")
Back to Journals » Infection and Drug Resistance » Volume 13
Carbapenem-Resistant Klebsiella aerogenes Clinical Isolates from a Teaching Hospital in Southwestern China: Detailed Molecular Epidemiology, Resistance Determinants, Risk Factors and Clinical Outcomes
Authors Ma DY, Huang HY, Zou H, Wu ML , Lin QX, Liu B, Huang SF
Received 24 October 2019
Accepted for publication 13 January 2020
Published 19 February 2020 Volume 2020:13 Pages 577—585
DOI https://doi.org/10.2147/IDR.S235975
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sahil Khanna
De-Yu Ma, 1,* Han-Yu Huang, 2,* Hua Zou, 1 Meng-Lu Wu, 1 Qiu-Xia Lin, 1 Bo Liu, 3 Shi-Feng Huang 1
1Department of Laboratory Medicine, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2Department of Radiology, Chongqing Health Center for Women and Children, Chongqing, People’s Republic of China; 3Department of Burn and Plastic Surgery, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bo Liu
Department of Burn and Plastic Surgery, The First Affiliated Hospital of Chongqing Medical University, Chongqing, China, No. 1 Friendship Road, Yuzhong District, Chongqing 400016, People’s Republic of China
Tel +86-18623007069
Fax +86-023-89012093
Email [email protected]
Shi-Feng Huang
Department of Clinical Laboratory, The First Affiliated Hospital of Chongqing Medical University, Chongqing, China, No. 1 Friendship Road, Yuzhong District, Chongqing 400016, People’s Republic of China
Tel +86-18623027077
Fax +86-023-89012513
Email [email protected]
Purpose: Little is known about the epidemiology and carbapenem-resistance determinants of carbapenem-resistant K. aerogenes (CRKA) isolated from a single medical center. The present study was initiated to characterize the molecular epidemiology and the carbapenem-resistance mechanisms of CRKA isolated during 2012– 2018 from a teaching hospital in southwest China, and to investigate the risk factors and clinical outcomes of CRKA infections as well.
Methods: Pulsed-field gel electrophoresis (PFGE) was employed for epidemiological analysis. PCR amplification and DNA sequencing were used to examine the antibiotic-resistance determinants. Plasmids were extracted and characterized by PCR-based replicon typing and conjugation assays. In order to further investigate the risk factors and clinical outcomes of CRKA infections, a retrospective case–control study was also performed.
Results: PFGE analysis showed 32 different PFGE patterns among the 36 non-duplicated CRKA strains collected. Most of the isolates harbored multi-drug resistance (MDR) genes, including 2 (5.6%) carrying blaNDM-1, 1 (2.8%) harboring blaKPC-2, 13 (36.1%) carrying ESBL genes, 23 (63.9%) carrying ampC genes, 34 (94.4%) carrying quinolone resistance determinants (QRD) genes and 9 (25%) carrying aminoglycoside resistance determinants (ARD) genes. The outer membrane porins, OmpE35 and OmpE36, were, respectively, lost in 4 and 2 isolates. The efflux pump inhibition experiments were positive in 25 (69.4%) of the CRKA strains. Multivariate analysis indicated that hypo-albuminaemia, invasive procedures, and carbapenem exposure were independent risk factors for acquiring CRKA infections.
Conclusion: No clonality relationship was identified among most of the 36 CRKA isolates. The over-expression of ESBLs and AmpC coupled with the efflux pumps contributed to carbapenem resistance in K. aerogenes. Additionally, this is the first report of CRKA isolate co-harboring blaNDM-1, blaCTX-M-15, blaEBC, blaACC, acc (6ʹ)-Ib, armA, qnrD and loss of OmpE36 in China. Hypo-albuminaemia, invasive procedures and carbapenem exposure were associated with acquisition of CRKA infections.
Keywords: case-control study, blaNDM-1, blaKPC-2, porins, efflux pumps
Introductions
With the increasing emergence of multi-drug-resistant (MDR) bacteria, carbapenems have been used as the last-line antibiotic for treating severe infections caused by gram-negatives and displayed strong activity against AmpC β-lactamase and/or ESBL hyper-producing isolates.1 Unfortunately, since the introduction of carbapenems into the clinical practice, nosocomial infections caused by carbapenem-resistant Enterobacteriaceae (CRE) have been increasing rapidly and posing serious challenges to the clinical management of infections caused by the gram-negatives.2 To help direct research and development efforts toward the production of novel drugs, CRE was recently listed as one of the three critical-priority pathogens by the World Health Organization (WHO).3
Klebsiella aerogenes (K. aerogenes), formerly described as Enterobacter aerogenes, is a gram-negative, rod-shaped, facultative anaerobic bacteria belonging to the family Enterobacteriaceae.4 It is an important nosocomial pathogen associated with a wide variety of infections including pneumonia, bacteremia, urinary tract and surgical site infections.5 Most importantly, K. aerogenes exhibited MDR phenotype during various hospital outbreaks.5,6
Although K. aerogenes belongs to the family Enterobacteriaceae, its resistance mechanisms against carbapenems remain relatively unclear due to the limited amount of work performed to date in this field. With the successive and increasing isolation of CRKA in our center in recent years, and the limited amount of work performed to date in CRKA, more attention has been evoking concerning its molecular epidemiology and carbapenem-resistance mechanisms. The present study was initiated to characterize the molecular epidemiology and the carbapenem-resistance mechanisms of CRKA isolated during 2012–2018 from a teaching hospital in southwest China, and to investigate the risk factors and clinical outcomes of CRKA infections as well.
Previous studies showed that carbapenem resistance in K. aerogenes mainly arises from the over-expression of ESBLs or AmpC enzymes coupled with mutations affecting membrane permeability.7 Carbapenemases, such as KPC, NDM, and OXA-48, have also been reported in clinical K. aerogenes isolates from different countries.8–10 However, the risk factors, molecular epidemiology, and clinical outcomes pertaining to CRKA infections in a single medical center have not been systematically characterized.
The present study was initiated: (i) to describe the prevalence of clinical CRKA isolates collected successively for approximately 6 years; (ii) to identify the carbapenem-resistance mechanisms and the clonal relatedness among CRKA strains; and (iii) to characterize the risk factors and clinical outcomes associated with the acquisition of CRKA infections.
Materials and Methods
Bacterial Strains
This retrospective study was performed in the First Affiliated Hospital of Chongqing Medical University, a 3200-bed tertiary hospital located in Southwest China. A total of 892 clinical K. aerogenes strains were isolated and identified from January 2012 to December 2018 by using the VITEK2 compact or VITEK MS (bioMerieux, Hazelwood, MO, United States) automated system at the department of laboratory medicine, among which 36 strains were resistant to at least one carbapenem on the basis of antimicrobial susceptibility testing results determined by the broth microdilution method, with the criteria of MIC of ≥2 mg/L for ertapenem, ≥4 mg/L for imipenem, and ≥4 mg/L for meropenem; and 5 strains were intermediate to at least one carbapenem, with the criteria of MIC of = 1 mg/L for ertapenem, = 2 mg/L for imipenem, and = 2 mg/L for meropenem (Supplementary Figure 1). Only the first isolate from each individual patient was included in this study.
Antimicrobial Susceptibility Testing and Activity of the Efflux Pumps
Initial antibiotic susceptibility testing was performed by using the VITEK2 compact (bioMerieux, Hazelwood, MO, USA) automated system. MICs of ertapenem (ETP), imipenem (IPM), and meropenem (MEM) were reassessed manually using the broth microdilution method and the results were categorized in accordance with the Clinical and Laboratory Standards Institute, M100-S28 (CLSI M100-S28) interpretive criteria. The activities of the efflux pumps were examined by comparing the MICs to carbapenems among resistant isolates in the presence and absence of carbonyl cyanide m-chlorophenylhydrazone (CCCP) as an efflux pump inhibitor. At least a two doubling dilution decrease in the resistance level was considered a positive result.10 K. aerogenes ATCC13048 was used as the reference strain.
PFGE
The molecular epidemiology of all the CRKA strains was determined by pulsed-field gel electrophoresis (PFGE) after total chromosomal DNA digestion with XbaI in accordance with a previous report.11 The genomic DNA restriction patterns of the isolates were analyzed and interpreted according to the previously proposed criteria.12
Detection of Antibiotic Resistance Genes
PCR analyses for the presence of carbapenemase-encoding genes (blaKPC, blaVIM, blaIMP, blaNDM, blaSME, blaOXA-48, blaOXA-23-like, blaOXA-58-like) were performed by using primers and conditions described previously.13 In addition, ESBLs genes (blaCTXM, blaTEM, blaSHV, blaOXA-1), AmpC genes (blaEBC, blaACC, blaACT, blaDHA, blaMOX), ARD genes (acc(6ʹ)-Ib, armA, rmtB), QRD genes (qnrA, qnrB, qnrC, qnrS, qnrD, acc(6ʹ)-Ib-cr), and porin genes (ompE35 and ompE36) were also investigated by PCR with previously designed primers and conditions.14 DNA sequencing with the BLAST program (http://www.ncbi.nlm.nih.gov/BLAST) was used to confirm the variants of the resistance genes.
Conjugation and Plasmid Replicon Typing
To confirm whether the carbapenemase genes were located on the plasmids, the carbapenemase-producing strains were collected and conjugation experiments were performed according to the previously described method.15 All the carbapenemase-producing strains were served as the donors, while the E. coli EC600 was employed as the recipient strain. Potential transconjugants were isolated on Mueller-Hinton agar plates containing 8 mg/L ertapenem and 256 mg/L rifampicin. The transconjugants were tested for antimicrobial susceptibility by the VITEK2 compact system, and the presence of resistance determinants was confirmed by PCR. Additionally, all CRKA strains plasmids were determined by using the PCR-based replicon typing method as described previously.16
Risk Factors and Clinical Outcomes of CRKA Infections
We conducted a retrospective case–control study to explore the risk factors and clinical outcomes of patients infected with CRKA from 2012 to 2018 in Chongqing, China. All hospitalized patients with K. aerogenes infections were included. Patients with CRKA infections were included as cases. Controls were identified as patients with carbapenem-susceptible K. aerogenes (CSKA) infections with well-balanced demographic characteristics, pre-existing medical conditions, and immune-compromising comorbidities as compared with the cases. Clinical and epidemiological data, including the demographics, underlying diseases, the primary diagnosis at admission, invasive procedures prior to the isolation of CRKA, previous exposures of antibiotic within 3 months, and the clinical outcomes, were extracted from the patients’ electronic medical records system and clinical microbiology laboratory database.
Statistical Analysis
All analyses were performed using SPSS v.22.0 software (SPSS Inc., Chicago, IL, United States). Univariate analyses were performed separately for each of the variables. Categorical variables were compared using a chi-square test or Fisher’s exact test as appropriate. Continuous variables were compared using Student’s t-test (normally distributed variables) and Wilcoxon rank-sum test (non-normally distributed variables) as appropriate. The odds ratio (OR) and 95% confidence interval (CI) were calculated to evaluate the strength of any association. Variables with P≤0.05 on univariate analysis were evaluated as potential covariates in a stepwise multivariate logistic regression model. For all calculations, P <0.05 was considered statistically significant.
Ethical Considerations
The data and samples analyzed in the present study were obtained in accordance with the standards and approved by the Chongqing Medical University Institutional Review Board and the Biomedical Ethics Committee. For this study, samples were collected at the microbiology laboratory of our hospital, with no contact with the patients. This study was retrospective and there was no patient identification performed during data collection. Therefore, the ethics committee determined that informed consent was not required.
Results
General Characteristics and Antimicrobial Susceptibility Profiles of 36 CRKA Isolates
During the 6-year period of the study, a total of 36 strains, which are resistant to at least one of the carbapenems tested (ertapenem, imipenem and meropenem), were isolated as CRKA. As shown in Table 1, these non-duplicated strains were mainly isolated from urine (10/36; 27.8%), followed by drainage-liquid (9/36; 25%), sputum (4/36; 11.1%), and bile (3/36; 8.3%). Among the 36 isolates, all were ertapenem-resistant, 72.2% (26/36) and 36.1% (13/36) of the isolates were resistant to imipenem and meropenem, respectively. In addition, CRKA isolates showed variable resistance rates to other antimicrobials: ceftazidime (35/36, 97.2%), ceftriaxone (32/36, 88.9%), cefepime (13/36, 36.1%), gentamicin (13/36, 36.1%), amikacin (5/36, 13.8%), tobramycin (9/36, 25.0%), ciprofloxacin (15/36, 41.6%), levofloxacin (12/36, 33.3%). Notably, 55.5% (20/36) of the CRKA isolates were classified as MDR as they were resistant to three or more classes of antimicrobials.
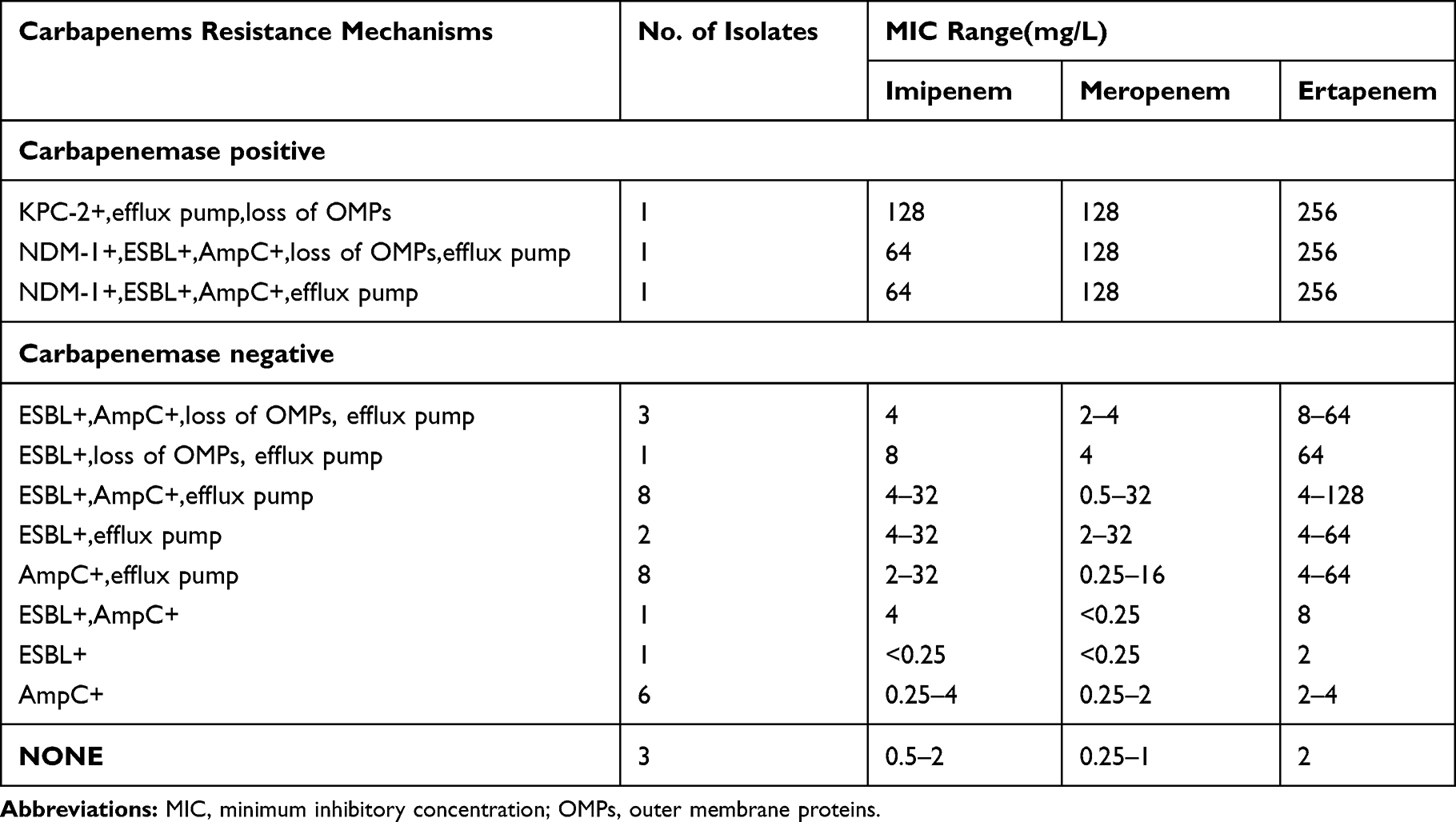 |
Table 1 Distribution and Corresponding Carbapenem MIC Ranges for Strains with Different Resistance Determinants |
Characterization of the Molecular Epidemiology of the 36 CRKA Isolates
The characteristics of the molecular epidemiology of the 36 CRKA strains are displayed in Figure 1. All the 36 CRKA isolates were grouped into 32 different PFGE patterns and exhibited a high degree of genetic diversities. While 8 isolates were grouped into 4 different PFGE patterns, with two individual isolates showing almost the same typing, the left 28 isolates belonged to 28 different PFGE patterns. Most notably, the two isolates (No. 8 and No. 9) belonging to pattern 20 were shown to be isolated from the same ward during the same time period. Nevertheless, the two isolates belonging to patterns 5, 22 and 23, respectively, were isolated from different wards.
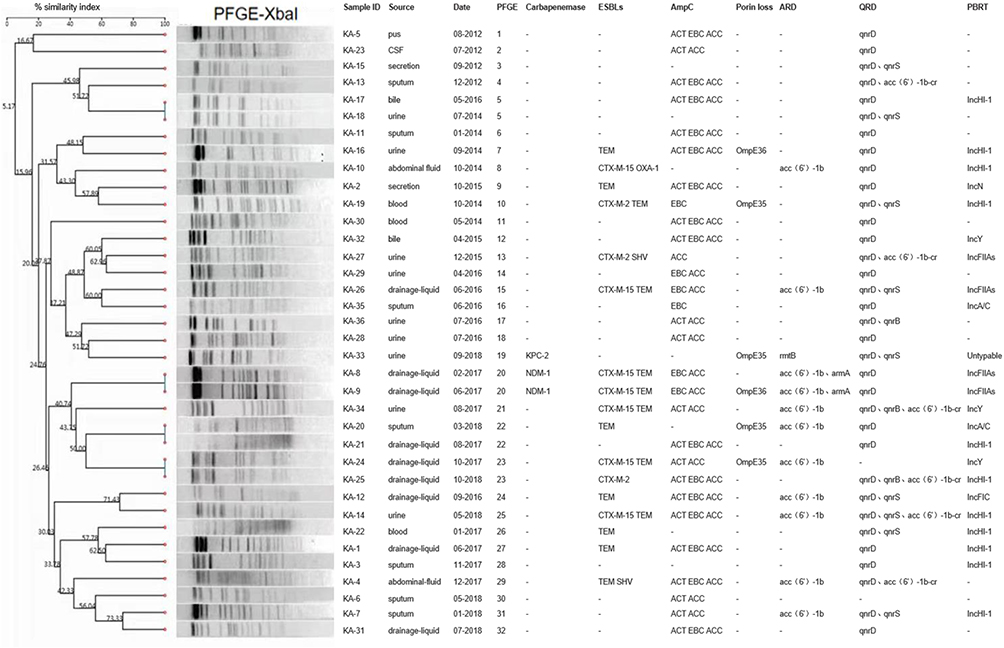 |
Figure 1 PFGE-based dendrogram of CRKA strains. Sample ID, source of initial isolation, and demographic information are included along each PFGE lane. Abbreviations: ESBLs, Extended-Spectrum Beta-Lactamases; QRD, quinolone resistance determinants; ARD, aminoglycoside resistance determinants; PBRT, PCR-based replicon type; “-”, not detected. |
Analysis of Molecular Resistance Mechanisms
Of the 36 CRKA isolates, 3 (8.3%) were identified as carbapenemase-producers: 2 (5.6%) with blaNDM-1, and 1 (2.8%) with blaKPC-2. In addition, these CRKA isolates showed relatively higher expression rates for ESBL (13/36, 36.1%) and AmpC genes (23/36, 63.9%), with 25% of the strains being positive for both genes. The prevalence of ESBLs/AmpC genes in the 36 isolates was presented as follows: 14 (38.9%) produced TEM, 7 (19.4%) produced CTX-M-15, 2 (5.6%) produced SHV, 3 (8.3%) produced CTX-M-2 and 1 (2.8%) produced OXA-1; 21 (58.3%) produced EBC, 27 (75%) produced ACC and 22 (61.1%) produced ACT. The prevalence of QRD genes in the 36 CRKA strains was 34 out of 36 (94.4%), with 34 strains carrying qnrD, 9 carrying qnrS, 3 carrying qnrB, and 6 carrying aac(6ʹ)-Ib-cr. The prevalence of ARD genes was 12 out of 36 (25%), and the genes aac (6ʹ)-Ib, armA, and rmtB were detected in 12, 2, and 1 of the 36 isolates, respectively. The outer membrane porin genes ompE35 and ompE36 were lost in 4 and 2 isolates, respectively. Sequencing analysis of the ompE35 and ompE36 genes of these CRKA isolates confirmed no mutations or insertions. Moreover, the addition of the efflux pump inhibitor CCCP reduced the MICs to ertapenem by 2–4 log2 dilutions in 69.4% (25/36) of the CRKA isolates. On the other hand, we have also provided the clinical and genotypic characteristics of the 5 CIKA strains having borderline MIC values (i.e., MIC = 1 mg/L for ertapenem, 2 mg/L for imipenem, and 2 mg/L for meropenem) as in Supplementary Table 1. None of them produced carbapenemases at detectable levels as has been demonstrated by the negative results from both the simplified Carbapenem Inactivation Method (sCIM) and PCR screening of the carbapenemase genes including blaKPC, blaVIM, blaIMP, blaNDM, blaSME, blaOXA-48, blaOXA-23-like, and blaOXA-58-like.
Conjugation and Plasmid Replicon Typing Analysis
Conjugation experiments showed that the transconjugants were obtained from two strains carrying blaNDM-1 at frequencies of 2×10−5 per recipient cell, while no transconjugants were obtained from the blaKPC-2-carrying strain. Susceptibility testings (Table 2) confirmed that the transconjugants exhibited resistance to the tested carbapenems and cephalosporins, and demonstrated significantly reduced susceptibilities to aminoglycosides, while remained susceptible to fluoroquinolones. PCR assays indicated that blaNDM-1, blaTEM, blaCTX-M-15, acc(6ʹ)-1b, and armA were successfully transferred by conjugation (Table 2). On the other hand, PCR-based replicon typing revealed that the CRKA plasmids belonged to the groups IncHI-1 (n =11), IncFIIAs (n = 4), IncY (n = 3), IncA/C (n = 2), IncN (n = 1), and IncFIC (n = 1) (Table 2).
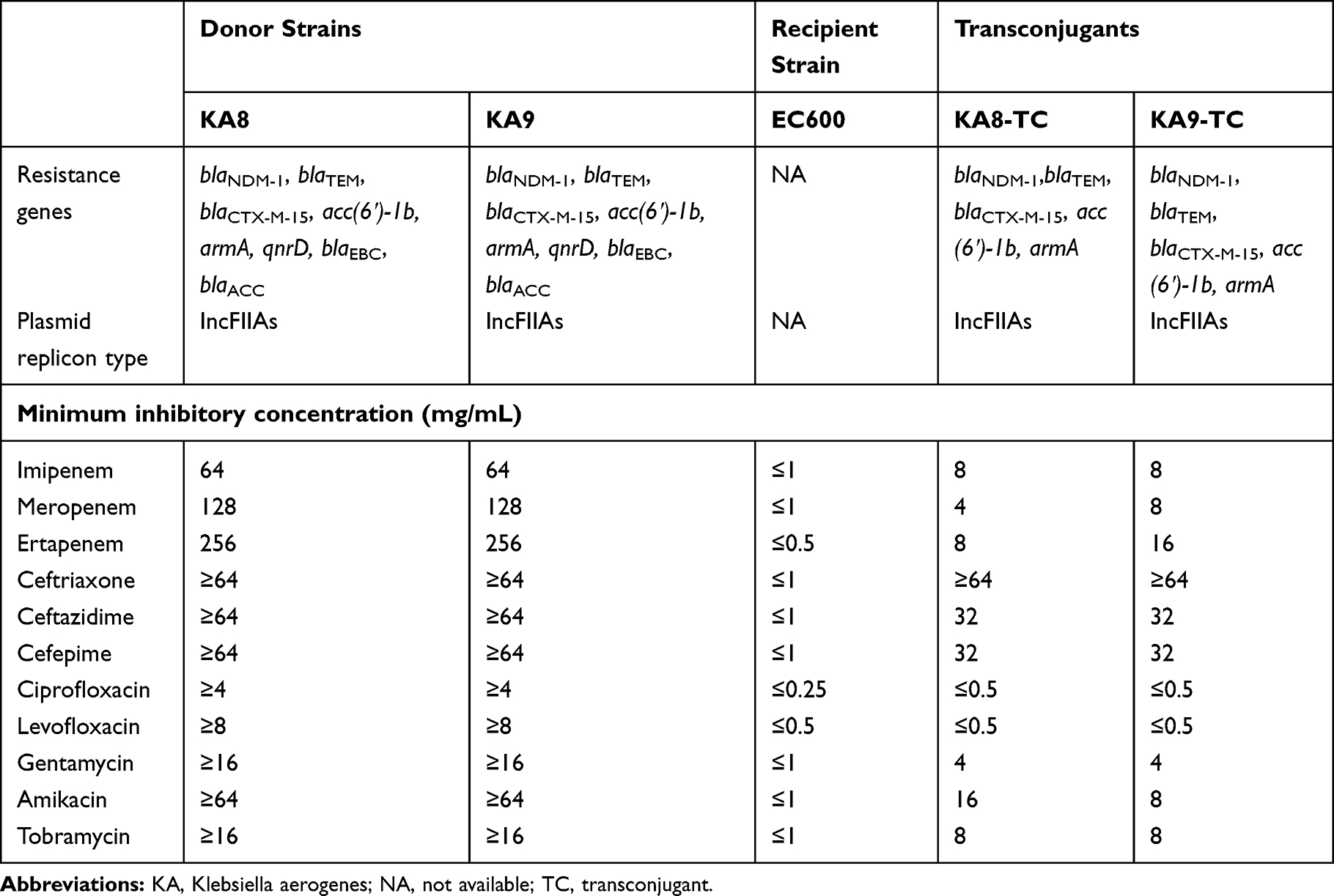 |
Table 2 Antibiotic Resistance Genes and Susceptibility Profiles in Donor, E. Coli EC600, and Transconjugants |
Risk Factors and Clinical Outcomes of CRKA Infections
The risk factors and outcomes of patients with CRKA infections are shown in Table 3. The univariate analysis indicated that hepatobiliary disease, gastrointestinal disease, hypo-albuminaemia, urinary tract infection, skin infection, drainage tube use, urinary catheter use, central venous catheter use, previous exposure to penicillins and carbapenems were significantly more frequent in patients with CRKA infections (P< 0.05). A multivariate logistic regression analysis showed that hypo-albuminaemia (OR [Odd ratio]: 3.57, 95% CI [Confidence Interval]: 1.04–12.48, P=0.044), drainage tube use (OR: 5.78, 95% CI:1.81–18.47, P=0.003), urinary catheter use (OR: 3.32, 95% CI:1.03–10.68, P=0.044), and previous exposure to carbapenems (OR: 5.00, 95% CI: 1.29–19.40, P=0.020) were independent risk factors for the acquisition of CRKA infections. For clinical outcomes, we found significant differences in post-culture length of stay (19 days vs 9 days; P =0.003) and total length of hospital stay (52.5 days vs 24 days; P <0.001) between cases and controls. In addition, 4 (11.1%) patients infected with CRKA and 5 (3.8%) patients infected with CSKA died during hospitalization, and no significant difference in in-hospital mortality rate was observed between the two groups.
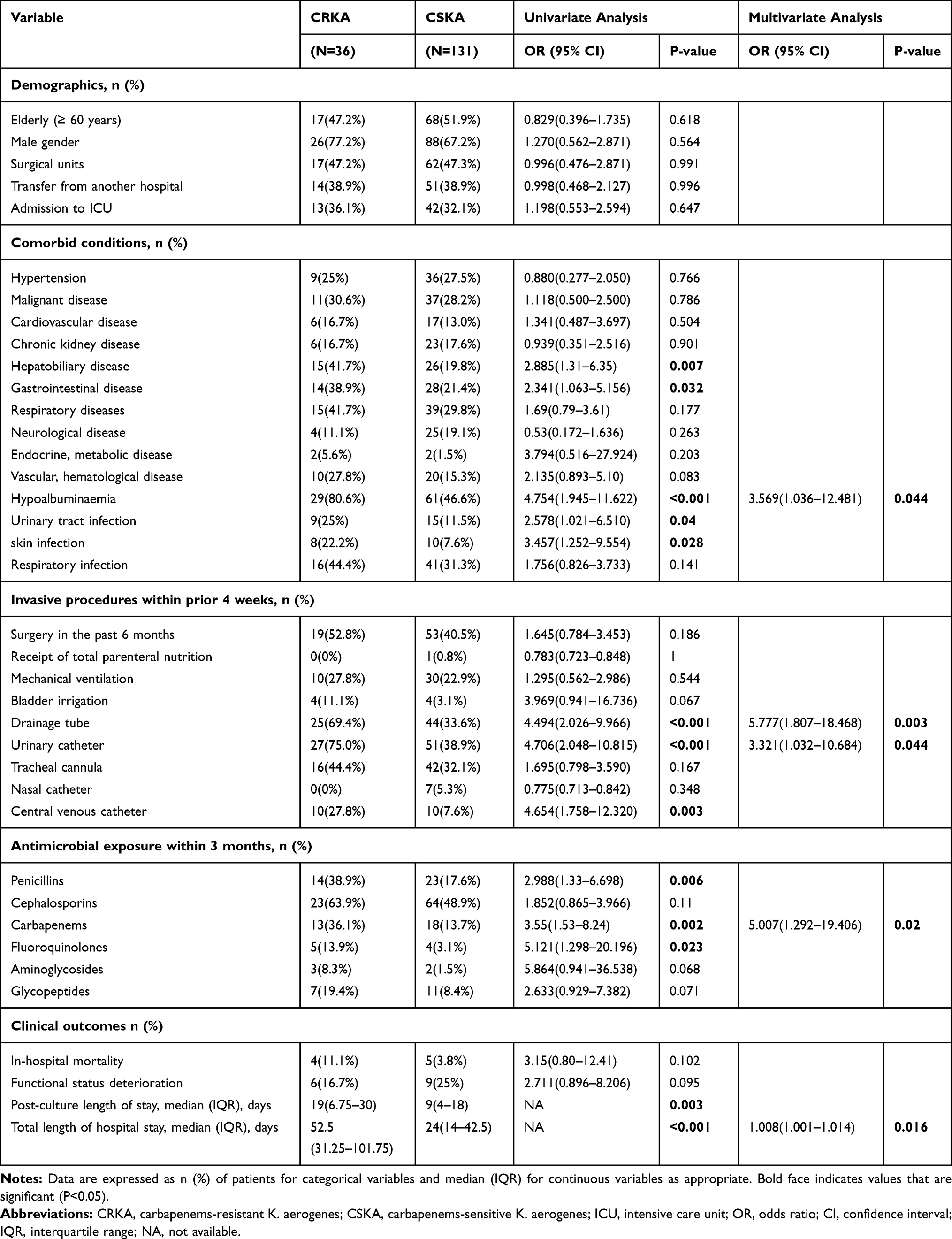 |
Table 3 Univariate and Multivariate Analyses of Risk Factors and Outcomes for Patients Infected with CRKA Isolates Compared with CSKA Isolates |
Discussion
Despite the fact that Enterobacter cloacae is now the most frequently isolated Enterobacter sp. in clinical settings and the species expressing the widest panel of new β-lactamases or carbapenemases, K. aerogenes more easily causes septic shock in infected patients, is associated with higher mortality (39% of patients), shows greater virulence, and have a broad ability to acquire antibiotic resistance mechanisms.4 Consequently, the issue of CRKA infection deserves particular attention. Our main findings of the present study were presented as follows:
First, previous studies indicated that the mechanisms underlying carbapenem resistance in K. aerogenes were carbapenemase-independent and were attributed to both AmpC β-lactamase over-expression and mutations affecting membrane permeabilities.4 However, in this study, we have demonstrated that carbapenem resistance in K. aerogenes was mainly associated with the over-expression of ESBLs and/or AmpC enzymes coupled with the efflux pumps, highlighting that efflux pump inhibitors (EPIs) could be used as an antibiotic adjuvant in CRKA infections. Of note, while the prevalence of carbapenemases was particularly low (3/36, 8.33%) in CRKA isolates, those carbapenemase-producing strains, which also co-expressed other drug-resistance determinants, showed the highest MICs for multiple antibiotics. Notably, even though no specific carbapenem-resistance mechanisms were detected, ten isolates (ESBL only, n=1; AmpC only, n=6; none, n=3) showed MIC values of ≥2 mg/L for ertapenem (Table 1), and the possible carbapenem-resistance mechanism might be due to mutations in penicillin-binding proteins (PBPs). To the best of our knowledge, this is also the first report on CRKA isolate co-harboring blaNDM-1, blaCTX-M-15, blaEBC, blaACC, acc (6)-Ib, armA, qnrD with loss of ompE36 in China.
Second, we performed conjugation experiments on carbapenemase-producing strains, and found that all the blaNDM-1 plasmids could be successfully transferred by conjugation. But the repeated transfer of blaKPC-2 was unsuccessful. The most plausible explanation of this result is that blaNDM-1 was carried on self-transmissible plasmids, while blaKPC-2 was located on non-self-transmissible plasmids or on the chromosome. Previous studies have shown the emergence of blaNDM-1 in China, with most of them being carried on the IncFIIAs-type plasmids.17 In this study, plasmids from all the blaNDM-1-carrying strains (including those in the donors and the transconjugants) also belonged to the plasmid replicon type IncFIIAs. In addition, the plasmids containing blaKPC-2 were un-typable. It is worth noting that multiple resistance genes were found to be co-expressed in the same self-transmissible plasmids, which might have allowed the accumulation and spread of multiple drug-resistance determinants.
Third, no clonality relationship was identified among most of the CRKA isolates. Therefore, the prevalence of these CRKA isolates could not be attributed to the spread of clonal dissemination. Interestingly, the two blaNDM-1-carrying isolates belonging to the PFGE pattern 20 were isolated from the same ICU ward in October 2014. This local spread from patient to patient appears to be caused by inadequate attention to infection control measures, especially handwashing.
Fourth, we initially performed an epidemiological investigation to assess the clinical predictors and outcomes for CRKA infections. In this retrospective case–control study, hypo-albuminaemia, drainage tube use, urinary catheter use, and previous carbapenem exposure were demonstrated to be independently associated with CRKA infections. One possible explanation for hypo-albuminaemia as an independent risk factor may be due to the hosts’ poor immunity and functional status. Moreover, the invasive medical procedures might have destroyed their natural barrier functions, promoted the formation of microbial biofilms, and possibly led to catheter-related infections, thus increasing mortality in these patients.18 Given that invasive procedures such as the use of drainage tube and urinary catheter were potential risk factors, infection control measures preventing the microbial colonization of the insertion sites are necessary. In addition, our study identified carbapenem exposure as being associated with CRKA infections for case patients, in agreement with previous reports on the assessment of CRE.19 One possibility is that inappropriate antibiotic therapy may disrupt the gastrointestinal microflora and eradicate susceptible competing strains, thus elevating the incidences of CRE infections.20 Considering that patients receiving carbapenem treatment may be exposed to further risk for CRKA isolation, it is crucial to maintain an effective administration of antimicrobial agents to avoid their further spread. Many outbreaks of CRE have been described in ICUs, where there were more patients with severe underlying diseases, thus conferring a greater possibility of contaminating life support equipment. Moreover, use of broad-spectrum antibiotics can further place patients at higher risk for poor outcomes.21,22 However, admission to ICU was not demonstrated to be a significant risk factor. This could be explained by the limited cases in our study. For the clinical outcomes, our results demonstrated a significant difference in total length of stay between case and control group, probably due to the fact that the patients infected with CRKA were generally at a higher risk of poorer outcomes than those with CSKA infections. Unexpectedly, no statistical significance was observed in in-hospital mortality, probably due to the small size of CRKA cases in our study.
Our study had several limitations. First, we did not perform real-time reverse transcription PCR to determine the levels of expression of outer membrane porins and efflux pumps in mRNA levels. Second, the significance of specific sequence types (STs) of CRKA remains unknown, and MLST is still needed for understanding the characteristics of each CRKA isolate. Finally, this was a retrospective single-center case–control study with a relatively small sample size, and our results might not be applicable to other settings.
In conclusion, this study provided the first comprehensive report of molecular epidemiology, carbapenem-resistance mechanisms, and risk factors for CRKA infections over a six-year period in one medical center. Our data showed that the production of ESBL and/or AmpC enzymes coupled with the efflux pumps was the main carbapenem-resistance mechanism for CRKA. As far as we know, this is the first report on MDR K. aerogenes isolate co-harboring blaNDM-1, blaCTX-M-15, blaEBC, blaACC, acc (6ʹ)-Ib, armA, qnrD with loss of OmpE36 in China. In addition, our findings showed that hypo-albuminaemia, invasive procedures such as drainage tube and urinary catheter use, and previous carbapenem exposure could be independently associated with the CRKA infections. Therefore, appropriate antimicrobial therapy and strict infection control measures are critical to reduce the frequency of CRKA infections.
Acknowledgments
This study was supported in part by the National Natural Science Foundation of China (Grant No. 81772239 and 31500749), the Science and Technology Research Program of Chongqing Municipal Education Commission (Grant No. KJ1500235 and KJ1702022), and the Medical Research Program of Chongqing Health and Family Planning Commission (No. 2018MSXM009 and 2016MSXM001).
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest.
References
1. D’Angelo RG, Johnson JK, Bork JT, Heil EL. Treatment options for extended-spectrum beta-lactamase (ESBL) and AmpC-producing bacteria. Expert Opin Pharmacother. 2016;17(7):953–967. doi:10.1517/14656566.2016.1154538
2. Potter RF, D’Souza AW, Dantas G. The rapid spread of carbapenem-resistant Enterobacteriaceae. Drug Resist Updat. 2016;29:30–46. doi:10.1016/j.drup.2016.09.002
3. WHO. WHO publishes list of bacteria for which new antibiotics are urgently needed. WHO Media Centre. 2017; 1–4. doi:/entity/mediacentre/news/releases/2017/bacteria-antibiotics-needed/en/index.html
4. Davin-Regli A, Lavigne JP, Pages JM. Enterobacter spp.: update on taxonomy, clinical aspects, and emerging antimicrobial resistance. Clin Microbiol Rev. 2019;32(4):e00002–19. doi:10.1128/CMR.00002-19
5. Malek A, McGlynn K, Taffner S, et al. Next-generation-sequencing-based hospital outbreak investigation yields insight into Klebsiella aerogenes population structure and determinants of carbapenem resistance and pathogenicity. Antimicrob Agents Chemother. 2019;63(6). doi:10.1128/AAC.02577-18
6. Salso S, Culebras E, Andrade R, Picazo JJ. Outbreak of TEM-24-producing Enterobacter aerogenes in a Spanish hospital. J Clin Microbiol. 2003;9(3):299–305. doi:10.1089/107662903322286517
7. Davin-Regli A, Pages JM. Enterobacter aerogenes and Enterobacter cloacae; versatile bacterial pathogens confronting antibiotic treatment. Front Microbiol. 2015;6:392. doi:10.3389/fmicb.2015.00392
8. Khajuria A, Praharaj AK, Kumar M, et al. Carbapenem resistance among Enterobacter species in a Tertiary Care Hospital in Central India. Chemother Res Pract. 2014;2014:972646. doi:10.1155/2014/972646
9. Franolić I, Bedenić B, Beader N, et al. NDM-1-producing Enterobacter aerogenes isolated from a patient with a JJ ureteric stent in situ. CEN Case Rep. 2018;8(1):38–41. doi:10.1007/s13730-018-0360-z
10. Torres E, López-Cerero L, Del Toro MD, Pascual Á. First detection and characterization of an OXA-48-producing Enterobacter aerogenes isolate. Enferm Infecc Microbiol Clin. 2014;32(7):469–470. doi:10.1016/j.eimc.2013.10.008
11. He J, Jia X, Yang S, et al. Heteroresistance to carbapenems in invasive Pseudomonas aeruginosa infections. Int J Antimicrob Agents. 2018;51(3):413–421. doi:10.1016/j.ijantimicag.2017.10.014
12. Tenover FC, Arbeit RD, Goering RV, et al. Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: criteria for bacterial strain typing. J Clin Microbiol. 1995;33(9):2233–2239. doi:10.1128/JCM.33.9.2233-2239.1995
13. Zhang C, Xu X, Pu S, et al. Characterization of carbapenemases, extended spectrum beta-lactamases, quinolone resistance and aminoglycoside resistance determinants in carbapenem-non-susceptible Escherichia coli from a teaching hospital in Chongqing, Southwest China. Infect Genet Evol. 2014;27:271–276. doi:10.1016/j.meegid.2014.07.031
14. Babouee Flury B, Ellington MJ, Hopkins KL, Turton JF, Doumith M, Woodford N. The differential importance of mutations within AmpD in cephalosporin resistance of Enterobacter aerogenes and Enterobacter cloacae. Int J Antimicrob Agents. 2016;48(5):555–558. doi:10.1016/j.ijantimicag.2016.07.021
15. Borgia S, Lastovetska O, Richardson D, et al. Outbreak of carbapenem-resistant Enterobacteriaceae containing blaNDM-1, Ontario, Canada. Clin Infect Dis. 2012;55(11):e109–117. doi:10.1093/cid/cis737
16. Carattoli A, Bertini A, Villa L, Falbo V, Hopkins KL, Threlfall EJ. Identification of plasmids by PCR-based replicon typing. J Microbiol Methods. 2005;63(3):219–228. doi:10.1016/j.mimet.2005.03.018
17. Jia X, Dai W, Ma W, et al. Carbapenem-resistant E. cloacae in Southwest China: molecular analysis of resistance and risk factors for infections caused by NDM-1-producers. Front Microbiol. 2018;9:658. doi:10.3389/fmicb.2018.00658
18. Zakhour R, Chaftari AM, Raad II. Catheter-related infections in patients with haematological malignancies: novel preventive and therapeutic strategies. Lancet Infect Dis. 2016;16(11):e241–e250. doi:10.1016/S1473-3099(16)30213-4
19. Hyle EP, Ferraro MJ, Silver M, Lee H, Hooper DC. Ertapenem-resistant Enterobacteriaceae: risk factors for acquisition and outcomes. infect Control Hosp Epidemiol. 2010;31(12):1242–1249. doi:10.1086/657138
20. Li S, Jia X, Li C, et al. Carbapenem-resistant and cephalosporin-susceptible: a notable phenotype in patients with bacteremia. Infect Drug Resist. 2018;11:1225–1235. doi:10.2147/IDR.S174876
21. Ibrahim ME. Prevalence of Acinetobacter baumannii in Saudi Arabia: risk factors, antimicrobial resistance patterns and mechanisms of carbapenem resistance. Ann Clin Microbiol Antimicrob. 2019;18(1):1. doi:10.1186/s12941-018-0301-x
22. Passarelli-Araujo H, Palmeiro JK, Moharana KC, Pedrosa-Silva F, Dalla-Costa LM, Venancio TM. Genomic analysis unveils important aspects of population structure, virulence, and antimicrobial resistance in Klebsiella aerogenes. FEBS J. 2019;286(19):3797–3810. doi:10.1111/febs.15005
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.