")
Back to Journals » Infection and Drug Resistance » Volume 15
Ceftazidime-Avibactam as Salvage Therapy in Pediatric Liver Transplantation Patients with Infections Caused by Carbapenem-Resistant Enterobacterales
Authors Wang W, Wang R, Zhang Y, Zeng L, Kong H, Bai X, Zhang W, Liang T
Received 6 April 2022
Accepted for publication 17 June 2022
Published 25 June 2022 Volume 2022:15 Pages 3323—3332
DOI https://doi.org/10.2147/IDR.S369368
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Weili Wang,1,2,* Rongrong Wang,3,* Yuntao Zhang,1,2 Lei Zeng,1,2 Haisen Kong,4 Xueli Bai,1,2 Wei Zhang,1,2 Tingbo Liang1,2,5,6
1Department of Hepatobiliary and Pancreatic Surgery, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2Liver Transplant Center, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 3Department of Clinical Pharmacy, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 4Department of Laboratory Medicine, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 5Zhejiang Provincial Key Laboratory of Pancreatic Disease, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 6Key Laboratory of Combined Multi-organ Transplantation of the Ministry of Health, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Tingbo Liang, Department of Hepatobiliary and Pancreatic Surgery, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China, Email [email protected]
Objective: There are few therapeutic options for infections caused by carbapenem-resistant Enterobacterales (CRE) in children following liver transplantation. Ceftazidime-avibactam (CAZ-AVI), a recently licensed antibacterial in China, was utilized as a salvage therapy against CRE in our center, and its efficacy and safety were therefore assessed.
Methods: The retrospective, observational study was conducted at the First Affiliated Hospital of Zhejiang University. Pediatric liver transplantation patients (≤ 12 years) who received CAZ-AVI as a salvage therapy against CRE infections were included from January 2020 to December 2021. Clinical success and all-cause death during hospitalization were the primary outcomes. Recurrence of infection, drug-related adverse events, and changes in inflammatory biomarkers were collected.
Results: Six children were enrolled, with a median age of 10.1 (interquartile range (IQR) 5.5– 13.8) months. Primary intraperitoneal infections occurred in all patients, with five patients developing bloodstream infections. KPC carbapenemases were detected in most isolates, and the susceptibility results showed general sensitivity to tigecycline, polymyxin B, and CAZ-AVI. Tigecycline-based therapy was taken as the initial treatment and withdrawn because of clinical failure (5 cases) or cholestasis (1 case). After CRE infection, the median time to convert to CAZ-AVI was 7.5 (IQR 7.0– 8.8) days, and the median CAZ-AVI treatment length was 21.0 (IQR 20.3– 28.5) days. Clinical success was achieved in all patients, with a zero percent all-cause death rate. No CRE infections recurred throughout hospitalization, and no resistance to CAZ-AVI was detected. Patients experienced vomiting (1/6), skin rash (1/6), and a transient increase in cystatin C (2/6), γ-glutamyltransferase (2/6), and alkaline phosphatase (3/6).
Conclusion: CAZ-AVI was shown to be a successful salvage treatment for CRE infection in pediatric liver transplant recipients, with minor and temporary drug-related side effects.
Keywords: ceftazidime-avibactam, carbapenem-resistant Enterobacterales, pediatric liver transplantation, salvage treatment, effectiveness, safety
Introduction
In recent years, infections caused by carbapenem-resistant Enterobacterales (CRE) have steadily increased in both adults and children.1–3 CRE infections have become a major public health concern worldwide and are linked to poor outcomes following solid organ transplantations.4–6 Our previous study found that CRE infections resulted in considerably worse 30-day and 180-day survival rates in adult liver transplant recipients.4 Children receiving liver transplants are also at risk from postoperative CRE infections, with 30-day death rates ranging from 6.8% to 23.8%, which was much greater than children without infections.7–10
Few antimicrobials are available to treat CRE; therefore, clinicians have to rely on antimicrobials with suboptimal pharmacokinetics or concerning toxicities, such as polymyxin, aminoglycosides, and trimethoprim sulfamethoxazole.2,11 In many complicated cases, combinations of two or more antimicrobials with relatively high doses were used;12 however, the data regarding clinical efficacy and toxicities are controversial, especially in pediatric patients. Once failure occurs, subsequent therapy will be particularly challenging. Fortunately, the National Medical Products Administration of China authorized ceftazidime-avibactam (CAZ-AVI), a new-lactamase inhibitor combination, in 2019. CAZ-AVI works against class A, class C, and some class D beta-lactamases,2 and has demonstrated promising results in adults with CRE infections.13–16 It is well tolerated and effective in children with complicated urinary tract infections (cUTIs)17 and complex intra-abdominal infections (cIAIs).18 However, its efficacy and safety have not been specially established in pediatric patients after liver transplantation. Therefore, we conducted a retrospective, observational study to evaluate the role of CAZ-AVI as salvage therapy in pediatric liver transplant recipients and provided a real-world experience for treating CRE in this vulnerable population.
Methods
Study Design and Participants
This was a retrospective, observational study conducted in the liver transplantation center of the First Affiliated Hospital of Zhejiang University (FAHZJ) in China. Pediatric liver transplant recipients who underwent liver transplantation from January 1, 2020, to December 31, 2021, were reviewed. The inclusion criteria were as follows: 1) hospitalized children ≥ three months to ≤12 years; 2) patients diagnosed with CRE infections after liver transplantation; 3) patients received CAZ-AVI as salvage therapy. The study was conducted following the principles of the Helsinki Declaration of 1975 and followed the statement of Strengthening the Reporting of Observational Studies in Epidemiology. Ethical approval was obtained from the authorized ethics committee of FAHZJ (IIT20210868A). The data were anonymous, and the requirement for informed consent was waived for our retrospective study. Since Jan 1, 2015, organ procurement from executed prisoners had been completely ceased in China. No organs from executed prisoners were used in any case involved in this study. All organs were donated voluntarily with written informed consent, and that this was conducted in accordance with the Declaration of Istanbul.
Antimicrobial Treatment and Dosage
CAZ-AVI was administered at a 62.5 mg/kg dose intravenously every eight hours. Initial antimicrobials against CRE were administrated according to the Vitro susceptibility test results and mainly included tigecycline, polymyxin B, and meropenem.
Antimicrobial Susceptibility Testing and Carbapenemase Testing
CRE isolates were collected from the drainage of ascites or bile and blood from these patients after transplantation. After obtaining single colonies, all isolates were identified using an automated Vitek 2 system (bioMérieux, France).
The polymyxins susceptibility data were interpreted in accordance with the European Committee on Antimicrobial Susceptibility Testing (EUCAST2021).19 The tigecycline susceptibility data were interpreted using the United States Food and Drug Administration breakpoints,20 with a minimal inhibitory concentration (MIC) ≤ 2 μg/mL considered sensitive. Other antibiotic susceptibility data were interpreted in accordance with the Clinical and Laboratory Standards (CLSI 2021).21 Susceptibility to CAZ-AVI was defined as an MIC ≤ 8 μg/mL. Carbapenemases in isolates were confirmed by the NG-Test CARBA5 immunochromatographic assay (NG Biotech).22
Data Collection
Demographic data (age, sex, body mass index [BMI]), medical history (eg, underlying disease, previous surgical history, preoperative antibiotic exposure), procedure-related information (eg, pediatric end-stage liver disease (PELD) score, graft information, and procedure-related information), status when diagnosed with CRE (intensive care unit (ICU) treatment, invasive mechanical ventilation, and postoperative complications), susceptibility testing results, experiment indicators, treatment therapy, and drug-related events of enrolled recipients were collected.
Definitions and Outcomes
CRE infections were identified according to the criteria outlined by CDC/NHSN 201923 and were described in detail in our previous report.24 Salvage therapy was defined as any antimicrobial administered after the withdrawal of the initial anti-CRE medicines because of clinical failure or adverse reactions.
The primary outcomes were clinical success and all-cause mortality during hospitalization. Clinical success was defined as the resolution of all symptoms, and no further antimicrobial treatment against CRE was required. Secondary outcomes included infection recurrence during hospitalization, variation in inflammatory biomarkers, and drug-related adverse reactions (eg, digestive tract symptoms, skin rashes, and abnormal kidney function) during treatment.
Statistical Analysis
A standard case report form was used to record all data collected, and descriptive statistics were used to characterize all variables. The count data is represented by n, the measurement data is depicted as median with interquartile range (IQR), and the R software was used for analysis. All data were clarified by three researchers.
Results
Baseline of Included Patients
A total of six children were enrolled; three were boys, with a median age of 10.1 (IQR 5.5–13.8) months and a median BMI of 17.6 (IQR 15.5–20.0) kg/m2. The primary liver disease was biliary atresia for all included patients, and hepatic portoenterostomy was conducted before liver transplantation. Regarding the graft type, five children received grafts from living donors and one from a donor after brain death. The six children had a history of carbapenem exposure three months before liver transplantation, and four were found to be colonized with CREs. The demographic and basic clinical characteristics are shown in Table 1.
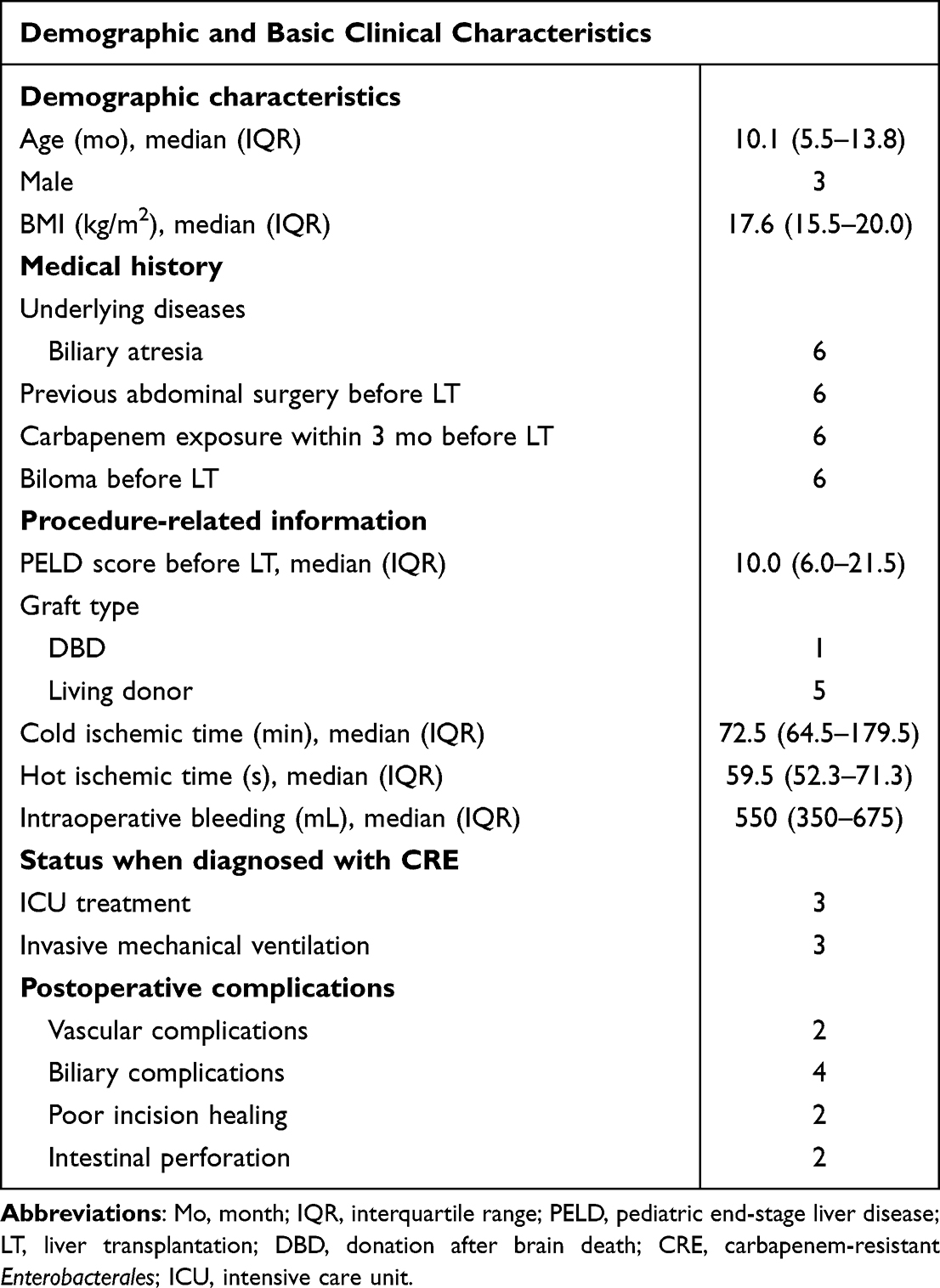 |
Table 1 Demographic and Essential Clinical Characteristics of Patients (N=6) |
Infection Characteristics
After transplantation, the median occurrence time of CRE infection was 3.0 (IQR 0.75–4.5) days. The primary infections were intraperitoneal infections in all patients, three with bile leak (case 3–5), one with bile leak and bowel perforation (case 2), one with bowel perforation (case 6), and another one (case 1) colonized with CRE before liver transplantation. CREs were isolated from the drainage of ascites or bile in all patients. Five children developed bloodstream infections. Carbapenem-resistant Klebsiella pneumonia (CR-KP) was isolated in all patients, and one child was also coinfected with Carbapenem-resistant Escherichia coli (CR-E.Coli). The susceptibility results showed that these isolated pathogens were generally resistant to carbapenems but sensitive to tigecycline, polymyxins, and CAZ-AVI (Table 2). Five (5/6) produced KPC carbapenemases for the six CR-KP isolates, while KPC, OXA-48-like, IMP, VIM, and NMD carbapenemases were not detected in one (1/6) isolate. NDM carbapenemases were detected in the CR-E.Coli isolate (Table 2).
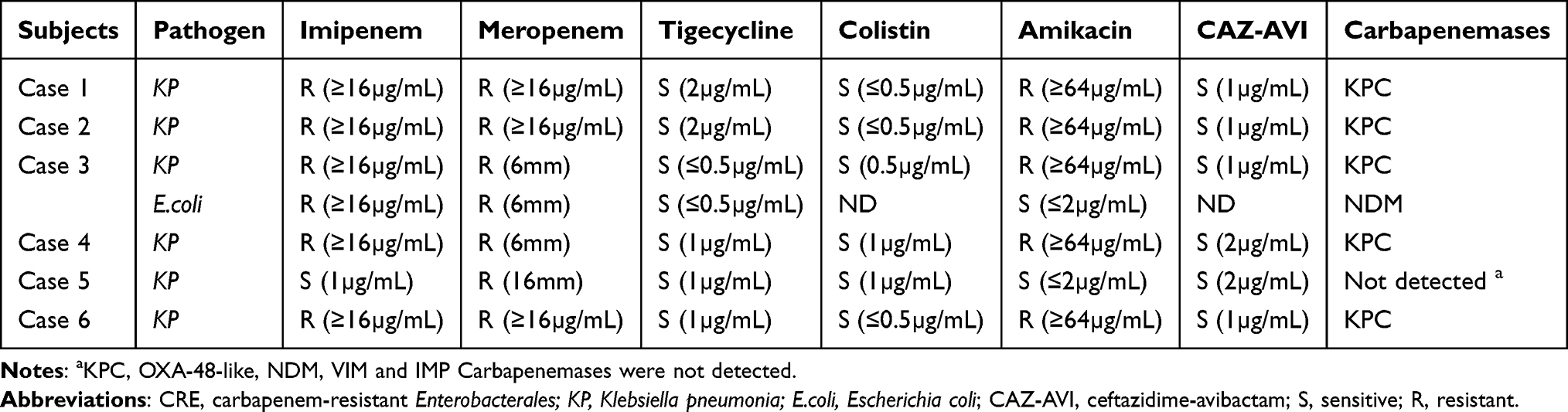 |
Table 2 Susceptibility Testing Results and Carbapenemases Type of CRE Isolates |
Treatments for CRE Infection
The initial treatment was tigecycline combined with meropenem in three patients and tigecycline combined with polymyxin B in others. The initial treatment failed in five patients, with slight or no improvement of the symptoms (repeated fever and non-recovery of inflammatory biomarkers, Figure 1) and persistent culture positivity for CREs. For case 3, the CR-E.Coli isolate was not detected on CAZ-AVI initiation, but the CR-KP still existed. One (case 1) patient experienced cholestasis during treatment with tigecycline combined with meropenem. The median conversion time to CAZ-AVI was 7.5 (IQR 7.0–8.8) days (Table 3). The salvage treatment was CAZ-AVI monotherapy in four children and CAZ-AVI combination therapy (CAZ-AVI with meropenem or polymyxin B) in two children (Table 3). Two children experienced exploratory laparotomy (cases 2 and 6) to control bowel perforation during treatment, and four children (cases 2–5) with bile leaks received adequate drainage.
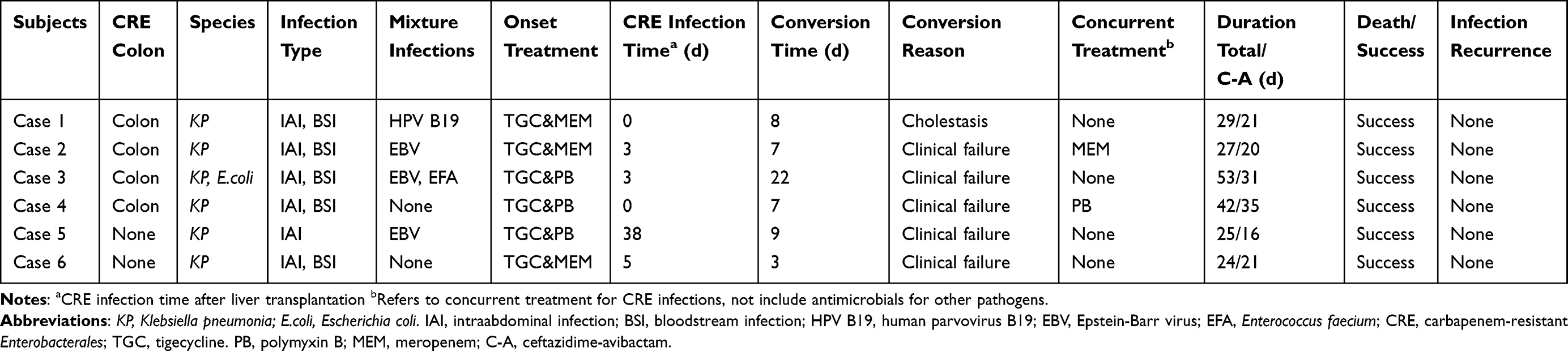 |
Table 3 Clinical Data of Patient Treated with Ceftazidime-Avibactam |
 |
Figure 1 Variation in inflammatory biomarkers during the treatment. (A–D) The variation in WBC, percentage of neutrophils, CPR, and PCT during treatment. Abbreviations: WBC, white blood cell counts; CRP, C-reactive protein; PCT, procalcitonin; C-A, ceftazidime/avibactam; CRE, carbapenem-resistant Enterobacterales. |
Clinical Outcomes
The symptoms of infection and inflammatory biomarkers in these children gradually improved after conversion (Figure 1), with a median treatment duration of 28.0 (IQR 25.5–38.8) days and a median CAZ-AVI treatment duration of 21.0 (20.3–28.5) days. During hospitalization, there was no all-cause mortality. CRE infections did not recur during hospitalization (Table 3), and no resistance to CAZ-AVI was observed.
Adverse Reactions
One patient experienced vomiting, and another experienced a rash while receiving CAZ-AVI treatment. In two patients (case 1 and case 2), alkaline phosphatase (ALP) and γ-glutamyltransferase (γ-GT) levels increased transiently. The rising trend of ALP in case 6 continued and gradually decreased nine days after CAZ-AVI therapy ended. In addition, after conversion, the cystatin C (CysC) level increased by more than twice the initial level in two patients before gradually returning to normal after CAZ-AVI treatment ended (Figure 2).
 |
Figure 2 Variation in laboratory indicators that may be related to adverse events during treatment. (A–D) The variation in ALP, γ-GT, Scr, and CysC during treatment. Abbreviations: ALP, alkaline phosphatase; γ-GT, γ-glutamyltransferase; Scr, serum creatinine; CysC, cystatin C; C-A, ceftazidime/avibactam; CRE, carbapenem-resistant Enterobacterales. |
Discussion
Salvage treatment for CRE can be complicated for clinicians after the initial treatment fails. The literature on CRE treatment in pediatric patients is more limited than that in adults.12,24 CAZ-AVI, a novel and promising antimicrobial, has been approved in many countries; however, its efficacy and safety in pediatric liver transplantation patients with CRE infections are unknown. To the best of our knowledge, this is the first study focused on CAZ-AVI as a salvage therapy for CRE infections in a group of pediatric liver transplant recipients. CAZ-AVI salvage treatment was successful in all cases, and none of the patients had a recurrence of CRE infections during their hospitalization. Some children experienced vomiting, skin rashes, and a transient increase in CysC, ALP, and γ-GT levels while on treatment. According to our findings, CAZ-AVI appears to be a promising option for salvage treatment in children with CRE infections after transplantation.
The Chinese National Medical Products Administration approved CAZ-AVI for marketing on May 21, 2019. Compared with other antimicrobials, such as aminoglycosides and colistin, observational studies showed that CAZ-AVI could improve treatment efficacy in adults with CRE infections without causing obvious side effects.13–16,25,26 However, there were some limitations to using CAZ-AVI up until now. The FDA expanded its indications for children older than three months, but it remains an off-label drug for children in China. Polymyxin B and tigecycline are covered by current healthcare insurance for infections caused by multidrug-resistant pathogens; however, CAZ-AVI is still self-funded in China. Furthermore, avibactam is currently on the WHO’s “reserve” list for children,27 indicating that it can be used if all other options fail or are inappropriate. After considering these factors, CAZ-AVI is currently being used as a salvage treatment for CRE infections in our center. The main type of infection of the enrolled patients was intraperitoneal infection, and the majority of them were combined with bloodstream infection. Other studies reported high death rates under similar situations, with 30-day death rates ranging from 6.8% to 23.8%.7–10 The overall mortality rate was 15.4% in a study using tigecycline against infections caused by carbapenem-resistant gram-negative bacteria in pediatric liver transplant recipients.24 Our center also tried a tigecycline-based regimen (combined with meropenem or polymyxin B); however, it did not work for these patients. Fortunately, all CR-KP isolates from the six children were sensitive to CAZ-AVI in Vitro. The infections were well controlled after conversion and did not recur during hospitalization. Notably, CAZ-AVI monotherapy was used in four children, with clinical success in all of them. CAZ-AVI combined with tigecycline, colistin, or carbapenems has shown synergistic activity against carbapenem-resistant pathogens in Vitro,28 encouraging clinicians to use CAZ-AVI combination therapy. Recently, two well-performed systematic reviews28,29 compared CAZ-AVI combination therapy with monotherapy in infections caused by carbapenem-resistant pathogens and found no difference in mortality rates between the two treatments, which agrees with our findings. Our results suggested that CAZ-AVI monotherapy could be an effective salvage treatment for pediatric liver transplant patients with CRE infections.
The median treatment duration for CAZ-AVI in our center was 21 days, which was longer than the treatment duration reported in two Phase 2 clinical trials (7–14 days for CAZ-AVI).17,18 However, treatment durations in children with severe and complex infections were reported to be similar or even longer.30,31 There is no conclusive data in the literature on the optimal treatment duration for CAZ-AVI. The children who received CAZ-AVI as salvage therapy in our center were immunocompromised and had severe infections, and most of them had bile leakage, which required a long healing time (such as in case 3 and case 4). If the anti-infection treatment is insufficient, there is a risk of infection recurrence and CAZ-AVI resistance, which might result in an increased economic burden. Therefore, our clinical team decided unanimously to use CAZ-AVI with conservatively long treatment duration.
The CysC levels in two children increased to twice their initial levels during treatment (their creatinine levels remained stable), which has never been reported before. Recent studies indicated that CysC might be a more sensitive indicator of renal damage.32 Our findings suggested that CAZ-AVI influences children’s renal function; this can be reversed after stopping the drug. In addition, patients experienced vomiting, rash, and a transient increase in ALP and γ-GT levels. It is worth noting that the complicated medicine used in these patients might contribute to the adverse events.
The present study had some limitations. First, this was a retrospective study with small sample size and no control group. It is difficult to conduct rigorous controlled studies because cases using CRE salvage treatment are uncommon, and treatment decisions were made based on the best treatment currently available. Second, our result cannot be extrapolated to CRE isolates with Metallo-b-lactamase. Although one isolated CR-E.coli produced NDM carbapenemases, it was not detected before CAZ-AVI initiation. Therefore, the initial therapy (tigecycline and polymyxin B) may be effective for this isolate. The “big 5” families of carbapenemases (KPC, OXA-48-like, NDM, VIM, and IMP) were not detected for one CR-KP isolate. The resistance to carbapenem of this isolate may be caused by the production of other kinds of carbapenemases or alterations in membrane permeability combined with the production of extended-spectrum β-lactamases or AmpC β-lactamases.12 For the latter condition, the in Vitro results indicated high susceptibility of novel beta-lactamase inhibitors (including CAZ-AVI, meropenem-vaborbactam, etc.) among these isolates,12 which was consistent with the in Vitro susceptibility testing result in our study. Despite these limitations, our experience provides real-world evidence for treating CRE infections in children after liver transplantation. It lays a foundation for future well-designed, comparable, multicenter studies.
Abbreviations
CRE, carbapenem-resistant Enterobacterales; CAZ-AVI, ceftazidime-avibactam; IQR, interquartile range; cUTIs, complicated urinary tract infections; cIAIs, complex intra-abdominal infections; MIC, minimal inhibitory concentration; CLSI, clinical and laboratory standards; PELD, pediatric end-stage liver disease; ICU, intensive care unit; BMI, body mass index.
Funding
This project was supported by the Provincial Key Research and Development Program of Zhejiang (2019C03019), the Natural Science Foundation of Zhejiang Province (LYY20H310001), and the project of the Zhejiang Pharmaceutical Association (2014ZYY04).
Disclosure
The authors declared that they have no conflicts of interest in this work.
References
1. Bonomo RA, Burd EM, Conly J, et al. Carbapenemase-producing organisms: a global scourge. Clin Infect Dis. 2018;66(8):1290–1297. doi:10.1093/cid/cix893
2. Durante-Mangoni E, Andini R, Zampino R. Management of carbapenem-resistant Enterobacteriaceae infections. Clin Microbiol Infect. 2019;25(8):943–950. doi:10.1016/j.cmi.2019.04.013
3. Logan LK, Weinstein RA. The epidemiology of carbapenem-resistant Enterobacteriaceae: the impact and evolution of a global menace. J Infect Dis. 2017;215(suppl_1):S28–S36. doi:10.1093/infdis/jiw282
4. Chen Y, Wang WL, Zhang W, et al. Risk factors and outcomes of carbapenem-resistant Enterobacteriaceae infection after liver transplantation: a retrospective study in a Chinese Population. Infect Drug Resist. 2020;13:4039–4045. doi:10.2147/IDR.S278084
5. Ferstl PG, Filmann N, Brandt C, et al. The impact of carbapenem resistance on clinical deterioration and mortality in patients with liver disease. Liver Int. 2017;37(10):1488–1496. doi:10.1111/liv.13438
6. Pagani N, Corcione S, Lupia T, et al. Carbapenemase-producing Klebsiella pneumoniae colonization and infection in solid organ transplant recipients: a single-center, retrospective study. Microorganisms. 2021;9(11):2272. doi:10.3390/microorganisms9112272
7. Sun Y, Zheng H, Zhang JL, et al. [Clinical characteristics of carbapenem-resistant Enterobacteriaceae infection in pediatric liver transplantation recipients]. Zhonghua Er Ke Za Zhi. 2020;58(8):640–645. Chinese. doi:10.3760/cma.j.cn112140-20200316-00239
8. Sun Y, Yu L, Gao W, et al. Investigation and analysis of the colonization and prevalence of carbapenem-resistant Enterobacteriaceae in pediatric liver transplant recipients. Infect Drug Resist. 2021;14:1957–1966. doi:10.2147/IDR.S304998
9. Ara-Montojo MF, Escosa-García L, Alguacil-Guillén M, et al. Predictors of mortality and clinical characteristics among carbapenem-resistant or carbapenemase-producing Enterobacteriaceae bloodstream infections in Spanish children. J Antimicrob Chemother. 2021;76(1):220–225.
10. Matsumura Y, Tanaka M, Yamamoto M, et al. High prevalence of carbapenem resistance among plasmid-mediated AmpC β-lactamase-producing Klebsiella pneumoniae during outbreaks in liver transplantation units. Int J Antimicrob Agents. 2015;45(1):33–40. doi:10.1016/j.ijantimicag.2014.08.015
11. Doi Y. Treatment options for carbapenem-resistant gram-negative bacterial infections. Clin Infect Dis. 2019;69(Suppl 7):S565–S575. doi:10.1093/cid/ciz830
12. Chiotos K, Hayes M, Gerber JS, Tamma PD. Treatment of carbapenem-resistant Enterobacteriaceae infections in children. J Pediatric Infect Dis Soc. 2020;9(1):56–66. doi:10.1093/jpids/piz085
13. Temkin E, Torre-Cisneros J, Beovic B, et al. Ceftazidime-avibactam as salvage therapy for infections caused by carbapenem-resistant organisms. Antimicrob Agents Chemother. 2017;61(2). doi:10.1128/AAC.01964-16
14. Shields RK, Nguyen MH, Chen L, et al. Ceftazidime-avibactam is superior to other treatment regimens against carbapenem-resistant Klebsiella pneumoniae bacteremia. Antimicrob Agents Chemother. 2017;61(8). doi:10.1128/AAC.00883-17
15. Castón JJ, Lacort-Peralta I, Martín-Dávila P, et al. Clinical efficacy of ceftazidime/avibactam versus other active agents for the treatment of bacteremia due to carbapenemase-producing Enterobacteriaceae in hematologic patients. Int J Infect Dis. 2017;59:118–123. doi:10.1016/j.ijid.2017.03.021
16. van Duin D, Lok JJ, Earley M, et al. Colistin versus ceftazidime-avibactam in the treatment of infections due to carbapenem-resistant Enterobacteriaceae. Clin Infect Dis. 2018;66(2):163–171. doi:10.1093/cid/cix783
17. Bradley JS, Roilides E, Broadhurst H, et al. Safety and efficacy of ceftazidime-avibactam in the treatment of children ≥3 months to <18 years with complicated urinary tract infection: results from a phase 2 randomized, controlled trial. Pediatr Infect Dis J. 2019;38(9):920–928. doi:10.1097/INF.0000000000002395
18. Bradley JS, Broadhurst H, Cheng K, et al. Safety and efficacy of ceftazidime-avibactam plus metronidazole in the treatment of children ≥3 months to <18 years with complicated intra-abdominal infection: results from a phase 2, randomized, controlled trial. Pediatr Infect Dis J. 2019;38(8):816–824. doi:10.1097/INF.0000000000002392
19. The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters; 2019. Available from: http://www.eucast.org.
20. Shen L, Lian C, Zhu B, et al. Bloodstream infections due to carbapenem-resistant Klebsiella pneumoniae: a single-center retrospective study on risk factors and therapy options. Microb Drug Resist. 2021;27(2):227–233. doi:10.1089/mdr.2019.0455
21. CLSI. Performance Standards for Antimicrobial Susceptibility Testing.
22. Hopkins KL, Meunier D, Naas T, Volland H, Woodford N. Evaluation of the NG-Test CARBA 5 multiplex immunochromatographic assay for the detection of KPC, OXA-48-like, NDM, VIM and IMP carbapenemases. J Antimicrob Chemother. 2018;73(12):3523–3526. doi:10.1093/jac/dky342
23. CDC/NHSN. CDC/NHSN surveillance definitions for specific types of infections. Available from: https://www.cdc.gov/nhsn/. pdfs/pscmanual/17pscnosinfdef_current.pdf.
24. Chen F, Shen C, Pang X, et al. Effectiveness of tigecycline in the treatment of infections caused by carbapenem-resistant gram-negative bacteria in pediatric liver transplant recipients: a retrospective study. Transpl Infect Dis. 2020;22(1):e13199. doi:10.1111/tid.13199
25. Sousa A, Pérez-Rodríguez MT, Soto A, et al. Effectiveness of ceftazidime/avibactam as salvage therapy for treatment of infections due to OXA-48 carbapenemase-producing Enterobacteriaceae. J Antimicrob Chemother. 2018;73(11):3170–3175. doi:10.1093/jac/dky295
26. Tumbarello M, Trecarichi EM, Corona A, et al. Efficacy of ceftazidime-avibactam salvage therapy in patients with infections caused by Klebsiella pneumoniae Carbapenemase-producing K. pneumoniae. Clin Infect Dis. 2019;68(3):355–364. doi:10.1093/cid/ciy492
27. World Health Organization. Model List of Essential Medicines – 22nd List 2021. Geneva: World Health Organization; 2021.
28. Onorato L, Di Caprio G, Signoriello S, Coppola N. Efficacy of ceftazidime/avibactam in monotherapy or combination therapy against carbapenem-resistant Gram-negative bacteria: a meta-analysis. Int J Antimicrob Agents. 2019;54(6):735–740. doi:10.1016/j.ijantimicag.2019.08.025
29. Fiore M, Alfieri A, Di Franco S, et al. Ceftazidime-avibactam combination therapy compared to ceftazidime-avibactam monotherapy for the treatment of severe infections due to carbapenem-resistant pathogens: a systematic review and network meta-analysis. Antibiotics. 2020;9(7):388. doi:10.3390/antibiotics9070388
30. Tamma PD, Fan Y, Bergman Y, et al. Successful treatment of persistent Burkholderia cepacia complex bacteremia with ceftazidime-avibactam. Antimicrob Agents Chemother. 2018;62(4). doi:10.1128/AAC.02213-17
31. Algwizani A, Alzunitan M, Alharbi A, et al. Experience with ceftazidime-avibactam treatment in a tertiary care center in Saudi Arabia. J Infect Public Health. 2018;11(6):793–795. doi:10.1016/j.jiph.2018.04.013
32. Inker LA, Eneanya ND, Coresh J, et al. New creatinine- and cystatin C-based equations to estimate GFR without race. N Engl J Med. 2021;385(19):1737–1749. doi:10.1056/NEJMoa2102953
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.