")
Back to Journals » Breast Cancer: Targets and Therapy » Volume 13
Breast Cancer Adjuvant Radiotherapy in BRCA1/2, TP53, ATM Genes Mutations: Are There Solved Issues?
Authors Lazzari G , Buono G, Zannino B, Silvano G
Received 13 February 2021
Accepted for publication 21 April 2021
Published 12 May 2021 Volume 2021:13 Pages 299—310
DOI https://doi.org/10.2147/BCTT.S306075
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Pranela Rameshwar
Grazia Lazzari,1 Giuseppe Buono,2 Benedetto Zannino,2 Giovanni Silvano1
1Radiation Oncology Unit, San Giuseppe Moscati Hospital, Taranto, 74100, Italy; 2Medical Oncology Unit, San Rocco Hospital, Sessa Aurunca, Caserta, 81037, Italy
Correspondence: Grazia Lazzari
Radiation Oncology Unit, San Giuseppe Moscati Hospital, Taranto, 74100, Italy
Email [email protected]
Abstract: BRCA1, BRCA2, TP53 and ATM gene mutations are the most studied tumour suppressor genes (TSGs) influencing the loco-regional approach to breast cancer (BC). Due to altered radio sensitivity of mutated cancer cells, mastectomy has always been advised in most patients with BC linked to TSGs mutations in order to avoid or minimize the use of adjuvant radiotherapy (ART). Whether ART is safe or not in these carriers is still debated. As a result, this issue has been widely discussed in the recent ASTRO and ASCO papers, yielding important and useful recommendations on the use of ART according to the mutational status. In this review, we have highlighted the impact of these mutations on local control, toxicities, second tumors, and contralateral breast cancers (CBCs) after ART to solve remaining doubts and encourage the safe use of ART when indicated.
Keywords: radiation, radiosensitivity, tumor suppressor genes
Introduction
The genetic basis of breast cancer (BC) is linked to several high- and/or moderate-penetrance mutations in BC susceptibility genes.1 Among them, mutations in the BRCA1, BRCA2, TP53 and ATM genes are the most studied tumour suppressor genes (TSGs) influencing the therapeutic approach to BC.2 In fact, with the widespread use of genomics, information on the pathogenic variants of these BC susceptibility genes has been integrated into local treatment and decision-making process for carriers patients with operable BC. The mutational status in these TSGs has implications for the use of ART due to their involvement in the DNA damage repair mechanisms. An impaired radiation response has been observed in vitro and evocated in vivo for patients with BC carrying these TSGs mutations, leading to limitations of ART, regardless of the clinical indications. Thus, mastectomy is the preferred choice.
Although guidelines for ART in mutation carrier patients with BC are lacking, several efforts have recently been made to solve this issue. In fact, an ASTRO review and the ASCO paper have highlighted several useful recommendations.3,4 Based on the above advice and literature certainties, we have focused this review on the impact of ART on TSGs mutations in breast cancer in terms of local control, acute toxicities, second tumours, and contralateral breast cancers (CBCs) in order to achieve a quick reference guidance in the context of a multidisciplinary team approach.
Tumour Suppressor Genes Mutations and Related Breast Cancer
BRCA1, BRCA2, TP53, and ATM are tumour suppressor genes (TSGs) that have attracted growing interest in the oncological field in light of the high incidence of their mutations in younger BC populations with a family history and an aggressive phenotype. Mastectomy instead of breast conserving therapy (BCT) including ART is the preferred approach in these carriers. Knowledge of the relation between BC mutational status and ART is crucial in therapeutic approaches, especially when ART is indicated. A multidisciplinary team sharing and genetic counselling is mandatory.
BC Features Related to BRCA 1/2 Mutations
Breast cancer (BRCA) 1 is located on chromosome 17q21, while BRCA2 is mapped to chromosome 13q12.3.5 Germline mutations in BRCA1 or BRCA2 are found in 3% to 4% of all women with BC.6,7 The lifetime risk of BC among BRCA mutation carriers is approximately 70%, within a range of 50% to 90% depending on the studied population, genetic tests and methods of analysis. These mutations, when associated with the autosomal dominant pathway, cause hereditary breast and ovarian cancer (HBOC) syndrome.8,9 Mutations in the BRCA1 gene are mainly associated with the development of high-grade and “triple-negative” BC,10 while BRCA2 seems to usually correlate with higher-grade BC compared to sporadic BC.11 BRCA gene mutations predispose patients to a younger age of BC development with a worse prognosis than sporadic BC in terms of overall survival (OS) and BC-specific survival, as confirmed by a meta-analysis by Beretta et al.12,13 Furthermore, as found in the POSH study, although patients with young-onset BC who carry a BRCA mutation show similar survival to noncarriers at any time point (2-5-10 years), in patients with BRCA mutation triple-negative BC, the survival advantage seems to be only during the first few years after diagnosis when compared with noncarriers. These data could be taken into account in the timing of prophylactic surgery planning.14
BC Features Related to TP53 Mutations
The tumour protein 53 (TP53) gene is a TSG that has been called the guardian of the genome. It is located on chromosome 17p13.1, encoding the cellular tumour antigen p53, a nuclear phosphoprotein directly involved in the regulation of cell cycle checkpoints, DNA repair and apoptosis in response to several damaging factors, such as ionizing radiation (IR).15 Germline TP53 mutations are associated with Li–Fraumeni syndrome, first described in 1969 by Li and Fraumeni, who reported a high incidence of soft tissue sarcomas and BC in young women belonging to four families.16 Regarding penetrance, the cumulative incidence of TP53-mutated BC has been estimated at 60 years in 85% of cases in the National Cancer Institute Li–Fraumeni Syndrome cohort,17 but a median onset age of nearly 34 years has been defined,18 with approximately 5–8% of TP53-mutated cases with BC diagnosed under 30 years, as reported by McCuaig et al.19 The absence of a family history in carriers of TP53 mutations is a typical feature.20 Mutations in TP53 correlate with a more aggressive tumour phenotype, characterized by genomic instability, a high mitotic index, high Ki-67 and cyclin E expression.21 Moreover, a high tumour burden, poor differentiation grade, lymph node metastases, negative hormone receptor status and cerbB2 hyperexpression have been noted.22 More than 50 of the changes affecting the TP53 gene are missense mutations followed by nonsense mutations (approximately 10%). However, single nucleotide polymorphisms (SNPs) are also associated with altered p53 function and with an increased cancer risk, rapid progression or an altered response to treatments. Currently, up to 80 SNPs have been identified, with most of them (90%) situated in introns, outside splicing sites, or in noncoding exons.23 Regardless of the kind of mutation, studies have demonstrated that the majority of somatic TP53 mutations in BC have important prognostic significance.24 In this regard, in a cohort study by Overgaard J on 294 patients with BC, TP53 mutation was associated with a significantly poorer outcome with univariate odds ratios for local failure of 2.04 (1.43–2.91, 95% confidence limit), distant metastasis of 3.56 (2.65–4.77), any failure or death (disease-free survival) 2.51 (1.89–3.32) and death 3.99 (2.97–5.37). Patients with TP53 mutations had an overall survival (OS) probability of 52% at 5 years compared with 82% in wild-type (WT) carriers (p < 0.0001). A similar pattern was observed in disease-free survival as the endpoint (69% in WT vs 47% no WT, p < 0.0003). Moreover, TP53 mutation was found in an independent prognostic marker of poor outcome regardless the nodal status. In node negative, patients’ OS was 89% in WT vs 64% in TP53 mutations carriers (p = 0.0002); in node positive, patients’ OS was 72% in WT vs 44% TP53 mutation carriers (p= 0.003).25
BC Features Related to ATM Mutations
The ATM gene is located on chromosome 11q22-23 and consists of a large genome spanning 150 kb encoding a ubiquitously expressed transcript named the ATM protein. This protein is involved in the recognition and repair of DNA double-strand breaks (DSBs) induced by IR, antineoplastic drugs, or oxidative stress.26 ATM gene mutations predispose patients to a rare autosomal recessive disorder named ataxia-telangiectasia (AT) and its variants.27 This is an autosomal recessive disorder characterized by cerebellar ataxia, oculomotor apraxia, immunodeficiency, choreoathetosis, conjunctival telangiectasias, sensitivity to radiotherapy, and an increased risk of malignancy. While AT syndrome is extremely rare (1 in 40,000–100,000 people worldwide), germline ATM heterozygosity occurs in approximately 1% of the population and has been associated with an increased cancer susceptibility.28 In fact, heterozygous carriers have an approximately twofold higher risk of developing BC than the general population, as described in a UK cohort study, showing a 4.94 relative risk amongst women under 50 years of age vs 2.23 in the general population.29 In another study on patients with familial BC, a 2.37 relative risk of BC development was shown among ATM heterozygotes mutation occurring in any functional domain of the ATM gene.30,31 Thus, ATM mutations involved in BC are classified into three main categories: 1) truncating mutations associated with no protein production; 2) mutations leading to the expression of a mutant protein lacking kinase activity; and 3) missense mutations associated with reduced kinase activity.32 In addition, several variants, so-called variants of uncertain significance (VUS), have also been identified, showing an undefined functional effect or no detrimental outcome after treatment with radiotherapy.33
TSGs Mutations and Radio Sensitivity Matter
All of these genes are involved in the DNA damage repair machinery after IR, impacting cell cycle recruitment, proliferation and apoptosis in various ways through impaired DNA DSBs repair pathways and, consequently, altered radiosensitivity, which is still a debated matter.
Radiosensitivity in BC Related to BRCA1/2 Mutations
Myths from retrospective data with a limited follow-up regarding local outcome assessment supported by the theory of genome instability have generated conflicting results and doubts about the efficacy of ART in patients with BC carrying BRCA1/2 mutations. It is well acknowledged that BRCA1 plays a key role in DNA DSBs repair pathways in the late S and G2 phases of the cell cycle, allowing the cell to repair DNA damage before proceeding to the next phase of the cell cycle.34 The functions of BRCA2 are largely limited to DSBs repair by promoting the mechanism of homologous recombination.35 Both together correlate with increased sensitivity of tumour cells to several antineoplastic drugs and to IR as reported by preclinical models and retrospective studies.36,37 Irradiated lymphoblastoid cell lines heterozygous for BRCA1/2 mutations showed a significantly higher number of chromatid breaks per cell than control cells, while irradiated BRCA1−/− MEFs were found to be highly sensitive to IR, as were HCC1937 human cancer cells with truncated BRCA1 expression.38–40 Most likely, BRCA 1 and 2 mutated cells show different radiosensitivity, as investigated by Baert et al, in two different studies, but no confirmations have been achieved in clinical reports.41,42 From a clinical point of view, this theoretically altered radiosensitivity seems to be quite different. In fact, Robson et al, in a descriptive analysis of 496 Ashkenazi BRCA1/2-mutated patients with BC managed with BCT, demonstrated no difference in terms of the local relapse rate when compared with non-BRCA-mutated patients (12% vs 8%, p = 0.68) at a median follow-up time of 9.7 years.43 Additionally, the retrospective study of Pierce et al showed no diversity in OS, local recurrence or cancer-specific survival between BRCA1/2 mutated vs nonmutated patients with stage I/II BC treated with surgery followed by ART at a median follow-up time of 5.3 years.44 Brekelmans et al, in subgroups of patients who underwent BCT, endocrine therapy and chemotherapy, regardless of their mutation status, demonstrated no difference in the 10-year local relapse rate among BRCA1-2-mutated and BRCA WT patients with BC treated with radiotherapy and chemotherapy (16%, 17%, and 21%, p = 0.6, respectively).45 Similarly, Kyrova et al found no significant differences in the recurrence rate (p=0.47) among patients with BC treated with surgery followed by ART carrying or not carrying BRCA1/2 mutations.46 A recent meta-analysis by Valachis et al reported no significant difference in terms of the local recurrence rate among BRCA-mutated vs WT patients with BC (p= 0.07). However, when the analysis was restricted to only the few studies with a follow-up time of at least 7 years (1634 patients), these differences reached statistical significance (23.7 vs 15.9%, p < 0.003).47 As concluded by Vallard et al, from a radiation oncologist’s point of view, there is no radiosensitivity difference sufficient to discourage the use of ART in patients with BC carrying BRCA1/2 mutations, although long-term data are needed.48
Radiosensitivity in BC Related to TP53 Mutations
Mutations in the TP53 gene lead to the production of a nonfunctional protein that is not capable of effectively binding DNA, thus resulting in the failure of DNA repair mechanisms and, subsequently, in abnormal proliferation of these mutated cells.15 The role of p53 in the radiosensitivity of human tumour cells has been assessed, identifying a loss of p53 function as a major cause of increased resistance to IR in murine cells.49 As confirmed by the in vitro models of Mcllwrath et al, a significant correlation between the level of IR-induced G1 arrest and radiosensitivity has been observed. These results support the theory that WT p53 function is required for the sensitivity of tumour cells to DNA-damaging agents, such as IR, and that the loss of p53 function in certain human tumour cells can lead to resistance to IR.50 In carefully controlled radiotherapy studies, the presence of mutant p53, regardless of the missense and nonmissense mutational condition, has been associated with decreased local control following radiotherapy and a worse prognosis.25,51,52 Nowadays, the current literature agrees with the theory of minimizing radiation exposure and avoiding high-dose schedules and re-irradiation in patients carrying TP53 mutations.53 In a study conducted by Kappel et al, a high rate of recurrence and a very low overall survival after intensive chemotherapy and radiotherapy protocols were observed in patients belonging to an Austrian family whose seven members were treated with chemo- and radiotherapy due to cancers that occurred at predominantly young ages, including eight breast cancers in six of them.54 All of these family members were screened for p53 mutations, and a rare missense mutation involving exon 10 of the TP53 gene was found.
Radiosensitivity in BC Related to ATM Mutations
ATM gene mutations show a wide spectrum of effects on radiosensitivity in vitro and in vivo. ATM-deficient cells show a loss in activating the G1–S, S, and G2–M cell cycle checkpoints after exposure to DNA damage; moreover, they develop a defect in stress response pathways, appearing to be more resistant to IR-induced apoptosis.55 Based on experiments in mice and cell culture of dermal fibroblasts, increased radiosensitivity in mutation carrier cells has been recorded linked to a downregulation of ATM protein levels, as also observed in a published case report.56–58 In vivo studies suggest a wide response spectrum in favour of the effectiveness of radiation in patients with BC carriers of a pathogenic ATM variant due to their deficiency in DNA mismatch repair mechanisms. In fact, the study by Su et al found a low rate of local failure in ATM single variant carrier BC patients treated with ART.59 At a median of 72-month follow-up time, recurrences were observed in 7% of women treated with radiation, in contrast to 48% of women not treated with ART. In the study by Meyer et al on a cohort of 138 patients with BC who received ART following BCS with 20 patient carriers of important sequence variants in the ATM gene, no difference was found in the actuarial 7-year local relapse-free survival of carriers vs noncarriers (88 vs 94% P=0.34).60 In the study of Bremer et al, among patients with BC carriers of a truncating ATM mutation with a splicing mutation 1066-6T-G who received at least one course of RT, at a median follow-up of 5.1 years (range 1.7–7.2) after completion of radiotherapy, none had relapsed.28 Local relapse occurred in a single patient who had declined ART following breast conservation surgery. In the case of ATM gene mutations classified as VUS, their functional effect on radiosensitivity seems to be irrelevant, as reported by Mullins et al. In this study, five patients with breast cancer and varying germline heterozygous ATM mutations, after RT, remained recurrence-free with a median duration of 18 months.33 Thus, as reported in a review by Jerzak et al, a well-defined ATM carrier status should be an asset in the therapeutic decision for ART indication.61
TSGs Mutations and ART Related Toxicity
Radiotherapy-induced acute and late toxicities are considered not only a consequence of irradiation techniques but also of patient-related factors, such as age and altered genetic background as occurs in BC related to TSGs mutations leading to several uncertainties on ART benefit.
ART Toxicity in BC Related to BRCA Mutations
In theory, BRCA-mutated tumours might be more sensitive to RT-induced effects due to their inability to repair DNA damage. However, BRCA1/2-mutated patients with BC are usually heterozygous, carrying a single mutated allele; therefore, the cells still possess a functional allele capable of partially maintaining a DNA repair capability.34 The condition of haploinsufficiency could explain the normal rate of acute and late toxicity after breast ART in patients with BC carrying a BRCA1/2-mutation, as recorded by several retrospective studies. In a study by Pierce et al, with a median follow-up of 5.3 years, no difference in late normal tissue toxicities was found in irradiated patients with BC and mutation carriers.44 Shanley et al found a trend toward an increased recall of acute pain in BRCA-mutated vs nonmutated patients with BC, although this event was not associated with an increase in inflammation signs or cosmesis outcomes.62 Furthermore, ethnicity does not seem to influence toxicity in BRCA mutations, as demonstrated by Park et al in a Korean study on 213 patients with BC undergoing ART, 20% of whom had BRCA1 and/or BRCA2 mutations. Although 27% of BRCA-mutated patients with BC developed RTOG grade 2 or higher skin toxicity, in multivariate analysis, BRCA1/2 mutation status was not significantly associated with acute skin toxicity.63 In the report by Huzno et al, no significant differences in terms of early acute and severe skin toxicity or complications requiring treatment discontinuation were observed among patients with BC carriers of BRCA mutation vs noncarriers (3% vs 4% p=0.880 and 0% vs 1% p = 0.860, respectively).64
ART Toxicity in BC Related to TP53 Mutations
Data on this issue are few due to a very limited use of ART in this set, but in vitro data seem to evocate a toxic effect. By in vitro studies, modified irradiation apoptosis (IA) in association with several TP53 polymorphisms has been related to late radiation-induced toxicity. In a study by Fuentes-Raspall et al, apoptosis levels in in vitro irradiated T lymphocytes from BC affected patients with radiotherapy-induced late effects within 6 years of follow-up were tested in a matched-control study.65 The TP53Arg72Pro genotype was determined by sequencing. As a result, patients with late radiotherapy toxicity showed less IA for all T lymphocytes except for CD8 NK cells. IA in patients with toxicity appeared to be lower than that in the control patients only in TP53Arg/Arg patients (P= 0.077). This difference was not present in patients carrying at least one Pro allele (P= 0.8266), suggesting that late side effects induced by radiotherapy are associated with low levels of IA in correlation with the 72Pro TP53 allele.65 Tan et al compared the acute radiation toxicity in TP53 72 (TP53 Arg72Pro) Pro carriers with that in noncarriers. Pro carriers had a no significantly decreased risk of acute skin toxicity in normal weight women but not in overweight patients (HR 1.07, 95% CI, 0.61–1.89). Haplotype analysis for the TP53 polymorphisms suggested that effect modification by TP53 72Pro may differ according to the p53PIN3 allele (P=0.06).66 Concerning the clinical outcome, Santi et al published a brief report on a small sample of patients, discovering a high rate of atypical vascular lesions occurring in the breast parenchyma after ART. Although these lesions were benign, they were thought to be precursors of RT induced angiosarcoma.67
ART Toxicity in BC Related to ATM Mutations
The RT-induced toxicity spectrum in patients with BC carrying ATM mutations is controversial because of the wide variety of ATM mutations acting alone or in combination. Weissberg et al studied ATM heterozygous patients with BC from A-T families and did not observe any severe acute or late radiation-induced toxicity after conventionally fractionated radiotherapy.68 In the analysis of Bremer et al on BC patients identified as ATM heterozygotes and treated with ART, with a 5.1-year median follow-up, no evidence of increased radiation-induced acute, late skin or subcutaneous reactions was recorded.28 Thus, several other conditions should be considered. For example, the condition of heterozygosity for truncating ATM mutations has been related to devastating normal tissue toxicity induced by RT, as reported in an overview by Pollard et al.69 Additionally, the ATM threshold might also play a role. Fang et al recorded a high risk of radiation-induced late adverse effects in the case of an ATM threshold of ~55% and a threshold of ~10% for more severe toxicities.70 Moreover, the concomitant presence of two pathogenic gene variants seems to be linked with grade 3–4 late subcutaneous toxicity, as reported by Iannuzzi et al among 3 out 6 ATM-mutated patients with BC carrying more than one missense variant in the ATM gene.71 In a case report by Byrd et al, the presence of biallelic mutations (one missense ATM mutation c.8672G4Ap. Gly2891Asp and a c.1A4G substitution) have been linked to a severe reaction after ART in breast cancer patients.72 Additional ATM gene polymorphisms are also involved, such as the polymorphism 1801516. This SNP, also known as G5557A or D1853N, due to a nonconservative substitution of aspartic acid for asparagine at amino acid position 1853 in an exon is the most studied variant related to skin toxicity in breast cancer radiotherapy.33 Ho et al showed that this SNP was associated with a significantly higher percentage of grade 2–4 late toxicity compared with noncarrier patients with BC.73 The issue of increased normal tissue injuries in BC patients with SNP receiving ART was also analyzed in three systematic reviews.74–76 Two of them recorded a significantly increased risk of acute toxicity and radiation-induced fibrosis among carriers of rs1801516.74,75 However, this effect has not been confirmed recently by a systematic review and meta-analysis with trial sequential analysis (TSA) by Terrazino et al. In this paper, pooled analyses of two cohorts revealed no association of ATM rs1801516 with radiation-induced telangiectasia (P = 0.316) but a significant correlation with radiation-induced fibrosis (P = 0.049).77 In carriers of VUS, no difference in toxicity has been reported.33
TSGs Mutations Related Breast Cancer and ART Induced Second Primary Malignancies (ART-SPMs)
Hereditary predisposition, young age at first diagnosis and increased radiologic surveillance have been identified as risk factors for second primary malignancies after RT in sporadic cancer (ART-SPMs).78 Indeed, the most common secondary tumour is radiation-induced sarcoma (RIS) of the breast, which, in association with sporadic BC, comprises approximately 3% of all soft-tissue sarcomas, and its cumulative incidence is 3.2 per 1000 versus 2.3 per 1000 for primary sarcoma in the general population.79 The incidence of ART-SPMs seems quite different among BC related to TSGs mutations.
ART-SPMs in BC Related to BRCA Mutations
Heterozygous BRCA1/2 carriers have a reduced capacity for DNA repair after IR, resulting in a heavy impact on genome stability. In some in vitro experiments by Nieuwenhuis et al, no differences in the repair of DNA-DBSs in a blind comparison of irradiated lymphocytes or fibroblasts derived from carriers or healthy controls was shown.80,81 Similarly, no differences were found in a study on the micronucleus test of irradiated cells derived from BRCA1/BRCA2 carriers with BC.82 The hypothesis of an increased incidence of radiation-induced second tumours, particularly in young patients who are carriers of genetic mutations, is actually based on data on young patients subjected to early intensive screening with mammography and chest X-rays. The published data are controversial, although they seem to support the hypothesis that radiation exposure at an early age (<30 years) may be a risk factor for BC development in patients carrying BRCA1 mutations, as reported by Pijpe et al and Andriew et al.83,84 Thus, there is uniform agreement in replacing mammography screening by magnetic resonance imaging for patients carrying BRCA1 mutations.85 However, the clinical data lead to different considerations. In the study of Schlosser et al on 3042 women who were BRCA carriers, among 230 patients with BRCA-linked BC who received ART with a median follow-up of 10 years, the authors described the development of 6 SPMs, among which only one developed papillary thyroid carcinoma within the radiation field 17 years after ART. Interestingly, no patient developed an in-field skin cancer or chest-wall sarcoma.86 The Kaplan-Meier estimate of 20 years of freedom from radiation-induced SPM was 99.5%. Radiation dose quantification outside the RT field ranged from 0.1 to 1 Gy, and no relationship was observed between the dose and the second cancer risk. In this large series, it has been well demonstrated that the risk of radiation-induced SPMs among BRCA mutated carriers with BC, compared to the control population, is not significantly increased.86 However, sarcoma is the most common reported histology. In a study by Kadoury et al, of 470 patients with BRCA mutations, seven developed a sarcoma in the radiation field, five in the chest wall and two in other sites. Genetic evaluation revealed BRCA1 mutations in two additional patients and BRCA2 mutations in another patient.87 Evron et al, among 162 BRCA mutation carrier patients treated with prophylactic breast radiotherapy, recorded only one case of pleomorphic sarcoma within the radiation field.88
ART-SPMs in BC Related to TP53 Mutations
It is well acknowledged that patients with TP53 mutations have an increased risk of other cancers other than primary or secondary BC, regardless of radiation exposure. With this regard, mouse models have confirmed that TP53 mutations enable cells to repair DNA damage induced by IR, leading to a significantly higher risk of tumour development.89 Small case series and retrospective studies demonstrated the emergence 2–3 years after treatment with ART radiotherapy-induced SPMs, of which the most common type was a soft-tissue sarcoma. Related aggressiveness has been reported in a case showing a de novo TP 53 mutation such as c.G841C, p.D281N, responsible for dramatic development 40 months after radiotherapy of a malignant fibrous histiocytoma of the right clavicle and another primary left BC in a 27-year-old woman treated with RT for bilateral BC.90 Nandikolla et al reported 2 cases of soft tissue sarcoma that developed after planned ART.91 Barbosa et al described a case of soft tissue angiosarcoma ten years after ART in the irradiated area of a young Li-Fraumeni patient treated with breast conservative surgery.92 Henry et al reported a case of leiomyosarcoma of the chest wall, which was diagnosed in a 24-year-old BC patient, occurring approximately 27 months after ART.93 Some authors also hypothesized that the impact of TP53 mutations could be influenced by geographical factors and ethnicity, in which some specific germline mutations are transmitted. Petry et al reported particularly high RT-induced damage in specific TP53 pathogenic germline variants, namely, those characterized by the c.1010G>A mutation in exon 10 (p. Arg337His, R337H), which is frequent in southern and south-eastern Brazil. In fact, the incidence of radiotherapy-induced malignancies was 16.6% in the group of patients treated with ART.94
ART-SPMs in BC Related to ATM Mutations
No data are available to this argument, but much evidence has been published in regard to the contralateral breast cancer (CBC) issue after ART.
TSGs Mutations Related Breast Cancer and ART-Induced Contralateral Breast Cancer (ART-CBC)
In sporadic breast cancer, an increased risk of CBC has been estimated among irradiated women younger than 45 years at the first diagnosis and after a latency period of at least 10–15 years, assuming the cause is due to the low-dose scatter radiation to the surrounding healthy tissue as a potential carcinogen with a significant dose–response relationship.95 This issue has been widely questioned in case of ART applied in patients with BC carrying TSGs mutations.
ART-CBC in BC Related to BRCA Mutations
It is well acknowledged that patients with BC carrying BRCA mutations per sé show a high risk of developing CBC. This risk has been found to be higher in patients with BC carrying BRCA1-mutations than BRCA2-mutations (p= 0.04), which is why prophylactic contralateral mastectomy is advised.47 Deleterious variants may play a role. In the WECARE study by Borg et al, deleterious mutations less than VUS mutations have been found occurring three times more often in patients BRCA carriers with CBC (15.3%) than in women with unilateral BC (5.2%).96 For information, sequence variants corresponding to deleterious mutations have been defined according the Breast Cancer Information Core (BIC) criteria: (1) all frameshift and nonsense variants with the exception of the neutral stop codon BRCA2 c.9976A>T (BIC: K3326X) and other variants located 3′ thereof; (2) all alterations in non-coding intervening sequences (IVS variants) occurring in the consensus splice acceptor or donor sequence sites, either within 2 bp of exon-intron junctions or when experimentally demonstrated to result in abnormal mRNA transcript processing; (3) missense variants that have been conclusively demonstrated, on the basis of data from linkage analysis of high-risk families, functional assays or biochemical evidence, to have a deleterious effect on known functional regions.97
However, data derived from retrospective studies have provided no clear evidence that patients with BC carriers of BRCA1/2 mutations are more predisposed to radiation-induced CBC than patients with sporadic breast cancer. In a recent multicentric study, the 10-year cumulative risk of developing CBC was found to be 25.1% (95% CI 19.6–31.9) for patients with BC carrying BRCA1 mutations, 13.5% (95% CI 9.2–19.1) for those carrying BRCA2 mutations and 3.6% (95% CI 2.2–5.7) for noncarriers. In the univariate analysis, the age at first diagnosis of BC was significantly associated with the risk of developing CBC in BRCA carriers.98 In the study conducted by Kyrova et al, the percentage of CBCs was significantly higher in familial cases of carriers versus noncarriers (p=0.02),46 but other analyses have provided contrasting results. In a retrospective study by Drooger et al enrolling 691 patients with BRCA1/2-associated breast cancer, most of them were younger than 40 years at the time of the first diagnosis, and no association between radiotherapy for the primary BC and the risk of CBC was found in both the global population (HR 0.82, 95% CI 0.45–1.49) and in the subgroup of patients younger than 40 years at first diagnosis (HR 1.36, 95% CI 0.60–3.09).99 Regarding the effect of the low doses received by the contralateral breast, a population-based nested case–control study conducted within a cohort of 52,536 survivors of unilateral breast cancer (UBC) with all women tested for BRCA1 and BRCA2 mutations yielded interesting findings. Among the women treated with radiation, the mean radiation dose was 1.1 Gy (range=0.02–6.2 Gy). The risk of developing CBC was elevated among women who carried a deleterious BRCA1/BRCA2 mutation (rate ratio, RR=4.5, confidence interval, CI=3.0–6.8) and among those treated with RT (RR=1.2, CI=1.0–1.6). However, among the mutation carriers, an incremental increase in the risk associated with the radiation dose was not statistically significant.100.
ART-CBC in BC Related to TP53 Mutations
There is no evidence concerning CBC incidence after ART in these patients due to the absolute contraindication of ART in this set.
ART-CBC in BC Related to ATM Mutations
As stated in the ASTRO recommendations, deleterious mutations are related to this risk, although they remain low.3 Probably, several conditions may play a role. It is not clear whether ATM mutations per sè or the dose scattered to the CB may predispose patients to CBC. The data suggest that carrying an ATM missense variant may accelerate the development of a second tumour and decrease the age at onset of the second breast tumour in cases of exposure to RT. Broeks et al reported that there is a nonsignificant increase in the risk of developing CBC among patients with BC who carry ATM missense variants not treated with ART (OR 0.77, 95% CI).101 Patients developing CBC with an ATM missense variant had a mean interval between the first and second breast tumours of ~101 months, compared to 122 months for patients who were noncarriers of ATM mutations (p = 0.085). Interestingly, the combination of radiation treatment and a missense variant resulted in an even shorter mean interval of 92 months in patients with CBC compared with 136 months for those who did not receive RT and did not carry a germline variant (p = 0.029).101 Bernstein et al performed a case–control study on a sample of 2105 women, analysing the association between ATM gene variants and the risk of developing synchronous CBC. They found no significant increase in the diagnosis of CBC among BC patients who carried any of the different types of ATM mutations compared with patients who were WT-ATM.102 With regard to the effect of low IR doses on CBC development, Nakamura et al demonstrated that AT cells may not be able to repair some fraction of the DNA damage and could be severely affected by low-dose-rate radiation (0,3 mGy/min).103 However, the low cumulative scattered doses to the contralateral breast estimated from simulations provide epidemiological evidence that genetic variations in ATM may truly affect the response to low individual radiation doses in the range of 50 mGy, impacting the IR-CBC incidence.104 Bernstein et al noted that in women with BC who carried ATM missense variants, those with radiation exposure levels of 1.0 Gy or higher had a significantly increased risk of CBC compared with patients with BC who were WT for ATM and who were unexposed to radiation (RR = 2.0, 95% CI = 1.1 to 3.9).102 Therefore, although the increased risk of radiation-related CBC associated with specific ATM mutations is not a key determinant in the treatment choice in breast cancer for most patients, it might warrant consideration with regard to a family history of A-T and for the adsorbed dose to the contralateral breast. No effects on CBC have been described for VUS.33
Conclusions
The lack of Phase II–III studies assessing the effect of ART in patients with BC carrying TSGs mutations like BRCA1/2, TP53 and ATM induces controversial data and uncertainties concerning the benefit of ART in these patients, supporting mastectomy as the preferred choice. Background consists of controversial retrospective data with a limited follow-up time, while genomic mutational differences and radiogenomic information are a work in progress. In light of recent literature data, the issues of ART in patients with BC carrying TSGs mutations seem to be solved in favour of a safe effect of ART when several conditions occur. The gene mutation status and the related risk should drive the choice of ART when indicated in these patients, as outlined by the ASTRO review and ASCO recommendations.3,4 In detail, BRCA mutational status does not represent per sé an absolute contraindication to ART when it is indicated in patients with moderate-risk gene mutations with caution in deleterious variants. However, as noted by Theoh et al, the choice of a risk-reducing bilateral prophylactic mastectomy should be carefully taken into account due to the risk of a new homolateral and contralateral BC, especially in younger patients.105 Mutations in TP53 are considered an absolute contraindication of radiotherapy except in those with a significantly very high risk of locoregional recurrence; mastectomy is increasingly advised.53 Radiotherapy may also be considered with caution in cases of ATM mutations, mainly in case of deleterious heterozygosity alone or in combination with ATM mutations in younger patients.102 Sharing this information in a BC multidisciplinary team discussion could be relevant. Useful and a quick guidance with information related to ART safety in patients with BC carrying TSGs mutations are summarized below in Table 1.
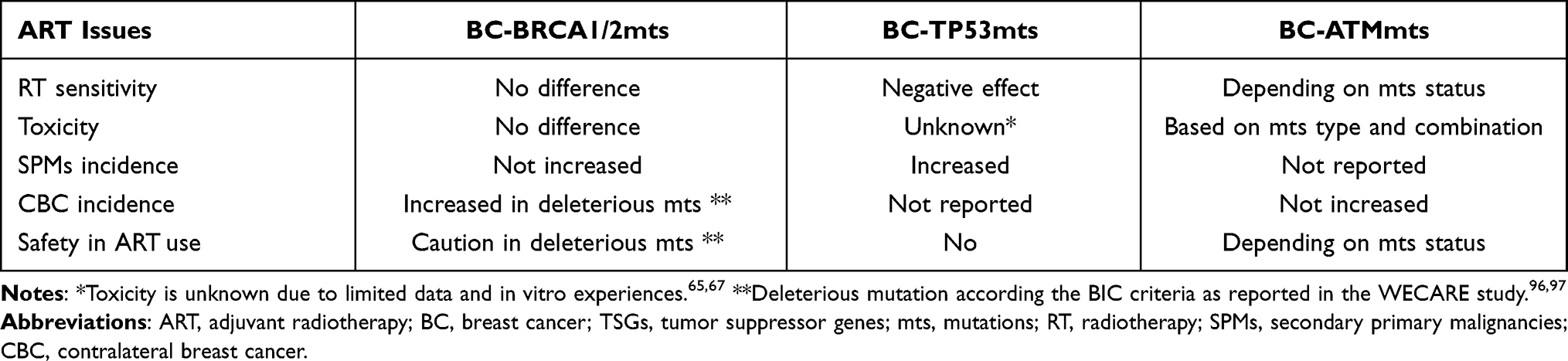 |
Table 1 Effects of ART Issues in BC Related to TSGs Mutations as Summarized in This Review |
Acknowledgment
The authors thank Mr James Andrew Bradley as Cambridge English Teacher Certificate supervisor.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Terui-Kohbata H, Yoshida M. Current condition of genetic medicine for hereditary breast cancer. Mol Clin Oncol. 2017;7:98–102. doi:10.3892/mco.2017.1260
2. Easton DF, Pharoah PDP, Antoniou AC, et al. Gene-panel sequencing and the prediction of breast-cancer risk. N Engl J Med. 2015;372:2243–2257. doi:10.1056/NEJMsr1501341
3. Bergom C, West CM, Higginson DS, et al. The implications of genetic testing on radiation therapy decisions: a guide for radiation oncologists. Int J Radiat Oncol Biol Phys. 2019;105:698–712. doi:10.1016/j.ijrobp.2019.07.026
4. Tung NM, Boughey JC, Pierce LJ, et al. Management of Hereditary Breast Cancer: American Society of Clinical Oncology, American Society for Radiation Oncology, and Society of Surgical Oncology Guideline. J Clin Oncol. 2020;38:2080–2106. doi:10.1200/JCO.20.00299
5. Shiovitz S, Korde LA. Genetics of breast cancer: a topic in evolution. Ann Oncol. 2015;26:1219–1291. doi:10.1093/annonc/mdv022
6. Ford D, Easton DF, Peto J. Estimates of the gene frequency of BRCA1 and its contribution to breast and ovarian cancer incidence. Am J Hum Genet. 1995;57:1457–1462.
7. Cancer Genome Atlas Network. Comprehensive molecular portraits of human breast tumours. Nature. 2012;490(7418):61–70. doi:10.1038/nature11412
8. Gonzalez-Angulo AM, Timms KM, Liu S, et al. Incidence and outcome of BRCA mutations in unselected patients with triple receptor-negative breast cancer. Clin Cancer Res. 2011;17:1082–1089. doi:10.1158/1078-0432.ccr-10-2560
9. Mavaddat N, Barrowdale D, Andrulis IL, et al. Pathology of breast and ovarian cancers among BRCA1 and BRCA2 mutation carriers: results from the Consortium of Investigators of Modifiers of BRCA1/2 (CIMBA). Cancer Epidemiol Biomarkers Prev. 2012;21:134–147. doi:10.1158/1055-9965.epi-11-0775
10. Risch HA, McLaughlin JR, Cole DE, et al. Population BRCA1 and BRCA2 mutation frequencies and cancer penetrances: a kin-cohort study in Ontario, Canada. J Natl Cancer Inst. 2006;98:1694–1706. doi:10.1093/jnci/djj465
11. Rakha EA, Reis-Filho JS, Ellis IO. Basal-like breast cancer: a critical review. J Clin Oncol. 2008;26:2568–2581. doi:10.1200/JCO.2007.13.1748
12. Lee EH, Park SK, Park B, et al. Effect of BRCA1/2 mutation on short-term and long-term breast cancer survival: a systematic review and metaanalysis. Breast Cancer Res Treat. 2010;122:11–25. doi:10.1007/s10549-010-0859-2
13. Baretta Z, Mocellin S, Goldin E, et al. Effect of BRCA germline mutations on breast cancer prognosis: a systematic review and meta-analysis. Medicine. 2016;95:e4975. doi:10.1097/MD.0000000000004975
14. Copson ER, Maishman TC, Tapper WJ, et al. Germline BRCA mutation and outcome in young-onset breast cancer (POSH): a prospective cohort study. Lancet Oncol. 2018;19:169–180. doi:10.1016/S1470-2045(17)30891-4
15. Petitjean A, Achatz MI, Borresen-Dale AL, et al. TP53 mutations in human cancers: functional selection and impact on cancer prognosis and outcomes. Oncogene. 2007;26:2157–2165. doi:10.1038/sj.onc.1210302
16. Li FP, Fraumeni JF, Mulvihill JJ, et al. A cancer family syndrome in twenty-four kindreds. Cancer Res. 1988;48:5358–5362.
17. Mai PL, Best AF, Peters JA, et al. Risks of first and subsequent cancers among TP53 mutation carriers in the National Cancer Institute LiFraumeni syndrome Cohort. Cancer. 2016;122:3673–3681. doi:10.1002/cncr.30248
18. Kamihara J, Rana HQ, Garber JE. Germline TP53 mutations and the changing landscape of Li-Fraumeni syndrome. Hum Mutat. 2014;35:654–662. doi:10.1002/humu.22559
19. McCuaig JM, Armel SR, Novokmet A, et al. Routine TP53 testing for breast cancer under age 30: ready for prime time? Fam Cancer. 2012;11:607–613. PMID: 22851211. doi:10.1007/s10689-012-9557-z
20. Gonzalez KD, Buzin CH, Noltner KA, et al. High frequency of de novo mutations in Li–Fraumeni syndrome. J Med Genet. 2009;46:689–693. doi:10.1136/jmg.2008.058958
21. Melhem-Bertrandt A, Bojadzieva J, Ready KJ, et al. Early onset HER2-positive breast cancer is associated with germline TP53 mutations. Cancer. 2012;118(4):908–913. doi:10.1002/cncr.26377
22. Rath MG, Masciari S, Gelman R, et al. Prevalence of germline TP53 mutations in HER2+ breast cancer patients. Breast Cancer Res Treat. 2013;139:193–198. doi:10.1007/s10549-012-2375-z
23. Packwood K, Martland G, Sommerlad M, et al. Breast cancer in patients with germline TP53 pathogenic variants have typical tumour characteristics: the Cohort study of TP53 carrier early onset breast cancer (COPE study). J Pathol Clin Res. 2019;5(3):189–198. doi:10.1002/cjp2.133
24. Liao H, Li H. Advances in the detection technologies and clinical applications of circulating tumor DNA in metastatic breast cancer. Cancer Manag Res. 2020;12:3547–3560. doi:10.2147/CMAR.S249041
25. Overgaard J. TP53 mutation is an independent prognostic marker for poor outcome in both node-negative and node-positive breast cancer. Acta Oncol. 2000;39(3):327–333. doi:10.1080/028418600750013096
26. Bartek J, Bartkova J, Lukas J. DNA damage signalling guards against activated oncogenes and tumour progression. Oncogene. 2007;26(56):7773–7779. doi:10.1038/sj.onc.1210881
27. Geoffroy-Perez B, Janin N, Ossian K, et al. Cancer risk in heterozygotes for ataxia–telangiectasia. Int J Cancer. 2001;93:288–293. doi:10.101002/ijc.1329
28. Bremer M, Klöpper K, Yamini P, et al. Clinical radiosensitivity in breast cancer patients carrying pathogenic ATM gene mutations: no observation of increased radiation-induced acute or late effects. Radiother Oncol. 2003;69:155–160. doi:10.1016/j.radonc.2003.08.004
29. Thompson D, Duedal S, Kirner J, et al. Cancer risks and mortality in heterozygous ATM mutation carriers. J Natl Cancer Inst. 2005;97:813–822. doi:10.1093/jnci/dji141
30. Renwick A, Thompson D, Seal S, et al. ATM mutations that cause ataxia-telangiectasia are breast cancer susceptibility alleles. Nat Genet. 2006;38:873–875. doi:10.1038/ng1837
31. Lavin MF, Scott S, Gueven N, et al. Functional consequences of sequence alterations in the ATM gene. DNA Repair. 2004;3(8–9):1197–1205. doi:10.1016/j.dnarep.2004.03.011
32. Scott SP, Bendix R, Chen P, et al. Missense mutations but not allelic variants alter the function of ATM by dominant interference in patients with breast cancer. Proc Natl Acad Sci USA. 2002;99:925–930. doi:10.1073/pnas.012329699
33. Mullins BT, Gupta G. Increased radiation toxicity with germline ATM variant of uncertain clinical significance. Rep Pract Oncol Radiother. 2019;24:672–680. doi:10.1016/j.rpor.2019.09.008
34. Venkitaraman AR. How do mutations affecting the breast cancer genes BRCA1 and BRCA 2 cause cancer susceptibility? DNA Repair. 2019;81:102668. doi:10.1016/j.dnarep.2019.102668
35. Moynahan ME, Pierce AJ, Jasin M. BRCA2 is required for homology-directed repair of chromosomal breaks. Mol Cell. 2001;7:263–272. doi:10.1016/S10972765(01)00174-5
36. Carey LA. Targeted chemotherapy? Platinum in BRCA1 – dysfunctional breast cancer. J Clin Oncol. 2010;28:361–365. doi:10.1200/JCO.2009.24.0838
37. Kan C, Zhang J. BRCA1 mutation: a predictive marker for radiation therapy? Int J Radiat Oncol Biol Phys. 2015;93:281–293. doi:10.1016/j.ijrobp.2015.05.037
38. Barwell J, Pangon L, Georgiou A, et al. Lymphocyte radiosensitivity in BRCA1 and BRCA2 mutation carriers and implications for breast cancer susceptibility. Int J Cancer. 2007;121:1631–1636. doi:10.1002/ijc.22915
39. Shen SX, Weaver Z, Xu X, et al. A targeted disruption of the murine Brca1 gene causes gamma-irradiation hypersensitivity and genetic instability. Oncogene. 1998;17:3115–3124. doi:10.1038/sj.onc.1202243
40. Foray N, Randrianarison V, Marot D, et al. Gamma-rays induced death of human cells carrying mutations of BRCA1 or BRCA2. Oncogene. 1999;18:7334–7342. doi:10.1038/sj.onc.1203165
41. Baert A, Depuydt J, Van Maerken T, et al. Increased chromosomal radiosensitivity in asymptomatic carriers of a heterozygous BRCA1 mutation. Breast Cancer Res. 2016;18:52–64. doi:10.1186/s13058-016-0709-1
42. Baert A, Depuydt J, Van Maerken T, et al. Analysis of chromosomal radiosensitivity of healthy BRCA2 mutation carriers and non-carriers in BRCA families with the G2 micronucleus assay. Oncol Rep. 2017;37:1379–1386. doi:10.3892/or.2017.5407
43. Robson ME, Chappuis PO, Satagopan J, et al. A combined analysis of outcome following breast cancer: differences in survival based on BRCA1/ BRCA2 mutation status and administration of adjuvant treatment. Breast Cancer Res. 2004;6:8–17. doi:10.1186/bcr658
44. Pierce LJ, Levin AM, Rebbeck TR, et al. Ten-year multi-institutional results of breastconserving surgery and radiotherapy in BRCA1/2 associated stage I/II breast cancer. J Clin Oncol. 2006;24:2437–2443. doi:10.1200/JCO.2005.02.7888
45. Brekelmans CTM, Tilanus-Linthorst MMA, Seynaeve C, et al. Tumour characteristics, survival and prognostic factors of hereditary breast cancer from BRCA2-, BRCA1- and non-BRCA1/2 families as compared to sporadic breast cancer cases. Eur J Cancer. 2007;43:867–876. doi:10.1016/j.ejca.2006.12.009
46. Kirova YM, Savignoni A, Sigal-Zafrani B, et al. Is the breast-conserving treatment with radiotherapy appropriate in BRCA1/2 mutation carriers? Long-term results and review of the literature. Breast Cancer Res Treat. 2010;120:119–126. doi:10.1007/s10549-009-0685-6
47. Valachis A, Nearchou AD, Lind P. Surgical management of breast cancer in BRCA mutation carriers: a systematic review and meta-analysis. Breast Cancer Res Treat. 2014;144:443–455. doi:10.1007/s10549-014-2890-1
48. Vallard A, Magnè N, Guy JB, et al. Is breast-conserving therapy adequate in BRCA1/2 mutation carriers? The radiation oncologist’s point of view. Br J Radiol. 2019;92:20170657 1–9. doi:10.1259/bjr.20170657
49. Kastan MB, Zhan O, El-Deiry WS, et al. A mammalian cell cycle checkpoint pathway utilizing p53 and GADD45 is defective in ataxia-telangiectasia. Cell. 1992;71:587–597. doi:10.1016/0092-8674(92)90593-2
50. Mcllwrath AJ, Vasey PA, Ross GM, et al. Cell cycle arrests and radiosensitivity of human tumor cell lines: dependence on wild-type p53 for radiosensitivity. Cancer Res. 1994;54:3718–3722.
51. Olivier M, Goldgar DE, Sodha N, et al. Li–Fraumeni and related syndromes: correlation between tumor type, family structure, and TP53 genotype. Cancer Res. 2003;63:6643–6650.
52. Schon K, Tischkowitz M. Clinical implications of germline mutations in breast cancer: TP53. Breast Cancer Res Treat. 2018;167:417–423. doi:10.1007/s10549-017-4531-y
53. McBride KA, Ballinger ML, Killick E, et al. Li–Fraumeni syndrome: cancer risk assessment and clinical management. Nat Rev Clin Oncol. 2014;11:260–271. doi:10.1038/nrclinonc.2014.41
54. Kappel S, Janschek E, Wolf B, et al. TP53 germline mutation may affect response to anticancer treatments: analysis of an intensively treated Li–Fraumeni family. Breast Cancer Res Treat. 2015;151:671–678. doi:10.1007/s10549-015-3424-1
55. Barlow C, Brown KD, Deng CX, et al. Atm selectively regulates distinct p53- dependent cell-cycle checkpoint and apoptotic pathways. Nat Genet. 1997;17:453–456. doi:10.1038/ng1297-453
56. Worgul BV, Smilenov L, Brenner DJ, et al. Atm heterozygous mice are more sensitive to radiation induced cataracts than are their wild-type counterparts. Proc Natl Acad Sci. 2002;99:9836–9839. doi:10.1073/pnas.162349699
57. Paterson MC, Anderson AK, Smith BP, et al. Enhanced radiosensitivity of cultured fibroblasts from ataxia telangiectasia heterozygotes manifested by defective colony-forming ability and reduced DNA repair replication after hypoxic gamma-irradiation. Cancer Res. 1979;39:3725–3734.
58. Clarke RA, Fang ZH, Marr PJ, et al. ATM induction insufficiency in a radiosensitive breast-cancer patient. Aust Radiol. 2002;46:329–335. doi:10.1046/j.1440-1673.2002.01072.x
59. Su Y, Swift M. Outcomes of adjuvant radiation therapy for breast cancer in women with ataxia–telangiectasia mutations. JAMA. 2001;286:2233–2234. doi:10.1001/jama.286.18.2233
60. Meyer A, John E, Dork T, et al. Breast cancer in female carriers of ATM gene alterations: outcome of adjuvant radiotherapy. Radiother Oncol. 2004;72:319–323. doi:10.1016/j.radonc.2004.07.010
61. Jerzak KJ, Mancuso T, Eisen A. Ataxia-telangiectasia gene (ATM) mutation heterozygosity in breast cancer: a narrative review. Curr Oncol. 2018;25(2):176–180. doi:10.3747/co.25.3707
62. Shanley S, McReynolds K, Ardern-Jones A, et al. LateToxicity is not increased in BRCA1/BRCA2 mutation carriers undergoing breast radiotherapy in the United Kingdom. Clin Cancer Res. 2006;12:7025–7032. doi:10.1158/1078-0432.CCR-06-1244
63. Park H, Choi DH, Noh JM, et al. Acute skin toxicity in Korean breast cancer patients carrying BRCA mutations. Int J Radiat Biol. 2014;90:90–94. doi:10.3109/09553002.2013.835504
64. Huszno J, Budryk M, Kołosza Z, et al. The risk factors of toxicity during chemotherapy and radiotherapy in breast cancer patients according to the presence of BRCA gene mutation. Contemp Oncol. 2015;19:72–76. doi:10.5114/wo.2015.50014
65. Fuentes-Raspall MJ, Caragol I, Alonso C, et al. Apoptosis for prediction of radiotherapy late toxicity: lymphocyte subset sensitivity and potential effect of TP53 Arg72Pro polymorphism. Apoptosis. 2015;20:371–382. doi:10.1007/s10495-014-1056-2
66. Tan XL, Popanda O, Ambrosone CB, et al. Association between TP53 and p21 genetic polymorphisms and acute side effects of radiotherapy in breast cancer patients. Breast Cancer Res Treat. 2006;97:255–262. doi:10.1007/s10549-005-9119-2
67. Santi R, Cetica V, Franchi A, et al. Tumour suppressor gene TP53 mutations in atypical vascular lesions of breast skin following radiotherapy. Histopathology. 2011;58:455–466. doi:10.1111/j.1365-2559.2011.03770.x
68. Weissberg JB, Huang DD, Swift M. Radiosensitivity of normal tissues in ataxia– telangiectasia heterozygotes. Int J Radiat Oncol Biol Phys. 1998;42:1133–1136. doi:10.1016/S0360-3016(98)00295-8
69. Pollard JM, Gatti RA. Clinical radiation sensitivity with DNA repair disorders: an overview. Int J Radiat Oncol Biol Phys. 2009;74:1323–1331. doi:10.1016/j.ijrobp.2009.02.057
70. Fang Z, Kozlov S, McKay MJ, et al. Low levels of ATM in breast cancer patients with clinical radiosensitivity. Genome Integr. 2010;1:9–20. doi:10.1186/2041-9414-1-9
71. Iannuzzi CM, Atencio DP, Green S, et al. ATM mutations in female breast cancer patients predict for an increase in radiation-induced late effects. Int J Radiat Oncol Biol Phys. 2002;52:606–613. doi:10.1016/S0360-3016(01)02684-0
72. Byrd PJ, Srinivasan V, Last JI, et al. Severe reaction to radiotherapy for breast cancer as the presenting feature of ataxiateleangectasia. Br J Cancer. 2012;106:262–268. doi:10.1038/bjc.2011.534
73. Ho AY, Fan G, Atencio DP, et al. Possession of ATM sequence variants as predictor for late normal tissue responses in breast cancer patients treated with radiotherapy. Int J Radiat Oncol Biol Phys. 2007;69:677–684. doi:10.1016/j.ijrobp.2007.04.012
74. Dong L, Cui J, Tang F, et al. Ataxia telangiectasia-mutated gene polymorphisms and acute normal tissue injuries in cancer patients after radiation therapy: a systematic review and meta-analysis. Int J Radiat Oncol Biol Phys. 2015;91:1090–1098. doi:10.1016/j.ijrobp.2014.12.041
75. Zhang Y, Liu Z, Wang M, et al. Single nucleotide polymorphism rs1801516 in Ataxia Telangiectasia-mutated gene predicts late fibrosis in cancer patients after radiotherapy: a PRISMA-compliant systematic review and meta-analysis. Medicine. 2016;95:e3267. doi:10.1097/MD.0000000000003267
76. Su M, Yin ZH, Wu W, et al. Meta-analysis of associations between ATM Asp1853Asn and TP53 Arg72Pro polymorphisms and adverse effects of cancer radiotherapy. Asian Pac J Cancer Prev. 2014;15:10675–10681. doi:10.7314/apjcp.2014.15.24.10675
77. Terrazzino S, Cargnin S, Deantonio L, et al. Impact of ATM rs1801516 on late skin reactions of radiotherapy for breast cancer: evidences from a cohort study and a trial sequential meta-analysis. PLoS One. 2019;14:e0225685. doi:10.1371/journal.pone.0225685
78. Zhang W, Becciolini A, Biggeri A, et al. Second malignancies in breast cancer patients following radiotherapy: a study in Florence, Italy. Breast Cancer Res. 2011;13:38–47. doi:10.1186/bcr2860
79. Sheth GR, Cranmer LD, Smith BD, et al. Radiation-induced sarcoma of the breast: a systematic review. Oncologist. 2012;17:405–418. doi:10.1634/theoncologist.2011-0282
80. Nieuwenhuis B, Van Assen-bolt AJ, Van Waarde-verhagen MAWH, et al. BRCA1 and BRCA2 heterozygosity and repair of X-ray-induced DNA damage. Int J Radiat Biol. 2002;78:285–295. doi:10.1080/09553000110097974
81. Speit G, Trenz K. Chromosomal mutagen sensitivity associated with mutations in BRCA genes. Cytogenet Genome Res. 2004;104(1–4):325–332. doi:10.1159/000077511
82. Bayens A, Thierens H, Claes K, et al. Chromosomal radiosensitivity in BRCA1 and BRCA2 mutation carriers. Int J Radiat Oncol Biol. 2004;80(10):745–756. doi:10.1080/09553000400017937
83. Pijpe A, Andrieu N, Easton DF, et al. Exposure to diagnostic radiation and risk of breast cancer among carriers of BRCA1/2 mutations: retrospective cohort study (GENERADRISK). Br Med J. 2012;6:e5660. doi:10.1136/bmj.e5660
84. Andrieu N, Easton FD, Chang-Claude J, et al. Effect of chest X-rays on the risk of breast cancer among BRCA1/2 mutation carriers in the International BRCA1/2 Carrier Cohort Study: a report from the EMBRACE, GENEPSO, GEO-HEBON, and IBCCS Collaborators’ Group. J Clin Oncol. 2006;24:3361–3366. doi:10.1200/JCO.2005.03.3126
85. Warner E. Impact of MRI surveillance and breast cancer detection in young women with BRCA mutations. Ann Oncol. 2011;22:44–49. doi:10.1093/annonc/mdq665
86. Schlosser S, Rabinovitch R, Shatz Z, et al. Radiation Associated secondary malignancies in BRCA mutation carriers treated for breast cancer. Int J Radiat Oncol Biol Phys. 2020;107:353–359. doi:10.1016/j.ijrobp.2020.02.020
87. Kadouri L, Sagi M, Goldberg Y, et al. Genetic predisposition to radiation induced sarcoma: possible role for BRCA and p53 mutations. Breast Cancer Res Treat. 2013;140:207–211. doi:10.1007/s10549-013-2621-z
88. Evron E, Ben-David AM, Goldberg H, et al. Prophylactic irradiation to the contralateral breast for BRCA mutation carriers with early-stage breast cancer. Ann Oncol. 2019;30:412–417. doi:10.1093/annonc/mdy515
89. Kasper E, Angot E, Colasse E, et al. Contribution of genotoxic anticancer treatments to the development of multiple primary tumours in the context of germline TP53 mutations. Eur J Cancer. 2018;101:254–262. doi:10.1016/j.ejca.2018.06.011
90. Salmon A, Amikam D, Sodha N, et al. Rapid development of post-radiotherapy sarcoma and breast cancer in a patient with a novel germline ‘De-Novo’ TP53 mutation. Clin Oncol. 2007;19:490–493. doi:10.1016/j.clon.2007.05.001
91. Nandikolla AG, Venugopal S, Anampa J. Breast cancer in patients with Li-Fraumeni syndrome – a case series study and review of literature. Breast Cancer (Dove Med Press). 2017;9:207–215. doi:10.2147/BCTT.S134241
92. Barbosa OV, Reiriz AB, Boff RA, et al. Angiosarcoma in previously irradiated breast in patient with Li-Fraumeni syndrome. A case report. Sao Paulo Med J. 2015;133:151–153. doi:10.1590/1516-3180.20126740004
93. Henry E, Villalobos V, Million L, et al. Chest wall leiomyosarcoma after breast conservative therapy for early-stage breast cancer in a young woman with Li-Fraumeni syndrome. J Natl Compr Cancer Netw. 2012;10:939–942. doi:10.6004/jnccn.2012.0097
94. Petry V, Colombo Bonadio R, Carneiro Cagnacci AQ, et al. Radiotherapy- induced malignancies in breast cancer patients with TP53 pathogenic germline variants (Li-Fraumeni syndrome). Fam Cancer. 2020;19:47–53. doi:10.1007/s10689-019-00153-5
95. Stovall M, Smith SA, Langholz BM, et al. Dose to the contralateral breast from radiation therapy and risk of second primary breast cancer in the WECARE Study. Int J Radiat Oncol Biol Phys. 2008;72:1021–1030. doi:10.1016/j.ijrobp.2008.02.040
96. Borg A, Haile RW, Malone KE, et al. Characterization of BRCA1 and BRCA2 deleterious mutations and variants of unknown clinical significance in unilateral and bilateral breast cancer: the WECARE Study. Hum Mutat. 2010;31(3):E1200–E1240. doi:10.1002/humu.21202
97. Cline MS, Liao MG, Parsons MT, et al. BRCA Challenge: BRCA Exchange as a global resource for variants in BRCA1 and BRCA2. PLoS Genet. 2018;14(12):e1007752. doi:10.1371/journal.pgen.10077527
98. Engel C, Fischer C, Zachariae S, et al. Breast cancer risk in BRCA1/2 mutation carriers and noncarriers under prospective intensified surveillance. Int J Cancer. 2020;146:999–1009. doi:10.1002/ijc.32396
99. Drooger JC, Akdeniz D, Pignol JP, et al. Adjuvant radiotherapy for primary breast cancer in BRCA1 and BRCA2 mutation carriers and risk of contralateral breast cancer with special attention to patients irradiated at younger age. Breast Cancer Res Treat. 2015;154:171–180. doi:10.1007/s10549-015-3597-7
100. Bernstein JL, Thomas DC, Shore RE, et al. Contralateral Breast Cancer after radiotherapy among BRCA 1 and BRCA 2 mutation carriers: a WECARE study report. Eur J Cancer. 2013;49(14):2979–2985. doi:10.1016/j.ejca.2013.04.028
101. Broeks A, Braaf LM, Huseinovic A, et al. The spectrum of ATM missense variants and their contribution to contralateral breast cancer. Breast Cancer Res Treat. 2008;107:243–248. doi:10.1007/s10549-007-9543-6
102. Bernstein JL, Concannon P; WECARE Study Collaborative Group. ATM, radiation, and the risk of second primary breast cancer. Int J Radiat Biol. 2017;93:1121–1127. doi:10.1080/09553002.2017.1344363
103. Nakamura H, Yasui Y, Saito N, et al. DNA repair defect in AT cells and their hypersensitivity to low-dose-rate radiation. Radiat Res. 2006;165:277–282. doi:10.1667/rr3519.1
104. Ojima M, Ban N, Kai M. DNA double-strand breaks induced by very low X-ray doses are largely due to bystander effects. Radiat Res. 2008;170:365–371. doi:10.1667/RR1255.1
105. Teoh V, Tasoulis MK, Gerald G. Contralateral prophylactic mastectomy in women with unilateral breast cancer who are genetic carriers, have a strong family history or are just young at presentation. Cancers. 2020;12:140. doi:10.3390/cancers12010140
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.