")
Back to Journals » Patient Preference and Adherence » Volume 15
Blood Pressure Control and Adherence to Drug Treatment in Patients with Hypertension Treated at a Specialized Outpatient Clinic: A Cross-Sectional Study
Authors Guimarães MCLP , Coelho JC, Silva GV, Drager LF, Gengo e Silva Butcher RDC, Butcher HK , Pierin AMG
Received 1 September 2021
Accepted for publication 21 October 2021
Published 10 December 2021 Volume 2021:15 Pages 2749—2761
DOI https://doi.org/10.2147/PPA.S336524
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Mayra Cristina da Luz Pádua Guimarães,1 Juliana Chaves Coelho,1 Giovanio Vieira da Silva,2 Luciano Ferreira Drager,2,3 Rita de Cassia Gengo e Silva Butcher,1 Howard K Butcher,4 Angela Maria Geraldo Pierin1
1Graduate Program in Adult Health Nursing (PROESA), University of São Paulo Nursing School, São Paulo, SP, Brazil; 2Hypertension Unit, Renal Division, University of São Paulo Medical School, São Paulo, SP, Brazil; 3Hypertension Unit, Heart Institute (InCor), University of Sao Paulo Medical School, São Paulo, SP, Brazil; 4Christine E. Lynn College of Nursing, Florida Atlantic University, Boca Raton, FL, USA
Correspondence: Mayra Cristina da Luz Pádua Guimarães
Graduate Program in Adult Health Nursing (PROESA), University of São Paulo Nursing School, São Paulo, SP, Brazil
Email [email protected]
Objective: To evaluate and identify variables associated with the control of hypertension and adherence to antihypertensive drug treatment in a group of patients with hypertension monitored in a specialized, highly complex outpatient service.
Methods: A prospective, cross-sectional study was carried out in the hypertension unit of a tertiary teaching hospital. Patients diagnosed with hypertensive aged 18 years and over and accompanied for at least six months were included in the study. Patients with secondary hypertension and pregnant women were excluded. The sample consisted of 253 patients. Adherence/concordance to antihypertensive treatment was assessed using the Morisky Green Levine Scale. Blood pressure control was set for values less than 140/90 mmHg. Variables with p≤ 0.20 in univariate analysis were included in multiple logistic regression. The level of significance adopted was p ≤ 0.05.
Results: Most of patients were white, married and women, with a mean age of 65 (13.3) years old, low income, and education levels. Blood pressure control and adherence were observed in 69.2% and 90.1% of the patients, respectively. Variables that were independently associated with blood pressure control were (OR, odds ratio; CI, 95% confidence interval): married marital status (OR 2.3; CI 1.34– 4.28), use of calcium channel blockers (OR 0.4; CI 0.19– 0.92) and number of prescribed antihypertensive drugs (OR 0.78; CI 0.66– 0.92). Adherence was not associated with any of the variables studied.
Conclusion: There was a high frequency of patients with satisfactory adherence to antihypertensive drug treatment. Blood pressure control was less frequent and was associated with social and treatment-related factors.
Keywords: hypertension, control, adherence, pharmacological treatment
Introduction
Hypertension is a chronic cardiovascular disease which affects as many as 1.39 billion people globally.1 Hypertension is the main risk factor for cardiovascular disease and mortality worldwide.2,3 The prevalence of hypertension has increased in several countries over the years, with a global increase from 25.9% in 2000 to 31.1% in 2010,4 being higher in low and middle-income countries (31.5%) than in high-income countries (28.5%). In Brazil, the scenario is similar and hypertension affects about 31%5 of adult individuals and more than 60% of the elderly.6
Despite the robust evidence on the positive impact on cardiovascular morbidity and mortality, and on the reduction of lesions in target organs when blood pressure is reduced,7 control rates of hypertension are still unsatisfactory, even in high-income countries. In low and middle-income countries, the scenario seems to be even worse.8 The Prospective Urban Rural Epidemiology (PURE) study sought to assess this variability and blood pressure control rates found in low, medium-low, medium-high, and high-income countries were only 12.7%, 9.9%, 15.6%, and 19.0%, respectively.9 An observational study10 evaluated control rates in several regions of Brazil, with the objective of identifying this estimate in a middle-income country and almost half (46.4%) of persons with hypertension were outside the control target.
Effective control of blood pressure is the main objective of the treatment of hypertension.11 However, several factors influence this control, such as therapeutic inertia, the complexity of the individual, the socioeconomic and education level, access to unstructured health services/health systems, and adherence to treatment, which is certainly one of the most important factors.12–15 The World Health Organization (WHO) has defined adherence as
the degree to which a person’s behavior - taking the medication, following a diet and/or making lifestyle changes - corresponds to the recommendations agreed on with a healthcare provider/practitioner.16
In another document on the subject, adherence was defined as a process characterized by three major components: Initiation, Implementation and Discontinuation. Initiation occurs when the patient takes the first dose of a prescribed medication.; implementation is the extent to which a patient’s actual dosing corresponds to the prescribed dosing regimen from initiation until the last dose; and discontinuation marks the interruption, occurs when the patient stops taking the prescribed medication, for whatever reason(s).17 However, adherence/concordance is still a major challenge in the treatment of hypertension, with inadequate prevalence in most countries,18 with rates of around 50% in developed countries and about only 30% in developing countries.16
Much of the data on blood pressure control in low- and middle-income countries, such as Brazil, originates from primary healthcare services.11,19 This knowledge gap can be a barrier to the development of public policies for persons with hypertension of greater complexity, that is, those who have comorbidities and greater complications of the disease, and therefore, need assistance in tertiary care. In this context, it is relevant to know the profiles of hypertensive patients, and to identify the prevalence and the variables associated with control and adherence to treatment in this population. Therefore, the present study aimed to assess and identify variables associated with the control of arterial hypertension and adherence to antihypertensive drug treatment in a group of persons with hypertension accompanied in a specialized, outpatient clinic.
Methods
Design, Population, and Sample
A prospective cross-sectional study was conducted between August 2018 and July 2019. The clinic cares for approximately 800 persons with hypertension in a specialized and outpatient service located in a tertiary teaching hospital in the city of São Paulo, Brazil. The sample size was calculated, considering a control rate of 60%18 and a significance level of 5%, leading to the selection of 253 patients. The medical records were analysed and included persons with hypertension aged 18 years or older, who had been accompanied at the outpatient clinic for at least six months, and who voluntarily agreed to participate in the study by signing the Free and Informed Consent Form, were included in the study. Patients with secondary arterial hypertension and pregnant women were excluded from the study (Figure 1). The invitation to participate in the study was made at the outpatient’s routine medical visit. The interview for data collection was scheduled for another time and held in individual offices, by trained nurses.
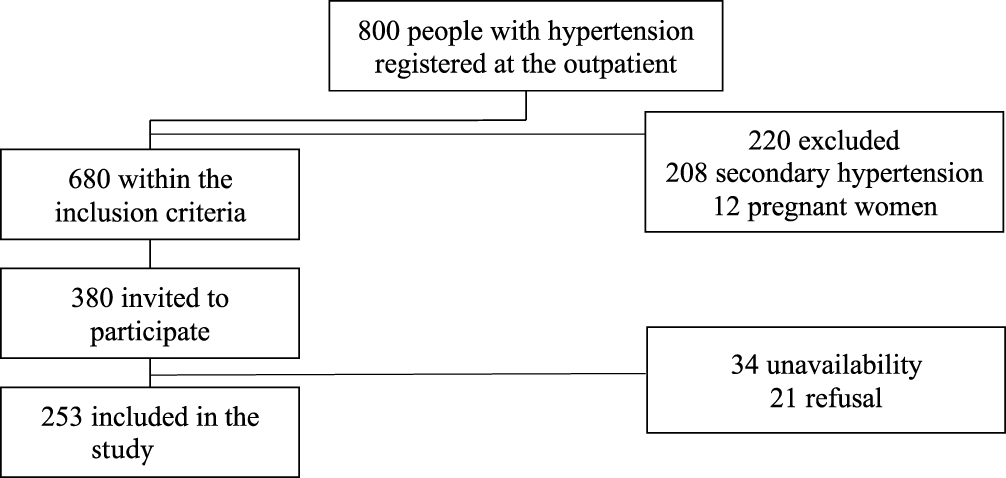 |
Figure 1 Flowchart of inclusion and exclusion of the hypertensive patients. |
Blood Pressure Control and Drug Treatment Adherence
Blood pressure control was assessed by blood pressure measurement and defined by systolic blood pressure less than 140 mmHg and diastolic blood pressure less than 90 mmHg. Blood pressure was measured by the principal investigator, in a calm and private environment, with a validated automatic device (Omron HEM-705 CP).20 Before blood pressure measuring, the investigator made sure that the patient did not have a full bladder; did not exercise for at least 60 minutes; not having ingested alcoholic beverages, coffee or food and not having smoked in the last 30 minutes.
The patients were kept seated, with their legs uncrossed, feet flat on the floor, back against the chair, and relaxed; with their one arm at the heart level with the palm of their hand facing up. A cuff suitable for the size of the arm was used. Three consecutive blood pressure measurements were taken, with an interval of two minutes between each measurement. The first blood pressure value was excluded and the mean value of the last two measurements was used.
Adherence/concordance to antihypertensive treatment was assessed using the Morisky Green Levine Medication Adherence Scale,21 which was validated for the Portuguese language in Brazil.22 The scale determines adherence to treatment based on the patient’s response to four questions that present a choice of dichotomous responses (yes or no). Adherence to drug treatment was considered when all responses were negative (final score = 0) and a positive response to one of the four items classifies the patient as non‐adherent to medication.
Study Variables
Biosocial data, habits and lifestyle, anthropometric measurements, body composition and laboratory data were collected. All instruments used were validated for the Portuguese language in Brazil.
Age, sex, race, marital status and education were obtained by self-report. For socioeconomic classification, the “Brazil Economic Classification Criterion” was used, which estimates the purchasing power of urban people and families.23 This classification assesses the possession and quantity of goods such as household appliances, housing, and education. The higher the score, the higher the socioeconomic status stratified into the following classes: A1, B1, B2, C1, C2, D, and Class E.23
Habits and lifestyles were also assessed by self-report and included smoking, alcohol consumption and physical activity. Regarding smoking, patients were classified as smokers, non-smokers and ex-smokers. The intake of alcoholic beverages was assessed by the Alcohol Use Disorders Test (AUDIT),24 which classifies patients according to scores on low-risk (between 0 and 7 points) consumption, risk use (8 to 15 points), harmful use (16 to 19 points), and probable dependence (≥20 points). Physical activity was assessed by a short version of the International Physical Activity Questionnaire (IPAQ)25 which classifies patients into: very active, active, irregularly active, or sedentary.
The psycho-emotional characteristics were analyzed using the SRQ-20-Self Report Questionnaire26 which assesses common non-psychotic mental disorders through 20 dichotomous questions (yes or no) and for each affirmative answer, 1 point is added. A person with a common mental disorder is considered when the patient reaches a final score> 6 points for men or> 8 points for women.
Anthropometric measures such as weight, height, body mass index, waist circumference, waist circumference, hip circumference, and neck circumference were also evaluated. Body composition was assessed using a calibrated bioimpedance scale and included: body fat percentage, visceral fat level, skeletal muscle percentage, and body age. All measurements were performed by the investigator. We also included data on fasting blood glucose, glycated hemoglobin, lipid profile, glomerular filtration rate analyzed by the MDRD equation, urea, creatinine, and proteinuria, in addition to information on the histories of comorbidities and drug treatments, all obtained from the patient’s electronic medical record.
Statistical Analysis
The level of significance adopted was 5% and used for categorical variables, Pearson’s chi-square test or Fischer’s exact tests, and for quantitative variables, the Wilcoxon-Mann–Whitney, Brunner-Munzel tests, and t-tests were used. In the logistic regression model, the candidate variables for predictors were those with a p-value <0.20 in the bivariate analysis of comparison between patients with controlled and uncontrolled blood pressure. The final model was presented according to the variables selected via LASSO (least absolute shrinkage and selection operator), in order to minimize the cross-validation error and respecting the standard error criterion.
Ethics
The research Ethics Committee of School of Nursing, University of São Paulo and Medical School, University of São Paulo approved the study, with reference numbers 3.003.912 and 2.831.454. All participants received a clear, plain-language summary of the study design, benefits, and risks and then signed voluntary informed consent forms. This study complies with the Declaration of Helsinki.
Results
Of the 253 persons with hypertension who composed the sample, 175 (69.2%) had their blood pressure under control and 228 (90.1%) adhered to drug treatment. Most of the analysed persons with hypertension were females (61.7%), white (63.2%), married (52.8%), and most (47.0%) belonged to a low socioeconomic stratum (C2). Most patients presented completed secondary education (44.3%), a monthly income in the range of 392.00 dollars. The mean age of the patients was 65.0 (13.3) years. Controlled persons with hypertension were statistically different (p <0.05) from uncontrolled ones only in relation to marital status, with a predominance of married individuals in the first group (58.9% vs 39.0%, respectively) (Table 1).
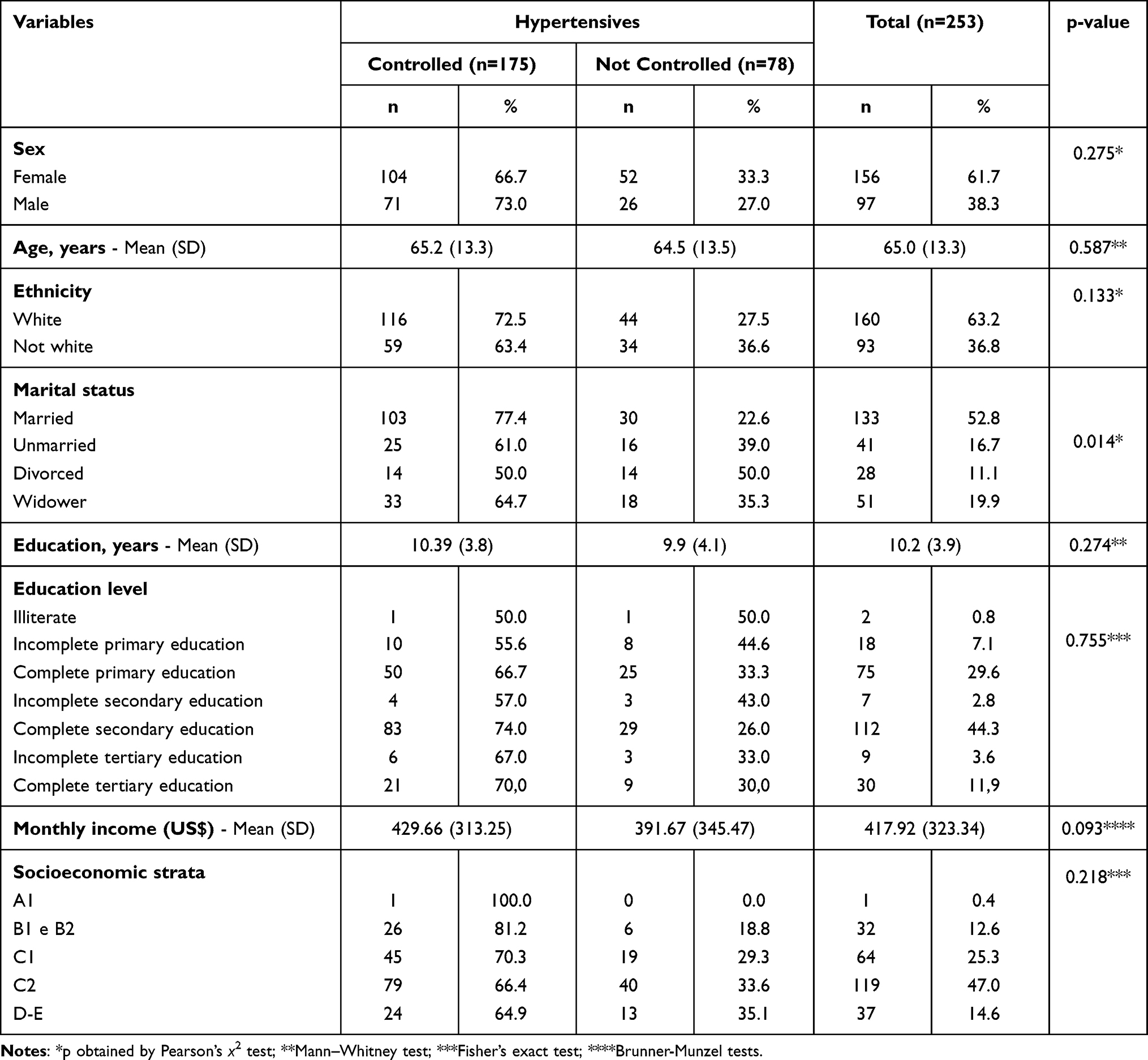 |
Table 1 Biosocial Variables, According to Groups of Controlled and Uncontrolled Persons with Hypertension Seen at a Specialized Outpatient Clinic |
Regarding habits and lifestyles, it was found that just over half of the patients (56.1%) reported not being smokers and only 21.7% practiced physical activity on a regular basis. A representative part of the sample (40.3%) used alcohol, however, almost all (98.8%) presented low-risk consumption (Table 2).
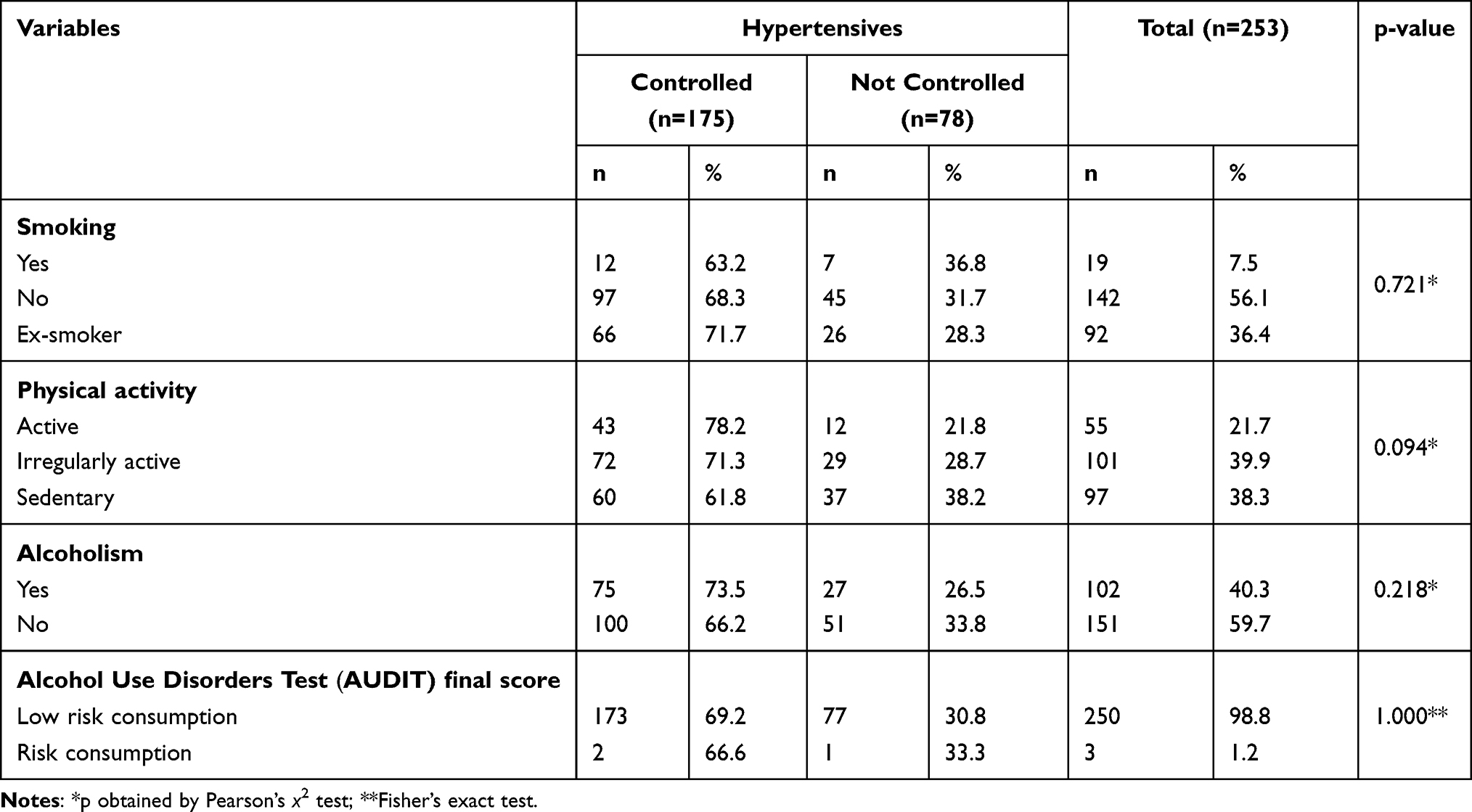 |
Table 2 Characteristics of Habits and Lifestyles According to Groups of Controlled and Uncontrolled Persons with Hypertension Seen at a Specialized Outpatient Clinic |
The data in Table 3 show that the body mass index was at the upper limit of the overweight range [29.5 (5.3) Kg/m2] and the expressive majority (81.4%) showed overweight/obesity. The means of abdominal circumference, waist-hip ratio, and neck circumference were altered, in the increased/greatly increased ranges. The variables of body composition, body fat, and visceral fat were in the high/very high ranges and the majority (56.1%) had a percentage of skeletal muscle qualified as low. The body age estimated by bioimpedance, was above the real biological age. Controlled persons with hypertension were statistically different (p <0.05) from uncontrolled ones, as they presented lower body mass index averages [29.0 (5.4) vs 30.6 (4.9) Kg/m2], waist circumferences [101.6 (13.7) vs 101.7 (10.4) cm], body fat index [36.1 (10.5) vs 38.1 (9.3)] and body age [64.9 (12.0) vs 68.1 (11.1)].
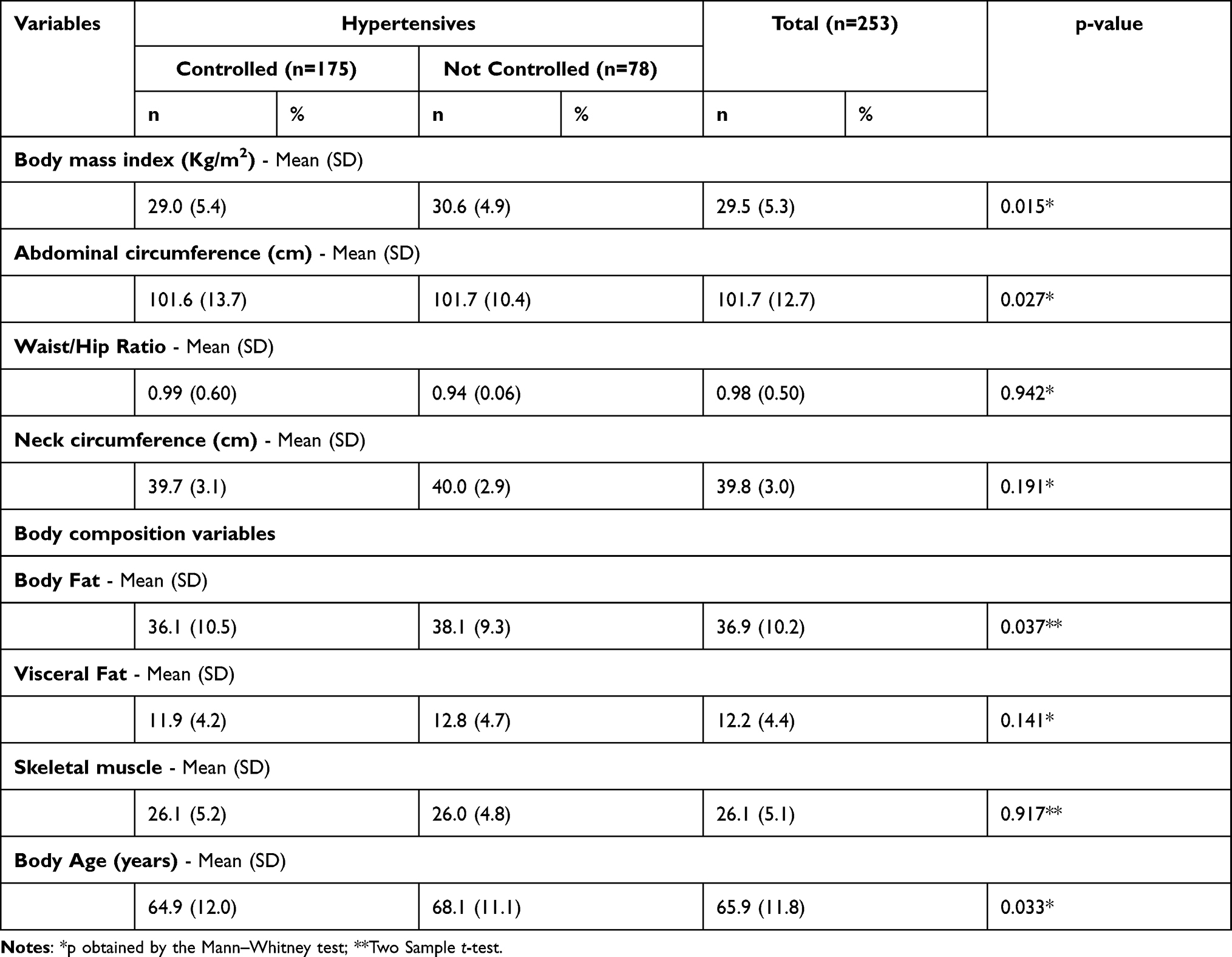 |
Table 3 Anthropometric Characteristics and Body Composition, According to Groups of Controlled and Uncontrolled Persons with Hypertension Seen at a Specialized Outpatient Clinic |
The analysis of laboratory tests showed that 15.6% had fasting glucose values compatible with diabetes. However, considering the values of glycated hemoglobin, the percentage rose to 30.4%. It is noteworthy that 40.7% had a medical diagnosis of diabetes mellitus. Most had desirable triglyceride values (63.6%), total cholesterol (69.6%) and HDL-cholesterol (81.4%). In relation to LDL-cholesterol, just over half (56.5%) presented values considered as excellent, however, dyslipidemia reported in medical records was the most prevalent morbidity (71.5%). Most presented values of urea and creatinine within the normal range (82.2% and 61.7%, respectively) and the estimated glomerular filtration rate, despite having the average with normal value, 31.6% of the persons with hypertension showed values <60 mL/min and 28.1% had protein in their urine. At lower frequencies, the presence of other comorbidities such as chronic kidney disease (19.0%), neoplasia (15.4%), and heart failure (13.4%) were also observed. Regarding psycho-emotional characteristics, 23.7% of the studied persons with hypertension were classified as having common mental disorders (Table 4).
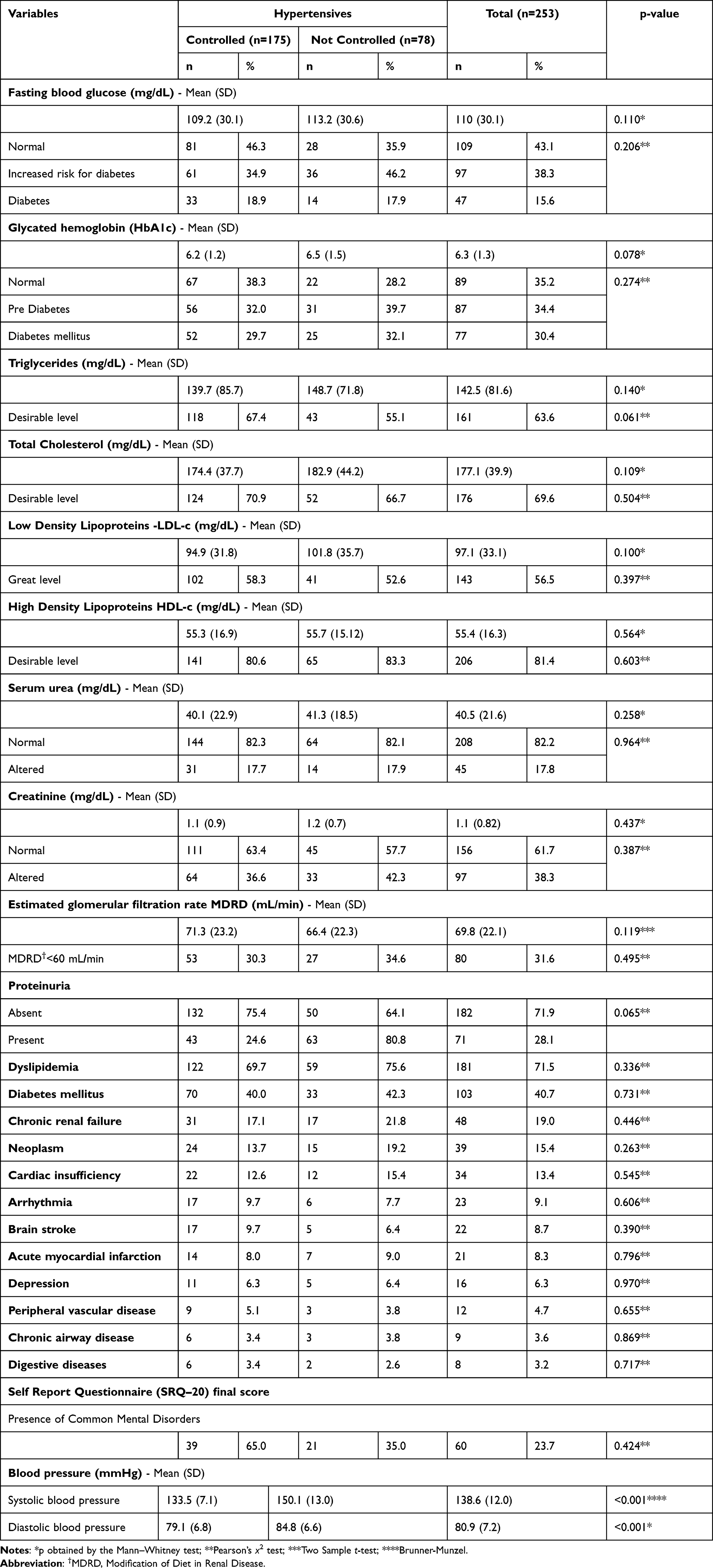 |
Table 4 Comorbidities and Laboratory Markers, According to Groups of Controlled and Uncontrolled Persons with Hypertension Seen at a Specialized Outpatient Clinic |
The average of the total number of drugs prescribed per patient was 8.0 (4.0) and the average number of antihypertensive drugs was 3.7 (1.9). Only 9.5% of persons with hypertension used only one antihypertensive medication, 42.7% two or three, and slightly less than half (47.8%) used four or more antihypertensive drugs. The most prescribed class of antihypertensive drugs was diuretics (78.3%), followed by calcium channel blockers (68.8%), AT1 receptor blockers (61.7%), beta-blocker (50.2%), angiotensin-converting enzyme inhibitor (30.4%), and at lower frequencies, centrally acting agents (15.8%), vasodilators (10.0%) and alpha-blockers (7.1%). Controlled persons with hypertension compared to uncontrolled ones were statistically different (p <0.05) since they presented the lowest total average of drugs prescribed per patient [7.6 (3.8) vs 9.1 (4.1)] and antihypertensive drugs [3.4 (1.7) vs 4.5 (2.1)]; in addition to a lower frequency of antihypertensive classes: calcium channel blockers (61.7% vs 84.6%), beta-blocker (44.0% vs 64.1%), centrally acting agents (12, 6% vs 23.1%), and vasodilators (5.7% vs 19.2%) (Table 5).
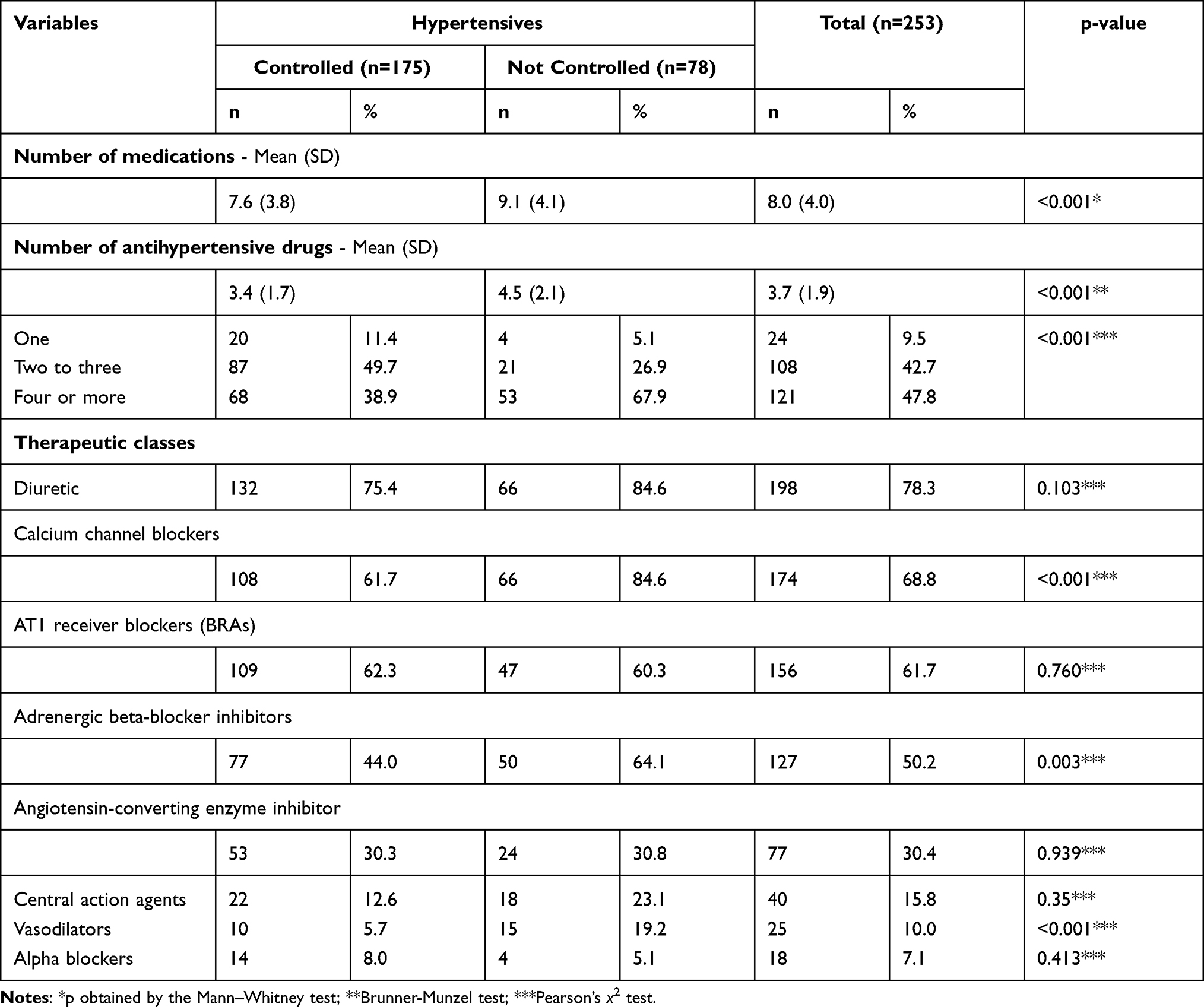 |
Table 5 Characteristics of Drug Treatment, According to Groups of Controlled and Uncontrolled Persons with Hypertension Seen at a Specialized Outpatient Clinic |
The multiple logistic regression analysis showed that there was an association (p <0.05) with blood pressure control the variables: marital status, use of calcium channel blockers, and the number of prescribed antihypertensive drugs. Thus, married persons with hypertension were 2.3 times more likely to control blood pressure than unmarried ones; those using calcium channel blockers were 55.9% less likely to control blood pressure; and with each antihypertensive medication added to the treatment, the chance of blood pressure control decreased by 21.3% (Table 6).
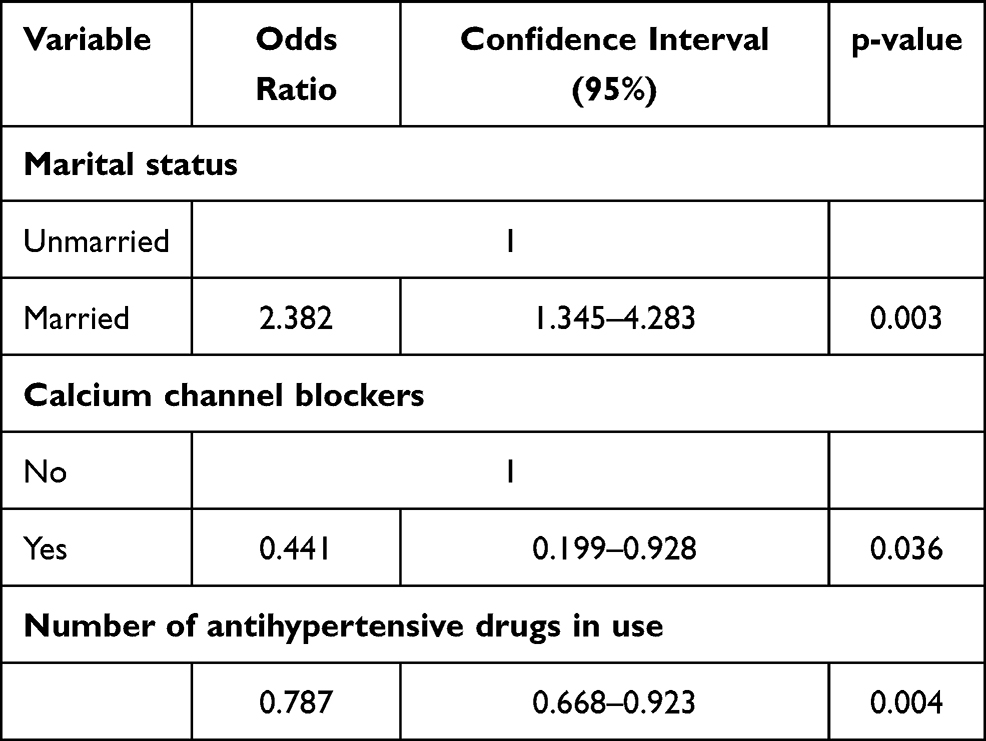 |
Table 6 Logistic Regression Model and Blood Pressure Control in Persons with Hypertension Seen at a Specialized Outpatient Clinic |
None of the variables studied was associated with adherence to antihypertensive drug treatment.
Discussion
The main results in this study showed that there was little agreement between the rates of blood pressure control and adherence/concordance to antihypertensive treatment (69.2% vs 90.1%). However, married marital status, the use of calcium channel blockers and the number of antihypertensive drugs were variables that were independently associated with blood pressure control.
The prevalence of hypertension control found here (~70%), although insufficient, was similar to that of developed countries and a reference in the treatment of hypertension, such as Canada, whose current estimate is 68%.27 Data from the National Health and Nutrition Examination Survey estimated that the proportion of blood pressure control increased from 31.8% in 1999–2000 to 48.5% in 2007–2008 (p <0.001), to 53.8% in 2013 −2014 (p = 0.14), and then dropped to 43.7% in 2017–2018 (p = 0.003).28 This decline is a worrying finding since the lack of hypertension control is directly related to the occurrence of cardiovascular diseases and death from all causes.6 Data from the 2017 Global Burden of Disease show that in Brazil the total number of deaths attributable to high systolic blood pressure increased by 53.4%, ranking first as the main risk factor for death in the period from 1990 to 2017.29 From this perspective, the global estimates for control are alarming, as seen in the “May Measurement Month, 2017” conducted in more than 80 countries, showing that among the persons with hypertension treated, only 46.3% had their blood pressure controlled.30 Results from Brazilian studies are similar, with rates around 50%.9,31,32 These control data are not very satisfactory, especially considering that in the majority, they result from persons with hypertension seen in primary healthcare, where patients with less severe disease are concentrated.
The measurement of blood pressure, despite being considered a standard procedure for the diagnosis and follow-up of people with hypertension, is subject to the influence of the observer and the environment.33,34 Thus, the optimized result of the prevalence of control found in the present study may also have been influenced by the fact that the patient was evaluated in an environment outside the place of treatment and blood pressure measurements were performed by a nurse, probably attenuating the white coat effect.
The prevalence of adherence to antihypertensive treatment, assessed by the Morisky Green Levine Scale, was higher than the data found in the literature. A systematic review with meta-analysis with the inclusion of studies that also used self-report measures showed that the prevalence of adherence/concordance ranged from 36.7% to 66.2%.35 In the present study it was found that adherence was not a predictor of blood pressure control and in persons with hypertension who reported being adherent to treatment, about a third did not have their blood pressure under control. The use of a self-report instrument to assess adherence may have influenced this result, since this method may overestimate the results. However, the instrument used is widely applied in studies with the same theme, and can be considered the most applicable tool to clinical practice, in view of its practicality and low cost. Measuring adherence/concordance to antihypertensive treatment is a complex task. There is no gold standard based on the combination of methods and various dimensions involving the treatment adherence process recommended by the World Health Organization.15 In this study, direct assessment was not possible due to financial issues.
Interestingly, marital status was the only biosocial variable that was associated with blood pressure control. Married patients with hypertension were more likely to control blood pressure in comparison to unmarried ones. Similarly, a meta-analysis study showed the influence of marital status on the incidence of cardiovascular disease, evidencing that single individuals were more likely to have cardiovascular disease compared to married couples.36 A study that evaluated adherence to drug treatment in patients after acute myocardial infarction also showed that married persons with hypertension were more adherent to treatment.37 The protective effect of a married marital status can be attributed to changes in behavior and social networks resulting from the union and the established family bond. The association between marital status and hypertension has been described in other studies.38–40 However, the influence of marital status in the control of hypertension is not frequent in the literature and expanding knowledge about this aspect is relevant. Family and social support is a fundamental part of the health-disease process and the fact of having a partner can be a facilitating agent in the treatment of hypertensive persons.
Uncontrolled persons with hypertension had a higher body mass index, waist circumference, body fat and body age in the bivariate analysis (p <0.05), when compared with the controlled subjects. Robust evidence41 already demonstrates this relationship and reinforces the need for measures that promote the adoption of healthier behaviors, especially among hypertensive persons, with the objective of achieving the blood pressure control goal.
The laboratory profile of hypertensive persons, consistent with the most prevalent comorbidities, pointed to an important percentage of persons with alterations in glycated hemoglobin, LDL and glomerular filtration rate, which are relevant markers when investigating the degree of severity of the hypertensive persons. Despite not being associated with blood pressure control, these results reinforce the severity profile of the studied persons, of whom 30.8% still remained uncontrolled. Another important finding was that control was associated with characteristics of drug treatment. With each antihypertensive added to the treatment, the chance of pressure control decreased by 21.3%. This result may be a consequence of the fact that the greater the number of medications, the greater the difficulty in correctly taking the medications and the lower the chance of adhering to the treatment, reflecting a worsening of control. However, only about 30% of hypertensive persons respond to treatment with monotherapy, therefore requiring more than one medication.42,43 However, there is evidence of low adherence to treatment in hypertensive persons with polypharmacy.44–46 The association of fixed doses of medications would be an alternative to reduce the number of medications taken, however, with the Brazilian public system for dispensing antihypertensive drugs it is not possible. It should be noted that the studied sample was composed of complex patients, with other diseases associated with hypertension, such as diabetes, dyslipidemia, in addition to lesions in target organs, justifying the need for more complex drug treatments.
The uncontrolled persons with hypertension presented prescriptions, in greater quantity (p<0.05), in the bivariate analysis of some pharmacological classes, however only the use of calcium channel blockers remained associated with the blood pressure control at the final multivariate model. Hypertensive persons using calcium channel blockers had a 55.9% less chance of controlling blood pressure. The negative association between the use of this medication and the control of blood pressure can be related to several factors, such as greater severity of persons with hypertension and more difficulty in controlling the disease. Calcium channel blockers are effective antihypertensives, reduce cardiovascular morbidity and mortality, have good tolerability and present safety in the treatment of arterial hypertension.47
Limitations
An important limitation of the present study was the use of a self-report instrument to assess adherence. It is a form of evaluation that can underestimate or overestimate the result. The ideal would be the combination of direct and indirect methods, however, the limitation of financial resources in the Brazilian reality was a limiting factor. It is worth mentioning that the Morisky Green Levine Scale has good psychometric characteristics, is an easy-to-use, widely used, low-cost method, in addition to identifying important attitudes towards barriers related to adherence. Another limitation is related to the cross-sectional design, which does not allow establishing relationships between cause and effect and the fact that it was carried out in a single center, resulting in difficulty in generalizing the data.
Conclusion
Despite the presence of important risk factors and target organ injuries in the studied persons with hypertension, the prevalence of control and adherence was satisfactory. The multiprofessional team has a privileged position in the health system to strengthen the social support network of persons with hypertension. Strategies that favour the integration between hypertensive persons, family, health services and other social facilities can be beneficial for the control of blood pressure and adherence to drug treatment. The goal of controlling persons with hypertension is not an easy task to be achieved, but population strategies must be implemented. Having a usual source of care, optimizing real adherence, and minimizing therapeutic inertia can lead to higher rates of blood pressure control. A collaborative partnership between patients, health professionals, and the health system, incorporates a multilevel approach to the control of hypertension and can bring satisfactory results. The findings of the present study made it possible to evaluate adherence to antihypertensive drug treatment in an indirect way, blood pressure control, and associated variables, in the largest public hospital complex in Latin America and the results can contribute to the improvement of public health policies.
Acknowledgments
This study was supported by the National Council of Technological and Scientific Development (CNPq; PhD Program), and The São Paulo Research Foundation (FAPESP; 2018/20948-2). This study was financed in part by the Coordination of Superior Level Staff Improvement - Brazil (CAPES) - Finance Code 001.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest relevant to this manuscript.
References
1. Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020;16:223–237. doi:10.1038/s41581-019-0244-2
2. GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1923–1994. doi:10.1016/S0140-6736(18)32225-6
3. GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1736–1788. doi:10.1016/S0140-6736(18)32203-7
4. Mills KT, Bundy JD, Kelly TN, et al. Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation. 2016;134:441–450. doi:10.1161/CIRCULATIONAHA.115.018912
5. Picon RV, Fuchs FD, Moreira LB, Riegel G, Fuchs SC. Trends in prevalence of hypertension in Brazil: a systematic review with meta-analysis. PLoS One. 2012;7:e48255. doi:10.1371/journal.pone.0048255
6. Picon RV, Fuchs FD, Moreira LB, Fuchs SC. Prevalence of hypertension among elderly persons in urban Brazil: a systematic review with meta-analysis. Am J Hypertens. 2013;26:541–548. doi:10.1093/ajh/hps076
7. Ettehad D, Emdin CA, Kiran A, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387:957–967. doi:10.1016/S0140-6736(15)01225-8
8. NCD Risk Factor Collaboration (NCD-RisC). Long-term and recent trends in hypertension awareness, treatment, and control in 12 high-income countries: an analysis of 123 nationally representative surveys. Lancet. 2019;394:639–651. doi:10.1016/S0140-6736(19)31145-6
9. Chow CK, Teo KK, Rangarajan S, et al. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. JAMA. 2013;310:959–968. doi:10.1001/jama.2013.184182
10. Lopes RD, Barroso WKS, Brandao AA, et al. The first Brazilian registry of hypertension. Am Heart J. 2018;205:154–157. doi:10.1016/j.ahj.2018.08.012
11. Malachias MVB, Souza WKSB, Plavnik FL, et al. 7th Brazilian guideline of arterial hypertension. Arq Bras Cardiol. 2016;107:1–83. doi:10.5935/abc.20160140
12. Redon J, Mourad JJ, Schmieder RE, Volpe M, Weiss TW. Why in 2016 are patients with hypertension not 100% controlled? A call to action. J Hypertens. 2016;34:1480–1488. doi:10.1097/HJH.0000000000000988
13. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: the Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J Hypertens. 2018;36:1953–2041. doi:10.1097/HJH.0000000000001940
14. Whelton PK, Carey RM. The 2017 clinical practice guideline for high blood pressure. JAMA. 2017;318:2073–2074. doi:10.1001/jama.2017.18209
15. Barroso WKS, Rodrigues CS, Bortolotto LA, et al. Brazilian guideline of hypertension - 2020. Arq Bras Cardiol. 2020. doi:10.36660/abc.20201238
16. Sabaté E. World Health Organization report: adherence to long-term therapies: evidence for action. Geneva, Switzerland: World Health Organization; 2003. Available from: http://www.who.int/chronic_conditions/adherencereport/en/.
17. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73:
18. Burnier M, Egan MB. Adherence in hypertension: a review of prevalence, risk factors, impact, and management. Circ Res. 2019;124:1124–1140. doi:10.1161/CIRCRESAHA.118.313220
19. Pinho NA, Pierin AMG. Hypertension control in Brazilian publications. Arq Bras Cardiol. 2013;101:e65–e73. doi:10.5935/abc.20130173
20. O’Brien E, Mee F, Atkins N, Thomas M. Evaluation of three devices for self-measurement of blood pressure according to the revised British Hypertension Society Protocol: the Omron HEM-705CP, Philips HP 5332, and Nissei DS-175. Blood Press Monit. 1996;1:55–61.
21. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24:67–74. doi:10.1097/00005650-198601000-00007
22. Oliveira-Filho AD, Morisky DE, Neves SJ, Costa FA, de Lyra DP. The 8-item Morisky Medication Adherence Scale: validation of a Brazilian-Portuguese version in hypertensive adults. Res Social Adm Pharm. 2014;10:554–561. doi:10.1016/j.sapharm.2013.10.006
23. ABEP. Brazil economic classification criterion. Brazilian Association of Research Companies; 2008.
24. Lima CT, Freire AC, Silva AP, Teixeira RM, Farrell M, Prince M. Concurrent and construct validity of the audit in an urban Brazilian sample. Alcohol Alcohol. 2005;40:584–589. doi:10.1093/alcalc/agh202
25. Matsudo S, Araujo T, Matsudo V, et al. Questionário Internacional de Atividade Física (IPAQ): estudo de validade e reprodutibilidade no Brasil. Ativ Fis e Saúde. 2001;6:5–18. doi:10.12820/rbafs.v.6n2p5-18
26. Mari JJ, Williams P. A validity study of a psychiatric screening questionnaire (SRQ-20) in primary care in the city of Sao Paulo. Br J Psychiatry. 1986;148:23–26. doi:10.1192/bjp.148.1.23
27. Schiffrin EL, Campbell NR, Feldman RD, et al. Hypertension in Canada: past, present, and future. Ann Glob Health. 2016;82:288–299. doi:10.1016/j.aogh.2016.02.006
28. Muntner P, Hardy S, Fine L, et al. Trends in blood pressure control among us adults with hypertension, 1999–2000 to 2017–2018. JAMA. 2020;324:1190–1200. doi:10.1001/JAMA.2020.14545
29. Nascimento BR, Brant LCC, Yadgir S, et al. Trends in prevalence, mortality, and morbidity associated with high systolic blood pressure in Brazil from 1990 to 2017: estimates from the “Global Burden of Disease 2017” (GBD 2017) study. Popul Health Metr. 2020;18:17. doi:10.1186/s12963-020-00218-z
30. Beaney T, Schutte AE, Tomaszewski M, et al. May Measurement Month 2017: an analysis of blood pressure screening results worldwide. Lancet Glob Health. 2018;6:e736–e743.
31. Firmo JOA, Peixoto SV, Loyola Filho AI, et al. Health behaviors and hypertension control: the results of ELSI-BRASIL. Cad Saúde Pública. 2019;35:e00091018. doi:10.1590/0102-311X00091018
32. Chor D, Ribeiro AL, Carvalho MS, et al. Prevalence, awareness, treatment and influence of socioeconomic variables on control of high blood pressure: results of the ELSA-Brasil Study. PLoS One. 2015;10:e0127382. doi:10.1371/journal.pone.0127382
33. Colósimo FC, Silva SSBE, Toma GA, Pierin AMG. Nursing actions increases the control of hypertensive patients and reduces white-coat effect. Rev Esc Enferm USP. 2012;46:10–15. doi:10.1590/S0080-62342012000700002
34. Tucker KL, Sheppard JP, Stevens R, et al. Self-monitoring of blood pressure in hypertension: a systematic review and individual patient data meta-analysis. PLoS Med. 2017;14:e1002389. doi:10.1371/journal.pmed.1002389
35. Nielsen JO, Shrestha AD, Neupane D, Kallestrup P. Nonadherence to anti-hypertensive medication in low- and middle-income countries: a systematic review and meta-analysis of 92443 subjects. J Hum Hypertens. 2017;31:14–21. doi:10.1038/jhh.2016.31
36. Wong CW, Kwok CS, Narain A, et al. Marital status and risk of cardiovascular diseases: a systematic review and meta-analysis. Heart. 2018;104:1937–1948. doi:10.1136/heartjnl-2018-313005
37. Pietrzykowski Ł, Michalski P, Kosobucka A, et al. Medication adherence and its determinants in patients after myocardial infarction. Sci Rep. 2020;10:12028. doi:10.1038/s41598-020-68915-1
38. Li T, Song X, Wu J, et al. Awareness of hypertension and related factors in northeastern China: a cross-sectional study. J Hum Hypertens. 2020;34:43–50. doi:10.1038/s41371-019-0263-2
39. Hosseini Z, Veenstra G, Khan NA, Conklin AI. Social connections and hypertension in women and men: a population-based cross-sectional study of the Canadian Longitudinal Study on Aging. J Hypertens. 2021;39:651–660. doi:10.1097/HJH.0000000000002688
40. Manfredini R, De Giorgi A, Tiseo R, et al. Marital status, cardiovascular diseases, and cardiovascular risk factors: a review of the evidence. J Womens Health. 2017;26:624–632. doi:10.1089/jwh.2016.6103
41. Jayedi A, Rashidy-Pour A, Khorshidi M, Shab-Bidar S. Body mass index, abdominal adiposity, weight gain and risk of developing hypertension: a systematic review and dose-response meta-analysis of more than 2.3 million participants. Obes Rev. 2018;19:654–667. doi:10.1111/obr.12656
42. Roldan PC, Ho GY, Ho PM. Updates to adherence to hypertension medications. Curr Hypertens Rep. 2018;20:1–7. doi:10.1007/s11906-018-0830-x
43. Verma AA, Khuu W, Tadrous M, Gomes T, Mamdani MM. Fixed-dose combination antihypertensive medications, adherence, and clinical outcomes: a population-based retrospective cohort study. PLoS Med. 2018;15:e1002584. doi:10.1371/journal.pmed.1002584
44. Poulter NR, Borghi C, Parati G, et al. Medication adherence in hypertension. J Hypertens. 2020;38:579–587. doi:10.1097/HJH.0000000000002294
45. Vrijens B, Antoniou S, Burnier M, de la Sierra A, Volpe M. Current Situation of Medication Adherence in Hypertension. Front Pharmacol. 2017;8:100. doi:10.3389/fphar.2017.00100
46. Abegaz TM, Shehab A, Gebreyohannes EA, Bhagavathula AS, Elnour AA. Nonadherence to antihypertensive drugs: a systematic review and meta-analysis. Medicine. 2017;96:e5641. doi:10.1097/MD.0000000000005641
47. Venkataraman R, Rashid M, Shashikantha B, et al. Prescribing pattern of antihypertensive medication and adherence to Joint National Commission-8 guidelines in a rural tertiary care Indian teaching hospital. J Basic Clin Physiol Pharmacol. 2019;31. doi:10.1515/jbcpp-2019-0133
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.