")
Back to Journals » Open Access Emergency Medicine » Volume 12
Brain CT Findings in Patients with First-Onset Seizure Visiting the Emergency Department in Mashhad, Iran
Authors Zarmehri B, Teimouri A , Ebrahimipour N , Foroughian M , Talebzadeh V , Saeidi M , Alirezaei M
Received 4 December 2019
Accepted for publication 2 June 2020
Published 10 June 2020 Volume 2020:12 Pages 159—162
DOI https://doi.org/10.2147/OAEM.S241124
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Bahram Zarmehri,1 Ali Teimouri,1 Navid Ebrahimipour,2 Mahdi Foroughian,1 Vahid Talebzadeh,3 Morteza Saeidi,4 Mehran Alirezaei5
1Department of Emergency Medicine, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran; 2Department of Emergency Medicine, Faculty of Medicine, North Khorasan University of Medical Sciences, Bojnurd, Iran; 3Department of Emergency Medicine, Faculty of Medicine, Gonabad University of Medical Sciences, Gonabad, Iran; 4Department of Neurology, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran; 5Department of Neurosurgery, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
Correspondence: Mehran Alirezaei
Department of Neurosurgery, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad 99199- 91766, Iran
Tel +98-51-38012613
Fax +98-51-38413493
Email [email protected]
Introduction: Regarding the complications and costs of CT imaging for patients, this study aimed at investigating the necessity of CT scans in patients visiting the emergency unit with first-onset seizure.
Methods: One hundred patients who had experienced their first seizure were enrolled. Their CT scan was studied, and based on the radiology report, the type of probable pathologies and their percentage were determined.
Results: The patient’s mean age was 39.78± 17.43 yrs. CT scan abnormalities were reported in 27 cases as follows: nonspecific senile changes in 11 (40.7%), encephalomalacia in 3 (11.1%), acute infarct in 5 (18.5%), lacunar infarct in 3 (11.1%), mass-like lesion in 4 (14.8%) and cerebral venous thrombosis (CVT) evidence in 1 (3.7%). Acute infarct and mass-like lesions were seen together in the CT scan of one patient. In only 9 of the 27 abnormal CT scans, the findings were in accordance with seizure consisting of an acute infarct, mass-like lesion, and CVT evidence.
Discussion: It seems that performing a CT scan in all patients referring to the emergency department with a first-onset seizure is not necessary.
Keywords: seizures, diagnostic imaging, tomography, cerebral infarction
Introduction
Seizure is a transient physiologic brain disorder resulting from abnormal electrical discharge in a group of neurons in the cortex, which its type depends on the function and replacement of the affected neurons.1 Myoclonic seizures consist of sudden, brief movements that are not associated with any apparent disturbance of consciousness.1 Seizures usually result in reduced or loss of consciousness.2 The most common cause of seizure is epilepsy; other causes include cerebrovascular diseases, head trauma, primary or metastatic brain tumors, central nervous system infections, and metabolic disorders.3 Epileptic seizures are caused by significant and recurrent disorders of brain activity. They can occur instantly, with no introduction. However, in some cases, just before the onset of seizure, the patient may experience a warning period (aura) with a series of symptoms such as a strange sensation or a specific odor or taste.1 Brain CT (computed tomography) scanning is a non-invasive method that facilitated the diagnosis of many neurologic diseases.4 However, during CT imaging, the patient is exposed to ionizing radiation, and studies have shown that these small amounts of radiation can be accompanied by a high risk of cancer, especially in children.5 As every CT scan is considered to be part of lifetime exposure to radiation, it is imperative to limit exposure to radiation through CT scanning.5 Specific strategies can be taken to decrease the risk of imaging methods in patients with first-onset seizures, such as performing a brain CT scan only when necessary, use of ultrasound or MRI (magnetic resonance imaging) instead of a CT where possible, and restricting the area, which is exposed to radiation.6 Generally, the workup of patients with first-onset seizure who visit the emergency department includes take a full medical history, performed a physical examination, and monitor focal neurologic findings.7 The indications of emergent CT scan include a new focal defect, acute changes in the level of consciousness, fever, recent trauma, persistent headache, history of cancer, anticoagulant agents consumption, Known or suspected history of AIDS, more than 40 years age, secondary generalized seizure and partial-complex seizure.8
In most patients with first-time seizure visiting the emergency department, chances of positive findings in brain CT scan that change management may be low, but these findings may change the management and outcome of patients.
In this study, we aimed to calculate the chance of positive findings that explain seizures in patients visiting the emergency department.
Patients and Methods
In this descriptive-analytical study, 100 patients with first-onset seizure visiting the Emergency department of Qaem Hospital, Mashhad, Iran from October 2017–2018 were enrolled.
Inclusion criteria were first-onset seizure and aged above 18 years old. Exclusion criteria were pseudo seizure, seizure in pregnancy, febrile seizure, and unwilling to participate in the study.
This study was conducted in accordance with the Declaration of Helsinki. The Ethics Committee approved the study protocol of Mashhad University of Medical Sciences also all patients sign written informed consent. Two associate professors of Mashhad University of Medical Sciences independently reported brain CT scans of these patients.
SPSS software (version 20; SPSS Inc., Chicago, IL) was employed for the statistical analysis. A P value of less than 0.05 was considered significant. Descriptive statistics such as mean and standard deviation were employed to describe data.
Results
A total of 100 patients were enrolled in this study. There were 62 (62.0%) males in these patients, and their mean age was 39.78±17.43 years (range: 18–78 years).
The CT scan results revealed a normal CT in 73 cases; it was abnormal in the remaining 27 cases. The right side was involved in 28.6% and the left side in 64.3%; it was bilateral in 7.1% (Table 1).
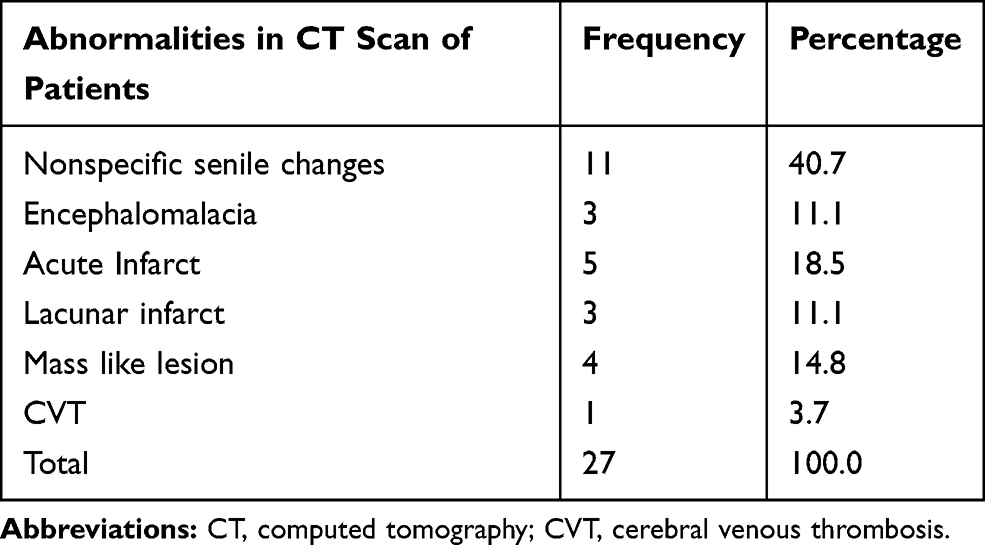 |
Table 1 Frequency and Percentage of Abnormalities in Brain CT Scan of Patients |
Regarding the 27 cases with an abnormal CT, nonspecific senile changes were observed in 11 (40.7%). Encephalomalacia in 3 (11.1%), acute infarct in 5 (18.5%), lacunar infarct in 3 (11.1%), mass-like lesion in 4 (14.8%) and cerebral venous thrombosis (CVT) evidence in 1 (3.7%) (Table 1).
In one case, both acute infarct and a mass-like lesion were seen together. Only in 9 cases out of the 27 patients with CT abnormalities the CT findings justified the seizure occurrence, they included an acute infarct, mass-like lesion, and CVT evidence.
Discussion
Among the 100 studied patients, nine had an abnormal CT justifying the existing condition. In this regard, Kotisaaari et al in 2017 performed a CT scan on 416 of the 449 patients visiting the emergency unit, among which 49 (12%) had emergent imaging findings in the CT scan.4 de la Sayette et al, in a study on 387 patients over 50 years of age with late-onset epilepsy, reported that most patients for whom CT scan was performed had either normal results or evidence of cerebral atrophy.9
In another study on children hospitalized due to afebrile seizure in Tehran, Iran, 90% of the CT scans were reported as normal, which is in accordance with our study.10
On the other hand, Smith et al in 2013 studied 309 patients with their first-onset seizure in South Africa. Emergent CT imaging was performed for 169 patients, for which 96 (56.8%) showed abnormalities, most commonly as infarction, intracerebral hemorrhage, and atrophy.11 Their findings are inconsistent with our results revealing a very lower rate of abnormalities in emergent CT scans. In the study by Kumar et al in India, 49% of the cases had abnormalities in their CT scan.12 The same figure was 44.3% of the 210 patients with seizure in Arruda et al study in Brazil.13 In the study by Gandon et al in 1983, among the 356 patients with seizure, 40% had an abnormal CT scan; this figure was 61% in Longe et al study in Saudi Arabia and 33% in Yang et al study.14–16 The results of the mentioned studies are different from ours; this can be explained by the different studied target groups and the rarity of studies on patients with first-onset seizures. Moreover, the different CT scan devices and the moderator-dependent reports can be taken into consideration when interpreting the different study results.
Nevertheless, in the current study, 27 patients had abnormalities in their CT scans. Nonspecific senile changes were observed in 11 (40.7%). Encephalomalacia in 3 (11.1%), acute infarct in 5 (18.5%), lacunar infarct in 3 (11.1%), the mass-like lesion in 4 (14.8%) and CVT evidence in 1 (3.7%) however only in 9 cases out of the 27 patients with CT abnormalities the CT findings justified the seizure occurrence, they included an acute infarct, mass-like lesion, and CVT evidence. In Smith et al study, acute infarction, intracerebral hemorrhage, and atrophy were the most common findings,11 whereas, in Long et al study, cerebral atrophy was the most common.15 In Gordon et al study, focal or generalized cerebral atrophy stood in the first place, which is consistent with our findings.17 The primary etiology of atrophy prevalence in such cases is the higher age of the studied cases. Therefore in studies that are performed in children, the CT scan findings may vary. As an example in Kumar et al study, the most common finding in CT imaging of epileptic children was ring-enhancing lesions.12 With the introduction of the CT scan to the field of diagnosis, a huge difference was made. As the accessibility to this device has been facilitated in the last 10–15 years, the physicians can request a CT more easily and more rapidly.18 Based on Hendel et al study, the main cause of CT imaging has been epilepsy and recurrent seizures.19 Harden et al also stated that a CT scan is very helpful in the diagnosis of seizure etiology in seizure patients with a predisposing history, focal seizure onset, an abnormal neurologic exam, a history of AIDS, or who are younger than six months old.20 Today health care costs are rising rapidly, and imaging is at the center of this massive flood of diagnostic measures with the fastest rising costs among medical services.21–23 Radiology services application increased by 14.6% between 1993 and 1999, accounting for approximately 10% of total medical services costs.6 However, it is believed that over 20% of the care provided to such patients is unnecessary, and inappropriate utilization is a major problem in health care, especially in capital-intensive fields such as imaging.6,10,24,25 According to a report from the Canadian Agency for Medicine and Technology in Health, 10% to 20% of imaging studies are unnecessary.6 In the study by Kotisaari et al, headache (odds ratio=3.62), movement symptoms (odds ratio=3.23), history of malignancy (odds ratio=3.05), unstable mental status (odds ratio=2.27) are dependent on the pathologic findings in the CT scan.4 Therefore, one could rely on the clinical symptoms before requesting a CT scan in patients with a first-onset seizure.
This study has potential limitations include the insufficient sample size. Also, we did not investigate the relationship between risk factors include headache or history of malignancy and abnormal CT scan findings in patients with a first seizure.
Conclusion
Taken together, it seems that chance of seeing abnormal findings that could explain the etiology of first seizure in those patients who did not have any risk factor is notable low.
Acknowledgments
This study was derived from a medical student’s thesis for obtaining a degree in Emergency Medicine (Code No. T5344).
The authors would like to thank the Research Council of Mashhad University of Medical Sciences for supporting the study financially and also the Emergency Dept. staff of Qaem Educational Hospital for their kind cooperation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stafstrom CE, Carmant L. Seizures and epilepsy: an overview for neuroscientists. Cold Spring Harb Perspect Med. 2015;5(6):a022426. doi:10.1101/cshperspect.a022426
2. Garcia J, Rosen G, Mahowald M. Circadian rhythms and circadian rhythm disorders in children and adolescents. Semin Pediatr Neurol. 2001;8(4):229–240. doi:10.1053/spen.2001.29044
3. Bergey GK. Management of a first seizure. Continuum (Minneap, Minn). 2016;22(1 Epilepsy):38–50. doi:10.1212/CON.0000000000000271
4. Kotisaari K, Virtanen P, Forss N, Strbian D, Scheperjans F. Emergency computed tomography in patients with first seizure. Seizure. 2017;48:89–93. doi:10.1016/j.seizure.2017.04.009
5. Sheppard JP, Nguyen T, Alkhalid Y, Beckett JS, Salamon N, Yang I. Risk of brain tumor induction from pediatric head CT procedures: a systematic literature review. Brain Tumor Res Treat. 2018;6(1):1–7. doi:10.14791/btrt.2018.6.e4
6. Wycliffe ND, Holshouser BA, Bartnik-Olson B, Ashwal S. 12 - Pediatric neuroimaging. In: Swaiman KF, Ashwal S, Ferriero DM. et al., editors. Swaiman’s Pediatric Neurology. Elsevier;2017:78–86. doi:10.1016/B978-0-323-37101-8.00012-6
7. Huff JS, Melnick ER, Tomaszewski CA, Thiessen MEW, Jagoda AS, Fesmire FM. Clinical policy: critical issues in the evaluation and management of adult patients presenting to the emergency department with seizures. Ann Emerg Med. 2014;63(4):437–47.e15. doi:10.1016/j.annemergmed.2014.01.018
8. Walls R, Hockberger R, Gausche-Hill M. Rosen’s emergency medicine: concepts and clinical practice. In: Rosen’s Emergency Medicine: Concepts and Clinical Practice. Philadelphia:Elsevier; 2018
9. de la Sayette V, Cosgrove R, Melanson D, Ethier R. CT findings in late-onset epilepsy. Can J Neurol Sci. 1987;14(3):286–289. doi:10.1017/s0317167100026627
10. Khodapanahandeh F, Hadizadeh H. Neuroimaging in children with first afebrile seizures: to order or not to order? Arch Iran Med. 2006;9(2):156–158.
11. Smith AB, Van Hoving DJ, Wallis LA. Emergency centre investigation of first-onset seizures in adults in the Western Cape, South Africa. S Afr Med J. 2013;103(10):723–727. doi:10.7196/samj.6821
12. Kumar R, Navjivan S, Kohli N, Sharma B. Clinical correlates of CT abnormality in generalized childhood epilepsy in India. J Trop Pediatr. 1997;43(4):199–203. doi:10.1093/tropej/43.4.199
13. Arruda WO. Etiology of epilepsy. A prospective study of 210 cases. Arq Neuropsiquiatr. 1991;49(3):251–254. doi:10.1590/s0004-282x1991000300003
14. Yang PJ, Berger PE, Cohen ME, Duffner PK. Computed tomography and childhood seizure disorders. Neurology. 1979;29(8):1084LP- 1084. doi:10.1212/WNL.29.8.1084
15. Longe AC, Omojola MF. Computed tomographic brain scan findings in Saudi epileptic patients. East Afr Med J. 1994;71(9):567–570.
16. Gandon Y, Baraton J, Aicardi J, Goutieres F. [“Efficacy” of the scanography in convulsions and epilepsy in children]. Ann Pediatr (Paris). 1983;30(3):195–200.French.
17. Gordon N. Computed tomography in childhood epilepsy. Arch Dis Child. 1988;63(9):1114. doi:10.1136/adc.63.9.1114
18. Blackmore CC, Mecklenburg RS, Kaplan GS. Effectiveness of clinical decision support in controlling inappropriate imaging. J Am Coll Radiol. 2011;8(1):19–25. doi:10.1016/j.jacr.2010.07.009
19. Hendel RC. Utilization management of cardiovascular imaging pre-certification and appropriateness. JACC Cardiovasc Imaging. 2008;1(2):241–248. doi:10.1016/j.jcmg.2008.01.008
20. Harden CL, Huff JS, Schwartz TH, et al. Reassessment: neuroimaging in the emergency patient presenting with seizure (an evidence-based review). Neurology. 2007;69(18):1772LP- 1780. doi:10.1212/01.wnl.0000285083.25882.0e
21. Novak EM, Terabe F, Nasimoto AL, et al. [Correlation between diagnostic hypothesis and result of cranial computed axial tomography]. Arq Neuropsiquiatr. 2001;59(3–B):761–767.Portuguese.
22. Aloui-Kasbi N, Azzabi O, Bousetta K, et al. [First seizure in children. Exploration strategy]. Tunis Med. 2004;82(12):1091–1096. French.
23. Weber C, Grzyska U, Lehner E, Adam G. [Clinical relevance of cranial CT under emergency conditions–basic neuroradiologic investigations]. Rofo. 2003;175(5):654–662. doi:10.1055/s-2003-39203
24. Bouhadiba Z, Dacher J, Monroc M, Vanhulle C, Menard JF, Kalifa G. [MRI of the brain in the evaluation of children with developmental delay]. J Radiol. 2000;81(8):870–873. French.
25. Shevell M, Ashwal S, Donley D, et al. Practice parameter: evaluation of the child with global developmental delay: report of the quality standards subcommittee of the American Academy of Neurology and the practice committee of the Child Neurology Society. Neurology. 2003;60(3):367–380. doi:10.1212/01.wnl.0000031431.81555.16
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.