")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 14
CHA2DS2-VASc, a Simple Clinical Score Expanding Its Boundaries to Predict Contrast-Induced Acute Kidney Injury After Primary Percutaneous Coronary Interventions
Authors Kumar R, Batra MK, Khowaja S, Ammar A, Kumar A, Shah JA, Sial JA, Saghir T, Karim M
Received 2 November 2021
Accepted for publication 9 December 2021
Published 31 December 2021 Volume 2021:14 Pages 495—504
DOI https://doi.org/10.2147/IJNRD.S347303
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Pravin Singhal
Rajesh Kumar,1 Mahesh Kumar Batra,1 Sanam Khowaja,1 Ali Ammar,1 Ashok Kumar,1 Jehangir Ali Shah,1 Jawaid Akbar Sial,1 Tahir Saghir,1 Musa Karim2
1Adult Cardiology Department, National Institute of Cardiovascular Diseases (NICVD), Karachi, Pakistan; 2Research Department, National Institute of Cardiovascular Diseases (NICVD), Karachi, Pakistan
Correspondence: Rajesh Kumar
National Institute of Cardiovascular Diseases (NICVD), Karachi, Pakistan
Email [email protected]
Objective: Promising results of CHA2DS2-VASc score have been reported for the prediction of contrast-induced acute kidney injury (CI-AKI) after percutaneous coronary intervention (PCI). However, data of its predictive strength in the context of primary PCI are not available. Therefore, in this study, we have assessed predictive value of CHA2DS2-VASc score for CI-AKI after primary PCI.
Methods: This analytical cross-sectional study was conducted between January 2021 and June 2021 at the National Institute of Cardiovascular Diseases (NICVD), Karachi, Pakistan. Inclusion criteria of the study was consecutive adult patients who had undergone primary PCI. Baseline CHA2DS2-VASc score was calculated, and either a 25% or 0.5 mg/dL increase in post-procedure serum creatinine level as compared to baseline level was categorized as CI-AKI.
Results: A total of 691 patients were included, of which 82.1% (567) were male. CI-AKI after primary PCI was observed in 63 (9.1%) patients, out of which 66.7% (42) of patients had CHA2DS2-VASc score of ≥ 2. The area under the curve (AUC) for the score was 0.725 [0.662 to 0.788] with a sensitivity and specificity of 66.7% [63.1% to 70.2%] and 66.7% [53.7% to 78.1%], respectively, at a cut-off value of ≥ 2. In multivariable analysis, left ventricular ejection fraction ≤ 30% and CHA2DS2-VASc ≥ 2 were found to be independent predictors with adjusted odds ratios of 2.19 [1.06– 4.5] and 2.13 [1.13– 4.01], respectively.
Conclusion: CHA2DS2-VASc score has a good predictive value for the prediction of CI-AKI after primary PCI. Criteria of CHA2DS2-VASc ≥ 2 can be used for the risk stratification of CI-AKI after primary PCI.
Keywords: ST elevation myocardial infarction, STEMI, percutaneous coronary intervention, primary PCI, contrast-induced acute kidney injury, CI-AKI, CHA2DS2-VASc score, contrast-induced nephropathy, CIN
Introduction
According to current clinical practice guidelines by the American College of Cardiology Foundation/American Heart Association (ACCF/AHA)1 and the European Society of Cardiology (ESC),2 the primary percutaneous coronary intervention (PCI) remains the first line treatment option for patients with ST-segment elevation myocardial infarction (STEMI) presenting to a PCI capable center within 12 hours of symptom onset. Adoption of primary PCI strategy has resulted in a significant improvement in outcomes of patients with STEMI,3 however, risk of contrast-induced acute kidney injury (CI-AKI), also called contrast-induced nephropathy (CIN), remains high in these patients with the reported incidence rate ranging from 5.5% to 21.6% in various studies depending on the definition used for the categorization of CI-AKI and inclusion criteria.4–20 CI-AKI is found to be associated with an increased risk of need for dialysis and mortality,16 chronic kidney disease (CKD) followed by CI-AKI in these patients, is found to be associated with an increased risk of long term adverse outcomes.21
In recent years, several studies have been performed evaluating various risk stratification tools and biomarkers in the context of CI-AKI after primary PCI which included the Mehran risk score (MRS),7,17 plasma N-terminal pro-brain natriuretic peptide (NT-proBNP),7,18 gamma-glutamyl transferase (GGT),20 thrombolysis in myocardial infarction risk index (TRI),8 PRECISE-DAPT risk score,10 Canada Acute Coronary Syndrome (C-ACS) score,11 fragmented QRS complexes (fQRS),12 and a combination of various other tools.13,15 However, search for an optimal risk stratification tool still continues which would be simple enough for clinical adoption yet is accurate enough to rely upon for clinical decision making. The two most recent studies by Chaudhary et al22 and Kurtul et al23 have reported promising results for CHA2DS2-VASC score with area under the curve (AUC) of 0.81 [95% CI: 0.73–0.90] and 0.769 [95% CI: 0.733–0.805] respectively for prediction of CI-AKI after PCI in patients with acute coronary syndrome (ACS). However, data regarding the predictive strength of this well-known embolic risk stratification modality is not available in the context of primary PCI for STEMI. Additionally, among various available risk stratification models for acute kidney injury (AKI), CHA2DS2-VASC score is more clinician-friendly and easy to adopt, especially in an emergency setting.24 Furthermore, CI-AKI is considered to be largely associated with baseline renal function, however, CHA2DS2-VASC score is independent of baseline kidney function therefore, it can be an effective tool for patients without pre-existing renal conditions.25 However, a recent study by Kumar et al26 reported CHA2DS2-VASc score to have poor discriminating power as compared to the MRS in contrast to the earlier studies in ACS patients. Therefore, this study was designed to assess the predictive value of CHA2DS2-VASc score for CI-AKI after primary PCI among patients with STEMI presented to a tertiary care cardiac center of Karachi, Pakistan.
Materials and Methods
This analytical cross-sectional study was conducted between January 2021 and June 2021 at the National Institute of Cardiovascular Diseases (NICVD), Karachi, Pakistan. The study protocol was approved by the ethical review committee (ERC) of the NICVD, Karachi (ERC-56/2021). As per the Declaration of Helsinki the purpose of the study was explained to all the participants and verbal consent was obtained from all the patients regarding their participation in this study. Due to the observational nature of the study written consent was waived and verbal informed consent was approved by the institutional ERC. Inclusion criteria of the study were consecutive adult patients (≥ 18 years) of either gender presented with STEMI and who had undergone primary PCI. Patients with chronic kidney disease (CKD) at baseline or on hemodialysis, prior myocardial infarction (MI), or in Killip class IV or in cardiogenic shock at presentation were excluded from the study. Additionally patients with contrast medium exposure within 1 week of the procedure were also excluded. The purpose of excluding this particular subset of patients with high risk features was to minimize biasness in the assessment of predictive value due to expected high incidence of complications in this particular group. Secondly, in general patients with high risk features tend to receive more close monitoring in comparison to relatively stable patients, therefore, this particularly stable group of patients may most benefit from a systematic risk assessment for the development of complications.
Baseline demographic and clinical characteristics were recorded on a predefined structured proforma. Baseline demographics and clinical characteristics consisted of age, gender, vitals at presentation (heart rate and blood pressure), serum creatinine level on arrival, type of MI, Killip class at presentation, and total ischemic time (the time between onset of symptoms and device activation). All PCI procedures were performed as per the institutional protocols and current clinical practice guidelines1 by the experienced interventional cardiologists. Angiographic and procedural characteristics such as number of diseased vessels, culprit artery, thrombus grade, vessel length and diameter, left ventricular end-diastolic pressure (LVEDP), left ventricular ejection fraction (LVEF), fluoroscopy time, and contrast volume were recorded. Pre and post procedure pharmacological and non-pharmacological management was the same for all the patients.
Diagnosis of STEMI was made based on history and presenting electrocardiography (ECG) as per the 4th universal definition of MI. The CHA2DS2-VASc risk score was calculated for all the patients at the time of presentation based on scoring schema proposed by Lip et al.27 A score of 1 for each of the parameters namely history of heart failure (C), hypertension (H), diabetes (D), vascular disease (V), female, and age 65–74 years of age and a score of 2 for each of the parameters namely of history of stroke (S2) and age equal to or higher than 75 years. MRS was also computed in accordance with the criteria defined by Mehran et al.28
Serum creatinine level after 48 to 72 hours of primary PCI were noted and CI-AKI was defined as either a 25% or 0.5 mg/dL increase in post-procedure serum creatinine level at 48 to 72 hours as compared to the baseline level.29 Even though several other definitions are available, such as KDIGO (Kidney Disease Improving Global Outcomes) criteria, to define acute kidney injury but in this study we have adopted the most commonly used definition of CI-AKI in the context of percutaneous coronary interventions.29 Along with CI-AKI various other post-procedure in-hospital complications were recorded which included slow flow/no-reflow (defined as 0-II intra-procedure TIMI flow), arrhythmias (needing pharmacotherapy), access site complications, bleeding (needing transfusion), cardiogenic shock, dissection, stroke (ischemic or hemorrhagic), and reinfarction (stent thrombosis).
Data analysis was performed with the help of IBM SPSS version 21. Collected data were summarized as mean ± standard deviation (SD) or frequency and percentage appropriately. Normality of distribution was tested with a Kolmogorov–Smirnov test and visual assessment of histogram. Variables with potentially skewed distribution were expressed as median [interquartile range (IQR)]. The ROC curve analysis was performed and AUC [95% confidence interval (CI)] was computed for both CHA2DS2-VASc score and MRS. The optimal cutoff value of CHA2DS2-VASc score to predict CI-AKI was determined by using the Youden Index (J statistic) and accuracy measures such as sensitivity, specificity, positive predictive value, negative predictive value and overall accuracy along with 95% confidence intervals were computed. Patients were categorized based on CI-AKI and clinical and demographic characteristics were compared by applying appropriate chi-square test or Fisher exact test and independent sample t-test or Mann–Whitney U-test. Univariate and multivariable logistic regression analyses for CI-AKI was performed and odds ratios (OR) [95% CI] were computed. Significant clinical and demographic characteristics which were not used for the calculation of CHA2DS2-VASc score were taken as independent variables in the multivariable logistic regression analysis along with CHA2DS2-VASc score. A P value ≤ 0.05 will be considered as statistically significant throughout the analysis.
Results
A total of 691 patients were included, out of which 82.1% (567) were male and the mean age of the study sample was 52.26 ± 10.96 years. Contrast-induced nephropathy was observed in 63 (9.1%) patients which was found to be associated with older age with 34.9% (22) vs 14.3% (90); p<0.001 patients ≥65 years of age in the CI-AKI and non-CI-AKI group respectively. Patients in CI-AKI group, as compared to non-CI-AKI group, were found to have higher total ischemic time (350 [260–500] minutes vs 320 [220–420] minutes; p = 0.033), increased heart rate (88.1 ± 23.3 bpm vs 82.7 ± 18.1 bpm; p = 0.030), high random blood sugar at presentation (163 [130–230] mg/dL vs 140 [121–179.5] mg/dL; p = 0.003), high Killip class III (12.7% (8) vs 3.3% (21); p < 0.001), and arrhythmias on presentation (15.9% (10) vs 6.7% (42); p = 0.008).
Similarly, pre-existing co-morbid conditions were also higher among the CI-AKI group, as compared to the non-CI-AKI group, such as hypertension (60.3% (38) vs 44.1% (277); p = 0.014), diabetes mellitus (46% (29) vs 24% (151); p < 0.001), cerebrovascular accident (4.8% (3) vs 0.8% (5); p = 0.005), congestive heart failure (63.5% (40) vs 32% (201); p < 0.001). High left ventricular end-diastolic pressure (20.3 ± 6.9 mmHg vs 16.6 ± 4.9 mmHg; p < 0.001) and low left ventricular ejection fraction (37.4 ± 9.6% vs 42.4 ± 8.4%; p < 0.001) were also observed in the CI-AKI group as compared to the non-CI-AKI group. Rate of placement of intra-aortic balloon pump was high in the CIN group with a rate of 6.3% (4) vs 0.6% (4); p < 0.001 for the CI-AKI and non-CI-AKI groups respectively. The finding of multi-vessel disease was more common in the CIN group as compared to the non-CI-AKI group with frequency of 31.7% (20) vs 18.2% (114); p = 0.009 respectively.
Mean CHA2DS2-VASc score was significantly higher among the CI-AKI group as compared to the non-CI-AKI group with mean scores of 2.22 ± 1.34 vs 1.16 ± 1.17; p < 0.001, and frequency of patient with score of ≥2 was also significantly higher among the CI-AKI group, 66.7% (42) vs 33.3% (209); p < 0.001, as compared to the non-CI-AKI group respectively.
In-hospital mortality rate was significantly higher in patients with CI-AKI with a mortality rate of 6.3% (4) vs 1.4% (9); p = 0.006 as compared to the non-CI-AKI group respectively. Similarly, post-procedure complications such as slow flow/no-reflow (41.3% (26) vs 15.9% (100); p < 0.001), arrhythmias needing pharmacotherapy (9.5% (6) vs 1.1% (7); p < 0.001), cardiogenic shock (4.8% (3) vs 0.8% (5); p = 0.005), stroke (1.6% (1) vs 0% (0); p = 0.002), and reinfarction (3.2% (2) vs 0.3% (2); p = 0.004) were significantly higher among the CI-AKI group as compared to the non-CI-AKI group respectively (Table 1).
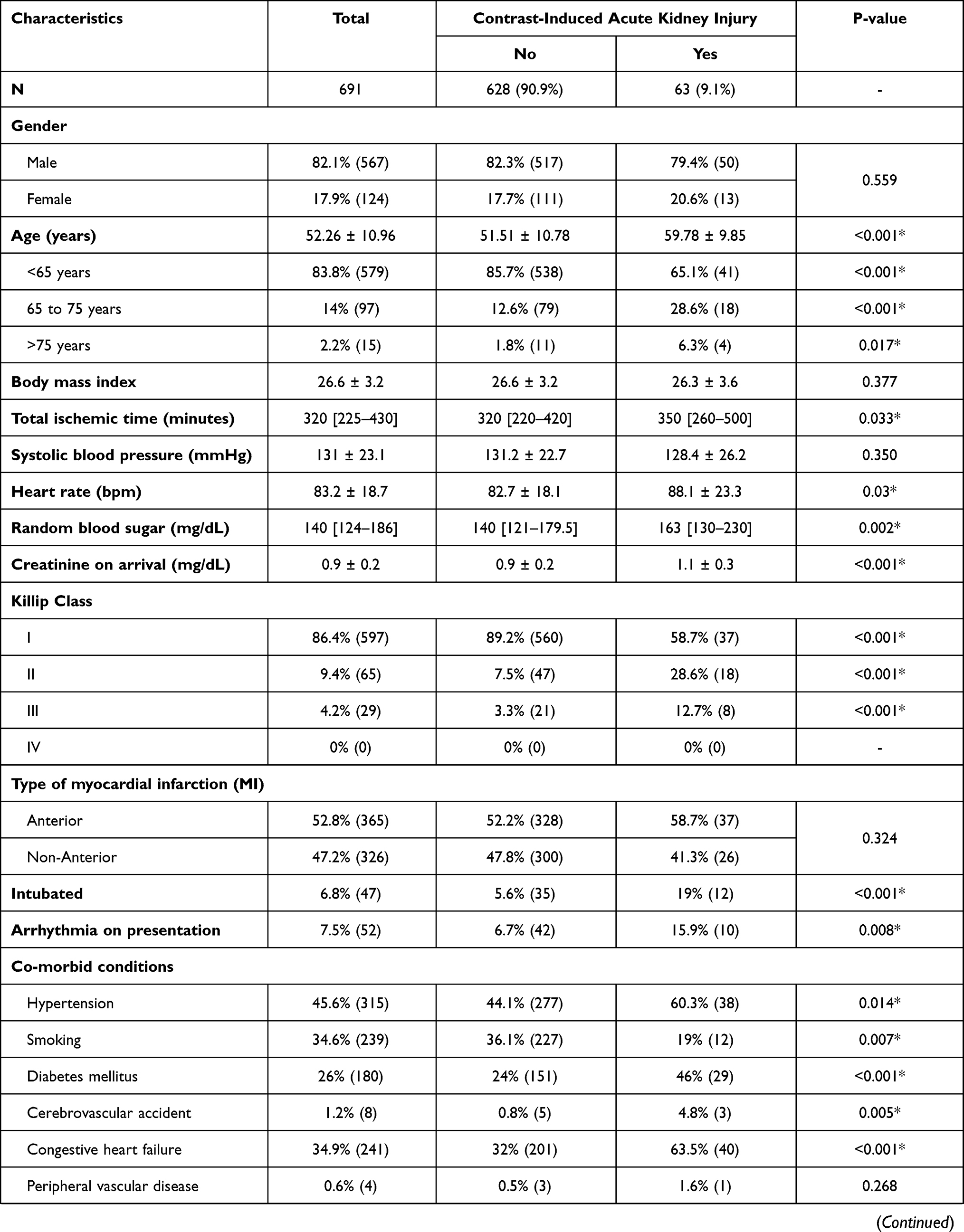 | 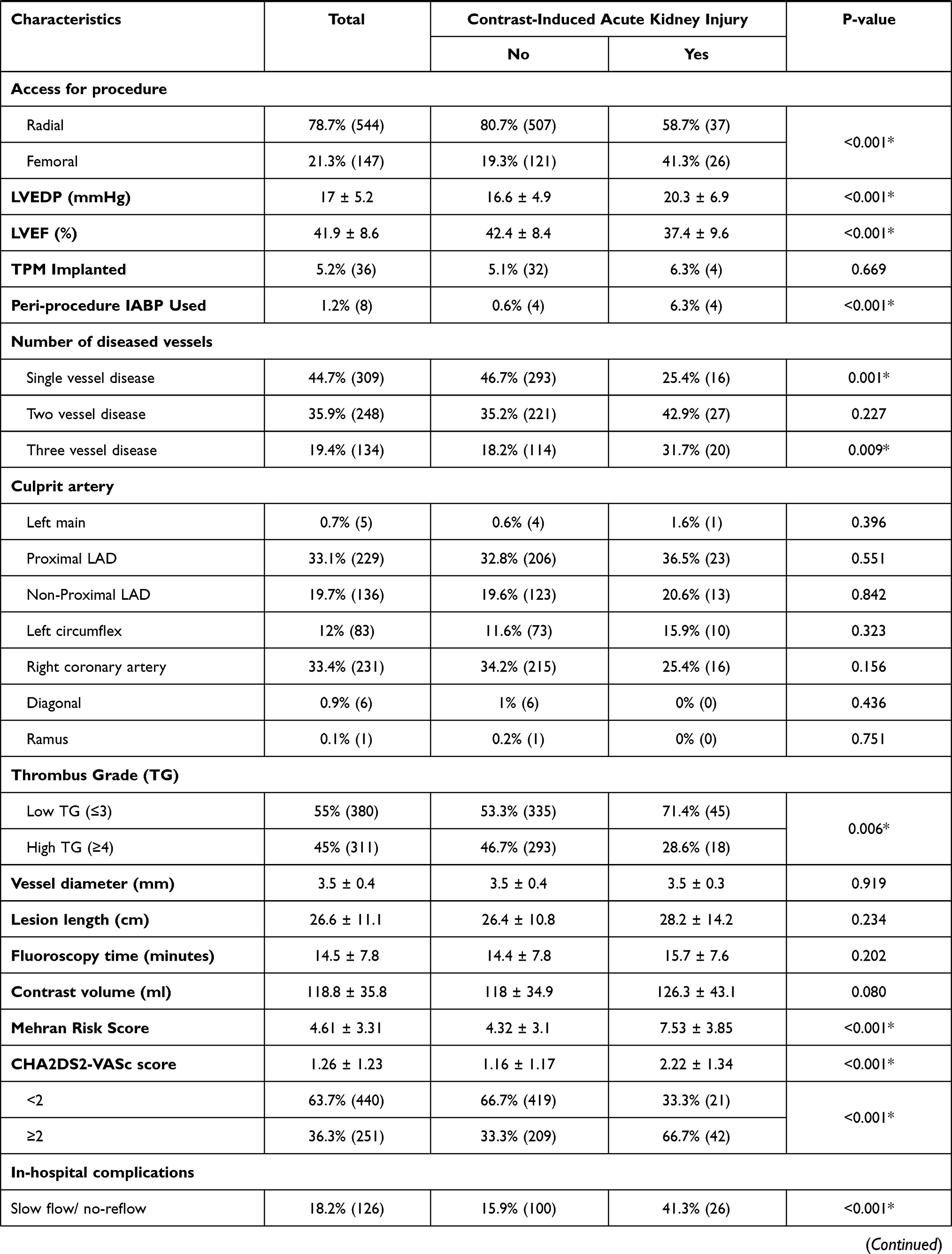 | 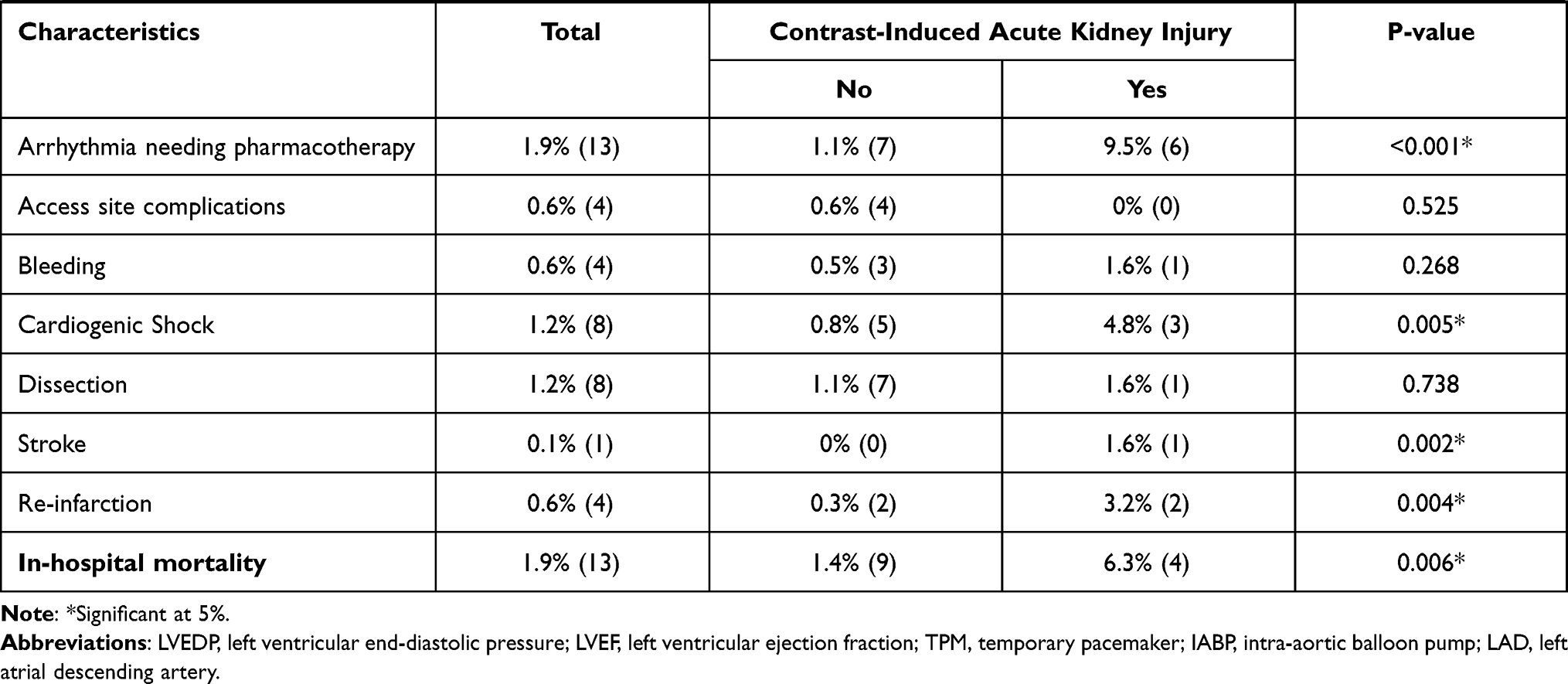 |
Table 1 Demographic, Clinical, and Procedural Characteristics and In-Hospital Outcome of Patients Stratified by Development of Contrast-Induced Acute Kidney Injury |
The AUC of CHA2DS2-VASc score for predicting CI-AKI after primary PCI was 0.725 [0.662 to 0.788] (Figure 1) and the optimal cutoff value was ≥2 with sensitivity of 66.7% [63.1% to 70.2%] and specificity of 66.7% [53.7% to 78.1%]. The rate of CI-AKI was 16.7% (42/251) vs 4.8% (21/440); p < 0.001 for patients with a CHA2DS2-VASc score of ≥2 and <2 respectively. The AUC for the Mehran score was found to be 0.745 [0.679 to 0.810]. Accuracy of the CHA2DS2-VASc score for prediction of CI-AKI after primary PCI is presented in Table 2.
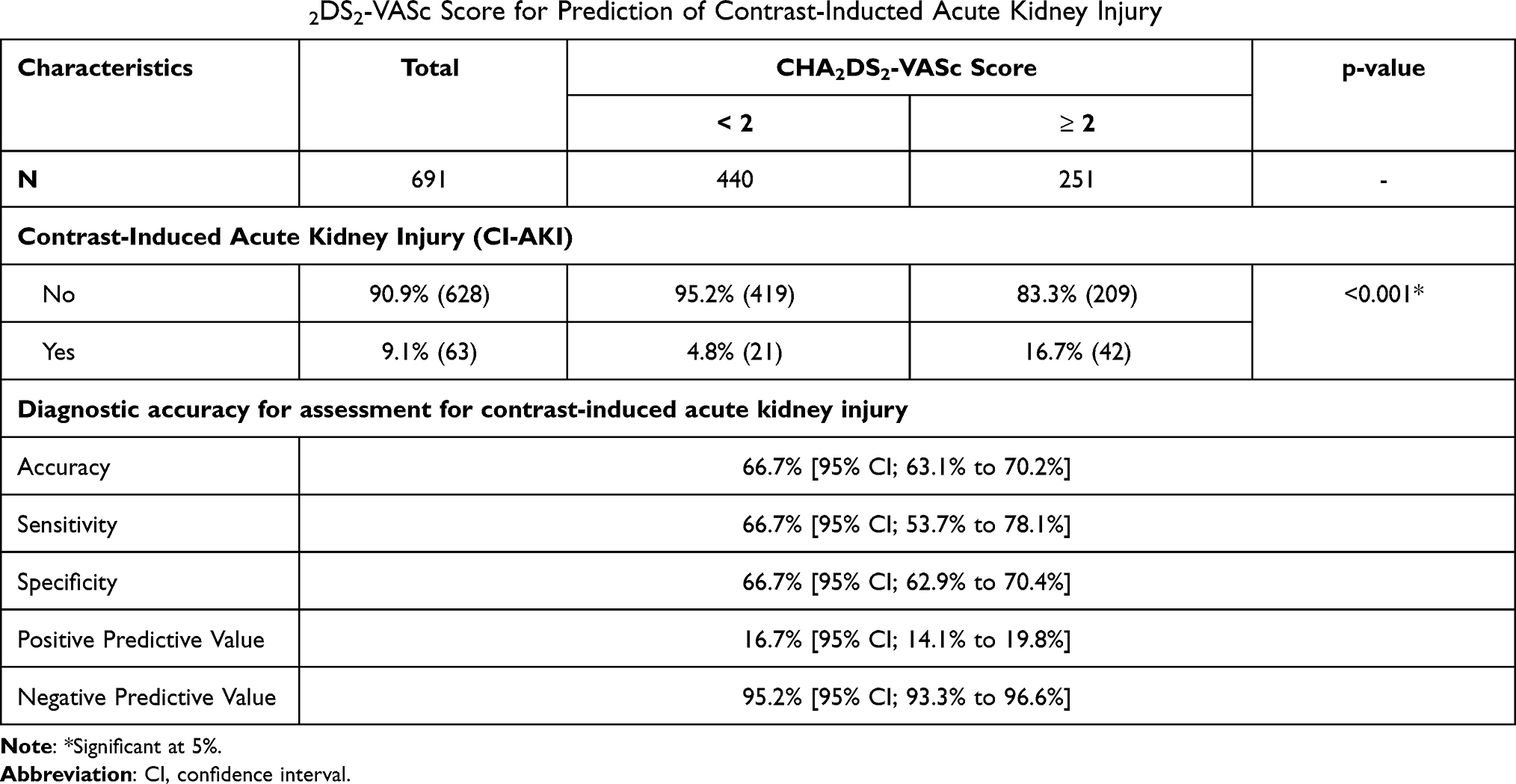 |
Table 2 Accuracy of CHA2DS2-VASc Score for Prediction of Contrast-Inducted Acute Kidney Injury |
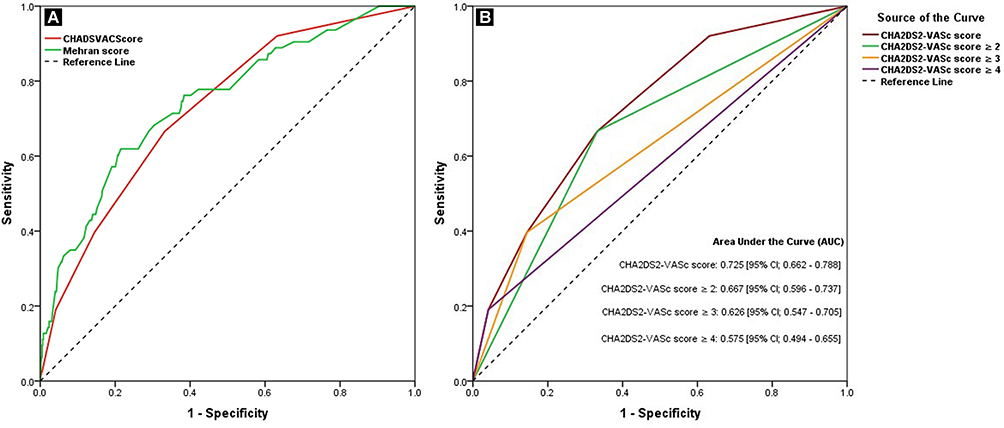 |
Figure 1 ROC curve analysis of Mehran risk score (A) and CHA2DS2-VASc score (B) for prediction of contrast-induced acute kidney injury after primary PCI procedure. |
Univariate and multivariable logistic regression analysis to determine the predictors of CI-AKI after a primary PCI procedure are presented in Table 3. Among the various characteristics, left ventricular ejection fraction of ≤30% and CHA2DS2-VASc score of ≥2 were found to be significantly independent predictors of post primary PCI CI-AKI development with adjusted OR of 2.19 [1.06–4.5] and 2.13 [1.13–4.01] respectively.
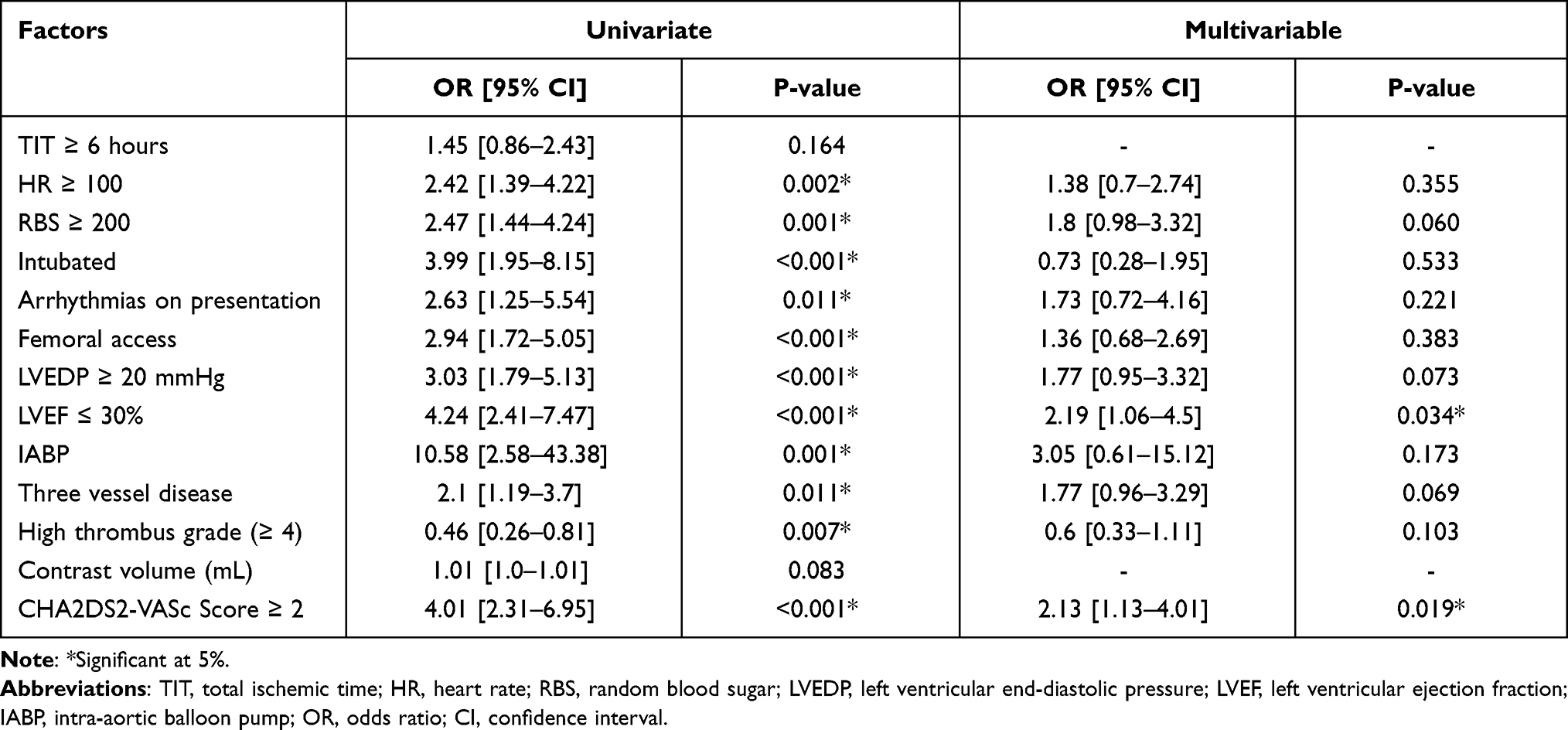 |
Table 3 Predictors of Contrast-Induced Acute Kidney Injury After Primary PCI Procedure |
Discussion
CHA2DS2-VASc score is a simple clinical risk assessment tool initially used for risk stratification of thromboembolism in atrial fibrillation. Now it is expanding its boundaries as a potential risk stratification model for CI-AKI. It is a simple and clinician-friendly scoring system with all the needed parameters readily available, especially in the context of primary PCI. Although patients with high risk features, such as cardiogenic shock or baseline impaired renal function, tend to receive much closer monitoring for peri-procedure complications, including CI-AKI. However, patients without conventional high risk CI-AKI features can most benefit from the CHA2DS2-VASc score based risk stratification before primary PCI. In our study a score value of ≥2 proved to be a good predictor of CI-AKI after primary PCI. This is the first study of its type in the Pakistani population, especially in a primary PCI setting. In this study we have observed significant association between CI-AKI after primary PCI and most of the parameters of CHA2DS2-VASc score namely age, hypertension, diabetes, congestive heart failure, and cerebrovascular accident. Hence, overall predictive power of CHA2DS2-VASc score was good and it was found to be an independent predictor of CI-AKI after primary PCI along with a reduced left ventricular ejection fraction (≤30%). However, reported AUCs of the score in PCI for acute coronary syndrome (ACS) are higher than the one we observed for primary PCI, 0.81 [0.73–0.90]22 and 0.769 [0.733–0.805].23
Among studies with AUC less than or close to the AUC observed for CHA2DS2-VASc score, a study conducted by Araujo et al5 reported a simple risk stratification model namely ACEF-MDRD based on age, glomerular filtration, and ejection fraction and tested against the reported Mehran score AUC of 0.733 [0.68 to 0.78] and 0.649 [0.59 to 0.70] respectively. Oksuz et al20 evaluated the accuracy of gamma-glutamyl transferase (GGT) for risk of CI-AKI after primary PCI in 473 patients and reported an AUC of 0.679. Similarly, the predictive value of thrombolysis in myocardial infarction risk index (TRI) was assessed by Kaya et al8 and the AUC was observed to be 0.740 [0.711 to 0.768].
Various other parameters have shown more promising results such as addition of elevated NT-proBNP to the Mehran score was reported to have an AUC of 0.833 vs 0.793 as against standard defined Mehran.7 N-terminal fragment of pro B-type natriuretic peptide (Nt-proBNP) alone was reported to also be a good predictor of CI-AKI with an AUC 0.74[0.70 to 0.78].18 PRECISE-DAPT score has also been found to be an independent predictor of CI-AKI with an AUC of 0.834 [0.812 to 0.854] and PRECISE-DAPT score of ≥21 has been reported to have 81.3% sensitivity and 72.7% specificity in categorizing CIN.10 The Canada Acute Coronary Syndrome (C-ACS) score was compared with Mehran for its predictive value for discrimination CI-AKI and an AUC of 0.822 vs 0.751 was reported.11 The fragmented QRS complex (fQRS) on a 12-lead electrocardiography has been shown to have an AUC of 0.779 while it is 0.794 for the total number of fQRS ≥3 leads.12 In a study by Koowattanatianchai et al17 a reported three variable model comprising of ejection fraction <40%, presence of three vessel diseases, and use of intra-aortic balloon pump (IABP) reported an AUC of 0.83 [0.76 to 0.90] vs 0.78 [0.69 to 0.87] as compared to the Mehran score.
However, the parameter structure of the CHA2DS2-VASc score is simple and easier for physicians to memorize. The simplicity of the score makes it an attractive choice for the risk stratification of patients at a high risk of developing CI-AKI as compared to the score with a complex formulation or that requiring laboratory assessment and complex ECG interpretations. Pre-procedural clinical risk stratification with such simple tools warns the physician about the potential risk of CI-AKI so that they become over-conscious in intra and post-procedure handling and management of the patient. Additional research is warranted for the calibration of the parameter structures of the CHA2DS2-VASc score in the context of CI-AKI prediction.
To the best of our knowledge this is the first study on the evolution of the CHA2DS2-VASc score for the prediction of CI-AKI in the context of primary PCI. However, some limitations of the study include the single center coverage of the study with a relatively small sample size, along with the exclusion of patients with high risk features, such as preexisting CKD or cardiogenic shock, and CI-AKI was categorized only based on raised creatinine level from baseline and no imaging devices such as IVUS or OCT were used due to the limitation of time and resources. More accurate and direct measures of renal function such as proteinuria and kidney morphology would have improved the accuracy of prediction. Finally, due to the limited number of events in the sample the statistical associations can have low power and further large scale studies are warranted to establish various predictors of CI-AKI.
Conclusion
In conclusion, CHA2DS2-VASc score has good predictive value for discriminating patients at high risk of CI-AKI after primary PCI. The criteria of CHA2DS2-VASc ≥2 can be used for the risk stratification of CI-AKI after primary PCI. However, further studies are needed to assess the predictive value of CHA2DS2-VASc score against other reported risk assessment tools and markers such as the PRECISE-DAPT risk score, NT-proBNP, and fragmented QRS complexes.
Acknowledgments
The authors wish to acknowledge the support of the staff members of the Clinical Research Department of the National Institute of Cardiovascular Diseases (NICVD). Special acknowledgement to those who participated in data collection; Dr. Afzal Hussain, Dr. Vinesh Kumar, Dr. Shahzad Khatti and the rest.
Disclosure
The authors report no conflicts of interest in this work.
References
1. O’Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61(4):e78–e140. doi:10.1016/j.jacc.2012.11.019
2. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119–177. doi:10.1093/eurheartj/ehx393
3. Chacko L, Howard PJ, Rajkumar C, et al. Effects of percutaneous coronary intervention on death and myocardial infarction stratified by stable and unstable coronary artery disease: a meta-analysis of randomized controlled trials. Circ Cardiovasc Qual Out. 2020;13(2):e006363.
4. Silvain J, Nguyen LS, Spagnoli V, et al. Contrast-induced acute kidney injury and mortality in ST elevation myocardial infarction treated with primary percutaneous coronary intervention. Heart. 2018;104(9):767–772. doi:10.1136/heartjnl-2017-311975
5. Araujo GN, Junior FP, Fuhr B, et al. Simplifying contrast-induced acute kidney injury prediction after primary percutaneous coronary intervention: the age, creatinine and ejection fraction score. Cardiovasc Interv Ther. 2018;33(3):224–231. doi:10.1007/s12928-017-0472-y
6. Park SH, Jeong MH, Park IH, et al. Effects of combination therapy of statin and N-acetylcysteine for the prevention of contrast–induced nephropathy in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Int J Cardiol. 2016;212:100–106. doi:10.1016/j.ijcard.2016.03.009
7. Liu Y-H, Jiang L, Chen J-Y, Tan N, Liu Y, Cheng HP. Does N-terminal pro-brain natriuretic peptide add prognostic value to the Mehran risk score for contrast-induced nephropathy and long-term outcomes after primary percutaneous coronary intervention? Int Urol Nephrol. 2016;48(10):1675–1682. doi:10.1007/s11255-016-1348-2
8. Kaya A, Karataş A, Kaya Y, Düğeroğlu H, Dereli S, Bayramoğlu A. A new and simple risk predictor of contrast-induced nephropathy in patients undergoing primary percutaneous coronary intervention: TIMI risk index. Cardiol Res Pract. 2018;2018:5908215. doi:10.1155/2018/5908215
9. Jo S-H, Hahn J-Y, Lee SY, et al. High-dose atorvastatin for preventing contrast-induced nephropathy in primary percutaneous coronary intervention. J Cardiovasc Med. 2015;16(3):213–219. doi:10.2459/JCM.0000000000000157
10. Çınar T, Tanık VO, Aruğaslan E, et al. The association of PRECISE-DAPT score with development of contrast-induced nephropathy in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention. Cardiovasc Interv Ther. 2019;34(3):207–215. doi:10.1007/s12928-018-0545-6
11. Liu Y-H, Jiang L, Duan C-Y, et al. Canada Acute Coronary Syndrome Score: a preprocedural risk score for contrast-induced nephropathy after primary percutaneous coronary intervention. Angiology. 2017;68(9):782–789. doi:10.1177/0003319717690674
12. Kurtul A, Duran M. Fragmented QRS complex predicts contrast‐induced nephropathy and in‐hospital mortality after primary percutaneous coronary intervention in patients with ST‐segment elevation myocardial infarction. Clinic Cardiol. 2017;40(4):235–242. doi:10.1002/clc.22651
13. Liu Y-H, Liu Y, Zhou Y-L, et al. Comparison of different risk scores for predicting contrast induced nephropathy and outcomes after primary percutaneous coronary intervention in patients with ST elevation myocardial infarction. Am J Cardiol. 2016;117(12):1896–1903. doi:10.1016/j.amjcard.2016.03.033
14. Huang J, Yuan M, Ma J, et al. Protective effects of salvianolate on contrast-induced nephropathy after primary percutaneous coronary intervention: a prospective multicenter randomized controlled trial. Cardiology. 2017;138(3):169–178. doi:10.1159/000475746
15. Lin K-Y, Zheng W-P, Bei W-J, et al. A novel risk score model for prediction of contrast-induced nephropathy after emergent percutaneous coronary intervention. Int J Cardiol. 2017;230:402–412. doi:10.1016/j.ijcard.2016.12.095
16. Jurado-Román A, Hernández-Hernández F, García-Tejada J, et al. Role of hydration in contrast-induced nephropathy in patients who underwent primary percutaneous coronary intervention. Am J Cardiol. 2015;115(9):1174–1178. doi:10.1016/j.amjcard.2015.02.004
17. Koowattanatianchai S, Chantadansuwan T, Kaladee A, Phinyo P, Patumanond J. Practical risk stratification score for prediction of contrast-induced nephropathy after primary percutaneous coronary intervention in patients with acute ST-segment elevation myocardial infarction. Cardiol Res. 2019;10(6):350. doi:10.14740/cr939
18. Goussot S, Mousson C, Guenancia C, et al. N-terminal fragment of pro B-type natriuretic peptide as a marker of contrast-induced nephropathy after primary percutaneous coronary intervention for ST-segment elevation myocardial infarction. Am J Cardiol. 2015;116(6):865–871. doi:10.1016/j.amjcard.2015.06.007
19. Ozturk D, Celik O, Erturk M, et al. Utility of the logistic clinical syntax score in the prediction of contrast-induced nephropathy after primary percutaneous coronary intervention. Can J Cardiol. 2016;32(2):240–246. doi:10.1016/j.cjca.2015.05.005
20. Oksuz F, Yarlioglues M, Cay S, et al. Predictive value of gamma-glutamyl transferase levels for contrast-induced nephropathy in patients with ST-segment elevation myocardial infarction who underwent primary percutaneous coronary intervention. Am J Cardiol. 2015;116(5):711–716. doi:10.1016/j.amjcard.2015.05.042
21. Nakahashi H, Kosuge M, Sakamaki K, et al. Combined impact of chronic kidney disease and contrast-induced nephropathy on long-term outcomes in patients with ST-segment elevation acute myocardial infarction who undergo primary percutaneous coronary intervention. Heart Vessels. 2017;32(1):22–29. doi:10.1007/s00380-016-0836-8
22. Chaudhary AK, Pathak V, Kunal S, Shukla S, Pathak P. CHA2DS2-VASc score as a novel predictor for contrast-induced nephropathy after percutaneous coronary intervention in acute coronary syndrome. Indian Heart J. 2019;71(4):303–308. doi:10.1016/j.ihj.2019.09.005
23. Kurtul A, Yarlioglues M, Duran M. Predictive value of CHA2DS2-VASC score for contrast-induced nephropathy after percutaneous coronary intervention for acute coronary syndrome. Am J Cardiol. 2017;119(6):819–825. doi:10.1016/j.amjcard.2016.11.033
24. Tasai TT, Patel UD, Chang TI, et al. Validated contemporary risk model of acute kidney injury in patients undergoing percutaneous coronary interventions: insights from the national cardiovascular data registry cath-PCI registry. JACC Cardiovasc Interv. 2014;7(01):1–9. doi:10.1016/j.jcin.2013.06.016
25. Shoji S, Sawano M, Sandhu AT, et al. Evidence-to-practice gap for preventing procedure-related acute kidney injury in patients undergoing percutaneous coronary intervention. J Am Heart Assoc. 2021;10(15):e020047. doi:10.1161/JAHA.120.020047
26. Kumar R, Khan KA, Rai L, et al. Comparative analysis of four established risk scores for predicting contrast induced acute kidney injury after primary percutaneous coronary interventions. Int J Cardiol Heart Vasc. 2021;37:100905. doi:10.1016/j.ijcha.2021.100905
27. Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137(2):263–272. doi:10.1378/chest.09-1584
28. Mehran R, Aymong ED, Nikolsky E, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. 2004;44:1393–1399. doi:10.1016/j.jacc.2004.06.068
29. Mehran R, Nikolsky E. Contrast-induced nephropathy: definition, epidemiology, and patients at risk. Kidney Int. 2006;69:S11–5. doi:10.1038/sj.ki.5000368
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.