")
Back to Journals » Psychology Research and Behavior Management » Volume 13
Care Is the Doctor’s Best Prescription: The Impact of Doctor-Patient Empathy on the Physical and Mental Health of Asthmatic Patients in China
Authors Wu H, Zhang Y, Li S, Liu Q, Yang N
Received 10 August 2019
Accepted for publication 17 January 2020
Published 11 February 2020 Volume 2020:13 Pages 141—150
DOI https://doi.org/10.2147/PRBM.S226706
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Huiduo Wu,1,* Yan Zhang,2,* Shiyue Li,3 Qiaoyun Liu,1 Ningxi Yang2
1Education and Rehabilitation Department, Faculty of Education, East China Normal University, Shanghai, People’s Republic of China; 2College of Humanities and Social Sciences, Harbin Engineering University, Harbin, Heilongjiang, People’s Republic of China; 3School of Health Sciences, Wuhan University, Wuhan, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiaoyun Liu
Education and Rehabilitation Department, Faculty of Education, East China Normal University, 3663 North Zhongshan Road, Shanghai 200062, People’s Republic of China
Tel +86 21 6223 2287
Email [email protected]
Ningxi Yang
College of Humanities and Social Sciences, Harbin Engineering University, No. 145 Nantong Road, Harbin, Heilongjiang, People’s Republic of China
Tel +86 188 1926 8616
Email [email protected]
Background: To explore the impact of empathy between Chinese doctors and patients on anxiety, self-efficacy, sleep and IL-6 levels in hospitalized asthmatic patients.
Methods: This study included 195 asthmatic patients and 30 respirologists in China. The Jefferson Empathy Scale (JSE) was used to measure the empathy level of doctors, and the consultation and relational empathy (CARE) scale was used to measure patients’ perception of empathy between themselves and their doctors. Doctors were divided into three groups, according to JSE scores. Data about anxiety, self-efficacy, sleep and IL-6 were collected and compared between patients in different JSE groups at admission (T1) and 3 months later (T2). The correlation between JSE scores and CARE scores was analyzed. Pearson correlation analysis along with a structural equation model was applied to explore the relevance among anxiety, self-efficacy, sleep, inflammatory factors (IL-6) and patients’ perception of empathy shown by their doctors.
Results: There was no statistical difference between the indices of patients in three groups at admission. For all patients, the changes of indicators were statistically different from T1 to T2. Three months later, patients in high empathy scoring group showed lower anxiety and IL-6, and higher self-efficacy and sleep quality. There was a positive correlation between JSE and CARE scores. Patients’ perception of doctor-patient empathy was negatively correlated to anxiety levels and IL-6, and positively correlated to self-efficacy and sleep quality. Anxiety, self-efficacy and sleep quality were mediators in the relationship between patients’ perception of empathy and IL-6.
Conclusion: In the Chinese sample, anxiety, self-efficacy, sleep, empathy between doctors and patients and IL-6 are closely correlated. Anxiety, self-efficacy and sleep may play additional roles in the influence of patients’ perception of empathy between doctors and patients on IL-6 in asthmatic patients.
Keywords: doctor-patient relationship, empathy, asthmatic, self-efficacy, anxiety, sleep, IL-6, China
Introduction
Bronchial asthma is a common psychosomatic disease of the respiratory system. Many mental stressors, such as anxiety, disappointment, distress, anger, fear and depression can cause asthma.1 At the same time, the quality of life of patients with asthma is reduced, and other psychological problems including depression, anxiety, mania, panic disorder, sleep disorder, and post-traumatic stress disorder can appear.2 Therefore, it is extremely important to support the psychological health of patients with asthma. In addition, because asthma is characterized by chronic airway inflammation, inflammatory factors are one of the important monitoring indicators of patients, which require attention from doctors.3
The doctor-patient relationship is important both medically and socially. At present, disputes between doctors and patients often occur in the mainland of China, and medical staff have been wounded or even killed in recent years.4 Unfortunately, Chinese doctors are facing more work pressures and have less time to communicate with patients.5 Additionally, they subjectively pay more attention to identifying the disease rather than listening to the patient, are unwilling to communicate or sympathize with the patient, and lack appropriate training.6 However, hospitalized patients are heavily dependent on their doctors for care and advice. A good doctor–patient relationship and communication are not only helpful in improving patient satisfaction, but also beneficial to patients’ mental health and hospital experience.7,8 Compared to skilled communication, empathy refers to the ability of one person to understand others’ unique experience, respond appropriately to it and demonstrate altruistic behavior.9
Doctor-patient empathy refers to the establishment and deep understanding of the emotional relationship between doctors and patients. The important role of doctor-patient empathy in patients’ physical, psychological health and social adaptation has been confirmed by many studies.10,11 Since asthma patients have a long course of illness and recurrent attacks, they require an understanding of their illness, as well as attention and support from caregivers. Therefore, this study focuses on the relationship between physical and mental health of hospitalized asthma patients and physician-patient empathy in the context of Chinese culture, and explores its possible effects.
Anxiety is an important psychological indicator that has been studied by many researchers in asthma patients. It is closely related to the patient’s quality of life, control of disease, and other outcomes.12–14 Self-efficacy refers to the degree of self-confidence of an individual in a specific situation. According to the theory, people who have high self-efficacy are motivated, demonstrate effort and persistence in their daily activities, and their health results are often good.15 As a result, self-efficacy is often used as one of the important indicators in the study of patients with chronic diseases.16 IL-6 is a cytokine which can stimulate cell proliferation, differentiation and improve the immune response. It also plays an important role in the health assessment of patients with inflammatory diseases.17 The correlation between IL-6 and mood has been confirmed.18 Therefore, in this study, we measured patients’ outcome including an assessment of anxiety, self-efficacy, sleep and IL-6, which are all closely related to the mental state of the patient.19 In this study, two hypotheses were proposed: 1) patient perception of doctor-patient relational empathy directly affects IL-6 production; 2) patient perception of doctor-patient relational empathy indirectly affects IL-6 with anxiety, self-efficacy and sleep having mediating roles.
Materials and Methods
Participants
From the total pool of asthmatic patients, we selected patients using a random number table method, who were offered study participation. The study included 195 patients with bronchial asthma who were hospitalized in 6 centers from January to August 2019. Selection criteria were as follows: 1) asthma was diagnosed and patient was hospitalized for at least 7 days, and 2) patients understood their diagnosis and provided informed consent to participation in the study. Patients with acute infectious disease, cancer, psychiatric disease, Parkinson’s disease and others which may have significant effects on sleep, mental state and/or IL-6 were excluded from the study. In this study, 30 respiratory specialists treated patients and provided health guidance to them.
Procedures
The main steps of the study are outlined in this section. First, the doctor’s ability to empathize was assessed with the Jefferson Empathy Scale (JSE) prior to the inclusion of the first patient in the study, and they were divided into three groups according to the average JSE scores with 10 doctors in each group. Second, on the day of admission (T1) and 3 months later (T2), anonymous cross-sectional questionnaires were conducted, including a scale to assess anxiety and self-efficacy. Data relating to sleep patterns and serum IL-6 were collected at the same time (T1 and T2). Data on patients’ perception of doctor-patient relational empathy were collected at T2. For all patients, their indexes at T1 and T2 were compared. The correlation between doctors’ empathy score and patient perception of doctor-patient relational empathy was analyzed. As a final point, the relationships between anxiety, self-efficacy, sleep, IL-6 and patients’ perception of doctor-patient relational empathy were explored.
Measures
Demographic and Disease Information
The gender and age of the patients and doctors were collected. The average number of days in hospital for each patient was recorded.
Assessment of Doctor’s Empathy
The Jefferson Empathy Scale (JSE), Chinese version, was applied to measure the empathy level of doctors. The scale was first developed at Jefferson Medical College in 2001 to measure the empathy level of medical staff in clinical work, and consists of three dimensions: compassionate care, perspective taking, and standing in the patient’s shoes.20 The assessment included 20 questions; each response was scored on a scale of 1–7. A score of 1 indicates “strong disagreement” and a score of 7 indicates “strong agreement”. Therefore, the JSE score ranges from 20 to 140, and the higher the score, the stronger the ability to empathize.21 The Cronbach’s alpha of JSE was 0.895 in this study.
Patient Perception of Doctor-Patient Relational Empathy
The patient’s perception of doctor-patient relational empathy was measured using the consultation and relational empathy (CARE) scale. There were 10 items in the questionnaire, and each item was assigned 1–5 points with the total score of the scale ranging from 10 to 50. The higher the score, the more the patients perceive doctor-patient empathy.22 The Cronbach’s alpha of CARE was 0.872 in the present study.
Assessment of Anxiety
We choose the Hospital Anxiety and Depression Scale (HADS) to measure the anxiety level of patients. The scale is divided into two parts, with 7 items measuring anxiety (HADS-a) and 7 items measuring depression (HADS-d). Each response is scored from 0 to 3, and each subscale scores from 0 to 21. Higher scores indicate that patients are more anxious or more depressed.23 For each subscale, scoring 8 or more indicates that the patient has anxiety or depression.24 Patients complete the scale according to their actual feeling in 1 month. In this study, anxiety was measured by HADS-a, and the Cronbach’s alpha was 0.902.
Assessment of Self-Efficacy
Patients’ self-efficacy was measured using the General Self-Efficacy Scale (GSES) which was developed by Ralf Schwarzer.25 The scale is widely used in China, and the reliability and validity are good.26 The scale consists of 10 items with each item scoring from 1 to 4, and the aggregate score ranges from 10 to 40. The standard score gets from the aggregate score divided by 10. Higher scores show that patients have more self-efficacy.25 The Cronbach’s alpha was 0.897.
Sleep Efficiency
Sleep efficiency (SE), defined as the ratio of total sleep time to bedtime, was used to measure sleep quality, and polysomnography was used to measure sleep efficiency. Patients arrived at the sleep monitoring room at 20:00 and began sleeping at their normal bedtime. All patients were tested with PSG and were asked to stay in bed for 8 hrs to make sure that the time in bed was controlled. In accordance with international standardized methods, we applied surface disc electrodes to record the electroencephalogram (EEG) signals of 6 areas synchronously (F3-A2, F4-A1, C3-A2, 01-A2, 02-A1). In order to record the electromyogram (EMG) of the chin, we applied 2 surface electrodes, and placed an electrode at 1 cm above and below the lateral canthus so that the eye movements of the two eyes could be recorded.
Measurement of IL-6
Patients were asked to fast for at least 10 hrs before blood was taken. In the morning, 3 mL of venous blood was collected with vacuum sampling without using anticoagulants. The blood samples were stored for 15 mins at room temperature and centrifuged in a high-speed desktop centrifuge for 20 mins at 2000–3000 r/s. We collected and stored the upper 0.5 mL layer of serum in an Eppendorf tube. Using an ELISA kit (Beijing Hotgen Biotech Co., Ltd), the concentration of IL-6 in serum was tested with the TAn SM802 enzyme-labeling instrument (Shanghai Yongchuang Medical Devices Co.).
Statistical Analysis
EPI 3.1 software was used to enter the data and the SAS 9.4 statistical software package was used for data analysis. The data are represented as mean ± standard error of the mean (SEM). Variance analysis was used to compare the indicators of the three groups, and the paired t-test was used to compare the indexes on admission and after 3 months. A Pearson correlation analysis was applied to test the correlation between the doctors’ empathy and patient perception of doctor-patient relational empathy. A Pearson correlation analysis and structural equation modeling were used to explore the correlations between anxiety, self-efficacy, sleep, serum IL-6, and patient perception of doctor-patient relational empathy.
Results
Sample
In this study, all 30 doctors agreed to participate. Twelve of them were male and 18 were female, with an average age was 41.26±5.78 years. The average empathy score of the high scoring group, moderate scoring group, low scoring group was 71.42±5.61, 90.27±4.83, and 113.62±5.36, respectively. There were significant differences in the scores of empathy between the three groups (F=165.50, P<0.0001). Two hundred and twenty (220) patients were invited to participate in the study, 195 patients enrolled, with a participation rate of 88.64%. The average age of the patients was 61.28±7.64 years, with an average hospitalization length of 7.56±0.88 days, and 102 male and 93 female participants.
Comparison of Patients’ Indexes Among Different Doctor Groups (Grouping by JSE Score) at Admission (T1) and 3 Months Later (T2)
At admission, there was no significant difference in index scoring between the three groups. Three months later, the indicators of the three groups were significantly different (P<0.0001). Patients in high empathy scoring doctor group reported significantly lower anxiety, lower serum IL-6, higher self-efficacy, and sleep quality than patients in the low empathy scoring doctor group. The indexes of patients by different levels of doctors’ empathy at the two time points are shown in Table 1.
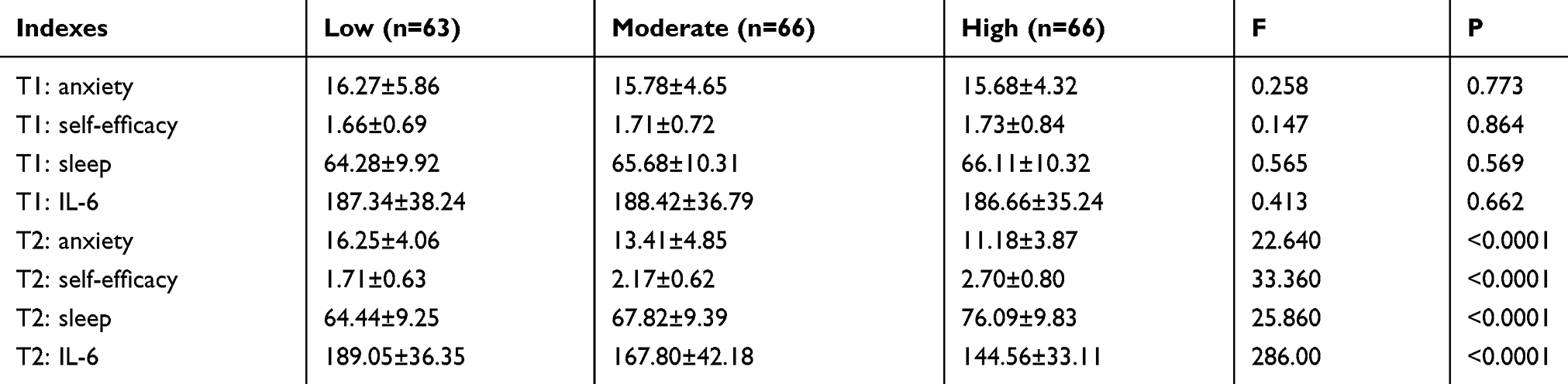 |
Table 1 Comparisons of Indexes of Patients in Three Groups of Doctors (Grouping by JSE Score) at Admission (T1) and Three Months After Admission (T2) |
Comparison of Patients’ Indexes at Admission (T1) and 3 Months Later (T2)
Patients’ indexes at admission and 3 months later were compared and the results are presented in Table 2. Changes in all the indexes showed significant differences between the 2 time points, the showed significant differences.
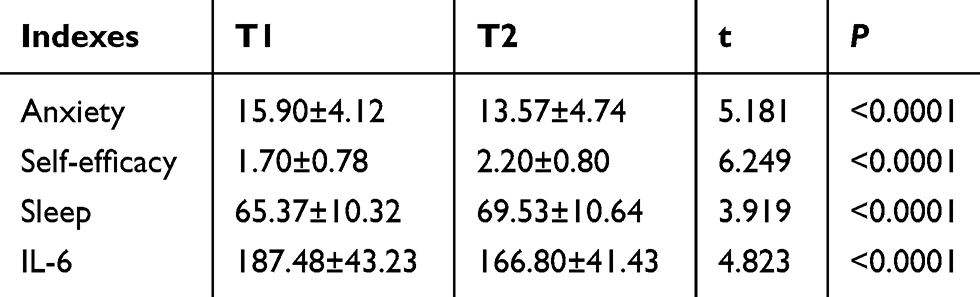 |
Table 2 Comparison of Patients’ Indexes at Admission (T1) and Three Months After Admission (T2) |
Correlation Between JSE and CARE
After analyzing the correlation between doctors’ empathy (JSE score) and patient perception of doctor-patient relational empathy (CARE score), we found there was a positive correlation between them (r=0.513, P<0.01).
Correlations Between Patients’ Perceptions of Doctor-Patient Relational Empathy (CARE) and Patients’ Anxiety, Self-Efficacy, Sleep and IL-6 at T2
A Pearson’s correlation test was used to measure the relationships between patients’ anxiety, self-efficacy, sleep, serum IL-6, and patients’ perception of doctor-patient relational empathy. The results showed that patients’ perceptions of doctor-patient relational empathy were negatively correlated with anxiety (r=−0.479, P<0.01) and serum IL-6 (r=−0.414, P<0.01), and were positively correlated with self-efficacy (r=0.497, P<0.01) and sleep (r=0.433, P<0.01), and these results were statistically significant. The results are shown in Table 3.
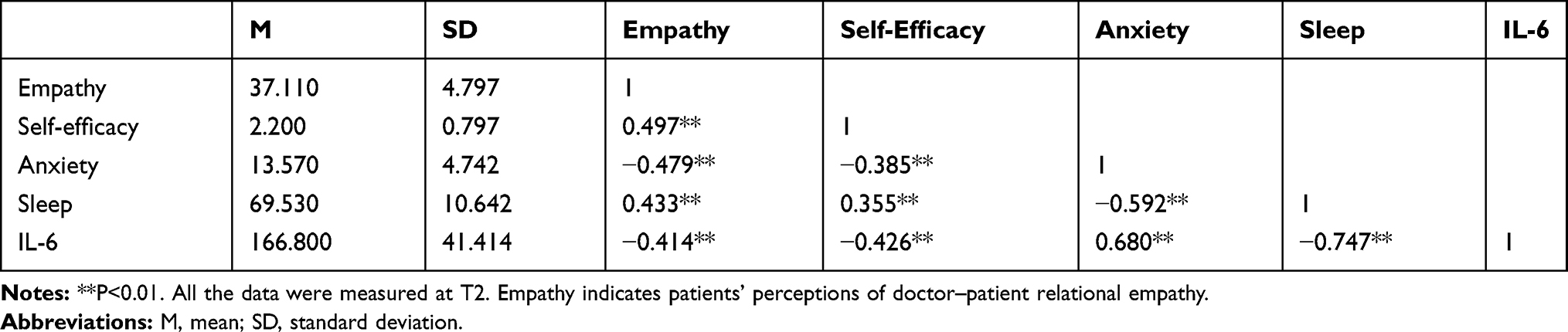 |
Table 3 The Relationship Between Patients’ Perceptions of Doctor–Patient Relational Empathy and Self-Efficacy, Anxiety, Sleep and IL-6 in Patients |
The Possible Mechanism of Impact of Patients’ Perceptions of Doctor-Patient Relational Empathy (CARE) on IL-6 at T2: Effects on Self-Efficacy, Anxiety and Sleep
To further explore the connections among the variables, we used the path analysis method to build multiple intermediary models and used AMOS software to confirm the models described in our hypotheses. The structural equation model among the variables fitted well (GFI =0.996, CFI =0.998, NFI=0.995, AGFI=0.942, RMSEA=0.068, χ2/df =1.905), with results shown in Figure 1.
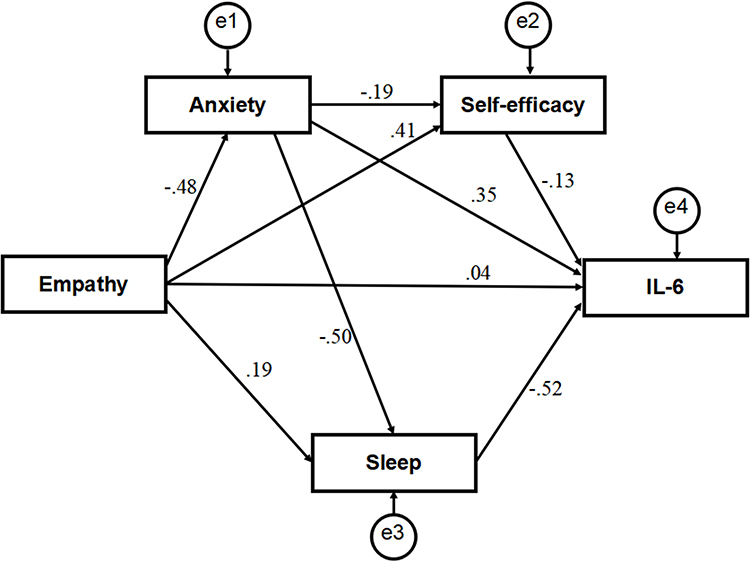 |
Figure 1 The model of relevance among patients’ perceptions of doctor-patient relational empathy and patients’ self-efficacy, anxiety, sleep quality and IL-6, with standardized beta weights. |
The normalized path coefficient is presented in Table 4. Patients’ perceptions of doctor-patient relational empathy (CARE) were negatively correlated with anxiety (β=−0.479, P < 0.05), and positively correlated with self-efficacy (β= 0.406, P < 0.05). Anxiety was negatively correlated with self-efficacy (β=−0.191, P < 0.05) and sleep (β=−0.499, P < 0.05). Patients’ perceptions of doctor-patient relational empathy had a positive association with sleep (β = 0.195, P < 0.05). Self-efficacy (β=−0.131, P < 0.05) and sleep (β=−0.516, P < 0.05) were negatively associated with serum IL-6, anxiety was positively associated with serum IL-6 (β= 0.346, P < 0.05). All the effects listed above were statistically significant. Patients’ perceptions of doctor-patient relational empathy showed no significant association with serum IL-6 (β= 0.038, P > 0.05). The above results indicate that hypothesis should be rejected.
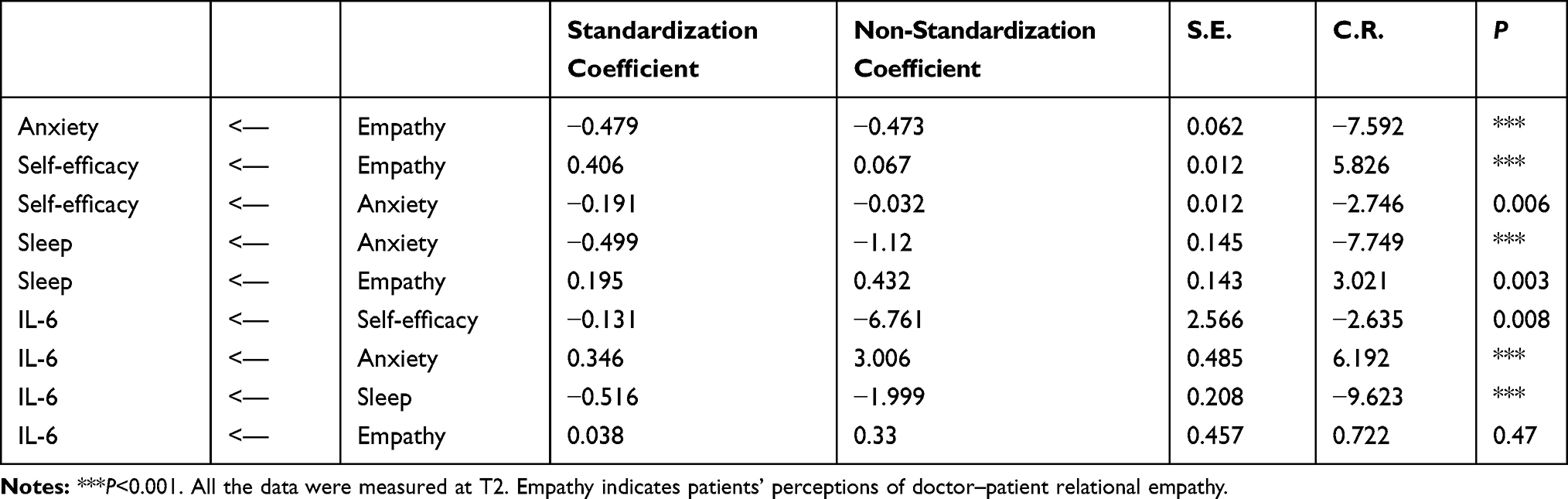 |
Table 4 Standardized Path Coefficients |
AMOS 21.0 was used to analyze the effect of mediation between variables. We set serum IL-6 as a dependent variable, self-efficacy, anxiety and sleep as intermediate variables, and patients’ perceptions of doctor-patient relational empathy as an independent variable for this analysis. The Bootstrap number was set to 5000, and the nonparametric percentile bootstrap method with deviation correction was chosen to test the degree of interaction between the variables. The results confirmed that when 0 was not contained in the confidence interval, the mediating effect was significant. In this study, five mediating paths existed between variables. Anxiety, sleep and self-efficacy worked had mediating roles between patients’ perceptions of doctor-patient relational empathy and serum IL-6, with effect sizes of −0.166 (95% CI: −2.091, −0.840), −0.101 (95% CI: −1.504, −0.326), and −0.053 (95% CI: −0.904, −0.109), respectively. In the path of patients’ perceptions of doctor-patient relational empathy-anxiety-self-efficacy-IL-6, when 0 was not contained in the confidence interval, the confidence interval of the effect was −0.012 (95% CI: −0.259, −0.020). According to the results, anxiety and self-efficacy played significant mediating roles between patients’ perceptions of doctor-patient relational empathy and serum IL-6. In the path of patients’ perceptions of doctor-patient relational empathy-anxiety-sleep-IL-6, when 0 was not contained in the confidence interval, the confidence interval of the effect was −0.123 (95% CI: −1.548, −0.699). Thus, anxiety and sleep played significant mediating roles between patients’ perceptions of doctor-patient relational empathy and serum IL-6; results are shown in Table 5.
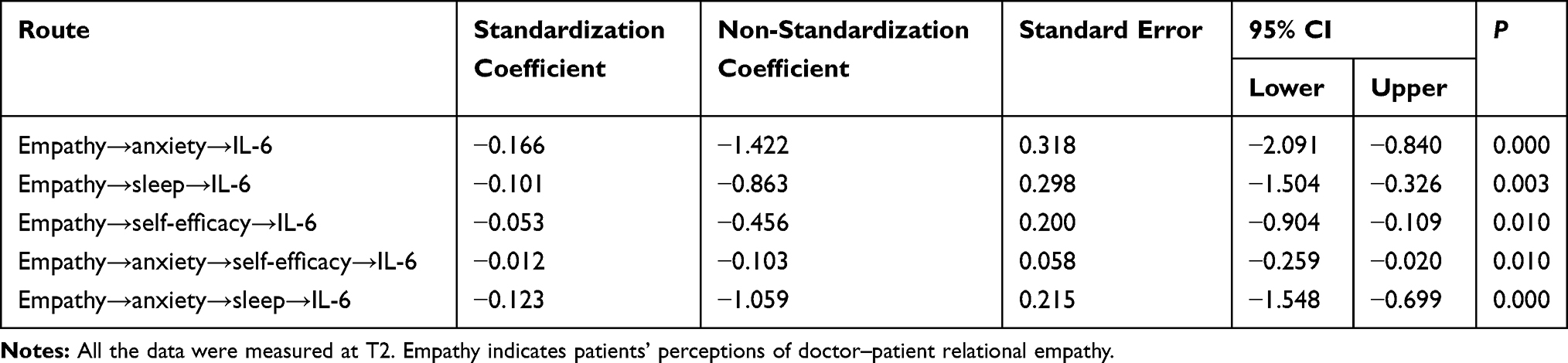 |
Table 5 Mediation Effect Analysis |
Discussion
Doctor Ability to Empathize and Patient Outcome
Doctor-patient empathy is the emotional interaction between doctors and patients, and the establishment of emotional community. This study analyzed the empathy between physicians and patients from two viewpoints: doctors’ ability to empathize, and patients’ perception of doctor’s empathy.
In terms of physicians’ empathy ability, our research confirmed that patients who were treated by doctors with high empathy presented better psychological well-being and lower serum IL-6 levels than patients treated by doctors with low empathy ability. This demonstrates that doctors who can strongly empathize with their patients are beneficial to those patients, as previous studies have also demonstrated. For example, patients whose doctors had high empathy ability showed improved results in glycosylated hemoglobin and low-density lipoprotein tests;27 and lower stigma, higher self-efficacy and level of NK cells.28
Previous studies have suggested that empathy is innate, but it can also be improved through training,29,30 and providing training to strengthen this ability in the medical staff is necessary. Empathy is a relatively stable ability, and doctors with this ability can show empathy with different patients.
Patient Perception of Doctor Empathy and Patients’ Outcome and Mechanisms
In this study, the positive impact of patients’ perception of doctor empathy on their physical and psychological indicators was demonstrated. In addition, patients’ perception of doctor empathy indirectly affects physiological indicators by influencing patients’ psychology, giving strength to our second hypothesis. The possible mechanisms are as follows:
First, patients’ perception of doctor empathy affects their anxiety, self-efficacy and sleep. The influence of empathy on patients’ psychology has been confirmed by previous studies. For example, patient-perceived nurses’ empathy had been confirmed to reduce the patients’ distress.31 This is especially likely for patients with cancer and chronic disease, as physician-patient empathy helps psychological adjustment.32
We believe that the reasons are as follows. First, by showing empathy, patients receive patient-centered care, and feel more love, support, concern and respect.33 Doctors also encourage patients to share their experiences and ideas, which helps to increase their self-efficacy and self-management ability when facing the disease, enhances their ability to cope with life and disease, and enhances their confidence in restoring health.34 Furthermore, empathy promotes the benefit of shared decision-making between doctors and patients, which increases patient autonomy, and helps them participate in the treatment and management of their own disease.35
Additionally, patients receive more personalized and in-depth health education after sharing their needs and opinions and being understood by the doctors, which helps to increase their compliance and reduce the uncertainty of disease. As a result, treatment effect and patients’ mood are better.36,37 Further, with empathetic treatment, patients’ can release negative emotions, and medical staff can respond to their story appropriately and give positive psychological guidance, which is of great benefit to patients’ mental health. Moreover, after empathizing with patients and sharing their stories, doctors may provide more humanistic care in the process of treatment, so patients’ mental state will be improved. Finally, the mental health of patients is improved, which affects serum IL-6. Similar to the results of this study, the effects of empathy on physiological indicators such as inflammatory markers have been confirmed in previous studies. For example, Rakel et al found that in patients with colds, neutrophil counts and IL-8 levels were lower in patients who perceived more empathy from doctors.38
The mechanism of the effect of mental health on proinflammatory factors has been investigated previously, and negative psychology, such as stress, can stimulate immune activation, leading to changes in cytokines.39 In addition, patients with positive psychology show strong adherence and disease management ability, which is conducive to the rehabilitation of the disease, so their proinflammatory factors are low.40 Previous studies have confirmed that sleep deprivation can also enhance cortisol and serum IL-6 levels.41
In addition, anxiety and self-efficacy, anxiety and sleep have chain-mediated effects on the impact of empathy on serum IL-6. Since empathy affects anxiety, anxiety can directly affect self-efficacy and sleep, and self-efficacy and sleep also affect serum IL-6. Anxiety affects self-efficacy because it acts as a negative psychological barrier to subjective initiative and positive behavior.42 Anxiety can directly affect sleep because anxiety affects people’s psychological state before falling asleep and delays the time to fall asleep.43 Long-term anxiety helps improve the arousal level of the brain when sleeping,44 increases cortisol, makes rhythm changes, and affects melatonin, which are closely related to sleep.45,46 Therefore, the emotional management of asthma patients should be included as a part of disease management.
Narrative Medicine: The Way to Realize Doctor-Patient Empathy
Narrative medicine and empathy are inseparable, and doctor-patient empathy is easy to achieve in the narrative process. The concept of narrative medicine was first proposed by Rita Charon at Columbia University in 2001. She described narrative ability as the ability to absorb, explain and respond to stories and other human predicaments.47 Narrative medicine enriches the medical staff’s understanding of life, suffering and death through patients’ stories, and encourages humanistic medical care in narration and empathy.48 Narrative medicine requires medical staff to listen carefully to patients’ stories and give them positive responses and appropriate guidance, which helps establish the emotional community between doctors and patients. As well, narrative medicine is the extension of narrative therapy, and narrative and empathy are part of a psychological intervention to some extent.49
At present, in medical education and clinical practice, the role of narrative medicine in enhancing the empathetic ability of medical staff and helping promote patients’ outcome has been well-established.50,51 Doctors should pay attention to practicing the concept of narrative medicine, and encourage patients to tell stories about their diseases, demonstrate empathy to patients in stories, and integrate narrative medicine into patient education. Narrative medicine education and empathy training should be included in medical education, especially in developing countries where medical humanities education is lacking, as to improve the physical and mental health of patients.
Limitations
This study has some limitations, including a small sample size, highlighting the need for further cohort and large sample size studies. Additionally, there are many factors that can affect serum IL-6, such as the severity of patient disease and heterogeneity of patients.
Conclusion
This study showed doctor-patient empathy, anxiety, self-efficacy and sleep may be factors that influence serum IL-6 in patients. Self-efficacy and sleep may play mediating roles in the effect of patients’ perception of doctor-patient relational empathy on serum IL-6. Therefore, clinical staff should pay attention to empathizing with patients in order to improve their physical and mental health.
Ethical Approval
The study procedures were in accordance with ethical standards. The sleep monitoring room was in the hospital and there were medical staff who could protect their health and safety. There was no risk from participating in the program, and the responses were treated confidentially. All participating patients were informed of the research process and provided written informed consent in accordance with the Declaration of Helsinki. The Wuhan University School of Medicine Ethics Committee approved the study (20160928).
Acknowledgment
We thank all the patients, who generously participated in the research at such a difficult time in their lives, and all the doctors who took part in the research.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Kawano T, Ouchi R, Ishigaki T, et al. Increased susceptibility to allergic asthma with the impairment of respiratory tolerance caused by psychological stress. Int Arch Allergy Imm. 2018;177(1):1–15. doi:10.1159/000488289
2. Goodwin RD, Pagura J, Cox B, Sareen J. Asthma and mental disorders in Canada: impact on functional impairment and mental health service use. J Psychosom Res. 2010;68(2):165–173. doi:10.1016/j.jpsychores.2009.06.005
3. Shen QY, Wu L, Wei CS, Zhou YN, Wu HM. Sevoflurane prevents airway remodeling via downregulation of VEGF and TGF-β1 in mice with OVA-induced chronic airway inflammation. Inflammation. 2019;42(3):1015–1022. doi:10.1007/s10753-019-00963-w
4. Wang F, Song Z, Zhang W, Xiao Y. Medical humanities play an important role in improving the doctor-patient relationship. Biosci Trends. 2017;11(2):134–137. doi:10.5582/bst.2017.01087
5. Wu SY, Zhu W, Li HY, Wang ZM. Relationship between job burnout and occupational stress among doctors in China. Stress Health. 2010;24(2):143–149. doi:10.1002/smi.1169
6. Liu X, Rohrer W, Luo A, Fang Z, He T, Xie W. Doctor-patient communication skills training in mainland China: a systematic review of the literature. Patient Educ Couns. 2014;98(1):3–14. doi:10.1016/j.pec.2014.09.012
7. Clever SL, Jin L, Levinson W, Meltzer DO. Does doctor-patient communication affect patient satisfaction with hospital care? Results of an analysis with a novel instrumental variable. Health Serv Res. 2008;43(5 Pt 1):1505–1519. doi:10.1111/j.1475-6773.2008.00849.x
8. Ballo P, Milli M, Slater C, et al. Prospective validation of the decalogue, a set of doctor-patient communication recommendations to improve patient illness experience and mood states within a hospital cardiologic ambulatory setting. Biomed Res Int. 2017;2017:2792131. doi:10.1155/2017/2792131
9. Jordan M, Amir D, Bloom P. Are empathy and concern psychologically distinct? Emotion. 2016;16(8):1107–1116. doi:10.1037/emo0000228
10. Neumann M, Scheffer C, Tauschel D, Lutz G, Wirtz M, Edelhäuser F. Physician empathy: definition, outcome-relevance and its measurement in patient care and medical education. GMS Z Med Ausbild. 2012;29(1):Doc11.
11. Yang NX, Xiao H, Cao YN, et al. Influence of oncology nurses’ empathy on lung cancer patients’ cellular immunity. Psychol Res Behav Manag. 2018;11:279–287. doi:10.2147/PRBM.S168649
12. Lomper K, Chudiak A, Uchmanowicz I, et al. Effects of depression and anxiety on asthma-related quality of life. Pneumonol Alergol Pol. 2016;84(4):212–221. doi:10.5603/PiAP.2016.0026
13. Urrutia I, Aguirre U, Pascual S, et al. Impact of anxiety and depression on disease control and quality of life in asthma patients. J Asthma. 2012;49(2):201–208. doi:10.3109/02770903.2011.654022
14. Dudeney J, Sharpe L, Jaffe A, et al. Anxiety in youth with asthma: a meta-analysis. Pediatr Pulmonol. 2017;52(9):1121–1129. doi:10.1002/ppul.v52.9
15. Marks R. Self-efficacy and arthritis disability: an updated synthesis of the evidence base and its relevance to optimal patient care. Health Psychol Open. 2014;1(1):2055102914564582. doi:10.1177/2055102914564582
16. Guo YJ, Tang Q, Gu Y. Measurements of self-efficacy in patients with chronic kidney disease: a literature review. Nephrol Nurs J. 2017;44(2):159–176.
17. Rincon M, Irvin CG. Role of IL-6 in asthma and other inflammatory pulmonary diseases. Int J Biol Sci. 2012;8(9):1281–1290. doi:10.7150/ijbs.4874
18. Glaus J, Vandeleur CL, von Känel R, et al. Associations between mood, anxiety or substance use disorders and inflammatory markers after adjustment for multiple covariates in a population-based study. J Psychiatr Res. 2014;58:36–45. doi:10.1016/j.jpsychires.2014.07.012
19. Fumaz CR, Gonzalez-Garcia M, Borras XO, et al. Psychological stress is associated with high levels of IL-6 in HIV-1 infected individuals on effective combined antiretroviral treatment. Brain Behav Immun. 2012;26(4):568–572. doi:10.1016/j.bbi.2012.01.001
20. Hojat M, Mangione S, Nasca TJ, et al. The jefferson scale of physician empathy: development and preliminary psychometric data. Educ Psychol Meas. 2001;61:349–365. doi:10.1177/00131640121971158
21. Hojat M, Mangione S, Kane GC, Gonnella GS. Relationships between scores of the Jefferson Scale of Physician Empathy (JSPE) and the Interpersonal Reactivity Index (IRI). Med Teach. 2005;27(7):625–628. doi:10.1080/01421590500069744
22. Mercer SW, Fung CS, Chan FW, Wong FY, Wong SY, Murphy D. The Chinese-version of the CARE measure reliably differentiates between doctors in primary care: a cross-sectional study in Hong Kong. BMC Fam Pract. 2011;12:43. doi:10.1186/1471-2296-12-43
23. Zigmond AS, Snaith RD. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67:361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
24. Bjelland I, Hahl AA, Hauq TT, Neckelmann D. The validity of the hospital anxiety and depression scale. An undated literature review. J Psychosom Res. 2002;52:69–77. doi:10.1016/S0022-3999(01)00296-3
25. Schwarzer R, Jerusalem M. Generalized self-efficacy scale. In: Weinman J, Wright S, Johnston M, editors. Measures in Health Psychology: A User’s Portfolio Causal and Control Beliefs. Windsor, UK: NFER-NELSON; 1995:35.
26. Zhang X, Zhan Y, Liu J, et al. Chinese translation and psychometric testing of the cardiac self-efficacy scale in patients with coronary heart disease in mainland China. Health Qual Life Outcomes. 2018;16(1):43. doi:10.1186/s12955-018-0872-4
27. Hojat M, Louis DZ, Markham FW, Wender R, Rabinowitz C, Gonnella JS. Physicians’ empathy and clinical outcomes for diabetic patients. Acad Med. 2011;86(3):359–364. doi:10.1097/ACM.0b013e3182086fe1
28. Yang NX, Xiao H, Wang W, et al. Effects of doctors’ empathy abilities on the cellular immunity of patients with advanced prostate cancer treated by orchiectomy: the mediating role of patients’ stigma and self-efficacy. Patient Prefer Adherence. 2018;12:1305–1314. doi:10.2147/PPA.S166460
29. Gerdes KE, Segal E. Importance of empathy for social work practice: integrating new science. Soc Work. 2011;56(2):141–148. doi:10.1093/sw/56.2.141
30. Bry K, Bry M, Hentz E, et al. Communication skills training enhances nurses’ ability to respond with empathy to parents’ emotions in a neonatal intensive care unit. Acta Paediatr. 2016;105(4):397–406. doi:10.1111/apa.2016.105.issue-4
31. Olson JK. Relationships between nurse-expressed empathy, patient-perceived empathy and patient distress. Image J Nurs Sch. 1995;27(4):317–322. doi:10.1111/j.1547-5069.1995.tb00895.x
32. Lelorain S, Brédart A, Dolbeault S, Sultan S. A systematic review of the associations between empathy measures and patient outcomes in cancer care. Psycho-Oncology. 2012;21(12):1255–1264. doi:10.1002/pon.v21.12
33. Piccolo LD. Empathy can make the difference. How? Patient Educ Counsel. 2018;101(7):1155–1156. doi:10.1016/j.pec.2018.05.010
34. Mercer SW, Neumann M, Wirtz M, Fitzpatrick B, Vojt G. General practitioner empathy, patient enablement, and patient-reported outcomes in primary care in an area of high socio-economic deprivation in Scotland–a pilot prospective study using structural equation modeling. Patient Educ Couns. 2008;73(2):240–245. doi:10.1016/j.pec.2008.07.022
35. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
36. Gaude GS, Hattiholi J, Chaudhury A. Role of health education and self-action plan in improving the drug compliance in bronchial asthma. J Family Med Prim Care. 2014;3(1):33–38. doi:10.4103/2249-4863.130269
37. Parker PA, Davis JW, Latini DM, et al. Relationship between illness uncertainty, anxiety, fear of progression and quality of life in men with favourable-risk prostate cancer undergoing active surveillance. BJU Int. 2016;117(3):469–477. doi:10.1111/bju.13099
38. Rakel D, Barrett B, Zhang Z, et al. Perception of empathy in the therapeutic encounter: effects on the common cold. Patient Educ Couns. 2011;85(3):390–397. doi:10.1016/j.pec.2011.01.009
39. Hamer M, Steptoe A. Association between physical fitness, parasympathetic control, and proinflammatory responses to mental stress. Psychosom Med. 2007;69(7):660–666. doi:10.1097/PSY.0b013e318148c4c0
40. Pierobon A, Bottelli ES, Ranzini L, et al. COPD patients’ self-reported adherence, psychosocial factors and mild cognitive impairment in pulmonary rehabilitation. Int J Chron Obstruct Pulmon Dis. 2017;12:2059–2067. doi:10.2147/COPD.S133586
41. Redwine L, Hauger RL, Gillin JC, Irwin M. Effects of sleep and sleep deprivation on interleukin-6, growth hormone, cortisol, and melatonin levels in humans. J Clin Endocrinol Metab. 2000;85(10):3597–3603. doi:10.1210/jcem.85.10.6871
42. Bandura A, Adams NE. Analysis of self-efficacy theory of behavior change. Cognitive Ther Res. 1977;1:287–310. doi:10.1007/BF01663995
43. Narisawa H. Anxiety and its related factors at bedtime are associated with difficulty in falling asleep. Tohoku J Exp Med. 2013;231(1):37–43. doi:10.1620/tjem.231.37
44. Benca RM, Peterson MJ. Insomnia and depression. Sleep Med. 2008;9:S3–S9. doi:10.1016/S1389-9457(08)70010-8
45. Katarina D, Janice N. The cortisol awakening response and major depression: examining the evidence. Neuropsych Dis Treat. 2015;11:1181–1189.
46. Cardinali DP, Srinivasan V, Brzezinski A, et al. Melatonin and its analogs in insomnia and depression. J Pineal Res. 2012;52:365–375. doi:10.1111/j.1600-079X.2011.00962.x
47. Charon R. Narrative medicine: a model for empathy, reflection, profession, and trust. JAMA. 2000;286(15):1897–1902. doi:10.1001/jama.286.15.1897
48. Charon R. Narrative medicine: form, function, and ethics. Ann Intern Med. 2001;134(1):83–87. doi:10.7326/0003-4819-134-1-200101020-00024
49. Hutto DD, Brancazio NM, Aubourg J. Narrative practices in medicine and therapy: philosophical reflections. Style. 2017;51(3):300.
50. Chen PJ, Huang CD, Yeh SJ. Impact of a narrative medicine programme on healthcare providers’ empathy scores over time. BMC Med Educ. 2017;17(1):108. doi:10.1186/s12909-017-0952-x
51. Knight I. The role of narrative medicine in the management of joint hypermobility syndrome/ehlers-danlos syndrome, hypermobility type. Am J Med Genet C Semin Med Genet. 2015;169C(1):123–129. doi:10.1002/ajmg.c.31428
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.