")
Back to Journals » International Journal of General Medicine » Volume 15
Biomechanical Assessment of Tilted Mandibular Second Molars with Full-Crown Adjacent to Implant-Supported Restoration: 3D Finite Element Analysis
Authors Li N, Li Y, Gao Y, Jiang L
Received 9 February 2022
Accepted for publication 23 March 2022
Published 29 March 2022 Volume 2022:15 Pages 3459—3470
DOI https://doi.org/10.2147/IJGM.S353134
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ning Li,* Yusi Li,* Yiming Gao, Liting Jiang
Department of Stomatology, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine; College of Stomatology, Shanghai Jiao Tong University, Shanghai, 200025, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liting Jiang; Yiming Gao, Department of Stomatology, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine; College of Stomatology, Shanghai Jiao Tong University, No. 197, The Second Ruijin Road, Huangpu District, Shanghai, 200025, People’s Republic of China, Tel +86 21 64370045, Email [email protected]; [email protected]
Purpose: The aim of this study was to investigate the effects of tooth root inclination and crown preparation angulation on the stress distribution of tilted second molars, supporting structures and adjacent implant by using the finite element analysis method.
Materials and Methods: 3D finite element models of tilted second molar and tooth-supporting structures, including the two designs with three different angles of root inclination and crown preparation angulations, were constructed for full-crown restoration. For all models, the stress distribution was analyzed under vertical and oblique loading conditions.
Results: The maximum equivalent stress (MES) increased as root inclination increased, and the highest stress value occurred in the tooth root furcation of the model with 30° root inclination under oblique loading. When root inclination was the same, the MES of each structure was approximate under the same direction load regardless of crown preparation angulation. Higher stress values were found on the tooth root, periodontal ligament, and cortical bone of all models under oblique load compared with vertical load. The highest stress value occurred in the distal adjacent area of implant.
Conclusion: Tooth roots with less than 30° inclination, occlusal preparation parallel to the bite plane and small oblique force loading are recommended as significant considerations for full-crown restoration of a mesial inclined mandibular second molar.
Keywords: tilted mandibular second molar, full-crown restoration, implant, 3D finite element analysis
Introduction
Full-crown restorations can offer successful long-term outcomes and have been widely proposed in prosthetic dentistry for decades. Restorations should allow practitioners to better reproduce natural contours for damaged and tilted teeth.1,2
In clinical practice, it is frequently found that the teeth adjacent to the edentulous area tend to tilt if the space has not been restored in time.3 The conventional approach has utilized a fixed partial denture (FPD) applying teeth tilted less than 24° as the abutment.4 Although tilted molars restored with FPD are expected to be weaker than natural teeth, the application can be considered a cost-effective and efficient alternative design option.
Recently, the development of implant technology has facilitated the scope of fixed denture prosthesis expansion. The missing tooth can be replaced by an implant, which avoids the tilted molar as an FPD abutment. Therefore, the complex FPD procedure is converted to a single tilted molar restoration. However, for excessively tilted molars, it is usually difficult to decide whether to choose either orthodontic treatment to upright them or to use a full crown (including post-core restorations) to adjust their axial inclination. Although orthodontic management is the ideal choice for tilted teeth, restorations are usually chosen to manage tilted teeth because of their convenience, low time consumption, and low cost.5
In general, the clinical longevity of the restoration can be affected by various factors, such as materials, design, and load. A stable, clinically successful restoration is related to the understanding of biomechanics. Stress analysis is a useful biomechanical tool for predicting the physical responses of a system, for example, the most likely fracture location. Much has been reported on the magnitude and distribution of stress associated with various types of restoration.6,7 However, few reports have described stress changes in mandibular second molars with different inclined angles after full-crown restoration. Previous studies demonstrate that the restorative materials can affect the mechanical response for full-crowns,8,9 but there is a lack of information about inclined root. In addition, few studies have examined how different occlusal surface preparation designs affect the stress distribution in tilted molars and supporting structures.
Therefore, this study aimed to investigate the effects of tooth root inclination and crown preparation angulation design on the stress distribution of tilted second molars, supporting structures and adjacent implant by using the finite element analysis (FEA) method.
Materials and Methods
A cone-beam CT-based (CBCT) technique was used for digital 3-D scanning (MCT-1, Morita, Japan) of the external profile of the tooth and bone. After obtaining the fully consented formal permission of the patient, with a mandibular first molar missing 6 years and a 30° root inclination of the second molar, the preliminary model was reconstructed according to the CBCT data. The Ethics Committee of Ruijin Hospital, Shanghai Jiao Tong University School of Medicine approved the study (2021–357). Next, the two designs were fabricated in terms of the preliminary model. As in the M1 model, a tooth with three angulations of the root from the vertical direction (0°, 15°, 30°) and simulated ideal alveolar bone were assembled. For the M2 model, a tooth with three angulations (10°, 20°, 30°) of crown preparation under the condition of 30° root inclination and part of the real alveolar bone with implant restoration was assembled. Standard crown preparations of M1 and M2 were designed with 5° convergence angle and an occlusal surface parallel to the bite plane. All models were restored computationally with a zirconia crown and cemented with the same resin cement.
SolidWorks 2018 software (SolidWorks Corporation, MA) was used to design diverse molar structures and their supporting structures (Figures 1 and 2). A periodontal ligament (PDL) zone with a 0.2 mm thickness was constructed to surround the outer surface of the portion of the two roots, starting from its tooth-bone junction. The cortical bone surrounding the cancellous bone core was 2 mm thick. Furthermore, the crown preparation geometry, corresponding resin cement layer (0.1 mm) and full-crown restoration were reconstructed sequentially under the unrestored molar. The final model was composed of 6 parts, as shown in Figure 1. Subsequently, the adjacent implant with 4.1mm diameter and corresponding abutment was assembled and shown in Figure 2.
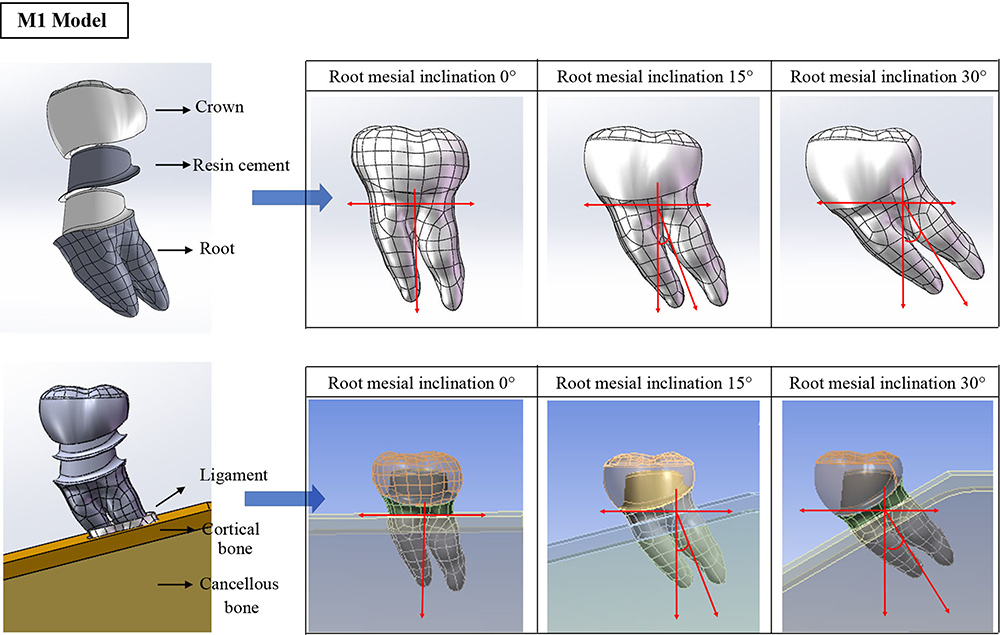 |
Figure 1 Models (M1) with three angles of tooth root from the vertical direction (0°, 15°, 30°) and exploded view of simulation model design. |
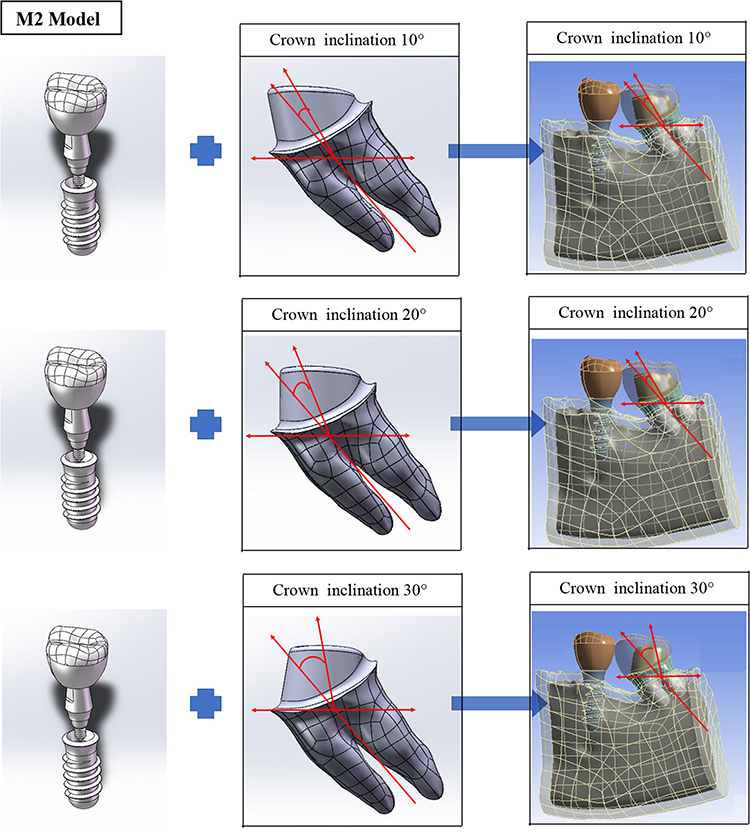 |
Figure 2 Models (M2) with implant and three angles of crown preparation from the tooth root (10°, 20°, 30°). |
The present work simulates occlusal events during chewing with respect to the stresses transferred to the tooth root, PDLs and alveolar bones due to forces with different directions. ANSYS Workbench R18 (ANSYS Inc., Canonsburg, PA) software was used to import the constructed model to generate a 3-D computational mesh (Figure 3). Mesh trials were first performed to achieve the final analyzed model. The structures of the model were assembled assuming linearly elastic and isotropic homogeneous materials, as shown in Table 1.10–14 Common contact between the assembly parts was assumed to be perfectly bonded, whereas the contact between two crowns was set as no separate.
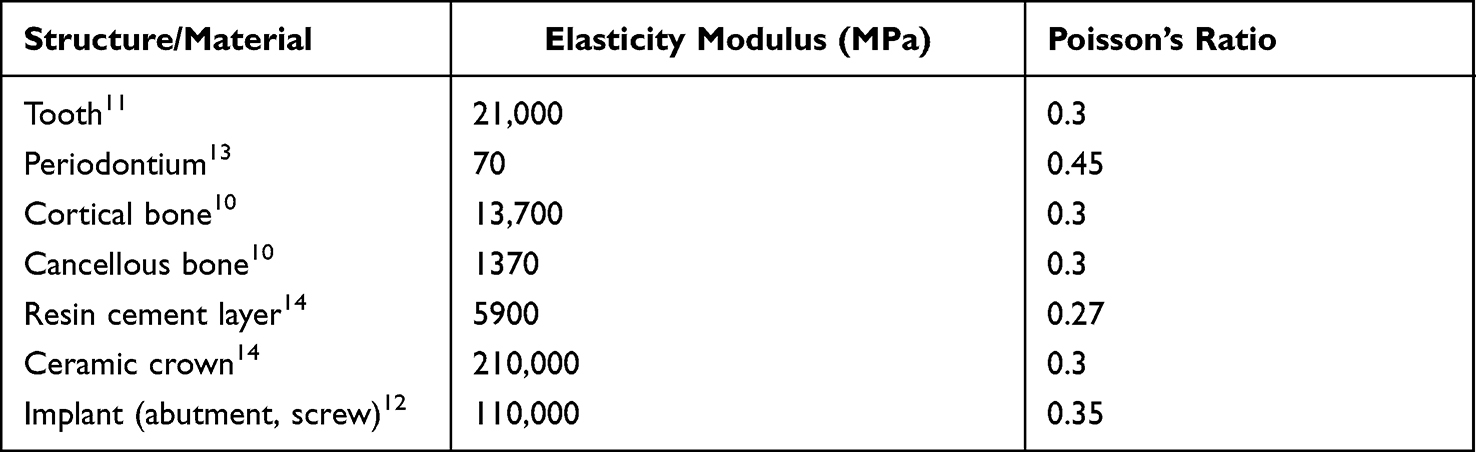 |
Table 1 Distribution of the Mechanical Properties of the Materials |
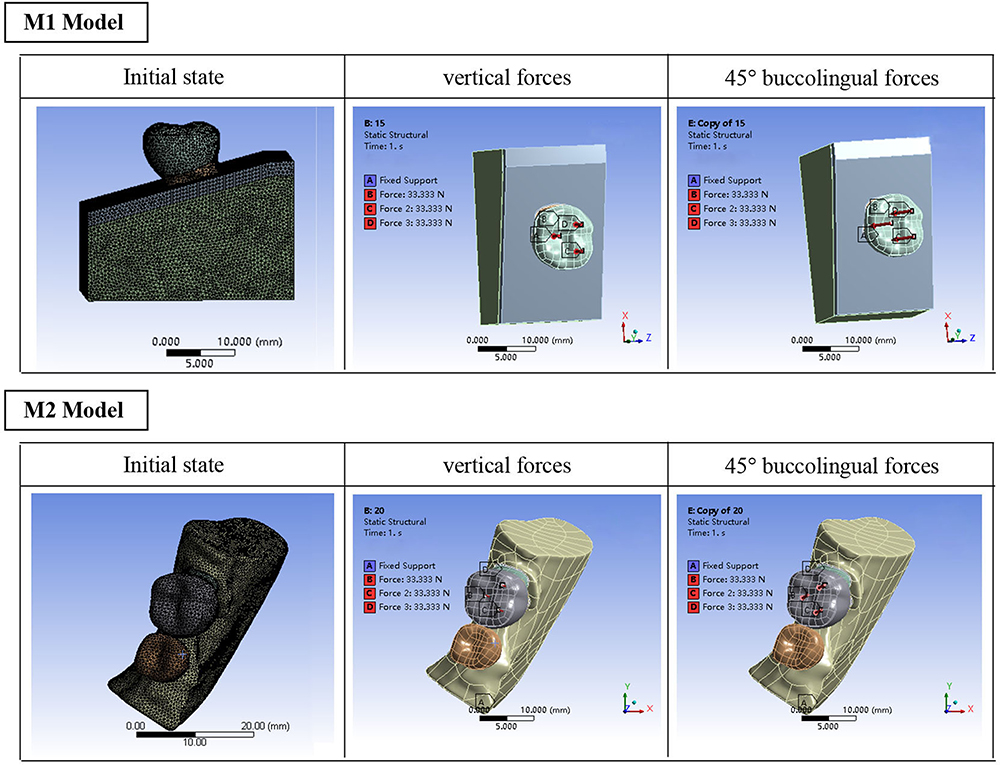 |
Figure 3 M1 and M2 model views of the present mesh, the three loading sites with vertical and 45° buccolingual forces. |
The normal occlusal load was assumed at three points of the modeled occlusal surfaces, which equally shared a force of 100 N. The analysis was carried out according to two angles of the applied force (0°, 45°) from the axial (vertical) direction of the crown.15 Axial and buccolingual forces are shown in Figure 3. For each load direction, a 3D FEA computation was carried out to detect the site and distribution of the stress within each part of the model.
Results
The maximum equivalent stress (MES) values in the tooth root and supporting structures were visualized using shaded images to demonstrate stress distributions.
M1 Model
The stress distribution of the M1 model under vertical and oblique loads is shown in Figure 4. MESs generated within the ligament and cortical bone of the models upon vertical loading were located in the mesial buccal neck, while MESs in cancellous bone were exhibited in the mesial root apical part. When the load direction was oblique, the MES within the above structures shifted to the mesial lingual cervical region, whereas the MES of cancellous bone was still in the mesial apical area. In addition, MES within the tooth root, as root angulation increased to 30°, shifted from the mesial buccal cervical region to the root furcation and reached the highest value. The magnitude of MES within diverse structures is presented in Table 2. The value of MES within the root and cortical region was higher and increased, followed by root inclination from 0° to 30°. Upon oblique loading, there was the same trend and an increase in the magnitude of the MES compared with vertical loading. It is worth noting that the site and value of the MES in the cancellous region were similar regardless of the force load direction.
 |
Table 2 MES Values Generated Within the Tooth Root, Periodontal Ligament, Cortical Bone, and Cancellous Bone of the Three Models as a Result of the Analyzed Occlusal Forces Applied at Different Load Inclinations |
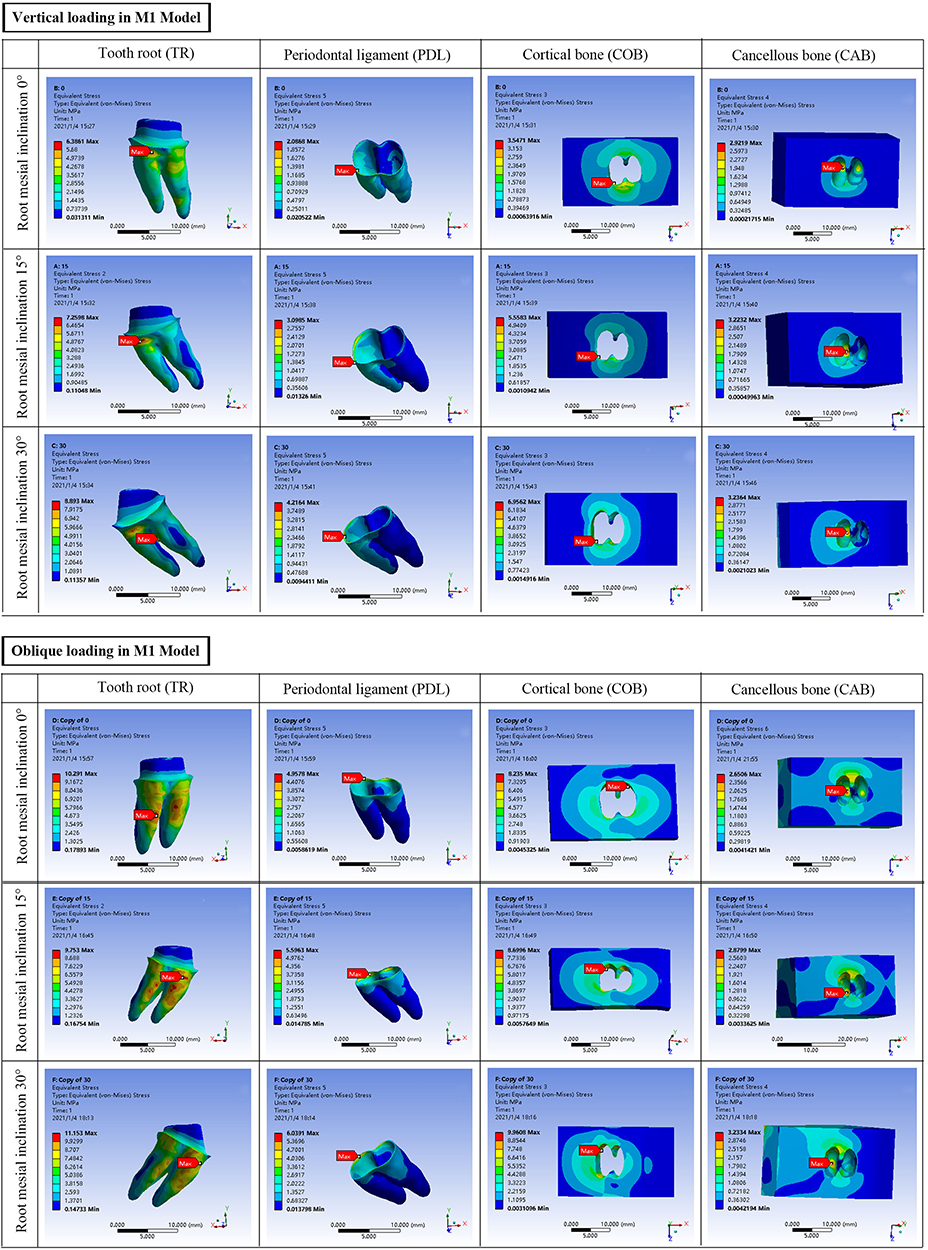 |
Figure 4 Stress distribution and maximum equivalent stress (MES) sites within the tooth root (TR), periodontal ligament (PDL), cortical bone (COB) and cancellous bone (CAB) of the M1 model under vertical load application and oblique load application. |
M2 Model
The M2 model was based on the design of a 30° tilted root from the M1 model. The main stress concentration of this model was on the MES sites and values at PDL, tooth root, cortical bone and implant of the model with the three angles of crown preparation from root. As shown in Figure 5, upon vertical loading, the MES occurred in similar zone of the same structure, and the value was approximate regardless of the crown preparation angle. The MES within the cortical bone shifted to the lingual zone of the alveolar socket and reached the highest value of 42.527 MPa at oblique 100 N loading. Table 3 lists the values of MES generated within three structures of the models designed with different angles of crown preparation at vertical and oblique loading. Moreover, the highest stress value occurred in the distal adjacent area of implant.
 |
Table 3 MES Values Generated Within the Tooth Root, Periodontal Ligament, Cortical Bone and Implant of the Three Models as a Result of the Analyzed Occlusal Forces Applied at Different Load Inclinations |
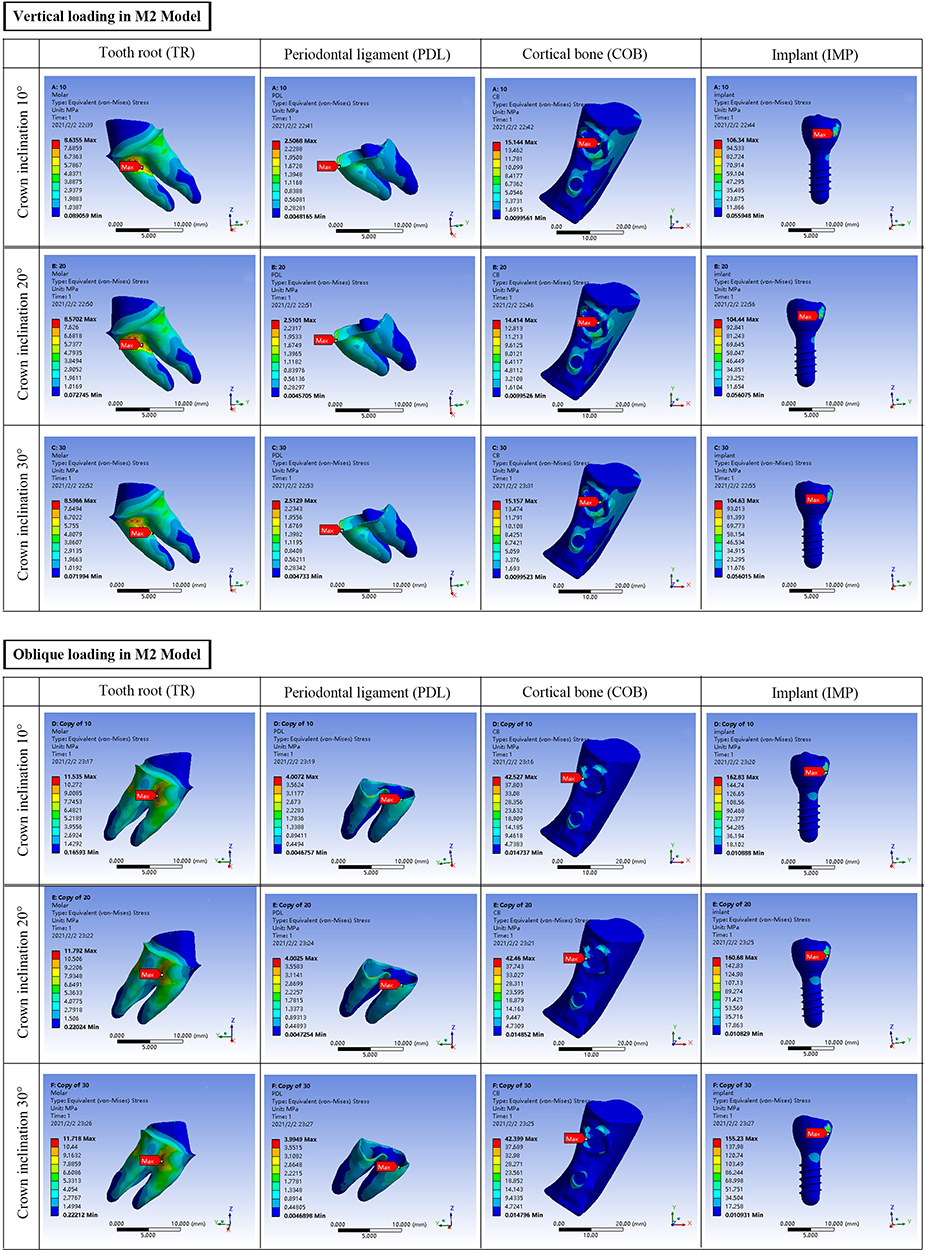 |
Figure 5 Stress distribution and MES sites within the tooth root (TR), periodontal ligament (PDL), cortical bone (COB) and implant (IMP) of M2 model under vertical load application and oblique load application. |
Discussion
It is well known that angled abutments can compensate for the installation of an implant in a nonoptimal position.16 Most FEA studies have reported that increased stress on implants and bone usually remains within physiological limits when abutments are angled.17,18 The present study was inspired by the biomechanics of implant restoration with angled abutments. In comparison with the straight molar, the MES in the root, ligament, and cortical bone of the 30° tilted molar under vertical load increased by 40–50% according to Table 2, which remained less than the stress values of the straight root under oblique load. From the results of stress analysis, the oblique load was the worst condition for all modalities, as it increased the intensity of the stresses and the number of concentration areas due to the lever arm that was formed.19
Tilted molar is responsible for many dental diseases such as food impaction, dental caries, periodontal and occlusion problems, which creates unstable occlusion and improper maintenance of oral hygiene.20 Therefore, it is advisable to initiate treatment as soon as possible to restore arch integrity and a stable occlusion. A previous study indicated an inverse relation between root tilt and the fracture resistance of restored teeth; furthermore, the stress distribution along roots of restored teeth is highly dependent on the mechanical characteristics of the restorative systems.21 With regard to the tilted molar in combination with missing teeth, current solutions of restoration consist of three-unit FPD and implant combined crown restoration. The introduction of FPD may modify the stress distribution around tilted molar abutments because the FPD can share the occlusal force on the tilted molar with the other abutments.22,23 However, the stress concentration of the first premolar was greater than that of the molar, and the pattern of stress distribution in tilted molars was not changed.24 It is appropriate to establish a balance between prosthetic and anatomical concerns when inserting an implant. In comparison with FPD, the single-unit crown has better biomechanical performance due to the force value reduction on the tilted root and bite force direction modification after the occlusal surface has been restored. According to our study results, stress value increased slowly in 15° and 30° tilted root compared to straight root, in addition, the sites of MES both located on the mesial zone when root was straight and 15° inclination. As the angle increased to 30°, MES concentrated on the furcation. The findings indicated that the results of the 30° inclination, especially in oblique loads, presented apparent stress increases and site shifts, which may explain the clinical problem that molars with crown restorations showed a higher prevalence of furcation involvement and attachment loss.25
The choice of full-crown restorative material is crucial for the tilted molar. Because of the trend toward more esthetic and biocompatible restoration, different all-ceramic systems have been developed,26 in which high-strength ceramic materials such as lithium-disilicate glass-ceramic and zirconia gained popularity.27 Since zirconia has higher flexural strength (>1000 MPa)28 than lithium disilicate (about 400 MPa),29 the fracture resistance of monolithic zirconia crowns may be acceptable at tilted molar restoration. Considering that the tilting occlusal surface is restored, excessive load is inevitable to correct, so the 100 N force was selected for the present investigation, which was commonly invoked in similar FEA studies. The magnitude of that force has no influence on achieving the objective of comparing the stresses generated within the periodontium of the three models at different load inclinations.15
Proper preparation can affect the load-bearing capability of restoration.6 Adequate preparation can lead to lower stress in the restoration because of the increased restoration thickness.30 A previous study showed that differences in occlusal preparation designs (anatomic, nonanatomic) did not result in differences in the distribution or amount of stress in pulp, dentin, or bone.31 Thus, concern regarding the preparation angulation of tilted molars was proposed to compare the stress of the M2 model. In Table 3 of the present study, the similar MES values and sites in the same structure can be attributed to the occlusal preparation design parallel to the bite plane. The findings indicated that the parallelism of occlusal surface preparation was more significant than the shape and angulation of preparation. Moreover, the highest stress was detected in the contact area between tilted tooth and implant, which was likely related to clinical problems such as food impaction and porcelain fracture.
Furthermore, the amount of tilting is directly related to the severity of both prosthetic and periodontal problems.32 In the literature, there should be less than 24° degree of tilt of fixed partial denture (FPD) abutment teeth,4 but the reference of single crown inclination has not been ascertained. Interestingly, when the root inclination is less than 30°, a successful computational model can be constructed by software during the crown preparation process. This result is in accordance with the clinical crown preparation with 5° convergence angle because root inclination exceeding 30° leads to difficulty in distal zone preparation. In addition, restored occlusal contact can prevent the stress distribution and MES site of the 30° inclination model from exceeding physiological limits. This might be useful for the design of the 30° inclination as the extreme full-crown restoration of compromise.
In the present study, the mechanics of different root inclinations were simulated using a typical M1 model. Moreover, comparisons of different preparation angles of 30° inclination were performed in vitro. Some of the limitations of the present study include static loads applied directly to the occlusal surfaces,33 which was a considerable simplification of real occlusal forces. In addition, a variety of angle oblique loads should be evaluated to simulate bite force during chewing. Although FEA is a useful tool for analyzing theoretical responses in biological investigations, in vitro studies have limitations over attempts to produce a real clinical situation. This study’s results do not necessarily reflect the clinical performance of the restorative approaches tested. Therefore, it might be considered from the achieved results that full-crown adjacent to implant-supported restoration is an option for 30° tilted molars compared with the conventional three-unit FPD.
Conclusions
Within the limitations of the study, it is possible to ascertain that the greater the inclination of the tooth root was, the higher the stresses that occurred in the tooth roots and supporting structure. Stress distribution within root and supporting structures was higher at oblique load than vertical load except for cancellous bone, whereas MES generated within the root and supporting structure of the model with the same 30° inclination was approximate when the occlusal preparation design parallel to the bite plane. Therefore, crown restoration for tooth roots with less than 30° inclination is acceptable for the mechanical property of structures. Regardless of angle of crown preparation, more attention should be paid on occlusal preparation parallel to the bite plane. In all modalities, the oblique load was the worst condition for full-crown restoration of a mesial inclined mandibular second molar.
Ethical Statement
The study was approved by the Ethics Committee at the Affiliated Ruijin Hospital, Shanghai Jiao Tong University School of Medicine. The guidelines according to the Declaration of Helsinki were followed.
Acknowledgments
This work was supported by National Natural Science Foundation of China (Grant No: 8190030859).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Poggio CE, Ercoli C, Rispoli L, Maiorana C, Esposito M. Metal-free materials for fixed prosthodontic restorations. Cochrane Database Syst Rev. 2017;12(12):Cd009606. doi:10.1002/14651858.CD009606.pub2
2. Abdelaziz KM, Khalil AA, Alsalhi IY, Almufarrij AJ, Mojathel AY. Fracture resistance of tilted premolars restored with different post-core systems. J Int Soc Prevent Community Dentistry. 2017;7(6):344–350. doi:10.4103/jispcd.JISPCD_382_17
3. Stern N, Revah A, Becker A. The tilted posterior tooth. Part I: etiology, syndrome, and prevention. J Prosthet Dent. 1981;46(4):404–407. doi:10.1016/0022-3913(81)90447-9
4. Hood JA, Farah JW, Craig RG. Modification of stresses in alveolar bone induced by a tilted molar. J Prosthet Dent. 1975;34(4):415–421. doi:10.1016/0022-3913(75)90159-6
5. Hou Y, Wu G, Qing H, Zhu Z. Effect of a differently tilted angle of mandibular premolar on fracture resistance of 3 postcore restorations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112(4):518–523. doi:10.1016/j.tripleo.2011.02.027
6. Shahrbaf S, vanNoort R, Mirzakouchaki B, Ghassemieh E, Martin N. Effect of the crown design and interface lute parameters on the stress-state of a machined crown-tooth system: a finite element analysis. Dent Mater. 2013;29(8):e123–e131. doi:10.1016/j.dental.2013.04.002
7. Proos KA, Swain MV, Ironside J, Steven GP. Finite element analysis studies of an all-ceramic crown on a first premolar. Int J Prosthodont. 2002;15(4):404–412.
8. Tribst JPM, Dal Piva AMO, de Jager N, Bottino MA, de Kok P, Kleverlaan CJ. Full-crown versus endocrown approach: a 3D-Analysis of both restorations and the effect of ferrule and restoration material. J Prosthodont. 2021;30(4):335–344. doi:10.1111/jopr.13244
9. Dal Piva AMO, Tribst JPM, Benalcázar Jalkh EB, Anami LC, Bonfante EA, Bottino MA. Minimal tooth preparation for posterior monolithic ceramic crowns: effect on the mechanical behavior, reliability and translucency. Dent Mater. 2021;37(3):e140–e150. doi:10.1016/j.dental.2020.11.001
10. Soares CJ, Raposo LH, Soares PV, et al. Effect of different cements on the biomechanical behavior of teeth restored with cast dowel-and-cores-in vitro and FEA analysis. J Prosthodont. 2010;19(2):130–137. doi:10.1111/j.1532-849X.2009.00527.x
11. Gomez JP, Peña FM, Martínez V, Giraldo DC, Cardona CI. Initial force systems during bodily tooth movement with plastic aligners and composite attachments: a three-dimensional finite element analysis. Angle Orthod. 2015;85(3):454–460. doi:10.2319/050714-330.1
12. Liao SH, Zhu XH, Xie J, Sohodeb VK, Ding X. Influence of trabecular bone on peri-implant stress and strain based on Micro-CT finite element modeling of beagle dog. Biomed Res Int. 2016;2016:3926941. doi:10.1155/2016/3926941
13. Kamposiora P, Papavasilious G, Bayne SC, Felton DA. Finite element analysis estimates of cement microfracture under complete veneer crowns. J Prosthet Dent. 1994;71(5):435–441. doi:10.1016/0022-3913(94)90179-1
14. Zhang S, Lü C, Li JH, Zhu BM, Wang WQ. [Three-dimensional finite element analysis of the influence of an abutment buffer layer on implant stress distribution]. Hua xi kou qiang yi xue za zhi. 2020;38(5):537–540. Chinese. doi:10.7518/hxkq.2020.05.011
15. Abuelenain DA, Ajaj R, El-Bab EI, Hammouda MM. Comparison of stresses generated within the supporting structures of mandibular second molars restored with different crown materials: 3-D finite element analysis (FEA). J Prosthodont. 2015;24(6):484–493. doi:10.1111/jopr.12240
16. Hotinski E, Dudley J. Abutment screw loosening in angulation-correcting implants: an in vitro study. J Prosthet Dent. 2019;121(1):151–155. doi:10.1016/j.prosdent.2018.03.005
17. Saba S. Occlusal stability in implant prosthodontics – clinical factors to consider before implant placement. Journal. 2001;67(9):522–526.
18. Cavallaro J
19. da Fonseca GF, de Andrade GS, Dal Piva AMO, Tribst JPM, Borges ALS. Computer-aided design finite element modeling of different approaches to rehabilitate endodontically treated teeth. J Indian Prosthodont Soc. 2018;18(4):329–335. doi:10.4103/jips.jips_168_18
20. Lundgren D, Kurol J, Thorstensson B, Hugoson A. Periodontal conditions around tipped and upright molars in adults. An intra-individual retrospective study. Eur J Orthod. 1992;14(6):449–455. doi:10.1093/ejo/14.6.449
21. Kondoh Y, Takeda T, Ozawa T, et al. Influence of different post-core systems on impact stress: a pilot study. Open Dent J. 2013;7:162–168. doi:10.2174/1874210601307010162
22. Yang HS, Thompson VP. A two-dimensional stress analysis comparing fixed prosthodontic approaches to the tilted molar abutment. Int J Prosthodont. 1991;4(5):416–424.
23. Jia J, Duan Y, Zhang S, et al. A three-dimensional finite element analysis of a tilted molar as a fixed partial denture abutment. Int Chin J Dent. 2007;7(1):23–26.
24. Chitumalla R, Munaga S, Khare A, Agarwal S, Bhoyar A, Parlani S. Stress distribution among periodontally compromised abutments: a comparative study using three-dimensional finite element analysis. Contemp Clin Dent. 2012;3(4):452–458. doi:10.4103/0976-237x.107439
25. Wang HL, Burgett FG, Shyr Y. The relationship between restoration and furcation involvement on molar teeth. J Periodontol. 1993;64(4):302–305. doi:10.1902/jop.1993.64.4.302
26. Beuer F, Schweiger J, Eichberger M, Kappert HF, Gernet W, Edelhoff D. High-strength CAD/CAM-fabricated veneering material sintered to zirconia copings–a new fabrication mode for all-ceramic restorations. Dent Mater. 2009;25(1):121–128. doi:10.1016/j.dental.2008.04.019
27. Sailer I, Makarov NA, Thoma DS, Zwahlen M, Pjetursson BE. All-ceramic or metal-ceramic tooth-supported fixed dental prostheses (FDPs)? A systematic review of the survival and complication rates. Part I: single crowns (SCs). Dent Mater. 2015;31(6):603–623. doi:10.1016/j.dental.2015.02.011
28. Nakamura K, Adolfsson E, Milleding P, Kanno T, Örtengren U. Influence of grain size and veneer firing process on the flexural strength of zirconia ceramics. Eur J Oral Sci. 2012;120(3):249–254. doi:10.1111/j.1600-0722.2012.00958.x
29. Alsarani M, Souza G, Rizkalla A, El-Mowafy O. Influence of crown design and material on chipping-resistance of all-ceramic molar crowns: an in vitro study. Dent Med Probl. 2018;55(1):35–42. doi:10.17219/dmp/85000
30. Oyar P, Ulusoy M, Eskitascioglu G. Finite element analysis of stress distribution of 2 different tooth preparation designs in porcelain-fused-to-metal crowns. Int J Prosthodont. 2006;19(1):85–91.
31. Oyar P, Ulusoy M, Eskitaşçıoğlu G. Finite element analysis of stress distribution in ceramic crowns fabricated with different tooth preparation designs. J Prosthet Dent. 2014;112(4):871–877. doi:10.1016/j.prosdent.2013.12.019
32. Mihram WL, Nemetz H. The tilted molar: a prosthetic and periodontal dilemma. Oral Health. 1991;81(10):11–15.
33. Imanishi A, Nakamura T, Ohyama T, Nakamura T. 3-D Finite element analysis of all-ceramic posterior crowns. J Oral Rehabil. 2003;30(8):818–822. doi:10.1046/j.1365-2842.2003.01123.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.