")
Back to Journals » Cancer Management and Research » Volume 11
Cancer prevalence among the rural poverty-stricken population in Northeast China
Authors Liu B, Lao X, Feng Y, Liu J, Jiao M, Zhao M, Wang J, Zhang X , Liu J, Qi X, Liu H, Chen R, Wu Q, Hao Y
Received 18 February 2019
Accepted for publication 5 May 2019
Published 31 May 2019 Volume 2019:11 Pages 5101—5112
DOI https://doi.org/10.2147/CMAR.S205867
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Baohua Liu,1,2,* Xinxin Lao,3,* Yang Feng,4,* Jiazhuo Liu,5 Mingli Jiao,1 Miaomiao Zhao,1 Jiahui Wang,1 Xin Zhang,1 Jingjing Liu,1 Xinye Qi,1 Huan Liu,1 Ruohui Chen,1 Qunhong Wu,1 Yanhua Hao1
1Department of Social Medicine, School of Public Health, Harbin Medical University, Heilongjiang, People’s Republic of China; 2Harbin Center for Disease Control and Prevention, Harbin, Heilongjiang, People’s Republic of China; 3Educational Administration Section, General Hospital of Heilongjiang Farms & Land Reclamation Administration, Harbin, Heilongjiang, People’s Republic of China; 4Network Communication Section, Heilongjiang Third Hospital, Beian, Heilongjiang, People’s Republic of China; 5Second Project Section, Project Fund Supervision Service Center of Heilongjiang Health and Family Planning Commission, Harbin, Heilongjiang, People’s Republic of China
*These authors contributed equally to this work
Purpose: The burden of cancer impacts many of the world’s top concerns, but little information is published about the characteristics of cancer prevalence in the poor population.
Materials and methods: Data on cancer prevalence were obtained from the Health Poverty Alleviation Information System of Heilongjiang province. Prevalence was defined as all living cancer cases on October 1, 2018. Geographical area, cancer site, sex, age, educational level, and time since diagnosis were investigated.
Results: There were 10,529 cancer cases among 624,869 poor rural people in Heilongjiang up to October 1, 2018, and 77% of them did not have labor ability. Females accounted for 53.4%. The top five common cancers were lung, breast, colorectal, stomach, and liver cancer. There were distinct regional, sex, and age distribution differences in cancers. The prevalence rate for overall cancers was 1,685.0 per 100,000 people, which was much higher than that of the national level. Cancer prevalence peaked at an earlier age group (65–69 year). The 5-year cancer prevalence was 80.1% of the total cases.
Conclusion: Cancer imposes significant health and financial burdens in the rural poor. This study presents total and partial prevalence for the first time using actual dates from a large poor population in China, providing valuable information for tailored cancer prevention and control, quantifying the cancer burden and identifying priorities for poverty alleviation plans.
Keywords: cancer burden, prevalence, rural, poverty-stricken population
Introduction
Cancer is a major life-threatening disease and the most important obstacle to the increase in life expectancy worldwide.1–4 In China, approximately 4,292,000 cancer cases were newly diagnosed, and 2,814,000 patients died of cancer in 2015.3 Cancer is the leading cause of death in China and is responsible for approximately one in four of total deaths.5
Cancer prevalence is a broad concept defined as all people alive at index-date who have a history of being diagnosed with cancer. Prevalence profiles can provide detailed descriptive information and evidence for cancer prevention and control strategies,6,7 which also serve as a vital measure used to describe cancer patterns. Due to the complexity and variety of the types of cancer, and their extremely complicated biological characteristics, it is usually unrealistic to census the prevalence data of cancer in massive populations, let alone census for the information of vulnerable populations. Previous studies were usually based on incidence and survival data from cancer registries to predict the partial prevalence of cancer;6–11 however, the quality of some registries is not sufficiently high for study and reporting.2,12,13 Therefore, it might be difficult to provide a complete picture of cancer features, and studies tended to focus on the burden of partial prevalence for cancer patients diagnosed within the first few years.14
Poverty and disease have an apparent interactive relationship;15,16 economic level and condition strongly influence human health.17 Previous studies have shown that socioeconomic status was significantly associated with cancer treatment and mortality.12,18,19 As the health-care cost of cancer treatment is usually extremely high,10,20–22 the economic burden from cancer has a greater impact on the vulnerable rural populations. A large proportion of cancer patients rely heavily on their family’s financial and care support during cancer treatment, especially in the last stage of their life.20 Many rural households experiencing financial catastrophes of cancer treatment are even falling into a vicious circle of disease and poverty.
Poverty reduction is a common goal of all countries in the world, and poverty is one of the most important issues world wide; however, the health situation of poverty-stricken people is a gravely understudied area. Cancer burden in poor populations is poorly documented, and there are very few publications concerning cancer characteristics in poverty-stricken populations. Attention to the health status of the poor can provide evidence and reference for the world’s poverty reduction goals and healthy development. This study aimed to present a comprehensive overview on cancer prevalence in a poverty-stricken population in the northeast province of China, to provide reliable evidence for developing more targeted cancer control actions and policy for the poor population in the future.
Materials and methods
Date source
The data for this study were extracted from the Health Poverty Alleviation Information System (HPAIS) of Heilongjiang, which is a database used to dynamically record the basic demographic, disease, treatment and medical expenses information of the rural poor. HPAIS covers approximately 0.62 million rural people living below the poverty line in 9,598 villages of Heilongjiang province. Definitions and standards of poverty line differ widely all around the world. The international poverty line is currently set at $1.90 in terms of 2011 purchasing power parity by the World Bank. The Chinese national rural poverty household standard was set at 2,300 yuan of per capita net income in 2010, which is dynamically adjusted according to price index and living index by year. The standard was adjusted to 3,535 yuan in 2018. In addition to income, the standard for selecting candidate poverty-stricken rural households also takes into consideration the housing situation, children’s attendance at school, sanitation facilities, health condition, and many other factors into comprehensive measurement for their poverty level in China.
Ethics statement
This study was reviewed and approved by the Research Ethics Committee of Harbin Medical University. The database used in this study was anonymized and without any individual patient identifiers.
Statistical analysis
Cancer was reported in this study for all cancers combined (International Statistical Classification of Diseases and Related Health Problems-10th Revision codes: C00–C97) and 26 types of cancers: lip, oral cavity, and pharynx (C00–10, C12–14); nasopharynx (C11); esophagus (C15); stomach (C16); colorectal (C18–21); liver (C22); gallbladder (C23–24); pancreas (C25); larynx (C32); lung (C33–34); other thoracic organs (C37–38); bone (C40–41); melanoma of the skin (C43); nervous system (C47); breast (C50); cervix (C53); uterus (C54–55); ovary (C56); prostate (C61); testis (C62); kidney (C64–66,C68); bladder (C67); brain and central nervous system (CNS) (C70–72); thyroid (C73); lymphoma (C81–85, 88, 90, 96); leukemia (C91–-95).
Crude rate (CR) and age-standardized rate (ASR) were calculated per 100,000 individuals for prevalence, corresponding population stratified by area, sex and cancer type. The World Health Organization (2000–2025) Standard Population was applied for calculating age-standardized rates. Age-specific prevalence was presented by top five common cancers by age group (younger than 14 years, 15–34 years, 35–64 years, and 65 years or older). Cancer prevalence was further stratified by time since diagnosis (within 1 year, 3 years, 5 years, 10 years, 15 years, and more than 15 years).
Role of the funding source
The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the article. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Results
Characteristics of the poor population and cancer cases
As of October 1, 2018, there were a total of 624,869 rural poor people in Heilongjiang Province. The mean age was 53 years and 35.4% were 65 years or above. Males accounted for 52.7% of the total. Only 4.3% of adults (≥18 years) had a senior school education or above, and 55.0% did not have the capacity to work. Of the total population, the number of cancer patients was 10,529. The mean age was 61 years and approximately 38.7% were 65 years old or above. Males comprised 46.6% of the cancer patients. Only 2.3% of adults with cancer had a senior school education or above, and up to 77.2% did not have the capacity to work. Among the total poor population, poverty caused by disease accounted for about 56% of the total reasons for poverty (Figure 1A). Regarding the poor who had been diagnosed with cancer, the burden from cancer accounted for 86% of all reasons for poverty (Figure 1B).
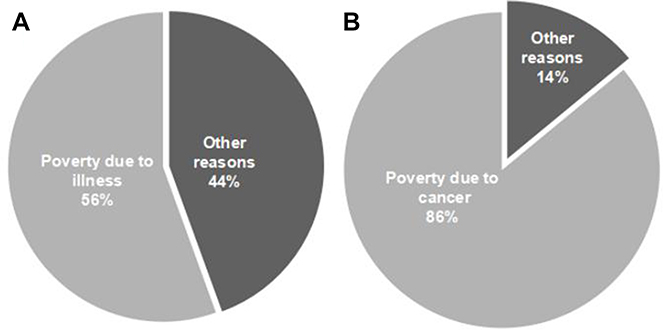 | Figure 1 Causes of poverty for the poor and cancer patients in Heilongjiang province, 2018. (A) All poor people. (B) Poor people with cancer. |
All rural poverty-stricken people recorded in HPAIS were covered by Basic Medical Insurance for Urban and Rural Resident with waivered of premiums. Among them, about 31.1% who were extremely poor and/or seriously ill were also covered by the Insurance Scheme for Catastrophic Diseases (ISCD). Regarding the poor people with cancer, the coverage rate of ISCD was about 37.4%.
Cancer prevalence by area
The cancer prevalence rates in the poor population were much higher in eastern areas than in other areas of Heilongjiang province (Figure 2). Of the 13 areas, breast cancer ranked first in eight areas and second in four areas; lung cancer ranked first in three areas, second in four areas, and third in four areas; colorectal cancer ranked first in two areas, second in four areas, and third in five areas; stomach cancer ranked third in two areas, while leukemia and liver cancer ranked third in one area. In the northernmost area, Daxing’anling, where the population is sparse, the air quality is excellent, the weather is colder, and the pace of life is slow and easy, the two most common cancers were esophagus cancer and nervous system cancer, which is clearly different from other areas.
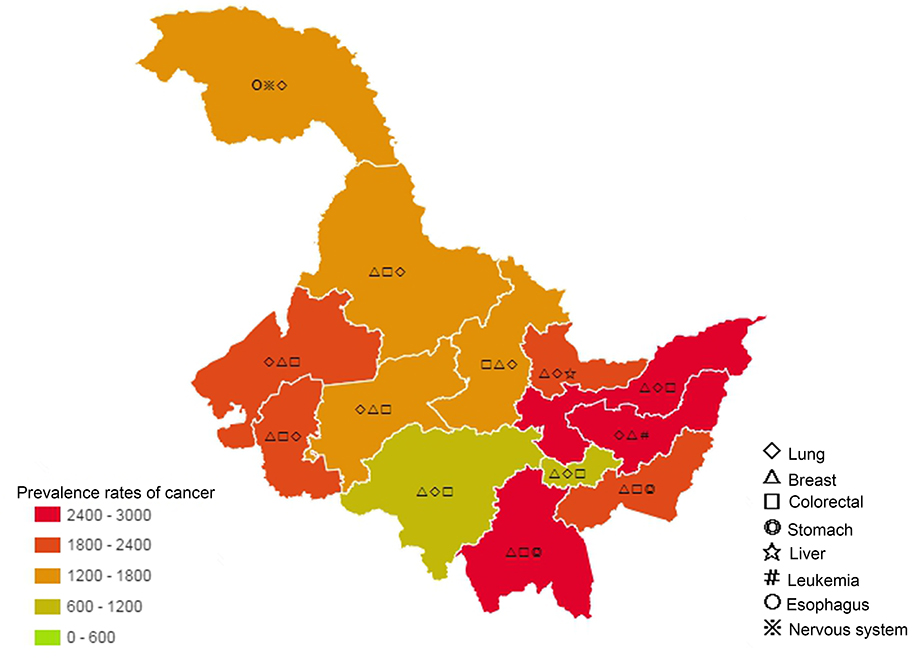 | Figure 2 Cancer prevalence rates (per 105) and common cancers in the rural poor of Heilongjiang province, by area, 2018. |
Cancer prevalence by type and sex
Among 10,529 cancer cases, the most frequent cancers were lung cancer (1,654 cases, 15.7%), followed by breast cancer (1,548 cases, 14.7%), colorectal cancer (1,121 cases, 10.6%), stomach cancer (664 cases, 6.3%), and liver cancer (643 cases, 6.1%) (Table 1). These five cancers accounted for 53.4% of the overall burden of cancers in rural poor people of Heilongjiang province. Among males, the most common cancers were lung (18.5%), colorectal (14.3%), stomach (10.5%), liver (10.1%), and bladder (6.4%). Among females, breast cancer occurred most frequently (27.2%), followed by lung (13.3%), cervical (7.7%), colorectal (7.4%), and thyroid (6.1%) cancers. The crude and age-standardized prevalence rates for overall cancers were 1,685.0 and 953.3 per 100,000 people, respectively.
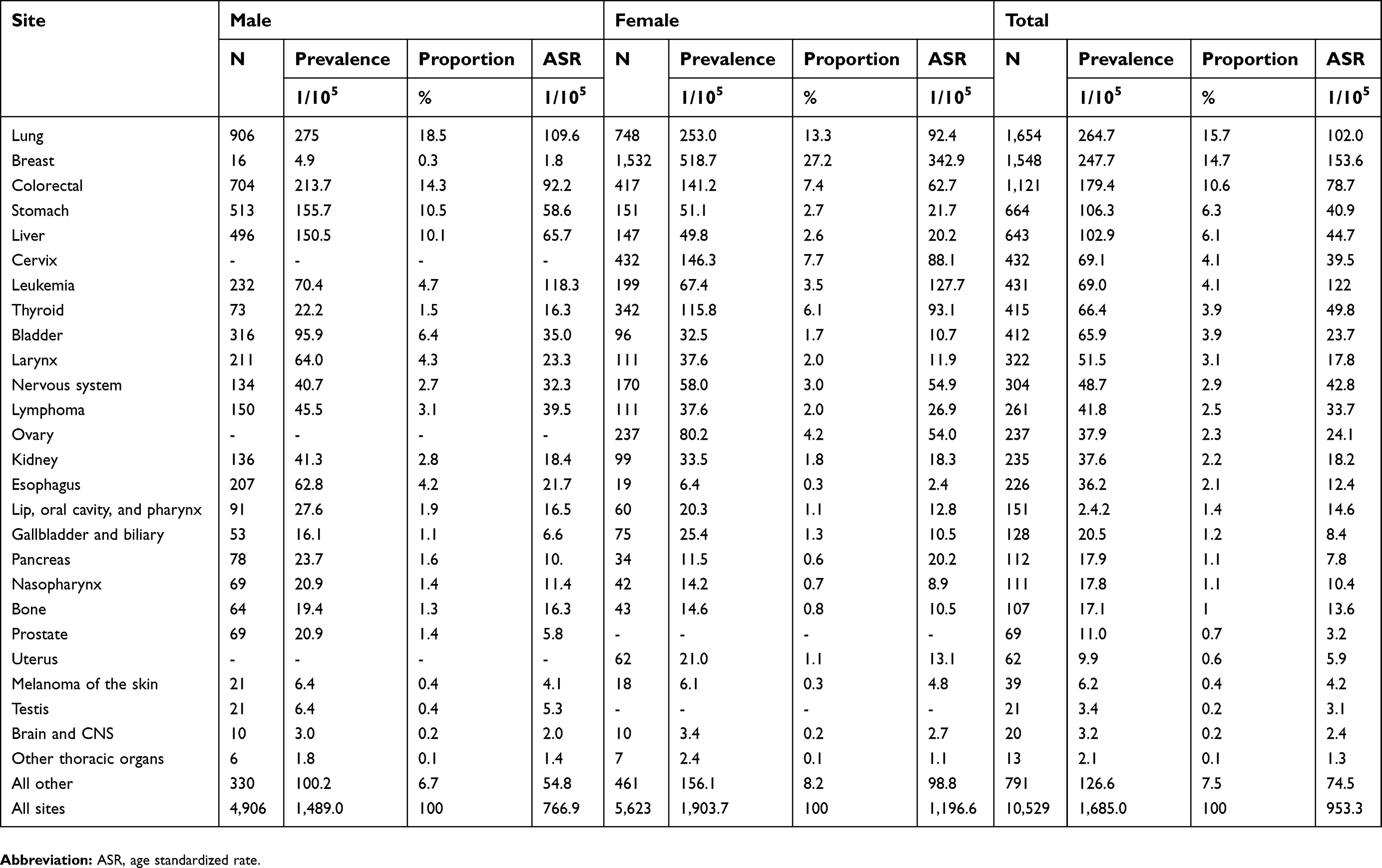 | Table 1 Number of cancer cases and prevalence rates in the rural poor population of Heilongjiang, by sex and rank, 2018 |
Age-specific prevalence
The number of cases and prevalence rates of all cancers combined for both males and females presented an inverted U-shaped pattern according to age (Figure 3). The number of cases of both sexes and the prevalence rate of males increased until reaching a maximum at 65–69 years and then decreased; however, the highest prevalence rate in females was at 50–54 years. There were distinct age-specific distribution features between males and females. In the age group 0–24 years, both male and female age-specific cancer prevalence rates were approximately the same lower level; however, from age group 25–29 years onward, the gap between female and male prevalence rates gradually increased with the prevalence rate in females accelerating from the 35–39-year age group. At the age group 45–49 years, during the female menopause period, the gap between the two sexes peaked; thereafter, it gradually narrowed and crossed at the age of 65 years.
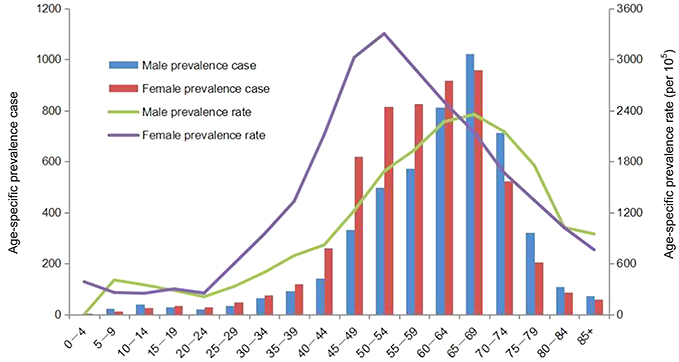 | Figure 3 Age-specific prevalence cases and age-specific prevalence rates (per 105) for all cancers, by sex, 2018. |
Among children and young people, leukemia was the most commonly diagnosed cancer for both sexes (Table 2). At age 35 years or older, lung cancer was the most frequently diagnosed cancer among men, followed by colorectal, liver or stomach, and bladder cancer. In the age range from 35 to 64 years, breast cancer was the most commonly diagnosed cancer in females, while among those aged 65 years or above, lung was the most common cancer. Figure 4 further details the distribution of the top 10 most common cancers between the sexes at different age stages. We found a peculiar phenomenon, in that for females, the sex-related cancers, ie, breast cancer, cervical cancer, ovarian cancer, and thyroid cancer (prone to occur in women), reached the highest prevalence at an earlier age between 45 and 59 years (Figure 4B), whereas the highest prevalence in males occurred later after the age of 60 years (Figure 4A).
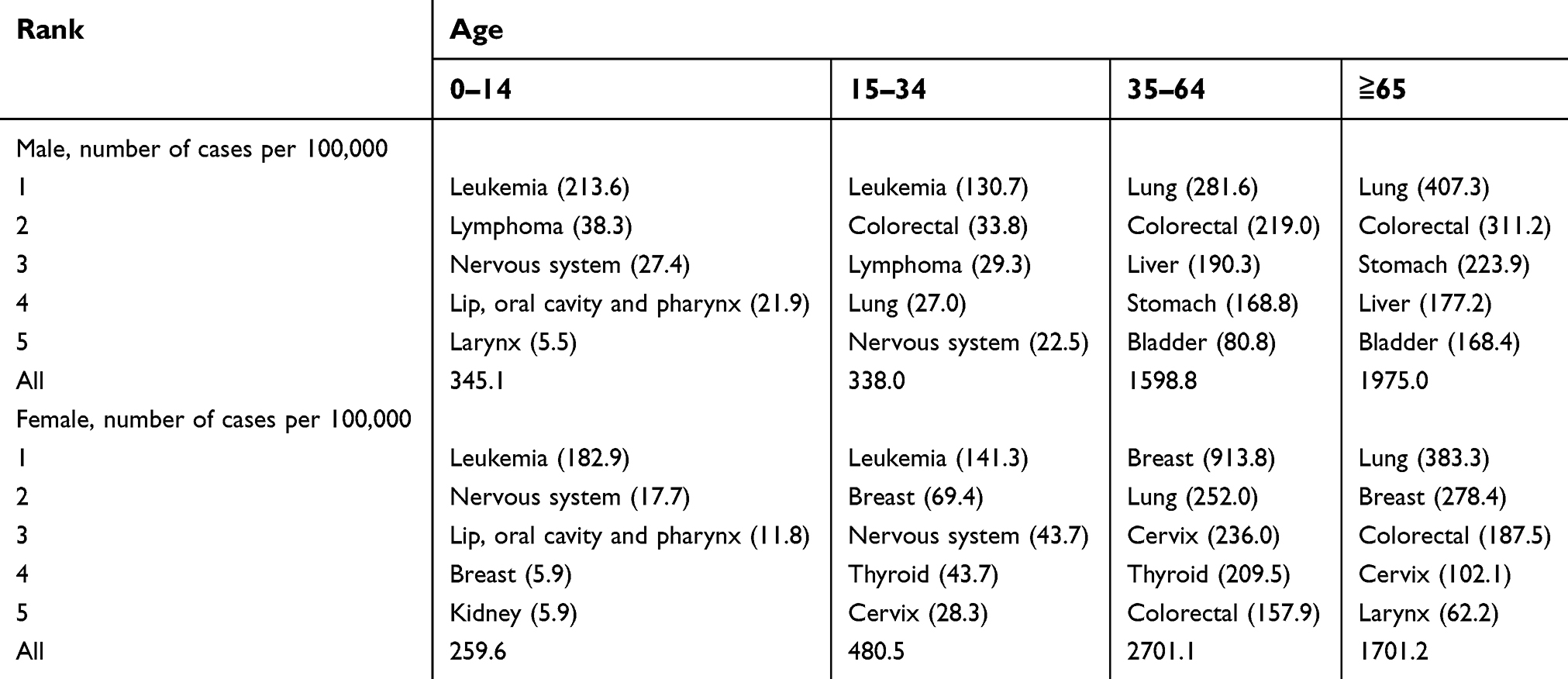 | Table 2 The prevalence rates of the top five common cancers in the rural poor population by age group and sex, 2018 |
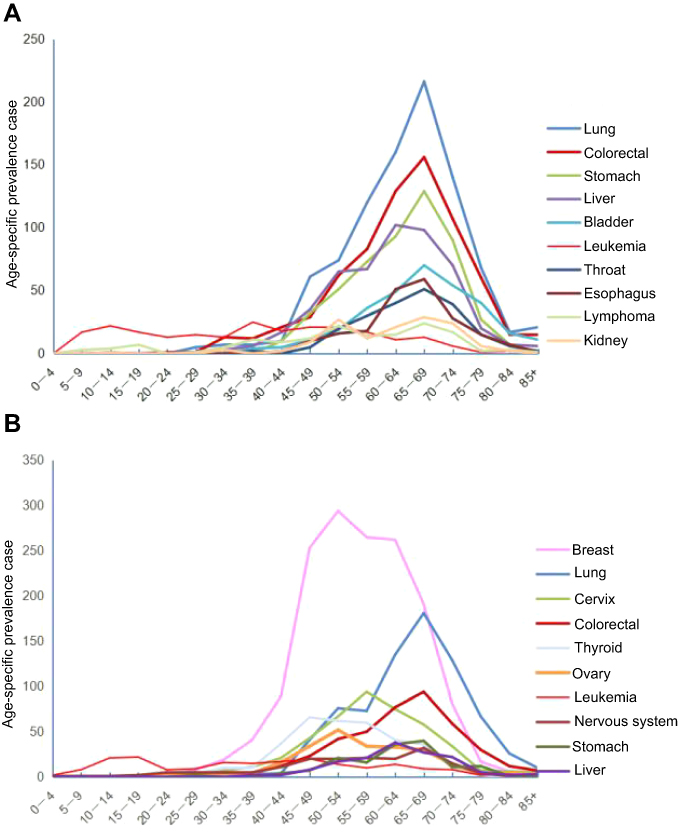 | Figure 4 Age-specific prevalence rates (per 105) of the top 10 cancers, 2018. (A) Male. (B) Female. |
The time span since the first diagnosis of cancer can be regarded as one way to distinguish people needing corresponding medical care or monitoring. Tables 3 and 4 describe the duration of prevalence for all living patients by sex. For short-term prevalence, the 3-year partial prevalence for all cancers combined in 2018 in the Heilongjiang rural poor was 6,755 (67.6% of total male and 61.1% of total female cases), and the 5-year prevalence for all cancers combined was 8,432 (82.8% of total male and 77.7% of total female cases). By sex, the top five 5-year prevalent cancers in males were lung (244.0), colorectal (177.9), liver (137.8), stomach (124.7), and bladder (81.0); among females, the top five 5-year prevalent cancers were breast (364.9), lung (230.6), colorectal (109.4), cervical (108.3), and thyroid (97.8).
 | Table 3 Time since first diagnosis among cancer cases in poor males, 2018 |
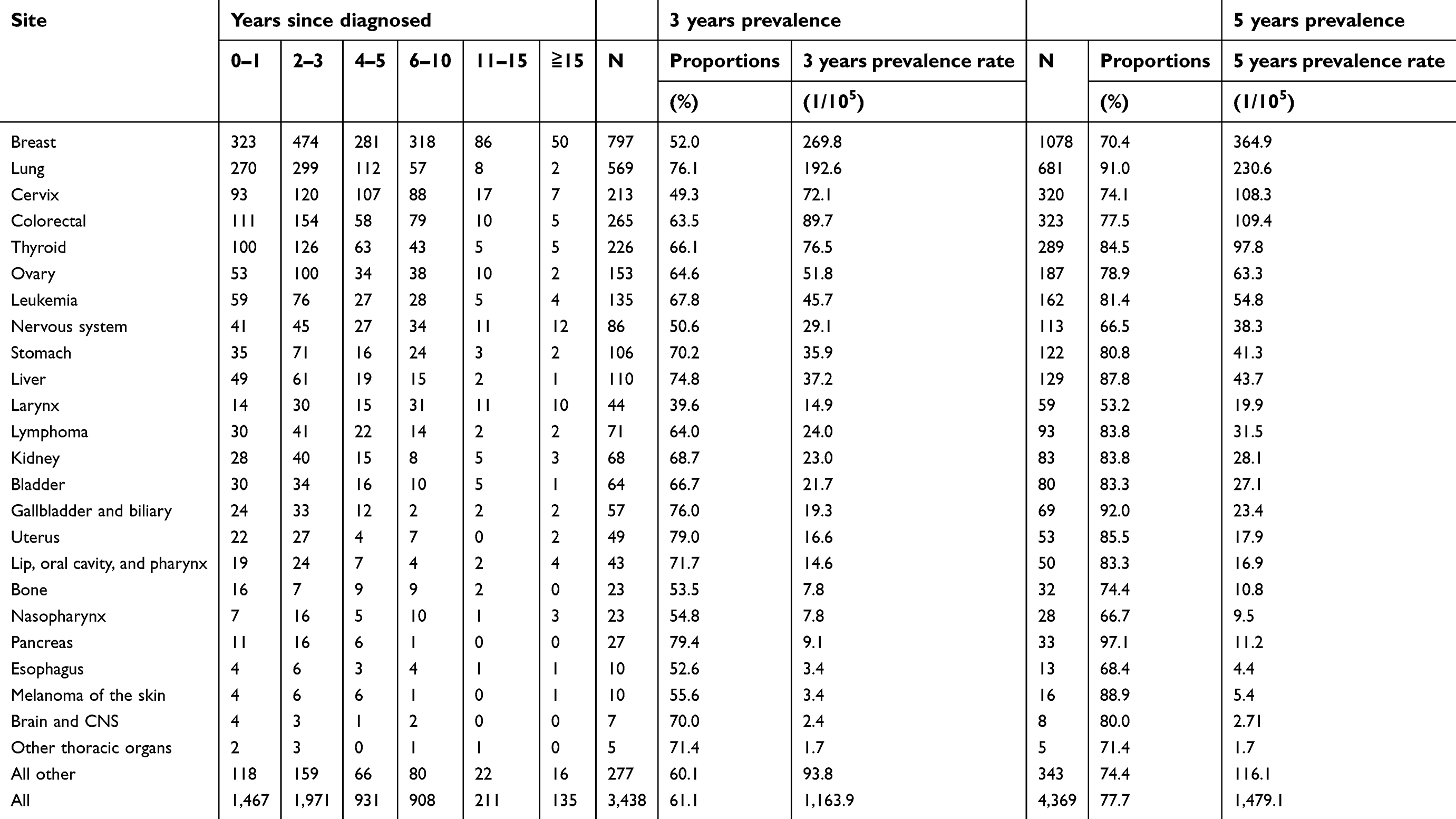 | Table 4 Time since first diagnosis among cancer cases in poor females, 2018 |
For cancer sites studied, breast (93.8%), liver (91.5%), lip, oral cavity, and pharynx (89.0%), lung (88.7%), and prostate (88.4%) in males had a higher proportion of the 5-year partial prevalence; in females, pancreas (97.1%), gallbladder and biliary (92.0%), lung (91.0%), melanoma of the skin (88.9%), and liver (87.8%) had a higher proportion of cases diagnosed within 5 years.
Discussion
This research provides systematic information on total and partial cancer prevalence for the rural poor in Heilongjiang, the characteristics of cancer prevalence were broken down by age pyramid, sex, region as well as cancer site. Overall, the number of the poor affected by cancer was 10,529 in 2018, the crude prevalence rate for all cancers combined was 1,685.0 per 100,000 people. The 5-year prevalence rates (1,233.1 per 100,000 in men and 1,479.1 per 100,000 in women) were much higher than the national 5-year cancer prevalence (666 per 100,000 in urban and 440 per 100,000 in rural, for both sexes) in 2011,6 while they were lower than that had been reported in Korea10 (3,162.8 per 100,000 people) and Western Australia (37.6 per 1,000 males and 36.5 per 1,000 females). The higher prevalence among the rural poor compared to the national level can be attributed to many factors, although there was no definite evidence that poverty would increase cancer prevalence due to economic conditions and unhealthy lifestyles. However, one reason that may explicate the disparities is the aging structure (average age 53 years) of the poor population,11 while according to the sixth national population census, the average age of Chinese people was less than 40 years old. In addition, Chen and colleagues founded people living in Heilongjiang Province had the highest overall level of combined risks of modifiable factors for cancer among 31 provinces in China, with women ranked first and men ranked second.23
The prevalence of cancer shows geographic differences.2,24,25 There were substantial variations in the cancer prevalence rate and cancer site between areas. The poverty-stricken population in eastern Heilongjiang had higher cancer prevalence rates than other areas. The top three common cancers in the poor population were lung, breast and colorectal cancer, but their ranking varied among regions. Further research should be conducted to explore the ecological, environmental, and economic factors that contribute to regional differences in the distribution of cancer, and effective control measures should be devised to cope with relatively higher local risks.
The prevalence of cancers was higher among females than in males (the ratio of female to male is 1.15). This finding is consistent with previous national3,6 and Sudanese5 statistics; however, it is contrary to the global,2 French,8 and Japanese26 statistics. There were also significant differences in cancer types between different sexes. The most common cancers were lung, colorectal, stomach, liver, and bladder in men, and breast, lung, cervical, colorectal and thyroid in women. A published review article showed that cancer prevalence usually peaks at ages 85–89 years, after which the rates decrease.11 However, cancer prevalence rates in this study showed a much earlier peak for both sexes and then dropped suddenly; cancer prevalence rate in men peaked in the 65–69 years age group, while in women it peaked at an even earlier age of 50–54 years. The earlier decline in prevalence might be associated with earlier deaths due to lack of effective early diagnostic strategies and suboptimal treatment, as well as poor economic support.18,19 Previous study showed that the survival rate for all cancer patients in China was lower in rural areas than in urban areas: the urban–rural survival gap was 13.1% in 2012–2015.1
The ranking of cancer prevalence in this study is different from that in China. For example, the most common cancers diagnosed in five years were lung, colorectal and liver in males, and breast, lung and colorectal in females, but national statistical results6 show that the most frequent cancers for males diagnosed in five years were stomach, lung and colorectal, and those for females were breast cancer, colorectal and cervix.
It is worth noting that 5-year prevalence of lung cancer in the poor population (244.0 per 100,000 in males and 230.6 per 100,000 in females) was much higher than in the 2011 national statistics (84.6 in males and 45.6 in females),6 the ratios were about 2.88 times for males and 5.06 times for females. Heilongjiang province is the coldest province located in the most northeastern part of China. The higher prevalence of lung cancer in the rural poor may be associated with outdoor and indoor air pollution caused by burning large amounts of solid fuels during cooking and heating.15 Smoking was reported to be the highest risk factor of cancer among females in Heilongjiang province, this finding may partly explain the high prevalence among females.23 Breast cancer is the most frequent type of cancer in females worldwide.2,27 In this study, the prevalence of breast cancer was the most common cancer among the poor in 8 of 13 regions in Heilongjiang province, and accounted for 27.2% of all cancer cases among poor rural females. Colorectal cancer was the second most common type in poor males; the prevalence rate of colorectal cancer was higher in males than in females. Leukemia was not a particularly common cancer among poor people; however, it accounted for the majority of cases in poor children and young people, which was consistent with previous studies.4,28 In addition, the prevalence rate of leukemia was very high (ranked second) after age standardization in the rural poor. In this study, we also found that several high-prevalence cancers, including stomach cancer (third common in males and ninth common in females), liver cancer (third common in males), and cervical cancer (third common cancer in females) are attributable to infection.24,29 Therefore, one of the effective ways to tackle the huge burden of cancer is to intervene in these infectious disease-related cancers, such as by vaccination.
In view of the broad definition of prevalence, partial prevalence makes it possible to identify the approximate number of patients needing clinical treatment and surveillance care.6–10 The usual classification is cancer patients who were diagnosed within 1 year and in the last year of life are cases related to the highest levels of health service utilization; 2–3 years indicates that the cases ought to have clinical follow-up; 2–5 years indicates they should be under close surveillance due to high probability of recurrence; 5–10 years indicates the probability of recurrence is low; and beyond 15 years, patients can be deemed to be cured. In the rural poor of Heilongjiang, 3-year prevalence and 5-year prevalence accounted for large proportions of the total cases (64.2% and 80.1%, respectively). This implies huge cancer treatment cost for poor households as well as a substantial economic burden to the local government in further financing and expanding the coverage of catastrophic medical schemes. In addition, it also exerts a huge social care burden on members of poor families who usually take over all the responsibilities and burden of those cancer patients.
This study found that the rural poor with cancer were confronted with unique multi-vulnerabilities, including poor and seriously ill, long-term and high medical treatment cost as well as social care burden, senior ages (mean age 65 years), without labor capacity (77.2%) and less educated. In addition, there is an unbalanced distribution of health-care resources between rural and urban regions.30,31 The national bureau of statistics of China in 2018 showed that in Heilongjiang Province, the number of health personnel per 1,000 was 10.25 in urban and only 4.19 in rural areas.5 Hospitals in China are rigorously classified into three levels, primary, secondary and tertiary, among which the tertiary hospitals are believed to provide the highest quality of medical services.30,32 Almost all tertiary hospitals are located in urban areas, while the county hospitals and township health centers usually have difficulty in diagnosing and treating complicated diseases like cancer due to a shortage of qualified professionals and medical technology.33,34 Due to the above reasons, poor cancer patients living in rural areas often have to travel long distances to the urban areas to get a more accurate diagnosis and complicated treatment, often generating additional costs to them. The combination of these unfavorable factors leads to difficulties in ongoing efforts of the government to get those who were stricken by both poverty and disease out of their dire situation. It is the government’s responsibility to establish a multiple health system guarantee for these vulnerable poor people, and more medical resources and capacity building should be provided to cope with the heterogeneous demands of medical care support. Cost-effectiveness analysis of cancer treatment and support should also be considered in poverty alleviation programs, and palliative therapy should be properly administered according to the actual situation of patients to avoid the large burden that families and society would have to bear due to excessive treatment.
Conclusion
Cancer imposes significant medical, financial, and social care burdens on the rural poor population. For the first time in China, this study drew a clear cancer prevalence profile among poor people. This study found out that there exists diverse distribution in cancers based on geography, age, and sex. In addition, the 5-year prevalence, which was deemed as an important way to identify patients needing treatment and care, was as high as 80.1%. The results of this study suggest that the government should formulate targeted treatment and poverty alleviation strategies for these vulnerable groups in order to meet the unique challenges. Timely economic assistance and rational allocation of finite health-care resources to address medical burden should depend on accurate quantification of future demands of high cancer prevalence. Determining the prevalence for the timely and high quality treatment of cancer treatment is closely related to prognosis for vulnerable poor populations. This study can also serve as a baseline for future comparisons with different regions and different groups of people. In addition, future rural health planning should focus on identifying risk factors and changing unhealthy lifestyles for good primary prevention.
Abbreviation list
HPAIS, Health Poverty Alleviation Information System; CR, crude rate; ASR, age-standardized rate; ISCD, insurance scheme for catastrophic diseases.
Ethics approval
This study was reviewed and approved by the Research Ethics Committee of Harbin Medical University.
Availability of data and materials
Cancer data were acquired from the Health Poverty Alleviation Information System (HPAIS) of Heilongjiang. To protect personal privacy, the data are not publically available.
Acknowledgments
This study was supported by the National Natural Science Fund (71333003). We gratefully acknowledge the Health Poverty Alleviation Information System of Heilongjiang in providing cancer records, data collection, and database creation.
Author Contributions
All authors contributed to data analysis, drafting the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zeng H, Chen W, Zheng R, et al. Changing cancer survival in China during 2003–15: a pooled analysis of 17 population-based cancer registries. Lancet Glob Health. 2018;6:e555–e67. doi:10.1016/S2214-109X(18)30127-X
2. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424.Epub 2018 Sep 12. doi:10.3322/caac.21492
3. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66:115–132. doi:10.3322/caac.21338
4. Chen W, Zheng R, Zhang S, et al. Cancer incidence and mortality in China, 2013. Cancer Lett. 2017;401:63–71. doi:10.1016/j.canlet.2017.04.024
5.
6. Zheng R, Zeng H, Zhang S, Chen T, Chen W. National estimates of cancer prevalence in China, 2011. Cancer Lett. 2016;370:33–38. doi:10.1016/j.canlet.2015.10.003
7. Colonna M, Danzon A, Delafosse P, et al. Cancer prevalence in France: time trend, situation in 2002 and extrapolation to 2012. Eur J Cancer. 2008;44:115–122. doi:10.1016/j.ejca.2007.10.022
8. Colonna M, Boussari O, Cowppli-Bony A, et al. Time trends and short term projections of cancer prevalence in France. Cancer Epidemiol. 2018;56:97–105. doi:10.1016/j.canep.2018.08.001
9. Maddams J, Utley M, Moller H. Projections of cancer prevalence in the United Kingdom, 2010–2040. Br J Cancer. 2012;107:1195–1202. doi:10.1038/bjc.2012.366
10. Jung KW, Won YJ, Kong HJ, Lee ES. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2015. Cancer Res Treat. 2018;50:303–316. doi:10.4143/crt.2018.143
11. Nolen SC, Evans MA, Fischer A, Corrada MM, Kawas CH, Bota DA. Cancer—incidence, prevalence and mortality in the oldest-old. A comprehensive review. Mech Ageing Dev. 2017;164:113–126. doi:10.1016/j.mad.2017.05.002
12. Hoang VM, Pham CP, Vu QM, et al. Household financial burden and poverty impacts of cancer treatment in Vietnam. Biomed Res Int. 2017;2017:1–8.
13. Forman D, Sierra MS. Cancer in Central and South America: introduction. Cancer Epidemiol. 2016;44:S3–10. doi:10.1016/j.canep.2016.04.008
14. Maxwell S, O’Leary P, Slevin T, Moorin R. The increase in cancer prevalence and hospital burden in Western Australia, 1992–2011. Popul Health Metr. 2014;12:33. doi:10.1186/s12963-014-0033-x
15. Aue K, Roosen J, Jensen HH. Poverty dynamics in Germany: evidence on the relationship between persistent overty and health behavior. Soc Sci Med. 2016;153:62–70. doi:10.1016/j.socscimed.2016.01.040
16. Porter J. Poverty, disease, and urban governance in late nineteenth-century Osaka. City, Cult Soc. 2012;3:73–78. doi:10.1016/j.ccs.2012.06.005
17. Menon J, Vijaykumar N, Joseph JK, et al. Below the poverty line and non-communicable diseases in Kerala: the epidemiology of non-communicable diseases in rural areas (ENDIRA) study. Int J Cardiol. 2015;187:519–524. doi:10.1016/j.ijcard.2015.04.009
18. Pou SA, Tumas N, Soria DS, Ortiz P, del Pilar Diaz M. Large-scale societal factors and noncommunicable diseases: urbanization, poverty and mortality spatial patterns in Argentina. Appl Geogr. 2017;86:32–40. doi:10.1016/j.apgeog.2017.06.022
19. de Grubb MCM, Kilbourne B, Kilbourne K, et al. Socioeconomic, environmental, and geographic factors and US lung cancer mortality, 1999–2009. Fam Med Community Health. 2017;5:3–12. doi:10.15212/FMCH.2017.0108
20. Luengo-Fernandez R, Leal J, Gray A, Sullivan R. Economic burden of cancer across the European Union: a population-based cost analysis. Lancet Oncol. 2013;14:1165–1174. doi:10.1016/S1470-2045(13)70442-X
21. Guy GP J, Yabroff KR, Ekwueme DU, et al. Healthcare expenditure burden among non-elderly cancer survivors. 2008–2012. Amer J Prev Med. 2015;49:S489–97. doi:10.1016/j.amepre.2015.09.002
22. Gilligan AM, Alberts DS, Roe DJ, Skrepnek GH. Death or debt? National estimates of financial toxicity in persons with newly-diagnosed cancer. Amer J Med. 2018;131:1187–99.e5.23. doi:10.1016/j.amjmed.2017.12.017
23. Chen W, Xia C, Zheng R, et al. Disparities by province, age, and sex in site-specific cancer burden attributable to 23 potentially modifiable risk factors in China: a comparative risk assessment. Lancet Glob Health. 2019;7:e257–69. doi:10.1016/S2214-109X(19)30013-0
24. Popat K, McQueen K, Feeley TW. The global burden of cancer. Best Pract Res Clin Anaesthesiol. 2013;27:399–408. doi:10.1016/j.bpa.2013.10.010
25. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. doi:10.3322/caac.21294
26. Nakagawa-Senda H, Yamaguchi M, Matsuda T, et al. Cancer prevalence in Aichi, Japan for 2012: estimates based on incidence and survival data from population-based cancer registry. Asian Pac J Cancer Prev. 2017;18:2151–2156. doi:10.22034/APJCP.2017.18.1.23
27. Wang W, Wang X, Liu J, et al. Breast cancer in young women of Chinese Han population: a retrospective study of patients under 25 years. Pathol Res Pract. 2016;212:1015–1020. doi:10.1016/j.prp.2016.08.010
28. Erdmann F, Li T, Luta G, et al. Incidence of childhood cancer in Costa Rica, 2000–2014: an international perspective. Cancer Epidemiol. 2018;56:21–30. doi:10.1016/j.canep.2018.07.004
29. Gandhi AK, Kumar P, Bhandari M, Devnani B, Rath GK. Burden of preventable cancers in India: time to strike the cancer epidemic. J Egypt Natl Can Inst. 2017;29:11–18. doi:10.1016/j.jnci.2016.08.002
30. Li Y, Sun Y, Zhang Y, Yi D, Ma C, Ma S. Rural–urban disparity in health care: observations from Suzhou, China. Public Health. 2016;138:164–167. doi:10.1016/j.puhe.2016.03.026
31. Li L. The challenges of healthcare reforms in China. Public Health. 2011;125(1):6–8. doi:10.1016/j.puhe.2010.10.010
32. Pan J, Qin X, Li Q, Messinad JP, Delamater PL. Does hospital competition improve health care delivery in China? China Econ Rev. 2015;33:179–199. doi:10.1016/j.chieco.2015.02.002
33. Yang M. Demand for social health insurance: evidence from the Chinese new rural cooperative medical scheme. China Econ Rev. 2018;52:126–135. doi:10.1016/j.chieco.2018.06.004
34. Younger DS. Health care in China. Neurol Clin. 2016;34(4):1115–1125. doi:10.1016/j.ncl.2016.06.003
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.