")
Back to Journals » Clinical Interventions in Aging » Volume 12
Bone cement distribution in the vertebral body affects chances of recompression after percutaneous vertebroplasty treatment in elderly patients with osteoporotic vertebral compression fractures
Authors Zhang L, Wang Q, Wang L, Shen J, Zhang Q, Sun C
Received 20 May 2016
Accepted for publication 7 July 2016
Published 22 February 2017 Volume 2017:12 Pages 431—436
DOI https://doi.org/10.2147/CIA.S113240
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi-Ying Wu

Liang Zhang, Qiang Wang, Lin Wang, Jian Shen, Qiwei Zhang, Changtai Sun
Department of Orthopedics, Beijing Hospital, National Center of Gerontology, People’s Republic of China
Objective: Percutaneous vertebroplasty (PVP) is a surgical procedure that has been widely used to treat patients suffering from osteoporotic vertebral compression fractures (OVCFs). The procedure involves injection of bone cement into a fractured vertebra. In this study, we investigated whether the distribution of the cement in the vertebral body is related to the occurrence of recompression after surgery.
Patients and methods: A total of 172 patients diagnosed with OVCF, from January 2008 to June 2013, were retrospectively reviewed. Fifty of these patients experienced recompression after surgery during the follow-up period (recompression group), and 122 patients had no recompression observed during the follow-up period (control group). Statistical analysis was performed to compare clinical and operative parameters between these two groups.
Results: Differences were found in bone cement distribution between the recompression group and control group (P=0.001). Patients with bone cement distributed around both upper and lower endplates had a significantly less incidence of recompression (4/50 patients), when compared to other patterns of cement distribution (eg, below upper endplate, above lower endplate, and in the middle of vertebral body). The logistic multiple regression analysis also indicated that patients with bone cement distributed around both the upper and lower endplates had a lower risk of recompression when compared to patients with bone cement distributed in the middle of vertebral body (odds ratio =0.223, P=0.003).
Conclusion: We herein suggest that the control of bone cement distribution during surgery provides beneficial effects on reducing the risks of recompression after PVP treatment in patients with OVCF.
Keywords: elderly, OVCF, PVP, bone cement
Introduction
Osteoporotic vertebral compression fracture (OVCF) is a common condition, especially among elderly population. In the US, ~40% of women at the age group of 80 years old suffer from OVCF. The incidence of OVCF is expected to increase with the growing of aging population.1 Patients with OVCF often experience difficulties in daily activities with their quality of life substantially being reduced. The available treatment options include surgical procedures, such as percutaneous vertebroplasty (PVP) and percutaneous balloon kyphoplasty (PKP). PVP performed under local anesthesia is minimally invasive, and thus is a preferred option for patients older than 80 years.2,3 The procedures of PVP include injection of bone cement, such as polymethyl methacrylate (PMMA), into a fractured vertebral body. This reduces pain and prevents further collapse of the vertebral body. Some patients, however, experience recompression of the PVP-operated vertebrae or new fractures at the neighborhood vertebrae.4 The incidence of subsequent fractures after PVP is not uncommon.5,6 Several reports have suggested that cement volume and distribution in treated vertebral body are potential risk factors for recompression.7–10 The treatment of recompression at the operated vertebrae remains challenging. Therefore, it is important to understand the measures that we can take to prevent recompression. In this study, we compared different clinical and surgical parameters between repression and control groups, and we evaluated whether they are associated with the recompression of the operated vertebrae.
Patients and methods
Patient population
A total of 172 patients were diagnosed with OVCF. These patients received PVP treatment at the Department of Orthopedics, Beijing Hospital, People’s Republic of China, between January 2008 and June 2013. Among these patients, 82 had complete information with mean follow-up times of 29.6 months (range:12–68 months). Patients were divided into two groups according to whether recompression was observed during the follow-up period. The two groups were 1) recompression group (n=50) and 2) control group (no recompression, n=122). The recompression group comprised 29 males and 21 females, with a mean age of 87.08 years. The control group comprised 122 patients (59 males and 63 females), with a mean age of 86.92 years. The preexisting medical conditions of patients included the following: high blood pressure (65 patients), ischemic heart disease (18 patients), atrioventricular block (13 patients), diabetes (32 patients), cerebrovascular diseases (18 patients), chronic obstructive pulmonary diseases (14 patients), and asthma (four patients). This study was approved by the Institutional Review Board of the Ethics Committee of Beijing Hospital. All participants received written and oral information prior to giving written consent, and the study was performed in accordance with the Helsinki II declaration.
Treatment of preexisting medical conditions
Patients in this study were all elderly. Complete examination and assessment of anesthetic risks were performed carefully before surgery. Patients with high blood pressure were given oral antihypertensive drugs to allow blood pressure to return to normal. Patients with symptoms of cardiac dysfunction underwent echocardiography, in which the left ventricular ejection fraction was required to be higher than 55% with no serious structural abnormalities observed in heart chamber and heart valves. Patients with cardiac conduction disturbances were examined using electrocardiogram (ECG); for those with bigamy of premature ventricular contractions, ECG was monitored for further 24 hours to ensure absence of serious heart diseases. For patients with ischemic heart disease, myocardial scintigraphy or computerized tomography (CT) scan on coronary arteries were performed to preclude patients with severe coronary artery stenosis or myocardial ischemia. Patients with prophylactic use of anticoagulants for cardiovascular and cerebrovascular diseases were required to stop taking aspirin for 3 days and oral clopidogrel/warfarin for 1 week before surgery. Routine subcutaneous injection of low-molecular-weight heparin was prohibited 12 hour before surgery; coagulation and platelet aggregation function were examined before surgery. Patients with diabetes continued to use medications, and their fasting blood glucose level was ~8.0 mmol/L and 2 hours postprandial blood glucose <13.0 mmol/L. Patients with COPD and asthma had no report on shortness of breath when in the prone position for 30 minutes. There were 18 patients with cerebrovascular disease; preoperative cranial magnetic resonance imaging examination was performed to ensure no new lesions in 6 months.
Inclusion and exclusion criteria
Inclusion criteria were as follows: 1) age ≥80 years; 2) first single segment OVCF at thoracic or lumbar spine; 3) local anesthesia on single vertebral, PVP being performed using bilateral pedicle puncture technique, with less than 3.0 mL total volume of bone cement injected; 4) patients being conscious and able to communicate clearly and provide ratings; 5) no allergic reactions and cardiac toxicity to bone cement; 6) no leakage of bone cement in the spinal canal; 7) no postoperative complications; and 8) completion of at least 1 year of follow-up and adherence to >80% of the standard anti-osteoporosis medication.
Exclusion criteria were as follows: 1) spinal metastases or history of cancer in combination with OVCF; 2) bone metabolic diseases; 3) damage of posterior wall of the vertebral body; 4) severe degenerative spinal deformities (such as scoliosis and kyphosis); 5) bone mineral density (BMD) less than −5.0; 6) symptoms of nerve root damage before surgery; 7) serious medical complications; 8) previous or concomitant use of hormone; 9) infection at sites of surgery; 10) intervertebral cleft; and 11) PMMA not used as bone cement material.
Clinical presentation and diagnostic imaging
Patients had no signs of trauma or only had a history of minor trauma. They often experienced back or lower back pain, in which the pain relieved in a supine position but worsened in erect stance. The location of the pain could be different from the location of the fractured vertebrae. During the examination of vertebral fractures, pain was experienced in response to percussion. All eligible patients had a detailed medical history and a complete physical examination was performed. Thoracolumbar lateral X-ray, and thoracic and lumbar magnetic resonance imaging scans were performed to rule out other spinal anomalies. Patients were diagnosed with OVCF (fractures of <3 weeks). At follow-up visits, patients were required to take thoracolumbar lateral X-ray.
Surgical technique
Patient was in prone position, with the fractured vertebra region supported. Using C-arm fluoroscopy, the location of fracture was identified. Surgical procedures were performed under local anesthetic with 1% lidocaine. Under guidance of X-ray, the needles were inserted at positions 10 o’clock of the left pedicle and 2 o’clock of the right pedicle at the craniolateral border of the pedicle. The needle was advanced through one-third of the anterior part of the affected vertebral body. The PMMA bone cement was prepared at appropriate viscosity and was injected. The injection process was monitored under lateral fluoroscopy to achieve appropriate filling of the space in the vertebral body. After 24 hours of surgery, patients were allowed to move freely with the aid of a waist protector.
Assessment of recompression
Recompression of the operated vertebral body was assessed through medical history, clinical manifestations, and X-ray imaging. Patients usually had back pain relieved within days after surgery, but later reappeared. X-ray imaging showed a decreased anterior body height at >1.0 mm, an increased Cobb angle >3°, and an increased kyphosis angle in the last follow-up visit when compared to day 1 after surgery.
Imaging analysis
All images were measured and analyzed by the first author of the present study. Thoracic and lumbar X-ray films were taken using digital photography technology and were analyzed using Image-pro plus 5.0 software (Microsoft Corporation, Redmond, WA, USA). The images were measured by the following methods: 1) the degree of vertebral compression – ratio of the height of the anterior vertebral wall to the height of the posterior vertebral wall; 2) the degree of recovery of the compression – changes in the height of the anterior and posterior vertebral walls, before and after surgery; and 3) bone cement distribution pattern – below the upper endplate, above the lower endplate, both the upper and lower endplates, and in the middle of the vertebral body. In the cases of “below the upper endplate”, contact was observed between superior end of the bone cement and the upper endplate. In the cases of “above the lower endplate”, contact was observed between inferior end of the bone cement and the lower endplate. If no contact was observed between the bone cement and upper/lower endplates, the case is classified as “in the middle of the vertebral body”.
Statistical analysis
SPSS 16.0 software (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Categorical data between two groups were analyzed using chi-square test. Continuous data between two groups were compared using Student’s t-test or nonparametric Mann–Whitney U-test. Multivariate logistic regression analysis was performed, in which the clinical characteristics of patients were used as independent variables and occurrence of recompression was used as dependent variables to evaluate the potential risk factors for recompression.
Results
The clinical and surgical parameters are summarized in Table 1. The parameters were compared between recompression and control groups. Bone cement was injected into vertebral body during PVP treatment, and the distribution of cement was classified into four categories: below upper endplate, above lower endplate, both the upper and lower endplates, and in the middle of vertebral body (Figure 1). Differences were found in the pattern of bone cement distribution between the recompression group and control group (P=0.001). The lowest incidence of recompression was observed in patients with bone cement distributed around both upper and lower endplates (8.16%), followed by distribution in the middle of vertebral body only (27.59%), below upper endplate (37.78%), and above upper endplate (42.86%). An X-ray image of a patient who experienced recompression is shown in Figure 2. Other significant differences between recompression and control groups include cement volume (P=0.047) and compression recovery level (P=0.048).
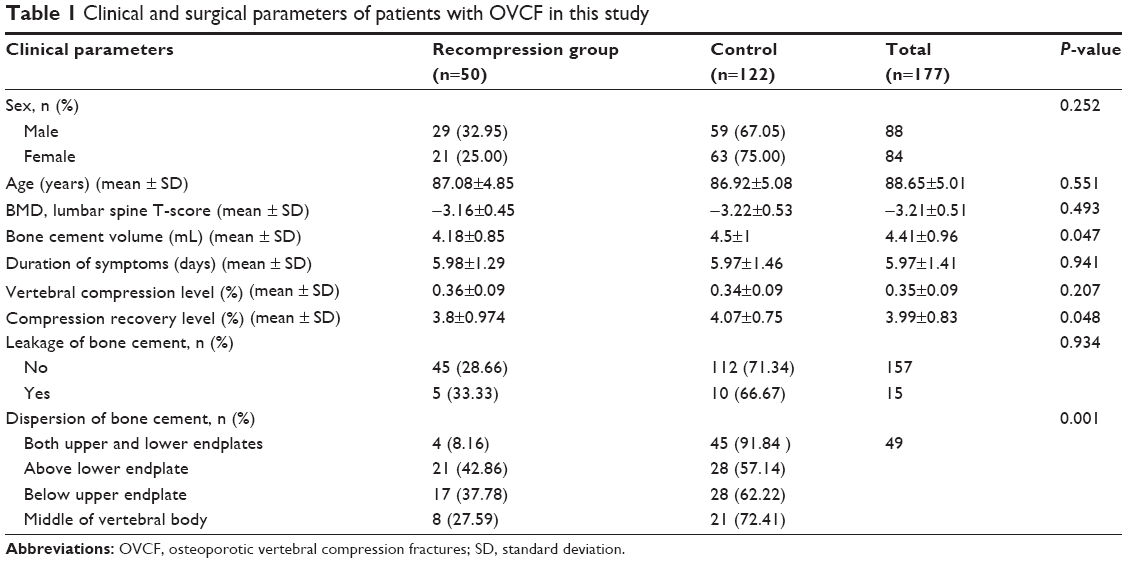 | Table 1 Clinical and surgical parameters of patients with OVCF in this study |
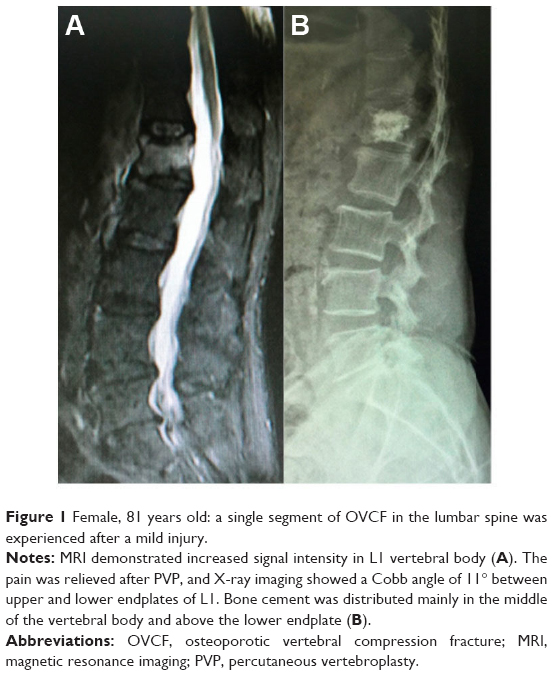 | Figure 1 Female, 81 years old: a single segment of OVCF in the lumbar spine was experienced after a mild injury. |
 | Figure 2 The patient had reappearance of back pain 12 months after surgery, with no obvious risk factor. |
To identify the risk factors associated with the occurrence of recompression, multivariate logistic regression analysis was performed (Table 2). The results indicated that when compared to the patients with bone cement distributed in the middle of vertebral body, lower risk was found in the “both upper and lower endplates” group (odds ratio [OR] =0.233, P=0.003), whereas the “above lower endplate” (OR =2.013, P=0.008) and “below upper endplate” (OR =1.155, P=0.353) groups had higher risk of recompression.
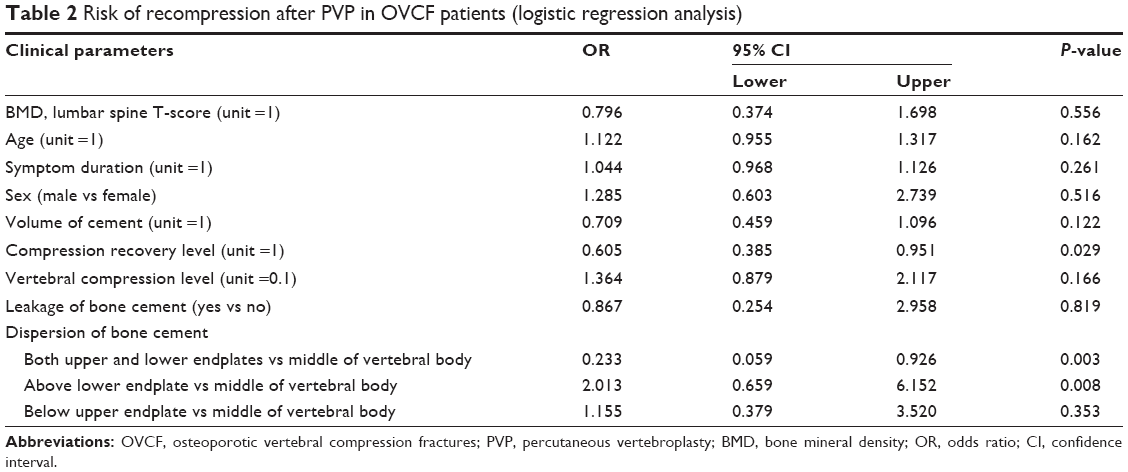 | Table 2 Risk of recompression after PVP in OVCF patients (logistic regression analysis) |
Discussion
There are many factors that contribute to the occurrence of recompression in patients with OVCF after PVP treatment, and the distribution of bone cement is one of the factors that can possibly be controlled by the surgeon. Gaughen et al6 suggested that sufficient filling of bone cement in vertebral body is a key factor associated with recompression. PMMA is the material that has been widely used in PVP treatment. Its distribution pattern is primarily in a solid lump; as such there are areas in the vertebral body that are not supported by PMMA. It has been found that recompression usually occurred at these non-PMMA supported areas.
In the present study, we found that patients with bone cement distributed around both the upper and lower endplates had the lowest rate of experiencing recompression compared to other patterns of bone cement distribution. Further analysis also indicated that cement distribution is a risk factor associated with recompression. We hypothesized that when bone cement is distributed around both the upper and lower endplates, it could provide a better support vertically, since the pressure was applied on both the upper and lower endplates that are harder in nature. When bone cement was distributed in other patterns, the support was relatively less, leading to a higher chance of recompression. A study in cadavers found that distribution of bone cement in PVP surgery was better than in PKP surgery.11 However, even in the PVP group, there were many cases in which the bone cement was not diffused fully.
During PVP procedures, several factors are found to affect the distribution of bone cement. 1) Vertebral body: uneven BMD was usually observed in vertebral body of patients with OVCF. Bone cement fills firstly with the low-density regions followed by high-density regions. If the site of bone cement injection is at the high-density region, it may affect the filling of the bone cement. In addition, if the vertebral body wall remains intact after compression, adequate filling of bone cement in the vertebral body can be achieved. It is also important to ensure that there is no intravertebral cleft; otherwise, it is likely that the bone cement will be distributed in cleft pattern rather than the trabecular pattern.12 The presence of hemangioma or Schmorl’s nodes will also affect the distribution, leading to leakage along the blood vessels or intervertebral disc. We found spinal manipulation could significantly improve the vertebral height, given there was adequate filling of the bone cement that provided support, otherwise, the fracture may worsen. 2) PMMA: cement needs to be injected when it is at the proper viscosity to allow sufficient filling of the cement. 3) Injection techniques: the needle is preferably advanced to one-third of the anterior part of the vertebral body. It is important to ensure the anterior vertebral wall is intact to prevent leakage. If damages of the vertebral body wall were found during CT scans, the PVP procedure should be postponed to allow repairing of the damage. Another method is to have the bone cement injected two times – high viscosity bone cement injected first, followed by low viscosity cement. This method is challenging, given the difficulty in determining the damage of the vertebral body wall and the precise positioning of the needle. Finally, the insertion of two needles may help the filling of cement. The positions could be parallel to the endplates, or one needle advanced toward the upper endplate and another one toward the lower endplate.
Limitations
This study has several limitations. First, two-dimensional X-ray images were used to determine the distribution of bone cement. In these images, fine structures are sometimes difficult to observe due to the overlaying bone cement. For accurate determination of bone cement distribution, three-dimensional CT scans will help. Second, the present study used a criterion, that is, decreased anterior body height of >1.0 mm, to assess the recompression. This criterion is very sensitive, and it is possible that some cases in the recompression group are false positives. Third, the quantification of the degree of contact between the bone cement and upper/lower endplates will provide data for a more comprehensive analysis; however, this will require a larger sample size. Finally, we found the total volume of bone cement injected and the severity of compression before surgery may also affect the dispersion of bone cement, as well as the strength of the vertebrae after surgery. Indeed, studies have shown that the cemented vertebral lead to increased endplate bulge and an altered load transfer in adjacent vertebrae, suggesting the importance of having optimal cement volume.13,14 However, we cannot draw a conclusive relationship between the cement volume and recompression rate due to the limited number of cases investigated.
Conclusion
In conclusion, we found that the distribution pattern of bone cement contributes to the occurrence of recompression in patients with OVCF. Some of the surgical techniques could improve the filling of bone cement in the vertebral body that help reduce the risk of future recompression.
Disclosure
The authors report no conflicts of interest in this work.
References
Old JL, Calvert M. Vertebral compression fractures in the elderly. Am Fam Phys. 2004;69(1):111–116. | ||
Chen LH, Hsieh MK, Liao JC, et al. Repeated percutaneous vertebroplasty for refracture of cemented vertebrae. Arch Orthop Trauma Surg. 2011;131(7):927–933. | ||
Wilke HJ, Mehnert U, Claes LE, Bierschneider MM, Jaksche H, Boszczyk BM. Biomechanical evaluation of vertebroplasty and kyphoplasty with polymethyl methacrylate or calcium phosphate cement under cyclic loading. Spine. 2006;31(25):2934–2941. | ||
Hulme PA, Krebs J, Ferguson SJ, Berlemann U. Vertebroplasty and kyphoplasty: a systematic review of 69 clinical studies. Spine. 2006;31(17):1983–2001. | ||
Heo DH, Chin DK, Yoon YS, Kuh SU. Recollapse of previous vertebral compression fracture after percutaneous vertebroplasty. Osteoporosis Int. 2009;20(3):473–480. | ||
Gaughen JR Jr, Jensen ME, Schweickert PA, Marx WF, Kallmes DF. The therapeutic benefit of repeat percutaneous vertebroplasty at previously treated vertebral levels. AJNR Am J Neuroradiol. 2002;23(10):1657–1661. | ||
Liebschner MA, Rosenberg WS, Keaveny TM. Effects of bone cement volume and distribution on vertebral stiffness after vertebroplasty. Spine. 2001;26(14):1547–1554. | ||
Kim JM, Shin DA, Byun D-H, Kim H-S, Kim S, Kim H-I. Effect of bone cement volume and stiffness on occurrences of adjacent vertebral fractures after vertebroplasty. J Korean Neurosurg Soc. 2012;52(5):435–440. | ||
Sun YC, Teng MM, Yuan WS, et al. Risk of post-vertebroplasty fracture in adjacent vertebral bodies appears correlated with the morphologic extent of bone cement. J Chin Med Assoc. 2011;74(8):357–362. | ||
Molloy S, Mathis JM, Belkoff SM. The effect of vertebral body percentage fill on mechanical behavior during percutaneous vertebroplasty. Spine. 2003;28(14):1549–1554. | ||
Kim MJ, Lindsey DP, Hannibal M, Alamin TF. Vertebroplasty versus kyphoplasty: biomechanical behavior under repetitive loading conditions. Spine. 2006;31(18):2079–2084. | ||
Oka M, Matsusako M, Kobayashi N, Uemura A, Numaguchi Y. Intravertebral cleft sign on fat-suppressed contrast-enhanced MR: correlation with cement distribution pattern on percutaneous vertebroplasty. Academic Radiol. 2005;12(8):992–999. | ||
Polikeit A, Nolte LP, Ferguson SJ. The effect of cement augmentation on the load transfer in an osteoporotic functional spinal unit: finite-element analysis. Spine. 2003;28(10):991–996. | ||
Trout AT, Kallmes DF. Does vertebroplasty cause incident vertebral fractures? A review of available data. AJNR Am J Neuroradiol. 2006;27(7):1397–1403. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.