")
Back to Journals » International Medical Case Reports Journal » Volume 14
Case Series: Management of Hypernatremia in DKA in a Tertiary Healthcare Setting in a Developing Country
Authors Nuwagaba J , Srikant S , Darshit D
Received 27 June 2021
Accepted for publication 14 August 2021
Published 27 August 2021 Volume 2021:14 Pages 567—571
DOI https://doi.org/10.2147/IMCRJ.S326350
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Julius Nuwagaba,1 Sanjanaa Srikant,2 Dave Darshit1
1Department of Medicine, Uganda Martyrs Hospital Lubaga, Kampala City, Uganda; 2Department of Medicine, Makerere University College of Health Sciences, Kampala City, Uganda
Correspondence: Julius Nuwagaba
Department of Medicine, Uganda Martyrs Hospital Lubaga, P.O.Box 14130, Kampala City, Uganda
Email [email protected]
Abstract: Diabetic ketoacidosis (DKA) commonly presents with hyponatremia, but hypernatremia is a rare case. We report two cases of hypernatremia, a 54-year-old woman (case 1) admitted with altered sensorium with blood glucose unrecordably high, serum sodium 134 mmol/L and an 18-year-old girl (case 2) admitted with reduced levels of consciousness, a random blood sugar of 21.2 mmol/L and serum sodium of 121 mmol/L. Case 1 was hydrated with isotonic saline and serum sodium values then escalated to 154 mmol/L on day 2, reaching 166 mmol/L on day 4. Case 2 was hydrated with isotonic saline and also given hypertonic saline for treatment of hyponatremia, and the sodium levels for this patient rose to 153 mmol/L on day 2 reaching a maximum of 176 mmol/L on day 3. On day 2, both patients were switched to half strength Darrow’s for correction of the hypernatremia along with insulin therapy. The patients recovered fully and were discharged without any sequelae. These reports exhibit a learning point in the choice of intravenous fluids for the treatment of DKA. They also show the need to delay the correction of hyponatremia in patients with high blood glucose levels.
Keywords: diabetic ketoacidosis, hypernatremia, hyperglycemia, diabetes, half strength Darrow’s solution
Introduction
Diabetes is found in every population in the world with steadily rising numbers. Without interventions to halt the surge in diabetes, the International Diabetes Federation (IDF) estimates at least 629 million people living with diabetes by 2045.1 Diabetic ketoacidosis (DKA) continues to be a severe medical emergency requiring intensive care (ICU) admission in most cases.2 Both patients were, however, managed in the High Dependency Unit (HDU) due to financial constraints. DKA consists of a biochemical triad of hyperglycemia, ketonemia, and high anion gap metabolic acidosis together with electrolyte derangements including dilutional or hyperosmolar hyponatremia.3
The management of DKA includes close monitoring, adequate and timely fluid resuscitation, insulin therapy, and electrolyte replacement to avoid adverse effects that could be fatal.4
Hypernatremia is a rare complication of DKA. Its etiology is unclear; however, it can be explained by water deficit from inadequate water intake, and free water loss that supersedes the electrolyte loss through diarrhea and vomiting.5 Together with CNS acidosis, hyperosmolarity has been known to contribute to CNS depression, which is associated with morbidity and mortality6 We hereby discuss unique cases of a 54-year-old female with hypernatremia in DKA secondary to severe hypotonic fluid loss, and an 18-year-old girl with hypernatremia in DKA secondary to correction of hyponatremia with 3% hypertonic saline. In this article, we present the management of this condition in resource-limited settings in a developing country.
Case One
A 54-year-old African female, with no known medical history of any chronic illness, presented with a day’s history of altered sensorium. This was preceded by 2 weeks history of polyuria and polydipsia, and a one-week history of generalized body weakness. She had no positive family history of diabetes.
On presentation, the patient was bound and responsive to pain, but poorly receptive to verbal stimuli. On a physical exam, she was afebrile, had severe dehydration with poor skin turgor, Kussmaul breathing with moderate distress, and tachypnea at about 40 breaths/minute, but pulse oximetry of 98% on ambient air. She had a blood pressure of 125/84 mmHg, she had tachycardia at 105 beats/minute.
On investigation, her random blood sugar (RBS) was unrecordably very high, serum ketones were 4.4 mmol/L, the admission serum: Sodium (Na+) 134 mmol/L, potassium (K+) 3.7 mmol/L, and HBA1C 14.1%. On day four of admission, she had Na+ 166 mmol/, K+ 3.2 mmol/L, and serum ketones 3.3 mmol/L. Table 1 shows the fluctuating RBS values appropriate to the time interval and Table 2 shows additional biochemical values as per the time interval. However, due to the limited resources and financial constraints, Arterial Blood Gases (ABGs) could not be conducted.
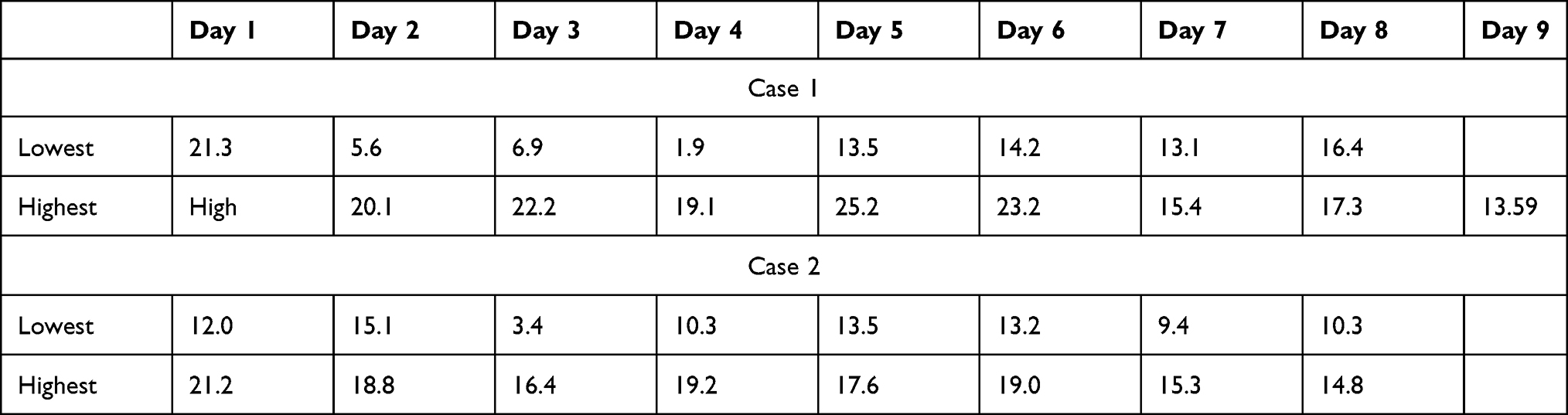 |
Table 1 Fluctuating Random Blood Sugar in Millimoles/L (mmol/L) for the Two Patients |
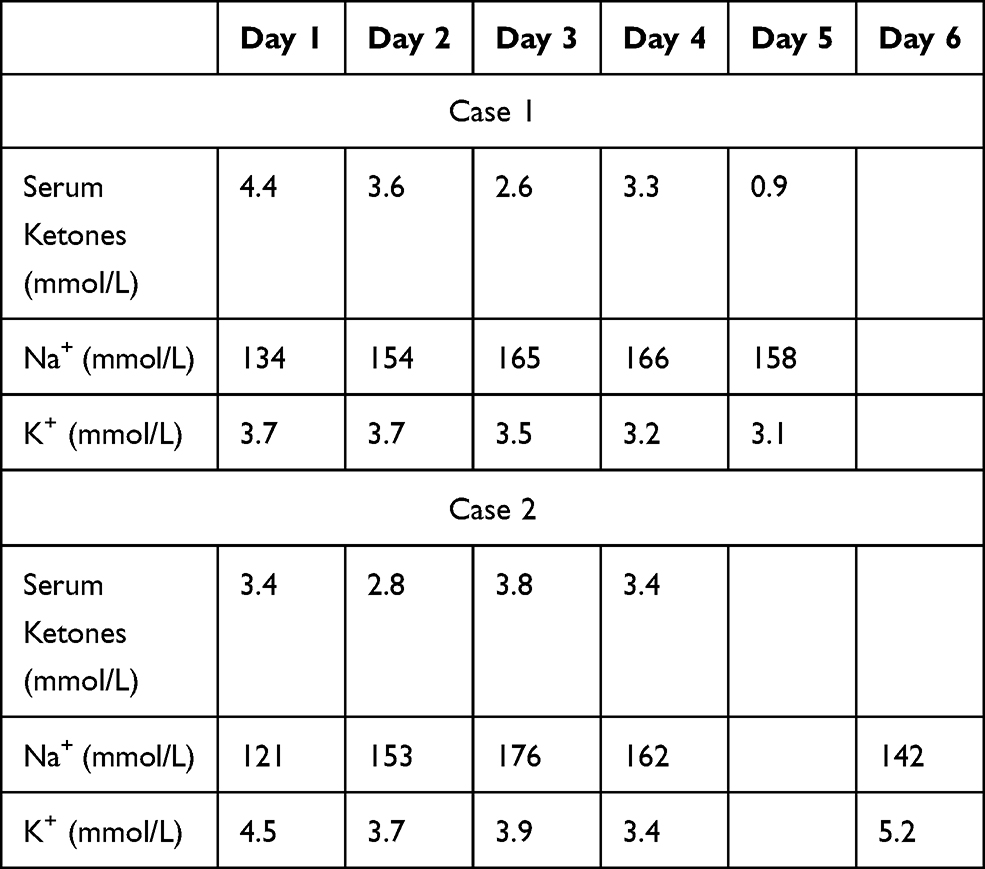 |
Table 2 Serial Values of Serum Ketones, Sodium, and Potassium Ions for the Two Patients |
The patient received initial fluid resuscitation, and, later admitted to Highly Dependent Unit (HDU) on medical ward requiring additional administration of 0.9% normal saline, initiation of intravenous rapid-acting insulin infusion to maintain random blood sugar between 8 and 13 mmol/L, intravenous potassium chloride (KCl) at 40 mmol twice a day. Brain Computed Tomography (CT) scan was, however, not done, though the patient was also initiated on mannitol 60 g 8 hourly on a presumptive clinical basis of cerebral edema.
By day 3, serum sodium value continued to peak. Because of severe hypernatremia, her fluid therapy was switched from 0.9% normal saline to half strength Darrow’s solution, and mannitol was also stopped. On day 4 of hospitalization, the patient became more restless and she was put on intramuscular haloperidol as needed (PRN) for the course of that day. She also developed fluctuating blood glucose levels with sudden spikes and drops between 20 mmol/L and 2 mmol/L; she was switched from IV rapid-acting insulin to 3 hourly subcutaneous rapid-acting insulin.
The patient was nil per OS (no oral intake) till day 5 until she could tolerate low volume oral sips of water because of dry oral mucous membranes that were developing sores. The patient started to be alert, awake, and responsive to commands while tolerating oral feeds and improvement from admission assessment, and haloperidol was thus stopped.
On day 7 of hospital stay, the patient was transferred out of HDU to the general medical ward for optimization of diabetic medication on subcutaneous mixtard at 30 international units (IU) pre-breakfast and 20 IU pre-supper, as well plus 8 IU of subcutaneous Actrapid pre-lunch.
The patient was eventually discharged without any further events on day 9 on subcutaneous mixtard (fast-acting [soluble] and long-acting [isophane] insulin) at 20 IU pre-breakfast and 10 IU pre-supper, metformin 850 mg 12 hourly, atorvastatin 40 mg once a day, losartan 50 mg once a day, and cefuroxime 500 mg twice a day. The pre-discharge random blood sugar was 13.5 mmol/L.
Case Two
An 18-year-old female, newly diagnosed Diabetic (unknown type) 2 months back, presented with a day’s history of altered sensorium and fast breathing. This was preceded by generalized malaise, joint pains, and heartburn for 4 days, and progressive weight loss. She was partially treated for 2 days from a clinic with subcutaneous Actrapid 15 IU stat; then, Metformin 500 mg once daily, received Normal Saline 500 mL twice daily, Folate, Ceftriaxone, Metronidazole, Omeprazole, TRAP. A month before the presentation, the patient had stopped taking her medication and was reportedly drinking plenty of drinks that contained processed sugar.
At admission, she was restless and disoriented with a Glasgow Coma Scale (GCS) of 11/15 (E4V2M5). She was afebrile at 36.4°C, had severe dehydration, Kussmaul breathing, mild distress, tachypnea at 30 breaths per minute, and pulse oximetry at 98% on ambient air. She had tachycardia at 112 beats per minute with a blood pressure of 146/75 mmHg.
On investigation, her random blood sugar was 21.2 mmol/L, serum ketones were 3.4 mmol/L, the admission serum: Sodium (Na+) 121 mmol/L, potassium (K+) 4.6 mmol/L, HBA1C 12.1%, CRP 1.69 mg/L, marked Leukocytosis of 16,480 cells/microliter, predominant neutrophilia of 12,840 cells/microliter, Thrombocytosis 419,000 cells/microliter. A respiratory exam revealed coarse crepitations in the right axillary region. The patient received initial fluid resuscitation, and, later admitted to the Highly Dependent Unit (HDU) on the medical ward requiring additional administration of 0.9% normal saline, ceftriaxone, initiation of intravenous rapid-acting insulin infusion, and intravenous KCl at 40 mmol twice a day. With a corrected Na+ level of 128 mmol/L hypertonic saline 150 mmol in 500 mL of Normal saline was initiated to run slowly over 24 hours.
On day 2 of admission, she had Na+ 153 mmol/, K+ 3.7 mmol/L, and serum ketones 2.8 mmol/L. She was switched to half strength Darrow’s and hypertonic saline stopped due to hypernatremia. Given the improving levels of consciousness and gradual reduction in RBS and Serum Ketones, she started on subcutaneous rapid-acting insulin. However, on day 4, Na+ continued to rise to 176 mmol/L and by day 5, Na+ was 162 mmol/L.
The patient was discharged on day 8 on mixtard 15 IU pre-breakfast, 10 IU pre-supper, and soluble insulin Actrapid at 6 IU pre-lunch in a stable condition.
Discussion
Hyperglycemia induces osmotic fluid shift and osmotic diuresis instigating electrolyte imbalances in patients with DKA. The admission serum sodium is usually low in patients with DKA. Serum glucose cannot penetrate the cells secondary to the insulinopenia of DKA. In hyperglycemic crises, glucose becomes osmotically effective and causes water to shift from intracellular space to extracellular space resulting in dilutional or hyperosmolar hyponatremia, a form of pseudo hyponatremia. Hypernatremia in DKA occurs as a result of hypotonic renal losses, which is water excretion secondary to glycosuria-mediated osmotic diuresis and inappropriate water replacement that causes a water deficit in excess of electrolytes.4,7
A correction factor of 1.6 millimoles per liter is recommended to be added to the measured plasma sodium concentration for each 5.55 mmol/L of glucose above the 5.55 mmol/L to account for the dilution effect of glucose.8 Corrected serum sodium provides a useful tool for monitoring and management during acute hyperglycemic crises by assessing the magnitude of the deficit of sodium and water and thus provides an initial estimate of the tonicity of the replacement fluids during the course of therapy.9 The corrected sodium for case 2 was 128 mmol/L and with this hypertonic saline should not have been given and hence reduced chances of developing hypernatremia.
Management of hypernatremia in DKA consists of initial fluid therapy, directed towards the expansion of the intravascular, interstitial, and intracellular volume. Infusing 0.9% normal (isotonic) saline, at a rate of 15–20 milliliters per kilogram per hour or 1–1.5 liters during the first hour, to maintain effective plasma osmolality, in addition to supplementation of potassium. Subsequently, the type of fluid replacement depends on the hemodynamics, state of hydration, serum electrolytes, and urinary output. 0.45% sodium chloride infused at 250–500 mL/hour as the corrected sodium concentration may be in excess of 145 mmol/liter, whereas 0.9% NaCl at a similar rate is appropriate if corrected serum sodium is low.10,11 For our patients, we used half-strength Darrow’s as our fluid therapy once the sodium concentration was above 145 mmol/L.
Precaution to avoid risking cerebral edema, from overcorrecting acute hypernatremia, includes decreasing plasma sodium concentration by 2 mmol/liter/hour until plasma concentration is 145 mmol/liter.12 However, for our patients, we only measured the electrolytes once a day to cut the cost of health care. One daily monitoring of electrolytes gave us a clear picture of electrolyte imbalance and correction for our patients.
The mainstay in the treatment of DKA involves the administration of regular insulin via continuous intravenous infusion or by frequent subcutaneous injections. The administration of continuous intravenous infusion of regular insulin is the preferred route because of its short half-life and easy titration.11 In moderate-to-severe DKA, treatment can be initiated with an IV bolus of regular insulin, 0.1 units/kg followed within 5 minutes by continuous IV infusion of 0.1 units/kg/hour. These doses of insulin decrease serum glucose by 2.8–3.9 mmol/L per hour. If glucose does not fall by this, from the initial value in the first hour, the insulin infusion rate should be doubled every hour until a steady decline in serum glucose of this magnitude is achieved. Alternatively, subcutaneous, rapid-acting insulin is an initial injection of 0.3 units/kg, followed by 0.1 units/kg every hour until the serum glucose is less than 13.9 mmol/L. The insulin dose is then decreased to 0.05 to 0.1 units/kg and administered every one or two hours until the resolution of the ketoacidosis.10,13
Once the plasma glucose is ∼ 11.1 to 13.9 mmol/L, 5% dextrose should be added to replacement fluids to allow continued insulin administration until ketonemia is controlled while at the same time avoiding hypoglycemia. Therefore, the insulin infusion rate should be reduced.14 For our patients, the infusion/injection rate of insulin was reduced from hourly to 4 to 6 hourly once the plasma glucose fell below 14 mmol/L.
Conclusion
Our article guides medical practitioners on altered sensorium in DKA, acute hypernatremia, fluctuating blood glucose levels, and an approach to the management of this condition. The cases also highlight the value of corrected sodium to guide the choice of fluid therapy. We, therefore, present the role of hypotonic fluids as a choice for DKA once the sodium concentration falls in excess of 145 mmol/L.
Informed Consent/Ethical Approval
Informed consent was obtained from both patients to publish their medical history/course and case details. This case series did not require any institutional review board approval.
Disclosure
The authors declare no conflicts of interest.
References
1. International Diabetes Federation. IDF DIABETES ATLAS Eighth edition 2017; 2017[cited June 13, 2021]. Available from: https://diabetesatlas.org/upload/resources/previous/files/8/IDF_DA_8e-EN-final.pdf. Accessed August 17, 2021.
2. Mendez Y, Surani S, Varon J. Diabetic ketoacidosis: treatment in the intensive care unit or general medical/surgical ward? World J Diabetes. 2017;8(2):40.
3. Kitabchi AE, Wall BM. Diabetic ketoacidosis. Med Clin N Am. 1995;79(1):9–37.
4. Gosmanov AR, Gosmanova EO, Kitabchi AE. Hyperglycemic Crises: Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar State. [Updated 2021 May 9]. In: Feingold KR, Anawalt B, Boyce A, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279052/.
5. Ibarra G, Majmundar MM, Pacheco E, et al. Hypernatremia in diabetic ketoacidosis: rare presentation and a cautionary tale. Cureus. 2020;12(12):e11841. doi:10.7759/cureus.11841
6. Estifan E, Nanavati SM, Kumar V, et al. Salty diabetes: a case series of hypernatremia presenting with diabetic ketoacidosis. AME Case Rep. 2019;3:27. doi:10.21037/acr.2019.07.04
7. Liamis G, Liberopoulos E, Barkas F, et al. Diabetes mellitus and electrolyte disorders. World J Clin Cases. 2014;2(10):488.
8. Palmer BF, Clegg DJ, Ingelfinger JR. Electrolyte and acid-base disturbances in patients with diabetes mellitus. N Engl J Med. 2015;373(6):548–559. doi:10.1056/NEJMra1503102
9. Ing TS, Ganta K, Bhave G, et al. The corrected serum sodium concentration in hyperglycemic crises: computation and clinical applications. Front Med. 2020;7. doi:10.3389/fmed.2020.00477
10. Gosmanov AR, Gosmanova EO, Dillard-Cannon E. Management of adult diabetic ketoacidosis. Diabetes Metab Syndr Obes. 2014;7:255.
11. Kitabchi AE, Umpierrez GE, Miles JM, et al. Hyperglycemic crises in adult patients with diabetes. Diabetes Care. 2009;32(7):1335–1343. doi:10.2337/dc09-9032
12. Sterns RH, Ingelfinger JR. Disorders of plasma sodium—causes, consequences, and correction. N Engl J Med. 2015;372(1):55–65. doi:10.1056/NEJMra1404489
13. Brown HD, Tran RH, Patka JH. Effect of Bolus insulin administration followed by a continuous insulin infusion on diabetic ketoacidosis management. Pharmacy. 2018;6(4):129. doi:10.3390/pharmacy6040129
14. Lizzo JM, Goyal A, Gupta V. (2021). Adult Diabetic Ketoacidosis. In StatPearls. StatPearls Publishing. Authors: Jenna M. Lizzo, Amandeep Goyal, Vikas Gupta
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.