")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Can Goal-Based Health Management Improve the Health Knowledge, Health Belief and Health Behavior in People at High Risk of Stroke? A Non-Randomized Controlled Trial
Authors He Y , Guo L , Liu Y, Wei M, Guo Y , Dong X , Yang C, Zhou Q, Lei X, Zhang G, Zhang M
Received 18 August 2021
Accepted for publication 23 September 2021
Published 8 October 2021 Volume 2021:17 Pages 3085—3095
DOI https://doi.org/10.2147/NDT.S334229
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jun Chen
Supplementary video 1 of "Effectiveness of goal-based health management" [ID 334229].
Views: 39
Yu He,1 Lina Guo,1 Yanjin Liu,2 Miao Wei,1 Yuanli Guo,1 Xiaofang Dong,1 Caixia Yang,1 Qing Zhou,3 Xiaoyu Lei,4 Gege Zhang,1 Mengyu Zhang4
1Department of Neurology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China; 2Department of Nursing, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China; 3Department of Rehabilitation, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China; 4College of Nursing, Zhengzhou University, Zhengzhou, People’s Republic of China
Correspondence: Yanjin Liu
Department of Nursing, The First Affiliated Hospital of Zhengzhou University, No. 1, Jianshe East Road, Erqi District, Zhengzhou, People’s Republic of China
Tel +86 183 9206 1307
Email [email protected]
Purpose: To examine the effectiveness of goal-based health management on health knowledge, health belief and health behavior in people at high risk of stroke.
Patients and Methods: This is a two-armed and non-randomized controlled trial from May 31, 2020 to December 31, 2020. Participants were arranged to receive regular health care (n=126) or goal-based health management (n=126). The generalized estimation equation was used to analyze the changes in the participants’ health knowledge, health belief and health behavior at baseline (T0), 1-month (T1), 3-month (T3), and 6-month (T6).
Results: A total of 243 participants completed the 6-month study, of which 123 were in the control group and 120 were in the intervention group. After receiving goal-based health management, participants’ health behavior (β= 27.154, p< 0.001), health knowledge (β= 10.504, p< 0.001) and health belief (β= 49.057, p< 0.001) scores increased significantly.
Conclusion: Goal-based health management can effectively improve the health knowledge, health belief and health behavior of people at high risk of stroke. We recommend that nurses can provide goal-based health management for people at high risk of stroke with support from hospitals and family members of people at high risk of stroke.
Keywords: stroke, prevention, goal setting theory, ecology of health
Introduction
Stroke has always been a global concern that cannot be ignored. Although the prevalence of stroke has declined, the aging of the population and the cumulative risk factors have led to an increased lifetime risk of stroke.1,2 The global average lifetime risk of stroke increased from 22.8% in 1990 to 24.9% in 2016.3 About 2.4 million people are diagnosed with stroke and 1.1 million die from the disease each year, with more than 11.1 million stroke patients in China every year.4
There are eight major risk factors for stroke in China: history of hypertension, diabetes, hyperlipidemia, heart disease or atrial fibrillation (AF); family history of stroke; obesity; lack of physical exercise; and smoking. People over 40 years old, with three or more factors, or with a history of stroke or transient ischemic attack (TIA) can be considered at high risk of stroke.5 Fortunately, long-term health behavior has been shown to reduce the incidence of stroke to less than 10%.6 And a cross-sectional survey shows that health knowledge and health belief are the influencing factors of health behavior.7 It is necessary to strengthen public education, screen those at high risk of stroke who need targeted treatment, and control risk factors by promoting a healthy lifestyle.8
Health management originated in the United States, where commercial medical insurance plays an extremely important role.9 The purpose of health management is from “disease intervention” to “disease prevention” and from “treatment of symptoms but not the cause of disease” to “treatment of both symptoms and cause”.10 Since the concept of health management was introduced into China at the end of the 20th century, it has been developed obviously in theoretical education and industrial practice.11 To explore a new health management mode, the National Stroke Prevention and Treatment Engineering Committee launched the cultivation program for stroke health managers (renamed as brain and heart health managers in 2018) in 2017, aiming to provide pre-hospital, in-hospital and post-hospital health management services for people at high risk of stroke (including patients with a history of stroke) with hospital support.12 The main responsibility is to conduct systematic, standardized and individualized scientific management for people at high risk of stroke through systematic cultivation, so as to reduce the incidence rate and recurrence rate of stroke.13
Previous health management programs do not seem to consider helping participants set goals.14–17 There is a review suggesting that setting goals can promote health behavior.18 The connotation of Goal Setting Theory is that when people promise and work hard for the goal, it is possible to achieve the desired result.19 Walker and Avant believed that the goals should have five characteristics: clarity; reality; quantification; time limit; and related to the desired result.20 Goals are divided into internal goals and external goals. Individuals pursuing internal goals (eg physical health and hedonism) are more likely to engage in activities that can lead to positive behavioral outcomes; while individuals pursuing external goals (eg financial success and popularity) has the opposite effect.21
The Goal Setting Theory points out the direction for the health management of people at high risk of stroke, while the Ecology of Health guides the process of health management. Ecology of Health advocates that individual health is the result of the interaction between individual and environmental factors.22 This theory believes that it is not only personal characteristics and lifestyle that can affect personal health, but also external environment, medical health, interpersonal culture and other factors.23 Our health management is jointly participated by one hospital, three communities, families, and individuals. Brain and heart health managers connected each part as a “bridge” in the process.
Patients and Methods
Objective
To analyze whether goal-based health management can improve the health knowledge, health belief and health behavior in people at high risk of stroke.
Design
This paralleled and non-randomized controlled trial from July 1, 2020 to December 31, 2020 was conducted in 3 communities in Zhengzhou City, Henan Province, China (30 people at high risk of stroke participated in the preliminary trial in June 2020.). Participants who are quarantined due to the prevention of the Corona Virus Disease-19 cannot participate in group meetings or activities and they were included in the controlled group. This study was registered before implementation (Clinical Trials. ChiCTR2000032817).
Study Interventions
Health Management Team
The health management team in this study was composed of neurologists (n=2), brain and heart health managers (neurology nurses) (n=4), rehabilitation therapist (n=1), contracted services of family doctors (community physicians) (n=4), and community health nurses (n=4). Neurologists, brain and heart health managers (neurology nurses) and the rehabilitation therapist were from the same hospital. The brain and heart health managers led the management activities of the entire team and they were responsible for helping contact team members.
Routine Care
During the trial, neurologists, contracted services of family doctors and rehabilitation therapists were invited once a month to preach the knowledge of stroke disease to the control group members through Tencent Meeting (an online conference tool, which can be linked through WeChat). There were two courses in each meeting, each lasting approximately one hour. At the end of each meeting, we distributed related health manuals to the control group participants (Appendix 1 shows the contents of courses).
Goal-Based Health Management
First, the health management team set goals based on previous research.7 Then face-to-face interviews were conducted with 10 people at high risk of stroke (not included in the intervention group) and the goals were set (Appendix 2 shows the contents of the interview). Finally, “Health management every day to keep stroke away” was taken as the final goal of health management. “Know yourself and know stroke”, “Well begun is half done”, “Stroke can’t be prevented in one day” were taken as the themes at each stage of health management.
Know Yourself and Know Stroke
This stage lasted for a month. The goal was to enable people at high risk of stroke to acquire knowledge related to stroke diseases and prevention of stroke, as well as to fully understand their situation. In addition to providing knowledge of stroke disease to the intervention group participants every week, the health management team also assessed the health status of each participant and informed them of precautions. This increased the interaction and communication between researchers and participants, and could more effectively help participants solve health problems.24
Well Begun is Half Done
This stage lasted for two months. The purpose was to encourage people at high risk of stroke to actively participate in health management. During this period, in addition to imparting stroke-related chronic disease management knowledge, the health management team also organized participants to share health management experience. Team members, participants, and participants communicate with each other through WeChat. Brain and heart health managers followed up the participants by telephone every two weeks to help them solve the problems encountered in the health management process in time. Telephone follow-up could potentially increase the enthusiasm of people at high risk of stroke to participate in health management.25
Stroke Cannot be Prevented in One Day
This stage lasted for three months and aimed to supervise and promote the adherence to health management of people at high risk of stroke. In this stage, the competition was added based on the intervention methods of the previous stage, and people at high risk of stroke who actively participated in health management were praised and rewarded. This might encourage people at high risk of stroke to adhere to health management.26 (Appendix 3 supplements the detailed intervention content; supplementary video 1 and Supplementary video 2 are used to show researchers’ efforts to promote the ability of people at high risk of stroke to identify acute stroke and maintain a healthy diet.)
Participants
Inclusion and Exclusion
The following population were included in this study: a. beyond the age of 40 years; b. having three or more risk factors, or having a history of stroke or TIA (mentioned in the introduction); c. having clear consciousness to complete the research; d. agreeing to participate. People at high risk of stroke with other serious acute or chronic diseases were excluded.
Sample Size
Health behavior was used as the main indicator to calculate the sample size in this study. The results (X1 =100.26, X2 =105.34, σ=17.57) of preliminary trial in 30 people at high risk of stroke were uploaded to a website that calculated the sample size (http://powerandsamplesize.com/Calculators/). The sample size was calculated to be 188 cases. Considering that there may be a 15% sample loss rate, the sample size was estimated to require at least 221 cases.27 Finally, we recruited 252 participants.
Data Collection
The results of the study were collected before the intervention (T0), 1-month (T1), 3-month (T3), and 6-month of the intervention (T6). Four trained researchers collected data through phone calls or face-to-face interviews. No hints are made to participants during the collection process. Take it back immediately after the participants complete the questionnaires. One-to-one collection of data ensured the integrity and reliability of the data. The data was entered into the computer in parallel by two researchers and others randomly checked the data before the analysis.
Outcomes and Measurements
Demographic variables: age, gender, spouse status, education level, capita monthly household income, sleep duration, family history of stroke, history of transient ischemic attack (TIA)/ stroke, hypertension, diabetes mellitus; dyslipidemia; coronary heart disease; overweight or obesity (BMI>26kg/m2); smoking; drinking and few physical activities. The 9-year of formal education was used to divide the education level. It’s a unique demarcation standard of education in China. Because tuition does not need to be paid for 6 years until high school.
The Stroke Prevention Knowledge Questionnaire (SPQ) was developed by Sun Yat-sen University in China.28 The questionnaire includes 36 items and 8 dimensions, namely daily life (8 items), exercise (4 items), diet (4 items), stroke risk factors (5 items), medication (5 items), blood pressure monitoring (2 items), stroke signs (6 items), stroke management (2 items). Each item has two options: “Know” or “Don’t know”. “Know” counts 1 point, “Don’t know” counts 0 point. This questionnaire has been widely used to investigate the health knowledge of stroke patients and confirmed that Cronbach’s alpha coefficient is 0.791.
The Champion Health Belief Model Scale (CHBMS) in the Chinese version has 33 items and 6 dimensions, including perceived susceptibility (5 items), perceived seriousness (6 items), perceived benefits (6 items), perceived barriers (6 items), health cues to action (5 items) and self-efficacy (5 items).29 The scale uses a Likert five-level scoring method, ranging from “completely disagree” to “completely agree” with a score of 1–5. The higher the score, the higher the belief in taking corresponding health behavior. The Cronbach’s α coefficient of the scale is 0.833.
The Health Promoting Lifestyle Profile II (HPLP II) is revised based on the HPLP.30 It was translated into Chinese and promoted to measure the health behavior of people at high risk of stroke.28 The scale includes 52 items and 6 dimensions: health responsibility (9 items), exercise (8 items), nutrition (9 items), self-actualization (9 items), interpersonal relationship (9 items) and stress response (8 items). Each item on the scale uses a Likert 4-level scoring method, ranging from “never” to “always” on a scale of 1–4 points, with a total score ranging from 52 to 208 points. The higher the score, the better the health behavior. This scale has good reliability and validity in China.31
Ethics
This experiment was approved by the ethics committee of the First Affiliated Hospital of Zhengzhou University (2018-KY-356). Participants were informed of the purpose and time of the trial before recruitment. Then they agreed to participate the trial through written documents. Participants had the right to withdraw at any time during the trial. Their personal information was stored in a computer folder with a password. And there will be no descriptions that can reveal the identity of the participants in the manuscript. This study was conducted in accordance with the Declaration of Helsinki.
Statistical Analysis
The results were statistically analyzed using IBM SPSS Statistics 21.0 software. The demographic characteristics of the participants were described by mean ± standard deviation (x ± s), frequency and percentage. Scale scores were described by mean ± standard deviation (x ± s). The differences between the two groups were compared through the Generalized Estimating Equation model (GEE). For repeated measurement data in clinical trials, the generalized estimation equation can effectively consider intra-group correlations and deal with data with missing values, which can evaluate health management effects more objective.32
Results
A total of 243 participants completed the 6-month study, of which 123 were in the control group and 120 were in the intervention group. The study flow is presented in Figure 1. Most of the participants were male, which is consistent with the characteristics of stroke disease in China.33 In this study, the age of the participants was high (range: 41–84 years, average age: 63.26±11.15) and the level of education was low (56.8% received less than 9 years of formal education). A small number of participants have a family history of stroke (19.8%) or a history of TIA (16.0%). Hypertension (58.5%) is the largest proportion of all risk factors among participants who completed this study. Table 1 lists the demographic characteristics of the population at high risk of stroke in the control group and the intervention group. There was no significant difference between the two groups of participants.
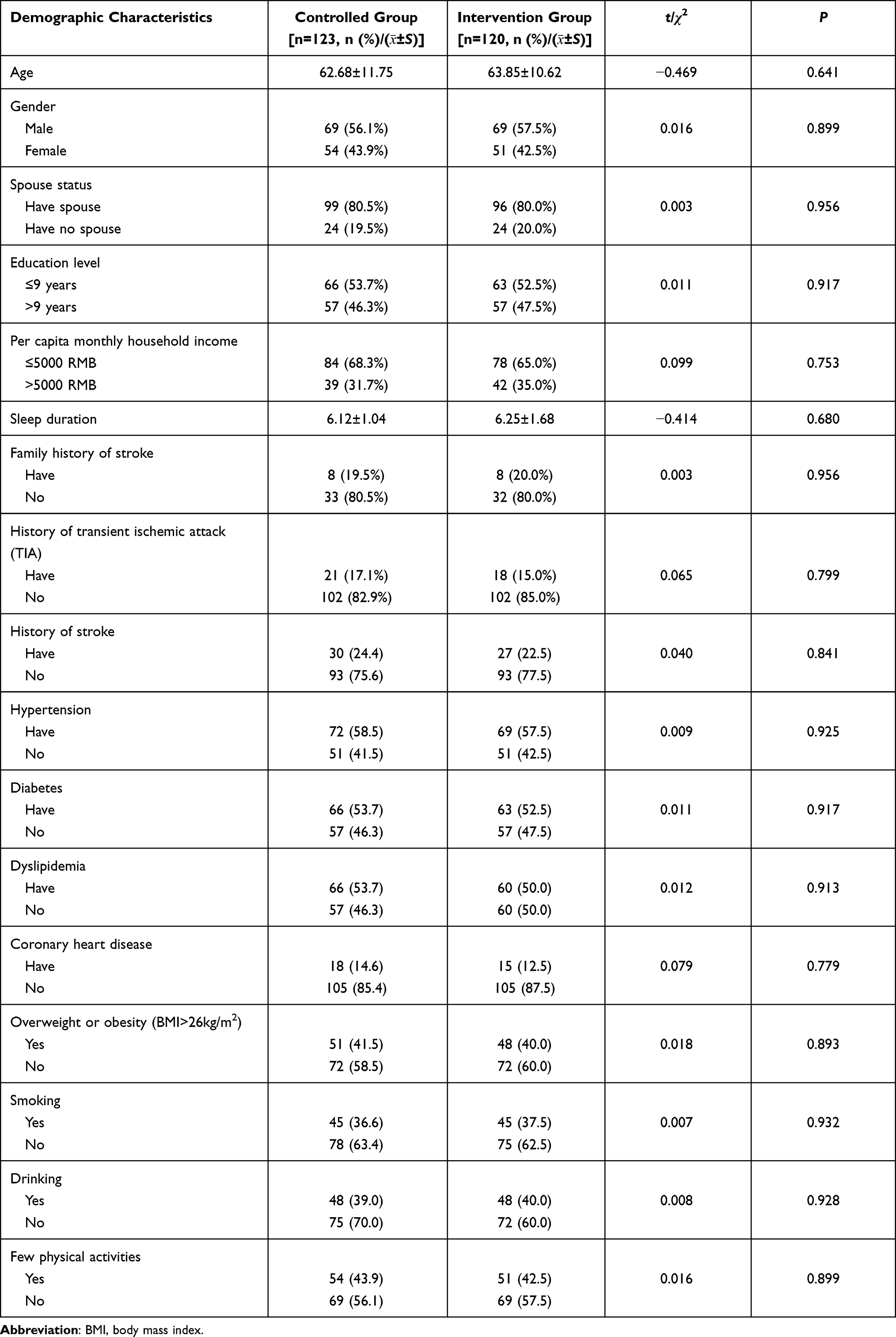 |
Table 1 The Demographic Characteristics of Participants |
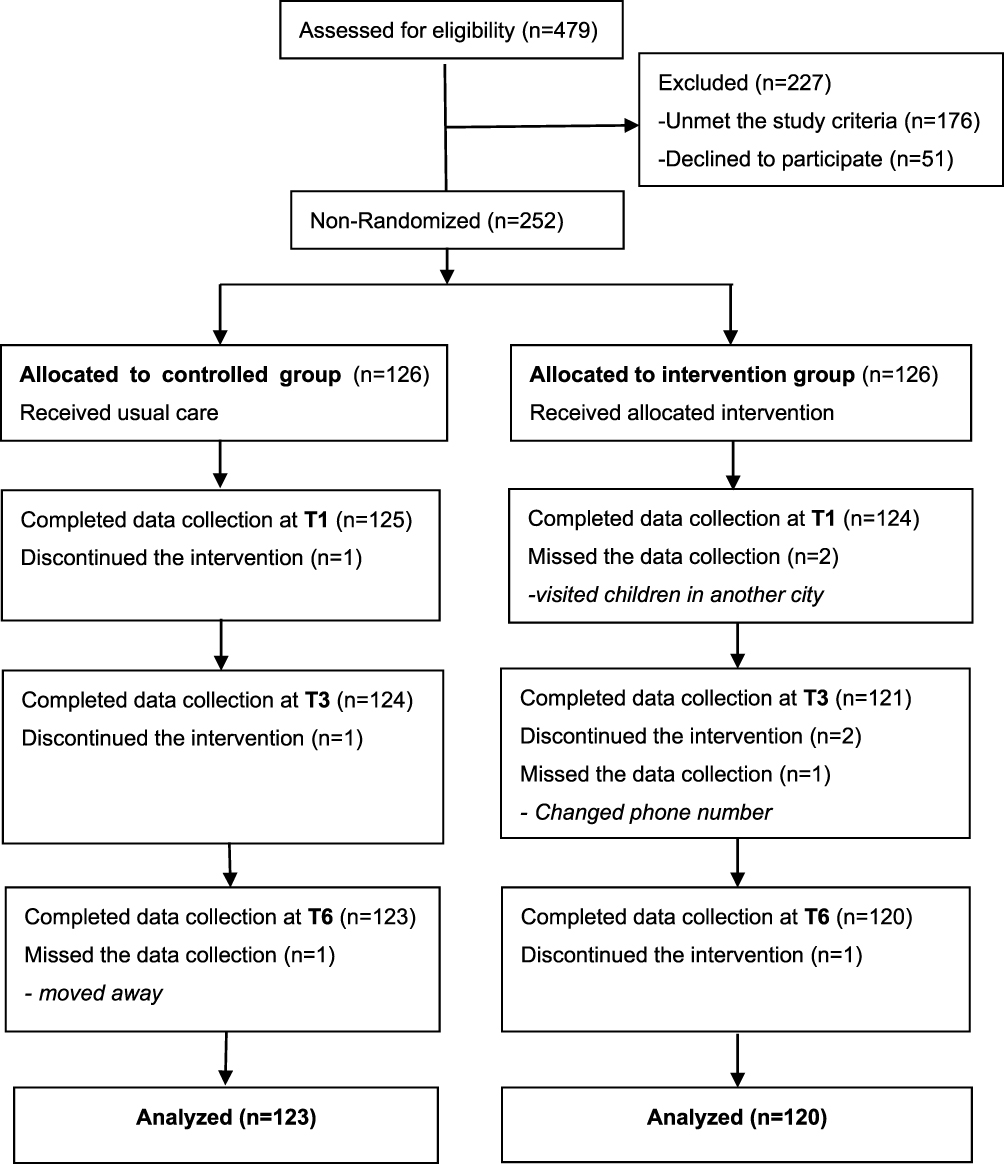 |
Figure 1 Flow diagram of participants. |
The effects of health management on the health knowledge, health belief and health behavior of people at high risk of stroke are represented by a Generalized Estimation Equation Model. The reference categories are the control group and the baseline values. Table 2 shows the mean and standard deviation of the health knowledge, health belief and health behavior of the two groups of people at high risk of stroke at the four measurement time points (T0, T1, T3, T6). After one month of goal-based health management, there were no significant differences in the scores of health behavior (β=2.279, p=0.641) between the two groups. After 6 months of health management, the average health behavior score of the control group rose from 101.24 to 119.56, and the intervention group rose from 101.48 to 140.00 (β=27.154, p<0.001). The health knowledge (β=10.504, p<0.001) and health belief (β=49.057, p<0.001) of participants in the intervention group also have been significantly improved.
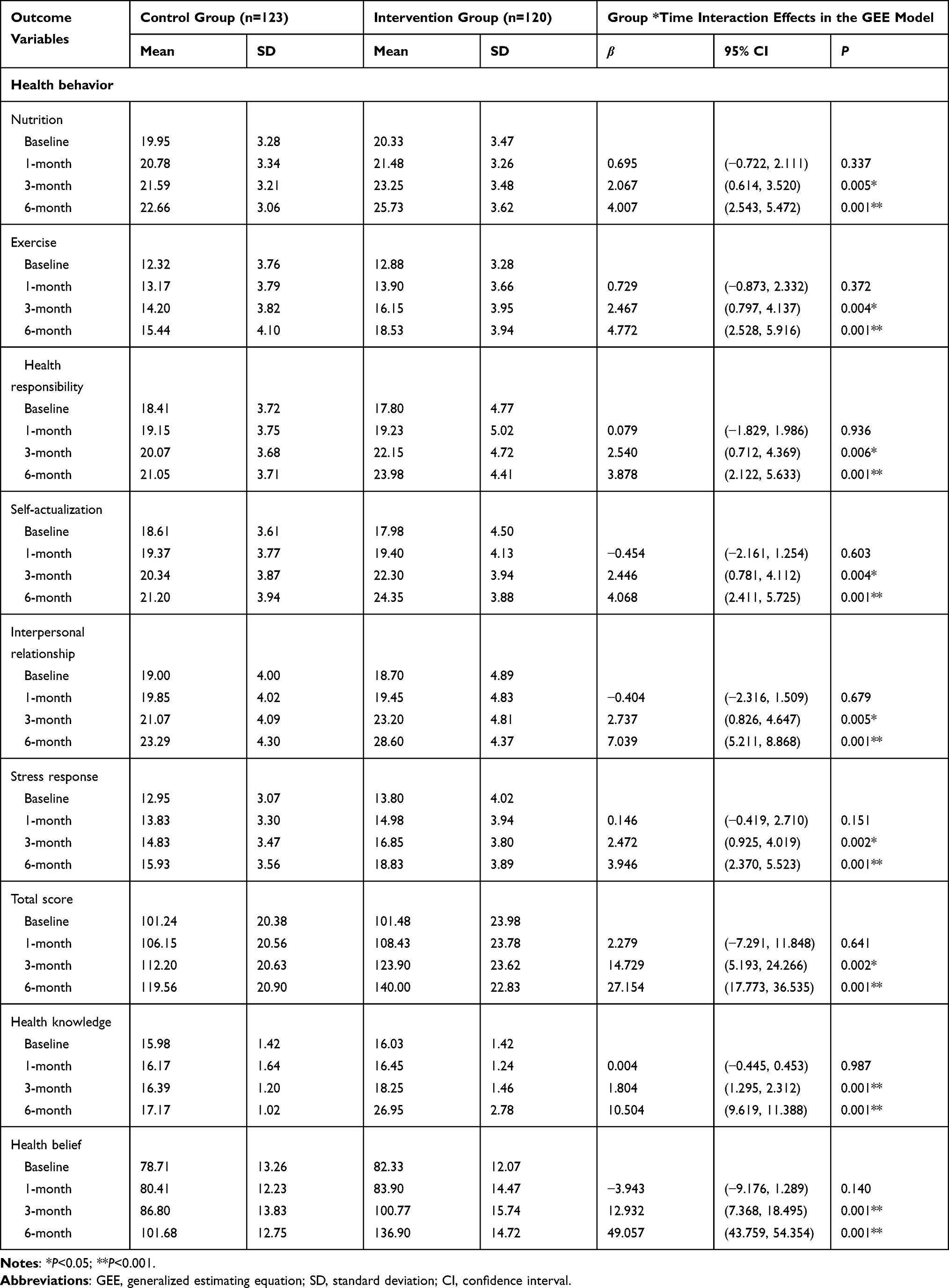 |
Table 2 Effectiveness of Goal-Based Health Management on Health Knowledge, Health Belief and Health Behavior |
Discussion
Goal-based management can promote the communication between managers and the managed and improve the effectiveness of problem solving.34 The goals for the three different stages of health management are determined by the researchers in collaboration with the participants, which can ensure the quality of the goals.35 The intervention aimed to enable people at high risk of stroke to adhere to health management to prevent stroke. The goal of each stage was consistent with this ultimate goal, which helped participants gradually receive health management. Measurement indicators and questionnaires helped researchers determine whether participants have achieved the goals of each stage. Our three goals are clear, time-limited, achievable, measurable, and consistent with expected results, which may be beneficial to health management.18
In this study, after one month, the health knowledge scores of the two groups of participants were not statistically different from the baseline. The reasons may be as follows: according to the arrangement, the two groups did not complete all courses in the month; participants did not use knowledge to maintain health. Knowledge can guide health behavior.36 In turn, health behavior can help participants better receive health knowledge.37 Health belief is the driving force of health behavior.38 Effective improvement of knowledge, belief, and behavior is the most basic requirement of health management for people at high risk of stroke. The change of health behavior is of great significance to the improvement of health management.39
In this study, the health behavior of the two groups was improved at the end of the trial, but the scores of the participants who received goal-based health management increased more significantly. This provides evidence that goal-based health management has a positive impact on the health behavior of people at high risk of stroke. In the baseline measurement, in terms of the intervention group, people at high risk of stroke had the highest scores on the nutrition dimension (20.33±3.47), followed by interpersonal relationship (18.70±4.89), self-actualization (17.98±4.50), health responsibility (17.80±4.77), and stress response (13.80±4.02). The lowest score was on the exercise dimension (12.88±3.28). After 6 months of goal-based health management, the participants scored the highest in interpersonal relationship (28.60±4.37), while the exercise dimension scored still the least (18.53±3.94). We analyzed the reasons for this change. WeChat and Tik Tok were used to help researchers connect with participants and to share health information. Internet social platforms enhanced the communication effect and enabled participants to obtain emotional support, which may be related to the changes in the participants’ interpersonal relationship dimension scores.40 The lowest score in the exercise dimension may be due to the fact that people at high risk of stroke are generally older (age: 63.85±10.62 years), ie, older people unable to maintain enough time or fail to achieve moderate intensity during physical exercise due to illness or fission.41 Moreover, the scores of nutrition dimension after intervention (25.73±3.62) indicated that people at high risk of stroke have the consciousness to choose a low-salt and low-fat healthy diet. This is consistent with previous research.42,43
There are some limitations to this study. Firstly, due to the impact of the COVID-19, this study only selected 3 communities in the central region of China. If the goal-based health management in this study is extended to other cities or even other countries in the future, there may be different results. Then, due to the weather, we occasionally followed up by phone instead of face-to-face. Since information can only be exchanged over the phone, the researchers cannot directly observe the health status of the participants. However, there is evidence that telephone follow-up is valuable.44 Although the two follow-ups may cause slight differences, our results are still reliable. Finally, this study was designed as a non-randomized controlled trial, which may be difficult to ensure uniformity between the groups before intervention. To increase the reliability of the sample, we have increased the number of people at high risk of stroke selected as much as possible.
Conclusion
In this study, goal-based health management was led by brain and heart health managers, hospitals and communities jointly for people at high risk of stroke. Social media platforms were used in the management process. The health knowledge, health belief and health behavior of the participants in the intervention group were significantly improved compared with the control group. We recommend that medical professionals set goals when implementing health management for people at high risk of stroke.
Data Sharing Statement
A small part data supporting the results of the study can be available from “figshare” after contacting the author (https://figshare.com/articles/dataset/health_management/14559756). If you need the rest of the data, you can contact Yu He through email ([email protected]).
Acknowledgments
We are grateful to all the participants.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study is funded by Medical Science and Technology Project of Henan Province (Grant No. SBGJ2018003) and Chinese Nursing Association (Grant No. ZHKY202025).
Disclosure
None of the authors of this study had a conflict of interest.
References
1. Avan A, Digaleh H, Di Napoli M, et al. Socioeconomic status and stroke incidence, prevalence, mortality, and worldwide burden: an ecological analysis from the Global Burden of Disease Study 2017. BMC Med. 2019;17(1):191. doi:10.1186/s12916-019-1397-3
2. Virani SS, Alonso A, Benjamin EJ, et al. Heart Disease and Stroke Statistics-2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139–e596.
3. Feigin VL, Nguyen G, Cercy K, et al. Global, regional, and country-specific lifetime risks of stroke, 1990 and 2016. N Engl J Med. 2018;379(25):2429–2437.
4. Wang W, Jiang B, Sun H, et al. Prevalence, incidence, and mortality of stroke in China: results from a nationwide population-based survey of 480 687 adults. Circulation. 2017;135(8):759–771.
5. Wang J, Wen X, Li W, Li X, Wang Y, Lu W. Risk factors for stroke in the Chinese population: a systematic review and meta-analysis. J Stroke Cerebrovasc Dis. 2017;26(3):509–517.
6. Larsson SC, Åkesson A, Wolk A. Primary prevention of stroke by a healthy lifestyle in a high-risk group. Neurology. 2015;84(22):2224–2228.
7. Guo L, Liu Y, Zhu Y, Wei M. Identification of health behaviour clusters among people at high risk of stroke: a latent class profile analysis. J Adv Nurs. 2020;76(11):3039–3047.
8. Wu S, Wu B, Liu M, et al. Stroke in China: advances and challenges in epidemiology, prevention, and management. Lancet Neurol. 2019;18(4):394–405.
9. Lichtenstein RL. The United States’ health care system: problems and solutions. Surv Ophthalmol. 1993;38(3):
10. James P, Kuzel A, Thompson B, Davis A, Grumbach K. Evolving perspectives on population health management. Ann Fam Med. 2014;12(5):481–482. doi:10.1370/afm.1702
11. Jiang L, Sha T, Ming L, et al. The current situation and development of health management in China. Strateg Stud CAE. 2017;19(02):8–15.
12. Baohua C, Jianmin L, Yilong W, et al. Stroke prevention and control in China: achievements, challenges and responses. Chinese Circ J. 2019;34(7):625–631.
13. Wang S, Li Y, Tian J, et al. A randomized controlled trial of brain and heart health manager-led mHealth secondary stroke prevention. Cardiovasc Diagn Ther. 2020;10(5):1192–1199.
14. Xiumei L, Caiying G, Hongyan J, et al. Exploration and practice of “family doctor”service mode among stroke patients in communities. Chinese J General Pract. 2015;13(06):981–983.
15. Thrift AG, Srikanth VK, Nelson MR, et al. Risk factor management in survivors of stroke: a double-blind, cluster-randomized, controlled trial. Int J Stroke. 2014;9(5):652–657.
16. Fletcher K, Mant J, McManus R, Hobbs R; Programme Grants for Applied Research. The Stroke Prevention Programme: A Programme of Research to Inform Optimal Stroke Prevention in Primary Care. Southampton (UK): NIHR Journals Library Copyright © Queen’s Printer and Controller of HMSO 2016. This work was produced by Fletcher et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK; 2016.
17. Kaddumukasa M, Nakibuuka J, Mugenyi L, et al. Feasibility study of a targeted self-management intervention for reducing stroke risk factors in a high-risk population in Uganda. J Neurol Sci. 2018;386:23–28.
18. Eckhoff DO, Weiss J. Goal setting: a concept analysis. Nurs Forum. 2020;55(2):275–281.
19. Locke EA, Latham GP. Building a practically useful theory of goal setting and task motivation. A 35-year odyssey. Am Psychol. 2002;57(9):705–717.
20. Walker L, Avant K. Strategies for theory construction in nursing. Pearson Schweiz Ag. 2010;44(44):434–436.
21. Vansteenkiste M, Lens W, Deci EL. Intrinsic versus extrinsic goal contents in self-determination theory: another look at the quality of academic motivation. Educ Psychol. 2006;41(1):19–31.
22. Rapport DJ, Howard J, Lannigan R, McCauley W. Linking health and ecology in the medical curriculum. Environ Int. 2003;29(2–3):353–358.
23. Tarkowski S. Human ecology and public health. Eur J Public Health. 2009;19(5):447.
24. Ford-Gilboe M, Varcoe C, Scott-Storey K, et al. Longitudinal impacts of an online safety and health intervention for women experiencing intimate partner violence: randomized controlled trial. BMC Public Health. 2020;20(1):260.
25. Crocker JB, Crocker JT, Greenwald JL. Telephone follow-up as a primary care intervention for postdischarge outcomes improvement: a systematic review. Am J Med. 2012;125(9):915–921.
26. Spilt JL, Leflot G, Onghena P, Colpin H. Use of praise and reprimands as critical ingredients of teacher behavior management: effects on children’s development in the context of a teacher-mediated classroom intervention. Prev Sci. 2016;17(6):732–742.
27. Kim SH, Utz S. Effectiveness of a social media-based, health literacy-sensitive diabetes self-management intervention: a randomized controlled trial. J Nurs Scholarsh. 2019;51(6):661–669.
28. Wan LH, Zhao J, Zhang XP, et al. Stroke prevention knowledge and prestroke health behaviors among hypertensive stroke patients in mainland China. J Cardiovasc Nurs. 2014;29(2):E1–9.
29. Liu ZY, Zhao JJ, Gao LL, Wang AY. Glucose screening within six months postpartum among Chinese mothers with a history of gestational diabetes mellitus: a prospective cohort study. BMC Pregnancy Childbirth. 2019;19(1):134.
30. Walker SN, Sechrist KR, Pender NJ. The Health-Promoting Lifestyle Profile: development and psychometric characteristics. Nurs Res. 1987;36(2):76–81.
31. Zheng X, Yu H, Qiu X, Chair SY, Wong EM, Wang Q. The effects of a nurse-led lifestyle intervention program on cardiovascular risk, self-efficacy and health promoting behaviours among patients with metabolic syndrome: randomized controlled trial. Int J Nurs Stud. 2020;109:103638.
32. Bible J, Albert PS, Simons-Morton BG, Liu D. Practical issues in using generalized estimating equations for inference on transitions in longitudinal data: what is being estimated? Stat Med. 2019;38(6):903–916.
33. Li F, Yang L, Yang R, et al. Ischemic stroke in young adults of Northern China: characteristics and risk factors for recurrence. Eur Neurol. 2017;77(3–4):115–122.
34. Raia AP. Goal setting and self‐control: an empirical study. J Manag Stud. 1965;2(1):34–51.
35. Maiyer NRF, Hoffman LR. Using trained developmental leaders to improve further the quality of group decisions. J Appl Psychol. 1960;44(4):247–251.
36. Yao K, Yao Y, Shen X, Lu C, Guo Q. Assessment of the oral health behavior, knowledge and status among dental and medical undergraduate students: a cross-sectional study. BMC Oral Health. 2019;19(1):26.
37. Lockyer J, Gondocz ST, Thivierge RL. Knowledge translation: the role and place of practice reflection. J Contin Educ Health Prof. 2004;24(1):50–56.
38. Fouladi N, Pourfarzi F, Mazaheri E, et al. Beliefs and behaviors of breast cancer screening in women referring to health care centers in northwest Iran according to the champion health belief model scale. Asian Pac J Cancer Prev. 2013;14(11):6857–6862.
39. Adam L, O’Connor C, Garcia AC. Evaluating the impact of diabetes self-management education methods on knowledge, attitudes and behaviours of adult patients with type 2 diabetes mellitus. Can J Diabetes. 2018;42(5):470–477.e472.
40. Chen X, Sun M, Wu D, Song XY. Information-sharing behavior on WeChat moments: the role of anonymity, familiarity, and intrinsic motivation. Front Psychol. 2019;10:2540.
41. Li J, Yu J, Chen X, Quan X, Zhou L. Correlations between health-promoting lifestyle and health-related quality of life among elderly people with hypertension in Hengyang, Hunan, China. Medicine (Baltimore). 2018;97(25):e10937.
42. Bhandari P, Kim M. Predictors of the health-promoting behaviors of Nepalese migrant workers. J Nurs Res. 2016;24(3):232–239.
43. Zhang SC, Tao FB, Ueda A, Wei CN, Fang J. The influence of health-promoting lifestyles on the quality of life of retired workers in a medium-sized city of Northeastern China. Environ Health Prev Med. 2013;18(6):458–465.
44. Starr N, Gebeyehu N, Tesfaye A, et al. Value and feasibility of telephone follow-up in Ethiopian surgical patients. Surg Infect (Larchmt). 2020;21(6):533–539.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.