")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 11
Catastrophic health expenditure of Vietnamese patients with gallstone diseases – a case for health insurance policy revaluation
Authors Tran BX, Tran TD, Nathan N , Ngo CQ , Nguyen LT, Nguyen LH , Nguyen HLT, Nguyen CT, Do HP, Nguyen THT, Tran TT , Thai TPT, Dang AK, Nguyen NB, Latkin CA , Ho CSH , Ho RCM
Received 18 October 2018
Accepted for publication 16 January 2019
Published 11 February 2019 Volume 2019:11 Pages 151—158
DOI https://doi.org/10.2147/CEOR.S191379
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Bach Xuan Tran,1,2,* Tho Dinh Tran,3,* Nila Nathan,4 Chau Quy Ngo,5 Loi Thi Nguyen,6 Long Hoang Nguyen,7 Huong Lan Thi Nguyen,8 Cuong Tat Nguyen,8 Huyen Phuc Do,7 Trang Huyen Thi Nguyen,9 Tung Thanh Tran,9 Thao Phuong Thi Thai,10,11 Anh Kim Dang,8 Nam Ba Nguyen,7 Carl A Latkin,2 Cyrus SH Ho,12 Roger CM Ho7,13
1Department of Health Economics, Institute for Preventive Medicine and Public Health, Hanoi Medical University, Hanoi, Vietnam; 2Department of Health, Behavior and Society, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, MD, USA; 3Department of Hepatobiliary Surgery, Vietnam-Germany Hospital, Hanoi, Vietnam; 4University of California, Santa Barbara, Santa Barbara, CA, USA; 5Department of Internal Medicine, Hanoi Medical University, Hanoi, Vietnam; 6Woolcock Institute of Medical Research Vietnam, Hanoi, Vietnam; 7Center of Excellence in Behavioral Medicine, Nguyen Tat Thanh University, Ho Chi Minh City, Vietnam; 8Institute for Global Health Innovations, Duy Tan University, Danang, Vietnam; 9Center of Excellence in Evidence-based Medicine, Nguyen Tat Thanh University, Ho Chi Minh City, Vietnam; 10Department of General Planning, Friendship Hospital, Hanoi, Vietnam; 11Department of Cardiology, Friendship Hospital, Hanoi, Vietnam; 12Department of Psychological Medicine, National University Hospital, Singapore; 13Department of Psychological Medicine, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
*These authors contributed equally to this work
Purpose: Despite gallstone diseases (GSDs) being a major public health concern with both acute and chronic episodes, none of the studies in Vietnam has been conducted to investigate the household expenditure for the GSD treatment. The objective of this study was to estimate the costs of managing GSD and to explore the prevalence and determinants of catastrophic health expenditure (CHE) among Vietnamese patients.
Materials and methods: A cross-sectional study was conducted from June 2016 to March 2017 in the Department of Hepatobiliary and Pancreatic Surgery, Viet Duc Hospital in Hanoi, Vietnam. A total of 206 patients were enrolled. Demographic and socioeconomic data, household income, and direct and indirect medical costs of patients seeking treatment for GSD were collected through face-to-face interview. Multivariate logistic regression was used to explore factors associated with CHE.
Results: The prevalence of CHE in patients suffering from GSD was 35%. The percentage of patients who were covered by health insurance and at risk for CHE was 41.2%, significantly higher than that of those noninsured (15.8%). Proportions of patients with and without health insurance who sought outpatient treatment were 30.6% and 81.6%, respectively. Patients who were divorced or widowed and had intrahepatic gallstones were significantly more likely to experience CHE. Those who were outpatients, were women, had history of pharmacological treatment to parasitic infection, and belong to middle and highest monthly household income quantile were significantly less likely to experience CHE.
Conclusion: The findings suggested that efforts to re-evaluate health insurance reimbursement capacity, especially for acute diseases and taking into account the varying preferences of people with different disease severity, should be conducted by health authority. Further studies concerning CHE of GSD in the context of ongoing health policy reform should consider utilizing WHO-recommended measures like the fairness in financial contribution index, as well as taking into consideration the behavioral aspects of health care spending.
Keywords: catastrophic health expenditure, gallstone, health insurance, out-of-pocket payments, Vietnam
Introduction
Gallstone disease (GSD) is a major public health concern worldwide, with disease prevalence in Europe amounting to 20% of the population and in the range of 2%–15% in Asia.1–4 In Vietnam, GSD is a common disease – the infected rate found through a number of community surveys ranged from 2.14% to 6.11%.5 The main cause of GSD in Vietnam, similar to other developing countries, has been found to be the parasitic infection. Treatment of GSD can be surgical, which include laparotomy and cholecystectomy, or nonsurgical like oral dissolution therapy, extracorporeal shock wave lithotripsy, and endoscopic sphincterotomy. Studies conducted in a range of countries have found that cost of surgery would be an issue for patients, even preventing them from getting the service. In Thailand, a study showed that patients with GSD were not able to afford surgical treatment and only 17% of patients went for surgical treatment.6 Other studies reported that patients with GSD from other developing countries in Asia such as Yemen and Pakistan faced similar difficulty to pay for high costs of surgical treatment.7,8 In the UK, researchers found that the largest proportion of the cost of managing GSD was contributed by surgery.9 There is, however, a paucity of information about the financial burden associated with GSD among Vietnamese.
In the past few decades, Vietnam has undergone rapid development that has contributed to the increase of health care expenditure. Health expenditure accounts for 7.1% of the Vietnam Gross Domestic Product (GDP) with total health expenditure per capita of US$ 142 in 2014.10 Although >80% of the Vietnamese population was covered by health insurance in 2017, thanks to the introduction of Law on Health Insurance and social health insurance for poor Vietnamese, elderly, and the ethnic minorities almost a decades ago, the out-of-pocket (OOP) payment of Vietnamese people still ranges from 50% to 70% of health expenditure.11,12 Heavy OOP for acute medical or surgical conditions can lead patients to pay a significant proportion of their income for treatment13 and result in catastrophic health expenditure (CHE). By definition, CHE occurs when the burden of OOP for health expenditure has reached a certain level that a household must forego expenditure on the needs of basic living in order to meet the medical or surgical expenses for a household member.14 CHE has been used to assess the financial burden of a population due to health care payment relative to the ability to pay.13 Vietnamese GSD patients, faced with potential CHE burden, can be said to be at risk of falling into a downward cycle of poverty and ill health.14
No study to our knowledge has studied CHE associated with GSD in Vietnam. Our study differs from previous studies on the determinants of CHE in Vietnam because we focused on a unique illness that could be asymptomatic for long period but suddenly present with acute cholecystitis, perforation of the gallbladder, and obstructive jaundice that require emergency treatment. Moreover, we believed that exploring the financial burden of GSD in Vietnam would give some useful suggestion for health policy and practices targeting patients of low- and middle-income countries, where the cause of disease differed significantly from that of developed countries. In our study, we explored GSD-related inpatient and outpatient costs, CHE due to GSD-related OOP, and the factors associated with CHE among GSD patients in Vietnam.
Materials and methods
Study setting
A cross-sectional study was conducted from June 2016 to March 2017 in the Viet Duc Hospital, Hanoi, the capital of Vietnam. Hanoi contains urban, rural, and mountainous areas. The population of Hanoi is 7.6 million, and the GDP is 3,500 US$ per capita. The health insurance coverage for Vietnamese is 84%.12 The sociodemographic characteristics of the population in Hanoi are diverse, which typically reflect the sociodemographic characteristics in other provinces in Vietnam. The Viet Duc Hospital is a central hospital that provides care to patients from Hanoi and other provinces. As the largest central hospital for surgical treatment and final destination for patient referrals from lower level health facilities, the GSD cases presented at Viet Duc Hospital are typical of diverse types and at more severe stages.
Study sample and data collection
All patients suffering from GSD aged over 18 years, with the capacity to provide informed consent and ability to complete a self-reported questionnaire, were eligible for this study. Patients who were handicapped or could not communicate were excluded.
A face-to-face interview was conducted using a structured questionnaire. The questionnaire had 35 items consisting of four parts: 1) demographic and socioeconomic data; 2) health care costs; 3) their ability to pay; 4) clinical characteristics such as the position of gallstones and type of treatment received. The demographic characteristics included age, educational attainment, employment status, gender, total household income and expenditures, and marital and health insurance status. The household income was separated into five quintiles from the poorest, poor, middle, rich, and richest. Meanwhile, the household expenditure included recurring spending in the past 30 days (for food, education, utility, etc) and nonrecurring spending in the past 12 months (for health care, construction, etc). Each interview lasted ~15–20 minutes.
Data collectors were well-trained students with Master in Public Health and undergraduate medical students at the Hanoi Medical University. Patients who met the inclusion criteria were invited to a private counseling room to ensure their confidentiality with the pleasant atmosphere.
Variables
Treatment costs were self-reported by patients and then categorized into direct and indirect costs. The direct costs consisted of medical and nonmedical costs.15 The direct medical costs included medication, hospitalization cost, outpatient consultation fee, inpatient and outpatient treatment, and costs of investigation and surgery. We asked patients to report how much they had to pay for each category (ie, OOP). Direct nonmedical costs included travel expenses, cost of meals, and accommodation per hospital-day and clinic visit.16 The indirect costs included loss of income by patients and caregivers, which were based on length of hospitalization and medical leave as well as personal salary per hour.17 All the cost data were collected in Vietnamese Dongs, and the final figures were presented in US dollars, where 22,700 VND =1 US$, at the conversion rate in 2017. We also estimated the ability to pay by asking patients to report whether they fully or partially paid or were unable to pay for the GSD-related fees.
In order to estimate the CHE due to GSD, we computed the following variables:
- The total of OOP due to GSD by summing expenditures incurred in the hospital, surgery, and medicines and other expenditures incurred by patients, family members for transportation, accommodation, and meals that were not reimbursed through other health finance channels.18
- Household’s consumption expenditure in the last 12 months = total recurring expenses × 12 + total nonrecurring expenses19
- Household’s subsistence spending: the minimum expenses to ensure fundamental life in a society (ie, expense for food).19
- Household’s capacity to pay = the total household’s consumption expenditure – household’s subsistence spending (ie, food expenditure)19
- CHE is defined as the value of OOP reached 40% or more of a household’s capacity to pay within the past 1 year.19,20
Statistical analysis
Data analysis was performed using Stata version 13.0 (StataCorp LP, College Station, TX, USA). The data on socioeconomic status, health care cost, and ability to pay for inpatient and outpatient services were presented. The chi-squared test, Fisher’s exact test, and Mann–Whitney test were used to explore the differences in proportions and means between patients with and without health insurance. Logistic regression was used to determine factors associated with CHE. In this study, we applied a stepwise backward selection strategy, which excluded variables having the P-value of the log likelihood test of >0.2, to produce a final reduced regression model. The exploratory variables were selected in the previous publication on CHE.15,18 Independent variables included demographic and clinical variables. Demographic variables included age, gender, marital status, and education background. Clinical variables included location of gallstones, type of treatment, location of treatment setting, and history of parasitic infection. A P-value <0.05 was considered to be statistically significant.
Ethics approval
This study was approved by the Institutional Ethics Committee of the Hanoi Medical University and Viet Duc Hospital. An informed written consent was obtained from all participants. The participants could refuse to participate at any time without any impact on their treatments. This study was conducted in accordance with the Declaration of Helsinki.
Results
Characteristics of participants
There were 210 patients who suffered from GSD eligible to participate in this study. Out of these, four did not wish to participate. Thus, a total of 206 patients with GSD were included in the study. A total of 127 patients (61.7%) were women, 118 (57.3%) were inpatients, 171 patients (83%) stayed with their spouses or partners, 113 patients (54.9%) had no formal or primary school education, and 55 patients (35%) experienced CHE. Table 1 compares the demographics between patients with and without health insurance. Significantly, the higher proportion of patients without health insurance sought outpatient treatment (81.6%) compared with patients covered by health insurance (30.6%) (P<0.05). The higher proportion of patients with health insurance (41.2%) experienced CHE compared with patients not covered by health insurance (15.8%) (P<0.05) (Table 1).
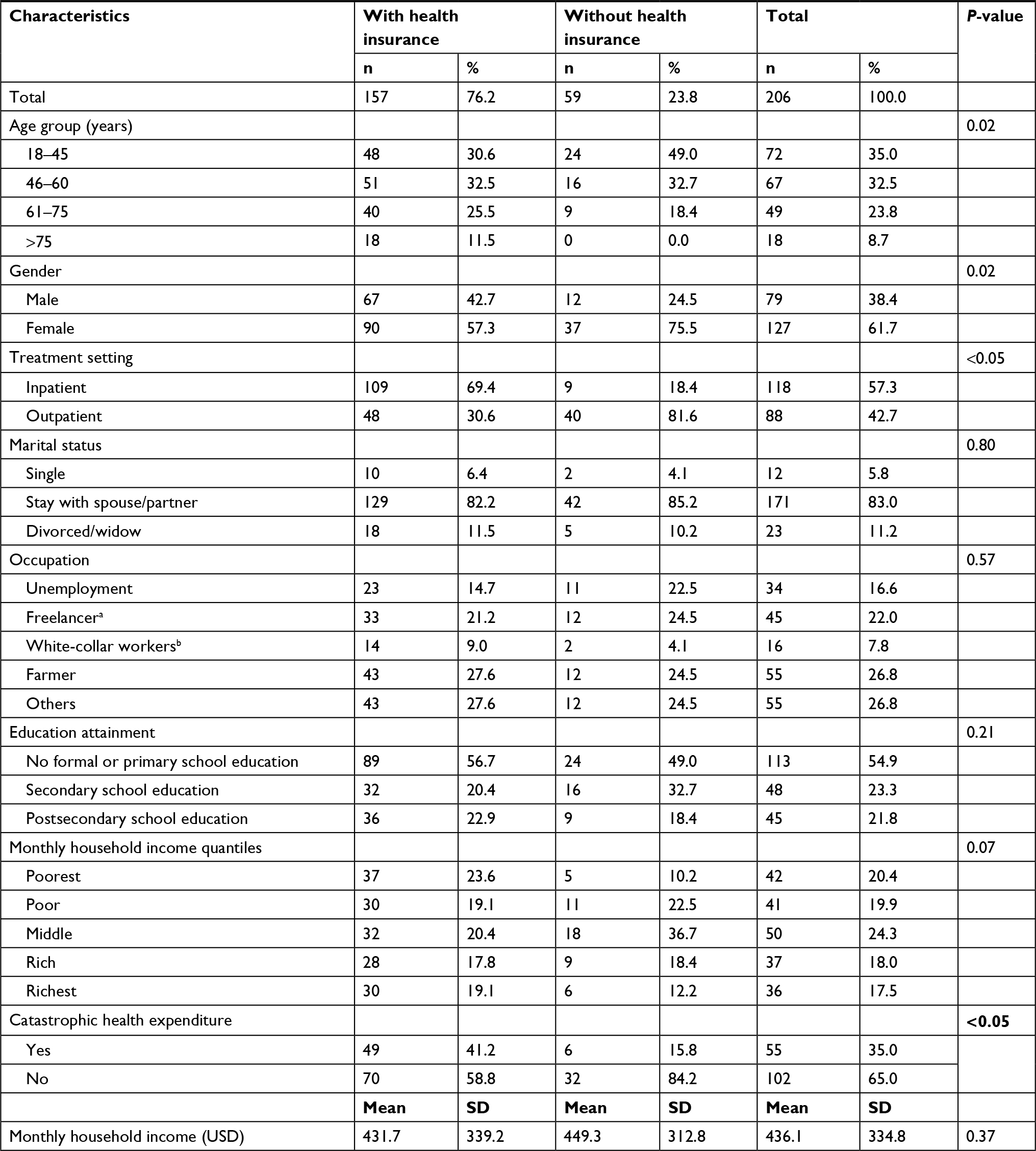 | Table 1 Comparison of demographic characteristics between patients with and without health insurance Notes: aFreelancers: those working without the formal labor contract. bWhite-collar workers: those with office or administrative jobs. Exchange rate: 22,700 VND =1 US$ (2017). |
Table 2 compares the illness and treatment characteristics between patients with and without health insurance. The most frequent location of gallstone was in the gallbladder (37.9%). The most common type of treatment was surgery (60.2%). Majority of patients did not have the history of parasitic infection in the biliary system (71.4%). Significantly, higher proportion of patients without health insurance had gallstones in the gallbladder (57.1% vs 31.9%, P<0.05), no treatment (42.9% vs 14.7%, P<0.05), pharmacological treatment (36.7% vs 16.6%, P<0.05), and other treatments (10.2% vs 0.6%, P<0.05) compared with patients covered by health insurance. In contrast, higher proportion of patients with health insurance received surgery (71.3% vs 24.5%) than those without health insurance (P>0.05).
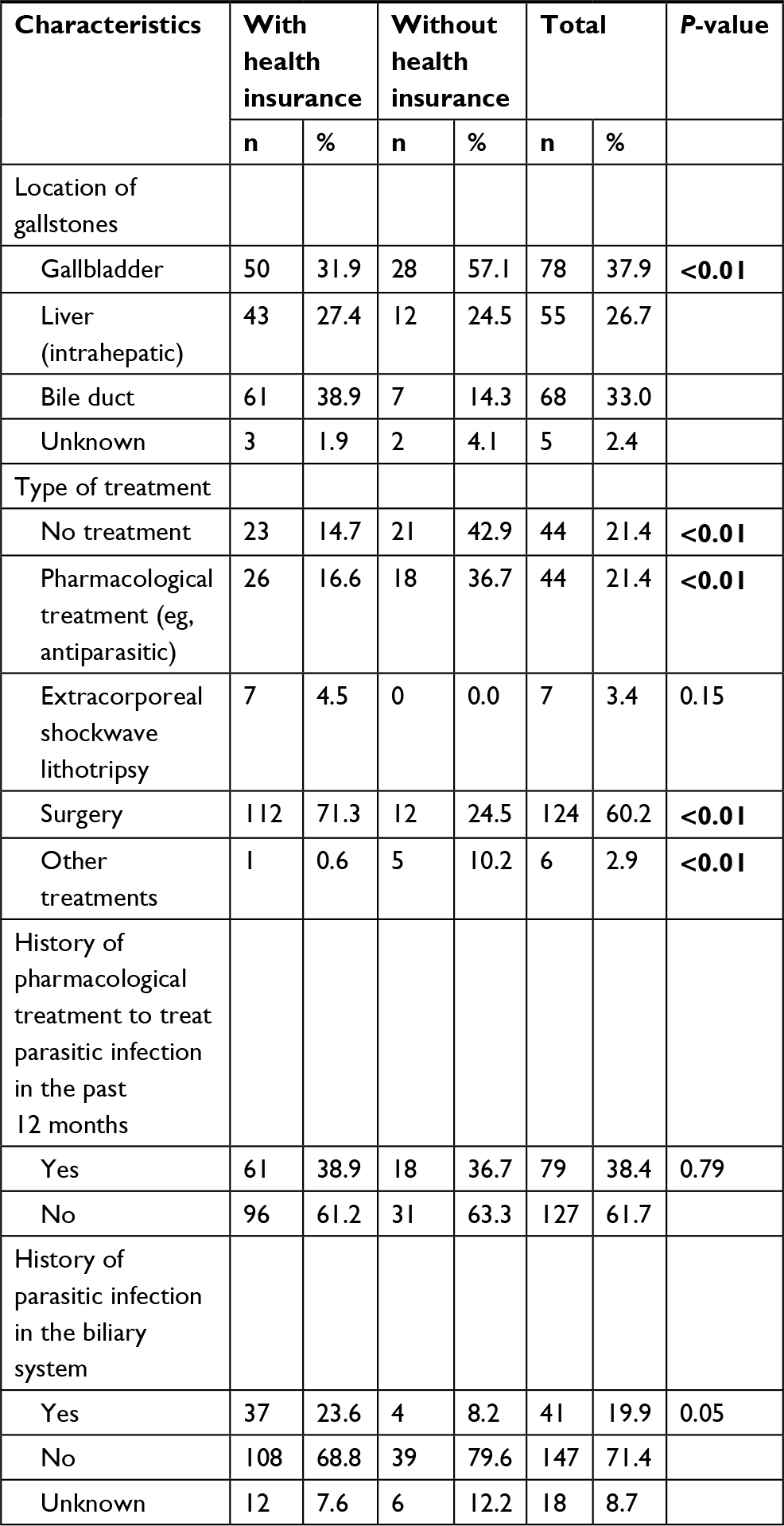 | Table 2 Comparison of illness and treatment characteristics between patients with and without health insurance |
Table 3 describes inpatient and outpatient costs of patients with GSDs. The total medical cost for inpatients was US$ 1,207.0 (SD =748.9), while the total outpatient medical cost was US$ 90.7 (SD =107.5). The majority of inpatients were able to pay partially for the inpatient medical costs (55.3%), while most of the outpatients were able to pay fully for the outpatient medical costs (71.4%).
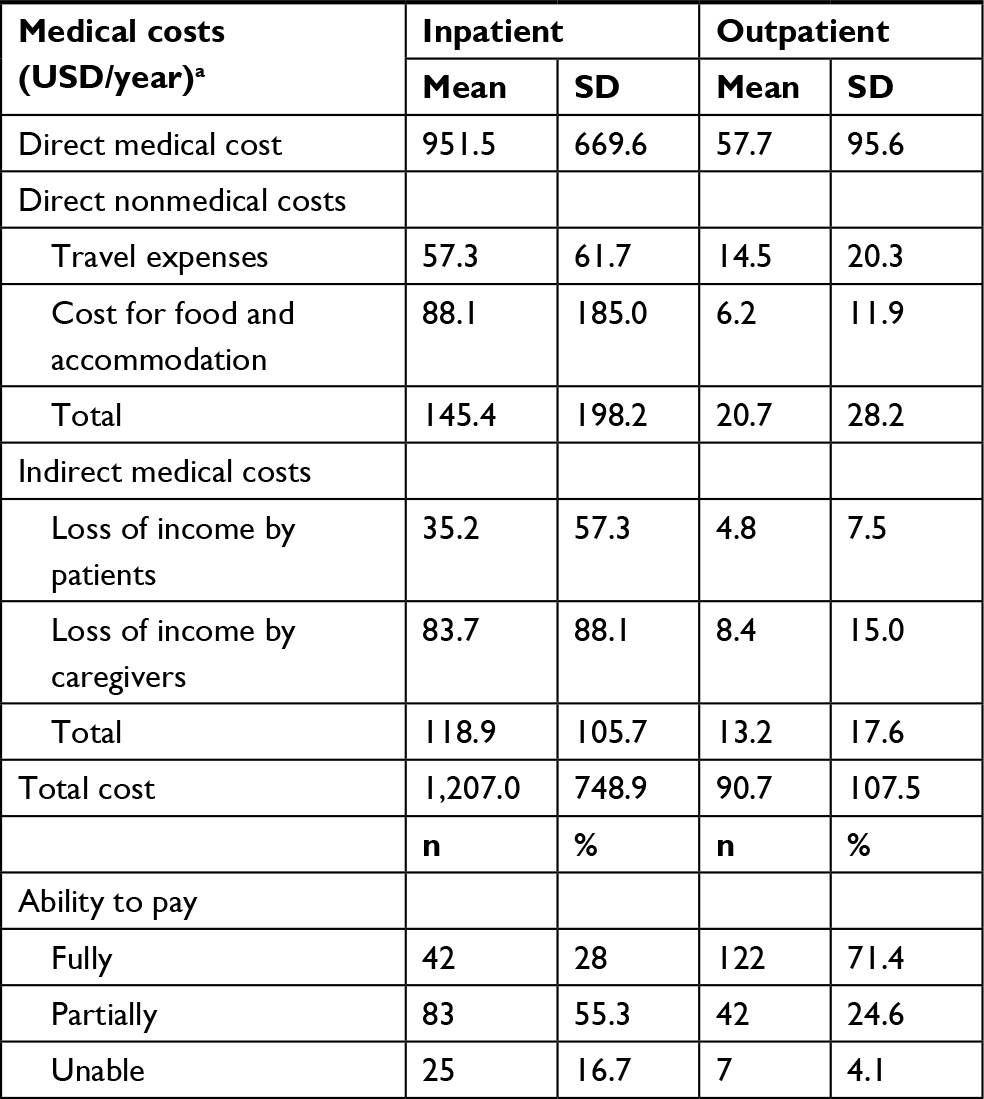 | Table 3 Inpatient and outpatient medical costs and ability to pay (N=118) Note: aExchange rate: 22,700 VND =1 US$ (2017). |
Table 4 indicates that patients who were divorced or widowed had a higher risk (OR: 8.38; 95% CI: 1.76–39.83) of experiencing CHE than those who were single. Regarding clinical characteristics, patients with intrahepatic gallstones had a higher risk (OR: 5.69, 95% CI: 1.65–19.61) of experiencing CHE than those with gallstones in the gallbladder. Outpatient status (OR: 0.05, 95% CI: 0.01–0.29), female gender (OR: 0.32, 95% CI: 0.1–1.01), history of pharmacological treatment to parasitic infection (OR: 0.33, 95% CI: 0.11–0.99), middle monthly household income quantile (OR: 0.28, 95% CI: 0.07–1.10), and highest monthly household income quantile (OR: 0.05, 95% CI: 0–0.52) offered a significant protection from CHE.
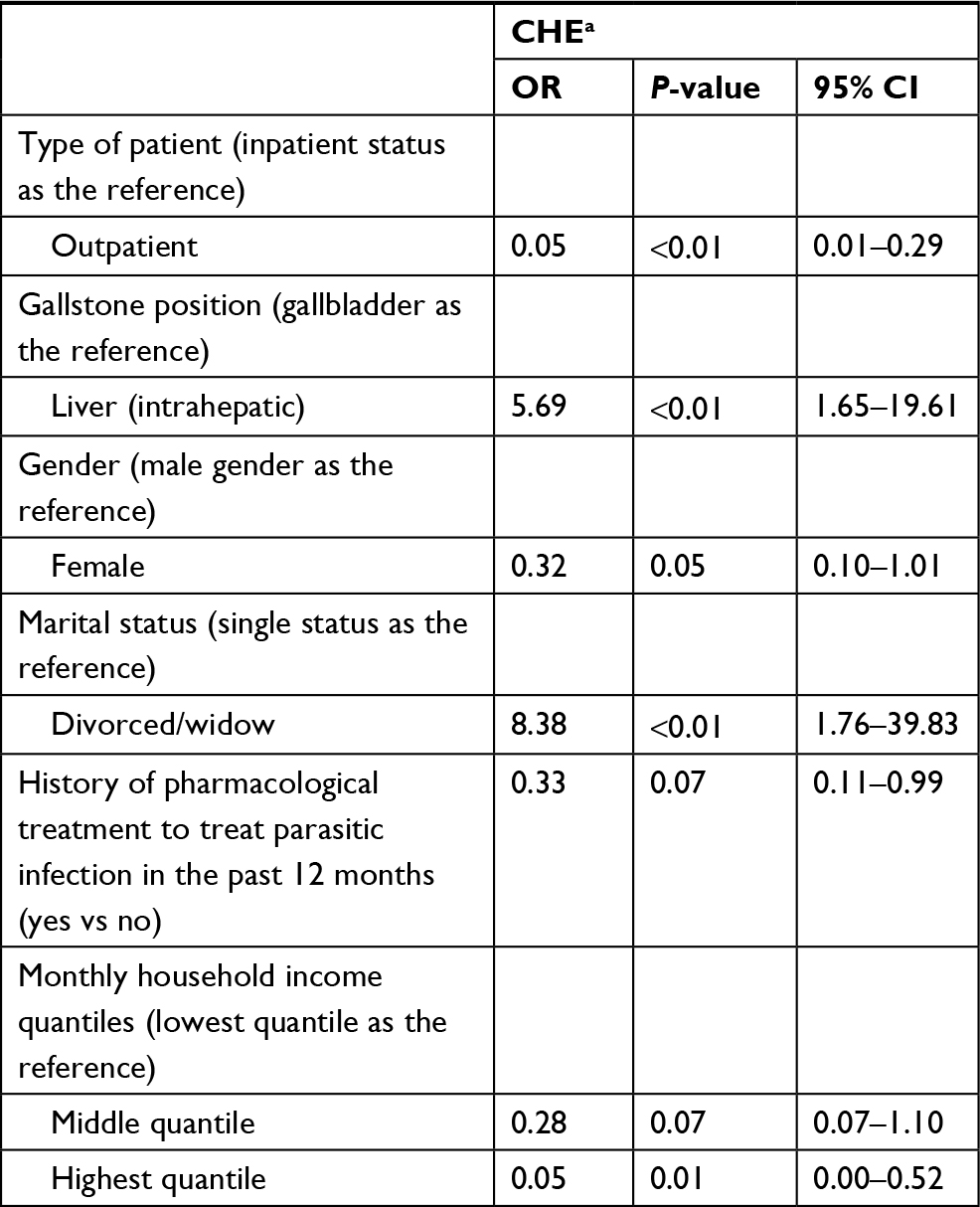 | Table 4 Factors associated with CHE Note: aCHE: 1 = yes, 0 = no. Abbreviation: CHE, catastrophic health expenditure. |
Discussion
This study revealed the prevalence of CHE in patients suffering from GSD to be 35%. Interestingly, it was found that higher proportion of patients with health insurance experienced CHE compared with their counterparts without health insurance, and there were no significant differences found in the inability to pay between patients with and without health insurance. Socioeconomic characteristics of patients, as well as their medical condition relating to GSD or GSD treatment, were found to influence the likelihood of experiencing CHE.
The prevalence of CHE in this study is much higher than the national average CHE rate 4.2%–8.2% reported previously in other studies in Vietnam, but lower than CHE prevalence of some other diseases, eg, cancer (CHE rate of 64.7%) or acute coronary events (CHE rate of 40%).21–23 The high prevalence of CHE-associated GSD is likely to be the result of its acute-on-chronic presentation: GSD can present as acute cholecystitis with a long period of the quiescent state. Diseases like cancer and cardiovascular, while being similar to GSD with acute and unpredictable onset, induce higher CHE rate probably due to their likely requirement for longer treatment than GSD. On the contrary, CHE prevalence in supposedly costly diseases of HIV/AIDS and opioid addiction with methadone maintenance treatment were found to be comparable or lower than On the contrary, CHE rates in HIV/AIDS (35.1%) and methadone maintenance treatment patients (12.8%) were comparable or lower than CHE rate in GSD patients. (ref 20, 24). It might be due to free antiretroviral therapy and methadone medication schemes offered by the Vietnamese government, which can reduce cost and OOP substantially.20,24 These findings suggested that diseases with acute-on-chronic nature like GSD would potentially lead to substantial CHE for patients, urging efforts from the government to tackle such financial burden of disease on the infected by providing direct aid, of which some supporting evidence is found, or by ensuring an effective health insurance scheme in place.
In contrast to our hypothesis that health insurance would build a strong financial buffer for preventing CHE, this study found that the higher proportion of patients covered by health insurance experienced CHE compared with those who were not. This is likely to reflect the local health insurance structure and hesitation of Vietnamese patients to utilize local level health facilities prior to admitting to central hospital. According to the Vietnamese Law of Health Insurance, if patients go to the provincial or central hospitals, health insurance requires patients to be referred by registered clinics or hospitals at the grassroots levels for full reimbursement, otherwise only up to a maximum of 40% of treatment cost would be covered. Meanwhile, perceived deficits in the accessibility of surgical services, long waiting hours, and inadequate infrastructure at grassroots level facilities might have motivated patients with GSD to go directly to Viet Duc Hospital – a central hospital, more so for those who were covered by health insurance with some extra financial buffers to spend resulting from insurance-related price subsidy offered by their health insurer.25 As a result, insurance-covered patients are more likely to bypass their registered clinics to be treated at the central hospital and incur OOP for potentially more costly services there, while those without health insurance would not engage in any costly services, thus less likely to experience CHE. In fact, this phenomenon was found in other developing countries such as Iran.26 On the contrary, the higher proportion of our participants without health insurance received nonsurgical treatment for GSD (compared with those insured). This further supports our argument that noninsured patients are more likely to deny more costly treatment, which usually is surgery. Such behavior would potentially undermine the GSD treatment outcome if surgical treatment is the kind of treatment needed.
Our study also found that compared with those at the poorest quintile, patients who belonged to the middle and richest quintiles were protected from experiencing CHE. Poorer households were particularly vulnerable to CHE without the capacity to pay for and spend on health care without affecting the consumption of necessities enjoyed by the rich.27 Job loss and decreased income, resulting from reduced work hours due to the treatment of GSD, might also lead to greater impact on patients with the lowest economic status. This would be particularly burdensome for those from rural areas, as they are likely to have later access to central health facilities due to geographical and financial constraints, leading to admission to central hospitals in more severe stage of illness which in turn results in higher treatment cost, longer recovery time, and heavier care burden on family members. In addition, although GSD prevalence might not differ greatly between urban and rural areas, as shown in other studies on Vietnamese cohorts, GSD among rural residents may present a larger threat since its potentially main cause is likely to be neglected.28,29 It has been found that a major cause of GSD in Vietnam is parasite infection, which presents mostly through consumption of food that has not been properly produced and prepared, for instance, raw or unwashed food.30–32 Meanwhile, safety standards in producing, preparing, and consumption of food are likely to receive insufficient attention in rural, lower income households. This suggested that efforts to alleviate the financial burden of GSD should probably focus more on supporting rural residents.
This study has several policy implications. Since the amount of OOP expenses paid by patients with GSD has been found to be still much higher than their capacity to pay, especially for those who require surgery, It is recommended that the healthcare authorities should re-evaluate the reimbursement capacity of current health insurance systems, especially for acute conditions. Moreover, some forms of instant reimbursement or prepayment policies should also be considered.25 and. Even in the case when health insurance reform is needed to address these issues, it is advised that the authority not press on having an “one-size-fits-all” policy, as recent studies on Vietnamese patients found that patients with varying conditions exhibit difference in preferences toward health care and health insurance, making generic coverage rather unrealistic.33,34 In fact, one study discovered that an insurance reimbursement threshold of 65% existed among nonresident patients – aiming for a rate higher than that would induce costs that overcompensate the benefits received.33 In addition, since many hospitals at lower levels, eg, provincial or district level ones, have been substantially renovated to improve their capacities in delivering services, patients with GSD should be encouraged to visit those facilities first instead of bypassing to the central level, a practice that would enable full reimbursement. Further collaboration between public and private health services as well as greater attention to public investment in social welfare is required to broaden the support to the low-income group. In addition, educational campaigns on food safety and general hygiene standards should be established and directed toward people from rural, less developed, and remote areas to ensure the risk of GSD caused by unsafe dietary and eating habit being properly addressed. Routine screening programs for GSD in Vietnam can also be conducted, as such screening regime was found to be both medically and economically valuable in some countries.35
Limitations
The above findings must be interpreted in light of the study’s limitations. First, this study was limited to assessing the cost of GSD during the first year after diagnosis. The income and cost of data were self-reported and recall bias could exist.20 In addition, the incidence of CHE is correlated with health care need of other household members, especially elderly.36 We did not obtain further information about other family members of the household who might suffer from chronic diseases and increase the risk of CHE. Finally, the sample size of this study was relatively small. Further studies on the larger set of participants and/or adopting a longitudinal setting are called to offer more information on the topic.
Conclusion
In conclusion, a significant number of Vietnamese patients with GSD were found to be at risk of CHE, especially those from lower income groups. Health insurance was discovered to not be able to offer sufficient protection from CHE for GSD patients, as those with health insurance exhibited higher likelihood of experiencing CHE compared with those without. Noninsured patients in our study tend to seek presumably less costly nonsurgical treatment, suggesting that financial disadvantages and potential burdens caused by GSD may prevent patients from getting the treatment needed. In accordance with the findings of this study, we suggest that efforts in re-evaluating health insurance reimbursement capacity, especially for acute diseases and taking into account the varying preferences of people with different disease severity, should be conducted by health authority. Educational campaigns to change an unsafe eating habit of those in rural areas should also be initiated. In addition, it is recommended that further studies concerning CHE of GSD in the context of ongoing health policy reform consider utilizing WHO-recommended measures like the fairness in financial contribution index,37 as well as taking into consideration the behavioral aspects of health care spending.38
Acknowledgments
The authors would like to acknowledge supports by Hanoi Medical University and Viet Duc Hospital for the acceptance to implement the study. There was no funding for this analysis.
Disclosure
The authors report no conflicts of interest in this work.
References
Afdhal NH, Zakko SF. Gallstones: Epidemiology, Risk Factors, and Prevention. 2016. Available from: https://www.uptodate.com/contents/gallstones-epidemiology-risk-factors-and-prevention. Accessed 10 October, 2018. | ||
European Association for the Study of the Liver (EASL). EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones. J Hepatol. 2016;65(1):146–181. | ||
Sun H, Tang H, Jiang S, et al. Gender and metabolic differences of gallstone diseases. World J Gastroenterol. 2009;15(15):1886–1891. | ||
Park YH, Park SJ, Jang JY, et al. Changing patterns of gallstone disease in Korea. World J Surg. 2004;28(2):206–210. | ||
Nguyen DT, Nguyen HTT. Assessment of post-laparoscopic cholecystectomy pain at Viet Duc Hospital, Vietnam. Health. 2015;7(3):346–354. | ||
Teerawattananon Y, Mugford M. Is it worth offering a routine laparoscopic cholecystectomy in developing countries? A Thailand case study. Cost Eff Resour Alloc. 2005;3(1):10. | ||
Hussain A, Mahmood HK, Dulku K. Laparoscopic cholecystectomy can be safely performed in a resource-limited setting: the first 49 laparoscopic cholecystectomies in Yemen. JSLS. 2008;12(1):71–76. | ||
Waqas A, Qasmi SA, Kiani F, Raza A, Khan KI, Manzoor S. Financial cost to institutions on patients waiting for gall bladder disease surgery. J Ayub Med Coll Abbottabad. 2014;26(2):158–161. | ||
Jones C, Mawhinney A, Brown R. The true cost of gallstone disease. Ulster Med J. 2012;81(1):10–13. | ||
The World Bank. Data bank; 2018. Available from: https://data.worldbank.org/indicator/. Accessed 10 October, 2018. | ||
World Health Organizations. Global Status Report on Noncommunicable Disease 2014. Geneva, Switzerland: World Health Organizations; 2014. | ||
Insurance VS. Situation of health insurance coverage in Vietnam in 2017. In: The Conference of Administrative Reform and Mission Deployment; Hanoi, Vietnam; 2017. | ||
Kim S, Kwon S. Impact of the policy of expanding benefit coverage for cancer patients on catastrophic health expenditure across different income groups in South Korea. Soc Sci Med. 2015;138:241–247. | ||
Li Y, Wu Q, Liu C, et al. Catastrophic health expenditure and rural household impoverishment in China: what role does the new cooperative health insurance scheme play? PLoS One. 2014;9(4):e93253. | ||
Azzani M, Yahya A, Roslani AC, Su TT. Catastrophic health expenditure among colorectal cancer patients and families: a case of Malaysia. Asia Pac J Public Health. 2017;29(6):485–494. | ||
Ibrahim N, Pozo-Martin F, Gilbert C. Direct non-medical costs double the total direct costs to patients undergoing cataract surgery in Zamfara state, Northern Nigeria: a case series. BMC Health Serv Res. 2015;15(1):163. | ||
Ho RC, Mak KK, Chua AN, Ho CS, Mak A. The effect of severity of depressive disorder on economic burden in a university hospital in Singapore. Expert Rev Pharmacoecon Outcomes Res. 2013;13(4):549–559. | ||
Sun J, Liabsuetrakul T, Fan Y, McNeil E. Protecting patients with cardiovascular diseases from catastrophic health expenditure and impoverishment by health finance reform. Trop Med Int Health. 2015;20(12):1846–1854. | ||
Van Minh H, Kim Phuong NT, Saksena P, James CD, Xu K. Financial burden of household out-of pocket Health expenditure in Vietnam: findings from the National living standard survey 2002–2010. Soc Sci Med. 2013;96:258–263. | ||
Tran BX, Duong AT, Nguyen LT, et al. Financial burden of health care for HIV/AIDS patients in Vietnam. Trop Med Int Health. 2013;18(2):212–218. | ||
Hoang VM, Oh J, Tran TA, et al. Patterns of health expenditures and financial protections in Vietnam 1992–2012. J Korean Med Sci. 2015;30(Suppl 2):S134–138. | ||
Jan S, Lee SW, Sawhney JP, et al. Catastrophic health expenditure on acute coronary events in Asia: a prospective study. Bull World Health Organ. 2016;94(3):193–200. | ||
Hoang VM. Household financial burden and poverty impacts of cancer treatment in Vietnam. Biomed Res Int. 2017;2017:9350147. | ||
Tran BX, Phan HT, Nguyen LH, et al. Economic vulnerability of methadone maintenance patients: implications for policies on co-payment services. Int J Drug Policy. 2016;31:131–137. | ||
Gu H, Kou Y, Yan Z, et al. Income related inequality and influencing factors: a study for the incidence of catastrophic health expenditure in rural China. BMC Public Health. 2017;17(1):727. | ||
Juyani Y, Hamedi D, Hosseini Jebeli SS, Qasham M. Multiple sclerosis and catastrophic health expenditure in Iran. Glob J Health Sci. 2016;8(9):194–199. | ||
Guo N, Iversen T, Lu M, Wang J, Shi L. Does the new cooperative medical scheme reduce inequality in catastrophic health expenditure in rural China? BMC Health Serv Res. 2016;16(1):653. | ||
Nguyen CC. Survey of gallstone disease in people over 50 years old in Ho Chi Minh City. Ho Chi Minh City J Med. 2010;14(1):47–54. | ||
Nguyen KT. Study on Some Epidemiological, Clinical and Surgical Complications of Acute Gallstone Disease in Adults in Thai Binh Province. Hanoi: Military Medical University; 2008:143. | ||
Lim JH, Kim SY, Park CM. Parasitic diseases of the biliary tract. AJR Am J Roentgenol. 2007;188(6):1596–1603. | ||
Lim T, Zelaya C, Latkin C, et al. Individual-level socioeconomic status and community-level inequality as determinants of stigma towards persons living with HIV who inject drugs in Thai Nguyen, Vietnam. J Int AIDS Soc. 2013;16(3 Suppl 2):18637. | ||
Parasites – Ascariasis; 2018 February 15, 2018 [cited July 7, 2018]. Available from: https://www.cdc.gov/parasites/ascariasis/. Accessed 10 October, 2018. | ||
Vuong QH. Sociodemographic factors influencing Vietnamese patient satisfaction with healthcare services and some meaningful empirical thresholds. Iran J Public Health. 2018;47(1):119–126. | ||
Tien TV, Phuong HT, Mathauer I, Phuong NTK. A Health Financing Review of Viet Nam with a Focus on Social Health Insurance. Geneva, Switzerland: World Health Organization; 2011. | ||
Shen HJ, Hsu CT, Tung TH. Economic and medical benefits of ultrasound screenings for gallstone disease. World J Gastroenterol. 2015;21(11):3337–3343. | ||
Edoka I, McPake B, Ensor T, Amara R, Edem-Hotah J. Changes in catastrophic health expenditure in post-conflict Sierra Leone: an Oaxaca-blinder decomposition analysis. Int J Equity Health. 2017;16(1):166. | ||
Daneshkohan A, Karami M, Najafi F, Matin BK. Household catastrophic health expenditure. Iran J Public Health. 2011;40(1):94–99. | ||
Vuong QH, Ho TM, Nguyen HK, Vuong TT. Healthcare consumers’ sensitivity to costs: a reflection on behavioural economics from an emerging market. Palgrave Commun. 2018;4(1):70. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.