")
Back to Journals » Drug Design, Development and Therapy » Volume 9
Brivaracetam: review of its pharmacology and potential use as adjunctive therapy in patients with partial onset seizures
Authors Mumoli L, Palleria C, Gasparini S, Citraro R, Labate A, Ferlazzo E, Gambardella A, De Sarro G, Russo E
Received 21 August 2015
Accepted for publication 28 September 2015
Published 19 October 2015 Volume 2015:9 Pages 5719—5725
DOI https://doi.org/10.2147/DDDT.S81474
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Wei Duan
Laura Mumoli,1 Caterina Palleria,2 Sara Gasparini,1 Rita Citraro,2 Angelo Labate,1 Edoardo Ferlazzo,1 Antonio Gambardella,1 Giovambattista De Sarro,2 Emilio Russo2
1Institute of Neurology, 2Institute of Pharmacology, University Magna Græcia, Catanzaro, Italy
Abstract: Brivaracetam (BRV), a high-affinity synaptic vesicle protein 2A ligand, reported to be 10–30-fold more potent than levetiracetam (LEV), is highly effective in a wide range of experimental models of focal and generalized seizures. BRV and LEV similarly bind to synaptic vesicle protein 2A, while differentiating for other pharmacological effects; in fact, BRV does not inhibit high voltage Ca2+ channels and AMPA receptors as LEV. Furthermore, BRV apparently exhibits inhibitory activity on neuronal voltage-gated sodium channels playing a role as a partial antagonist. BRV is currently waiting for approval both in the United States and the European Union as adjunctive therapy for patients with partial seizures. In patients with photosensitive epilepsy, BRV showed a dose-dependent effect in suppressing or attenuating the photoparoxysmal response. In well-controlled trials conducted to date, adjunctive BRV demonstrated efficacy and good tolerability in patients with focal epilepsy. BRV has a linear pharmacokinetic profile. BRV is extensively metabolized and excreted by urine (only 8%–11% unchanged). The metabolites of BRV are inactive, and hydrolysis of the acetamide group is the mainly involved metabolic pathway; hepatic impairment probably requires dose adjustment. BRV does not seem to influence other antiepileptic drug plasma levels. Six clinical trials have so far been completed indicating that BRV is effective in controlling seizures when used at doses between 50 and 200 mg/d. The drug is generally well-tolerated with only mild-to-moderate side effects; this is confirmed by the low discontinuation rate observed in these clinical studies. The most common side effects are related to central nervous system and include fatigue, dizziness, and somnolence; these apparently disappear during treatment. In this review, we analyzed BRV, focusing on the current evidences from experimental animal models to clinical studies with particular interest on potential use in clinical practice. Finally, pharmacological properties of BRV are summarized with a description of its pharmacokinetics, safety, and potential/known drug–drug interactions.
Keywords: brivaracetam, epilepsy, partial seizure, adjunctive therapy, antiepileptic drugs
Corrigendum for this paper has been published.
Introduction
Although about two-thirds of patients with epilepsy (PWE) treated with antiepileptic drugs (AEDs) reach seizure-freedom, about one-third remains drug-resistant to the current therapies.1 Despite the introduction of new AEDs with a better pharmacokinetic and safety profile compared to old generation AEDs, today, one of the major causes of failure of antiepileptic treatment is poor adherence often due to occurrence of adverse drug reactions (ADRs), leading up to 25% of patients to discontinue treatment before the achievement of effective doses and with a consequent increase of health care costs.2,3
During the last 25 years, many efforts have been directed to the development of new AEDs with different mechanisms of action able to reduce brain hyperexcitability; recently considerable interest has been focused on synaptic vesicle protein 2A (SV2A) and its role as a target for AEDs.4 The first drug of this new class approved for epilepsy is levetiracetam (LEV), and from this lead compound, several racetam analogs have been synthesized.5
Based on target-drug program, brivaracetam (BRV) (2S)-2-[(4R)-2-oxo-4-propylpyrro-lidinyl]butanamide, an n-propyl analog of LEV has been identified and has entered clinical trials for PWE;6 it is an SV2A ligand with high selectivity and a 10–30-fold higher potency, depending on the experimental conditions, when compared to LEV.7,8
The purpose of this review is to present updated data available on the pharmacology, efficacy, and tolerability of BRV. We have conducted a systematic search in the PubMed and Cochrane Library databases up to August 14, 2015 summarizing all relevant data for efficacy, safety, and tolerability of BRV in the treatment of partial-onset seizure.
BRV mechanism of action and summary of its efficacy in experimental animal models of epilepsy
BRV has been widely studied in in vivo models of epilepsy. Although the correlation between SV2A binding and anticonvulsant potency in animal models has been previously demonstrated, the role of SV2A in neurotransmission still remains unclear.9 In fact, even if it has been established that SV2A protein is involved in normal synaptic vesicle function, the exact mechanism of synaptic vesicle cycling regulation and neurotransmitter release remains unknown.5,9
Several preclinical studies have demonstrated that BRV is more potent and efficacious than LEV in animal models of both focal and generalized epilepsy.10 In particular, in fully amygdala-kindled rats, BRV induced a significant suppression in motor-seizure severity from a dose of 21.2 mg/kg, whereas LEV caused a similar effect from a dose of 170 mg/kg. BRV also significantly reduced the after-discharge duration at the highest dose tested (212.3 mg/kg), whereas LEV was inactive on this parameter up to 1,700 mg/kg.10 Moreover, BRV protected significantly against both partial and generalized seizures in fully amygdala-kindled mice resistant to phenytoin (effective dose 50 [ED50]: 68.3 mg/kg, intraperitoneal [IP]).10 Recently, it has been demonstrated that BRV has a higher brain permeability than LEV, with consequently more rapid onset of action after acute dosing in audiogenic mice; this fast onset of action might also have a potential clinical relevance for the treatment of status epilepticus or cluster seizures.11
Another study confirmed the protective activity of BRV against kindled seizures with focal seizure threshold and significantly severity significantly modified.12 Furthermore, a recent study, using a rapid kindling model in P14, P21, P28, and P60 rats, has evaluated two doses of BRV 10 and 100 mg/kg, demonstrating that BRV 100 mg/kg significantly increased the after-discharge threshold at all ages, whereas BRV 10 mg/kg increased after-discharge threshold in P60, P28, and P21 rats. BRV also reduced the after-discharge duration, achieving statistical significance with 10 and 100 mg/kg at P60 and with 100 mg/kg, at P21. At P60, BRV increases the number of stimulations required to reach stage 4–5 seizures in a dose-dependent manner. At P28 and P21, BRV increased the number of stimulations required to develop stage 4–5 seizures in a dose-dependent manner, with almost complete elimination of stage 4–5 seizures.13 Moreover, BRV showed a marked synergism with diazepam to reduce seizure duration in self-sustained status epilepticus induced by stimulation of the perforant path.14 A recent study has evaluated the antiseizure and antimyoclonic activities of BRV in comparison to LEV in an animal model of posthypoxic myoclonus, showing higher efficacy of BRV (0.3 mg/kg) than LEV (3 mg/kg) against posthypoxic seizures.15
Furthermore, recent experiments conducted in transgenic mice with Alzheimer’s disease supported an adjunctive and peculiar role of BRV that not only revealed an efficacy against spike-wave discharges similar to ethosuximide, but it showed the ability to reverse memory impairment, thus extending the potential spectrum of action of this new AED.16
In addition to SV2A block, BRV also exhibits inhibitory activity on neuronal voltage-gated sodium channels (VGSC) playing a role as a partial antagonist, as has been reported for other AEDs.17,18 In particular, experimental studies on primary cortical cultures have demonstrated that BRV is able to prolong the sodium channel time recovery from fast inactivation, and this effect could reduce the availability of sodium channel during high-frequency repetitive firing.17,19 Even if this data has been refuted by another recent experimental study that has showed that this VGSC inhibition does not impair sustained repetitive firing in neurons of neuroblastoma cells,20 this is an important aspect, which deserves to be better clarified, since the lack of effect of BRV to reduce neuronal excitability by blocking high repetitive firing in neurons might exclude that the modulation of VGSC contributes to antiseizure effects of BRV.
Pharmacokinetic profile of BRV
BRV presents a favorable pharmacokinetic profile, linear and predictable, with low intersubject variability and almost 100% bioavailability.21–23 The pharmacokinetic properties of BRV have been studied in healthy adult volunteers, in the elderly, in patients with PWE, and in those with hepatic or renal impairment.22–25 The pharmacokinetic differences in elderly subjects compared to healthy volunteers are not so important as to require any dose adjustment.25
Absorption of BRV is unaffected by the presence of food, including high fat meals; after oral administration, BRV is rapidly absorbed by the gastrointestinal tract, and displays linear and dose-proportional profile over the dose range tested.22,26 Its distribution volume is close to total body water (Vz=0.5 L/kg), and it binds weakly to plasma proteins (17.5%). Its terminal half-life is ~9 hours.21 Saliva and plasma BRV levels are highly correlated, BRV crosses the mucosa by passive diffusion, therefore, the saliva concentration of BRV is correlated with plasma concentration. It is possible to speculate that saliva might be a suitable sample for monitoring BRV levels when blood sampling could be a limiting factor.23
BRV is extensively metabolized through several metabolic pathways and is fully excreted by urine (only 8%–11% remains unchanged). BRV is eliminated primarily by metabolism, with the major metabolic pathway involving hydrolysis of the acetamide group resulting in formation of an acid metabolite (BRV-AC; 34.2% of a radiolabeled dose in urine).21 A secondary pathway, mainly mediated by cytochrome P450 (CYP) 2C19,27 forms a hydroxy metabolite (BRV-OH; 15.9% of dose in urine).21 A combination of these two pathways leads to the formation of a hydroxyacid metabolite (15.2% of dose in urine);21,28 only 8.6% of the dose is recovered as the unchanged compound in urine.21 All three metabolites of BRV are pharmacologically inactive (unpublished results)
In an open-label study conducted in patients with liver disease, the plasma half-life of BRV was prolonged up to 17.4 hours in correlation with the severity of hepatic impairment; however, the exposure to BRV is increased by 50%–60% in patients with hepatic impairment, irrespective of severity classified by Child–Pugh score.25,26 These data suggest that the maximum daily dose of BRV might be reduced by one-third in patients with hepatic impairment.25
In severe renal impairment, the exposure to a single oral dose of 200 mg BRV not requiring dialysis (creatinine clearance <15 mL/min), and renal clearance of three metabolites (acid, hydroxy, and hydroxyacid), was decreased 10-fold in patients with severe renal impairment.24 Nevertheless, there are data showing a toxicological coverage for metabolites, without the evidence of any safety issues (UCB data file). Based on these observations, a dose adjustment for BRV should not be required at any stage of renal dysfunction. No data are currently available for pediatric population.
Efficacy of BRV in PWE: effect on partial seizures
The efficacy of BRV as add-on therapy in patients with uncontrolled partial seizures has been assessed in six randomized placebo-controlled clinical trials (Table 1).29
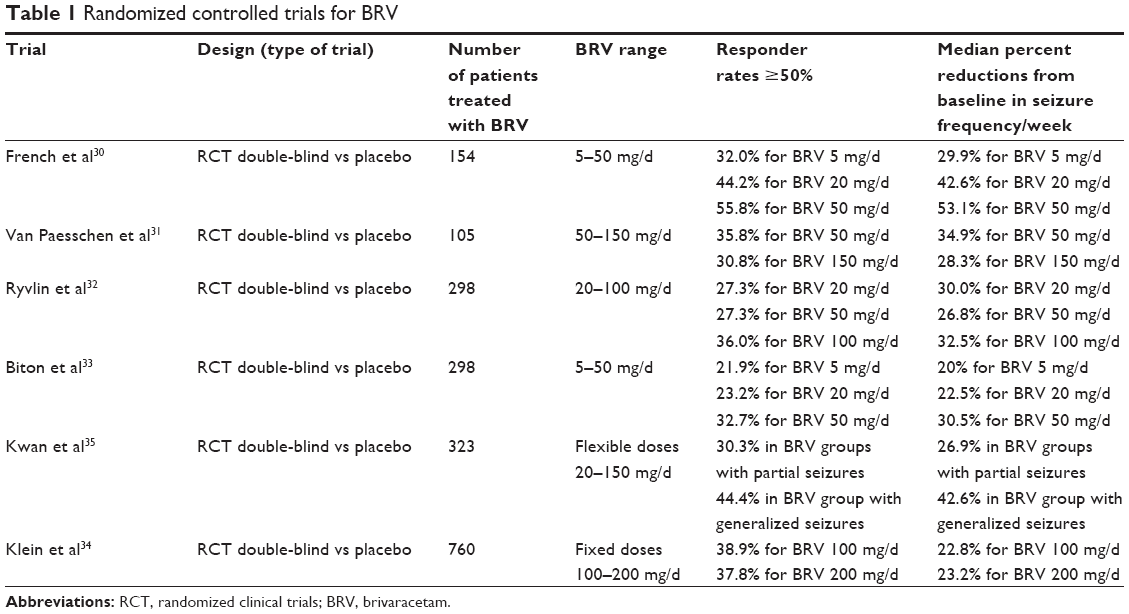 | Table 1 Randomized controlled trials for BRV |
In the first two studies, BRV as adjunctive therapy in adult patients with partial epilepsy and poor control with 1–2 concomitant AEDs, at different doses (5, 20, 50, and 50–150 mg/d) has been evaluated.30,31 French et al30 reported a statistically significant reduction of seizure frequency achieved at the 50 mg/d dose, with high tolerability and infrequent ADRs. In particular, the percentage reduction over placebo in focal seizure frequency/week was directly correlated to BRV dose, respectively 9.8% at 5 mg/d, 14.9% at 20 mg/d, and 22.1% at 50 mg/d, with a median percent reduction from baseline in seizure frequency/week of 21.7% (placebo), 29.9% (BRV5), 42.6% (BRV20), and 53.1% (BRV50); ≥50% responder rates were 16.7% (placebo), 32.0% (BRV5), 44.2% (BRV20), and 55.8% (BRV50); seizure freedom rates during the 7-week treatment period were 1.9% (placebo), 8.0% (BRV5), 7.7% (BRV20), and 7.7% (BRV50). On the other hand, higher doses of BRV would not seem to be more effective, in fact, Van Paesschen et al31 did not find significant differences in seizure frequency reduction between BRV 50 and 150 mg/d during the 7-week maintenance period. In particular, the median seizure frequency/week was 1.00, 1.96, and 1.86 in the group treated with BRV 50 mg/d, BRV 150 mg/d, and placebo, respectively.31 The reduction in baseline-adjusted seizure frequency/week over placebo during the maintenance period was 14.7% in the BRV 50 mg/d group and was 13.6% in the BRV 150 mg/d group; however, a significant difference over placebo was observed on several secondary efficacy outcomes (10 weeks combined up-titration and maintenance period).31 In fact, after the 10-week treatment period, the median seizure frequency/week was 1.10, 2.05, and 1.95 in the BRV 50 mg/d, BRV 150 mg/d, and placebo groups, respectively. In the maintenance period, 50% responder rates were 23.1% for placebo compared with 39.6% for BRV50 and 33.3% for BRV150. During the treatment period, 50% responder rates were 17.3% for placebo compared with 35.8% for BRV50 and 30.8% for BRV150. Nine patients were seizure-free during the 10-week treatment period in the BRV50 group (three in the BRV150 group, only one in the placebo group).
In the study by Ryvlin et al,32 the efficacy and safety/tolerability of BRV (at doses of 20, 50, and 100 mg/d) in patients with uncontrolled partial seizures with/without secondary generalization, despite treatment with one or two concomitant AEDs, was investigated. The percent reduction over placebo in baseline-adjusted seizure frequency/week was 6.8%, 6.5%, and 11.7% in the BRV 20, 50, and 100 mg/d groups, respectively. The percent reduction over placebo in baseline-adjusted seizure frequency/28 days was 9.2% and 20.5% in the BRV 50 and 100 mg/d groups, respectively. Median percent reductions from baseline were 30.0% for BRV 20 mg/d, 26.8% for BRV 50 mg/d, and 32.5% for BRV 100 mg/d in comparison to 17.0% for placebo. Responder rates (≥50%) were 27.3%, 27.3%, and 36.0% for BRV 20, 50, and 100 mg/d, respectively, in comparison to 20.0% for placebo. Based on these results, only BRV 100 mg/d was able to significantly reduce seizure frequency/week over placebo.
Biton et al33 confirmed that BRV efficacy might be dose-related. Indeed, in their randomized placebo-controlled trial, adjunctive BRV at a daily dose of 50 mg significantly decreased seizure frequency, while lower dosages (5 and 20 mg/d) did not achieve significant differences.33 In more detail, the percent reduction in partial-onset seizure frequency/week in comparison to placebo was −0.9% (P=0.885) for BRV 5 mg/d, 4.1% (P=0.492) for BRV 20 mg/d, and 12.8% (P=0.025) for BRV 50 mg/d; in the BRV 50 mg/d group, statistical significance was also observed for the ≥50% responder rate (BRV 32.7% vs placebo 16.7%) and median percent reduction from baseline in focal seizure frequency/week (BRV 30.5% vs placebo 17.8%).
Recently a randomized, multicenter, double-blind Phase III trial was conducted by Klein et al34 to evaluate the efficacy and the safety profile of BRV at fixed doses of 100–200 mg/d in adult patients with refractory partial onset seizures. Responder rate was 21.6% for placebo group, 38.9% for BRV 100 mg/d, and 37.8% for BRV 200 mg/d; the percent reduction of partial onset seizures in 28-day frequency was 22.8% for BRV 100 mg and 23.2% for BRV 200 mg.
Interestingly, BRV has been shown to be effective in generalized seizures as well. Kwan et al35 conducted a double-blind, randomized, placebo-controlled trial investigating the safety and tolerability profile of adjunctive BRV (at individualized tailored doses ranging from 20 to 150 mg/d) in patients with partial or generalized refractory epilepsies. The percent of reduction of focal seizure frequency/week in the BRV group in comparison to placebo was 7.3%, while only in the generalized seizures group, the number of seizure days/week decreased from 1.42 at baseline to 0.63 during the treatment period in BRV-treated patients (n=36), and from 1.47 at baseline to 1.26 during the treatment period in the placebo group (n=13).35 The median percent reduction in baseline-adjusted seizure frequency/week was 26.9% BRV vs 18.9% placebo, and the ≥50% responder rate was 30.3% BRV vs 16.7% placebo. The median percent reduction from baseline in generalized seizure days/week was 42.6% vs 20.7%, and the ≥50% responder rate was 44.4% vs 15.4% in BRV-treated and placebo-treated patients, respectively.
Similar to LEV, BRV might become a useful AED for the treatment of myoclonic seizures occurring in the setting of idiopathic generalized epilepsies (eg, Juvenile Myoclonic Epilepsy)36 or of progressive myoclonic epilepsies.37 Two randomized, placebo-controlled trials evaluating efficacy and safety of adjunctive BRV (5–150 mg/d) in Unverricht–Lundborg Disease, the most common and less severe form of progressive myoclonic epilepsies,38 failed to show a significant improvement of myoclonus in these patients.39 However, sample size was small (106 patients randomized in the two trials), and the patients were allowed to receive LEV.39 Moreover, it is well known that myoclonus may present high inter- and intrapatients variability (with patients experiencing “good days” and “bad days”) in Unverricht–Lundborg disease. Hence, further studies evaluating BRV in epilepsies with myoclonic seizures are warranted.
Currently an open-label, multicenter, follow-up study to evaluate the long-term safety and efficacy of BRV is ongoing (BRITE study-NCT01339559).
Finally, to date, in all studies performed, BRV was evaluated as an oral tablet formulation, and no data are available about intravenous infusion since the study NCT02088957, aiming at a comparison of the efficacy and safety of intravenous BRV vs phenytoin in adult subjects with nonconvulsive electrographic seizures, was terminated for low enrollment.
Safety profile of BRV
The most commonly reported adverse effects with BRV in adults were primarily related to the central nervous system and included somnolence, fatigue, and dizziness.22 These adverse effects were mild to moderate, and the tolerability profile is so excellent that it did not impair therapeutic compliance. In fact, the daily dose of BRV (20–150 mg) was well tolerated and associated with 6.1% of discontinuation rates due to ADRs compared to 5.0% of the placebo group.35 Furthermore, ADRs induced by BRV seem to be time-related, disappearing during the course of treatment.
The entity of sedative effects of BRV measured by psychometric tests is dose-related in healthy men and appeared clearly from 600 mg upwards as a decrease in attention, motor control, and alertness.22 Moreover, the type and the severity of ADRs are not influenced by food.22
As demonstrated in healthy males, a twice-daily dosing regimen could be a good clinical practice to reduce blood fluctuations and peak, which might influence the appearance of adverse events.22 No effects on cardiac function were reported even at very high daily dosages (up to 800 mg/d).40
No data about fertility and/or potential teratogenic effect of BRV in humans are currently available; however, no adverse effects were detected up to the highest tested oral dose of 400 mg/kg/d on fertility, and no effects on pregnancy or fetal development at 600 mg/d were observed in animals.26 Seizure aggravation or the appearance of new generalized seizures was rare: three studies reported this adverse event, occurring in similar proportions between placebo and treated group (4.3% vs 5.2%, P=0.67).32,33,35
In the above-reported five randomized clinical trials, 1,639 subjects were included in an intention-to-treat analysis (1,214 treated with BRV and 425 with placebo).30–35 No differences were observed in the proportion of subjects experiencing at least one adverse event (65.5% with BRV vs 60.5% with placebo, P=0.10). Most events were mild to moderate; actually, comprehensive withdrawal rate due to adverse events was quite low and similar in BRV and placebo arms (5.4% with BRV vs 4.2% with placebo, P=0.37). Serious adverse events were quite rare and equally distributed (2.9% with BRV vs 4.4% with placebo, P=0.16). Adverse events that were observed in at least 5% of subjects in either group are listed in Table 2. The proportion of patients reporting fatigue and somnolence was significantly higher in BRV group compared to placebo (Table 2). Irritability was reported in three studies only, and it was present in a small proportion of subjects (3% receiving BRV, 1% receiving placebo, P=0.36).
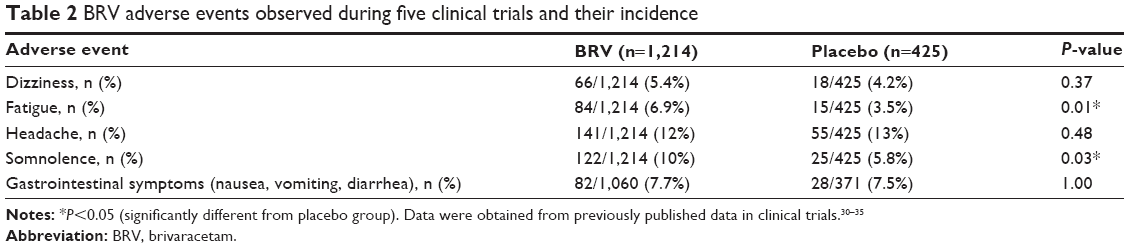 | Table 2 BRV adverse events observed during five clinical trials and their incidence |
Known drug–drug interactions
Because of its advantageous pharmacokinetic profile, BRV treatment does not appear to influence plasma concentrations of other AEDs such as carbamazepine, lamotrigine, LEV, oxcarbazepine, topiramate, or valproic acid.41 However, carbamazepine plasma levels are slightly reduced by coadministration of BRV (400 mg/d), while levels of carbamazepine-epoxide are increased in a dose-dependent manner.26,42 This increase of plasma concentration of carbamazepine-epoxide is the result of inhibition by BRV of epoxide hydrolase that metabolizes carbamazepine-epoxide into carbamazepine-diol.42
High doses of BRV (400 mg/d) cause a moderate decrease of ethinylestradiol and levonorgestrel plasma levels (components of oral contraceptives) but this posological range has no impact on ovulation. No effect on contraceptive disposition is reported at therapeutic doses of BRV 100 mg/d.39 Interestingly, there is a possible negative interaction between BRV and LEV, in fact, the concomitant use of both drugs may reduce BRV efficacy; however, this evidence is not robust because the number of patients with concomitant LEV was very small, other studies may be useful to assess this apparent pharmacodynamic interaction.33
Conclusion
BRV is a novel AED whose efficacy in partial epilepsies has been studied and established in five randomized controlled trials;30–35 furthermore, two recent meta-analyses have confirmed significant effects for BRV in patients with refractory partial seizures.29,43
Considering that BRV shares part of its mechanism of action with LEV and that its ability to inhibit VGSC (still debated) is in common with several other AEDs, it will be very intriguing to see how this drug will behave in real-life clinical practice. Accordingly, it could be hypothesized that BRV might possess at least the same effectiveness as LEV. Based on this hypothesis, BRV may be reasonably considered as a valuable add-on AED in patients with partial seizures, also considering its suggested good tolerability. However, specific studies are needed to confirm its efficacy in specific epileptic syndromes, for example, a decreased expression of SV2A in the hippocampus of patients with temporal lobe epilepsy with hippocampal sclerosis has been documented and might represent a pharmacoresistance mechanism in some cases; however, LEV has been reported to be effective.44,45 In addition, because of its good safety and pharmacokinetic profile, BRV might be ideal for use in monotherapy, as previously demonstrated for LEV.46
Finally, few studies have been performed, and more randomized double-blind studies are needed to confirm these considerations and to demonstrate if BRV might really confirm its promises and become a new tool for epileptologists.
Disclosure
Angelo Labate received speaker fees from UCB; Emilio Russo received speaker fees from Almirall, Eisai, and Lundbeck; Antonio Gambardella received speaker fees from UCB, Eisai, and Novartis; and Edoardo Ferlazzo received speaker fees from UCB. The authors report no other conflicts of interest in this work.
References
Berg AT. Identification of pharmacoresistant epilepsy. Neurol Clin. 2009;27(4):1003–1013. | ||
Perucca P, Gilliam FG. Adverse effects of antiepileptic drugs. Lancet Neurol. 2012;11(9):792–802. | ||
Leporini C, De Sarro G, Russo E. Adherence to therapy and adverse drug reactions: is there a link? Expert Opin Drug Saf. 2014;13 Suppl 1:S41–S55. | ||
Lyseng-Williamson KA. Levetiracetam: a review of its use in epilepsy. Drugs. 2011;71(4):489–514. | ||
Mendoza-Torreblanca JG, Vanoye-Carlo A, Phillips-Farfan BV, Carmona-Aparicio L, Gomez-Lira G. Synaptic vesicle protein 2A: basic facts and role in synaptic function. Eur J Neurosci. 2013;38(11):3529–3539. | ||
Kenda BM, Matagne AC, Talaga PE, et al. Discovery of 4-substituted pyrrolidone butanamides as new agents with significant antiepileptic activity. J Med Chem. 2004;47(3):530–549. | ||
Lynch BA, Lambeng N, Nocka K, et al. The synaptic vesicle protein SV2A is the binding site for the antiepileptic drug levetiracetam. Proc Natl Acad Sci U S A. 2004;101(26):9861–9866. | ||
Gillard M, Fuks B, Leclercq K, Matagne A. Binding characteristics of brivaracetam, a selective, high affinity SV2A ligand in rat, mouse and human brain: relationship to anti-convulsant properties. Eur J Pharmacol. 2011;664(1–3):36–44. | ||
Kaminski RM, Matagne A, Leclercq K, et al. SV2A protein is a broad-spectrum anticonvulsant target: functional correlation between protein binding and seizure protection in models of both partial and generalized epilepsy. Neuropharmacology. 2008;54(4):715–720. | ||
Matagne A, Margineanu DG, Kenda B, Michel P, Klitgaard H. Anti-convulsive and anti-epileptic properties of brivaracetam (ucb 34714), a high-affinity ligand for the synaptic vesicle protein, SV2A. Br J Pharmacol. 2008;154(8):1662–1671. | ||
Bialer M, Johannessen SI, Levy RH, Perucca E, Tomson T, White HS. Progress report on new antiepileptic drugs: a summary of the Twelfth Eilat Conference (EILAT XII). Epilepsy Res. 2015;111:85–141. | ||
Detrait ER, Leclercq K, Loscher W, et al. Brivaracetam does not alter spatial learning and memory in both normal and amygdala-kindled rats. Epilepsy Res. 2010;91(1):74–83. | ||
Dupuis N, Matagne A, Staelens L, et al. Anti-ictogenic and antiepileptogenic properties of brivaracetam in mature and immature rats. Epilepsia. 2015;56(5):800–805. | ||
Wasterlain CG, Baldwin R, Naylor DE, Thompson KW, Suchomelova L, Niquet J. Rational polytherapy in the treatment of acute seizures and status epilepticus. Epilepsia. 2011;52 Suppl 8:70–71. | ||
Tai KK, Truong DD. Brivaracetam is superior to levetiracetam in a rat model of post-hypoxic myoclonus. J Neural Transm. 2007;114(12):1547–1551. | ||
Nygaard HB, Kaufman AC, Sekine-Konno T, et al. Brivaracetam, but not ethosuximide, reverses memory impairments in an Alzheimer’s disease mouse model. Alzheimers Res Ther. 2015;7(1):25. | ||
Zona C, Pieri M, Carunchio I, Curcio L, Klitgaard H, Margineanu DG. Brivaracetam (ucb 34714) inhibits Na(+) current in rat cortical neurons in culture. Epilepsy Res. 2010;88(1):46–54. | ||
Kohling R. Voltage-gated sodium channels in epilepsy. Epilepsia. 2002;43(11):1278–1295. | ||
Rogawski MA, Loscher W. The neurobiology of antiepileptic drugs. Nat Rev Neurosci. 2004;5(7):553–564. | ||
Niespodziany I, Andre VM, Leclere N, Hanon E, Ghisdal P, Wolff C. Brivaracetam differentially affects voltage-gated sodium currents without impairing sustained repetitive firing in neurons. CNS Neurosci Ther. 2015;21(3):241–251. | ||
Sargentini-Maier ML, Espie P, Coquette A, Stockis A. Pharmacokinetics and metabolism of 14C-brivaracetam, a novel SV2A ligand, in healthy subjects. Drug Metab Dispos. 2008;36(1):36–45. | ||
Sargentini-Maier ML, Rolan P, Connell J, et al. The pharmacokinetics, CNS pharmacodynamics and adverse event profile of brivaracetam after single increasing oral doses in healthy males. Br J Clin Pharmacol. 2007;63(6):680–688. | ||
Rolan P, Sargentini-Maier ML, Pigeolet E, Stockis A. The pharmacokinetics, CNS pharmacodynamics and adverse event profile of brivaracetam after multiple increasing oral doses in healthy men. Br J Clin Pharmacol. 2008;66(1):71–75. | ||
Sargentini-Maier ML, Sokalski A, Boulanger P, Jacobs T, Stockis A. Brivaracetam disposition in renal impairment. J Clin Pharmacol. 2012;52(12):1927–1933. | ||
Stockis A, Sargentini-Maier ML, Horsmans Y. Brivaracetam disposition in mild to severe hepatic impairment. J Clin Pharmacol. 2013; 53(6):633–641. | ||
von Rosenstiel P. Brivaracetam (UCB 34714). Neurotherapeutics. 2007;4(1):84–87. | ||
Stockis A, Watanabe S, Rouits E, Matsuguma K, Irie S. Brivaracetam single and multiple rising oral dose study in healthy Japanese participants: influence of CYP2C19 genotype. Drug Metab Pharmacokinet. 2014;29(5):394–399. | ||
Nicolas JM, Chanteux H, Rosa M, Watanabe S, Stockis A. Effect of gemfibrozil on the metabolism of brivaracetam in vitro and in human subjects. Drug Metab Dispos. 2012;40(8):1466–1472. | ||
Tian X, Yuan M, Zhou Q, Wang X. The efficacy and safety of brivaracetam at different doses for partial-onset epilepsy: a meta-analysis of placebo-controlled studies. Expert Opin Pharmacother. 2015;16(12):1755–1767. | ||
French JA, Costantini C, Brodsky A, von Rosenstiel P, Group NS. Adjunctive brivaracetam for refractory partial-onset seizures: a randomized, controlled trial. Neurology. 2010;75(6):519–525. | ||
Van Paesschen W, Hirsch E, Johnson M, Falter U, von Rosenstiel P. Efficacy and tolerability of adjunctive brivaracetam in adults with uncontrolled partial-onset seizures: a phase IIb, randomized, controlled trial. Epilepsia. 2013;54(1):89–97. | ||
Ryvlin P, Werhahn KJ, Blaszczyk B, Johnson ME, Lu S. Adjunctive brivaracetam in adults with uncontrolled focal epilepsy: results from a double-blind, randomized, placebo-controlled trial. Epilepsia. 2014;55(1):47–56. | ||
Biton V, Berkovic SF, Abou-Khalil B, Sperling MR, Johnson ME, Lu S. Brivaracetam as adjunctive treatment for uncontrolled partial epilepsy in adults: a phase III randomized, double-blind, placebo-controlled trial. Epilepsia. 2014;55(1):57–66. | ||
Klein P, Schiemann J, Sperling M, et al. A randomized, double-blind, placebo-controlled, multicenter, parallel-group study to evaluate the efficacy and safety of adjunctive brivaracetam in adult patients with partial-onset seizures (S31.009). Neurology. Available from: https://www.aan.com/uploadedFiles/Website_Library_Assets/Documents/7.Conferences/1.CONFERENCES/1.Annual_Meeting/15AM%20AbstractListing.pdf. Accessed October 12, 2015. | ||
Kwan P, Trinka E, Van Paesschen W, Rektor I, Johnson ME, Lu S. Adjunctive brivaracetam for uncontrolled focal and generalized epilepsies: results of a phase III, double-blind, randomized, placebo-controlled, flexible-dose trial. Epilepsia. 2014;55(1):38–46. | ||
Crespel A, Gelisse P, Reed RC, et al. Management of juvenile myoclonic epilepsy. Epilepsy Behav. 2013;28 Suppl 1:S81–S86. | ||
Magaudda A, Ferlazzo E, Nguyen VH, Genton P. Unverricht-Lundborg disease, a condition with self-limited progression: long-term follow-up of 20 patients. Epilepsia. 2006;47(5):860–866. | ||
Franceschetti S, Michelucci R, Canafoglia L, et al. Progressive myoclonic epilepsies: definitive and still undetermined causes. Neurology. 2014;82(5):405–411. | ||
Stockis A, Watanabe S, Fauchoux N. Interaction between brivaracetam (100 mg/day) and a combination oral contraceptive: a randomized, double-blind, placebo-controlled study. Epilepsia. 2014;55(3):e27–e31. | ||
Rosillon D, Astruc B, Hulhoven R, et al. Effect of brivaracetam on cardiac repolarisation – a thorough QT study. Curr Med Res Opin. 2008;24(8):2327–2337. | ||
Bialer M, Johannessen SI, Levy RH, Perucca E, Tomson T, White HS. Progress report on new antiepileptic drugs: a summary of the Ninth Eilat Conference (EILAT IX). Epilepsy Res. 2009;83(1):1–43. | ||
Stockis A, Chanteux H, Rosa M, Rolan P. Brivaracetam and carbamazepine interaction in healthy subjects and in vitro. Epilepsy Res. 2015;113:19–27. | ||
Ma J, Huang S, You C. Adjunctive brivaracetam for patients with refractory partial seizures: a meta-analysis of randomized placebo-controlled trials. Epilepsy Res. 2015;114:59–65. | ||
Mula M, Sander JW, Trimble MR. The role of hippocampal sclerosis in antiepileptic drug-related depression in patients with epilepsy: a study on levetiracetam. Seizure. 2006;15(6):405–408. | ||
van Vliet EA, Aronica E, Redeker S, Boer K, Gorter JA. Decreased expression of synaptic vesicle protein 2A, the binding site for levetiracetam, during epileptogenesis and chronic epilepsy. Epilepsia. 2009;50(3):422–433. | ||
Gambardella A, Labate A, Colosimo E, Ambrosio R, Quattrone A. Monotherapy for partial epilepsy: focus on levetiracetam. Neuropsychiatr Dis Treat. 2008;4(1):33–38. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.