")
Back to Journals » OncoTargets and Therapy » Volume 15
Cetuximab and Dabrafenib Plus Trametinib for Untreated Colonic Metastasis of BRAFV600E Mutant Primary Lung Adenocarcinoma with Signet Ring Cell Features: An Interesting and Rare Case Report
Authors Jiang S, Wu Y, Wei W, Wang Z, Wang Q
Received 19 May 2022
Accepted for publication 20 September 2022
Published 26 September 2022 Volume 2022:15 Pages 1057—1062
DOI https://doi.org/10.2147/OTT.S375436
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr William C. Cho
Shujun Jiang,1 Yanran Wu,1 Wenjie Wei,2 Zi Wang,3 Qi Wang1
1Department of Integrated Traditional Chinese and Western Medicine, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2Department of Oncology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 3Department of Radiology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
Correspondence: Qi Wang, Department of Integrative Traditional Chinese and Western Medicine Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, People’s Republic of China, Tel +86-18627822851, Fax +86-27-83663532, Email [email protected]
Abstract: Colonic metastases of lung adenocarcinoma are extremely rare. Signet ring cell adenocarcinoma (SRCA) has not been described in patients with gastrointestinal metastasis of lung adenocarcinoma. SRCA is a unique subtype of adenocarcinoma with strong invasion and a poor prognosis, and most SRCA found in the lung are due to gastrointestinal metastases. This report describes a rare case of colonic metastasis from primary lung SRCA. A 64-year-old female was admitted to Sun Yat-sen University Cancer Center for feeling of nausea and malaise. Following a positron emission tomography CT (PET-CT) scan, widespread metastases of tumor cells were found in the bilateral lung, liver, bone, and multiple lymph nodes, but there was no evidence of metastasis to the colon. Two months later, the patient received a liver biopsy at Tongji Hospital in Wuhan. Pathology revealed a poorly differentiated adenocarcinoma with SRCA conformation, but immunohistochemical staining did not identify the original source of tumor cells. Considering that SRCA mainly derives from the gastrointestinal tract and that serum gastrointestinal tumor markers were elevated, we performed gastrointestinal endoscopy on the patient. The results showed an isolated polyp in the colon, and the pathology results indicated a poorly differentiated adenocarcinoma that was considered to originate from the lung based on immunohistochemical staining. Meanwhile, genetic tests identified a BRAF V600E mutation. The final diagnosis was colonic metastasis of BRAFV 600E mutated lung SRCA. Considering the positive expression of EGFR in this case, cetuximab was innovatively added to the first-line treatment regime (dabrafenib and trametinib). To date, the patient has received thirty-two weeks of treatment. Interestingly, lung and liver tumors shrank and tumor markers in the blood normalized. Our findings offer valuable diagnostic and therapeutic information for colonic metastasis of BRAFV600E mutant primary lung adenocarcinoma with signet ring cell features.
Keywords: colonic metastasis, lung adenocarcinoma, signet ring cell adenocarcinoma, case report, BRAF V600E mutant
Introduction
Lung cancer is the most common tumor malignancy with high mortality in the world.1 Distant metastases from primary lung cancer usually occur in the bone, brain, liver and adrenal glands, while the gastrointestinal tract is a very rare site of metastases.2 To our knowledge, there have been no case reports describing signet ring cell adenocarcinoma (SRCA) in gastrointestinal metastases of lung cancer. SRCA is a specific type of mucin-secreting adenocarcinoma characterized by abundant intracytoplasmic mucins that push the nucleus to one side of the cell. SRCA originates from undifferentiated stem cells from the mucosal lamina propria. Once SRCA infiltrates beyond the submucosa, the signet ring cells will spread widely and form distant metastases, suggesting high aggressiveness and poor prognosis.3 Primary SRCA usually originates from the gastrointestinal tract, and most SRCAs observed within the lung are metastatic carcinomas from the gastrointestinal tract.4,5 Primary lung SRCA is extremely rare6,7 and therefore the SRCA found in the lung can easily be mistaken for a metastasis from the gastrointestinal tract. Histopathology and immunohistochemistry will help to make a definite diagnosis. This report describes an interesting case of a SRCA in a patient with colonic metastasis of primary lung adenocarcinoma, a type of non-small cell lung cancer (NSCLC). NSCLC accounts for more than 80% of all lung cancers. Unfortunately, few patients with NSCLC are eligible for radical treatment. Since most patients have advanced disease at the time of diagnosis, chemotherapy is the main therapeutic strategy, which has achieved an effective plateau in improving the survival of patients with NSCLC, although treatment outcomes are still considered disappointing.8 NSCLC treatment has changed significantly with the discovery of specific drug targets. BRAF-mutated NSCLC is considered a rare form of lung cancer. The most common BRAF mutation, V600E, is observed in 1–2% of lung adenocarcinomas.9 Clinical trial data has confirmed that BRAF/MEK inhibition is an effective therapy in BRAFV600E-mutated NSCLC.10,11 In 2017, the United States Food and Drug Administration approved the combination of BRAF inhibitor (darafenib) and MEK inhibitor (trametinib) for the treatment of NSCLC with BRAF V600E mutation.12 BRAF serine/threonine protein kinase is a downstream signaling protein in the epidermal growth factor receptor (EGFR)-activated mitogen-activated protein kinase (MAPK) pathway. BRAF V600E inhibition leads to rapid negative feedback activation of EGFR, which promotes tumor proliferation. The addition of EGFR inhibition to BRAF inhibitors can suppress MAPK reactivation and increases antitumor activity.13,14 In this case, immunohistochemistry showed positive expression of EGFR, so we attempted adding cetuximab to first-line therapy (dabrafenib and trametinib) for lung adenocarcinoma with BRAFV600E mutant.
Case Report
A 64-year-old woman was admitted to the Sun Yat-sen University Cancer Center with complaints of nausea and malaise. The serum tumor markers test showed that levels of carbohydrate antigen (CA-199) and carcinoembryonic antigen (CEA) were significantly elevated. After a positron emission tomography CT (PET-CT) scan, tumor cells were found to have widely metastasized to the bilateral lungs, liver, bone, and multiple lymph nodes, but there was no evidence of metastasis to the colon. There were multiple low-density shadows in the liver (standard uptake value (SUV) 16.5) with a maximum of 5.5×10.1 cm (Figure 1A) and multiple pulmonary nodules (SUV 7.3) with a maximum of 1.8×2.0 cm (Figure 2A) on PET-CT scan. Taking into account the short survival and the poor prognosis, the patient asked to abandon treatment, but the family requested additional therapy. Two months later, the patient received a liver biopsy at Tongji Hospital in Wuhan. Pathology showed a poorly differentiated adenocarcinoma with a signet ring cell carcinomatous conformation (Figure 3A), but immunohistochemical staining did not identify the original source of tumor cells. Considering that SRCA derives primarily from the gastrointestinal tract and that gastrointestinal tumor markers were elevated in the blood, we performed a gastrointestinal endoscopy. Gastroscopy revealed the absence of nodules and masses in the stomach. Colonoscopy revealed an isolated polyp in the colon (0.4 x 0.3cm) and two polyps in the rectum (0.6 x 0.7cm, 0.5×0.5cm). The result of the histopathological examination of the colonic polyp demonstrated poorly differentiated adenocarcinoma (Figure 3B). To further identify the source of the malignancy, immunohistochemical staining was used to detect typical immunohistochemical markers of lung and colorectal cancer. The result showed positive expression of cytokeratin 7 (CK7), thyroid transcription factor-1 (TTF1), and NapsinA, but negative expressions of cytokeratin 20 (CK20) and caudal-type homeobox 2 (CDX2), which supported metastatic adenocarcinoma of pulmonary origin, rather than a primary colonic adenocarcinoma.
 |
Figure 1 Liver computed tomography images. (A) PET-CT scan revealed that the largest liver mass was 5.5×10.1 cm before treatment. (B) CT reexamination showed that the largest liver mass was shrunken to 5.9×3.0 cm after 8 weeks of treatment. (C) CT reexamination showed that the largest liver mass was shrunken to 4.5×1.8 cm after 16 weeks of treatment. (D) CT reexamination showed that the largest liver mass had been stable at 4.5×1.8 cm after 24 weeks of treatment. (E) CT reexamination showed that the largest liver mass was shrunken to 1.8×1.8 cm after 32 weeks of treatment. |
 |
Figure 2 Chest computed tomography images. (A) PET-CT scan revealed that the largest pulmonary nodule was 1.8×2.0 cm before treatment. (B) CT reexamination showed that the largest pulmonary nodule had shrunken to 1.0×0.8 cm after 8 weeks of treatment. (C–E) CT reexamination showed that the largest pulmonary nodule had been stable at 1.0×0.8 cm after 16, 24 and 32 weeks of treatment. |
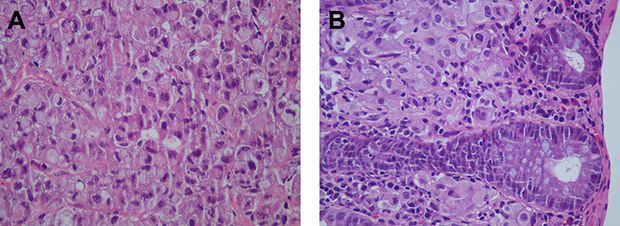 |
Figure 3 Hematoxylin and eosin staining. (A) low differentiated adenocarcinoma with signet ring cell carcinomatous conformation in the biopsy specimen of liver. (B) poorly differentiated adenocarcinoma in the biopsy specimen of colonic polyp. |
The therapeutic outcome of chemotherapy is relatively poor for advanced lung adenocarcinoma, and the patient refused chemotherapy. We advised her to undergo genetic testing, and eventually a BRAF V600E mutation was identified. Considering that advanced primary lung adenocarcinoma with the BRAFV600E mutant is highly malignant and had a poor prognosis, we chose targeted therapy (dabrafenib and trametinib). In this case, we found that EGFR expression was positive in the patient. To further improve efficacy, we conducted a literature review to identify the treatment strategy. Finally, a combination treatment with cetuximab (500 mg/m2 every two weeks) and dabrafenib (150 mg bid) plus trametinib (2 mg qd) was administered with the consent of the patient on 26 September 2021. There were no uncomfortable symptoms during treatment. After two months of treatment, follow-up CT reexamination showed that the largest lung mass had shrunken to 1.0×0.8 cm (Figure 2B) and the largest liver mass was significantly reduced to 5.9×3.0 cm (Figure 1B). Levels of the serum tumor marker CEA decreased significantly and CA199 decreased to the normal range. Subsequently, the dose of cetuximab was reduced to 250 mg/m2 because the patient developed a systemic rash. The treatment was fully tolerated by the patient, with no adverse reactions and no uncomfortable symptoms.
The patient underwent 32 weeks of treatment before this report was submitted for publication. Follow-up CT re-examination demonstrated no significant changes in lung mass since the last review (Figure 2C–E). Abdominal CT scan showed that the largest liver mass had shrunk to 4.5×1.8 cm at 16 and 24 weeks of treatment (Figure 1C–D) and 1.8×1.8 cm at 32 weeks of treatment (Figure 1E). The patient achieved a partial response. The serum tumor marker CEA and CA199 decreased to the normal levels. The disease has remained stable at the time of submission of this manuscript.
Discussion
Lung cancer is the leading cause of cancer death around the world, with an estimated 1.6 million deaths each year.15 NSCLC accounts for approximately 85% of cases, of which lung adenocarcinoma (LUAD) is the most common subtype.16 Most patients with LUAD are in an advanced stage at diagnosis and their 5-year survival rate is less than 5%.17 The most common metastatic site of NSCLC is the bone (34%), followed by the lungs (32%), brain (28%), adrenal glands (17%), liver (13%), and lymph nodes (9%),18 colonic metastasis is very rare. The incidence of gastrointestinal metastases of lung cancer was <2% in a previous clinical study, while the incidence of colon metastases was approximately 12% according to autopsy studies. The clinical incidence of gastrointestinal metastasis is lower than that reported by autopsy data, probably because gastrointestinal metastasis is usually asymptomatic.19,20 In our case, the patient did not experience any gastrointestinal symptoms and gastrointestinal metastasis could easily be missed. Therefore, gastrointestinal endoscopy and polyp biopsy are necessary to determine whether there is hidden gastrointestinal metastasis in patients with lung cancer.
There was an interesting finding in our case report. After a liver biopsy, histopathology revealed a poorly differentiated adenocarcinoma with SRCA conformation, although immunohistochemistry could not determine the specific source. Most SRCA found in the lung originates from the gastrointestinal tract. Sangang et al found that only 3.1% of SRCA originated in the lungs and the vast majority derived from the gastrointestinal tract.4 Based on previous findings and the elevated serum gastrointestinal tumor markers (CA-199 and CEA), the tumor could easily have been mistaken for a metastasis from colonic origin in our case. To further distinguish whether the tumor originated from the lung or colon, immunohistochemical staining for specific markers were performed. In our case, TTF1, CK7, and NapsinA, markers of primary adenocarcinoma of the lung, were positive, while CK20, CDX2, markers of primary gastrointestinal tract tumor, were negative,21 therefore the tumor was determined to be colonic metastasis of the primer lung SRCA. Platinum-based chemotherapy is traditionally used to treat advanced NSCLC, but relapse rates are high with significant toxicity.
To select a better treatment approach, genetic testing was performed in our case. The results revealed that the patient was positive for a BRAF V600E mutation. The BRAF gene is an oncogene that is a critical component of the RAS-RAF-MEK-ERK signaling axis that regulates cell growth and division. Once the signaling reaches the next point in the cascade, BRAF kinase is inactivated through negative feedback in healthy tissue. BRAF mutations act as oncogenic drivers that lead to continuous activation of downstream cell signals, which promote cell growth and proliferation.22 The V600E mutation is the most common BRAF point mutation of is independently associated with a poor prognosis. Patients with BRAF V600E mutations achieve lower responses to platinum-based chemotherapy compared to patients with non-V600E mutations.23 BRAF V600E is a valuable target for drug therapy with BRAF inhibitors. Resistance to the BRAF inhibitor eventually emerges due to MAPK pathway reactivation.24
The addition of downstream MEK inhibitor to block ERK signaling, and thus interferes with the MAPK pathway to the maximum extent, allows to delay the emergence of resistance mechanisms. The combination of the BRAF V600E specific inhibitor dabrafenib and the MEK inhibitor trametinib was approved for the treatment of BRAF V600E-mutated lung cancer by the FDA in 2017.12 The epidermal growth factor receptor (EGFR) is a molecular target for inhibition in NSCLC. Between 57% and 88% of primary NSCLC is found to express or overexpress EGFR.25 Some studies have shown that inhibition of BRAF (V600E) leads to rapid feedback activation of EGFR, which supports continued proliferation in the presence of BRAF V600E inhibition. Strong synergism was observed when BRAF inhibition was associated with EGFR inhibition in colon cancer with the BRAF V600E mutation, suggesting increased antitumor activity and efficacy.13 As EGFR expression was found to be positive in this case, we innovatively added the EGFR-targeted drug cetuximab to the first-line therapy (dabrafenib and trametinib) in order to improve the therapeutic effect. After 32 weeks of treatment, the lung and liver masses shrank significantly, serum tumor markers dropped to normal, and routine blood counts, coagulation activity, and liver and kidney function remained normal. There were no obvious adverse reactions and uncomfortable symptoms. The disease remained stable as submission of the manuscript.
Conclusions
We report the first case of colonic metastasis of BRAF V600E mutated lung adenocarcinoma with signet ring cell features. Similar cases are prone to misdiagnosis and missed diagnosis, thus, gastroenteroscopy should be performed even in the absence of gastrointestinal symptoms to detect occult gastrointestinal metastases and histopathology and immunohistochemistry should be performed to make a clear diagnosis. Similarly, cetuximab was first used in combination with dabrafenib and trametinib in the treatment of advanced BRAF V600E mutant lung adenocarcinoma. The patient will continue to be observed for follow-up treatment efficacy. Whether the new treatment regimen can truly offer clinical benefit needs to be further explored in prospective studies with a large sample size.
Ethics Statements
The Affiliated Tongji Hospital of Huazhong University of Science and Technology approved publishing the case details.
Consent for Publication
The patient’s informed consent was obtained for the publication of this case details and images.
Acknowledgments
This work was funded by the National Natural Science Foundation of China (No. 81703886) and Hubei Provincial Science and Technology Project (No. ZY2019M040).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Mao Y, Yang D, He J, et al. Epidemiology of lung cancer. Surg Oncol Clin N Am. 2016;25(3):439–445. doi:10.1016/j.soc.2016.02.001
2. Yoshimoto A, Kasahara K, Kawashima A. Gastrointestinal metastases from primary lung cancer. Eur J Cancer. 2006;42(18):3157–3160. doi:10.1016/j.ejca.2006.08.030
3. Yamashina M. A variant of early gastric carcinoma. Histologic and histochemical studies of early signet ring cell carcinomas discovered beneath preserved surface epithelium. Cancer. 1986;58(6):1333–1339. doi:10.1002/1097-0142(19860915)58:6<1333::AID-CNCR2820580625>3.0.CO;2-B
4. Wu SG, Chen XT, Zhang WW, et al. Survival in signet ring cell carcinoma varies based on primary tumor location: a surveillance, epidemiology, and end results database analysis. Expert Rev Gastroenterol Hepatol. 2018;12(2):209–214. doi:10.1080/17474124.2018.1416291
5. Cai Y, Xie Y, Xiong Y, et al. Clinicopathological characteristics and survival in lung signet ring cell carcinoma: a population-based study. Bosnian J Basic Med Sci. 2021;21(6):752–759. doi:10.17305/bjbms.2020.5454
6. Livieratos S, Smith JK, Fatakhov E, et al. Primary signet ring cell carcinoma of the lung: a rare subtype. BMJ Case Rep. 2013;2013(sep20 1):bcr2013200111–bcr2013200111. doi:10.1136/bcr-2013-200111
7. Yang M, Yang Y, Chen J, et al. A case report of primary signet ring cell carcinoma of the lung: imaging study and literature review. Transl Lung Cancer Res. 2021;10(9):3840–3849. doi:10.21037/tlcr-21-654
8. Pfister DG, Johnson DH, Azzoli CG, et al. American Society of Clinical Oncology treatment of unresectable non-small-cell lung cancer guideline: update 2003. J Clin Oncol. 2004;22(2):330–353. doi:10.1200/JCO.2004.09.053
9. Barlesi F, Mazieres J, Merlio J-P, et al. Routine molecular profiling of patients with advanced non-small-cell lung cancer: results of a 1-year nationwide programme of the French Cooperative Thoracic Intergroup (IFCT). Lancet. 2016;387(10026):1415–1426. doi:10.1016/S0140-6736(16)00004-0
10. Dudnik E, Bar J, Peled N, et al. Efficacy and safety of BRAF inhibitors with or without MEK inhibitors in BRAF-mutant advanced non-small-cell lung cancer: findings from a real-life cohort. Clin Lung Cancer. 2019;20(4):278–286 e271. doi:10.1016/j.cllc.2019.03.007
11. Planchard D, Smit EF, Groen HJM, et al. Dabrafenib plus trametinib in patients with previously untreated BRAFV600E-mutant metastatic non-small-cell lung cancer: an open-label, Phase 2 trial. Lancet Oncol. 2017;18(10):1307–1316. doi:10.1016/S1470-2045(17)30679-4
12. Odogwu L, Mathieu L, Blumenthal G, et al. FDA approval summary: dabrafenib and trametinib for the treatment of metastatic non-small cell lung cancers harboring BRAF V600E mutations. Oncologist. 2018;23(6):740–745. doi:10.1634/theoncologist.2017-0642
13. Prahallad A, Sun C, Huang S, et al. Unresponsiveness of colon cancer to BRAF(V600E) inhibition through feedback activation of EGFR. Nature. 2012;483(7387):100–103. doi:10.1038/nature10868
14. Corcoran RB, Ebi H, Turke AB, et al. EGFR-mediated re-activation of MAPK signaling contributes to insensitivity of BRAF mutant colorectal cancers to RAF inhibition with vemurafenib. Cancer Discov. 2012;2(3):227–235. doi:10.1158/2159-8290.CD-11-0341
15. Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. doi:10.3322/caac.21262
16. Molina JR, Yang P, Cassivi SD, et al. Non–small cell lung cancer: epidemiology, risk factors, treatment, and survivorship. Mayo Clin Proc. 2008;83(5):584–594. doi:10.1016/S0025-6196(11)60735-0
17. Miller KD, Nogueira L, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2019. CA Cancer J Clin. 2019;69(5):363–385. doi:10.3322/caac.21565
18. Hillers TK, Sauve MD, Guyatt GH. Analysis of published studies on the detection of extrathoracic metastases in patients presumed to have operable non-small cell lung cancer. Thorax. 1994;49(1):14–19. doi:10.1136/thx.49.1.14
19. Hu Y, Feit N, Huang Y, et al. Gastrointestinal metastasis of primary lung cancer: an analysis of 366 cases. Oncol Lett. 2018;15(6):9766–9776. doi:10.3892/ol.2018.8575
20. Taira N, Kawabata T, Gabe A, et al. Analysis of gastrointestinal metastasis of primary lung cancer: clinical characteristics and prognosis. Oncol Lett. 2017;14(2):2399–2404. doi:10.3892/ol.2017.6382
21. Alabdullah B, Hadji-Ashrafy A. Identification of the most specific markers to differentiate primary pulmonary carcinoma from metastatic gastrointestinal carcinoma to the lung. Diagn Pathol. 2022;17(1):7. doi:10.1186/s13000-021-01184-2
22. Amaral T, Sinnberg T, Meier F, et al. The mitogen-activated protein kinase pathway in melanoma part I - Activation and primary resistance mechanisms to BRAF inhibition. Eur J Cancer. 2017;73:85–92. doi:10.1016/j.ejca.2016.12.010
23. Marchetti A, Felicioni L, Malatesta S, et al. Clinical features and outcome of patients with non-small-cell lung cancer harboring BRAF mutations. J Clin Oncol. 2011;29(26):3574–3579. doi:10.1200/JCO.2011.35.9638
24. Chan XY, Singh A, Osman N, et al. Role played by signalling pathways in overcoming BRAF inhibitor resistance in melanoma. Int J Mol Sci. 2017;18(7):1527. doi:10.3390/ijms18071527
25. Pirker R, Pereira JR, Szczesna A, et al. Cetuximab plus chemotherapy in patients with advanced non-small-cell lung cancer (FLEX): an open-label randomised Phase III trial. Lancet. 2009;373(9674):1525–1531. doi:10.1016/S0140-6736(09)60569-9
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.