")
Back to Journals » Cancer Management and Research » Volume 12
BMI May Be a Prognostic Factor for Local Advanced Rectal Cancer Patients Treated with Long-Term Neoadjuvant Chemoradiotherapy
Authors Liu H , Wei R, Li C, Zhao Z, Guan X, Yang M, Liu Z, Wang X, Jiang Z
Received 1 July 2020
Accepted for publication 15 September 2020
Published 20 October 2020 Volume 2020:12 Pages 10321—10332
DOI https://doi.org/10.2147/CMAR.S268928
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Antonella D'Anneo
Hengchang Liu,1,* Ran Wei,1,* Chunxiang Li,2 Zhixun Zhao,1 Xu Guan,1 Ming Yang,1 Zheng Liu,1 Xishan Wang,1 Zheng Jiang1
1Department of Colorectal Surgery, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100021, People’s Republic of China; 2Department of Thoracic Surgery, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100021, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zheng Jiang; Xishan Wang Tel +86-010-88788798
Email [email protected]; [email protected]
Objective: This study aims to develop feasible nomograms to predict the overall survival (OS) and cancer-specific survival (CSS) of the local advanced rectal cancer (LARC) patients who were treated with neoadjuvant chemoradiotherapy (nCRT) and operation.
Methods: A total of 243 LARC patients undergoing nCRT followed by total mesorectal excision (TME) were enrolled. Preoperative clinical features and postoperative pathological characteristics were collected. A Cox regression analysis was performed, and Cox-based nomograms were developed to predict the OS and CSS. We assessed the predictive performance of the nomogram with concordance index and calibration plots.
Results: A total of 243 patients were included with a median follow-up period of 46 months (range from 9 to 86 months). Cox regression analysis showed that low BMI (BMI < 18.5, HR= 21.739, P < 0.05), high level of preoperative CA19-9 (HR = 3.369, P = 0.036), high ypStage (HR = 19.768, P < 0.001), positive neural invasion (HR = 4.218, P = 0.026) and no adjuvant chemotherapy (HR = 5.495, P < 0.001) were independent predictors of poor OS. Age ≥ 70 (HR = 2.284, P < 0.001), low BMI (BMI < 18.5, HR = 3.906, P < 0.05), positive preoperative CA19-9 (HR = 1.920, P = 0.012), high ypStage (HR = 5.147, P < 0.001) and positive neural invasion (HR = 2.873, P = 0.022) were independent predictors of poor CSS. The predictive nomograms were developed to predict the OS and CSS with a C-index of 0.837 and 0.760. Good statistical performance on internal validation was shown by calibration plots.
Conclusion: In conclusion, this study demonstrated that BMI was an independent prognostic factor for OS and CSS in LARC patients treated with nCRT followed TME. A nomogram incorporating BMI, neural invasion, pre-CA19-9, ypStage, age, and adjuvant chemotherapy could be helpful to predict the OS and CSS.
Keywords: local advanced rectal cancer, neoadjuvant chemoradiotherapy, nomogram, body mass index, prognosis, overall survival, cancer-specific survival
Introduction
In order to improve the local control rate of patients with locally advanced rectal cancer (LARC), National Comprehensive Cancer Network (NCCN) guideline recommends that neoadjuvant chemoradiotherapy (nCRT) combined with radical resection is an ideal treatment.1–3 However, LARC patients have a wide range of responses to neoadjuvant therapy, so the survival rate is very heterogeneous.4 At present, the way of predicting the prognosis of LARC patients treated with nCRT is still the same as that of patients with surgery only.5 There are a few studies on the prognosis of LARC patients after nCRT, and most of them are based on AJCC staging, including some improved staging systems, such as T-Plus staging and TNM improved analysis system.6–8 Nevertheless, the disadvantage of these studies is that they only analyze the prognosis of patients from the tumor pathologico-anatomical point of view. Some biological characteristics of patients are ignored, such as body mass index (BMI), family history of cancer, and the level of serum tumor markers and so on. Another prognosis model is based on high-throughput sequencing of blood or tumor tissue, and constructing the model according to the differential expression of genes or proteins.9–11 But there were few overlapped genes or proteins between the results of these studies,12,13 and the results lack of evidence support, so it is difficult to apply them into clinical practice. Moreover, it is too expensive to be suitable for all patients.
Nomogram is a quantitative model to predict the prognosis. It uses the biological characteristics and clinical variables of large samples to calculate a statistical prediction model. This model can calculate the probability of a certain outcome according to the specific clinical and pathological characteristics of patients.14 This study aimed to develop a feasible nomogram to predict the 3- and 5-years overall survival (OS) and cancer-specific survival (CSS) of the LARC patients who were treated with nCRT and curative resection.
Patients and Methods
Patients
A total of 243 LARC patients were consecutively evaluated from our database. These patients were treated with nCRT followed by total mesorectal excision (TME) from Jan 2010 to Jul 2018 in the Department of Colorectal Surgery, Cancer Hospital Chinese Academy of Medical Sciences. The inclusion criteria were as follows: 1) histopathologically confirmed rectal adenocarcinoma; 2) completed long-term nCRT (45~50Gy/25 fraction) followed by TME and post-operative chemotherapy ±; 3) clinical staging was diagnosed based on preoperative MRI and CT examinations. The exclusion criteria were as follows: 1) serum tumor markers were not detected before nCRT; 2) previous or concurrent malignant tumors; 3) after nCRT, distant metastasis were found by imaging examination before an operation.
All the available detailed pre-nCRT clinical characteristic and pathological parameters were collected, including age, gender, smoking history, drinking history, chronic disease, family history of cancer, distance from the tumor inferior margin to the anal verge, the level of carcinoembryonic antigen (CEA) and carbohydrate antigen 19–9 (CA19-9) before nCRT (named pre-CEA and pre-CA19-9), yield pathologic TNM stage (ypStage), Dworak tumor regression grade (TRG), neural invasion, vascular invasion, nCRT-protocol, adjuvant chemotherapy, and the interval of time between nCRT and operation. According to Dworak tumor regression grade, we define TRG-1 and TRG-2 as poor response, TRG-3 and TRG-4 as good response.
Ethical approval was obtained from the ethics committee of our hospital (ID: NCC2016JZ-06).
Treatment
In brief, a total dose of 45–50Gy (1.8–2.0 Gy/fraction) to the whole pelvis in 25 fractions for 5 weeks, plus 5.4 to 9 Gy (1.8 Gy/fraction) to the tumor volume, with 6 to 15 MV energy photons.15 Two schemes of concurrent chemotherapy as follows: (i) capecitabine 1650 mg/m2 daily concurrent with radiotherapy; (ii) oxaliplatin combined with capecitabine (capecitabine 1650 mg/m2, oxaliplatin 130 mg/m2/w). All the patients received TME surgery for at least four weeks after nCRT treatment.16
Follow-Up
All the patients received postoperative reviews every 3 months at our center or local hospital within 2 years, and every 6 months from 3 to 5 years after operation. The postoperative-review examinations included physical examination, peripheral blood tumor markers (eg, CEA, CA19-9), fecal occult blood, chest and abdominal CT, pelvic CT or MRI, and whole-body PET-CT if necessary. Tumor metastasis or recurrence was defined by imaging results or histopathological diagnosis. OS was defined as the time between the date of surgery and the date of death from any cause or the last follow-up. CSS was defined from the date of operation to the date of cancer – related death.
Statistical Analysis
Univariate and multivariate cox regression models were used to identify the factors predicting OS and CSS. Nomograms were constructed based on statistically significant factors identified by the multivariate analysis from the Cox regression model to predict the 3- and 5-years OS and CSS. Kaplan-Meier survival method was used to analyze the 5-years OS and CSS. Log rank tests were employed to assess the statistical significance. Multivariate analyses using Cox proportional hazards models were used to identify the independent prognostic factors for overall survival and cancer-specific survival. Statistical analyses were performed and graphics were created using IBM SPSS Statistics software version 25.0 (IBM Corporation, Armonk, NY, USA). The nomogram analysis was conducted using R version 3.6.3 (https://www.rproject.org/). Statistical significance was set at a two-sided P-value <0.05.
Results
Patient Characteristics
A total of 243 patients were assessed for our study, including 166 males and 77 females. The range of age is from 23 to 82, and the median age is 55 years old. The BMI is (23.8 ± 3.3) kg/m2. The mean distance from the tumor inferior margin to the anal verge is 4.57 cm. With a median follow-up period of 46 months (range from 9 to 86 months). For details see Table 1.
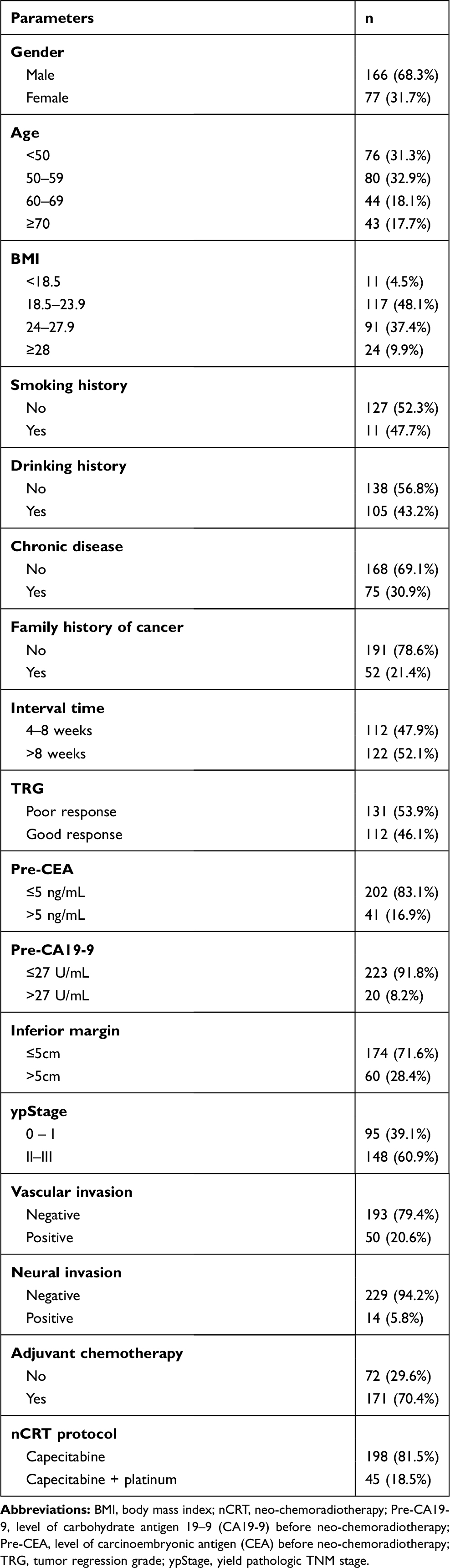 |
Table 1 Baseline Clinicopathological Characteristics in Patients |
Univariate and Multivariate Analysis of Prognostic Factors for OS and CSS
Univariate analysis was performed on all the variables, BMI, pre-CA19-9, ypStage, vascular invasion, neural invasion and adjuvant chemotherapy were independently associated with OS in LARC patients treated with nCRT and curative resection. Multivariate Cox regression analysis was performed using the significant prognostic factors identified in univariate analysis. We found that BMI (BMI < 18.5, HR= 21.739, P < 0.05), pre-CA19-9 (pre-CA19-9 ≥ 27, HR = 3.369, P = 0.036), ypStage (ypStage = II–III, HR = 19.768, P < 0.001), neural invasion (HR = 4.218, P = 0.026) and no adjuvant chemotherapy (HR = 5.495, P < 0.001) were independent predictors of poor OS. Detailed in Table 2.
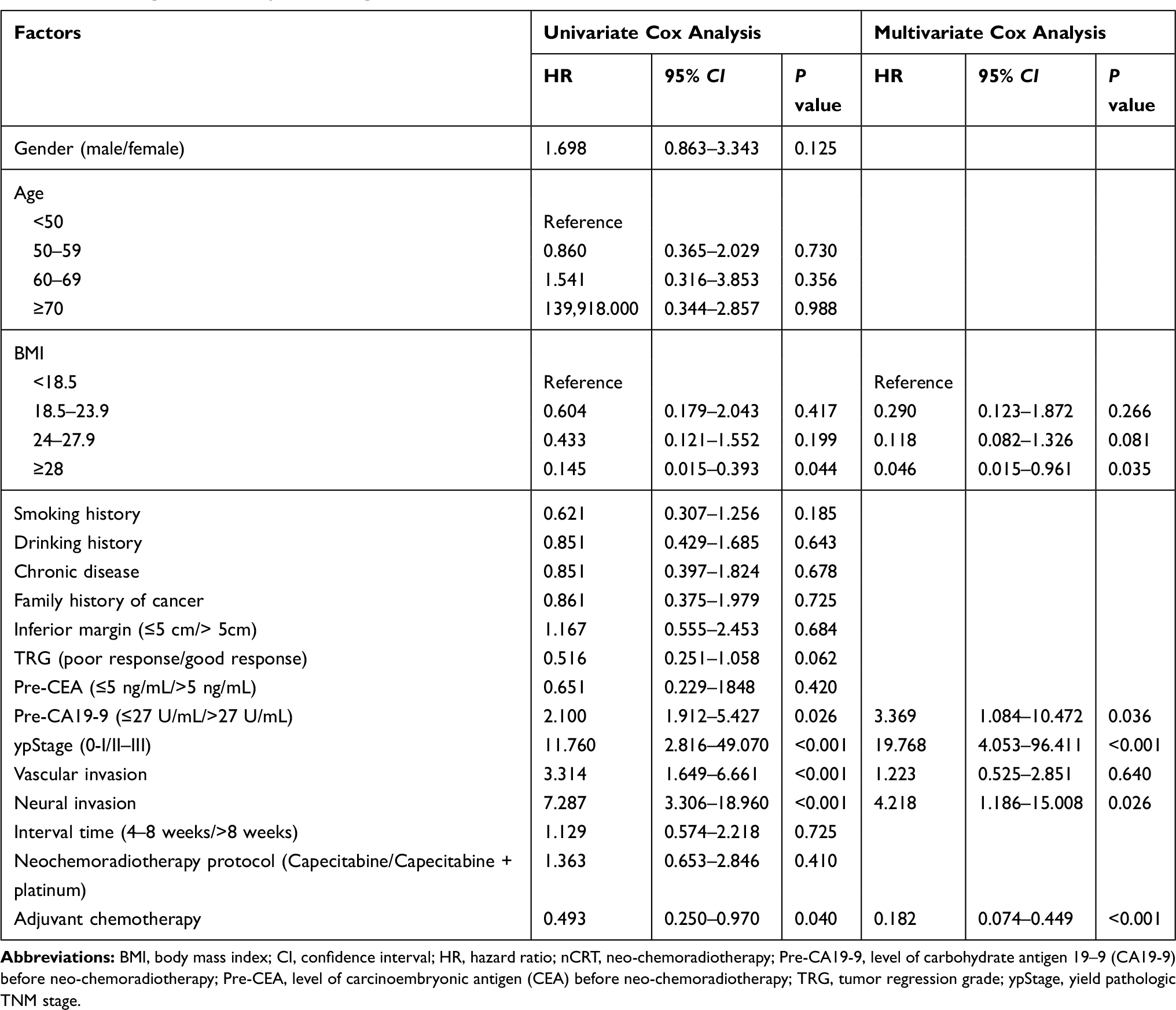 |
Table 2 Cox Regression Analysis of Prognostic Factors for OS |
Table 3 lists the results of univariate analysis of the prognostic factors for CSS. Age, BMI, TRG, pre-CA19-9, ypStage, vascular invasion and neural invasion were prognostic factors for CSS. All significant parameters in the univariate analysis were entered into the multivariable analysis based on the Cox regression. Age (Age ≥70, HR = 2.2844, P <0.05), BMI (BMI < 18.5, HR = 3.906, P < 0.05), pre-CA19-9 (HR = 1.920, P = 0.012), ypStage (HR = 5.147, P <0.001) and neural invasion (HR = 2.873, P = 0.022) were independent predictors of poor CSS.
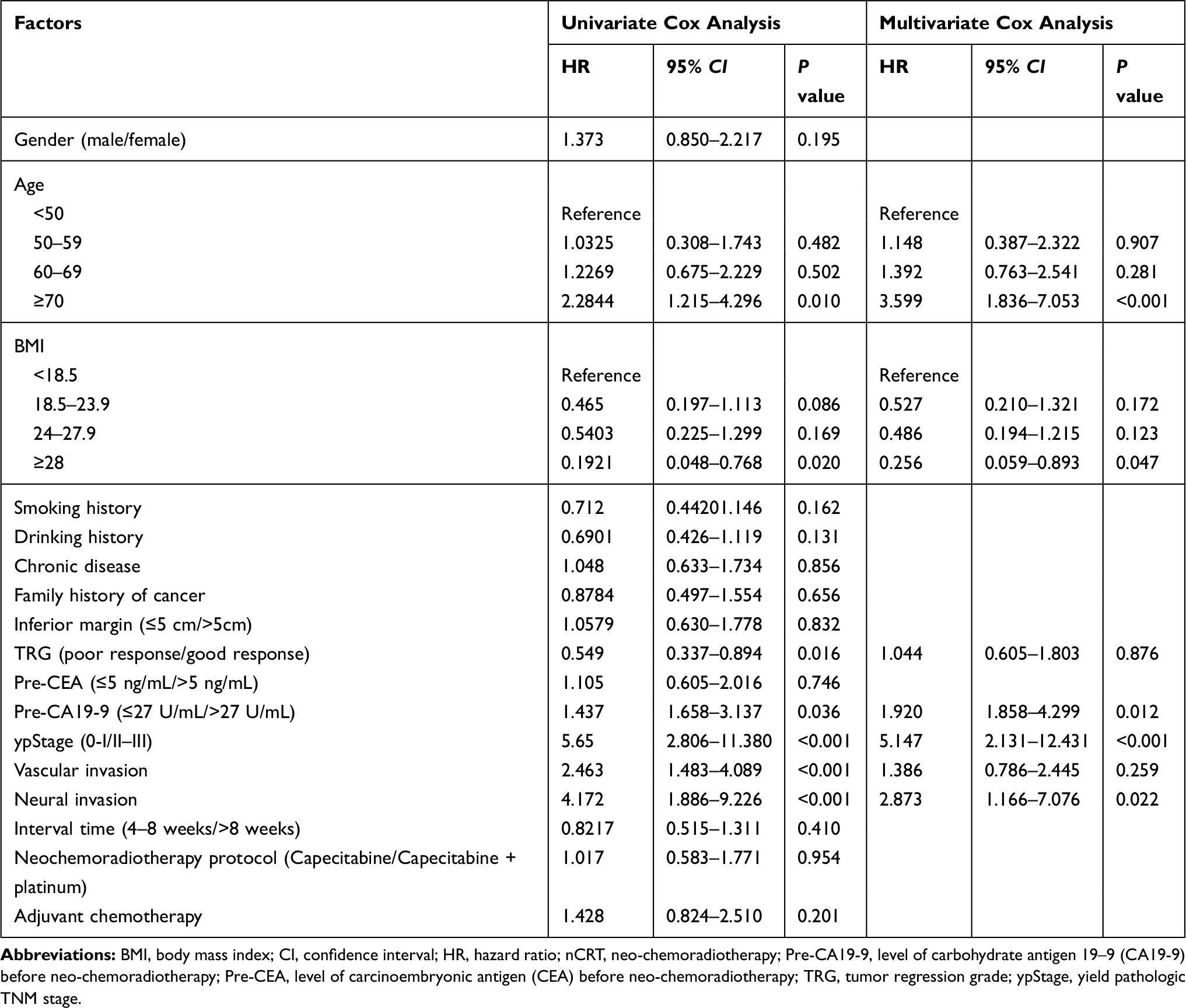 |
Table 3 Cox Regression Analysis of Prognostic Factors for CSS |
Construction of a Nomogram to Predict OS and CSS
We established a nomogram for quantitative prediction of OS (Figure 1A) and CSS (Figure 1B) in LARC patients who received nCRT and TME based on Cox regression analysis results. A total of 5 variables were included. In addition to the 4 same variables such as BMI, neural invasion, pre-CA19-9, and ypStage, there are some subtle differences between the two nomograms. Adjuvant chemotherapy has a major impact on OS, but little effect on CSS. We found that the patients aged ≥70 have a higher risk of tumor recurrence after treatment than other age groups.
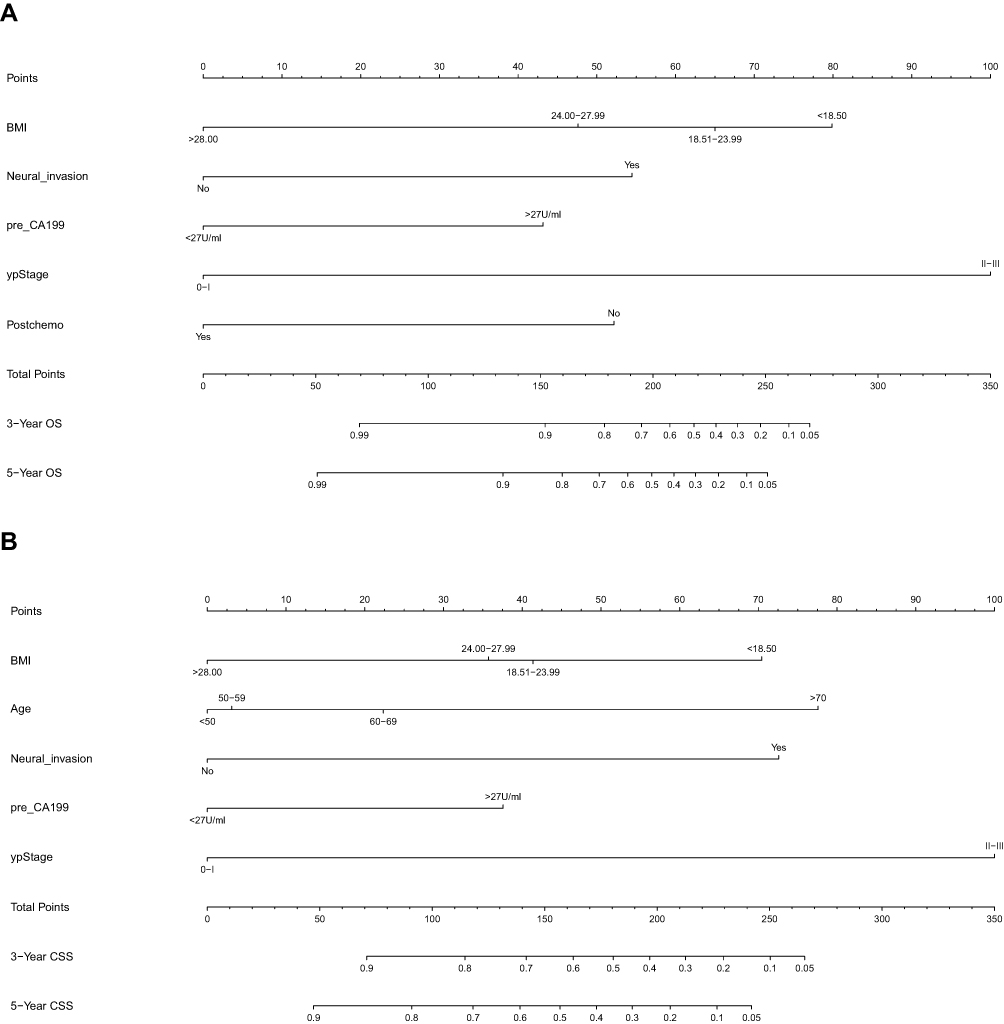 |
Figure 1 Nomograms for predicting 5-years OS (A) and CSS (B) of patients with LARC treated by nCRT and curative resection. |
Calibration of the Nomogram
Bothnomograms were further validated internally using 2000 bootstrapping resamples. The C-index of the OS and CSS nomograms are 0.837 and 0.760, respectively. The calibration plots demonstrated satisfactory statistical performance upon internal validation between the nomogram prediction and actual observation for the probability of 3- (Figure 2A) and 5-years (Figure 2B) OS, and 3- (Figure 2C) and 5-years (Figure 2D) CSS in internal validation cohort.
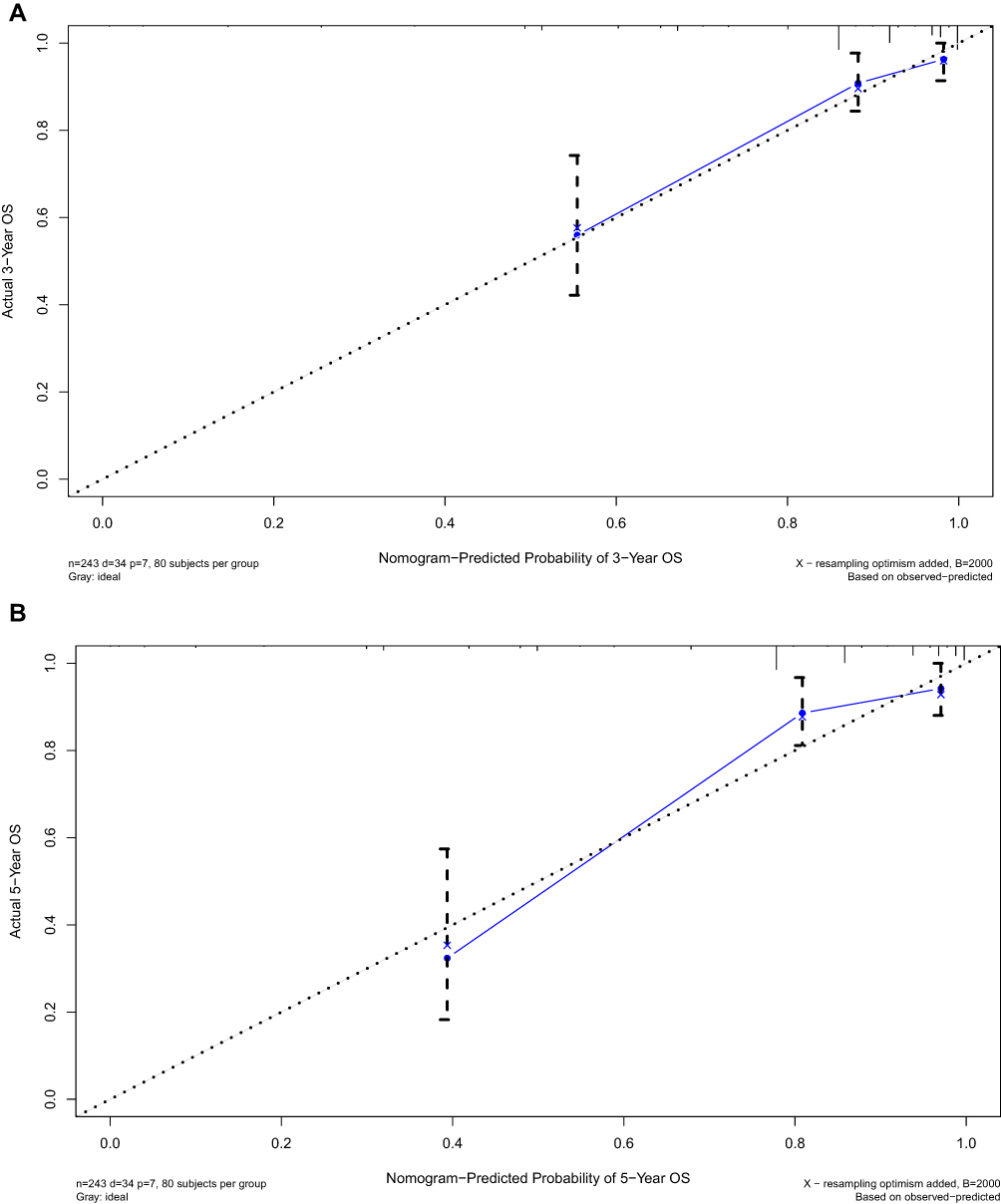 |
Figure 2 Continued. |
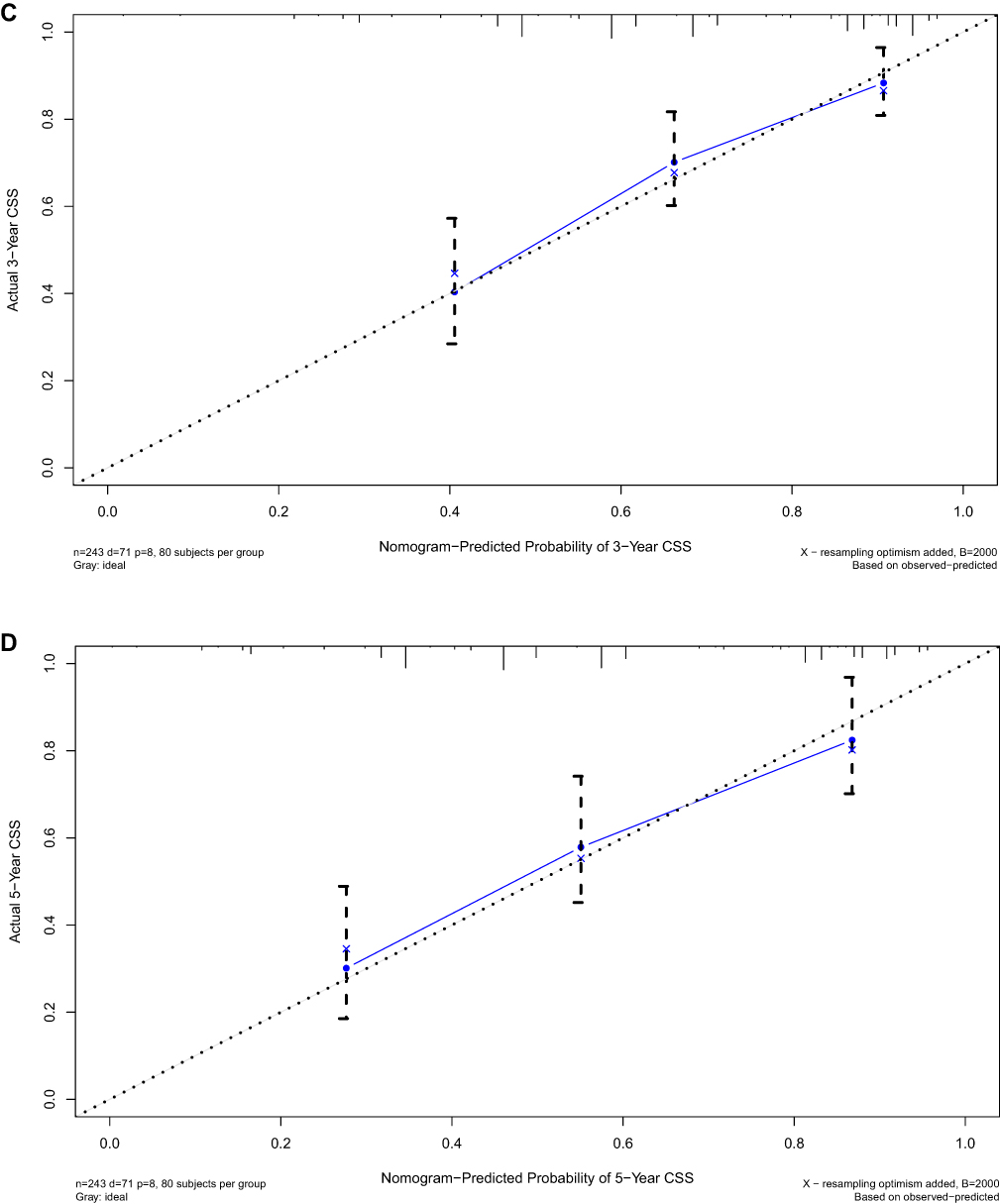 |
Figure 2 Calibration plots for 3- (A) and 5-years (B) OS and 3- (C) and 5-years (D) CSS in internal validation cohort. |
Prognosis Value of BMI
In Cox regression analysis, we found that BMI may be related to OS and CSS of LARC patients treated with nCRT. Higher BMI was associated with a higher probability of 5-years OS (Figure 3A) and CSS (Figure 3B). Although only when BMI ≥ 28, its 5-year OS and CSS were significantly higher than BMI < 18.5 (P = 0.042 and 0.014), there is a trend that the higher BMI the better OS and CSS for patients.
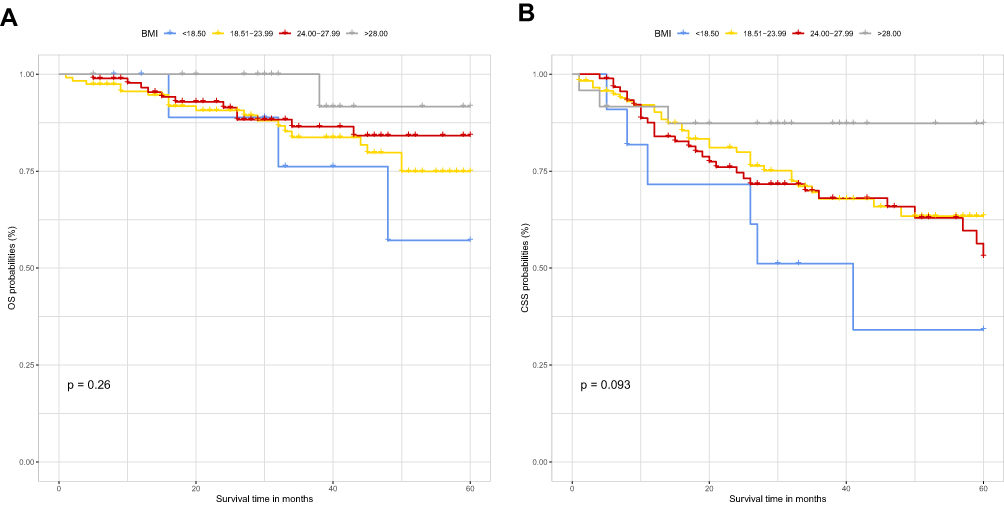 |
Figure 3 Kaplan–Meier curves showed higher BMI was associated with a higher probability of 5-years OS (A) and CSS (B). |
Discussion
NCCN guideline has recommended nCRT followed by TME as a standard care approach for patients with LARC.17 Although this treatment can improve the local control rate of tumors, there are still great differences in prognosis among patients.18,19 However, to the best of our knowledge, there are few studies on the prognosis of these patients. Most studies focused on tumor characteristics, but ignored the characteristics of patients themselves.20–22
This study included a large number of LARC patients with clinical history and tumor characteristics. The univariate analysis implies that BMI < 18.50, positive pre-CA19-9, higher ypStage, positive vascular and neural invasion, and no adjuvant chemotherapy were associated with a lower rate of overall survival. Patients aged ≥70, BMI < 18.50, lower TRG (TRG-1 and TRG-2), positive pre-CA19-9, higher ypStage, positive vascular invasion, and neural invasion were associated with a lower rate of cancer-specific survival. We built the nomograms for predicting 3- and 5-years OS and CSS. In these nomograms, we demonstrated that BMI, neural invasion, pre-CA19-9, ypStage, and adjuvant chemotherapy have been integrated to predict OS. And age, BMI, neural invasion, pre-CA19-9, and pStage to predict CSS.
Besides pathological TNM stage is a well-known predictor of prognosis, our study has also found several factors. Correlation of CA19-9 but not CEA as a serum biomarker of OS and CSS. These two serum biomarkers are mainly used to monitor the recurrence of the tumor during the re-examination after finishing the whole treatment.23 If the level of CA19-9 increases after nCRT, it indicates that patients will have worse OS and DFS.24 The results of previous studies showed that the level of CA19-9 before treatment could predict whether patients could benefit from nCRT.25,26 In this study, 15 of 20 patients who had a positive CA19-9 before nCRT have no down-staging after nCRT, which is consistent with the above conclusion. It also suggests that we should pay more attention to the significance of CA19-9 in the prognosis and monitoring of rectal cancer. However, the number of CA19-9 positive patients before treatment in this study was small, which needs further confirmation by expanding the sample size.
The neural invasion (NI) prevalence and neural invasion severity strongly vary within gastrointestinal malignancies.27 There were 14 patients (5.98%) with NI in this study, which is lower than the previous study.28 However, most studies demonstrated that neural invasion not only increases the risk of tumor recurrence, but also lead to a poor response to nCRT.28–30 In current clinical practice, neural invasion is considered to be one of the conditions for adjuvant chemotherapy. In our patient cohort, 4 of 14 patients had not received adjuvant chemotherapy, and recurrence occurred in 3 patients (75%), the earliest tumor recurrence occurred at two months after surgery, and all 3 patients had passed away when we did the survival analysis. In the present study, we found neural invasion had a negative correlation with both OS and CSS, indicating that it was a prognostic factor of LARC patients treated with nCRT.
Interestingly, BMI might have a negative correlation with the prognosis. In our study, the patients whose BMI more than 28.0 had the best OS and CSS. It seems to become a common sense that obesity means a high risk of cancer.31,32 However, the relationship between high BMI and prognosis seems to be controversial. Sweigert et al showed a positive correlation between obesity and the incidence of postoperative complications.33 Several studies had also found that higher BMI may be related to a better prognosis of rectal cancer.34–36 And other studies demonstrated that BMI does not seem to be related to prognosis or even contrary.36–38
Visceral fat area (VFA) and skeletal muscle area (SMA) are two obesity-associated parameters.39 They can assess the role of fat in the treatment in more detail. Visceral obesity (VO) was considered as a metabolic risk factor that negatively impacts surgical outcome in colon cancer.40 At present, VO is thought to be related to the incidence of postoperative complications and poor prognosis.41–44 But this is a controversial view.45,46 In our study, the patients were divided into four groups according to BMI. Although only patients with BMI ≥ 28.0 had significantly higher OS and CSS than patients with BMI < 18.5, the disadvantage of this study is that the proportion of the two groups in the patients’ cohort is relatively small, which is 4.5% (BMI < 18.5) and 9.9% (BMI ≥ 28.0) respectively. However, we can find a trend that the higher BMI the better prognosis. The reason might be that the change of SMA in the course of nCRT is little and the decrease of SMA content may have an adverse effect on the prognosis.47,48 Some studies even found that SMA increased after treatment with nCRT.41 Although our study did not measure VFA and SMA in patients, this issue is still worthy of further study.
There were still several shortcomings in our study. First, this is a single-center retrospective study, and these findings should be corroborated by multi-center prospective studies. Second, only 24 patients with BMI ≥ 28.0, it is impossible to confirm whether or not in obese patients, the higher the BMI, the better the prognosis. A range of BMI should be clearly defined to explore the significance in survival.
In conclusion, the present study demonstrated that BMI was an independent prognostic factor for LARC patients treated with nCRT, and nomograms incorporating clinical characteristics we built could be helpful to predict the survival outcome.
Ethical Approval Statement
Our study was approved by Cancer Hospital, Chinese Academy of Medical Sciences; National GCP Center for Anticancer Drugs; The Independent Ethics Committee (approval no. NCC2016JZ-06). All patients were informed of the purpose of the study at follow-up and received oral consent. Ethics committee approved the verbal informed consent process, and that this study was conducted in accordance with the Declaration of Helsinki.
Funding
The authors wish to thank all the patients enrolled in this study. This work was supported by National Key R&D Program of China (2018YFC1315000/2018YFC1315005), National Natural Science Foundation of China (81572930), Beijing Science and Technology Program (D17110002617004), Non-profit Central Research Institute Fund of Chinese Academy of Medical Sciences (2018PT32012), CAMS Innovation Fund for Medical Sciences (CIFMS) (2019-I2M-2-002).
Disclosure
All authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. These authors contributed equally: Hengchang Liu and Ran Wei.
References
1. Roh MS, Colangelo LH, O’Connell MJ, et al. Preoperative multimodality therapy improves disease-free survival in patients with carcinoma of the rectum: NSABP R-03. J Clin Oncol. 2009;27(31):5124–5130. doi:10.1200/JCO.2009.22.0467
2. van Gijn W, Marijnen CA, Nagtegaal ID, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomized controlled TME trial. Lancet Oncol. 2011;12(6):575–582. doi:10.1016/S1470-2045(11)70097-3
3. Sauer R, Liersch T, Merkel S, et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized Phase III trial after a median follow-up of 11 years. J Clin Oncol. 2012;39(16):1926–1933. doi:10.1200/JCO.2011.40.1836
4. Kong JC, Guerra GR, Warrier SK, et al. Prognostic value of tumour regression grade in locally advanced rectal cancer: a systematic review and meta-analysis. Colorectal Dis. 2018;20(7):574–585. doi:10.1111/codi.14106
5. Wei J, Huang R, Guo S, et al. ypTNM category combined with AJCC tumor regression grade for screening patients with the worst prognosis after neoadjuvant chemoradiation therapy for locally advanced rectal cancer. Cancer Manag Res. 2018;10:5219–5225. doi:10.2147/CMAR.S179151
6. Li J, Yi CH, Hu YT, et al. TNM staging of colorectal cancer should be reconsidered according to weighting of the T stage: verification based on a 25-year follow-up. Medicine (Baltimore). 2016;95(6):e2711. doi:10.1097/MD.0000000000002711
7. Gunderson LL, Jessup JM, Sargent DJ, et al. Revised TN categorization for colon cancer based on national survival outcomes data. J Clin Oncol. 2010;28(2):264–271.
8. Hashiguchi Y, Hase K, Kotake K, et al. Evaluation of the seventh edition of the tumour, node, metastasis (TNM) classification for colon cancer in two nationwide registries of the United States and Japan. Colorectal Dis. 2012;14(9):1065–1074. doi:10.1111/j.1463-1318.2011.02917.x
9. Ji D, Yi H, Zhang D, et al. Somatic mutations and immune alternation in rectal cancer following neoadjuvant chemoradiotherapy. Cancer Immunol Res. 2018;6(11):1401–1416. doi:10.1158/2326-6066.CIR-17-0630
10. Lee IH, Kang K, Kang BW, et al. Genetic variations using whole-exome sequencing might predict response for neoadjuvant chemoradiotherapy in locally advanced rectal cancer. Med Oncol. 2018;35(11):145. doi:10.1007/s12032-018-1202-8
11. Tweedle EM, Khattak I, Ang CW, et al. Low molecular weight heat shock protein HSP27 is a prognostic indicator in rectal cancer but not colon cancer. Gut. 2010;59(11):1501–1510. doi:10.1136/gut.2009.196626
12. Ryan JE, Warrier SK, Lynch AC, et al. Predicting pathological complete response to neoadjuvant chemoradiotherapy in locally advanced rectal cancer: a systematic review. Colorectal Dis. 2016;18(3):234–246. doi:10.1111/codi.13207
13. Redalen KR, Sitter B, Bathen TF, et al. High tumor glycine concentration is an adverse prognostic factor in locally advanced rectal cancer. Radiother Oncol. 2016;118(2):393–398.
14. Balachandran VP, Gonen M, Smith JJ, et al. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16(4):e173–180. doi:10.1016/S1470-2045(14)71116-7
15. Roels S, Duthoy W, Haustermans K, et al. Definition and delineation of the clinical target volume for rectal cancer. Int J Radiat Oncol Biol Phys. 2006;65(4):1129–1142. doi:10.1016/j.ijrobp.2006.02.050
16. Deng X, Liu P, Jiang D, et al. Neoadjuvant radiotherapy versus surgery alone for stage II/III mid-low rectal cancer with or without high-risk factors: a prospective multicenter stratified randomized trial. Ann Surg. 2019. doi:10.1097/SLA.0000000000003649
17. Benson AB
18. Keller DS, Berho M, Perez RO, et al. The multidisciplinary management of rectal cancer. Nat Rev Gastroenterol Hepatol. 2020.
19. Huang MY, Huang CW, Wang JY. Surgical treatment following neoadjuvant chemoradiotherapy in locally advanced rectal cancer. Kaohsiung J Med Sci. 2020;36(3):152–159. doi:10.1002/kjm2.12161
20. Sun Y, Huang Z, Chi P. An inflammation index-based prediction of treatment response to neoadjuvant chemoradiotherapy for rectal mucinous adenocarcinoma. Int J Clin Oncol. 2020.
21. Sun Y, Zhang Y, Huang Z, et al. Prognostic implication of negative lymph node count in ypn+ rectal cancer after neoadjuvant chemoradiotherapy and construction of a prediction nomogram. J Gastrointest Surg. 2019;23(5):1006–1014. doi:10.1007/s11605-018-3942-3
22. Sun Y, Zhang Y, Wu X, et al. Prognostic significance of neoadjuvant rectal score in locally advanced rectal cancer after neoadjuvant chemoradiotherapy and construction of a prediction model. J Surg Oncol. 2018;117(4):737–744. doi:10.1002/jso.24907
23. Gao XH, Yu GY, Gong HF, et al. Differences of protein expression profiles, KRAS and BRAF mutation, and prognosis in right-sided colon, left-sided colon and rectal cancer. Sci Rep. 2017;7(1):7882. doi:10.1038/s41598-017-08413-z
24. Zhang LN, OuYang PY, Xiao WW, et al. Elevated CA19-9 as the most significant prognostic factor in locally advanced rectal cancer following neoadjuvant chemoradiotherapy. Medicine (Baltimore). 2015;94(45):e1793. doi:10.1097/MD.0000000000001793
25. Yılmaz Rakıcı S, Bedir R, Hatipoğlu C. Are there predictors that can determine neoadjuvant treatment responses in rectal cancer? Turk J Gastroenterol. 2019;30(3):220–227. doi:10.5152/tjg.2018.18179
26. Song J, Huang X, Chen Z, et al. Predictive value of carcinoembryonic antigen and carbohydrate antigen 19-9 related to downstaging to stage 0-I after neoadjuvant chemoradiotherapy in locally advanced rectal cancer. Cancer Manag Res. 2018;10:3101–3108. doi:10.2147/CMAR.S166417
27. Liebl F, Demir IE, Mayer K, et al. The impact of neural invasion severity in gastrointestinal malignancies: a clinicopathological study. Ann Surg. 2014;260(5):900–907. doi:10.1097/SLA.0000000000000968
28. Nikberg M, Chabok A, Letocha H, et al. Lymphovascular and perineural invasion in stage II rectal cancer: a report from the Swedish colorectal cancer registry. Acta Oncol. 2016;55(12):1418–1424. doi:10.1080/0284186X.2016.1230274
29. Peng J, Sheng W, Huang D, et al. Perineural invasion in pT3N0 rectal cancer: the incidence and its prognostic effect. Cancer. 2011;117(7):1415–1421. doi:10.1002/cncr.25620
30. Bacha D, Talbi G, Ben Slama S, et al. Predictive factors for histological response to neo-adjuvant treatment in rectal cancers. Tunis Med. 2019;97(11):1284–1290.
31. Renehan AG, Tyson M, Egger M, et al. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet. 2008;371(9612):569–578. doi:10.1016/S0140-6736(08)60269-X
32. Garcia H, Song M. Early-life obesity and adulthood colorectal cancer risk: a meta-analysis. Rev Panam Salud Publica. 2019;43:e3. doi:10.26633/RPSP.2019.3
33. Sweigert PJ, Chen C, Fahmy JN, et al. Association of obesity with postoperative outcomes after proctectomy. Am J Surg. 2020;
34. Abdel-Rahman O. Effect of body mass index on 5-FU-based chemotherapy toxicity and efficacy among patients with metastatic colorectal cancer; a pooled analysis of 5 randomized trials. Clin Colorectal Cancer. 2019;18(4):e385–e393. doi:10.1016/j.clcc.2019.07.005
35. Kalb M, Langheinrich MC, Merkel S, et al. Influence of body mass index on long-term outcome in patients with rectal cancer – a single centre experience. Cancers (Basel). 2019;11(5):E609. doi:10.3390/cancers11050609
36. Shahjehan F, Merchea A, Cochuyt JJ, et al. Body mass index and long-term outcomes in patients with colorectal cancer. Front Oncol. 2018;8:620. doi:10.3389/fonc.2018.00620
37. Zhang X, Wu Q, Gu C, et al. The effect of increased body mass index values on surgical outcomes after radical resection for low rectal cancer. Surg Today. 2019;49(5):401–409. doi:10.1007/s00595-019-01778-w
38. Lino-Silva LS, Aguilar-Cruz E, Salcedo-Hernández RA, et al. Overweight but not obesity is associated with decreased survival in rectal cancer. Contemp Oncol (Pozn). 2018;22(3):158–164.
39. Clark W, Siegel EM, Chen YA, et al. Quantitative measures of visceral adiposity and body mass index in predicting rectal cancer outcomes after neoadjuvant chemoradiation. J Am Coll Surg. 2013;216(6):1070–1081. doi:10.1016/j.jamcollsurg.2013.01.007
40. Rickles AS, Iannuzzi JC, Mironov O, et al. Visceral obesity and colorectal cancer: are we missing the boat with BMI? J Gastrointest Surg. 2013;17(1):133–143. doi:10.1007/s11605-012-2045-9
41. Heus C, Cakir H, Lak A, et al. Visceral obesity, muscle mass and outcome in rectal cancer surgery after neo-adjuvant chemo-radiation. Int J Surg. 2016;29:159–164. doi:10.1016/j.ijsu.2016.03.066
42. Goulart A, Malheiro N, Rios H, et al. Influence of visceral fat in the outcomes of colorectal cancer. Dig Surg. 2019;36(1):33–40. doi:10.1159/000486143
43. Lee KH, Kang BK, Ahn BK. Higher visceral fat area/subcutaneous fat area ratio measured by computed tomography is associated with recurrence and poor survival in patients with mid and low rectal cancers. Int J Colorectal Dis. 2018;33(9):1303–1307. doi:10.1007/s00384-018-3065-z
44. Zhou CJ, Cheng YF, Xie LZ. Metabolic syndrome, as defined based on parameters including visceral fat area, predicts complications after surgery for rectal cancer. Obes Surg. 2020;30(1):319–326. doi:10.1007/s11695-019-04163-1
45. Tokunaga R, Nakagawa S, Miyamoto Y, et al. The clinical impact of preoperative body composition differs between male and female colorectal cancer patients. Colorectal Dis. 2020;22(1):62–70. doi:10.1111/codi.14793
46. Yu H, Joh YG, Son GM, et al. Distribution and impact of the visceral fat area in patients with colorectal cancer. Ann Coloproctol. 2016;32(1):20–26. doi:10.3393/ac.2016.32.1.20
47. De Nardi P, Salandini M, Chiari D, et al. Changes in body composition during neoadjuvant therapy can affect prognosis in rectal cancer patients: an exploratory study. Curr Probl Cancer. 2019;100510.
48. Takeda Y, Akiyoshi T, Matsueda K, et al. Skeletal muscle loss is an independent negative prognostic factor in patients with advanced lower rectal cancer treated with neoadjuvant chemoradiotherapy. PLoS One. 2018;13(4):e0195406. doi:10.1371/journal.pone.0195406
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.