")
Back to Journals » Journal of Pain Research » Volume 13
Cancer Pain Management: An Italian Delphi Survey from the Rational Use of Analgesics (RUA) Group
Authors Varrassi G , De Conno F , Orsi L, Puntillo F , Sotgiu G, Zeppetella J, Zucco F
Received 20 December 2019
Accepted for publication 16 April 2020
Published 8 May 2020 Volume 2020:13 Pages 979—986
DOI https://doi.org/10.2147/JPR.S243222
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Michael A Ueberall
Giustino Varrassi,1 Franco De Conno,2 Luciano Orsi,3 Filomena Puntillo,4 Giovanni Sotgiu,5 John Zeppetella,6 Furio Zucco7
1Paolo Procacci Foundation, Rome, Italy; 2Palliative Care, Pain Therapy and Rehabilitation Unit, Fondazione IRCCS Istituto Nazionale Tumori, Milan, Italy; 3SC Cure Palliative ASST Carlo Poma, Mantova, Italy; 4Anesthesia and Intensive Care Unit, Department of Emergency and Organ Transplants, University Hospital of Bari, Bari, Italy; 5Clinical Epidemiology and Medical Statistics Unit, Department of Medical, Surgical and Experimental Sciences, University of Sassari, Sassari, Italy; 6St Claire’s Hospice, Hastingwood, UK; 7Azienda Ospedaliera Salvini, Garbagnate Milanese, Italy
Correspondence: Giustino Varrassi
Paolo Procacci Foundation, Via Tacito 7, Rome 00193, Italy
Email [email protected]
Background: In patients with cancer, the prevalence of pain is high, and pain management is often challenging despite the wide availability of drugs and guidelines.
Methods: This Delphi survey was organized within the Rational Use of Analgesics (RUA) Group projects to reach a consensus among Italian palliative care specialists on pain assessment and management. Items were identified from recent publications on cancer pain and guidelines.
Results: This survey included input from 190 palliative care specialists representing all Italian territory. A consensus was reached on 17 statements. Items concerning pain assessment achieved over 70% agreement amongst the participants. Items on principles of pain management and management according to type of pain, including breakthrough cancer-related pain and neuropathic pain also achieved high levels of agreement.
Conclusion: Results from the RUA project showed that Italian palliative care specialists had a particular interest in items related to pain challenges, in addition to the evaluation and control of pain associated with cancer. However, some discrepancies between current guidelines and clinical practice were observed.
Keywords: cancer, pain, breakthrough cancer pain, neuropathic pain, Delphi survey
Introduction
In patients with cancer, pain prevalence ranges from 33% (after curative treatment) to 59% (in patients on anticancer treatment), reaching up to 64% in patients with metastatic, advanced or terminal disease.1 Furthermore, approximately 5–10% of patients who survive cancer suffer from chronic severe pain that significantly interferes with their daily functioning.1
In 1986, the World Health Organization (WHO) released guidelines on Comprehensive Management of Cancer Pain2 which was updated 10 years later. To manage pain in cancer patients, these guidelines proposed the use of four different classes of drugs: non-opioids, weak opioids, strong opioids and adjuvant drugs. The sequence of administration would depend on the increase in the severity of pain as the disease progresses, with an increase in the analgesic strength of the drugs from non-opioids (Step I) to weak opioids (Step II) and then to strong opioids (Step III). This treatment sequence was named as the “three-step analgesic ladder”.3 However, there are many gaps; eg, the WHO guidelines do not specify the extent of efficacy nor the rationale for not using strong opioids as first-line treatment, especially in patients with terminal cancer. Compared with pain management as per WHO guidelines, the use of strong opioids as first-line treatment in patients with terminal cancer resulted in significantly better pain relief, fewer changes in therapy, greater reduction in pain following modifications in therapy, and greater satisfaction with treatment (P < 0.041).4 The latest European Society for Medical Oncology (ESMO) guidelines recommend strong opioids as the mainstay of analgesic therapy in treating moderate to severe cancer-related pain.1 Among a variety of equivalent drugs, morphine was the most widely available and most prescribed strong opioid; however, there is no superiority of one strong opioid over another.1 The choice of opioid and the dose titration are important to achieve an optimum balance between analgesia and unwanted adverse effects. Therefore, pain treatments are suggested to follow multimodal approaches considering 1) the intensity of pain, 2) the pathophysiology of pain, 3) the complexity of symptoms, 4) the presence of comorbidities, 5) the social context, and 6) the “time” of illness.5 Such multimodal approaches would allow managing cancer-associated pain in a holistic manner and providing a personalized therapy in clinical practice. This multimodal and personalized approach is particularly relevant for elderly patients who are often affected by many comorbidities and are frail. In these patients, a detailed pain assessment should be done, when possible utilizing the geriatric assessment that can help clinicians uncover problems not routinely assessed in the standard oncologic evaluation.6 For older adults with cancer pain, opioid medications are safe and effective as long as these medications are closely monitored and titrated slowly; however, clinicians need to be aware of the unique risks in this population, which could include delirium, polypharmacy, and falls in addition to the well-known adverse effects of these drugs.6 A central role in multimodal approach is also played by caregivers and familiars who are mainly involved in pain management in everyday life.7 Home care includes complex and sometimes unfamiliar procedures for carers who may become distressed at this increased burden. Caregivers share the same beliefs as patients concerning addiction, harmful analgesic side effects and masking disease progression. These attitudes can lead to undertreatment of pain and an over-zealousness in protecting patients from analgesic overuse. Therefore, it is important to identify and resolve caregiver barriers with respect to pain control to improve pain management quality and the quality of life of the patient.7
In some cases, despite stable and well-controlled background pain, breakthrough cancer pain (BTcP) can occur spontaneously or in response to a trigger.8 In this case, opioids providing rapid analgesia are commonly given as needed in addition to the background analgesic medication, such as oral opioids and nasal/transmucosal preparations of fentanyl, also named rapid-onset opioids (ROO).9 Furthermore, if necessary, it is possible to combine adjuvant drugs at any step of WHO ladder, including tricyclic antidepressants, serotonin norepinephrine-reuptake inhibitors, gabapentinoids, lidocaine 5% patches or later-line adjuvants (eg, older anticonvulsants, corticosteroids, and N-methyl-D-aspartate [NMDA] receptor antagonists) that may help some patients.10
Despite availability of guidelines and treatment options, undertreatment of pain is common among patients with cancer. Furthermore, different clinicians may have a varied diagnosis and perception of patients’ pain, and pain management is, therefore, often ineffective.1 The Rational Use of Analgesics (RUA) project was aimed to investigate the current clinical practices to manage pain in patients with cancer in Italy. Several meetings were organized for this purpose to address the debate on pain management and its assessment and management in clinical practice, based on the most recent guidelines.1 During these meetings, a Delphi survey was organized to achieve a consensus on overall pain management, use of analgesic drugs as per guidelines and partially approaching the BTcP.
Materials and Methods
Design and Identification of Experts
The Delphi survey is an indirect, anonymous, iterative process aimed at achieving consensus among experts, in consecutive stages of the process, based on the systematic feedback from the results of the previous related surveys.11–13 A board of experts was selected by a steering committee of seven specialists in the fields of pain management and palliative care, based on documented expertise (authorship of research paper and/or at least 5 years of clinical experience in cancer or palliative treatment).
Delphi Rounds/Topics
The steering committee discussed 50 statements, on which literature seems not to be completely in accordance, elaborated from publications focused on pain management in oncology.1,4,8,9,14 These statements were structured into seven categories, mirroring the section of the ESMO guidelines (assessment; principles of pain management, treatment of mild to moderate pain, treatment of moderate to severe pain, end of life pain, BTcP, cancer-related and neuropathic pain). The steering committee rated and suggested the statements and relevant items (27 in total) to be included in the two rounds of questionnaires.
The first-round questionnaire was delivered at the RUA meeting, during which experts received a brief overview of the project. Each expert was, then, asked to fill the Delphi survey anonymously. Participants were asked to rate their agreement to each statement from 0 to 4 (0, complete disagreement; 4, complete agreement) in a 5-point Likert-type scale. Text-free space was allocated to encourage comments. The median consensus score (MED) and the interquartile range (IQR) were calculated for each statement. A consensus on a statement was achieved if the MED (expressed as value at which at least 50% of participants agreed) was 4 and the IQR was 3–4.
In the second-round questionnaire, the first-round MED and IQR values for each statement were enclosed and statements were re-scored and re-rated. Experts had the option to explain their choices in a comments section. The second-round questionnaire was sent by e-mail to participants and, once completed, the final MED and IQR values were re-calculated. Also, amendments of statements were allowed in round 2.
Feedback was also provided on the interest of the participants in the RUA project.
Since this study is not considered as a clinical trial per local law, the approval of an Ethics Committee was not required.
Statistical Analysis
Qualitative variables were summarized with absolute and relative (percentages) frequencies, whereas quantitative variables were described using means (standard deviations) or medians (interquartile ranges) based on their parametric and non-parametric distribution, respectively.
Chi-squared or Fisher exact tests were used to compare groups in relation to qualitative variables. A two-tailed p-value of less than 0.05 was considered statistically significant. The statistical software used for all statistical computations was STATA version 14 (StataCorp, Texas, US).
Results
The first-round questionnaire was filled by 190 experts during the RUA meetings in October 2018. Experts were representative of both the entire national territory and population density (69 from Northern Italy, 63 from Central Italy and 58 from Southern Italy) and were specialized physicians in 81% of cases (30% oncologists, 13% specialized in anesthesia, 13% palliative care specialists, 44% other specialists, including specialized in geriatrics, neurosurgery, surgery, internal medicine, hematology, gastroenterology, infectiology, radiotherapy); they had an average experience in palliative care of 9.27 years both in hospital/hospice (65.1%) and in homecare assistance (34.9%) and they cared an average of 181.3 patients per year (range 10–1000 patients/year).
The second-round questionnaire was sent by e-mail in January 2019 to all 190 experts who participated in the first round: 149 participants answered, achieving a response rate of 78%.
As shown in Table 1, a consensus was reached for 17 statements. Statements concerning pain assessment achieved the highest level of agreement, with more than 70% of the experts were in complete agreement with them. Particularly, the statement “Clinicians should evaluate qualitative and quantitative characteristics of pain, in particular circadian exacerbations, by using validated scales” obtained complete agreement among 86.8% of participants in the first round of the Delphi survey, and maintained this high level of agreement in the second round (85.2%). Similarly, most participants (95.3% in the first round and 91.3% in the second round) completely agreed with the item “Clinicians should always evaluate if and how pain does affect daily activities and sleep, possibly interacting with the patient”.
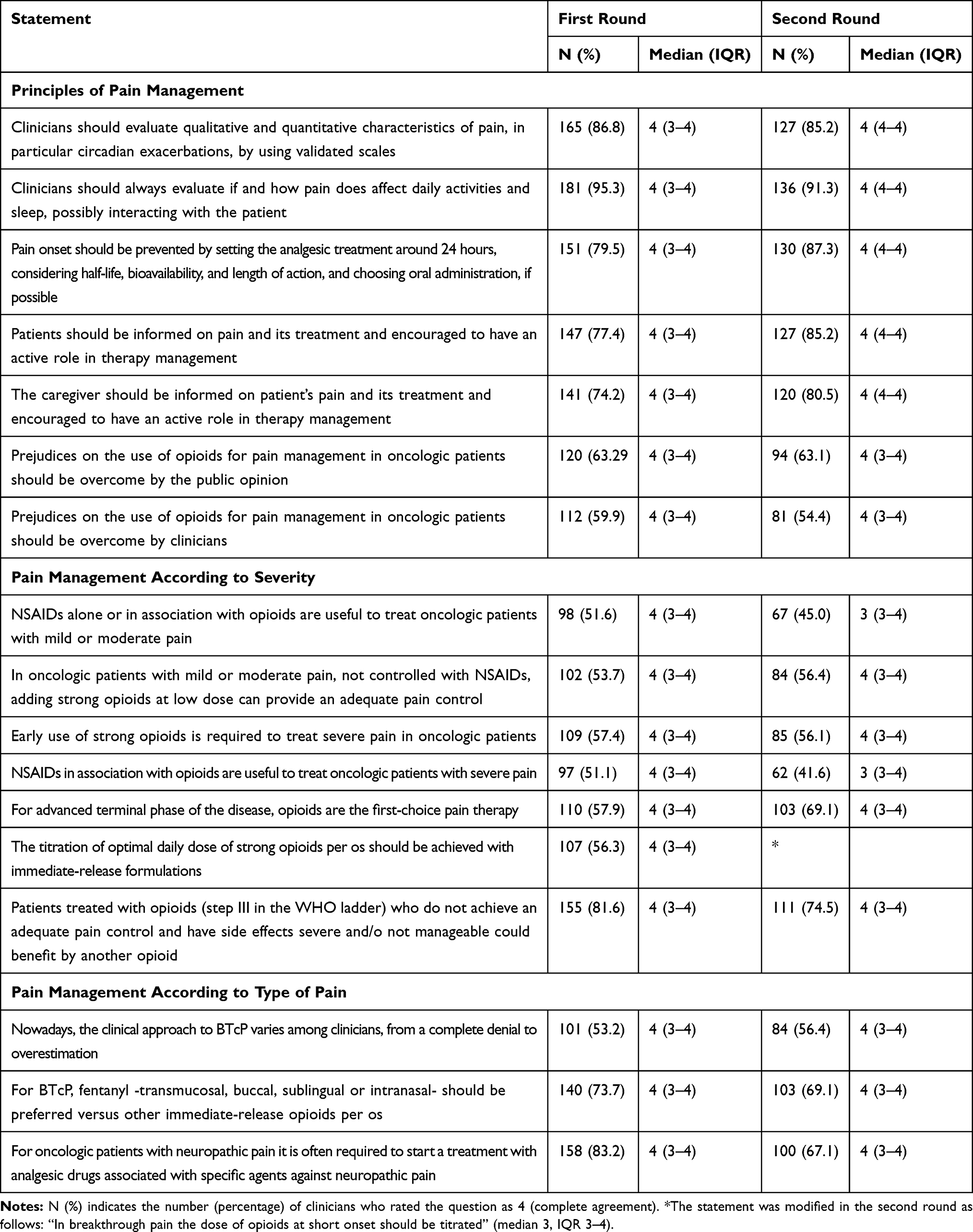 |
Table 1 Statements with a Consensus in Both the First and Second Rounds of the Delphi Survey |
Regarding the statements concerning the principle of pain management, the item "Pain onset should be prevented by setting the analgesic treatment around 24 hours, considering half-life, bioavailability, and length of action, and choosing oral administration, if possible" achieved a consensus among 79.5% of participants in the first round and the rate of agreement increased in the second round, reaching 87.3%. Furthermore, there was a high consensus on the importance of involving patients and their caregivers in pain management, as indicated by the agreement rates on the following statements: “Patients should be informed on pain and its treatment and encouraged to have an active role in therapy management” (77.4% completely agreed in the first round and 85.2% in the second round) and “The caregiver should be informed on patient’s pain and its treatment and encouraged to have an active role in therapy management” (74.2% agreed in the first round and 80.5% in the second round). The two statements on pain management according to severity had mixed consensus scores. In the first and second rounds, 81.6% and 74.5% of the participants, respectively, were in complete agreement with "Patients treated with opioids (step III in the WHO ladder) who do not achieve an adequate pain control and have side effects severe and/o not manageable could benefit from another opioid".
In contrast, participants disagreed with the statement “In oncologic patients with severe pain, not controlled with non-opioid analgesics adding a weak opioid provides an adequate analgesia” (67.9% and 16.3% gave scores of 0 and 1, respectively, [MED 0, IQR 0–1]).
For the other items concerning pain management according to pain severity or type of pain, the overall agreement (adding combined scores of 3 and 4) was again higher than 70%, with the majority of participants in complete agreement (score 4).
Eight statements did not reach a consensus: the statements concerning the current validity of WHO guidelines did not achieve a consensus in either rounds of the Delphi survey, even after being rewritten for the second round. Furthermore, there was a common disagreement on statements regarding the use of pharmacological agents, including paracetamol, corticosteroids and opioids (Table 2).
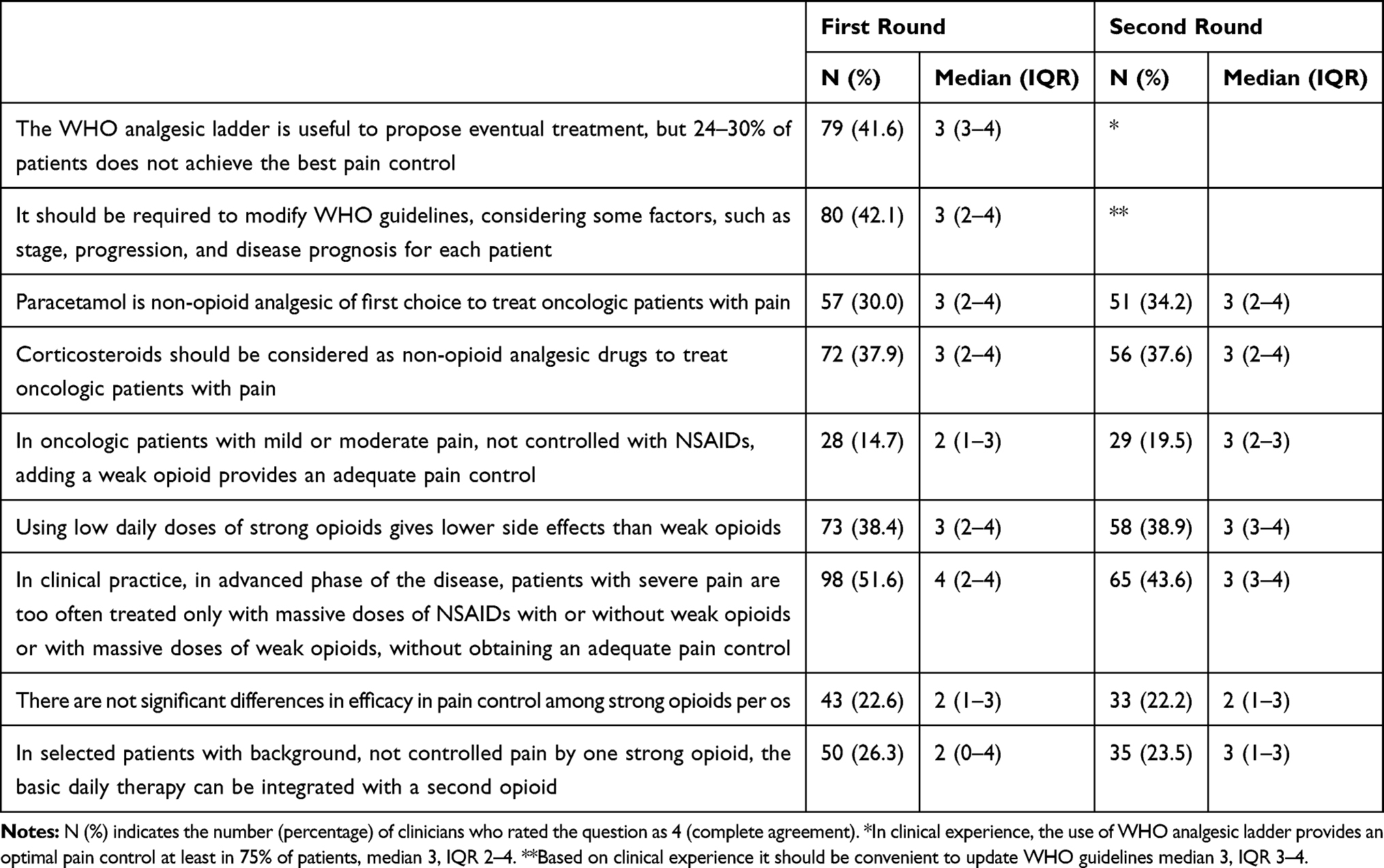 |
Table 2 Statements Without a Consensus in Either the First or Second Rounds of the Delphi Survey |
Overall, the RUA project, including meetings, discussions and the Delphi survey, was well received by the participants and was scored to be constructive and useful by 81.6% of the participants.
Discussion
This Delphi survey was set out to assess statements regarding overall pain management, application of the WHO analgesic ladder and BTcP among Italian oncologists and palliative care specialists. The statements were formulated on the basis of recent guidelines1 with the aim to identify some potential gaps between these documents and the real-world practice. A literature review was also performed to historically track the debate on pain management and discuss on current validity of WHO ladder and to consider the most relevant approaches that are usually utilized in clinical pain management. A third group of statements concerned the most specific and crucial topic of BTcP management, based on the results of a recent clinical study8 and literature review.9
A consensus was gained on all statements that covered the assessment, general principles and management as per type of pain (neuropathic and BTcP). There was disagreement on certain items regarding the pharmacological approaches to manage mild-to-moderate and moderate-to-severe pains.
All participants/responders valued the importance of pain assessment and setting-up the subsequent therapy through the active involvement of patients and their caregivers. The initial and ongoing assessment of pain is considered as an integral part of cancer care and should indicate if an additional comprehensive evaluation would be needed. The usefulness of WHO ladder in pain management was under debate and two items regarding this topic did not reach a consensus. The participants did not agree on items on the use of paracetamol and corticosteroids in cancer pain management. As most oncologists and palliative care specialists highlighted that still there is prejudice on the use of opioids among both clinicians and lay population, this uncertainty may partially explain the lack of consensus in items regarding the use of weak or strong opioids in treating uncontrolled pain. No difference of opinion was observed by the geographical distribution of participants or their specialties.
The participants in this Delphi survey agreed that nonsteroidal anti-inflammatory drugs (NSAIDs), alone or in combination with opioids, could be used to manage mild-moderate and severe pains. NSAIDs are useful for mild to moderate pain with an inflammatory component (eg, bone metastases or fungating lesions). Regularly scheduled NSAIDs should be taken for maximal efficacy and adding an NSAID to an opioid for severe pain may enhance analgesia and allow lower opioid doses.14 In the choice of an NSAID, it should be considered that those with longer half-life require less frequent dosing but may increase the risk for adverse effects, especially in elderly or unhealthy people. Furthermore, NSAIDs have an analgesic ceiling, above which only toxicity increases. A safe strategy is topical NSAID application over a painful site, which may decrease pain with little risk for systemic absorption and adverse effects.14
According to the Delphi survey results, the use of strong opioids is useful to treat uncontrolled pain, severe pain and end-of-life pain. The role of weak opioids, however, was less agreed on amongst participants. The unreached consensus on items concerning weak opioids reflects the debate on these drugs in the management of cancer pain. The effectiveness of weak opioids – the second step of the WHO ladder – was limited to 30–40 days for most patients because of insufficient analgesia, rather than to adverse effects.3 Despite similar side effects, such as constipation, drowsiness and nausea, several clinical trials reported that weak opioids were less effective than strong opioids in controlling chronic pain.5 Therefore, many authors suggested the elimination of the second step in the WHO ladder or the introduction as the second step of strong opioids at low dosing (morphine <30 mg/die, oxycodone <20 mg/die, even in combination with paracetamol).3,5,14
BTcP is defined as a transitory flare of pain that occurs on a background of relatively well-controlled baseline pain.1,15 The use of immediate-release opioids and transmucosal fentanyl to treat unpredictable and rapid-onset BTcP is proposed by the ESMO guidelines; in the case of slow-onset or predictable BTcP, standard normal-release oral opioids (eg, morphine) are recommended.1 Participants in this Delphi study agreed about the existence of a wide range of BTcP attitudes and perceptions in clinical practice, but a consensus was achieved on the use of fentanyl formulations to manage BTcP and on dosing titration with immediate-release formulations.
Neuropathic cancer pain arises as a direct consequence of a cancer-induced injury to the somatosensory system. This type of neuropathic cancer pain must be distinguished from other neuropathic pains, eg, due to cancer treatment.1 ESMO guidelines suggest that non-opioid and opioid analgesics may be combined with tricyclic antidepressants (TCAs) or anticonvulsants in cancer patients with neuropathic pain. The efficacy and tolerability of the therapy should be monitored over time.1 Gabapentin, pregabalin, TCAs and serotonin reuptake inhibitors (SNRIs) are strongly recommended as single agents for first-line treatment against neuropathic pain.10 Gabapentin and pregabalin bind to and modulate voltage-gated calcium channels, inhibit neurotransmitter release, and stabilize neuronal cell membranes.10 Either drug usually relieves neuropathic cancer pain within 1 to 2 weeks. Starting dose is 100 mg three times per day, but a single 300-mg dose at bedtime may aid sleep and minimize daytime sleepiness. Pregabalin has linear pharmacokinetics, therefore dosing is straightforward. Patients who tolerate the first dose level (150 mg/day) but do not attain pain relief can be increased to 300 mg/day after 1 week and to 600 mg/day a week later.10 The TCAs inhibit norepinephrine and serotonin reuptake at dorsal spinal cord synapses and secondarily block neural sodium channels and NMDA glutamate receptors. In a meta-analysis, TCA confirmed their effectiveness in about one-third of patients who experienced almost 50% relief of neuropathic pain, and only 4% had dose-limiting adverse effects.16 Among selective SNRIs, duloxetine and venlafaxine are effective for neuropathic pain and have fewer adverse effects than TCAs.16 Duloxetine dosing is simple: 60 mg once or twice a day is equally effective and safe since duloxetine does not cause clinically important electrocardiographic or blood pressure changes. Cardiovascular effects are rare with venlafaxine, which typically decreases pain after the dose is increased from 75 mg to ≥150 mg/day.10
When these drugs are not enough to achieve pain control by themselves, they are used in association with opioids.1,10 Participants agreed with the latter statement, as reflected in the consensus on the need to associate the use of analgesics and specific agents against neuropathic pain.
Conclusion
The results from the RUA project reflected the importance of pain management among Italian palliative care specialists, who agreed that both the assessment and control of pain are pivotal in the management of patients with cancer. This study highlighted also the differences between guidelines and clinical practice, and the need to overcome such challenges to ensure an effective pain management. Despite the Delphi method limitations, we obtained a high agreement rate. Nevertheless, one third of the proposed statements did not reach the consensus; the still uncertain ones concerned the current validity of WHO guidelines and the peculiar use of paracetamol, corticosteroids and opioids. Further debate could contribute to better understand how cancer pain could be properly managed in clinical practice and how pharmacological options, especially opioids, must be used amongst oncologists and palliative care specialists.
Acknowledgments
This study has been possible thanks to the unconditional support of Paolo Procacci Foundation. Editorial support was funded by L. Molteni & C Dei Fratelli Alitti and provided by Content Ed Net, with the helpful contribution of Elisa Sala, PhD, Medical Writer, in drafting the text and Mr. Bilal Bham and Hussein Hijazi in the final reading of the manuscript for English language improvement. Collaborators for this study are as follows: Adile C, Aicardi M, Aiello A, Alessandri AC, Alfieri S, Alongi A, Angilletta N, Angiolillo SM, Apicella A, Apicella S, Ballarin S, Balloni AG, Barchetta R, Barone AB, Bellavia G, Bergamini C, Bertolucci A, Betti E, Bilani F, Bonato C, Borando M, Brizio A, Brogi L, Bruera G, Brusco G, Burato AM, Calabrese G, Caldarulo C, Calligaris M, Canzio D, Carella C, Carinci PP, Carnicella A, Catania E, Cereda S, Cerera V, Chiadò Cutin S, Ciampo G, Cocchiarella A, Colombo LM, Conti A, Corsi G, Cortinovis D, Cossotto D, Costa F, Costanzo MG, Crispi M, Cuccu G, Dafni V, D’Alessandro S, D’amato G, De Clementi M, De Gasperi M, De Lisi A, De Meo A, De Ruvo M, De Santis S, De Tursi M, Defendi S, Degl’Innocenti M, Delli Santi I, Di Bartolomeo C, Di Ciaula G, Di Fonzo C, Di Marzo A, Di Prinzio M, D’Imporzano E, Diodati M, Drago A, Facciuto P, Falco V, Faraone E, Fassone F, Ferla F, Ferrara P, Fiorani AM, Flora R, Forno B, Franceschini G, Franchi B, Galbiati D, Galbiati F, Galizia B, Galli B, Gallio I, Gallo P, Gemelli MT, Gentile AL, Gialma Carlà L, Gildetti S, Ginex G, Giuliana F, Grassi U, Gravina S, Gucciardino C, leri T, Jamara G, La Marca L, Lanfranco C, Lo Mauro M, Luisi D, Lungu V, Mabilia R, Macaluso S, Maggipinto C, Maglio M, Maione A, Malorgio F, Mancuso A, Mangiola D, Mansueto G, Marciello L, Mariani M, Marinaccio M, Masi D, Mauceri M, Mazza L, Menegatti F, Messanelli RM, Mezzabotta M, Mirabile A, Mocci M, Montagna MC, Mortella A, Napolitano G, Nuzzolillo L, Occhigrossi F, Orlandi E, Orlandini G, Pacchioni M, Pace M, Pacifico C, Paladini A, Paolucci V, Pascazio AM, Patanella I, Pedaci E, Pellegrini A, Pepe V, Perin R, Perrone MA, Petrella G, Pinto TG, Pirajno G, Pollastrini C, Priori R, Prisco M, Putignano D, Rampello G, Ravoni G, Redivo L, Repole C, Ricchini F, Rigotti L, Rinaldi D, Ronga G, Rosafio, Roselli L, Ruggeri L, Saetta A, Sanzeni C, Sarnelli R, Sartore G, Sartori S, Sbanotto A, Schirinzi A, Scibilia C, Scriboni S, Semeraro L, Sergi G, Serrati A, Silverj E, Simone F, Sironi A, Sironi O, Sorbello P, Sosta E, Spinelli G, Tartaglia L, Taveggia D, Tempera S, Terranova A, Timpini A, Tinari N, Trapasso T, Trivellato E, Valente R, Vallisneri C, Visconti E, Zampi M, Zaza A, Zoccali S, Zuccarino L.
Disclosure
G. Varrassi is President of the Paolo Procacci Foundation. He is also consultant for several pharmaceutical companies and serves in some Editorial Board of scientific journals. The authors report no other conflicts of interest in this work.
References
1. Fallon M, Giusti R, Aielli F, et al. Management of cancer pain in adult patients: ESMO clinical practice guidelines. Ann Oncol. 2018;29(Supplement 4):iv166–iv191. doi:10.1093/annonc/mdy152
2. World Health Organization. Cancer Pain Relief. Geneva: Office of Publications, World Health Organization; 1986.
3. Ventafridda V, Tamburini M, Caraceni A, et al. A validation study of the WHO method for cancer pain relief. Cancer. 1987;59:850–856. doi:10.1002/1097-0142(19870215)59:4<850::AID-CNCR2820590432>3.0.CO;2-1
4. Marinageli F, Ciccozzi A, Leonardis M, et al. Use of strong opioids in advanced cancer pain: a randomized trial. J Pain Symptom Manage. 2004;27:409–416. doi:10.1016/j.jpainsymman.2003.10.006
5. Cuomo A, Bimonte S, CA F, et al. Multimodal approaches and tailored therapies for pain management: the trolley analgesic model. J Pain Res. 2019;12:711–714. doi:10.2147/JPR.S178910
6. Guerard EJ, Cleary JF. Managing cancer pain in older adults. Cancer J. 2017;23(4):242–245. doi:10.1097/PPO.0000000000000276
7. Konstantis A, Exiara T. Family caregiver beliefs and barriers to effective pain management of cancer patients in home care settings. J BUON. 2018;23(7):144–152.
8. Mercadante S, Adile C, Masedu F, et al. Factors influencing the use of opioids for breakthrough cancer pain: A secondary analysis of the IOPS‐MS study. Eur J Pain. 2019;23:719–726. doi:10.1002/ejp.1339
9. Zucco F, Bonezzi C, Fornasari D. Breakthrough cancer pain (BTcP): a synthesis of taxonomy, pathogenesis, therapy, and good clinical practice in adult patients in Italy. Adv Ther. 2014;31:657–682. doi:10.1007/s12325-014-0130-z
10. Wickham RJ. Cancer pain management: comprehensive assessment and nonopioid analgesics, part 1. Adv Pract Oncol. 2017;8:475–490.
11. Jones J, Hunter D. Consensus methods for medical and health services research. BMJ. 1995;311:376–380. doi:10.1136/bmj.311.7001.376
12. Keeney S, Hasson F, McKenna H. Consulting the oracle: ten lessons from using the Delphi technique in nursing research. J Adv Nurs. 2006;53(2):205–212. doi:10.1111/j.1365-2648.2006.03716.x
13. Keeney S, Hasson F, McKenna H. The Delphi Technique in Nursing and Health Research. West Sussex: John Wiley & Sons Ltd; 2010:55.
14. Caraceni A, Hanks G, Kaasa S, et al. Use of opioid analgesics in the treatment of cancer pain: evidence-based recommendations from the EAPC. Lancet Oncol. 2012;13(2):e58–e68. doi:10.1016/S1470-2045(12)70040-2
15. Løhre ET, Klepstad P, Bennett MI, et al. From “breakthrough” to “episodic” cancer pain? A European Association for Palliative Care Research Network Expert Delphi survey towards a common terminology and classification of transient cancer pain exacerbations. J Pain Symptom Manage. 2016;51(6):1013–1019. doi:10.1016/j.jpainsymman.2015.12.329
16. Vadalouca A, Raptis E, Moka E, et al. Pharmacological treatment of neuropathic cancer pain: a comprehensive review of the current literature. Pain Pract. 2012;12(3):219–251. doi:10.1111/j.1533-2500.2011.00485.x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.