")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Biopsychology of Physical Activity in People with Schizophrenia: An Integrative Perspective on Barriers and Intervention Strategies
Authors Arnautovska U , Kesby JP , Korman N, Rebar AL, Chapman J, Warren N, Rossell SL, Dark FL, Siskind D
Received 18 October 2022
Accepted for publication 2 December 2022
Published 15 December 2022 Volume 2022:18 Pages 2917—2926
DOI https://doi.org/10.2147/NDT.S393775
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Urska Arnautovska,1,2 James P Kesby,3,4 Nicole Korman,1,2 Amanda L Rebar,5 Justin Chapman,2,3 Nicola Warren,1,2 Susan L Rossell,6,7 Frances L Dark,1,2 Dan Siskind1,2,4
1Faculty of Medicine, The University of Queensland, Woolloongabba, QLD, Australia; 2Metro South Addictions and Mental Health Service, Woolloongabba, QLD, Australia; 3Centre for Mental Health, Griffith University, Nathan, QLD, Australia; 4Queensland Centre for Mental Health Research, Wacol, QLD, 4076, Australia; 5Motivation of Health Behaviours Lab, Appleton Institute, School of Health, Medical, and Applied Sciences; Central Queensland University, Rockhampton, QLD, Australia; 6Centre for Mental Health, School of Health Sciences, Swinburne University of Technology, Hawthorn, VIC, Australia; 7Psychiatry, St Vincent’s Hospital Melbourne, Fitzroy, VIC, Australia
Correspondence: Urska Arnautovska, Faculty of Medicine, The University of Queensland, Princess Alexandra Hospital, Building 19 (Room 1MH.44.0), 199 Ipswich Road, Woolloongabba, QLD, 4102, Australia, Tel +61 7 3176 5813, Fax +61 7 3176 2821, Email [email protected]
Abstract: People with severe mental illness such as schizophrenia experience high physical comorbidity, leading to a 15– 20-year mortality gap compared with the general population. Lifestyle behaviours such as physical activity (PA) play important roles in the quest to bridge this gap. Interventions to increase PA engagement in this population have potential to be efficacious; however, their effectiveness can be hindered by low participant engagement, including low adherence and high drop-out, and by implementation of interventions that are not designed to compensate for the cognitive and motivational impairments characteristic for this group. Moreover, and importantly, the negative symptoms of schizophrenia are associated with neurobiological changes in the brain, which—based on principles of biopsychology—can contribute to poor motivation and impaired decision-making processes and behavioural maintenance. To increase PA levels in people with schizophrenia, better understanding of these neurological changes that impact PA engagement is needed. This has the potential to inform the design of interventions that, through enhancement of motivation, could effectively increase PA levels in this specific population. Incorporating strategies that address the dopamine dysregulation associated with schizophrenia, such as boosting the role of reward and self-determined motivation, may improve long-term PA maintenance, leading to habitual PA. Consideration of motivation and behavioural maintenance is also needed to impart health benefits such as prevention of chronic disease, which is associated with currently low PA levels in this high metabolic risk population. Taking a biopsychological perspective, we outline the neural pathways involved in motivation that are impacted by schizophrenia and propose strategies for promoting motivation for and PA engagement from adoption to habit formation.
Keywords: exercise, psychosis, autonomous motivation, behaviour change, lifestyle interventions, behavioural maintenance
Introduction
Since the publication of Crider’s detailed textbook Schizophrenia: A Biopsychological Perspective in 1979,1 empirical knowledge about the complexities of schizophrenia as a biopsychological condition has advanced immensely. However, a comprehensive understanding of the condition as complex as schizophrenia requires an integration of evidence from various disciplines. Our integrative perspective to this field contributes to evidence that has a potential to address the high rates of physical health comorbidity in people with schizophrenia, resulting in a 20-year mortality gap compared with the general population.2 This mortality gap is largely due to higher rates of cardiovascular disease, driven by a combination of genetic factors, poor diet, inadequate exercise, smoking, metabolic adverse effects of antipsychotic medications, and health inequalities.3 Obesity and metabolic disease are major concerns for people with schizophrenia and can lead to unwillingness to take regular medication, relapse, avertable hospitalisation, and further worsening of health.2
Given accumulating evidence highlighting the role of health behaviour such as physical activity (PA) in improving health in this population,4–6 our intention is to advance the understanding of the connections between findings from biology, behavioural neuroscience and psychology, to design more effective interventions for promoting PA engagement in this high metabolic-risk population. This endeavour is especially important in light of evidence showing that individuals with schizophrenia with comorbid metabolic syndrome or diabetes mellitus experience more severe cognitive deficits than those without increased risk of metabolic syndrome.7 Understanding the motivational processes underlying PA, and the impact of neurobiology associated with schizophrenia, is vital for informing the design of PA interventions because schizophrenia is thought to be associated with dopaminergic dysregulation, which can significantly impact motivation, cognition, as well as behavioural change.8,9 Specifically, these altered dopaminergic pathways in the brain lead to impairments in predicting the value of rewards, including salience.9 Salience is the perceived importance of a stimulus which drives cognition, behavioural activation, and effort-related decision-making, and is therefore a key consideration for understanding motivational processes.10 Although antipsychotic medications have been suggested to negatively impact cognition through their anticholinergic effects,11 there is limited evidence to support their impact, positively or negatively, on motivation.12 As such, in our perspective, we address likely key barriers to PA engagement experienced by individuals living with schizophrenia and provide recommendations for designing psychosocial PA interventions that can effectively target motivational systems, while considering the role of the neural circuits involved in motivation. These processes are highly complex and interconnected, however this reductionistic approach is aimed at enabling an easier translation into the proposed strategies to increase PA engagement in this population.
Current Evidence
The need to increase PA in people with schizophrenia has been incorporated in clinical guidelines,2 based upon empirical evidence demonstrating positive effects of PA on both physical health and psychiatric symptoms.13 Specifically, PA interventions have been found to reduce positive, negative and total symptoms, improve quality of life, global functioning and depressive symptoms significantly more than control conditions,14 and have also been found effective in reducing cardiometabolic disease in this population.2 People with schizophrenia have lower levels of PA than the general population, with the majority not meeting the recommended PA levels, hampered by poor uptake and high dropout rates.15 The reasons for insufficient PA are likely to be multifactorial and include psychological factors, such as low mood, stress,6,16 psychiatric symptoms and social physique anxiety,5 physical factors such as physical illness and fatigue,16 the sedative effects of psychotropic medications,17,18 and environmental factors (eg, access to facilities).5 However, low motivation for PA is one of the most commonly reported psychological barriers by both people with schizophrenia19 and by mental health staff.20 Due to such complexity of factors and challenges associated with PA engagement, effectively increasing motivation for PA can present a challenge, both to clinicians and people living with schizophrenia.
Mechanisms of Action: From Reward-Driven Action Towards Habit Formation
Motivation is a dynamic process that incorporates both reflective (intentional) and more automatic (non-conscious) processes.21 This distinction is based upon evidence that humans use two memory systems: an automatic system that learns associations through experiences and is largely independent from working memory, and a reflective system that can learn rules based on language and logic following even a single experience when sufficient cognitive capacity is available.22 Both processes play a unique role across different stages of behaviour change and, combined, have been found to influence PA engagement in other population groups.23
The two stages of PA engagement (see Table 1)—initiation (adoption) and maintenance21—involve a series of continuous sub-processes, including reward-driven action and goal-directed decision-making (adoption stage), and habit-formation (maintenance stage).24 Initially, reward-driven action generates motivation by anticipating the reward/positive behaviour (or avoiding a negative outcome), encoding its value, and updating the relative value of reward. This process is followed by more reflective cognitive processes, specifically goal-directed decision-making, which aims for sustained motivation through effort–reward trade-off and effective cognitive control, including skills of delayed planning, retaining the goal, monitoring the performance, and regulating action,25 to enable pursuit of future goals.26 Finally, to achieve habit-formation and continuous engagement in PA, sustained motivation and adequate goal-directed decision-making is required to maintain the target behaviour.21 This process leads to learning of a specific stimulus–outcome association, through recurring context cues, where activities are performed with less conscious effort and independent of immediate rewards27 and short-term changes in goals.28 There are numerous theories explaining the mechanisms behind the role of the above concepts for health behaviour change; we encourage interested readers to seek a more detailed understanding of these theories and processes in a review of behaviour theories29 or original publications.27,30–34 Taking an integrative biopsychological perspective, enriched by the clinical and academic experiences of our multidisciplinary authorship team, this perspective aims to tackle the most encountered barriers to PA in people with schizophrenia and propose strategies for promoting motivation for and PA engagement from adoption to habit formation.
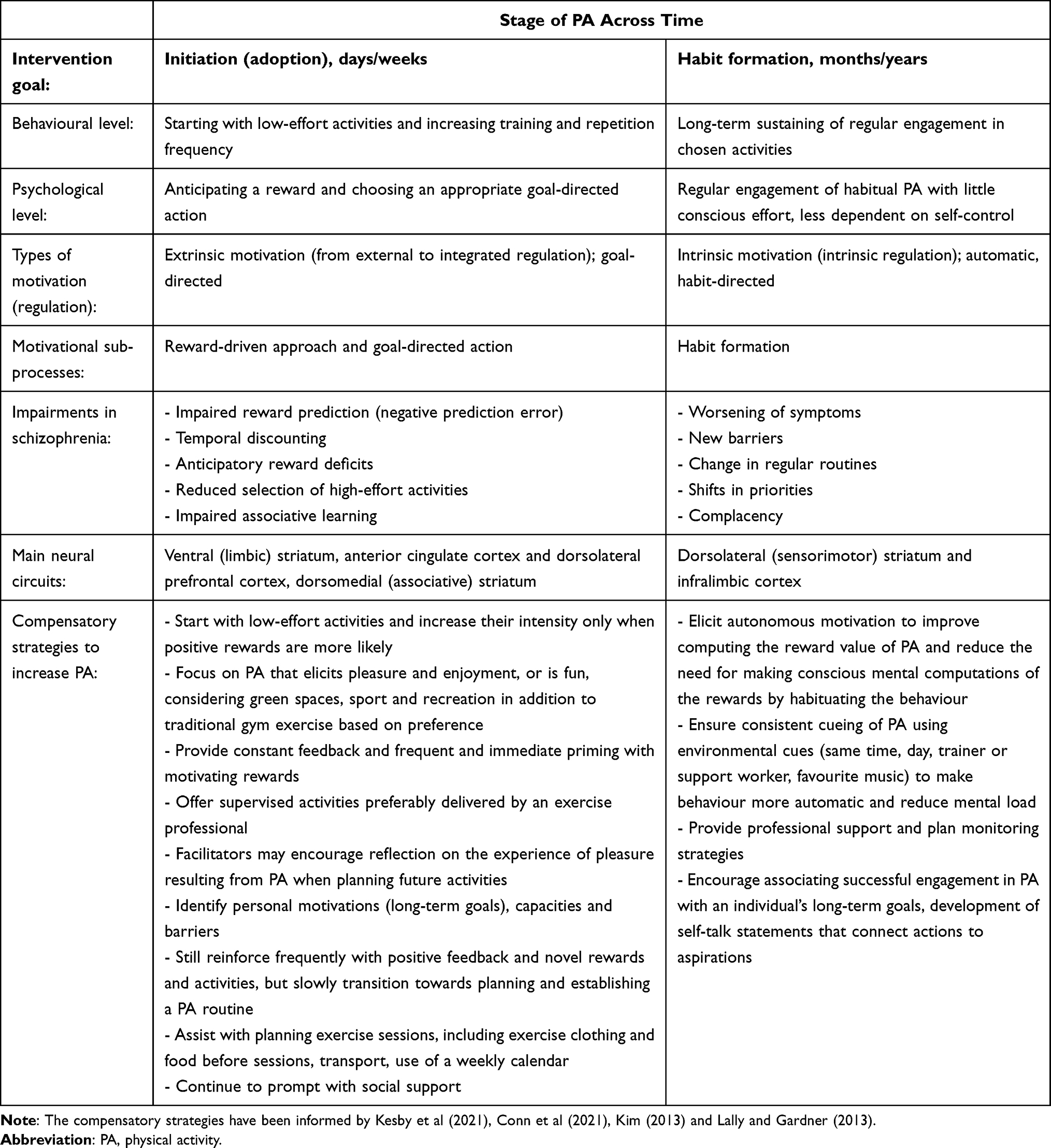 |
Table 1 Compensatory Strategies to Facilitate Behaviour Change Across Two Stages of PA Behaviour Engagement |
Barriers and Strategies to Adopt and Maintain Physical Activity Behaviour
Broad aims of interventions to promote PA are to: (i) facilitate positive experiences with the target behaviour, (ii) incorporate learning to develop skills and positive attitudes related to the behaviour, and (iii) develop habitual responses involving the behaviour in relevant contexts.35 However, as mentioned, the barriers to achieving these aims in individuals with schizophrenia are complex,6,16 reflecting the impairments in the neurobiological pathways underlying motivation in schizophrenia. Specifically, dopaminergic pathways, which play an important role in motivational processes, are impacted in schizophrenia. A recent review concluded that both cortical and subcortical dopamine exhibit a strong influence on a range of cognitive domains, including attention, reward learning, goal-directed action and decision-making.9 These cognitive impairments are reflected in unique challenges faced by individuals with schizophrenia at adoption and maintenance stages of PA behaviour.
Adoption of Physical Activity Behaviour
Problems with motivation for PA engagement, frequently reported by people with schizophrenia,16 which in part result from dopamine dysregulation associated with schizophrenia, include altered reward prediction, reduced higher-effort allocation to obtain rewarding experiences, and reduced selection of high-effort alternatives.
Reward Prediction Error
People with schizophrenia commonly underestimate potential positive experiences and benefits of PA. This is partly due to deficits in reward prediction error, which can lead to slower and more difficult reinforcement learning (ie, associating the valuable outcome with the activity that preceded it). Lower reward prediction error impairs the ability to fully encode the rewarding value of PA, and therefore sustains the prior underestimate of the expected reward undermining the adoption of PA engagement.24 To facilitate uptake of PA in this population, it is therefore paramount to design strategies that compensate for reward prediction error by maximising the reward value of known motivators for PA,16 for example by highlighting the critical role of regular PA for healthy ageing, preventing functional and cognitive decline, and promoting independent mobility and quality of life—the positive rewards of PA advocated at the general population-level.36 On the other hand, PA-promoting strategies should minimise the cost and effort involved in doing the activities by choosing the intensity of activities that is appropriate for an individual,37 to assist encoding and reinforcement learning.
The strategy of maximising the rewards of PA has its rationale in altering the motivational modulation of PA behaviour, which is thought to depend on the limbic striatum.9 Strategies that would maximise social rewards and positive experiences with PA (eg, doing PA with a group of people will be fun) may stimulate the limbic striatum, which encodes motivational variables that are then used by cortical subregions and the associative striatum to select future actions and encourage repetition of behaviour. Given the dopaminergic dysregulation associated with schizophrenia, it is noteworthy to mention that dopaminergic neurons in the midbrain, which project to the ventral (limbic) striatum, are strongly involved in mediating the rewarding effects of stimuli.9,38 Importantly, animal and human studies have shown that activation of the ventral tegmental area from hedonic stimuli, such as food and social connection, results in phasic dopamine release to the nucleus accumbens.39,40
Therefore, motivation for PA may also be increased through social and hedonic experiences (eg, enjoying exercising with a group of people). As such, when promoting adoption of PA among people with schizophrenia, social rewards could be facilitated by playing a person’s favourite music in a welcoming environment either in groups of people who share similar experiences or individually, depending on the preference, with a facilitator who employs person-centred and inclusive approaches.41 Previous research has highlighted the importance of providing positive and encouraging feedback in learning a new complex behaviour.42,43 Taking a reward-driven approach, this positive feedback should be provided in close proximity to the PA itself and repeated often in the PA adoption phase, to account for the reinforcement learning deficits associated with schizophrenia.9 Through frequent repetition of such experiences, and with consistent social and environmental cues, striatal neurons will gradually form associations with these conditioning stimuluses (eg, music, friendly social group) following principles of general reinforcement learning models.44 Such associations are highly dependent on dopamine signalling in the striatum, a core part of learning-related circuits. Through this process of reinforcement learning, the formation of action–outcome associations may be purposefully built, which is especially relevant in people with schizophrenia who typically show difficulty in integrating action–outcome learning to guide choice.9,45
Temporal Discounting
Another barrier to the adoption of PA in people with schizophrenia is that the incentive value of a stimuli is reduced when the expected reward is delayed (ie, temporal discounting is increased). Such temporal discounting of the reward further conflates problems computing the expected value of a reward.46 For example, a person with schizophrenia may not perceive the health benefits of PA as valuable due to poor reinforcement learning and may be further discouraged to continue with activities if the goals they have set up are several months away. Similar problems cause impairments in the ability to anticipate pleasure and recall pleasure retrospectively, resulting in less likely engagement in activities based on an expectation that the effort required to engage in activity will not be worth it.47 Social influences may be helpful to minimise the impact of these disrupted anticipatory reward processes on the likelihood of maintaining the newly adopted activities.29
Based on habit theories (eg, Rothman et al, 2009),21 maintenance of PA may be supported through a supportive environment (eg, easy access to facilities) and positive social connections while exercising, which would lower the perceived costs of the new behaviour, including the amount of decision-making and resources required by an individual.29 As such, carefully designing activities so they are pleasurable and maximise enjoyment48 in the adoption phase is essential, and could include diverse strategies such as using fun games, exercising within green spaces,49 and offering sport and recreation that are closely linked with hedonic experiences.50,51 To address the anticipatory reward deficits,21 staff involved in the support of PA adoption could affirm any positive feelings individuals may have after engaging in PA, and later help them to recall and discuss these positive memories when the individual is considering future PA.52 Further, supervisors and facilitators aware of the negative symptoms of schizophrenia, related to motivational impairments, can ensure that a more reward-driven approach (eg, provide constant feedback and immediate priming with motivating rewards) is adopted during the uptake of activities to reduce high drop-out in this population. During the maintenance of activities, they can also transition to supporting an individual’s goal-directed action by assisting more actively with planning a PA routine and strengthening the associations with long-term goals.
Planning Deficits
Executive functions, and specifically planning, have been consistently shown to be impaired in schizophrenia.53,54 Evidence suggests that impaired executive functioning is associated with reduced activation in the left dorsolateral prefrontal cortex, rostral/dorsal anterior cingulate cortex, left thalamus, and inferior/posterior cortical areas55 and that planning deficits in individuals with schizophrenia are not task specific, but rather affect central cognitive processes critical for planned behaviour.56 It is, therefore, likely that motivation for PA in people with schizophrenia is impacted by a deregulation of planning and decision-making. Given an increasing body of evidence that supports the role of specific detailed plans of when, where, with whom, and how people will be active (ie, action planning) and if–then plans that structure PA as part of a routine (ie, implementation intentions)31 in enhancing motivation and PA behaviour, the observed planning deficits in people with schizophrenia could be addressed by implementing strategies that would involve an individual in formulating specific if–then plans (eg, “when the support worker arrives on Monday morning, it is time for a 30-minute walk”).34 Such strategies may also have the benefit of leading to long-term habits for PA.57,58
Further, impaired executive control and planning skills are also hypothesised to be reflected in an individual’s self-regulatory capacity, which includes processes of self-monitoring, self-evaluation and self-reinforcement.29 To support these processes externally, those involved in facilitating PA, such as clinicians, exercise professionals, disability support workers or peer health coaches, may assist individuals with schizophrenia so that PA activities are incorporated explicitly into their daily and weekly schedules, and provide assistance with planning and problem solving regarding transport to PA if required, given this can be a barrier to engagement.20,42 Regular supervision by an exercise professional such as a physiotherapist or accredited exercise physiologist is likely to be beneficial when individuals become more motivated but have not yet developed habitual PA engagement.15 At this stage, supervisors can assist with establishing a concrete plan of activities leading to a specific long-term goal, monitoring progress, or selecting a new strategy or activity to pursue the goal if needed.
Effective monitoring and providing real-time memory aids of planned and scheduled activities could be achieved by the use of digital health interventions, such as mobile apps that use peer community, goal and achievement tracking, along with structured motivational coaching.59 More recent evidence shows that people with severe mental illness and specifically with schizophrenia are accepting of and willing to use digital health tools like mobile apps for improving care.60,61 This approach could also be complemented by regular motivational sessions, led by a professional from a health-related field (eg, psychology, physiology, nutrition), where progress towards goals is assessed in the context of PA guidelines and benefits, combined with self-monitoring of PA using fitness trackers providing real-time feedback.59
Goal-directed action and associative learning are driven primarily by the dorsomedial (associative) striatum.9,55 However, in schizophrenia, associative striatal dysfunction compromises goal-directed action, making it difficult to integrate action–outcome learning to guide choice.9 To elicit more goal-directed control for PA, facilitating self-determined motivation by identifying a person’s reasons for wanting to be physically active and goal they want to achieve with PA may boost self-regulatory functioning, and enhance the perceived value of the target behaviour.62 While the above strategies broadly aim to establish learned context–action associations, which are thought to trigger automatically cued behavioural activities (eg, when a specific music plays or a specific support person arrives at the same time each week, it is time for a specific exercise routine), habit-formation models become more dominant for designing interventions, once the motivation for PA engagement is sufficiently elicited with rewarding experiences and other rewards.27
Behavioural Maintenance Towards Habit Formation
Increasing the motivation for PA is crucial during the adoption stage when a person starts engaging in regular PA. At this stage, support requires frequent, novel rewards and planning strategies. In contrast, habitual responding is a self-initiated action less dependent on rewards. The process of habit formation is thought to rely on the activity in the dorsolateral (sensori-motor) striatum, rather than the associative or limbic striatum.9 As such, to facilitate long-term and habitual PA engagement, it is important to tap into individuals’ intrinsic motivations (eg, because it is enjoyable),63 which may lead to more regular behaviour–reward pairings that can support habit formation.
One way of encouraging maintenance of PA that could lead to habit formation is establishing intervention conditions that are conducive to integration of PA within a person’s value system and strengthening autonomous motivation, a concept derived from self-determination theory (SDT).64 There is growing empirical evidence on the importance of autonomous motivation in adopting and maintaining PA in people with severe mental illness, and specifically in schizophrenia.65 For an overview of intervention studies in this area and the associations of different motivational constructs, see Farholm and Sorensen.66 According to SDT, autonomously motivated individuals engage in an activity out of personal interest and satisfaction, experiencing a sense of personal choice and autonomy in pursuing the behaviour, which is not contingent on external demands or incentives. Evidence from studies with people with schizophrenia support the theoretically-predicted pattern of those who engage in regular PA having more self-determined forms of motivation (performing activities out of inherent interest/enjoyment and because it is personally valued).67 The role of autonomous motivation has also been highlighted in increasing the acceptability of lifestyle (diet and exercise) interventions within a residential rehabilitation setting for people with severe mental illness.51
According to SDT, autonomous motivation can be facilitated in environments that promote psychological needs for autonomy (experiencing psychological freedom when engaging in physical activities), relatedness (being socially connected) and competence (feeling effective in doing the exercises or achieving the outcomes).64 Strategies to increase autonomous motivation for PA (rather than being externally motivated) should facilitate satisfaction of these needs, including using mobile apps or co-design principles, where service users are consulted on their preferences regarding the development and implementation of exercise interventions. In people with schizophrenia with low motivation for PA, clinicians can support their sense of autonomy by using autonomy supportive language (eg, “could”, “choose”, rather than “should” or “have to”), offering choices around the types of PA, and considering an individual’s preferences (eg, individual/group setting). Activities tailored to an individual’s current ability and provided with clear instructions may help with strengthening a sense of competency.68 Based on goal-setting theory, discovering individuals’ aspirations for PA and assistance with developing personalised goals is vital; utilising SMARTS goals (specific, measurable, achievable, realistic, time-bound, and self-determined) has been an established strategy.68 However, for inactive individuals, prior research has shown that the pursuit of SMARTS goals can lead to reduced pleasure, enjoyment and motivation as well as individuals’ efforts to engage in future PA.69 Goals that are non-specific and focus on the process (eg, “do your best”, “see how active you can be”), rather than a specific amount of PA may, therefore, be preferable.
This stage of PA engagement also requires a shift from extrinsic motivation and rewards towards more intrinsic forms of regulation. Behaviour strategies to achieve this shift include encouragement, personalised goal setting, and individualisation of the program to suit an individual’s capacities and preferences.66,70 Exercise professionals and mental health clinicians can play an important role in helping individuals to connect actions with their aspirations to assist with the development of more autonomous motivation. For example, facilitators may assist individuals to reflect on their successes and develop positive self-talk statements, such as “every time I do PA/exercise/sport, I am getting closer to my goal of improving my fitness”.71 To progressively reduce dependence on rewards and other external reinforcement, it is useful to conceptualise optimal behaviour as determined not only by the rewards obtained but also by the minimization of the cost related to a specific set of actions needed to accomplish the action.72
A schematic representation of the different stages of PA across time, starting with adoption (days/weeks) and, ideally, leading to long-term maintenance or habit formation (months/years), with associated motivational and neurobiological processes and the proposed strategies to facilitate behaviour change in people with schizophrenia is provided in Table 1. While behaviour change models that are currently applied in clinical practice to increase PA in the general population,73 and specifically in people with severe mental illness,74 such as SDT64 or the transtheoretical model75 that takes a more macro-level perspective, can be helpful in encouraging individuals in the general population to engage in more PA,73 the biopsychological perspective on promoting PA in individuals with schizophrenia, depicted in Table 1, adds value to these existing models by highlighting the neurobiological processes that may hinder the efforts of people living with schizophrenia, clinicians, peer support workers, and other carers in facilitating a positive behaviour change (ie, increased PA engagement). We propose that, by understanding the altered dopaminergic pathways in the brain of individuals with schizophrenia that are involved in motivation and behaviour change, the intervention strategies can be tailored to compensate or, through engaging habitual, autonomic processes,76 to by-pass some of the unique, and pronounced, cognitive and motivational deficits experienced by people with schizophrenia.
Conclusions and Future Directions
While evidence supports the significant benefits of PA on a wide range of domains, people with schizophrenia still engage in insufficient PA to achieve health benefits.2 Those with high metabolic or cardiovascular risk could especially benefit from increased PA engagement.
Through a biopsychological perspective, we illustrated how neurobiological dysfunction associated with schizophrenia may impact motivation for PA, which can contribute to poor adoption and maintenance of PA behaviour. With this understanding—and acknowledging that our perspective is not based on a systematic review of the literature, but rather presents an integration of key findings from relevant disciplines—it is essential that PA and lifestyle interventions for people with schizophrenia incorporate strategies that enhance motivational processes through maximising the reward value and facilitating satisfaction of the psychological needs of autonomy, competency and relatedness to promote autonomous motivation. When promoting PA in people with schizophrenia, it is important to tailor the intervention targets to an individual’s phase of PA engagement. Identifying whether an individual is at the stage of adopting or initiating a PA routine or is already headed towards behaviour maintenance and habit formation can inform clinicians’ decision-making regarding the most appropriate motivational processes to target and the relevant behaviour change strategies. Such individualised interventions should be informed by further research into the modifiable mechanisms underlying motivation for PA in schizophrenia, with consideration of different stages of schizophrenia (early/chronic psychosis) and across different settings (eg, in-/out-patient).
Additionally, habit formation theory shows promise in potentially by-passing the prominent negative and other cognitive symptoms that present a challenge to increasing PA, by fostering a cognitively less effortful and, as such, more association-based engagement in PA. To support people with schizophrenia in the formation of habitual PA, it may be helpful to assist with planning to ensure a consistent PA routine is practised regularly and to the point of being encoded in the memory as motor-cue associations. Future research should test the potential value of habit formation theory and systematically evaluate the potential of specific behaviour change techniques for increasing motivation for and engagement in PA in people with schizophrenia.
Finally, highlighting the recommendation of the Lancet Commission on physical health comorbidity of people with mental illness,2 the assessment of PA should become complementary to anthropomorphic measurement, to create a prompt need for a multidisciplinary approach to increase PA levels in people with schizophrenia and, thus, to improve their physical and mental health. With clinical guidelines increasingly recognising the need for the assessment of PA within routine clinical care, it may be timely that such assessment would also include a measure of motivation or behavioural regulation in PA which could inform the development of a tailored, person-centred plan to promote autonomous motivation for PA. Our intention is also to highlight the value of PA as a modifiable lifestyle factor which can support schizophrenia treatment, in the hope that the identified strategies to address the known neurobiological challenges of schizophrenia will assist clinicians and people with schizophrenia in increasing PA engagement and contribute to further research of this important health behaviour.
Disclosure
Dr Nicola Warren reports personal fees from Otsuka, personal fees from Lundbeck, personal fees from Janssen, outside the submitted work. DS is funded in part by an NHMRC Investigator Grant (GNT1194635). SLR is funded by an NHMRC Senior Research Fellowship (GNT1154651). The authors report no conflicts of interest in this work.
References
1. Crider A. Schizophrenia: A Biopsychological Perspective. Routledge; 2020.
2. Firth J, Siddiqi N, Koyanagi A, et al. The lancet psychiatry commission: a blueprint for protecting physical health in people with mental illness. Lancet Psychiatry. 2019;6(8):675–712. doi:10.1016/S2215-0366(19)30132-4
3. Laursen TM, Nordentoft M, Mortensen PB. Excess early mortality in schizophrenia. Annu Rev Clin Psychol. 2014;10(1):425–448. doi:10.1146/annurev-clinpsy-032813-153657
4. Firth J, Solmi M, Wootton RE, et al. A meta-review of “lifestyle psychiatry”: the role of exercise, smoking, diet and sleep in the prevention and treatment of mental disorders. World Psychiatry. 2020;19(3):360–380. doi:10.1002/wps.20773
5. Soundy A, Freeman P, Stubbs B, Probst M, Coffee P, Vancampfort D. The transcending benefits of physical activity for individuals with schizophrenia: a systematic review and meta-ethnography. Psychiatry Res. 2014;220(1–2):11–19. doi:10.1016/j.psychres.2014.07.083
6. Rebar AL, Taylor A. Physical activity and mental health; it is more than just a prescription. Ment Health Phys Act. 2017;13:77–82. doi:10.1016/j.mhpa.2017.10.004
7. Bora E, Akdede B, Alptekin K. The relationship between cognitive impairment in schizophrenia and metabolic syndrome: a systematic review and meta-analysis. Psychol Med. 2017;47(6):1030–1040. doi:10.1017/S0033291716003366
8. Sumiyoshi T, Kunugi H, Nakagome K. Serotonin and dopamine receptors in motivational and cognitive disturbances of schizophrenia. Front Neurosci. 2014;8:395. doi:10.3389/fnins.2014.00395
9. Conn K-A, Burne TH, Kesby JP. Subcortical dopamine and cognition in schizophrenia: looking beyond psychosis in preclinical models. Front Neurosci. 2020;14:542. doi:10.3389/fnins.2020.00542
10. Salamone JD, Yohn SE, López-Cruz L, San Miguel N, Correa M. Activational and effort-related aspects of motivation: neural mechanisms and implications for psychopathology. Brain. 2016;139(5):1325–1347. doi:10.1093/brain/aww050
11. Joshi YB, Thomas ML, Braff DL, et al. Anticholinergic medication burden–associated cognitive impairment in schizophrenia. Am J Psychiatry. 2021;178(9):838–847. doi:10.1176/appi.ajp.2020.20081212
12. Fervaha G, Takeuchi H, Lee J, et al. Antipsychotics and amotivation. Neuropsychopharmacology. 2015;40(6):1539–1548. doi:10.1038/npp.2015.3
13. Ashdown-Franks G, Firth J, Carney R, et al. Exercise as medicine for mental and substance use disorders: a meta-review of the benefits for neuropsychiatric and cognitive outcomes. Sports Med. 2020;50(1):151–170. doi:10.1007/s40279-019-01187-6
14. Firth J, Cotter J, Elliott R, French P, Yung AR. A systematic review and meta-analysis of exercise interventions in schizophrenia patients. Psychol Med. 2015;45(7):1343–1361. doi:10.1017/S0033291714003110
15. Vancampfort D, Rosenbaum S, Schuch FB, Ward PB, Probst M, Stubbs B. Prevalence and predictors of treatment dropout from physical activity interventions in schizophrenia: a meta-analysis. Gen Hosp Psychiatry. 2016;39:15–23. doi:10.1016/j.genhosppsych.2015.11.008
16. Firth J, Rosenbaum S, Stubbs B, Gorczynski P, Yung AR, Vancampfort D. Motivating factors and barriers towards exercise in severe mental illness: a systematic review and meta-analysis. Psychol Med. 2016;46(14):2869–2881. doi:10.1017/S0033291716001732
17. Roberts SH, Bailey JE. An ethnographic study of the incentives and barriers to lifestyle interventions for people with severe mental illness. J Adv Nurs. 2013;69(11):2514–2524. doi:10.1111/jan.12136
18. Leutwyler H, Hubbard EM, Jeste DV, Vinogradov S. “We’re not just sitting on the periphery”: a staff perspective of physical activity in older adults with schizophrenia. Gerontologist. 2013;53(3):474–483. doi:10.1093/geront/gns092
19. Deighton S, Addington J. Exercise Practices of Young People at Their First Episode of Psychosis. Elsevier Science; 2014.
20. Happell B, Scott D, Platania-Phung C, Nankivell J. Nurses’ views on physical activity for people with serious mental illness. Ment Health Phys Act. 2012;5(1):4–12. doi:10.1016/j.mhpa.2012.02.005
21. Rothman AJ, Sheeran P, Wood W. Reflective and automatic processes in the initiation and maintenance of dietary change. Ann Behav Med. 2009;38(suppl_1):s4–s17. doi:10.1007/s12160-009-9118-3
22. Barrouillet P. Dual-process theories and cognitive development: advances and challenges. Dev Rev. 2011;31(2–3):79–85. doi:10.1016/j.dr.2011.07.002
23. Arnautovska U, Fleig L, O’Callaghan F, Hamilton K. A longitudinal investigation of older adults’ physical activity: testing an integrated dual-process model. Psychol Health. 2017;32(2):166–185. doi:10.1080/08870446.2016.1250273
24. Kim S-I. Neuroscientific model of motivational process. Front Psychol. 2013;4:98. doi:10.3389/fpsyg.2013.00098
25. Michie S, Abraham C, Whittington C, McAteer J, Gupta S. Effective techniques in healthy eating and physical activity interventions: a meta-regression. Health Psychol. 2009;28(6):690. doi:10.1037/a0016136
26. Lally P, Gardner B. Promoting habit formation. Health Psychol Rev. 2013;7(sup1):S137–S158. doi:10.1080/17437199.2011.603640
27. Gardner B, Rebar AL. Habit formation and behavior change. In: Oxford Research Encyclopedia of Psychology. Oxford; 2019.
28. Wood W, Rünger D. Psychology of habit. Ann Rev Psychol. 2016;67(1):289–314. doi:10.1146/annurev-psych-122414-033417
29. Kwasnicka D, Dombrowski SU, White M, Sniehotta F. Theoretical explanations for maintenance of behaviour change: a systematic review of behaviour theories. Health Psychol Rev. 2016;10(3):277–296. doi:10.1080/17437199.2016.1151372
30. Sheeran P. Intention—behavior relations: a conceptual and empirical review. Eur Rev Soc Psychol. 2002;12(1):1–36. doi:10.1080/14792772143000003
31. Sniehotta FF. Towards a theory of intentional behaviour change: plans, planning, and self-regulation. Br J Health Psychol. 2009;14(2):261–273. doi:10.1348/135910708X389042
32. Schwarzer R. Self-efficacy in the adoption and maintenance of health behaviours: theoretical approaches and a new model. In: Self-Efficacy: Thought Control of Action. Vol. 217. Washington, DC: Hemisphere; 1992:242.
33. Ajzen I. The theory of planned behaviour is alive and well, and not ready to retire: a commentary on Sniehotta, Presseau, and Araújo-Soares. Health Psychol Rev. 2015;9(2):131–137. doi:10.1080/17437199.2014.883474
34. Webb TL, Sheeran P. Does changing behavioral intentions engender behavior change? A meta-analysis of the experimental evidence. Psychol Bull. 2006;132(2):249. doi:10.1037/0033-2909.132.2.249
35. Heath GW, Parra DC, Sarmiento OL, et al. Evidence-based intervention in physical activity: lessons from around the world. Lancet. 2012;380(9838):272–281. doi:10.1016/S0140-6736(12)60816-2
36. Ding D, Varela AR, Bauman AE, et al. Towards better evidence-informed global action: lessons learnt from the lancet series and recent developments in physical activity and public health. Br J Sports Med. 2020;54(8):462–468. doi:10.1136/bjsports-2019-101001
37. Vancampfort D, Rosenbaum S, Probst M, et al. Promotion of cardiorespiratory fitness in schizophrenia: a clinical overview and meta‐analysis. Acta Psychiatr Scand. 2015;132(2):131–143. doi:10.1111/acps.12407
38. Berridge KC, Robinson TE. What is the role of dopamine in reward: hedonic impact, reward learning, or incentive salience? Brain Res Rev. 1998;28(3):309–369. doi:10.1016/s0165-0173(98)00019-8
39. Tanaka SC, Doya K, Okada G, Ueda K, Okamoto Y, Yamawaki S. Prediction of immediate and future rewards differentially recruits cortico-basal ganglia loops. In: Behavioral Economics of Preferences, Choices, and Happiness. Springer; 2016:593–616.
40. Galaj E, Ranaldi R. Neurobiology of reward-related learning. Neurosci Biobehav Rev. 2021;124:224–234. doi:10.1016/j.neubiorev.2021.02.007
41. Whybird G, Nott Z, Savage E, et al. Promoting quality of life and recovery in adults with mental health issues using exercise and nutrition intervention. Int J Ment Health. 2020;2020;1–24.
42. Carless D, Douglas K. Social support for and through exercise and sport in a sample of men with serious mental illness. Issues Ment Health Nurs. 2008;29(11):1179–1199. doi:10.1080/01612840802370640
43. McDevitt J, Snyder M, Miller A, Wilbur J. Perceptions of barriers and benefits to physical activity among outpatients in psychiatric rehabilitation. J Nurs Scholarsh. 2006;38(1):50–55. doi:10.1111/j.1547-5069.2006.00077.x
44. Graybiel AM. Habits, rituals, and the evaluative brain. Annu Rev Neurosci. 2008;31(1):359–387. doi:10.1146/annurev.neuro.29.051605.112851
45. Suetani S, Baker A, Garner K, et al. Impairments in goal-directed action and reversal learning in a proportion of individuals with psychosis. Cogn Affect Behav Neurosci. 2022;22;1–14.
46. Schlosser D, Campellone T, Kim D, et al. Feasibility of PRIME: a cognitive neuroscience-informed mobile app intervention to enhance motivated behavior and improve quality of life in recent onset schizophrenia. JMIR Res Protoc. 2016;5(2):e5450. doi:10.2196/resprot.5450
47. Ritch J, Velligan DI. The Motivation and Engagement Program (MOVE) for Negative Symptoms and Functional Impairment in Schizophrenia; 2015.
48. Teychenne M, White RL, Richards J, Schuch FB, Rosenbaum S, Bennie JA. Do we need physical activity guidelines for mental health: what does the evidence tell us? Ment Health Phys Act. 2020;18:100315. doi:10.1016/j.mhpa.2019.100315
49. Barton J, Pretty J. What is the best dose of nature and green exercise for improving mental health? A multi-study analysis. Environ Sci Technol. 2010;44(10):3947–3955. doi:10.1021/es903183r
50. Soundy A, Roskell C, Stubbs B, Probst M, Vancampfort D. Investigating the benefits of sport participation for individuals with schizophrenia: a systematic review. Psychiatr Danub. 2015;27(1):0–13.
51. Korman N, Fox H, Skinner T, et al. Feasibility and acceptability of a student-led lifestyle (diet and exercise) intervention within a residential rehabilitation setting for people with severe mental illness, GO HEART (group occupation, health, exercise and rehabilitation treatment). Front Psychiatry. 2020;11:319. doi:10.3389/fpsyt.2020.00319
52. Painter JM, Kring AM. Toward an understanding of anticipatory pleasure deficits in schizophrenia: memory, prospection, and emotion experience. J Abnorm Psychol. 2016;125(3):442. doi:10.1037/abn0000151
53. Kluwe-Schiavon B, Sanvicente-Vieira B, Kristensen C, Grassi-Oliveira R. Executive functions rehabilitation for schizophrenia: a critical systematic review. J Psychiatr Res. 2013;47(1):91–104. doi:10.1016/j.jpsychires.2012.10.001
54. Eisenberg DP, Berman KF. Executive function, neural circuitry, and genetic mechanisms in schizophrenia. Neuropsychopharmacology. 2010;35(1):258–277. doi:10.1038/npp.2009.111
55. Kesby JP, Murray GK, Knolle F. Neural circuitry of salience and reward processing in psychosis. In: Biological Psychiatry Global Open Science. Elsevier; 2021.
56. Holt DV, Wolf J, Funke J, Weisbrod M, Kaiser S. Planning impairments in schizophrenia: specificity, task independence and functional relevance. Schizophr Res. 2013;149(1–3):174–179. doi:10.1016/j.schres.2013.06.018
57. Verplanken B, Faes S. Good intentions, bad habits, and effects of forming implementation intentions on healthy eating. Eur J Soc Psychol. 1999;29(5–6):591–604. doi:10.1002/(SICI)1099-0992(199908/09)29:5/6<591::AID-EJSP948>3.0.CO;2-H
58. Holland RW, Aarts H, Langendam D. Breaking and creating habits on the working floor: a field-experiment on the power of implementation intentions. J Exp Soc Psychol. 2006;42(6):776–783. doi:10.1016/j.jesp.2005.11.006
59. Naslund JA, Aschbrenner KA, Scherer EA, McHugo GJ, Marsch LA, Bartels SJ. Wearable devices and mobile technologies for supporting behavioral weight loss among people with serious mental illness. Psychiatry Res. 2016;244:139–144. doi:10.1016/j.psychres.2016.06.056
60. Firth J, Torous J. Smartphone apps for schizophrenia: a systematic review. JMIR Mhealth Uhealth. 2015;3(4):e4930. doi:10.2196/mhealth.4930
61. Berry N, Lobban F, Emsley R, Bucci S. Acceptability of interventions delivered online and through mobile phones for people who experience severe mental health problems: a systematic review. J Med Internet Res. 2016;18(5):e5250. doi:10.2196/jmir.5250
62. Vancampfort D, De Hert M, Vansteenkiste M, et al. The importance of self-determined motivation towards physical activity in patients with schizophrenia. Psychiatry Res. 2013;210(3):812–818. doi:10.1016/j.psychres.2013.10.004
63. Teixeira PJ, Carraça EV, Markland D, Silva MN, Ryan RM. Exercise, physical activity, and self-determination theory: a systematic review. Int J Behav Nutr Phys Act. 2012;9(1):78. doi:10.1186/1479-5868-9-78
64. Deci EL, Ryan RM. Self-determination theory: a macrotheory of human motivation, development, and health. Can Psychol. 2008;49(3):182. doi:10.1037/a0012801
65. Vancampfort D, De Hert M, Stubbs B, et al. Negative symptoms are associated with lower autonomous motivation towards physical activity in people with schizophrenia. Compr Psychiatry. 2015;56:128–132. doi:10.1016/j.comppsych.2014.10.007
66. Farholm A, Sørensen M. Motivation for physical activity and exercise in severe mental illness: a systematic review of cross-sectional studies. Int J Ment Health Nurs. 2016;25(2):116–126. doi:10.1111/inm.12217
67. Vancampfort D, Stubbs B, Venigalla SK, Probst M. Adopting and maintaining physical activity behaviours in people with severe mental illness: the importance of autonomous motivation. Prev Med. 2015;81:216–220. doi:10.1016/j.ypmed.2015.09.006
68. Swann C, Rosenbaum S. Do we need to reconsider best practice in goal setting for physical activity promotion? Br J Sports Med. 2018;52:485–486.
69. Swann C, Jackman PC, Lawrence A, et al. The (over) use of SMART goals for physical activity promotion: a narrative review and critique. Health Psychol Rev. 2022;2022:1–16.
70. Matthews EW, Cowman M, Brannigan M, et al. Implementing experience-based co-design to develop a physical activity programme in recovery-focused outpatient mental health services. Int J Ther Rehabil. 2022;29(4):1–16. doi:10.12968/ijtr.2021.0101
71. Beck AT, Grant PM, Inverso E, Brinen AP, Perivoliotis D. Recovery-Oriented Cognitive Therapy for Serious Mental Health Conditions. New York (NY): Guilford Press; 2021.
72. Graybiel AM, Grafton ST. The striatum: where skills and habits meet. Cold Spring Harb Perspect Biol. 2015;7(8):a021691. doi:10.1101/cshperspect.a021691
73. Rhodes RE, McEwan D, Rebar AL. Theories of physical activity behaviour change: a history and synthesis of approaches. Psychol Sport Exerc. 2019;42:100–109. doi:10.1016/j.psychsport.2018.11.010
74. Gorczynski P, Faulkner G, Greening S, Cohn T. Exploring the construct validity of the transtheoretical model to structure physical activity interventions for individuals with serious mental illness. Psychiatr Rehabil J. 2010;34(1):61. doi:10.2975/34.1.2010.61.64
75. Prochaska JO, DiClemente CC. Transtheoretical therapy: toward a more integrative model of change. Psychotherapy. 1982;19(3):276. doi:10.1037/h0088437
76. Rebar AL, Dimmock JA, Jackson B, et al. A systematic review of the effects of non-conscious regulatory processes in physical activity. Health Psychol Rev. 2016;10(4):395–407. doi:10.1080/17437199.2016.1183505
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.