")
Back to Journals » Infection and Drug Resistance » Volume 13
Ceftobiprole for Treatment of MRSA Blood Stream Infection: A Case Series
Authors Mahmoud E , Al Mansour S, Bosaeed M , Alharbi A, Alsaedy A, Aljohani S , Alalwan B , Alothman A
Received 18 March 2020
Accepted for publication 16 July 2020
Published 3 August 2020 Volume 2020:13 Pages 2667—2672
DOI https://doi.org/10.2147/IDR.S254395
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Ebrahim Mahmoud,1 Sarah Al Mansour,1 Mohammad Bosaeed,1– 3 Ahmad Alharbi,1 Abdulrahman Alsaedy,1,2 Sameera Aljohani,2,4 Bassam Alalwan,4 Adel Alothman1,2, †
1Division of Infectious Diseases, Department of Medicine, King Abdulaziz Medical City - Riyadh, Riyadh, Saudi Arabia; 2College of Medicine, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 3King Abdullah International Medical Research Center (KAIMRC), Riyadh, Saudi Arabia; 4Department of Pathology & Laboratory Medicine, King Abdulaziz Medical City - Riyadh, Riyadh, Saudi Arabia
†Doctor Adel Al Othman passed away on June 8, 2020
Correspondence: Ebrahim Mahmoud
Division of Infectious Diseases, Department of Medicine, King Abdulaziz Medical City - Riyadh, P.O. Box 22490, Riyadh 11426, Saudi Arabia
Tel +966 500081418
Email [email protected]
Abstract: While methicillin-resistant Staphylococcus aureus (MRSA) bacteremia has poor outcomes, we describe our experience with Ceftobiprole mainly as a combination therapy for the treatment of MRSA bacteremia. All the cases of MRSA bacteremia in our center at the King Abdulaziz Medical City (KAMC), Riyadh, that had undergone Ceftobiprole treatment were included. We had six cases of MRSA bacteremia between 2018 and 2019, secondary to different infectious syndromes including endocarditis. There was a severe infection that required intensive care unit (ICU) admission in four cases. Ceftobiprole is used in combination with vancomycin in four cases. On day 14, all cases had a favorable outcome with microbiological and clinical improvement. However, three patients died after months of suffering from bacteremia from unrelated causes for the infection. The clinical outcome in our series of treatment of MRSA bacteremia using Ceftobiprole was favorable. Further studies for the evaluation of the use of Ceftobiprole in MRSA bacteremia should be encouraged.
Keywords: methicillin-resistant Staphylococcus aureus, bacteremia, Ceftobiprole, treatment
Introduction
Ceftobiprole is a relatively novel fifth-generation cephalosporin with in vitro activity against both Gram-positive and Gram-negative bacteria, including methicillin-resistant Staphylococcus aureus (MRSA).1,2 Since its approval for the treatment of adult community-acquired pneumonia (CAP) and hospital-acquired pneumonia (HAP) in Europe,1 more reports have emerged about using Ceftobiprole for different indications, including infective endocarditis.3 Furthermore, an ongoing phase three trial compares it to daptomycin for the treatment of MRSA bacteremia.4
MRSA bacteremia has been shown to result in significant morbidity and mortality, with an estimated 30-day all-cause mortality rate of 20%.5 While MRSA epidemiology in the Middle East is variable, the overall estimation of the prevalence of MRSA in Saudi Arabia (KSA) was 35.6% from a pooled estimation of 22,793 S. aureus strains from 2002 to 2012.6 Thus, MRSA is a relatively common infection in regions including the Middle East, with limited treatment options. In this article, we are reporting our experience in using Ceftobiprole as an alternative option for MRSA bacteremia treatment.
Patients and Methods
We included patients who received Ceftobiprole for more than 72 hours and have MRSA bacteremia. From January 2017 to December 2019, there was a total of six patients in our case series. The clinical and demographic data of eligible patients were obtained from electronic medical records using our local health information system (Best Care). Methicillin-resistant Staphylococcus aureus clinical isolates and their susceptibility results were identified using the routine microbiological methods applied in the microbiology laboratories using the automated machine VITEK 2. We evaluated clinical success based on microbiological clearance (whenever repeated cultures were available), clinical resolution of signs and symptoms of infection, and 30-day in-hospital survival after initiation of Ceftobiprole treatment. The study was approved by the Institutional Review Board (IRB) in King Abdullah International Medical Research Center (KAIMRC) (Protocol number RC20/152/R).
Results
The six patients’ descriptions are listed in Table 1. All the cases were male with a mean age of 52 years. The mean duration of treatment using Ceftobiprole was 31 days. In two cases, Ceftobiprole was used as the initial combination therapy, while in others, it was used as the salvage therapy. Most patients had comorbidities, but there were no intravenous drug users among them. Four out of the six patients required ICU admission. There were two cases of bacteremia related to osteomyelitis, one case related to endocarditis, one central line-associated bacteremia (CLABSI) case, one skin and soft tissue infection (SSTI) secondary to a burn, and one case of pneumonia. The MIC for vancomycin was one or less, except in one case, while susceptibility for Ceftobiprole was tested in two cases and was sensitive in both (the minimum inhibitory concentration (MIC) was less than 2).
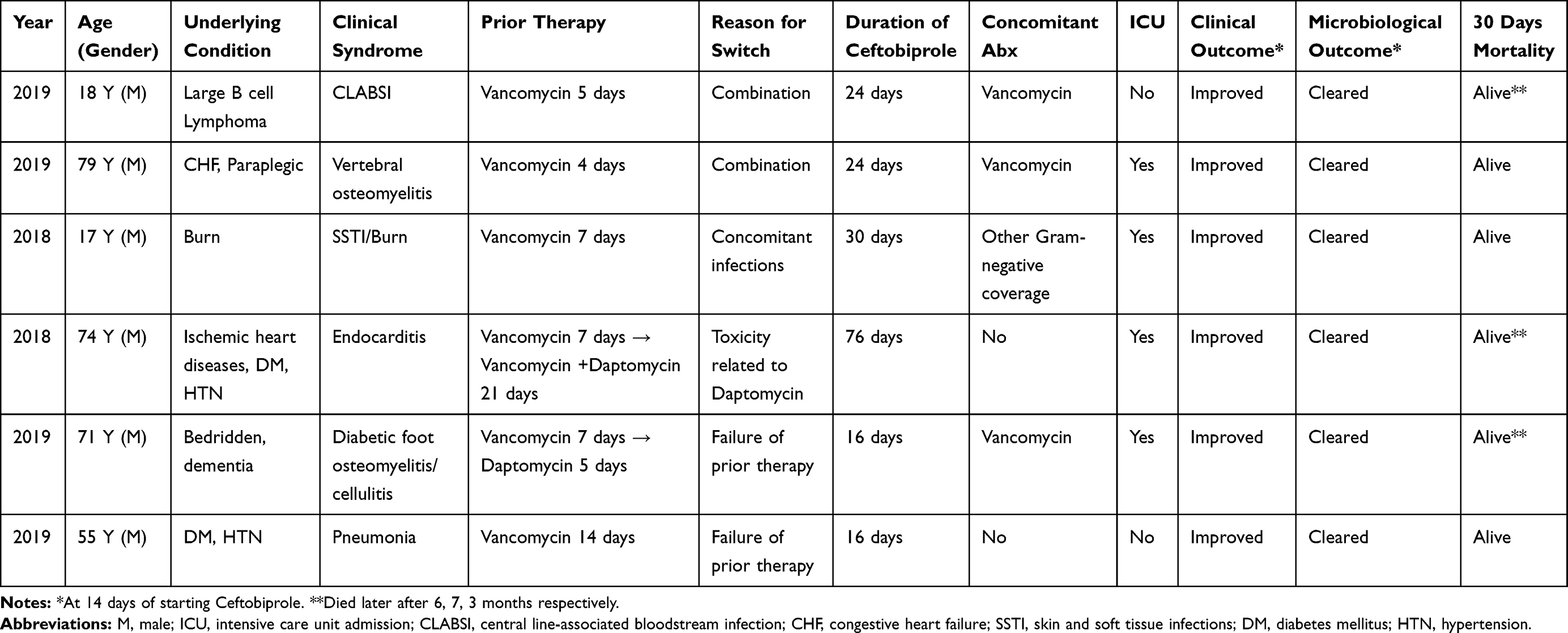 |
Table 1 Descriptions of the Cases |
Vancomycin was used in all the cases, whether concomitantly with ceftobiprole or prior to its use. Ceftobiprole used in combination with vancomycin in four cases and there were no reported side effects of the drug or safety concerns.
The following section contains summaries of all the cases.
Case 1
An 18-year-old male was diagnosed with large B cell lymphoma. He was evaluated by infectious disease specialists for febrile neutropenia, after receiving the fifth cycle of chemotherapy. He was started on vancomycin on the first day of fever in addition to meropenem (for Gram-negative coverage). Blood culture grew MRSA (vancomycin MIC < 0.5) on the second day of fever and persisted for three days, which was judged to be related to CLABSI and exit site infection. The central line was removed on the same day of obtaining the culture result. Although the bacteremia cleared, the fever persisted and the patient was still neutropenic. Therefore, Ceftobiprole was combined with vancomycin on the fifth day of fever and both drugs were continued for 21 days. In the same neutropenic episode, his chest CT scan showed multiple lung lesions that were likely invasive pulmonary aspergillosis (IPA). Amphotericin B liposomal was started and the repeated radiological exam after two weeks showed complete resolution. Importantly, the transesophageal echocardiography (TEE) was negative for endocarditis. Clinically, the fever defervesced after four days of adding Ceftobiprole and on day 14, the patient was well with no signs or symptoms of infection.
Case 2
The patient was a 79-year-old male with comorbidities of diabetes, heart failure, and paraplegia after road traffic accidents. He was brought to the emergency room (ER) because of fever and back pain. Blood culture grew MRSA (vancomycin MIC 1) and a spinal MRI scan showed spondylodiscitis of L3–4 and early osteomyelitis with abscess of dimensions 4.6 x 4.1 x 2 cm. He was initially started on vancomycin and Ceftobiprole was added after four days. Bacteremia cleared on day three of admission. No surgical intervention was done for the patient as attempting abscess aspiration under interventional radiology failed.
The patient had good clinical outcomes and further, radiological imaging after four weeks showed near resolution of the collection and improvement in the finding of spondylodiscitis. Although Ceftobiprole was continued for 24 days, vancomycin administration was stopped after five weeks due to worsening renal function. It was replaced by doxycycline for four more weeks. He was discharged after two months of admission in a stable clinical condition.
Case 3
A 17-year-old male, medically free, was transferred from another hospital as a case of second-degree flame burns (70–80%) with mixed deep and partial thickness that had occurred two months prior. Upon initial assessment, the patient was febrile. Blood culture from the central venous catheter grew methicillin-resistant Staphylococcus aureus (vancomycin MIC 1), Klebsiella pneumonia, and Pseudomonas aeruginosa. Blood culture remained positive for MRSA for a further four days and MRSA also grew from the infected burn tissue cultures, but not from respiratory samples. Empirically, he was on vancomycin for seven days. Subsequently, the treatment with Ceftobiprole with other Gram-negative coverage was started. The patient stayed in the hospital for around four months as he had a complicated course with multiple infections, including pneumonia and skin soft tissue infections. Multiple debridements along with skin grafts for bilateral upper and lower limbs and anterior and posterior trunks were done as source control. Ceftobiprole was continued for a total of 30 days with evidence of microbiological resolution of MRSA. At the time of discharge, his wounds had healed very well, and he was discharged in good condition.
Case 4
A 74-year-old man who was known to have multiple comorbidities including ischemic heart diseases, uncontrolled diabetes mellitus and end-stage renal disease was admitted. He presented to the emergency department complaining of chills and rigors. Several blood cultures grew MRSA (vancomycin MIC 0.75) and a diagnosis of infective endocarditis was made based on the echocardiography findings that showed large vegetation in the mitral valve.
He was initially started on vancomycin monotherapy for a week. Although repeated blood cultures were all negative, daptomycin was added to vancomycin on day seven. The patient underwent mitral valve excision, radical debridement, and mitral valve tissue repair in the fourth week of his admission. A few days after surgery, the patient had QT interval prolongation that was attributed to daptomycin and a decision was made to stop the current regimen and start Ceftobiprole as monotherapy. The administration of Ceftobiprole was continued for 76 days. His course following the surgery was complicated with hospital-acquired infections, including hospital acquired pneumonia. Nevertheless, subsequent echocardiogram, including Transesophageal echocardiography (TEE), was negative for endocarditis and no positive microbiological culture was noted for MRSA.
Case 5
A 71-year-old male patient with diabetes, hypertension, Chronic obstructive pulmonary disease (COPD), post right above-knee amputation, and vascular dementia was admitted. He presented to the hospital with fever and SOB for three days. His blood culture grew MRSA (vancomycin MIC 1.5) that was secondary to cellulitis and osteomyelitis. A left foot MRI scan confirmed osteomyelitis that involved the forefoot and distal end of tibia and fibula with multiple pockets of fluid collection. Empirically, upon admission, vancomycin and meropenem were started. However, because of the persistence of positive blood culture with MRSA on day seven, vancomycin was replaced with daptomycin. There was no source control achieved for the patient as the aspiration of the collection failed. On day 12 of admission, his blood culture remained positive after five days of being on daptomycin. Therefore, Ceftobiprole was started in combination with vancomycin. Blood culture sterilized after two days on the new combination. To rule out the possibility of endocarditis, TEE was conducted that was negative. There was a good clinical response to the combination of Ceftobiprole and vancomycin that was continued for 16 days. Further, vancomycin was continued by itself for a total of six weeks, with a good clinical outcome.
Case 6
A 55-year-old male patient, known to have diabetes, hypertension, and depression presented to the hospital with abdominal pain and vomiting. The blood culture grew MRSA (vancomycin MIC 0.38), with chest X-ray findings compatible with pneumonia. Empirically, the patient was started on piperacillin-tazobactam and vancomycin.
Although the repeated blood culture on the third day of admission was negative, he continued to be febrile till day 10. The chest computerized tomography (CT) scan was repeated on day 14 and showed interval development of cavitary lesion in the upper right lobe. Based on the failure of vancomycin with the progression of the disease, the drug was changed to Ceftobiprole.
He received Ceftobiprole for 16 days with a good clinical response and the next chest CT scan showed resolution of the cavitary lesion two weeks from starting Ceftobiprole. He was discharged following a chest CT scan after one day in a stable condition to continue on oral doxycycline for one week.
Discussion
MRSA infections represent a common medical challenge with serious complications and higher mortality compared to other bacterial infections. In 2017, the United States reported an estimated 120,000 cases of Staphylococcus aureus bacteremia resulting in 20,000 deaths.7 In this study, we present our experience with Ceftobiprole for MRSA bacteremia with various infectious syndromes. In our cohort, all the cases had a favorable 14-day outcome, both microbiological and clinical. Three patients died after a few months due to different reasons, unrelated to the MRSA infection.
Different antibiotics were used in our series. However, vancomycin was used in all the cases initially (congruent with the guideline recommendations as the standard of care therapy), but some changes were made later due to clinical or microbiological reasons. Although there is no specific recommendation for combination therapy in the guideline,8 several trials attempted to answer the question of whether combination therapy would improve MRSA bacteremia’s outcome. The recent CAMERA2 trial that included 352 patients failed to prove the superiority of the combination of standard of care with antistaphylococcal β-lactam (flucloxacillin, cloxacillin, or cefazolin) and the trial was stopped early because of side effects in the combination arm.9 However, there is still ample evidence that beta-lactam combination therapy is synergistic in killing S. aureus,10–12 including the results of a randomized clinical trial for the treatment of bacteremia.13 Thus, it is worth exploring these possibilities in greater detail, especially in cases that are difficult to treat.
Concerning Ceftobiprole, studies in animal models have demonstrated the potency of Ceftobiprole and its superiority to vancomycin, daptomycin, and linezolid against infective endocarditis caused by S. aureus.14 Therefore, the result of the ongoing phase three trial for ceftobiprole for MRSA bacteremia will add to our knowledge regarding the efficacy of this treatment option.4
Interestingly, our series included a patient with febrile neutropenia who had a good response in a short period, although the failure rate of MRSA bacteremia in patients with cancer was reported to be as high as 52%.15 Further, the positive response in the endocarditis case is in line with the good outcome reported in Tascini et al study where the cure rate was 83% (10/12 patients); however, only three cases had MRSA pathogens in that study and the combination was with daptomycin in 11 of the cases.3
The debate on whether a higher vancomycin MIC is associated with the failure of therapy is still ongoing owing to the conflicting and inconsistent data reporting the outcome with high MIC.16–21 Nevertheless, we encountered only one case with a slightly high MIC, where the vancomycin therapy failed. However, it will be difficult to attribute the failure only to the drug because there was a lack of source control.
Our case series will help in managing difficult cases with MRSA bacteremia when there are not many options, but it will not add significantly to current practice. Given the fact of the small number of and heterogeneity in our cases, a larger cohort and well-designed trial may be of great help in answering these questions. Finally, the retrospective chart review may be considered a major drawback in this study, due to the possibility of bias and missing essential data.
Conclusion
In conclusion, the addition of anti-MRSA Cephalosporin (ie, Ceftobiprole) showed promising results and an excellent clinical outcome in the treatment of MRSA bacteremia, even in the case of endocarditis and an immunocompromised patient. Further studies are needed to understand the optimal therapeutic options for MRSA bacteremia and the advantage of antibiotic combinations.
Ethics and Consent
The study was approved by the Institutional Review Board (IRB) in King Abdullah International Medical Research Center (KAIMRC) (Protocol number RC20/152/R). Written informed consent has been provided by the patients themselves* (except the patients who died, next of kin for the patient provided the informed consent). *The patient of case 3, he had MRSA bacteremia in 2018. However, at the time of consent, he was 18 years and he signed the consent by himself.
*The patient of case 3, he had MRSA bacteremia in 2018. However, at the time of consent, he was 18 years and he signed the consent by himself.
Disclosure
The authors reports no conflicts of interest in this work and received no financial support for the research, authorship, and/or publication of this article.
References
1. Falcó V, Burgos J, Almirante B. Ceftobiprole medocaril for the treatment of community-acquired pneumonia. Expert Opin Pharmacother. 2018;19(13):1503–1509. doi:10.1080/14656566.2018.1516749
2. Pfaller MA, Flamm RK, Mendes RE, et al. Ceftobiprole activity against gram-positive and -negative pathogens collected from the United States in 2006 and 2016. Antimicrob Agents Chemother. 2018;63(1):e01566–18. doi:10.1128/AAC.01566-18
3. Tascini C, Attanasio V, Ripa M, et al. Ceftobiprole for the treatment of infective endocarditis: a case series. J Glob Antimicrob Resist. 2019;20:56–59. doi:10.1016/j.jgar.2019.07.020
4. Hamed K, Engelhardt M, Jones ME, et al. Ceftobiprole versus daptomycin in Staphylococcus aureus bacteremia: a novel protocol for a double-blind, Phase III trial. Future Microbiol. 2020;15(1):35–48. doi:10.2217/fmb-2019-0332
5. Lesens O, Methlin C, Hansmann Y, et al. Role of comorbidity in mortality related to staphylococcus aureus bacteremia: a prospective study using the Charlson weighted index of comorbidity. Infect Control Hosp Epidemiol. 2003;24(12):890–896. doi:10.1086/502156
6. Yousef SA, Mahmoud SY, Eihab MT. Prevalence of methicillin resistant Staphylococcus aureus in Saudi Arabia: systemic review and meta-analysis. Afr J Clin Exp Microbiol. 2013;14(3):146–154.
7. Kourtis AP, Hatfield K, Baggs J, et al. Vital signs: epidemiology and recent trends in Methicillin-resistant and in Methicillin-susceptible staphylococcus aureus bloodstream infections - United States. MMWR Morb Mortal Wkly Rep. 2019;68(9):214–219. doi:10.15585/mmwr.mm6809e1
8. Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis. 2011;52(3):e18–e55.
9. Tong SYC, Lye DC, Yahav D, et al. Effect of vancomycin or daptomycin with vs without an antistaphylococcal β-lactam on mortality, bacteremia, relapse, or treatment failure in patients with MRSA bacteremia: a randomized clinical trial. JAMA. 2020;323(6):527–537. doi:10.1001/jama.2020.0103
10. Davis JS, Van Hal S, Tong SYC. Combination antibiotic treatment of serious methicillin-resistant Staphylococcus aureus infections. Semin Respir Crit Care Med. 2015;36(1):3–16. doi:10.1055/s-0034-1396906
11. Dhand A, Sakoulas G. Daptomycin in combination with other antibiotics for the treatment of complicated methicillin-resistant Staphylococcus aureus bacteremia. Clin Ther. 2014;36(10):1303–1316. doi:10.1016/j.clinthera.2014.09.005
12. Sieradzki K, Roberts RB, Haber SW, et al. The development of vancomycin resistance in a patient with methicillin-resistant staphylococcus aureus infection. N Engl J Med. 1999;340(7):517–523. doi:10.1056/NEJM199902183400704
13. Geriak M, Haddad F, Rizvi K, et al. Clinical data on daptomycin plus ceftaroline versus standard of care monotherapy in the treatment of methicillin-resistant staphylococcus aureus bacteremia. Antimicrob Agents Chemother. 2019;63(5):e02483–18. doi:10.1128/AAC.02483-18
14. Tattevin P, Basuino L, Bauer D, et al. Ceftobiprole is superior to vancomycin, daptomycin, and linezolid for treatment of experimental endocarditis in rabbits caused by methicillin-resistant Staphylococcus aureus. Antimicrob Agents Chemother. 2010;54(2):610–613. doi:10.1128/AAC.00886-09
15. Mahajan SN, Shah JN, Hachem R, et al. Characteristics and outcomes of methicillin-resistant staphylococcus aureus bloodstream infections in patients with cancer treated with vancomycin: 9-year experience at a comprehensive cancer center. Oncologist. 2012;17(10):1329–1336. doi:10.1634/theoncologist.2012-0029
16. Baxi SM, Clemenzi-Allen A, Gahbauer A, et al. Vancomycin MIC does not predict 90-day mortality, readmission, or recurrence in a prospective cohort of adults with staphylococcus aureus bacteremia. Antimicrob Agents Chemother. 2016;60(9):5276–5284. doi:10.1128/AAC.00658-16
17. Kalil AC, Van Schooneveld TC, Fey PD, et al. Association between vancomycin minimum inhibitory concentration and mortality among patients with Staphylococcus aureus bloodstream infections: a systematic review and meta-analysis. JAMA. 2014;312(15):1552–1564. doi:10.1001/jama.2014.6364
18. Lodise TP, Graves J, Evans A, et al. Relationship between vancomycin MIC and failure among patients with methicillin-resistant Staphylococcus aureus bacteremia treated with vancomycin. Antimicrob Agents Chemother. 2008;52(9):3315–3320. doi:10.1128/AAC.00113-08
19. Soriano A, Marco F, Martinez JA, et al. Influence of vancomycin minimum inhibitory concentration on the treatment of methicillin-resistant Staphylococcus aureus bacteremia. Clin Infect Dis. 2008;46(2):193–200. doi:10.1086/524667
20. van Hal SJ, Lodise TP, Paterson DL. The clinical significance of vancomycin minimum inhibitory concentration in Staphylococcus aureus infections: a systematic review and meta-analysis. Clin Infect Dis. 2012;54(6):755–771. doi:10.1093/cid/cir935
21. Adani S, Bhowmick T, Weinstein MP, et al. Impact of vancomycin MIC on clinical outcomes of patients with methicillin-resistant staphylococcus aureus bacteremia treated with vancomycin at an institution with suppressed MIC reporting. Antimicrob Agents Chemother. 2018;62(4):e02512–17. doi:10.1128/AAC.02512-17
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.