")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 14
Ceftaroline Fosamil for the Empiric Treatment of Hospitalized Adults with cSSTI: An Economic Analysis from the Perspective of the Spanish National Health System
Authors Torres A, Soriano A, Rivolo S, Remak E, Peral C, Kantecki M, Ansari W, Charbonneau C, Hammond J, Grau S, Wilcox M
Received 7 October 2021
Accepted for publication 3 March 2022
Published 18 March 2022 Volume 2022:14 Pages 149—161
DOI https://doi.org/10.2147/CEOR.S329494
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Antoni Torres,1 Alex Soriano,2 Simone Rivolo,3 Edit Remak,4 Carmen Peral,5 Michal Kantecki,6 Wajeeha Ansari,7 Claudie Charbonneau,8 Jennifer Hammond,9 Santiago Grau,10 Mark Wilcox11
1Servei de Pneumologia Hospital Clinic, University of Barcelona, IDIPAPS, CIBERES, ICREA, Barcelona, Spain; 2Hospital Clínic of Barcelona,University of Barcelona, IDIBAPS, Barcelona, Spain; 3Modeling and Simulation, Evidera, London, UK; 4Formerly Modeling and Simulation, Evidera, Budapest, Hungary; 5Health Economics and Outcomes Research, Pfizer, Madrid, Spain; 6Global Medical Affairs, Pfizer, Paris, France; 7Patient & Health Impact, Pfizer, New York, NY, USA; 8Patient & Health Impact, Pfizer, Paris, France; 9Global Product Development, Pfizer, Collegeville, PA, USA; 10Hospital del Mar,Universitat Pompeu Fabra, Barcelona, Spain; 11University of Leeds, Leeds, UK
Correspondence: Wajeeha Ansari, Tel +1 212 733 5001, Email [email protected]
Purpose: Complicated skin and soft tissue infections (cSSTI) are associated with high healthcare resource use and costs. The emergency nature of cSSTI hospitalizations requires starting immediate empiric intravenous (IV) antibiotic treatment, making the appropriate choice of initial antibiotic therapy crucial.
Patients and Methods: The use of ceftaroline fosamil (CFT) as an alternative to other IV antibiotic therapies for the empiric treatment of hospitalized adults with cSSTI (vancomycin, linezolid, daptomycin, cloxacillin, tedizolid) was evaluated through cost consequences analysis. The model structure was a decision tree accounting for four different pathways: patients demonstrating early response (ER) either discharged early (with oral antibiotic) or remaining in hospital to continue the initial therapy; non-responders either remaining on the initial IV therapy or switching to a second-line antibiotic. The model perspective was the Spanish National Health System.
Results: CFT resulted in average percentage of patients discharged early (PDE) of 24.6% (CI 19.49– 30.2%) with average total cost per patient of € 6763 (€ 6268–€ 7219). Vancomycin, linezolid, daptomycin and tedizolid resulted in average PDE of 22% (17.34– 27.09%), 26.4% (20.5– 32.32%), 28.6% (22.08– 35.79%) and 26.5% (20.39– 33.25%), respectively, for a total cost per patient of € 6,619 (€ 5,902–€ 6,929), € 6,394 (€ 5,881–€ 6,904), € 6,855 (€ 5,800–€ 7,410) and € 7,173 (€ 6,608–€ 7,763), respectively. Key model drivers were ER and antibiotic treatment duration, with hospital costs accounting for over 83% of the total expenditures.
Conclusion: Given its clinical and safety profile, CFT is an acceptable choice for cSSTI empiric therapy providing comparable ER and costs to other relevant antibiotic options.
Keywords: complicated skin and soft tissue infection, cost-consequences, Spain, ceftaroline fosamil
Introduction
Complicated skin and soft tissue infections (cSSTI), similarly to most infectious diseases, cause widespread morbidity frequently leading to hospitalization.1,2 In these cases, such infections are associated with high healthcare resource use and costs, particularly driven by hospital length of stay.3–5 Given the emergency nature of these hospitalizations, and the urgent need to initiate antimicrobial therapy, empiric intravenous (IV) antibiotic treatment is commonly started before the causative pathogen has been identified.6 However, patients failing to respond to initial antibiotic therapy are associated with a higher risk of mortality, morbidity and prolonged hospital stay,6 in turn resulting in increased hospital expenditures.7–9 Therefore, the appropriate choice of initial antibiotic therapy is pivotal.
Skin and soft tissue infections (SSTIs) may be complicated (cSSTI), due to the severity of infection, need for surgical intervention and/or concomitant morbidities.10 The management of cSSTI has been recently further complicated by the rise of hospitalizations for Staphylococcus aureus (SA)-associated SSTI,11,12 along with the concomitant rise in antibiotic resistant SA strains, including methicillin-resistant SA (MRSA).13,14 Upon admission, prior to isolation of the causative organism, cSSTI patients are generally treated empirically with intravenous penicillin with or without a β-lactamase inhibitor, and other antibiotics, such as vancomycin and daptomycin.15 Clinical review of the patient after 48–72 hours is essential to assess response to treatment, and to align with the results of microbiological testing.13 Early response by Day 3 is indicative of less severe disease and better clinical outcome,16,17 possibly enabling a switch to oral therapy and potentially resulting in early discharge.15 Conversely, patients without signs of early response, as seen in those with more severe disease, co-morbidities or more difficult-to-treat micro-organisms, may require longer treatment and/or broadening of the initial treatment to enhance the possibility of clinical response. Ultimately, failure of initial antibiotic therapy and consequent treatment modification has been demonstrated to lead to higher mortality, longer hospital stay and in turn higher costs.17,18 Therefore, to minimize the risk of initial antibiotic failure and consequently the length of hospital stay for hospitalized cSSTI patients, an antibiotic with relatively high early response efficacy is highly desirable.
Ceftaroline fosamil (CFT; Zinforo® in Europe and Teflaro® in US) combines the safety and tolerability of a cephalosporin with efficacy against important pathogens responsible for cSSTI, including MRSA. Two non-inferiority studies (CANVAS 1 and CANVAS 2) demonstrated that CFT has comparable efficacy with vancomycin + aztreonam, in the empiric treatment of hospitalized adults with cSSTI.19 Furthermore, in comparison with vancomycin, daptomycin, linezolid or tigecycline, CFT was associated with comparable in-hospital mortality rate and significantly lower length of stay and in-patient costs.20
The availability of newer agents, such as CFT, increases the choice of cSSTI treatment options for clinicians. However, treatment decisions are made considering both clinical benefit as well as economic value, given the rising concern of national health system expenditures. Therefore, a cost-consequence analysis was developed to evaluate the impact of using IV CFT in the empiric treatment of cSSTI as an alternative to other IV relevant antibiotic treatments from the perspective of the Spanish National Health System. The cost-consequence analysis allows to compare early response and the individual costs categories (eg, hospitalization costs, antibiotic costs) associated with each cSSTI treatment option.
Patients and Methods
Model Structure
Microsoft Excel 2016® (Microsoft Corporation, Redmond, WA, USA) was used to develop a decision-tree model, evaluating the use of CFT 600mg every 12 hours (q12h) or other antibiotic therapies for the empiric treatment of hospitalized adult patients with cSSTI. The model structure chosen was a decision-tree since costs and clinical outcomes (resolution of signs and symptoms of the infection) occur over a relatively short period of time, typically <3 weeks from hospital admission to discharge.15 Furthermore, a similar model design has been used in previous economic evaluations of cSSTI treatments available in the literature.21–24
Each branch of the decision-tree shown in Figure 1 represents a clinical pathway. The square in the schematic of the model represents a decision node where the decision to use CFT or other comparators is made. The circles represent chance nodes where probabilities determine the pathway that a trial simulation will travel. The triangles represent terminal nodes at which the total direct costs are determined for that specific branch of the model. The decision-tree probabilities can be found in Table 1.
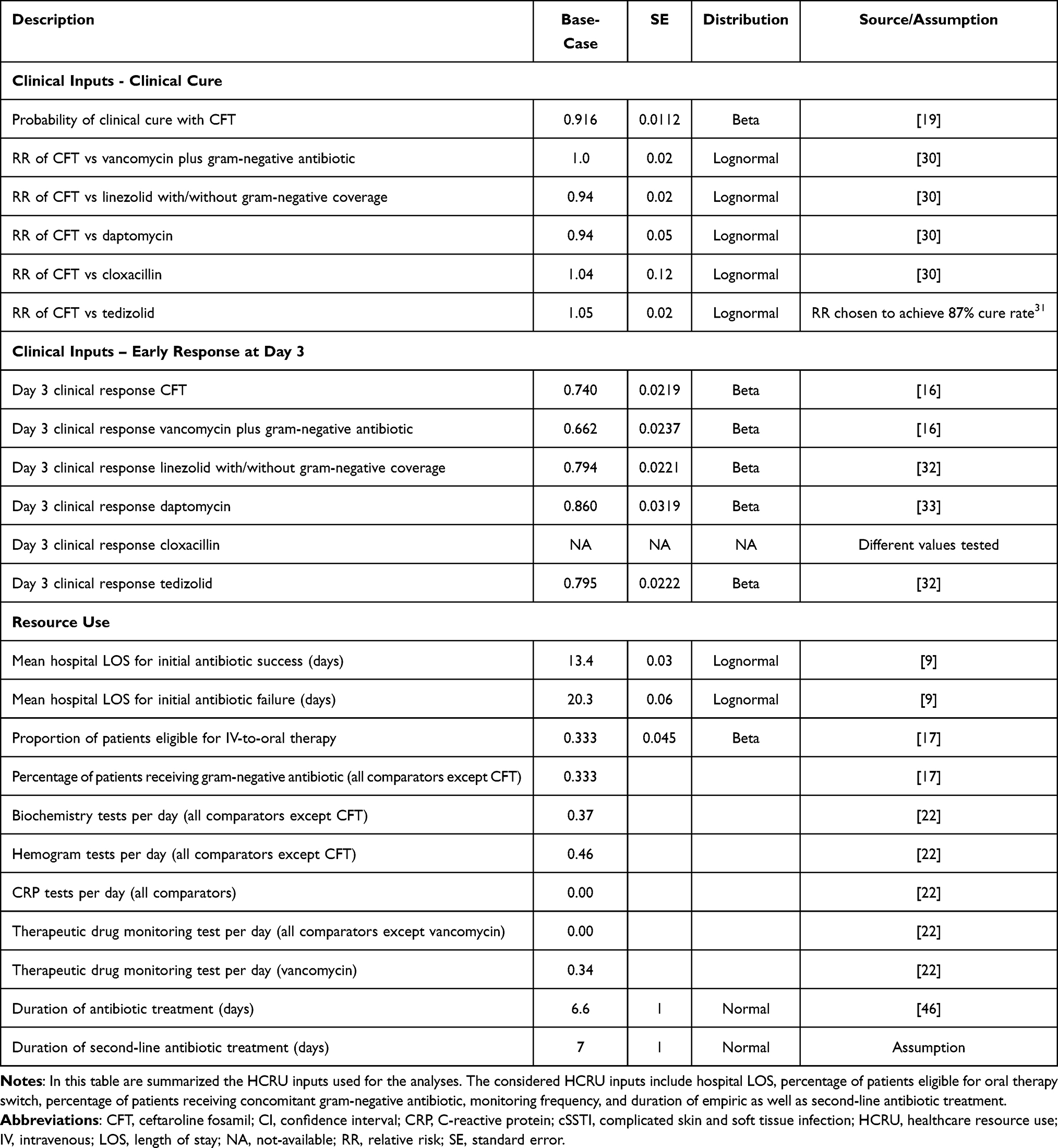 |
Table 1 Summary of Clinical Inputs and Resource Use Along with SE and Distribution Used for Base-Case and Sensitivity Analyses |
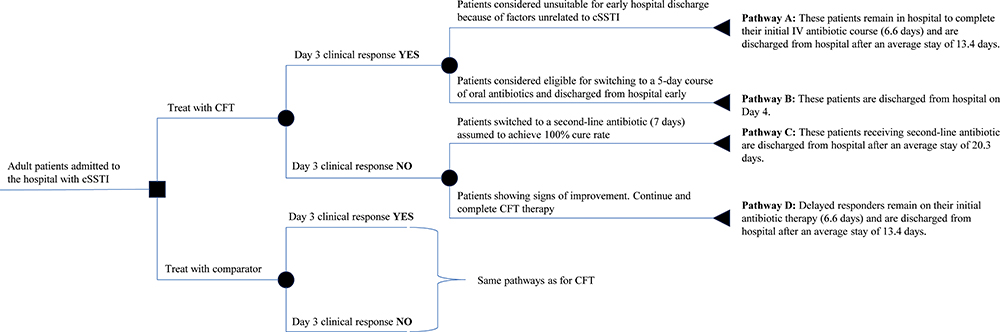 |
Figure 1 Schematic representation of the decision tree model with the patient pathways described above each branch. The decision-tree probabilities used in the analysis can be found in Table 1. Abbreviations: CFT, ceftaroline fosamil; cSSTI, complicated skin and soft tissue infection; IV, intravenous; LOS, length of stay. |
An hypothetical cohort of adult patients with cSSTI hospital admission requiring immediate empiric IV antibiotic therapy is simulated in the model (Figure 1). Patients are immediately started on IV antibiotic therapy, before clinical and microbiological assessment, after which the treatment pathways diverge. Patients demonstrating early response are either discharged early switching to an oral antibiotic or remain in hospital continuing the initial IV antibiotic therapy, due to factors unrelated to cSSTI (eg, unable to swallow). On the contrary, non-responders either remain on their initial IV antibiotic or switch to a second-line antibiotic until clinical cure and discharge. Therefore, the model considers as clinical outcomes early response at Day 3 and clinical cure rate at test-of-cure.
The comparator antibiotics considered in the economic analysis were vancomycin 1g q12h, linezolid 600mg q12h, daptomycin 4–10mg/kg/day, tedizolid 200mg every 24 hours (q24h) and semi-synthetic penicillin (cloxacillin) 1–2g every 4–6 hours (q4–6h), based on cSSTI guidelines25–28 and clinical experts consultation. The model perspective was the Spanish National Health System.
Early response is assessed at Day 3, as recommended by cSSTI guidelines (ie, 48–72 hours after initiation of therapy28), and all Day 3 non-responders are assumed to continue treatment in the general ward. Following clinical specialists’ consultation, amoxicillin clavulanate (vial formulation) was chosen as 2nd line antibiotic while amoxicillin clavulanate (oral formulation) was chosen as oral step-down antibiotic (more details can be found in the Economic Inputs section).
Model Inputs
Clinical Inputs
Table 1 summarizes the clinical inputs used to parametrize the cost-consequence analysis for all comparators, with the first section of Table 1 summarizing the clinical cure rate, while the second section of Table 1 listing the clinical inputs for early response at Day 3.
The clinical cure rate at the test-of-cure visits (8–15 days after the last dose of study drug)19 for CFT (91.6%) was derived from a pooled analysis of the two Phase III RCTs CANVAS 1 and CANVAS 2, in the clinically evaluable (CE) population (defined as all randomized patients who received any treatment, who met clinical disease criteria for cSSTI, received a prespecified minimum amount of study drug, and for whom outcome information was available).19 The baseline characteristics of CANVAS 1 and CANVAS 2 patients have been reported in the literature19 and are briefly summarized here. Patients had a median age of 48 years with a higher proportion of males (61–64%) and United States as region of enrollment (43%) compared to Europe (EU: 21%; non-EU:27%) and Latin America (8%). Patients median BMI was 27, with a diabetes mellitus prevalence of 17%, peripheral vascular disease of 13% and injection drug use of 7%-8%. The most common site of primary infection was the lower limb (48–49%) with head/neck being less common (4–6%), and the median size of infection was 15 cm in length and 10 cm of width. About a third of patients had prior antimicrobial therapy (38–39%), with 14–16% of patients having received more than one surgical procedures on primary infection within 48 hours of enrollment, 5–7% having received incision and drainage and 4% debridement.19 The Wilson Disease Severity Score was not considered in the CANVAS 1 and 2 pooled analysis19 but was calculated afterwards in a prospective study, which derived a median Wilson Disease Severity Score for CANVAS patients of 76.5.29
Head-to-head data for the comparators were not available. Therefore, clinical cure rates for the comparators were estimated from a published network meta-analysis (NMA).30 The NMA used a systematic literature review (SLR) to estimate the relative efficacy of CFT against initial IV antibiotics in methicillin-resistant Staphylococcus aureus (MRSA)-suspected cSSTI. The search strategy was restricted to English language manuscripts with a publication date until November 2015. Fixed-effect model NMA was conducted to assess effect size in three population sets (intention-to-treat (ITT), clinically-evaluable (CE), and microbiologically-evaluable (ME)), with no adjustments assumed for multiple comparisons. The NMA results in the CE population were used to ensure consistency with CFT cure rate estimate, with the relative risk (RR) of CFT versus vancomycin, linezolid, daptomycin and cloxacillin estimated at 1.00 (95% CI 0.97–1.03), 0.94 (95% CI 0.91–0.99), 0.94 (95% CI 0.85–1.03) and 1.04 (95% CI 0.83–1.32), respectively (Table 1).
For tedizolid, which was not included in the NMA, the clinical cure rate (87%) was derived from ESTABLISH-2,31 a Phase III trial which evaluated IV tedizolid for cSSTI.
Day 3 clinical response, which was sourced from the literature, was based as meeting both cessation of infection spread (no increase in baseline lesion width or length measurement) and absence of fever (temperature ≤ 37.6°C).16 Patients who did not meet both criteria were considered non-responders. Day 3 clinical response rates for CFT (74%) and vancomycin (66.2%) were sourced by a pooled analysis of CANVAS 1 and 2 phase III RCTs,16 consistent with the clinical cure rate derivation. Linezolid’s day 3 clinical response (79.4%),32 tedizolid day 3 clinical response (79.5%)31 and daptomycin day 3 clinical response (86%)33 were derived from the literature. Cloxacillin early response criteria utilized in the identified evidence in the literature was significantly different with respect to the one utilized for ceftaroline fosamil, thus hampering the possibility of direct comparison. Nevertheless, threshold analysis was performed.
Economic Inputs
Tables 1 and 2 summarize the health-care resource use and costs used in the base case analysis, along with the source and the distribution used for sensitivity analysis. The average hospital length of stay (LOS) for patients responding or not responding to initial antibiotic therapy and not discharged early (13.4 and 20.3 days respectively) was sourced from a retrospective observational study in Italy.9 Limited information was available to inform the base case input of the proportion of treatment responders eligible for iv-to-oral switch. Based on the available literature17 and clinical experts consultation 33.3% of patients were assumed to eligible for IV-to-oral therapy switch. Amoxicillin clavulanate (vial formulation) was selected as 2nd line antibiotic while amoxicillin clavulanate (oral formulation) was chosen as oral step-down antibiotic. Furthermore, it was assumed that all comparators except for ceftaroline fosamil may require pairing with a gram-negative antibiotic (aztreonam 1g q8hr) and that gram-negative antibiotic would be used in 33% of patients.17 Daptomycin 4mg/kg/day, cloxacillin 1g/q6hr and aztreonam 1g/q8hr dosages were the base case inputs, since they were used in the clinical trials from which the clinical inputs were derived. Nevertheless, in scenario analysis, alternative dosages of daptomycin 4–10mg/kg/day, cloxacillin 1–2g/q4-6hr and aztreonam 2g q8hr were simulated to match dosages more commonly used in clinical practice.25–28 Finally, based on clinical experts consultation, no treatment monitoring was assumed for CFT while biochemistry and hemogram were considered for all other comparators and therapeutic drug monitoring for vancomycin only, with the frequency based on a previous cSSTI economic study.22
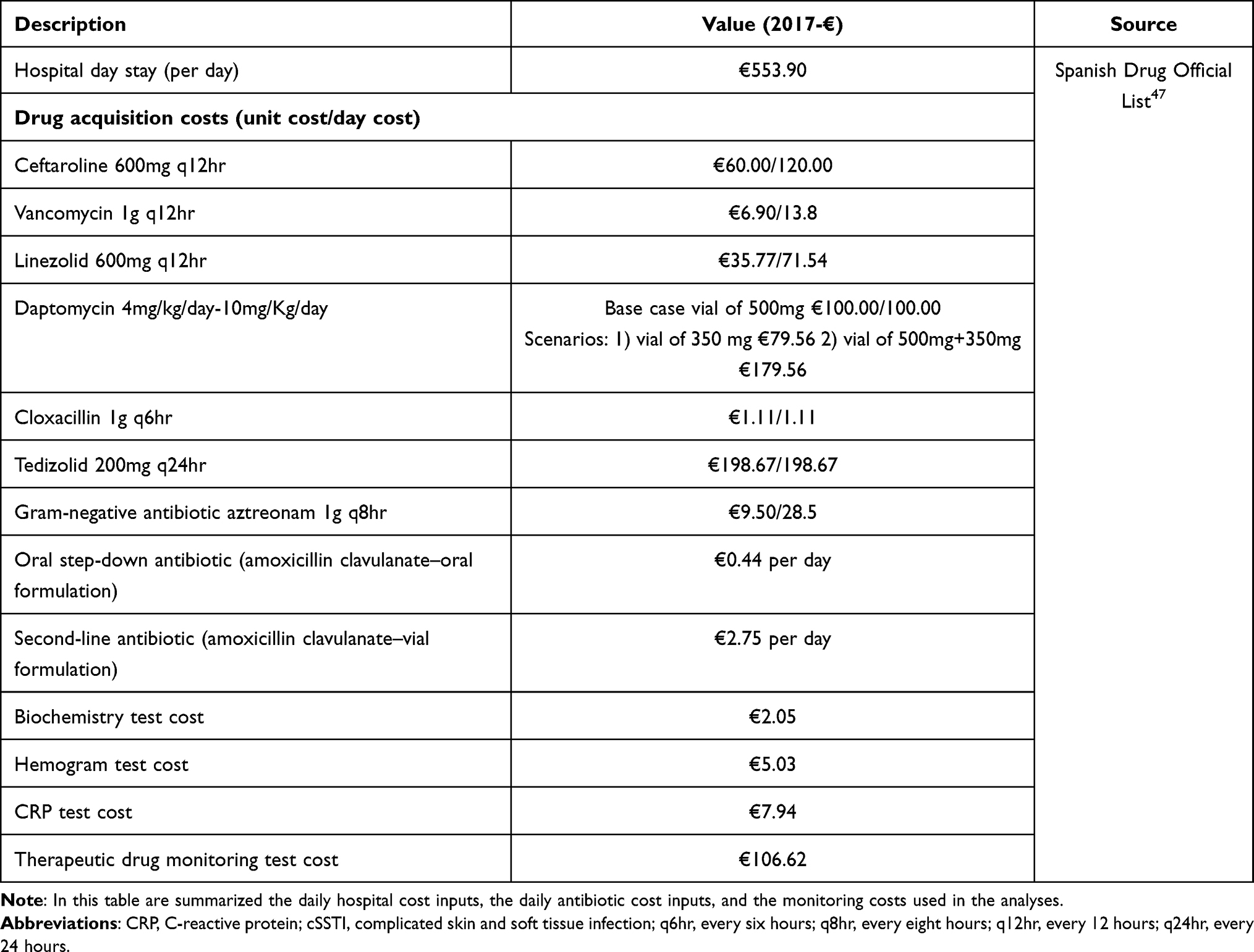 |
Table 2 Cost Inputs Used for the Analyses |
Model Assumptions
During the model development, multiple assumptions were needed to simplify the clinical pathways and enable to parametrize the model integrating data from multiple sources. Firstly, the early response rates across trials were assumed to be comparable. Secondly, the IV antibiotic treatment duration for patients not being discharged early was assumed to be the same for CFT and all the comparators considered, due to the lack of treatment specific data published in the literature. Thirdly, the 2nd line antibiotic efficacy was assumed to be 100% implying that all the patients failing initial antibiotic therapy would respond to the 2nd line treatment. Finally, the modeled early response and clinical cure rates were derived from the clinical trials and indirect treatment comparison, and assumed to represent the overall effectiveness of each antibiotic considered. Early response and clinical cure rates are likely driven by multiple factors (eg, co-morbidities, disease severity, prognostic factors) that are not explicitly modeled (eg, through risk equations linking patient baseline characteristics with the probability of response at Day 3).
Model Analyses
The health outcomes predicted by the economic model were the proportion of patients with early discharges (PDE), the percentage of patients switched to 2nd line antibiotic, the overall costs per patient and the incremental costs of CFT with respect to the alternative antibiotic treatments considered in the analysis.
Deterministic (DSA) and probabilistic (PSA) sensitivity analyses were conducted to evaluate the impact of input parameters uncertainty. DSA enabled identification of key drivers of model outcomes, by varying univariately (one parameter for each simulation) the base-case estimates within their 95% confidence interval (CI). PSA enabled to quantify the impact of joint uncertainty of the inputs parameters on the model outcomes, by simultaneously varying the model inputs over 1000 simulations.
The statistical distributions used for sensitivity analysis are summarized in Tables 1 and 2, with the beta distribution used for probabilities, and relative risks assumed to be log-normally distributed.36 The hospitalization and treatment monitoring costs were varied in DSA by ±25%.
Results
The analysis results are summarized in Figure 2, with each bar representing the base case result and the confidence interval (CI) based on 1,000 probabilistic simulations (CI provided in Figure 2). CFT resulted in average PDE of 24.6% (Figure 2B) with average total cost per patient of €6,763 (Figure 2A). Vancomycin, linezolid, daptomycin and tedizolid resulted in average PDE of 22%, 26.4%, 28.6% and 26.5%, respectively (Figure 2B) for a total cost per patient of €6,619, €6,394, €6,855 and €7,173, respectively (Figure 2A). The percentage of patients switched to 2nd line antibiotic was 2.18%, 2.84%, 0.52%, 0.35% and 2.66% for CFT, vancomycin, linezolid, daptomycin and tedizolid, respectively (see Figure 2C for confidence intervals). Based on threshold analysis, cloxacillin early response rate of 50.2%–53.3% resulted in total cost neutrality vs CFT, depending on the cloxacillin dosage considered.
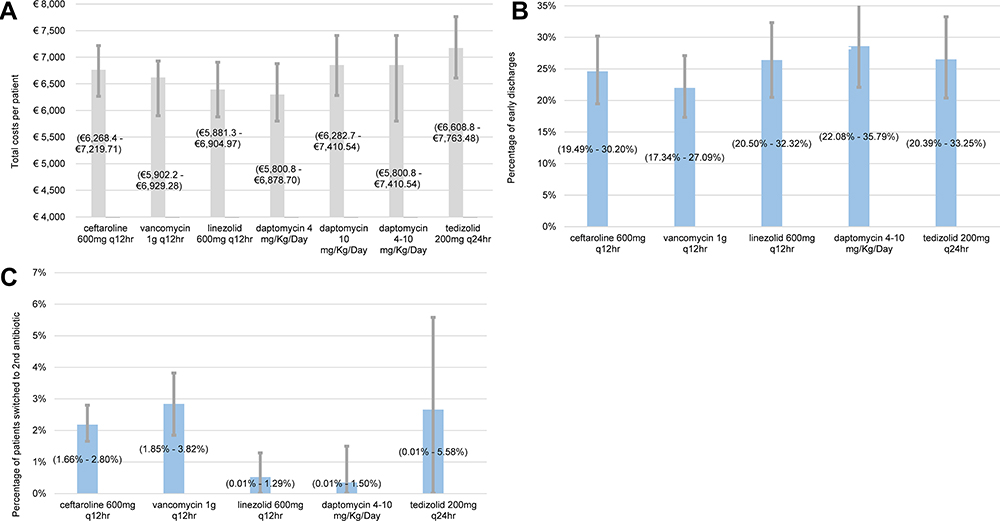 |
Figure 2 cSSTI analysis—total costs per patient (A), percentage of early discharges (B) and percentage of patients switched to 2nd line antibiotic (C) predicted by the model (based on 1,000 simulations – 95% confidence intervals estimates provided). Abbreviations: q12hr, every 12 hours; q24hr, every 24 hours. |
Furthermore, the results demonstrated that the antibiotic costs account for a limited proportion of total costs (6%–17%), with hospital costs being the largest component of the total costs (>83%), as shown in Figure 3. Specifically, hospitalization costs were €6,086, €6,261, €5,919, €5,786, and €5,999, respectively, while initial antibiotic therapy costs were €676, €79, €403, €556 (€442–€998 depending on the dosage) and €1,103 for CFT, vancomycin, linezolid, daptomycin, and tedizolid, respectively. The monitoring costs were relatively large for vancomycin, (€225), while all other treatments had limited monitoring costs (<€18). Similarly, the costs of gram negative pairing were limited across comparators (€52–€54).
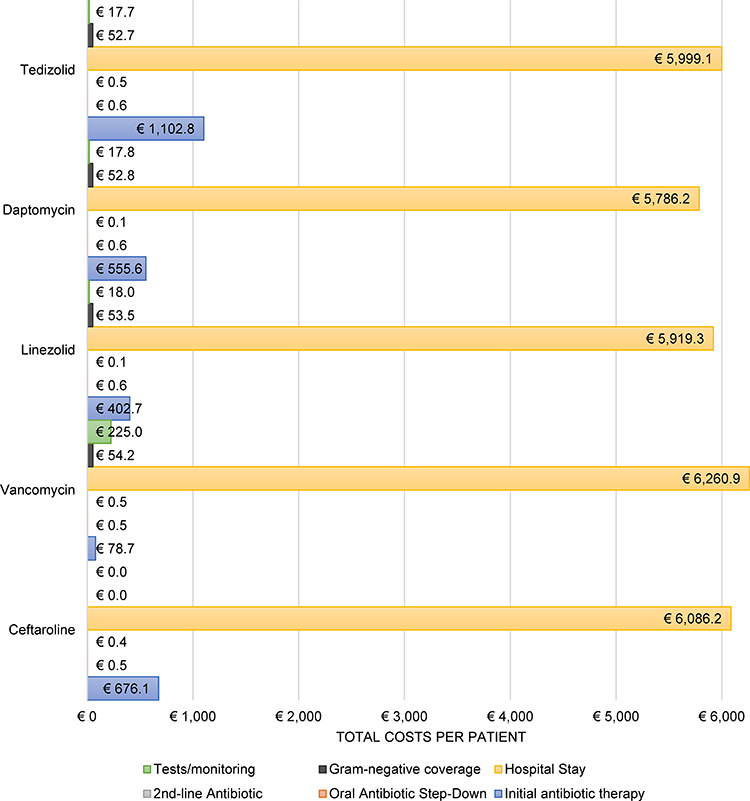 |
Figure 3 Detailed costs predicted by the model for cSSTI. Abbreviation: cSSTI, complicated skin and soft tissue infection. |
The percentage of patients discharged early (Day 3) ranged between 17%–35% resulting in longer hospitalization for more than 65%–83% of the patients starting empiric antibiotic treatment, as summarized in Figure 2B.
Simulating an increased dosage for daptomycin 4–10mg/kg/day, cloxacillin 1–2g/q4-6hr and aztreonam 2g q8hr to mimic the dosages commonly used in clinical practice, had a limited effect on the overall predicted costs with <10% differences, despite the increase in initial antibiotic costs associated with the higher dosages. This is because the initial antibiotic costs account for 6%–17% of the overall costs, as described in the previous paragraph (see also Figure 3).
Finally, the deterministic sensitivity analysis (DSA) demonstrated that the probability of early (Day 3) response, the duration of antibiotic treatment and the LOS in the hospital are the main determinants of total costs, as shown in Figure 4 for CFT with respect to vancomycin. Similar results were obtained when the DSA was performed for CFT versus the other comparators.
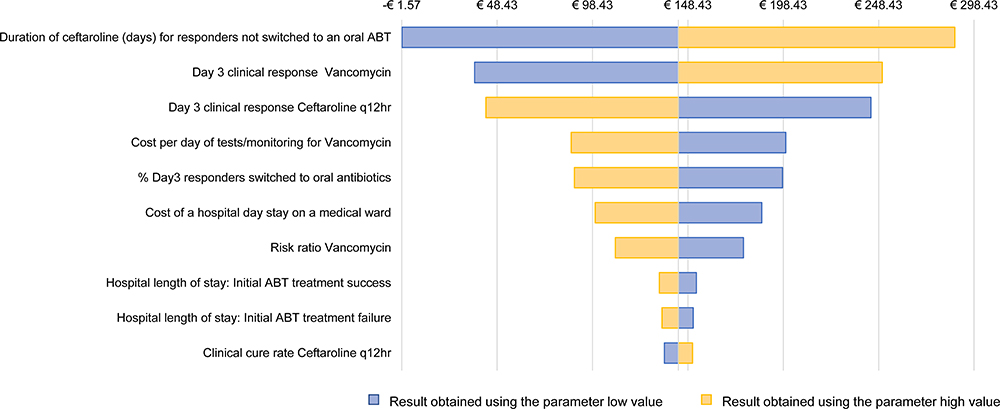 |
Figure 4 Tornado diagram showing, in decreasing order, the key parameters that generated the most variation in the total incremental cost per patient, when comparing ceftaroline fosamil with vancomycin. Abbreviation: cSSTI, complicated skin and soft tissue infection. |
Discussion
As described in the Introduction, selecting the right antibiotic for clinical experts remains highly challenging, especially in empiric settings.14 This analysis attempts to quantify the cost and consequences, from the Spanish NHS perspective, of using CFT or alternative antibiotics commonly used in hospitalized adults with cSSTI.
The model structure and analysis was built with the objective of comparing to agents with MRSA activity, based on available guidelines,25–28 expert opinion, and microbiological activity of ceftaroline fosamil, noting that MRSA cannot be ruled out in the empirical treatment of cSSTI. The current model does capture step down 1) for patients responding at Day 3 and eligible for switch to oral antibiotic and early discharge or 2) for non-responders switching to a second-line antibiotic. Adaptation of the antibiotic once the culture is positive (methicillin-susceptible Staphylococcus aureus [MSSA] or polymicrobial) was not considered in the model because, after discussion with clinical experts, the microbiology results might not be readily available in clinical practice, thus patients are treated according to risk factors for having MRSA. Therefore, this analysis can be considered as a pessimistic scenario for the overall costs of treating MRSA-suspected infections, since availability of microbiology results would allow a significant proportion of patients (80% to 90% based on clinical experts) to be switched to a narrow-spectrum antibiotic (resulting in lower costs). Furthermore, in the cSSTI trials used to parametrize the model,19,31,32 MSSA and polymicrobial infections were included (approximately 27% to 55% of patients). Therefore, the trial-based clinical cure rates used in the economic analysis include patients with MRSA, MSSA, and polymicrobial infections.
The use of ceftaroline fosamil as a treatment option was associated with comparable percentage of early discharges and overall costs with respect to the comparators included in the analyses. In the base case, as summarized in Figure 3, CFT was associated with higher initial antibiotic therapy costs with respect to vancomycin and linezolid, comparable initial antibiotic therapy costs with daptomycin (depending on the dosage considered) and lower costs than tedizolid. The CFT cost difference with respect to vancomycin in initial antibiotic therapy was partially offset by reduced hospitalization costs and monitoring costs associated with CFT. Furthermore, as highlighted in Figure 2, the overlapping of the 95% CIs generated from the probabilistic sensitivity analyses (1,000 simulations) highlighted the similarity with respect to total costs per patients and PDE with CFT as with the other antibiotics considered in the analysis.
The DSA highlighted that the most influential parameters of overall treatment costs are early response, the duration of antibiotic treatment and the duration of hospitalization, which is consistent with previous reports for cSSTI.9 This could suggest shifting the payers’ attention towards the overall economic burden of managing patients hospitalized with cSSTI rather than focusing on pharmacy spend alone.
As presented in Table 1, the clinical cure rate used in the analysis for CFT (91.6%) was derived from a pooled analysis of the two phase III RCTs CANVAS 1 and CANVAS 2, in the clinically evaluable (CE) population.19 A more recent systematic review and meta-analysis of CFT trials estimated CFT clinical cure rate of 89.6% in the CE population.34 However, this meta-analysis also included CFT 600mg q8hr (not considered in the current analysis) and a CFT open-label study, thus focusing on CFT 600mg q12hr double blinded RCTs was preferred. Furthermore, this ensured consistency with the studies used for the network meta-analysis (NMA), from which comparative effectiveness was derived.
One key study limitation is that most of the included comparators evidence was not obtained from head to head clinical trials between the comparator and CFT. Therefore the clinical inputs needed to parametrize the model were sourced from either an indirect comparison (NMA) or directly from the available literature and validated by discussion with clinical experts.30 Two alternative NMA studies available in the literature were not used, for the clinical cure rate inputs, either because only considering CFT Phase 2 trial in the network of evidence35 or because the study was not available at the time of this analysis.36 Nevertheless, a comparison with the current analysis inputs (Table 1) and the two alternative NMAs identified is provided. McCool et al35 odds ratios of each comparator considered vs tedizolid for clinical response at test-of-cure were extracted (from Table 2 of the publication) and converted in risk ratios vs CFT using tedizolid clinical cure rate of 87% as anchor (same cure rate for tedizolid as in the current analysis – see Table 1). The resulting risk ratios derived from McCool et al35 are relatively comparable with the current analysis inputs for CFT vs vancomycin (1.00 vs 1.08), linezolid (0.94 vs 1.00), daptomycin (0.94 vs 1.05) and tedizolid (1.05 vs 1.00). However, it is important to highlight that using McCool et al35 estimates would have resulted in a more favorable analysis for CFT vs vancomycin, linezolid and daptomycin, with only tedizolid risk ratio being lower (1.00) than what used in the current analysis (1.05). A similar comparison was performed based on Vlachaki et al 2021 NMA results,36 with the odds ratios of each comparator vs delafloxacin for composite clinical response extracted (from Figure 3 of the publication) and converted in risk ratios vs CFT using delafloxacin clinical cure rate of 87.2% as anchor (from delafloxacin Phase III trial37). The risk ratios derived from Vlachaki et al36 are relatively comparable with the current analysis inputs for CFT vs vancomycin (1.00 vs 1.00), linezolid (0.94 vs 1.04), daptomycin (0.94 vs 1.00) and tedizolid (1.05 vs 1.04). Similarly to McCool et al35 comparison, it is important to highlight that using Vlachaki et al36 estimates would have resulted in a more favorable analysis for CFT vs linezolid and vancomycin.
Multiple additional limitations need to be acknowledged for the developed model. Firstly, inclusion of cloxacillin in the base case analysis was not possible, given the significant differences in the definition of early response (Day 3) between cloxacillin and CFT clinical evidence. Secondly, treatment related serious AEs (SAEs) were not considered in the economic analysis given the relative low incidence and the similarity of SAEs across comparators.31,32,38–40 Therefore, this limitation is unlikely to have a strong impact on the incremental differences between the comparators considered. Thirdly, the duration of antibiotic treatment has been assumed equivalent between CFT and the other antibiotic treatments (see Table 1), given the lack of treatment specific inputs available in the literature. Since the duration of antibiotic treatment was one of the key drivers of total costs in the DSA, it might be of interest to include in the analysis treatment duration specific to each antibiotic, when these estimates will become available from real-world evidence studies. Fourthly, the antibiotic dosages used in the clinical trials may differ from those used in routine clinical practice. Therefore, multiple scenarios with increased antibiotic dosage but same clinical efficacy were evaluated, with the increase in antibiotic dosage having a limited impact on the overall model outcomes and conclusions. Fifthly, susceptibility rates were not considered into the analysis, which might be a critical factor in countries with high levels of emerging antibiotic resistance.14,25 Specifically, different type of causative organisms (eg, Staphylococcus aureus) might affect differently the clinical efficacy of each antibiotic considered in the analysis. While modeling this aspect would require country-specific susceptibility patterns and clinical inputs stratified by causative organism, this could be of significant interest to fully capture the economic benefit of newer antibiotics such as ceftaroline fosamil. Finally, while the impact of antibiotic resistance has not been included in the current analysis, as detailed above, ceftaroline fosamil should be used in accordance with antimicrobial stewardship, as with all antibacterial agents. Furthermore, while the presented analysis focused on the current relevant treatment options from the perspective of the Spanish National Health System, new approved dosages in the future and antibiotic resistance patterns will dictate modified cost-benefit results.
While the economic analysis has limitations, as discussed above, it also as strengths which make it relevant to the Spanish NHS for inpatient treatment of cSSTI. Specifically, all key antibiotic treatments relevant for the Spanish decision problem were considered, the analysis was based on efficacy estimates derived from Phase III RCTs, which provide the largest sample size, and comparative effectiveness within the same RCT for CFT vs vancomycin was used. In addition, the results are presented probabilistically (over 1,000 simulations) to account for uncertainty in the mean estimates. Finally, the model structure used in the analysis is common to other economic models previously published in cSSTI21,22 and in other types of infections, such as treatment for bacteremia,23 community acquired pneumonia,41 urinary tract infections,42 persistent febrile neutropenia,43 hospitalized influenza and intra-abdominal infections.44 This is due to the common clinical pathways observed across different types of infections where resolution of signs and symptoms occur over a relatively short period of time. The chosen model structure allowed to focus on early response and treatment failure with consequent switch to 2nd line, given the importance of these two aspects in clinical practice.45
Conclusion
The model results support CFT being a valid choice for cSSTI empiric therapy providing comparable percentage of early discharged patients and costs as the other commonly used antibiotics considered. Furthermore, the model results demonstrate that early response and duration of antibiotic treatment are the key drivers of total costs of managing cSSTI, with hospital costs accounting for over 83% of the total expenditures.
Availability of additional data quantifying the average treatment duration specific to each antibiotic treatment and extension of the model structure to account for switch due to microbiology availability are currently under consideration for extending and strengthening the current analysis.
Data Sharing Statement
Upon request, and subject to certain criteria, conditions and exceptions see (https://www.pfizer.com/science/clinical-trials/trial-data-and-results for more information), Pfizer will provide access to individual de-identified participant data from Pfizer-sponsored global interventional clinical studies conducted for medicines, vaccines and medical devices (1) for indications that have been approved in the US and/or EU or (2) in programs that have been terminated (ie, development for all indications has been discontinued). Pfizer will also consider requests for the protocol, data dictionary, and statistical analysis plan. Data may be requested from Pfizer trials 24 months after study completion. The de-identified participant data will be made available to researchers whose proposals meet the research criteria and other conditions, and for which an exception does not apply, via a secure portal. To gain access, data requestors must enter into a data access agreement with Pfizer.
Acknowledgments
Julia Donnelly (on behalf of Evidera) for medical writing assistance. This paper was presented at the International Society for Pharmacoeconomics and Outcomes Research Europe Congress, 10–14 November 2018, Barcelona, Spain as a poster presentation with interim findings. The poster’s abstract reference is Soriano et al. ”PIN63 - A COST-MINIMIZATION MODEL TO EVALUATE THE IMPACT OF CEFTAROLINE FOSAMIL FOR THE TREATMENT OF COMPLICATED SKIN AND SOFT TISSUE INFECTIONS IN HOSPITALIZED ADULTS IN SPAIN.” Value in Health 21: S231.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by Pfizer. Evidera received consulting fees from Pfizer for undertaking this economic analysis.
Disclosure
A.S reports grants, personal fees from Pfizer, during the conduct of the study; personal fees and/or grants from MSD, Shionogi, Angelini, Gilead, and Menarini, outside the submitted work. S.R (an employee of Evidera) and E.R (a former employee of Evidera), were paid consultants to Pfizer in connection with the study and the development of this manuscript.
MK, CP, CC, WA, JH are employees of and shareholders in Pfizer. M.W received research funding and consultancy payments from Pfizer for infection topics that are not directly related to this manuscript. The authors report no other conflicts of interest in this work.
References
1. Christensen KL, Holman RC, Steiner CA, Sejvar JJ, Stoll BJ, Schonberger LB. Infectious disease hospitalizations in the United States. Clin Infect Dis. 2009;49(7):1025–1035. doi:10.1086/605562
2. Suk JE, Semenza JC. Future infectious disease threats to Europe. Am J Public Health. 2011;101(11):2068–2079. doi:10.2105/AJPH.2011.300181
3. Seaton RA, Johal S, Coia JE, Reid N, Cooper S, Jones BL. Economic evaluation of treatment for MRSA complicated skin and soft tissue infections in Glasgow hospitals. Eur J Clin Microbiol Infect Dis. 2014;33(3):305–311. doi:10.1007/s10096-013-1956-z
4. Ostermann H, Blasi F, Medina J, Pascual E, McBride K, Garau J. Resource use in patients hospitalized with complicated skin and soft tissue infections in Europe and analysis of vulnerable groups: the REACH study. J Med Econ. 2014;17(10):719–729. doi:10.3111/13696998.2014.940423
5. Tun K, Shurko JF, Ryan L, Lee GC. Age-based health and economic burden of skin and soft tissue infections in the United States, 2000 and 2012. PLoS One. 2018;13(11):e0206893–e0206893. doi:10.1371/journal.pone.0206893
6. Kollef MH. Broad-spectrum antimicrobials and the treatment of serious bacterial infections: getting it right up front. Clin Infect Dis. 2008;47(Suppl 1):S3–S13. doi:10.1086/590061
7. Lipsky BA, Napolitano LM, Moran GJ, et al. Economic outcomes of inappropriate initial antibiotic treatment for complicated skin and soft tissue infections: a multicenter prospective observational study. Diagn Microbiol Infect Dis. 2014;79(2):266–272. doi:10.1016/j.diagmicrobio.2014.02.013
8. Lipsky BA, Weigelt JA, Gupta V, Killian A, Peng MM. Skin, soft tissue, bone, and joint infections in hospitalized patients: epidemiology and microbiological, clinical, and economic outcomes. Infect Control Hosp Epidemiol. 2007;28(11):1290–1298. doi:10.1086/520743
9. Tarricone R, Aguzzi G, Capone A, et al. How complicated skin and soft tissue infections are treated in Italy: economic evaluation of inpatient intravenous antibiotic treatment in seven hospitals. J Med Econ. 2008;11(2):265–279. doi:10.3111/13696990802113196
10. Dryden MS. Complicated skin and soft tissue infection. J Antimicrob Chemother. 2010;65(Suppl 3):iii35–iii44. doi:10.1093/jac/dkq302
11. Suaya JA, Mera RM, Cassidy A, et al. Incidence and cost of hospitalizations associated with Staphylococcus aureus skin and soft tissue infections in the United States from 2001 through 2009. BMC Infect Dis. 2014;14:296. doi:10.1186/1471-2334-14-296
12. Zervos MJ, Freeman K, Vo L, et al. Epidemiology and outcomes of complicated skin and soft tissue infections in hospitalized patients. J Clin Microbiol. 2012;50(2):238–245. doi:10.1128/JCM.05817-11
13. Nathwani D, Dryden M, Garau J. Early clinical assessment of response to treatment of skin and soft-tissue infections: how can it help clinicians? Perspectives from Europe. Int J Antimicrob Agents. 2016;48(2):127–136. doi:10.1016/j.ijantimicag.2016.04.023
14. Pulido-Cejudo A, Guzman-Gutierrez M, Jalife-Montano A, et al. Management of acute bacterial skin and skin structure infections with a focus on patients at high risk of treatment failure. Ther Adv Infect Dis. 2017;4(5):143–161. doi:10.1177/2049936117723228
15. Garau J, Ostermann H, Medina J, et al. Current management of patients hospitalized with complicated skin and soft tissue infections across Europe (2010–2011): assessment of clinical practice patterns and real-life effectiveness of antibiotics from the REACH study. Clin Microbiol Infect. 2013;19(9):E377–385. doi:10.1111/1469-0691.12235
16. Friedland HD, O’Neal T, Biek D, et al. CANVAS 1 and 2: analysis of clinical response at day 3 in two Phase 3 trials of ceftaroline fosamil versus vancomycin plus aztreonam in treatment of acute bacterial skin and skin structure infections. Antimicrob Agents Chemother. 2012;56(5):2231–2236. doi:10.1128/AAC.05738-11
17. Garau J, Blasi F, Medina J, McBride K, Ostermann H; group Rs. Early response to antibiotic treatment in European patients hospitalized with complicated skin and soft tissue infections: analysis of the REACH study. BMC Infect Dis. 2015;15:78. doi:10.1186/s12879-015-0822-2
18. Edelsberg J, Berger A, Weber DJ, Mallick R, Kuznik A, Oster G. Clinical and economic consequences of failure of initial antibiotic therapy for hospitalized patients with complicated skin and skin-structure infections. Infect Control Hosp Epidemiol. 2008;29(2):160–169. doi:10.1086/526444
19. Corey GR, Wilcox M, Talbot GH, et al. Integrated analysis of CANVAS 1 and 2: phase 3, multicenter, randomized, double-blind studies to evaluate the safety and efficacy of ceftaroline versus vancomycin plus aztreonam in complicated skin and skin-structure infection. Clin Infect Dis. 2010;51(6):641–650. doi:10.1086/655827
20. Karve S, Hackett J, Levinson J, Gibson E, Battersby A. Ceftaroline fosamil treatment outcomes compared with standard of care among hospitalized patients with complicated skin and soft tissue infections. J Comp Eff Res. 2016;5(4):393–405. doi:10.2217/cer-2015-0024
21. Athanasakis K, Petrakis I, Ollandezos M, et al. Antibacterial treatment of methicillin-resistant Staphylococcus aureus complicated skin and soft tissue infections: a cost and budget impact analysis in Greek hospitals. Infect Dis Ther. 2014;3(2):257–268. doi:10.1007/s40121-014-0044-8
22. Schurmann D, Sorensen SV, De Cock E, Duttagupta S, Resch A. Cost-effectiveness of linezolid versus vancomycin for hospitalised patients with complicated skin and soft-tissue infections in Germany. Eur J Health Econ. 2009;10(1):65–79. doi:10.1007/s10198-008-0104-7
23. Grau S, Mateu-de Antonio J, Soto J, Marin-Casino M, Salas E. Pharmacoeconomic evaluation of linezolid versus teicoplanin in bacteremia by Gram-positive microorganisms. Pharm World Sci. 2005;27(6):459–464. doi:10.1007/s11096-005-1638-8
24. Bounthavong M, Zargarzadeh A, Hsu DI, Vanness DJ. Cost-effectiveness analysis of linezolid, daptomycin, and vancomycin in methicillin-resistant Staphylococcus aureus: complicated skin and skin structure infection using bayesian methods for evidence synthesis. Value in Health. 2011;14(5):631–639. doi:10.1016/j.jval.2010.12.006
25. Bassetti M, Baguneid M, Bouza E, Dryden M, Nathwani D, Wilcox M. European perspective and update on the management of complicated skin and soft tissue infections due to methicillin-resistant Staphylococcus aureus after more than 10 years of experience with linezolid. Clin Microbiol Infect. 2014;20(Suppl 4):3–18. doi:10.1111/1469-0691.12463
26. Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the infectious diseases society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis. 2011;52(3):e18–55.
27. Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft-tissue infections. Clin Infect Dis. 2005;41(10):1373–1406. doi:10.1086/497143
28. Leong HN, Kurup A, Tan MY, Kwa ALH, Liau KH, Wilcox MH. Management of complicated skin and soft tissue infections with a special focus on the role of newer antibiotics. Infect Drug Resist. 2018;11:1959–1974.
29. Talbot GH, O’Neal T, Das AF, Thye D. Prospective study of the Wilson severity-of-illness scoring system for complicated skin and skin structure infections. Antimicrob Agents Chemother. 2013;57(1):647–650. doi:10.1128/AAC.01344-12
30. Rao N, Gibson E, Lawson R, et al. ZinforoTM (ceftaroline fosamil) versus other empiric initial IV antibiotics for complicated skin and soft tissue infections.
31. Moran GJ, Fang E, Corey GR, Das AF, De Anda C, Prokocimer P. Tedizolid for 6 days versus linezolid for 10 days for acute bacterial skin and skin-structure infections (ESTABLISH-2): a randomised, double-blind, phase 3, non-inferiority trial. Lancet Infect Dis. 2014;14(8):696–705. doi:10.1016/S1473-3099(14)70737-6
32. Prokocimer P, De Anda C, Fang E, Mehra P, Das A. Tedizolid phosphate vs linezolid for treatment of acute bacterial skin and skin structure infections: the ESTABLISH-1 randomized trial. JAMA. 2013;309(6):559–569. doi:10.1001/jama.2013.241
33. Kauf TL, McKinnon P, Corey GR, et al. An open-label, pragmatic, randomized controlled clinical trial to evaluate the comparative effectiveness of daptomycin versus vancomycin for the treatment of complicated skin and skin structure infection. BMC Infect Dis. 2015;15:503. doi:10.1186/s12879-015-1261-9
34. Lan S-H, Chang S-P, Lai -C-C, Lu L-C, Chao C-M. Ceftaroline efficacy and safety in treatment of complicated skin and soft tissue infection: a systemic review and meta-analysis of randomized controlled trials. J Clin Med. 2019;8(6):776. doi:10.3390/jcm8060776
35. McCool R, Gould IM, Eales J, et al. Systematic review and network meta-analysis of tedizolid for the treatment of acute bacterial skin and skin structure infections caused by MRSA. BMC Infect Dis. 2017;17(1):39. doi:10.1186/s12879-016-2100-3
36. Vlachaki I, Vacchelli M, Zinzi D, et al. Comparative efficacy of delafloxacin for complicated and acute bacterial skin and skin structure infections: results from a network meta-analysis. BMC Infect Dis. 2021;21(1):1036. doi:10.1186/s12879-021-06736-x
37. O’Riordan W, McManus A, Teras J, et al. A comparison of the efficacy and safety of intravenous followed by oral delafloxacin with vancomycin plus aztreonam for the treatment of acute bacterial skin and skin structure infections: a phase 3, multinational, double-blind, randomized study. Clin Infect Dis. 2018;67(5):657–666. doi:10.1093/cid/ciy165
38. Corrado ML. Integrated safety summary of CANVAS 1 and 2 trials: Phase III, randomized, double-blind studies evaluating ceftaroline fosamil for the treatment of patients with complicated skin and skin structure infections. J Antimicrob Chemother. 2010;65(Suppl 4):iv67–iv71. doi:10.1093/jac/dkq256
39. Arbeit RD, Maki D, Tally FP, Campanaro E, Eisenstein BI. The safety and efficacy of daptomycin for the treatment of complicated skin and skin-structure infections. Clin Infect Dis. 2004;38(12):1673–1681. doi:10.1086/420818
40. Konychev A, Heep M, Moritz RK, et al. Safety and efficacy of daptomycin as first-line treatment for complicated skin and soft tissue infections in elderly patients: an open-label, multicentre, randomized phase IIIb trial. Drugs Aging. 2013;30(10):829–836. doi:10.1007/s40266-013-0114-8
41. Martin M, Quilici S, File T, Garau J, Kureishi A, Kubin M. Cost-effectiveness of empirical prescribing of antimicrobials in community-acquired pneumonia in three countries in the presence of resistance. J Antimicrob Chemother. 2007;59(5):977–989. doi:10.1093/jac/dkm033
42. Bosmans JE, Coupé VM, Knottnerus BJ, Geerlings SE, Moll van Charante EP, Ter Riet G. Cost-effectiveness of different strategies for diagnosis of uncomplicated urinary tract infections in women presenting in primary care. PLoS One. 2017;12(11):e0188818. doi:10.1371/journal.pone.0188818
43. Martín-Peña A, Gil-Navarro MV, Aguilar-Guisado M, et al. Cost-effectiveness analysis comparing two approaches for empirical antifungal therapy in hematological patients with persistent febrile neutropenia. Antimicrob Agents Chemother. 2013;57(10):4664–4672. doi:10.1128/AAC.00723-13
44. Kongnakorn T, Eckmann C, Bassetti M, et al. Cost-effectiveness analysis comparing ceftazidime/avibactam (CAZ-AVI) as empirical treatment comparing to ceftolozane/tazobactam and to meropenem for complicated intra-abdominal infection (cIAI). Antimicrob Resist Infect Control. 2019;8:204. doi:10.1186/s13756-019-0652-x
45. Bassetti M, Montero JG, Paiva JA. When antibiotic treatment fails. Intensive Care Med. 2018;44(1):73–75. doi:10.1007/s00134-017-4962-2
46. File, Jr TM
47. Botplusweb.portalfarma.com. BOT Plus 2. Base de Datos de Medicamentos [Internet]. Available from: https://botplusweb.portalfarma.com/botplus.aspx/.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.