact with women and are more willing to address their emotional distress.
Conclusion: Maternal mental health care, contingent on pregnancy, childbirth, and puerperium care at primary care centers is currently not possible due to the lack of knowledge, barriers, and directors’ dependence on hospital management decisions.
Keywords: maternal mental health, perinatal depression, primary health care
Introduction
Perinatal depression (PD), defined as depression that occurs during pregnancy and up to twelve months after childbirth,1 is a common mental disorder regarded as a serious public health problem worldwide. Prevalence during pregnancy is estimated at between 9.2% and 19.2%2 and between 9.5% and 19.7% during the postpartum period.2,3
Untreated PD has a significant impact, not only on the mother, but also on the baby and family. Depression during pregnancy (DDP) is associated with risky behaviors on the part of the mother, such as failure to seek timely prenatal care, alcohol and drug use, and nutritional deficiency, which, in turn, are associated with a higher risk of having a preterm childbirth, a baby with low birthweight, and postpartum depression (PPD).4
For its part, PPD makes the parenting process difficult, which affects the health of the infant, who is more likely to present problems such as diarrhea, fever, and overall distress, as well as difficulty establishing sleep patterns and harm to their motor, cognitive, language and social development.5 The impact of PPD is also reflected in the physical health of the mother, who experiences greater physical discomfort, difficulty establishing breastfeeding and the need to seek medical care more frequently. PPD is often accompanied by anxious symptoms and longer depressive episodes; having the feeling of experiencing more stressful situations, having little social support and unsatisfactory relationships.6 Women with pregnancy or PPD often feel irritable and overwhelmed by the demands of motherhood, which makes close contact with the baby difficult, affecting the development of adequate mother-child attachment.6 The evidence shows a greater presence of insecure, disorganized attachment in the children of depressed mothers.7
There is evidence of a higher prevalence of PD in low- and middle-income countries,2 in which the most vulnerable members of the population, who have less educational attainment and are unpartnered and unemployed, are the most severely affected.8 In Mexico, data from Mexico City show that between 4.3% and 30.7% of pregnant women experience depression in pregnancy (The Structured Clinical Interview, SCID),9,10 while between 5.8% and 24.1% suffer PPD.9,11
The evidence points to the importance of treating PD in a timely manner and preventing its emergence as far as possible.12 In recent decades, studies have shown that incorporating mental health care into primary health services that provide pregnancy care makes it easier for women to seek help for depressive symptoms.12 As a result, countries such as England and Australia have incorporated the detection of mental health problems into prenatal and postpartum care in primary care during prenatal check-ups and in childcare during the first year of life.13,14 These actions have made it possible to promote the initial contact between first cases and mental health services, improve case detection and refer severe cases.
In Mexico, perinatal mental health has been neglected. In one `, the official standard for the care of women during pregnancy, childbirth, and the puerperium15 recommends “identifying data on depression or any other disorder related to mental health during pregnancy, childbirth and puerperium”, without providing any further details. The same year this standard was published, the Ministry of Health expanded its clinical practice guidelines for addressing various health problems to include a clinical guide for the prevention, diagnosis, and management of prenatal depression, which was revised in 2021.16 It has been observed that this standard is not applied in clinical practice since it fails to specify the mechanisms for its implementation or provide health services with the specialized mental health personnel required. At the same time, the fact that perinatal mental health is not considered a priority health problem in Mexico also contributes to the fact that this standard is not seen as relevant.17,18
In this context, the following question is of interest: How prepared are primary health services that provide pregnancy and postpartum care to treat PD? It is also necessary to ask how willing health personnel are to make the changes they would have to effect in their day-to-day activities if they were obliged to perform new tasks.19 Accordingly, the objectives of this study were a) To explore the opinions and beliefs about PD of health care personnel at primary health care centers in Mexico City, b) To identify the actions currently taken when a mental health problem is detected; and c) To analyze the barriers to managing these problems and the actions that could be undertaken to implement strategies for the timely detection and prevention of postpartum depression. The results of this study could be relevant for the implementation of programs and interventions to address mental health in perinatal clinical practice since their successful adoption requires considering the context, physical space, environment, and opinion of the professionals responsible for executing them.20
Materials and Methods
An exploratory study with a qualitative approach was designed to determine the opinions and perceptions of a group of health professionals. This design was used to record the stories and meanings respondents have about PD and the strategies for caring for women who suffer from it. One of the central ideas of the qualitative approach is that the world of everyday life is shared and constructed through the subjectivities of individuals (intersubjective).21
Setting
The study was conducted at four health centers we call A, B, C and D, which belong to the Mexico City government and provide care for people who do not have social security. These centers were chosen since they offer psychological or psychiatric care, in addition to family medicine offices, which made it possible to explore the role they play in maternal mental health care.
Health centers “A” and “B” serve mainly low-income patients, whereas health centers “C” and “D” serve those from various areas and socioeconomic levels.
Subjects
Twenty health professionals (including four doctors, four nurses and four social workers), who had been assigned to a maternal and childcare activity during that period, were interviewed. Three psychologists and a psychiatrist were also interviewed, together with the directors of each health center. Participants included six men (two directors, two doctors, a psychologist, and a psychiatrist) and fourteen women (two directors, two doctors, four nurses, four social workers and two psychologists). The age range was 31 to 63 years, the majority lived with their partners and eight had completed graduate studies (four directors, a nurse, a social worker, a psychologist, and a psychiatrist) (Table 1).
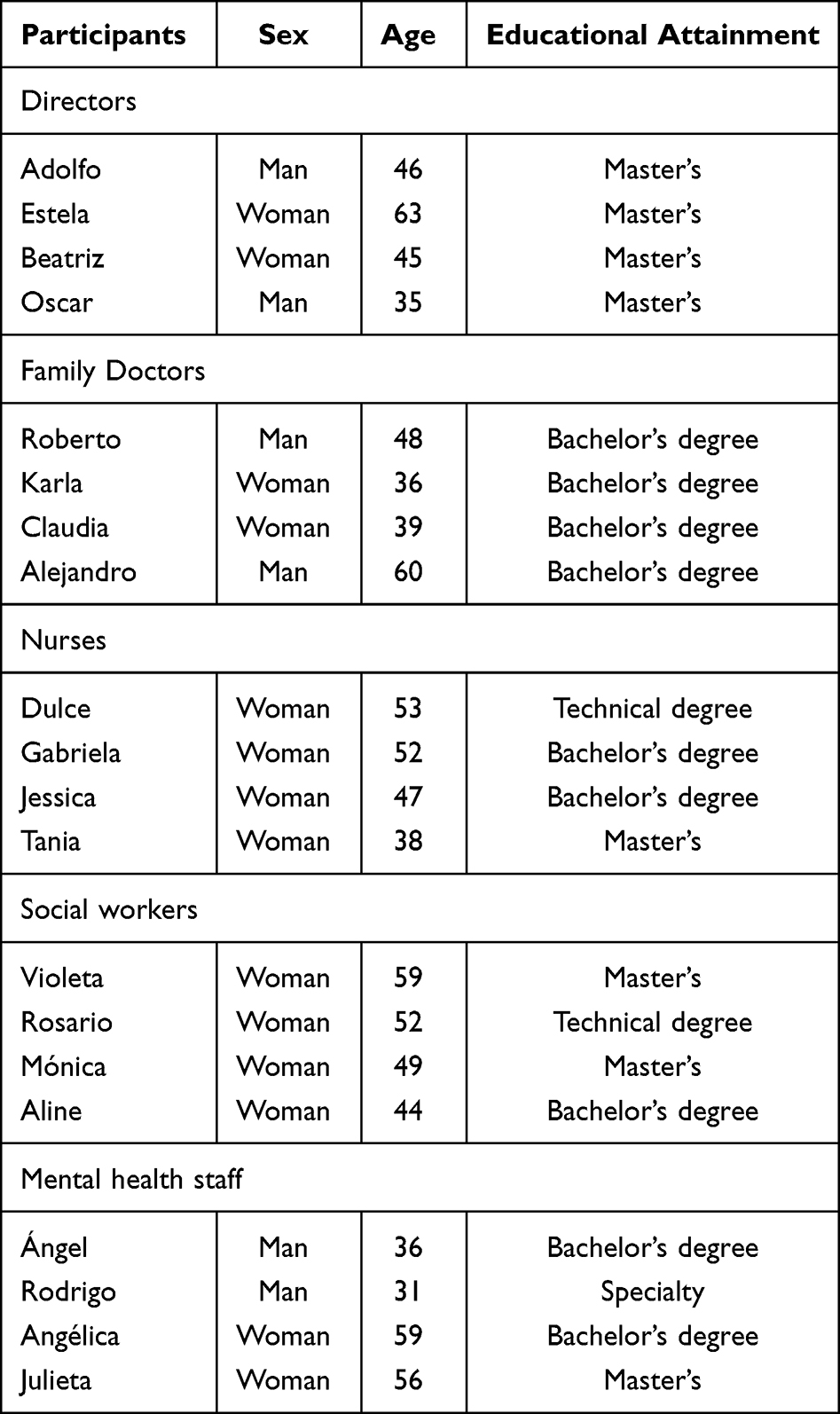 |
Table 1 Sociodemographic Characteristics |
Data Collection and Procedure
Fieldwork was undertaken from September 2018 to February 2019. Contact with the health centers selected was made with the support of the Mexico City Ministry of Health authorities. The directors of each center and the staff involved in antenatal care were invited to participate in the study. Semi-structured interviews were conducted with those who agreed to participate (Semi-structured interviews have greater flexibility than structured interviews because they begin with planned questions, which can be adjusted to the subjects. One of their advantages is that they can be adapted to subjects and are designed to encourage respondents to clarify terms, identify ambiguities and reduce needless formalities22).
An interview guide based on a literature review with key issues was used to explore 1) knowledge of PD, 2) type/level of participation in prenatal care and 3) perinatal mental health in primary care and program implementation. Subjects were asked open questions such as “Tell me what a normal day of activities at this health center is like;” Have you heard about postpartum depression? What do you understand by postpartum depression?” and “In your view, what would improve the detection of PD?”
A pilot study of the interview with nursing staff in each health center was conducted.
Interviews were conducted in subjects’ work areas, at a time of their choosing, to maximize privacy and prevent interruptions. All interviews were conducted by the first author of the article, who had had previous training in qualitative methods. Interviews lasted an average of forty-five minutes, were completed in a single session and audio-recorded for their subsequent transcription.
Data Analysis
The thematic analysis method was used.23 Interview transcripts were checked to ensure their quality. After a detailed reading of the interviews, analysis codes and categories were developed, which made it possible to extract smaller discursive units that could be more easily compared. Analysis categories were identified based on the objectives proposed in the interview guide and each of them was defined by establishing a consensus among the research team to facilitate coding. A deductive or theoretical thematic analysis was performed. The two researchers familiarized themselves with the information, created the initial codes, and searched for the themes (Laura Navarrete (LN) obtained a master’s degree in public mental health, while Valeria Zempoalteca (VZ) obtained a master’s degree in psychology. Both have knowledge and experience in conducting qualitative analysis.). They subsequently reviewed the topics, definitions, and denominations of topics based on consensus and drafted a report. The categories for the purposes of this study were: 1) knowledge of postpartum depression, 2) detection and treatment, c) barriers and necessary conditions for the implementation of actions for the detection and prevention of PD. MAXQDA 2020 software24 was used to organize the analysis categories.
Ethical Considerations
This project was approved by the Research Ethics Committee of the Ramón de la Fuente Muñíz National Institute of Psychiatry (CEI/C/036/2018). Each participant was asked for their consent for the interview, as well as the audio recording. All participants provided written informed consent prior to enrollment in the study. The testimonials of the participants are presented with pseudonyms to guarantee confidentiality. As a way of giving back to the participants, information related to mental health was offered to those interested in these issues.
Results
The main findings yielded by the thematic analysis are described below.
Knowledge of Perinatal Depression
Regarding knowledge of the “Guide to Perinatal Depression Care in Primary and Secondary Health Care”16 only five of the twenty participants had heard of this, and none of them had examined it in detail. The rest of the professionals “were unaware of its existence” and thought that “these guidelines should be disseminated, since the information does not always reach this level” in other words, primary health care.
Participants found it difficult to define postpartum depression, and instead gave the reasons why they thought women had postpartum depression. It is important to note that the definitions and risk factors always centered on PPD and did not mention DDP at any time (Table 2).
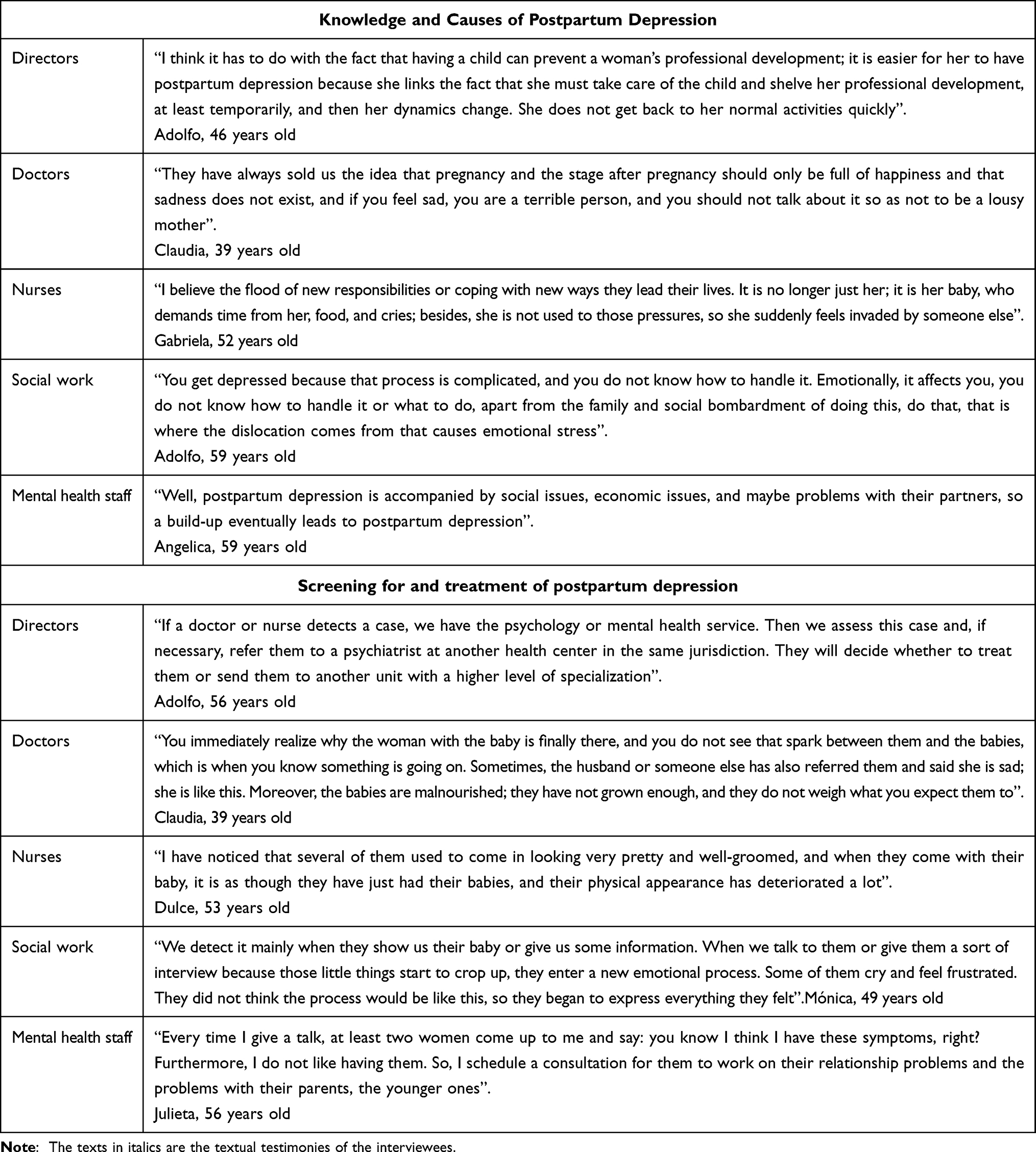 |
Table 2 Fragments of Interviews on Knowledge and Causes of Postpartum Depression and Screening for and Treatment of Postpartum Depression |
Most participants cited hormonal changes as the main cause of postpartum depression. For example, doctors referred to it using phrases such as “hormonal imbalance.” Nurses thought it was related to the “emotional lability of patients because hormones drop” while social workers considered PPD to be a feeling of sadness caused by “the decrease in hormones, due to childbirth.” Only the psychiatrist and the psychologists defined PPD as a particular type of depression that should be distinguished from postpartum sadness, since the latter has a hormonal origin, whereas PPD is multifactorial.
For all the health and mental health personnel and managers, PD is also the result of various psychosocial factors, such as being unemployed, the lack of social support networks, economic problems, experiencing violence and the number of children.
It should be noted that certain sex differences were observed among the group of physicians. Male doctors pointed out that since women are not merely caregivers in the family, this makes it easier for them to want to do other things and to see pregnancy and childbirth as something that prevents them from doing so. Conversely, for female doctors, the cultural conception of motherhood—which assumes that women should be happy merely because they are mothers—prevents them from talking about their negative emotions during this period and isolates them, causing them emotional distress. This opinion was shared by social workers, who pointed out that depression arises from the fear of “being unable to meet the social expectations of what it means to be a good mother” and provide proper care for the baby.
It was observed that erroneous perceptions persist among certain health professionals, who stigmatize PD. One of the directors pointed out that PPD was something recent “…because before, women did not have time to get depressed, they immediately had to go back to what they were supposed to do”, while nurses thought it was because “they do not use birth control and have several children.”
Detection and Treatment
The directors of the health centers said that as a result of their administrative functions, they do not have direct contact with the users who come to their center, and therefore have limited information on the occurrence of postpartum depression. However, they thought that there were only a few cases of the latter. It is striking that perinatal mental health is not included among the Work Plan Indicators directors are obliged to report to their superiors. As a result, they do not request this information from the health personnel who work at their centers, far less order that actions be taken to address the issue (Table 2).
Even though doctors are responsible for prenatal care and monitoring the health of newborn babies, they do not systematically inquire about the mental health of women. In some cases, in which they find symptoms such as “sadness, crying and detachment from the infant”, which they regard as indicators that something is amiss—they attempt to confirm with family members whether this happens frequently.
They also detect that there are emotional problems in women, when they continuously present physical problems such as “colitis or headache, or when babies are underweight or have other health problems.” In these cases, doctors provide brief guidance and if necessary, prescribe antidepressants. When they consider that the problem is severe, they refer patients to the psychology or psychiatry department of the health center. If this service is overwhelmed, patients are referred to the social work department to find another center that will provide low-cost care.
For nurses and social workers, lack of personal grooming, being uninterested in having a conversation or failing to remember basic things such as dates of birth, and crying, are indicators that the woman may have an emotional problem. However, nurses usually feel that women should be able to solve this problem themselves, without offering any type of help. They think it is enough “for them to want to feel better.” When social workers, identify a woman with possible postpartum depression, they talk to her on their own initiative, offer advice, and remind her that there is a psychologist at the health center. However, this communication is informal, and they do not follow up on the case.
At the same time, mental health personnel consider that doctors take a long time to identify cases of postpartum depression, which partly explains why women do not “seek care.” They note that very few women visit the mental health services of a health center of their own accord. They usually do so after they hear a talk, organized by the social work staff, about emotions during the perinatal period. However, it is unusual for social workers to become directly involved due to their work overload.
Perception of Participants of the Barriers and Necessary Actions for the Prevention and Early Detection of Perinatal Depression
Table 3 shows the categories of the barriers to PD care, as well as the actions that could encourage its detection and prevention. As can be seen from the answers of the participants, the main barriers are structural and involve the institutional practice of designing health programs that fail to consider the care needs of women. At the same time, the work programs implemented during every new administration are poorly planned. In addition, they are not assigned sufficient budgets or human resources to run them. Health personnel, who already face work overload, are affected by these measures since they must perform these new functions without receiving any training or support. For this reason, one of the directors interviewed thought that PD prevention and detection should be the sole responsibility of mental health staff. However, this view obviates the possibility of early identification of cases of PD, since doctors and nurses have the greatest contact with women and are therefore able to detect and refer possible cases.
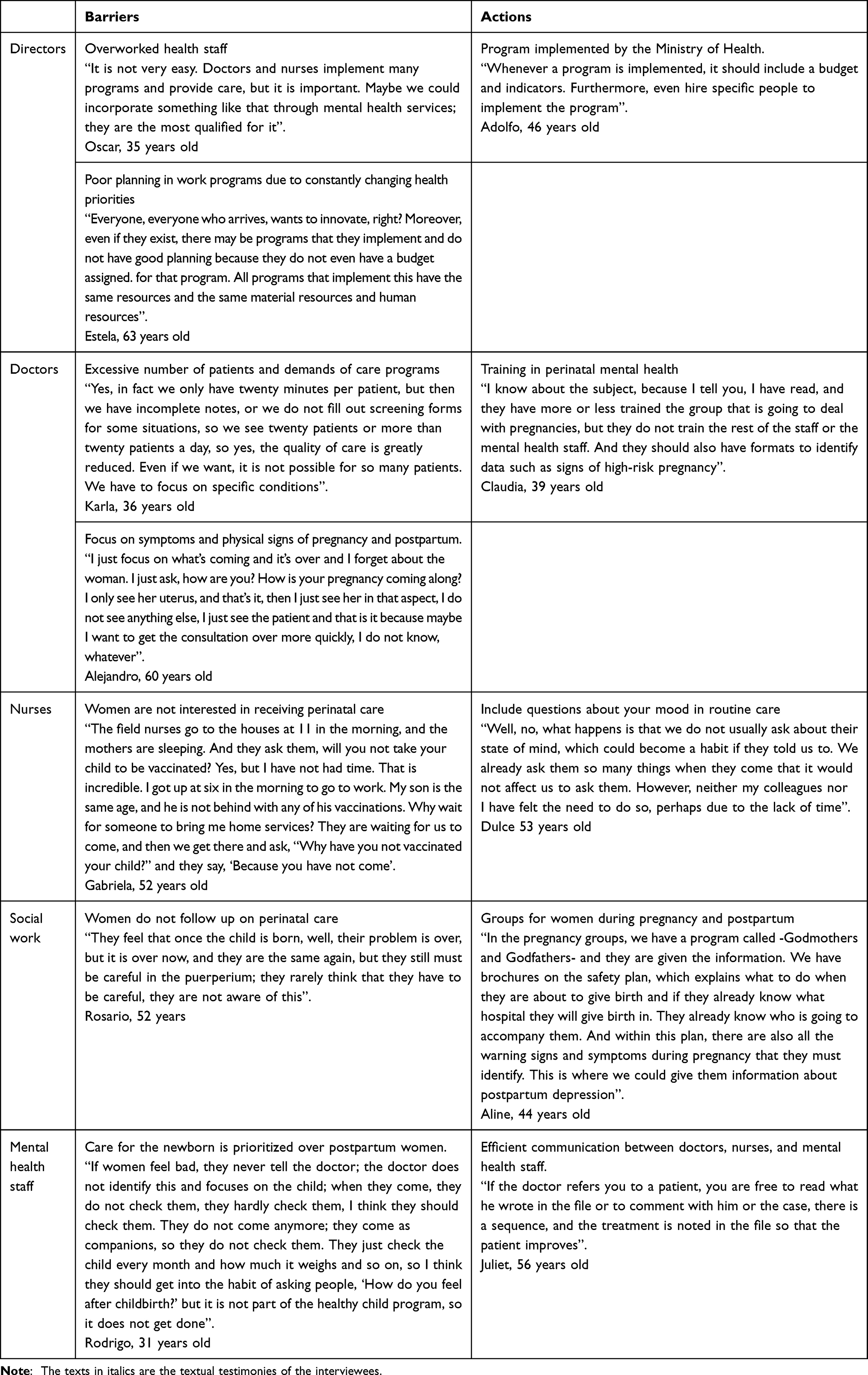 |
Table 3 Fragments of Interviews on the Topic of Barriers and Actions for the Implementation of Postpartum Depression Programs |
In addition, other respondents mentioned that the time allocated for medical consultation is extremely limited and insufficient for the detection of problems other than those included in their checklists, and that there is a lack of suitable spaces for providing mental health care. Another barrier is the obsolete programs that continue to be implemented in care centers, based on a fragmented vision of health, which prioritizes physical over mental health, particularly maternal mental health. As can be seen from the answers of the respondents, some reported that doctors sometimes administer medication (psychopharmaceuticals) unnecessarily, without undertaking a psychological follow-up of the causes of their emotional distress.
At the same time, there are certain entrenched practices that show that health and reproductive health programs are failing to reach the target population. These problems continue to be addressed within a welfare framework, as borne out by the answers of the respondents. For example, when a nurse asks a patient she visits in her community, “Why haven’t you vaccinated your child?” the woman replies, “because you didn’t come.” These practices prevent the population from becoming involved in their health-disease-care process, in addition to contributing to the exhaustion of health personnel. The latter end up blaming women for the problem, stating that women have no interest in prenatal care, lack information or only seek help when they have physical symptoms that interfere with their activities. In this regard, it is worth reflecting that, rather than blaming women, maternal health should be a priority issue that is the responsibility of state public health policies.
Finally, regarding the actions required to promote better care for postpartum depression, respondents mentioned the importance of having the Ministry of Health implement programs that would include specific actions for the care of these women. Actions could include training health staff to provide them with the tools for mental health care; encouraging collaborative work between professionals from the different disciplines involved in care, and the detection of emotional problems in groups organized by social workers, such as healthy pregnancy and early stimulation, which could promote better, more comprehensive care.
It should be noted that female social workers showed the greatest willingness and interest in becoming involved in preventive actions provided they had the support of psychology staff, and in giving women information on the emotional changes that take place during this period, PD, the identification of support needs and providing help for their families.
Discussion
The results of this study provide an overview of the knowledge, perceptions, barriers and actions required by health and administrative staff at primary health care centers offering pregnancy care. These results show how prepared these centers are to detect and prevent PD, as suggested by the Official Standard on “The care of women during pregnancy, childbirth and the puerperium, and of the newborn.”
In the first instance, most health professionals were found to be unaware of the clinical guidelines in the protocols for the detection and care of PD. Likewise, depression during this period is not considered a priority health problem by health authorities. The directors of the centers perceive that their function is to follow the indicators stipulated by the health jurisdictions. Accordingly, they do not feel it is their responsibility to establish programs or actions that would enable PD to be detected or reported.
This is how, although PD is included in maternal and childcare regulations, there is no initiative for it to be conveyed to health personnel or for it to be included in routine care.17 A similar situation occurs in other countries such as the United Kingdom and Australia, where a care policy for women suffering from PD contingent on obstetric care has already been implemented. However, despite this policy, there are deficiencies such as the fact that PD is not always identified in a timely manner, because detection instruments are inconsistently used.25 In this regard, it is important to reflect on the importance of implementing actions designed to raise awareness and train health personnel as part of their functions for the correct identification of possible risk factors that may affect pregnancy and the postpartum period, beyond merely focusing on the regulations that force them to provide care.
Previous studies have shown the usefulness of interventions designed for health personnel in which they are trained to manage perinatal depression, provided with resources so that they can trust their case management skills, recognize the importance of their participation in prevention and early detection actions, and become aware of the suffering depression can cause perinatal women.26
Other possible barriers include the lack of knowledge reported by respondents about postpartum depression and its potential causes. Health personnel views depression as the result of hormonal changes. Similar results were found primary health care staff conceptualize postpartum depression as a biochemical matter resulting from hormonal adjustments due to the baby’s birth.27 A possible explanation could be that doctors and nurses receive limited information on mental health during their training, as a result of which they find it extremely difficult to identify the symptoms associated with PD.28 Although it is true that reproductive hormones modulate emotional, behavioral, and cognitive responses in women during pregnancy and postpartum,29 PD is multicausal and the presence of psychosocial factors plays a fundamental role in its development.30
The emphasis on hormonal aspects by respondents can be explained by a gender bias, in which PD is normalized. For this reason, health professionals must be sensitive to the gender perspective in health problems and individual experiences between men and women. They must also be aware of the social and cultural context in which care is provided, including doctor-patient relationships31 so as not to overlook perinatal mental health problems.
Along these lines, it is important to reflect on the beliefs of health professionals regarding motherhood and the way they impact care for pregnant and postpartum women. Despite the changes that have occurred regarding the role of women in society, it is still considered that the main function of women is reproduction, and that this moment should be lived naturally and joyfully.32 This raises the question of how the view that motherhood is the most satisfying and rewarding experience for women is maintained when they suffer from PD. Although this is a pervasive notion regardless of the gender of the respondent, the most extreme position was observed in men. Accordingly, men perceived PPD as a passing fad that used not to occur, since women were devoted to raising their children. Some of the women interviewed agree with this view and consider that the difficulty of accepting the changes in their bodies is the most important reason for emotional distress, which, in turn, leads them to neglect their infants. Respondents who suffered from PD or who knew someone close to them who had suffered from it are more empathetic and recognize the importance of mental health care in this period. At the same time, empathy on the part of health personnel is something that enables women to have a greater adherence to health services, particularly when they feel listened to and identified by care providers.33
The discourse of most doctors, nurses and managers shows that maternal and child health care, which is a window for detecting and treating postpartum depression, focuses on the well-being of the child and neglects the care of women, who become companions of the baby and are only seen when they have a health problem. This is consistent with a review article on prenatal care and mental health, which found that the lack of mother-centered perinatal care contributes to delays in help-seeking.34
Likewise, some answers suggest that women’s attitudes are to blame for the fact that perinatal care is overlooked, because women fail to regularly attend prenatal and postpartum consultations. This reflects a paternalistic attitude on the part of health professionals, who consider that women’s autonomy leads them make the wrong decisions, which in turn affects the health of their babies and their own health.35 This can also be considered a structural barrier since one of the most deeply rooted practices in health services is the asymmetry in the doctor-patient relationship, in which women are not always given full information. This prevents them from exercising their freedom to be active participants in the decisions made in the doctor’s office regarding their health.
The lack of a protocol for detecting and caring for depression during pregnancy and postpartum sometimes causes doctors and nurses to overlook depressive symptoms or fail to associate them with their perinatal condition, as a result of which they follow the established route to care for clinical depression. This can either help women achieve psychological care in time or alienate them because their emotional needs during pregnancy and postpartum are not considered.36 Likewise, the workload and the duration of the consultations leads to the prioritization of physical health, as a result of which doctors do not ask patients about their mood, as has been reported in other countries.14 Other studies found that health personnel who were concerned about the emotional well-being of pregnant women and spent their consultation time talking about this with them, were regarded by their colleagues as “slow” and inefficient.34 As a result, much to their regret, they stopped doing so, even though they knew they could give women useful information. This means that women do not find an atmosphere of trust in the nursing or medical staff in which to express their emotions.27
It is important to note that there is no collaboration between health personnel, which could contribute to enhancing care for women. On the contrary, there is a division of labor and communication is limited. For example, little communication is observed between mental health staff and medical staff (such as family doctors and nurses), who, although they share information through patient files, do not engage in direct communication that would enable them to monitor their patients’ mental health. This observation is consistent with other studies that note that the lack of communication between health personnel, teamwork and the absence of protocols specifying who should detect PD, and who they should be referred to delays psychological care for women with depressive symptoms for years.27,34
The personnel most aware of the emotional needs of women during pregnancy and postpartum are social workers. Including the latter in the prevention and detection of PD can be extremely positive since they constitute a key link between women and the institution. Social workers refer women to hospital care at the time of delivery and provide information through “healthy pregnancy” and “early stimulation” groups.
Social workers report that they detect signs of depression in women such as carelessness in their personal grooming and sadness, in addition to the fact that women sometimes talk to them directly about their relationship and family problems. In Mexico, people seeking specialized mental health care generally go to primary health care, where their first contact is with social workers, who refer them to mental health personnel or institutions where they can receive care.37 This underlines the importance of these health personnel, who can play a key role in the detection of PD, since they are willing to become more involved with pregnant and postpartum women and are sensitive to their emotional needs.
It is also important to bear in mind the groups that social workers coordinate, because they are spaces where women can share their experiences during pregnancy and postpartum. If they are included in early stimulation sessions, the management of emotions in women and the participation of mental health personnel can help overcome some of the barriers mentioned by women to help seeking, such as not knowing that this service exists in their clinic and what they must do to make an appointment with the psychology department.34,38
It is worth remembering that, although PPD is the best-known type of depression in the medical field, prevention and treatment should not be restricted to this period since disabling depressive symptomatology is present from the time of pregnancy and addressing it in a timely manner can reduce the severity of subsequent consequences in both mother and baby.
Strength and Limitations
This study is important because it is one of the few in Mexico to show the current status of health centers that care for women during pregnancy and postpartum in terms of PD care. It may also help health authorities to plan public health measures to improve maternal and child health.
These findings are limited by the small number of health centers evaluated, since the study was restricted to Mexico City. At the same time, some of the health professionals’ answers may have been biased because the interviews were conducted in their work areas. Although every attempt was made to create an environment of trust and confidentiality, sometimes respondents did not provide further details for fear of receiving a negative evaluation of their work.
At the same time, the number of people interviewed was established by the research protocol and could not be modified in the study, meaning that there were not enough interviews to complete the theoretical saturation. Thus, more health professionals should be interviewed to achieve a better understanding of the barriers to implementing perinatal mental health detection and prevention strategies at the primary health care level.
For future research, it would be advisable to include interviews with the authorities of the jurisdictions and with other decision makers, and to consider women who receive care during pregnancy and postpartum.
Conclusion
This study has found that health centers are currently unprepared to deal with PD since although there is a standard that suggests it should be addressed and clinical guidelines for doing so, this problem has not been included in priority health programs, meaning that directors of the centers are not obliged to treat it. Staff who care for women in pregnancy and postpartum are unaware of the problem and lack the knowledge, training, time, and organization to detect and prevent PD. Women’s low adherence to medical care during pregnancy and postpartum also hampers detection and follow-up. The attitude and closeness of social workers to the women who come to the center may help prevention activities by promoting the monitoring of women’s physical and mental health during pregnancy and postpartum.
Ethics Approval and Consent to Participate
This project was approved by the Research Ethics Committee of the Ramón de la Fuente Muñíz National Institute of Psychiatry (CEI/C/036/2018). All methods were performed in accordance with relevant guidelines, regulations, and the principles of the Declaration of Helsinki. All participants were informed about the confidentiality of the information and the study’s purpose, and they were only enrolled in the study if they agreed to do so, after which signed informed consent was obtained.
Acknowledgments
We are grateful to the Ramón de la Fuente Muñiz National Institute of Psychiatry, the Mexico City Ministry of Health, particularly Feliciano Bartolo Solís, and the participants who shared their experiences to make this study possible. Thanks are due to the Master’s and Doctoral Program in Medical, Odontology, and Health Sciences (PMDCMOS) of the National Autonomous University of Mexico. We would also like to thank Valeria Zempoalteca García for her support and feedback in the data analysis, and social service students Dania Ruiz Alarcón, Sarahit Guzmán Corona, Ma. Elena Sánchez Enciso and Delia Vázquez Méndez, who helped with the transcription and review of the interviews.
Author Contributions
All the authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas. They took part in drafting, revising or critically reviewing the article; gave their final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from public, commercial, or not-for-profit funding agencies.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. O’Hara MW, McCabe JE. Postpartum depression: current status and future directions. Annu Rev Clin Psychol. 2013;9:379–407. doi:10.1146/annurev-clinpsy-050212-185612
2. Woody CA, Ferrari AJ, Siskind DJ, Whiteford HA, Harris MG. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J Affect Disord. 2017;219:86–92. doi:10.1016/j.jad.2017.05.003
3. Shorey S, Chee CYI, Ng ED, Chan YH, Tam WWS, Chong YS. Prevalence and incidence of postpartum depression among healthy mothers: a systematic review and meta-analysis. J Psychiatr Res. 2018;104:235–248. doi:10.1016/j.jpsychires.2018.08.001
4. Fekadu Dadi A, Miller ER, Mwanri L. Antenatal depression and its association with adverse birth outcomes in low and middle-income countries: a systematic review and meta-analysis. PLoS One. 2020;15(1):e0227323. doi:10.1371/journal.pone.0227323
5. Slomian J, Honvo G, Emonts P, Reginster JY, Bruyère O. Consequences of maternal postpartum depression: a systematic review of maternal and infant outcomes. Womens Health. 2019;15:1745506519844044. doi:10.1177/1745506519844044
6. Letourneau NL, Dennis CL, Cosic N, Linder J. The effect of perinatal depression treatment for mothers on parenting and child development: a systematic review. Depress Anxiety. 2017;34(10):928–966. doi:10.1002/da.22687
7. Hayes LJ, Goodman SH, Carlson E. Maternal antenatal depression and infant disorganized attachment at 12 months. Attach Hum Dev. 2013;15(2):133–153. doi:10.1080/14616734.2013.743256
8. Lara MA, Navarrete L, Nieto L. Prenatal predictors of postpartum depression and postpartum depressive symptoms in Mexican mothers: a longitudinal study. Arch Womens Ment Health. 2016;19(5):825–834. doi:10.1007/s00737-016-0623-7
9. Lara MA, Navarrete L, Nieto L, Martín JP, Navarro JL, Lara-Tapia H. Prevalence and incidence of perinatal depression and depressive symptoms among Mexican women. J Affect Disord. 2015;175:18–24. doi:10.1016/j.jad.2014.12.035
10. Luna D, Castañeda-Hernández DV, Guadarrama-Arteaga AL, et al. Psychometric properties of the Hospital Anxiety and Depression Scale in Mexican pregnant women. Salud Mental. 2020;43(3):137–146. doi:10.17711/SM.0185-3325.2020.019
11. Flom JD, Chiu YM, Tamayo-Ortiz M, et al. Subconstructs of the Edinburgh postpartum depression scale in a postpartum sample in Mexico City. J Affect Disord. 2018;238:142–146. doi:10.1016/j.jad.2018.05.049
12. Falek I, Acri M, Dominguez J, et al. Management of depression during the perinatal period: state of the evidence. Int J Ment Health Syst. 2022;16(1):21. doi:10.1186/s13033-022-00531-0
13. Buist AE, Austin MP, Hayes BA, et al. Postnatal mental health of women giving birth in Australia 2002–2004: findings from the beyondblue national postnatal depression program. Aust N Z J Psychiatry. 2008;42(1):66–73. doi:10.1080/00048670701732749
14. Milgrom J, Gemmill AW. Screening for perinatal depression. Best Pract Res Clin Obstet Gynaecol. 2014;28(1):13–23. doi:10.1016/j.bpobgyn.2013.08.014
15. Secretaría de Salud. Norma Oficial de Atención del Embarazo y Posparto (NOM-007-SSA2-2016). Secretaria de Salud; 2018. Available from: https://www.dof.gob.mx/normasOficiales/5950/salud12_C/salud12_C.html.
16. Secretaría de Salud. Guía de Práctica Clínica “Prevención, Diagnóstico y Manejo de la Depresión Prenatal y Posparto en el Primero y Segundo Niveles de Atención”. Secretaria de Salud; 2021. Available from: http://www.cenetec-difusion.com/CMGPC/GPC-SS-666-21/ER.pdf.
17. Place JM, Billings DL, Frongillo EA, et al. Policy for promotion of women’s mental health: insight from analysis of policy on postnatal depression in Mexico. Adm Policy Ment Health. 2016;43(2):189–198. doi:10.1007/s10488-015-0629-x
18. Lara MA, Patiño P, Navarrete L, Nieto L. Depresión posparto, un problema de salud pública que requiere de mayor atención en México. Género y Salud en Cifras. 2017;15:12–22.
19. Weiner BJ. A theory of organizational readiness for change. Implement Sci. 2009;4(1):67. doi:10.1186/1748-5908-4-67
20. Langlois EV, Becerril Montekio V, Young T, Song K, Alcalde-Rabanal J, Tran N. Enhancing evidence informed policymaking in complex health systems: lessons from multi-site collaborative approaches. Health Res Policy Syst. 2016;14:20. doi:10.1186/s12961-016-0089-0
21. Bradshaw C, Atkinson S, Doody O. Employing a qualitative description approach in health care research. Glob Qual Nurs Res. 2017;4:2333393617742282. doi:10.1177/2333393617742282
22. Díaz-Bravo L, Torruco-García U, Martínez-Hernández M, Varela-Ruiz M. La entrevista, recurso flexible y dinámico. Investigación en educación médica. 2013;2(7):162–167. doi:10.1016/s2007-5057(13)72706-6
23. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
24. VERBI Software. MAXQDA 2022. Berlin: VERBI Software; 2021.
25. Hazell Raine K, Thorpe K, Boyce P. Perinatal depression screening in Australia: a position paper. Nurs Health Sci. 2021;23(1):279–287. doi:10.1111/nhs.12793
26. Phoosuwan N, Lundberg PC, Phuthomdee S, Eriksson L. Intervention intended to improve public health professionals’ self-efficacy in their efforts to detect and manage perinatal depressive symptoms among Thai women: a mixed-methods study. BMC Health Serv Res. 2020;20(1):138. doi:10.1186/s12913-020-5007-z
27. Place JM, Billings DL, Blake CE, Frongillo EA, Mann JR, deCastro F. Conceptualizations of postpartum depression by public-sector health care providers in Mexico. Qual Health Res. 2015;25(4):551–568. doi:10.1177/1049732314552812
28. Viveiros CJ, Darling EK. Perceptions of barriers to accessing perinatal mental health care in midwifery: a scoping review. Midwifery. 2019;70:106–118. doi:10.1016/j.midw.2018.11.011
29. Trifu S, Vladuti A, Popescu A. The neuroendocrinological aspects of pregnancy and postpartum depression. Acta Endocrinol. 2019;15(3):410–415. doi:10.4183/aeb.2019.410
30. Dagher RK, Bruckheim HE, Colpe LJ, Edwards E, White DB. Perinatal depression: challenges and opportunities. J Womens Health. 2021;30(2):154–159. doi:10.1089/jwh.2020.8862
31. Celik H, Lagro-Janssen TA, Widdershoven GG, Abma TA. Bringing gender sensitivity into healthcare practice: a systematic review. Patient Educ Couns. 2011;84(2):143–149. doi:10.1016/j.pec.2010.07.016
32. Ambrosini A, Stanghellini G. Myths of motherhood. The role of culture in the development of postpartum depression. Ann Ist Super Sanita. 2012;48(3):277–286. doi:10.4415/ANN_12_03_08
33. Biggs LJ, McLachlan HL, Shafiei T, Liamputtong P, Forster DA. ‘I need help’: reasons new and re-engaging callers contact the PANDA-perinatal anxiety and depression Australia national helpline. Health Soc Care Comm. 2019;27(3):717–728. doi:10.1111/hsc.12688
34. Sambrook Smith M, Lawrence V, Sadler E, Easter A. Barriers to accessing mental health services for women with perinatal mental illness: systematic review and meta-synthesis of qualitative studies in the UK. BMJ Open. 2019;9(1):e024803. doi:10.1136/bmjopen-2018-024803
35. Bullock E. Paternalism and the practitioner/patient relationship. In: Grill K, Hanna J, editors. The Routledge Handbook of the Philosophy of Paternalism. Ney York: Taylor & Francis; 2018.
36. Cochran AL, Pingeton BC, Goodman SH, et al. A transdiagnostic approach to conceptualizing depression across the perinatal period in a high-risk sample. J Abnorm Psychol. 2020;129(7):689–700. doi:10.1037/abn0000612
37. Saavedra NI, Berenzon S, Galván J. The role of social workers in mental health care: a study of primary care centers in Mexico. Qualitative Social Work. 2019;18(6):1017–1033. doi:10.1177/1473325018791689
38. Lara MA, Navarrete L, Nieto L, Berenzon S. Acceptability and barriers to treatment for perinatal depression. An exploratory study in Mexican women. Salud Mental. 2014;37(4):293. doi:10.17711/sm.0185-3325.2014.034
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.