")
Back to Journals » Biologics: Targets and Therapy » Volume 16
Biological Therapies for the Management of Enteric Disease: Considerations for the Clinician
Authors Saleh A , Ansari U, Abughazaleh S , Glassner K, Abraham BP
Received 26 January 2022
Accepted for publication 25 May 2022
Published 17 June 2022 Volume 2022:16 Pages 67—83
DOI https://doi.org/10.2147/BTT.S335697
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Shein-Chung Chow
Adam Saleh,1,2 Usman Ansari,2 Shaadi Abughazaleh,2 Kerri Glassner,2 Bincy P Abraham2
1Engineering Medicine, Texas A&M University, Houston, TX, USA; 2Department of Medicine – Division of Gastroenterology, Houston Methodist, Houston, TX, USA
Correspondence: Bincy P Abraham, Department of Medicine – Division of Gastroenterology, Houston Methodist, 6550 Fannin St. Suite 1201, Houston, TX, 77030, USA, Tel +1-713-441-5042, Fax +1-713-797-0622, Email [email protected]
Abstract: Several biologic therapies have been approved for enteric diseases. We evaluate each biologic’s role based on their mechanism of action in treating these conditions. This review examines data on efficacy and safety, as well as considerations for using these therapies in clinical practice in inflammatory bowel diseases, enteric infections—specifically Clostridioides difficile colitis—and potentially in the increasingly prevalent disorder of eosinophilic esophagitis. When choosing an appropriate therapy, it is important to assess patient severity, as most biologics are approved for those with moderate to severe disease activity. With many years of data from clinical trials and real-world experience, these therapies have been shown to improve outcomes overall in enteric diseases, contributing to more options for our patients.
Keywords: biologics, Crohn’s disease, ulcerative colitis, Clostridioides difficile colitis, microscopic colitis, enteric disease
Introduction
Since their introduction in 1998, with infliximab’s approval for treatment of Crohn’s disease, biologics have revolutionized outcomes in enteric diseases. Biologics are monoclonal antibodies that work to block certain pathways of the immune system that include cytokines such as TNF-alpha and interleukins, as well as to block leukocyte trafficking pathways such as integrins. In this review, we summarize the data on biologic therapies in Crohn’s disease (CD), ulcerative colitis (UC), microscopic colitis, and C. difficile infections, as well as emerging therapies in the field of eosinophilic esophagitis and celiac disease. With multiple options of treatment and many emerging therapies on the horizon, we have provided a summary of efficacy and safety considerations for clinicians and providers managing these diseases based on existing evidence from the pivotal randomized controlled trials, real-world evidence studies, and, where there are limited data, from case series and reports.
Biologics in Crohn’s Disease
TNF-Alpha Inhibitors
Tumor necrosis factor (TNF)-alpha inhibitors are a class of biologic agents utilized in the treatment of moderate to severe Crohn’s disease. They are monoclonal antibodies that target TNF-alpha, a cytokine that is upregulated in patients with active inflammatory bowel disease (IBD) and that is linked to immune system dysregulation.1 Three TNF-alpha inhibitors are approved for the treatment of CD: infliximab, adalimumab, and certolizumab pegol.
Infliximab
In the first randomized controlled trial (RCT) involving infliximab, patients with moderate to severe CD were evaluated for clinical response after being randomly assigned to receive a single intravenous infusion of either infliximab or placebo in a dose of 5, 10, or 20 mg/kg. Higher rates of clinical remission (Crohn’s Disease Activity Index [CDAI] <150) were observed in patients treated with infliximab (33%) than in those treated with placebo (4%) (p = 0.005).2 In another RCT, CD patients with draining abdominal or perianal fistulas of at least 3 months’ duration were randomly assigned placebo, 5 mg/kg of infliximab, or 10 mg/kg of infliximab at weeks 0, 2, and 6. A reduction in the number of draining fistulas of >50% from baseline was observed in 68% and 56% of patients in the infliximab groups (5 and 10 mg/kg, respectively), compared with only 26% in the placebo group (p = 0.002 and p = 0.02, respectively).3
The ACCENT I trial evaluated the long-term treatment of moderate to severe CD with infliximab. Patients with a CDAI score of at least 220 received a 5 mg/kg IV infusion of infliximab at week 0. The patients who achieved clinical remission were randomized to receive infliximab 10 mg/kg, 5 mg/kg, or placebo at weeks 2 and 6 and then every 8 weeks thereafter until week 46. At week 30, 21% of patients in the placebo group remained in remission, compared to 39% of the 5 mg/kg infliximab group (p = 0.003) and 45% of the 10 mg/kg infliximab group (p = 0.0002).4
The ACCENT II trial evaluated the long-term treatment of patients with fistulizing CD. Patients received 5 mg/kg IV infusion of infliximab at weeks 0, 2, and 6, then were randomly assigned to receive placebo or 5 mg/kg of infliximab and were followed to week 54. Time to loss of response in control of abdominal or perianal fistula closure was >40 weeks for patients in the infliximab group, as compared to 14 weeks in the placebo group (p < 0.001).5
The SONIC trial evaluated the efficacy of infliximab monotherapy, azathioprine monotherapy, and both drugs combined in patients with moderate to severe CD with no prior exposure to previous biologic or immunosuppressive therapy. Patients on combination therapy had higher rates of corticosteroid-free clinical remission (56.8%) than those on infliximab monotherapy (44.4%) or azathioprine monotherapy (30%) (p = 0.02 and p < 0.001, respectively).6
Although designed differently than the SONIC trial, the COMMIT trial did not show that infliximab combined with methotrexate was superior to infliximab monotherapy.7 The trial’s study design may explain this finding, as the trial was not designed to evaluate the superiority of combination therapy over infliximab monotherapy in patients who experienced prior failure with azathioprine or methotrexate. Another concern was whether the data showing the non-superiority of infliximab combined with methotrexate could be extrapolated to infer the non-inferiority of other TNF-alpha inhibitors.8
The suggested target drug trough concentration level with infliximab is >5 microg/mL for patients with luminal disease, but some studies have associated perianal fistula healing with higher trough levels.9 Specifically, a trough level >10 microg/mL has been suggested as a treat-to-target strategy for patients with fistulizing disease.10
Infliximab has been the most studied biologic in complicated fistulizing Crohn’s disease. As such, it has the most robust evidence base and should be considered as a first-line therapy in the management of fistulizing disease, ideally at higher trough levels, whether it is administered as a monotherapy or in combination with immunomodulators, such as azathioprine, 6-mercaptopurine, or even methotrexate.
Adalimumab
The CLASSIC I trial assessed patients with moderate to severe CD who were naïve to TNF-alpha inhibitor therapy. Patients were randomized to adalimumab at varying doses or placebo administered at weeks 0 and 2, then assessed for clinical remission (CDAI < 150) at week 4. The remission rate for the placebo group was 12%; remission rates for the adalimumab 40/20 mg, 80/40 mg, and 160/80 mg groups were 18% (p = 0.36), 24% (p = 0.06), and 36% (p = 0.001), respectively.11
The CLASSIC 2 trial took patients from CLASSIC I, administered adalimumab 40 mg at weeks 0 and 2, and then re-randomized those patients who were in clinical remission at weeks 0 and 4 to 40 mg every other week, 40 mg weekly, or placebo through 56 weeks. The remission rates were 79% for patients who received adalimumab 40 mg every other week, 83% for patients who received 40 mg weekly, and 44% for the placebo group (p < 0.05 for both adalimumab groups vs placebo).12
The CHARM trial confirmed the superiority of adalimumab over placebo in maintaining clinical remission. The investigators also found that adalimumab was superior to placebo in complete closure of fistulas at week 56 (33% vs 13%, p = 0.016).13
The EXTEND trial evaluated mucosal healing (absence of ulcerations) of the ileocolonic mucosa in patients treated with adalimumab maintenance therapy. By week 12, 27% of the adalimumab group, and by week 52, 24% of the adalimumab group achieved mucosal healing compared to only 13% and 0% by weeks 12 and 52, respectively, in the placebo group (p = 0.056 and p < 0.001, respectively).14
The GAIN trial demonstrated the superiority of adalimumab over placebo in inducing clinical remission at week 4 (21% vs 7%, p < 0.001) in patients who had lost response to or were unable to tolerate infliximab.15
Certolizumab Pegol
A placebo-controlled study evaluated certolizumab pegol at doses of 100, 200, or 400 mg in patients with moderate to severe CD. As early as week 2, a significant clinical benefit with noted clinical response (decrease in CDAI > 100 from baseline) was noted in all certolizumab pegol dose groups (33%), in comparison to the placebo group (15%) (p = 0.01).16
The PRECiSE 1 trial further evaluated the efficacy of certolizumab pegol as compared to placebo. For induction therapy, patients were administered certolizumab pegol 400 mg or placebo at weeks 0, 2, and 4, and the CDAI-100 response (decrease in baseline CDAI > 100) was determined. In the certolizumab group, response rate at week 6 was 35%, compared to 27% in the placebo group (p = 0.02). Rates of remission at week 6 did not differ significantly between the two groups (p = 0.17).17
The PRECiSE 2 trial evaluated maintenance treatment. Patients continued to receive either certolizumab pegol or placebo every 4 weeks from week 8 until week 26. Maintenance of clinical remission was more frequently observed in the certolizumab group (48%) than in the placebo group (29%) (p < 0.001).18
The MUSIC trial showed that certolizumab led to mucosal healing (CDEIS score <6) at week 54 in 27% of patients. The investigators also noted greater rates of fistula closure in patients on certolizumab maintenance therapy (36%) than placebo (17%) (p = 0.038).19
The WELCOME trial showed that, in patients who lost response to infliximab, switching to certolizumab led to a clinical response in 62% of patients at 6 weeks after induction, and maintenance of clinical response was noted in 40% of patients at week 26.20
Anti-Integrins
Natalizumab
Natalizumab is a humanized IgG4 monoclonal antibody that was approved for the treatment of moderate to severe CD in patients who were refractory to TNF-alpha inhibitor–based therapies. Also approved for the treatment of multiple sclerosis, this biologic acts by decreasing T-cell–mediated inflammation in the gut and the brain. It prevents the passage of T cells through the gut’s vascular endothelium and across the blood–brain barrier by blocking the alpha-4 beta-1 integrin receptor expressed on the T cell surface.21
In the ENACT-1 RCT, patients with moderate to severe Crohn’s disease were randomized to receive three infusions of natalizumab 300 mg or placebo over 8 weeks. At week 10, a clinical response (CDAI improvement of at least 70) was observed in 56% of patients treated with natalizumab, compared to 49% of patients treated with placebo (p = 0.051).22 Clinical remission (CDAI < 150) was observed in 37% of natalizumab patients and 30% of placebo group patients (p = 0.124), but patients with C-reactive protein (CRP) levels above the upper limit of normal showed clinically and statistically significant improvements in clinical response and clinical remission on natalizumab compared to placebo. The maintenance of therapy study ENACT-2 clearly demonstrated the long-term efficacy of natalizumab in patients who responded to induction therapy. Patients treated with natalizumab showed higher rates of sustained clinical response (61% vs 28%, p < 0.001) and clinical remission (44% vs 26%, p = 0.003) through week 36 than those treated with placebo.22
The ENCORE trial was a global multi-center study that further evaluated the efficacy of natalizumab as induction therapy in patients with active moderate to severe CD. Patients were randomized to receive intravenous natalizumab 300 mg or placebo at weeks 0, 4, and 8. At week 8, clinical response was observed in 48% of the natalizumab group and 32% of the placebo group (p < 0.001). At week 12, sustained clinical remission was observed in 26% of the natalizumab group and 16% of the placebo group (p = 0.002).23 Although these studies did not evaluate endoscopic assessment, another retrospective review of a small population of patients (n = 32) treated with natalizumab for a mean duration of 14.1 months did show mucosal healing (decrease in simple endoscopic score for Crohn’s disease [SES-CD] >70% from baseline) in 42.3% of patients.24
Vedolizumab
Vedolizumab is a humanized IgG1 monoclonal antibody that is approved for the treatment of moderate to severe CD. This biologic acts by antagonizing the alpha-4 beta-7 integrin receptor expressed on the T cell surface, which prevents interaction with mucosal addressin cell adhesion molecule-1 that is mainly expressed on gut endothelial cells. This complex sequence blocks the migration of a subset of memory gut-homing T cells into inflamed intestinal tissue. The gut specificity of vedolizumab’s mechanism of action limits its systemic and neurologic side effects, so patients are not at increased risk of PML with this medication.25
The GEMINI 2 trial evaluated the efficacy and safety of vedolizumab in patients with moderate to severe CD. In the induction trial, patients were randomized to intravenous vedolizumab 300 mg or placebo at weeks 0 and 2. At week 6, clinical remission (CDAI < 150) was observed in 14.5% and 6.8% of the vedolizumab and placebo groups, respectively (p = 0.02). A CDAI-100 response was observed in 31.4% of patients in the vedolizumab group and 25.7% of patients in the placebo group (p = 0.23). Patients who responded to induction therapy were further randomized to receive either vedolizumab every 8 weeks, vedolizumab every 4 weeks, or placebo. At week 52, clinical remission was observed in 39%, 36.4%, and 21.6% of patients in the 8 week, 4 week, and placebo groups, respectively (p < 0.001 and p = 0.004 for the two vedolizumab groups compared to placebo).26
The GEMINI 3 trial evaluated the efficacy of vedolizumab specifically in patients with moderate to severe CD who had failed, lost response, or developed intolerance to prior TNF-alpha inhibitor therapy. At weeks 6 and 10, patients who were randomized to receive vedolizumab had 15.2% (week 6) and 26.6% (week 10) clinical remission, while patients who received placebo had 12.1% (week 6) and 12.1% (week 10) clinical remission (p = 0.433, p = 0.001, respectively).27
The LOVE-CD study endoscopically evaluated patients treated with maintenance vedolizumab therapy. At weeks 26 and 52, endoscopic remission (SES-CD <4) was noted in 33% and 36% of patients, respectively. Endoscopic responses at weeks 26 and 52 were noted in 40% and 45% of patients, respectively.28
Anti-Interleukin 12/23
Ustekinumab
Ustekinumab is a humanized IgG1 monoclonal antibody that antagonizes interleukin (IL)-12 and IL-23, pro-inflammatory cytokines involved in natural killer (NK) cell activation and CD4+ T cell differentiation and activation. Inhibiting IL-12 and IL-23 reduces the inflammatory cascade and the differentiation of inflammatory T cells.29
The UNITI-1 and UNITI-2 trials evaluated the efficacy and safety of ustekinumab in patients with moderate to severe CD that were either naïve or exposed to TNF-alpha inhibitors. Patients were randomized to receive IV ustekinumab 130 mg or approximately 6 mg/kg or placebo in both trials. Clinical response and remission rates (decrease from baseline CDAI score >100 or a CDAI score <150) at week 6 for patients in the UNITI-1 (TNF-exposed) trial were 34.3%, 33.7%, and 21.6% (p < 0.003 for both comparisons with placebo) for the three treatment groups, respectively; clinical response and remission rates for patients in the UNITI-2 trial were 51.7%, 55.5%, and 28.7% (p < 0.001 for both comparisons with placebo) for the three treatment groups, respectively.30
Patients who had a clinical response in the UNITI induction trials proceeded to the IM-UNITI maintenance study, where they were re-randomized to receive subcutaneous injections of ustekinumab 90 mg either every 8 weeks or every 12 weeks or placebo. Clinical remission rates at week 44 were 53.1%, 48.8%, and 35.9% among the three treatment groups, respectively (p = 0.005 for every 8 weeks vs placebo, p = 0.04 for every 12 weeks vs placebo).31
Patients in the UNITI and IM-UNITI trials underwent endoscopic studies to assess for endoscopic disease activity. At week 8, patients treated with ustekinumab had a greater reduction in simple endoscopic scores (SES-CD) than those treated with placebo (2.8 vs 0.7, p = 0.012). At week 44, with every 8-week dosing, differences in reductions in the SES-CD from the induction baseline were less significant but were greater overall in the ustekinumab group than in the placebo group (3.1 vs 1.9, p = 0.107). Long-term extension data across all ustekinumab-treated patients were gathered until week 152. Remission rates were 56.3% and 55.1% for every 12-week and every 8-week dosing, respectively.35
Biologics in Development in Crohn’s Disease
Risankizumab
Risankizumab is a humanized monoclonal antibody that targets the p19 subunit of IL-23. The biologic has been studied through clinical trials in patients with moderate to severe Crohn’s disease. A Phase II RCT at week 12 showed that clinical remission was achieved in 25 (31%) of 82 patients treated with risankizumab in comparison to six (15%) of 39 patients treated with placebo (p = 0.0489).32 In an extension study to evaluate the long-term efficacy of risankizumab, at week 26, clinical remission was observed in 54 (53%) of 101 patients treated with 600 mg risankizumab. At week 52, clinical remission was maintained in 44 (71%) patients; 50 (81%) patients had a clinical response. Short- and long-term adverse event profiles were similar, most commonly consisting of arthralgia, headache, abdominal pain, nasopharyngitis, nausea, and pyrexia. Risankizumab has shown promising results in clinical trials with short- and long-term efficacy with a low risk of serious adverse events in patients with moderate to severe Crohn’s disease.33
Biologics in Ulcerative Colitis (UC)
Anti-TNFs (Infliximab, Adalimumab, Golimumab)
Tumor necrosis factor alpha (TNF-alpha) is a cytokine that is significantly increased in the setting of inflammatory bowel disease, as well as other conditions such as rheumatoid arthritis, psoriasis, and psoriatic arthritis. Similar to their use in CD, the anti-TNF biologics used in ulcerative colitis (UC) are all IgG molecules that bind to soluble and bound TNF-alpha. The exact molecular mechanism through which anti-TNF agents contribute to disease suppression is still a matter of debate. The current prevailing explanation is that direct neutralization of TNF-alpha is the central feature of significance for IBD patients, but this explanation is hindered by the fact that anti-tumor necrosis factor (anti-TNF) agents such as etanercept, though effective as a treatment for rheumatoid arthritis, fails to induce remission in IBD patients. Other central features, such as the influence on the intestinal barrier function, the induction of apoptosis in mucosal immune cells, and the formation of regulatory macrophages, have been discussed as alternative central features.34
Nonetheless, anti-TNF agents are effective in both inducing and maintaining remission in patients with moderate to severe UC. Three anti-TNF agents are currently approved by the FDA for the treatment of ulcerative colitis (infliximab, adalimumab, and golimumab), and all have demonstrated superiority over placebo in achieving primary endpoints of response and remission.35 The first anti-TNF trial in UC patients was conducted in the ACT I and ACT II trials, with infliximab showing superior rates of inducing remission (defined as Mayo Score of 2 or less and no subscore greater than 1) at 8 weeks compared to placebo. Mucosal healing (defined as absolute Mayo endoscopy subscore of 0 or 1) was achieved at a higher rate in patients on infliximab than those on placebo as well (62% vs 34%, p < 0.001). Finally, for maintenance therapy, infliximab demonstrated superiority over placebo in both the ACT I and ACT II trials, with values of 23% (p = 0.001) and 14% (p < 0.001), compared to placebo at 8%, through 30 weeks.36 The ULTRA I and ULTRA II trials both demonstrated higher rates of remission in UC patients on adalimumab at 8 weeks than those on placebo (18.5% vs 9.2%, p = 0.031). Additionally, with a maintenance dose of 40 mg SQ every other week, 17% of patients on adalimumab vs 8.5% on placebo (p = 0.004) maintained clinical remission through week 52.37 Finally, the PURSUIT-SC trial showed that UC patients treated with golimumab were more likely to achieve clinical remission through 6 weeks than patients on placebo (18% vs 6.4%, p < 0.001).38 Additionally, the PURSUIT-M trial showed that golimumab can sustain clinical remission through 54 weeks more effectively than placebo (28% vs 15.6%, p = 0.004).39 Thus, all three anti-TNF agents available for UC treatment are recommended as first-line treatment options in the UC management guidelines.
When compared to one another in the recent AGA technical review and network meta-analysis of biologic-naïve UC patients with moderate to severe disease activity, infliximab demonstrated superiority over adalimumab for reaching the endpoints of clinical and endoscopic remission.7 This review also showed that the rate of endoscopic remission was higher in patients treated with infliximab than those treated with golimumab.40 An additional network meta-analysis of 29 studies, four of which were head-to-head RCTs, further substantiated this, with infliximab ranking superior to all other biologic interventions with induction of clinical remission being the primary endpoint.41 Other head-to-head studies have been limited, but numerous observational studies have suggested a lower risk of hospitalization, corticosteroid use, and serious infections in patients treated with infliximab than those treated with adalimumab.42 Additionally, a patient-level analysis from Phase 3 trials showed that infliximab had higher rates of resolution of moderate to severe symptoms of UC than golimumab.43
There are limited data on the use of combination therapy in UC patients. When considering combination therapy with anti-TNFs, the only trials conducted have compared infliximab monotherapy with combination therapy. Using infliximab in combination therapy during induction appears to increase efficacy and decrease the risk of immunogenicity. This was demonstrated in the SUCCESS trial, which showed that combination therapy with infliximab (5 mg/kg) and azathioprine daily (2.5 mg/kg) achieved higher rates of corticosteroid-free clinical remission than infliximab monotherapy alone (40% vs 22%, p = 0.017) for UC patients.44 However, there are additional safety considerations when using combination therapy instead of monotherapy.
As the patent coverage expires for existing anti-TNFs, there has been a rise in the number of biosimilars available for use in UC. Biosimilars exist for both infliximab and adalimumab and have similar efficacy levels and indications for use in UC. This includes infliximab-dyyb, infliximab-abda, infliximab-qbtx, adalimumab-atto, and adalimumab-abdm.45–49 Currently, data are limited on head-to-head analyses of biosimilars in comparison to their original counterpart for the treatment of UC. However, large scale clinical trials have demonstrated their effectiveness as a first-line option for CD.50,51
Anti-Integrin (Vedolizumab)
Vedolizumab stands out among biologics available for UC due to its excellent safety profile.52,53 It functions by inhibiting alpha-4 beta-7–mediated lymphocyte trafficking, confining its immunosuppressive effects to the gut. The efficacy and safety of vedolizumab have been demonstrated in numerous studies since the initial GEMINI trial. A retrospective review from fourteen centers with a total of 303 UC patients demonstrated a 79% clinical response rate at three months and a 60% rate of clinical remission at 12-month follow-up.54 An additional network meta-analysis demonstrated that vedolizumab is the biologic agent with the best safety profile.41
Additionally, clinical response to vedolizumab appears to be better in anti-TNF–naïve patients, as rates of clinical remission were 1.8 times greater in patients who had not been exposed to anti-TNF agents.54 There appears to be no advantage to using combination therapy with immunomodulators, which do not seem to affect the efficacy, clearance or immunogenicity of vedolizumab.55 However, there are currently limited data on the use of other combination therapies with vedolizumab.
A head-to-head trial comparing vedolizumab to adalimumab showed higher rates of clinical remission in those treated with vedolizumab (31.3% vs 22.5%; p = 0.006) and endoscopic improvement with vedolizumab (39.7% vs 27.7%; p < 0.001), but not corticosteroid-free remission (12.6% vs 21.8%).56 Scott et al developed a Markov model consisting of a base case of a 35-year-old male with steroid-dependent moderately to severely active UC who was initiating steroid-sparing medical therapy in the outpatient setting. The model used inputs from randomized controlled trials of various drug efficacies for transition probabilities and concluded that vedolizumab should be considered as first-line treatment, prior to thiopurines or other biologic therapies, for moderately to severely active steroid-dependent UC.57
Anti-IL 12/23 (Ustekinumab)
Ustekinumab, an antibody to the p40 subunit of IL-12 and 23, has shown efficacy in both bio-naïve and bio-experienced UC patients in randomized controlled trials (RCT).58 It should be noted, however, that only six of those who had previously failed biologic therapy (491) had previously used vedolizumab, which makes the efficacy of ustekinumab use post-vedolizumab failure less clear. Clinical response was seen in these patients as early as week two, with a significant reduction in CRP and fecal calprotectin. By week eight, ustekinumab was significantly more effective than placebo in clinical response and remission, endoscopic improvement, health-related quality of life, and histo-endoscopic mucosal healing. The long-term efficacy and safety of ustekinumab use in the patients of this study were analyzed through week 92 (efficacy) and week 96 (safety).59 The study confirmed the efficacy of ustekinumab in maintaining remission through two years of treatment with no new safety signals detected through 96 weeks.
As with vedolizumab, the use of combination therapy with immunomodulators does not appear to confer any additional benefit over monotherapy with ustekinumab alone.55 Similar to the other biologics used in UC, there are limited data on combination therapy in general with ustekinumab.
Biologics in Development for UC
There are numerous biologics in development for the treatment of UC; however, the following drugs have results from Phase III clinical trials and are perhaps the closest to gaining full FDA approval for UC treatment.
Etrolizumab
Etrolizumab is a gut-targeted anti-beta-7 monoclonal antibody with mixed results from recently completed phase III clinical trials. Importantly, in all five completed phase III clinical trials, etrolizumab demonstrated an excellent safety profile. In the HIBISCUS I trial, etrolizumab demonstrated greater efficacy over placebo (19.4% vs 6.9%, p = 0.017), but failed to demonstrate superiority in HIBISCUS II. The HICKORY trials showed etrolizumab to be more effective than placebo in inducing remission (at week 14, 18.5% vs 6.3%, p = 0.0033), but no difference in the maintenance of remission was measured at week 66. The LAUREL and GARDENIA clinical trials also failed to demonstrate a statistically significant difference between etrolizumab and placebo in the treatment of UC.60,61 Although the clinical trials did not yield overwhelmingly positive results, the mixed nature of these results warrants further investigation.
Mirikizumab
Mirikizumab is a humanized IgG4 monoclonal antibody that binds to the p19 subunit of IL-23. Currently, mirikizumab is undergoing a phase III clinical trial (LUCENT-I) with an expected end date of October 2022. Preliminary results from LUCENT-I have been published with 24.2% of patients reaching the primary endpoint of clinical remission by 12 weeks compared to 13.3% for placebo (p = 0.00006).62
Biologics in Acute Severe Ulcerative Colitis (ASUC)
In the setting of acute severe ulcerative colitis (ASUC), the primary goal is to deescalate disease severity to provide outpatient management while limiting the need for surgery.
Anti-TNFs
Infliximab should be considered in patients hospitalized with severe UC who have not responded to IV corticosteroids. Patients treated with infliximab have lower rates of colectomy and higher rates of steroid-free remission at 12 months than those on placebo.40 Additionally, a systematic review of 2158 patients found that colectomy-free survival of ASUC patients treated with infliximab was 79.7% at 3 months and 69.8% at 12 months.63 As such, ACG guidelines currently recommend administering infliximab as a rescue therapy for patients with ASUC who have failed to adequately respond to IV corticosteroids by 3–5 days.35 Unfortunately, we have no data to support the use of adalimumab or golimumab in the setting of ASUC.
Vedolizumab
Research on the use of vedolizumab in patients with ASUC is limited; however, this biologic may be used for hospitalized ASUC patients for whom other small molecule or biologic treatment options are contraindicated or have failed. In a retrospective study of 39 steroid-refractory UC patients (most were also refractory to anti-TNF agents), combination treatment with vedolizumab and a calcineurin inhibitor prevented colectomy in two-thirds of patients.64
Ustekinumab
No clinical studies exist to support the use of ustekinumab to treat ASUC.
When selecting biologic therapies for UC patients, numerous factors should be considered, such as patient preference and comorbidities. Patient preferences for oral, intravenous, or subcutaneous (SQ) injections are important for their adherence. Comorbidities, such as cardiac disease, extraintestinal manifestations or other conditions, affect the mechanism of action selected for biologic therapy.
Biologics in Clostridioides difficile Infection
Bezlotoxumab
Bezlotoxumab is a fully humanized IgG1/kappa monoclonal antibody65 that binds to two distinct sites of the C. difficile toxin B, which in turn directly blocks its carbohydrate binding pockets, thus preventing its attachment to colonic mucosal cells.66 This medication is administered as a single IV dose of 10 mg/kg over 60 minutes.67 Bezlotoxumab is indicated for adults ≥18 years at high risk of recurrent C. difficile infection (CDI) in combination with conventional anti-CDI therapies. High-risk patients were defined as patients with CDI in the previous 6 months, severe CDI (Zar score ≥2), patients ≥65 years of age, patients who had received one or more systemic antibacterial drugs, immunocompromising conditions and CDI due to hypervirulent ribotype strains 027, 078, or 244.68
In a phase III trial, patients treated with bezlotoxumab had lower rates of CDI recurrence than those treated with placebo (17% vs 30%). In this study, 77% of patients had one or more risk factors for CDI. Following treatment with bezlotoxumab in 710 patients in two phase III trials, none of the evaluated patients tested positive for treatment-emergent anti-bezlotoxumab antibodies.68
Microscopic Colitis
Biologics have been used in patients with microscopic colitis that is refractory to established treatment modalities or in patients that present with severe symptoms.
Anti-TNFs
Although no large randomized studies have been published, two case series and multiple case reports have described anti-TNF therapies (adalimumab, infliximab) used successfully to avoid colectomy.69–71 These reports demonstrated a 60–90% decrease in bowel movements after one dose, and 75% of patients in one case series demonstrated long-term clinical remission (more than one year).
Vedolizumab
A case series examining the use of vedolizumab in patients with refractory colitis showed that sustained clinical improvement occurred in 75% of treated patients. These patients achieved clinical response in under 8 weeks after induction.66 Another small case series of three patients described clinical response after the first two induction doses in patients who were previously steroid-dependent.67
Ustekinumab
Ustekinumab has also been evaluated for use in refractory microscopic colitis, but results have been less consistent. One case report showed successful treatment in a patient when ustekinumab was used in conjunction with azathioprine; however, another case report described no improvement in a patient’s clinical condition after a trial of treatment.68,69 Clinicians can consider these biologics as an option in these patients if conventional therapies have failed.
Eosinophilic Esophagitis
In patients with eosinophilic esophagitis (EOE), biologics have been proposed as potential treatment options in patients who have failed to respond to conventional therapies.
Dupilumab
Given the role that cytokines are suspected to play in the pathogenesis of EOE, dupilumab (monoclonal antibody to the alpha subunit of IL-4) was assessed in a Phase 2 randomized trial of 47 patients with active EOE. Dupilumab reduced symptoms of dysphagia and also reduced both histological and endoscopic features of EOE.70 Dupilumab was recently approved by the FDA for treatment of EOE.
RPC4046
Another biologic, RPC4046, a monoclonal antibody against IL-13 under investigation in a Phase 2 trial of 99 patients with active EOE, showed significant improvement in patient-reported symptoms, clinician’s global assessment of disease severity, endoscopic appearance, and histological grade and stage at 16 weeks compared to placebo.72 Follow-up studies found that patients on RPC4046 maintained these responses at 52 weeks of treatment.73
Mepolizumab and Reslizumab
Two monoclonal antibodies against IL-5 (mepolizumab and reslizumab) have also been investigated for EOE, but their role in treatment has been less clear. In multiple studies, mepolizumab reduced the histological severity of EOE, but with no statistically significant improvement in clinical symptoms.74–76 A larger study of over 220 children and adolescents showed a significant histological reduction in eosinophil counts in patients who received reslizumab at 15 weeks. However, patients in both treatment groups reported symptom improvement, which was not associated with changes in histological eosinophil count.77
Biologics in Celiac Disease
Celiac disease is defined by immune-mediated damage to the small intestine precipitated by exposure to gluten in genetically susceptible individuals. Similar to other enteropathies, celiac disease can present with symptoms such as malabsorption, diarrhea, failure to thrive and weight loss.78 A gluten-free diet is the primary treatment for patients with celiac disease, but this can be complicated by a persistent active form of celiac disease despite proper gluten restriction. Refractory celiac disease (RCD) is divided into two categories defined by T-cell flow cytometry, RCD-I and RCD-II. In RCD-I, aberrant T cells comprise less than 20% of the total intraepithelial lymphocytes, whereas in RCD-II, the percentage of aberrant T cells is greater than 20%.79 A systematic review of existing gastroenterology guidelines on the treatment of celiac disease shows only the European Society for the Study of Celiac Disease (ESsCD) recommending the use of biologics in celiac disease, specifically infliximab as a second-line treatment option in RCD-I.79
Anti-TNFs (Infliximab)
In patients with RCD-1 who have not responded to first-line therapies (budesonide, prednisone, or azathioprine), infliximab can be considered, though data are limited, as only a few cases have been reported.80–82 In all three case reports, the patients (two adult, one pediatric) were diagnosed with RCD and had insufficient response to corticosteroids. All three patients achieved histological remission after therapy with infliximab (5 mg/kg); however, the protocol followed was slightly different in each of the case reports. One of the adult patients was treated with only one dose of infliximab and had dramatic clinical improvement within days. After three months, the patient demonstrated histological remission and was commenced on azathioprine. The patient remained in remission up to 18 months after the single infusion of infliximab.80 The other adult patient case report appeared to initially follow the aforementioned protocol until the patient lost clinical response six months after the single infliximab infusion despite azathioprine background therapy.82 The patient was then initiated on a maintenance therapy of infliximab every eight weeks and remained in remission up to two years later. Finally, the pediatric patient was given an induction dose of infliximab followed by maintenance infusions every eight weeks and was followed for eight months and remained in remission.81 Large-scale clinical trials are necessary to fully determine the clinical utility of anti-TNFs in RCD.
Alemtuzumab
Alemtuzumab is an anti-CD52 monoclonal antibody routinely used in the treatment of chronic lymphocytic leukemia (CLL) with potential applications in RCD, especially in patients with high risk for enteropathy-associated T-cell lymphoma. A 56-year-old woman with a two-year history of RCD treated with prednisone (20 mg per day) underwent alemtuzumab therapy (30 mg two times per week for 12 consecutive weeks). Prednisone was withdrawn after eight weeks of therapy, and the patient remained asymptomatic after nine months of treatment. Duodenal biopsy showed complete recovery, and flow cytometry confirmed a decrease in aberrant T-cell populations.83 Additional trials are needed to understand how alemtuzumab should be used in the treatment of RCD.
Future Use of Biologics in Celiac Disease
PRV-015, a fully human monoclonal antibody against interleukin 15 (IL-15), is currently undergoing phase 2b clinical trial on patients (aged 18–70) with RCD on a gluten-free diet with an estimated completion date of July 2022. The overexpression of IL-15 is linked with the immunopathology of celiac disease, with murine models demonstrating IL-15 as a key player in the maintenance and expansion of cytotoxic T lymphocytes, natural killer cells, and natural killer T cells.84 Further studies in murine models have shown that anti-IL-15 treatment targets lymphoid cells such as small intestine intraepithelial lymphocytes and inflammatory CD3+ T lymphocytes, making it a promising target in celiac disease.85 The first anti-IL-15 monoclonal antibody (AMG 714) underwent a phase 2 clinical trial in 2016 that failed to demonstrate efficacy in achieving the clinical endpoint of a change in villous height-to-crypt depth ratio when compared to placebo; however, the effects on intraepithelial lymphocyte density and clinical symptoms warrant further investigation.86
Adverse Effects of Biologics
Safety of Anti-TNFs
The use of TNF inhibitors may be limited by safety concerns due to their black box warnings. These include the risk of lymphoma, as well as the potential risk for opportunistic infections, the development of anti-drug antibodies leading to infusion/injection site reactions, neurologic side effects, psoriasis, congestive heart failure exacerbation in patients with significant underlying cardiovascular disease, and other less frequently seen side effects. Overall, however, because we have several decades of clinical knowledge of the use of TNF inhibitors, clinicians can advise their patients of the potential risks but explain and weigh the benefits against these risks based on each individual patient. For most patients with moderate to severe gastrointestinal diseases, the benefits of these medications will far outweigh the potential risks, especially if they are closely monitored.
The adverse events seen with anti-TNFs in the clinical trials were consistent across its indications. The overall risk of serious infections in patients using anti-TNFs (monotherapy, or combined with an immunomodulator) was <1%.40 In general, the risk of adverse events appears to be higher in older patients with comorbidities. Combination therapy with an immunomodulator appears to carry more significant risk, with the chance of opportunistic infections doubling and the chance of lymphoma tripling over monotherapy with an anti-TNF agent.87,88
Real-World Data of TNF-Alpha Inhibitors
A large observational study of 6,273 patients with data compiled over 13 years showed that adverse events, including serious events, occurred at a higher rate among patients treated with infliximab than among those treated with all other therapies. Mortality (0.57/100 patient-years, 0.67/100 patient-years) and malignancy rates (0.69/100 patient-years, 0.71/100 patient-years) for patients treated with infliximab and all other treatments, respectively, were similar. Serious infection rates were higher for infliximab-treated patients (2.15/100 patient-years) than patients treated with all other treatments (0.86/100 patient-years).89
A large observational study evaluating 389 patients for long-term safety (3-year time span) of adalimumab revealed that 105 patients (27%) and 43 patients (11.1%) experienced adverse drug reactions and serious adverse drug reactions, respectively. A total of 37 patients (9.5%) and 17 patients (4.4%) reported infections and serious infections, respectively. Out of 310 patients evaluated for long-term effectiveness, the remission rate increased from 37.8% to 73.9% at week 4 and remained greater than 70% over the 3-year follow-up duration. This study demonstrated the long-term effectiveness and safety of adalimumab.90
Long-term safety data of patients treated with certolizumab pegol in Crohn’s disease along with other autoimmune conditions were pooled into a meta-analysis. Of the 11,317 total patients evaluated, infections were the most common serious adverse event (incident rate 3.62/100 patient-years). The rate for malignancies was 0.82/100 patient-years. Major adverse cardiovascular events and gastrointestinal perforation rates were 0.47/100 and 0.08/100 patient-years, respectively. The safety data correlated well with expected general population data.91
Safety of Anti-Integrins
The most commonly reported adverse effects associated with natalizumab use are headache, nausea, abdominal pain, nasopharyngitis, dizziness, fatigue, and exacerbation of Crohn’s disease. Three cases of progressive multifocal leukoencephalopathy (PML) associated with natalizumab use (two cases in the treatment of multiple sclerosis and one case in Crohn’s disease in the ENCORE-2 trial) led to the restructuring of guidelines for utilization of the drug. Due to this, consider using natalizumab in patients that have both Crohn’s disease and multiple sclerosis due to its efficacy in both diseases. Since the risk of PML occurs with the John Cunningham (JC) virus, patients considered for natalizumab therapy should be tested for this virus. If present, consider other therapies that do not increase risk of PML.
Vedolizumab has an excellent safety profile with no increased risk for opportunistic infections or malignancies in approximately 3,000 patients treated with vedolizumab for five years.52 Reported adverse events associated with vedolizumab use in the Crohn’s disease and ulcerative colitis trials include nasopharyngitis, arthralgia, headache, pyrexia, nausea, abdominal pain, upper respiratory infection, and fatigue. A meta-analysis evaluating vedolizumab safety found no association with increased rates of any serious adverse effects, serious infections, or other adverse events including PML, death, and cancer.53 The clinical trials also noted low rates of anti-drug antibodies for vedolizumab, and there was no benefit in efficacy or trough levels from adding immunomodulators such as methotrexate, azathioprine, or 6-mercaptopurine. Thus, vedolizumab should be considered as a monotherapy to reduce the risks associated with immunomodulators.
Real-World Data of Vedolizumab
A large multi-center retrospective study including 212 patients with moderate to severe CD treated with vedolizumab showed that 12-month cumulative rates of clinical remission, mucosal healing, and deep remission were 35%, 63%, and 26%, respectively. During 160 patient-years of follow-up, five patients developed infusion reactions (3.5 per 1,000 infusions), 21 developed serious infections (13 per 100 patient-years), and 17 developed serious adverse events (10 per 100 patient-years). Discontinuation of therapy resulted from a minority of adverse events (6 per 100 patient-years). These real-world data show the safety and efficacy of vedolizumab in patients with moderate to severe CD.92
Safety of Anti-Interleukins
Ustekinumab is also considered to have an excellent profile with minimal reports of serious adverse events in UC and CD. From weeks 44–96 of ustekinumab use, the rate of adverse events, malignancies and serious infections per hundred patients was lower in the ustekinumab group than the placebo group.59 Safety events at week 152 of the UNITI trial were similar among the ustekinumab and placebo groups. Serious adverse events were noted in 18.97% vs 19.54%, and serious infections were noted in 4.21% vs 3.97% of patients in the ustekinumab and placebo groups, respectively.93 Like vedolizumab, ustekinumab showed low rates of anti-drug antibodies and no benefit in efficacy or trough levels from being used in combination with immunomodulators. Thus, ustekinumab also should be used as a monotherapy in patients with IBD.
Real-World Data of Ustekinumab
A single-center prospective study evaluated the real-world experience of ustekinumab in Crohn’s disease. Of 84 patients who received induction therapy, 53% had a clinical response, while clinical remission was observed in 8%. Evaluation at one year on maintenance dosing showed clinical response and remission in 71% and 14% of patients, respectively. Adverse events included the following: four patients experienced infections, one patient had a drug-related rash, and seven patients experienced worsening of underlying disease.94
Safety of Bezlotoxumab
The most common adverse reactions included nausea, pyrexia, and headache. These occurred in the first four weeks after infusion and were found in 4–7% of participants. Heart failure exacerbation was reported more commonly in patients treated with bezlotoxumab (12.7%) than with placebo (4.8%) during the twelve-week trial in patients with a known history of congestive heart failure (CHF). There were also more deaths in this subgroup of the bezlotoxumab treatment group (19.5%) than in the placebo group (12.5%). Given these findings, it is recommended that, for patients with a history of CHF, bezlotoxumab should be reserved for use when the benefits outweigh the risk.68
Safety of Dupilumab
Side effects of injection-site erythema and nasopharyngitis were more commonly seen in the treatment group in the EOE phase 2 trial than in the placebo group.95
Safety of Biologics in Pregnancy
A large meta-analysis including forty-eight studies and a total of 6963 patients evaluated the safety of biologics in pregnant patients with IBD. There was a pooled prevalence of 8% (95% CI, 6–10%) for early pregnancy loss, 9% (95% CI, 7–11%) for preterm birth, 0% (95% CI, 0–0%) for stillbirth, 8% (95% CI, 5–10%) for low birth weight, and 1% (95% CI, 1–2%) for congenital malformations. The prevalence of early pregnancy loss with anti-TNF agents was lower (7% [95% CI, 5–8%]) than with vedolizumab (18% [95% CI, 12–24%]) and ustekinumab (17% [95% CI 12–22%]). The prevalence of preterm birth (birth between 20 and 37 weeks) with anti-TNF agents (8% [95% CI, 6–10%]) and with ustekinumab (8% [95% CI, 4–14%]) was lower than with vedolizumab (19% [95% CI 12–26%]). There was no risk of stillbirth with any agent. The prevalence of low birth weight was slightly greater in pregnant patients treated with anti-TNF (8% [95% CI 5–10%]) than those treated with vedolizumab (5% [95% CI 1–23%]). The prevalence of congenital malformation was greater in pregnant patients treated with ustekinumab (5% [95% CI, 2–8%]) than in patients treated with anti-TNF agents (1% [95% CI, 1–2%]) and with vedolizumab (1% [95% CI 0–4%]). There was no association found between disease activity or concomitant thiopurine use and adverse outcomes.96
Anti-TNFs in Pregnancy
Certolizumab pegol has been studied for safety in pregnancy and breastfeeding. The CRIB study evaluated 16 women and their infants for certolizumab group levels immediately after delivery and found that only one infant had minimal levels, while the other infants had undetectable levels. The mothers remained within the therapeutic range.97 The CRADLE study similarly showed undetectable to minimal certolizumab group levels in breast milk in a patient population of 17. The PEG molecule prevents placental transfer as well as transfer to breast milk.98 These findings support the use of certolizumab pegol as an ideal therapeutic option for young females of childbearing age with Crohn’s disease.
Although there has not been a full clinical trial to evaluate the safety of all other anti-TNFs in pregnancy, existing meta-analyses have consistently demonstrated that the use of anti-TNFs does not increase the risk of unfavorable pregnancy outcomes in women with IBD. This includes rates of early pregnancy loss, risk of preterm birth, low birth weight, and congenital malformations.96,99 In general, it is recommended to continue all anti-TNFs throughout pregnancy and breastfeeding. However, it is recommended to avoid live virus vaccinations in the new-born of mothers on anti-TNFs, with the exception of certolizumab, due to its specific lack of placental transfer properties.
Anti-Integrins in Pregnancy
Vedolizumab has been classified as FDA pregnancy category B. The safety profile of vedolizumab’s use during pregnancy is still being explored, but recent studies, including the European CONCEIVE study, which analyzed outcomes in 79 pregnancies (73 patients with IBD), have discovered no new safety signals.100 Nursing appears to be safe, with only miniscule amounts of vedolizumab being reported in breast milk (peak amounts 2–3 days after infusion) and the expected proteolysis in the infant’s stomach; however, larger studies are warranted.101 Additionally, paternal exposure to vedolizumab does not appear to affect pregnancy.101 Another meta-analysis also recently demonstrated the safety of vedolizumab with no difference in pooled prevalence between pregnant women with IBD using vedolizumab and the general population in the rates of early pregnancy loss, risk of preterm birth, low birth weight, and congenital malformations.96
Anti-Interleukins in Pregnancy
Similar to vedolizumab, ustekinumab is classified as FDA pregnancy category B and has no expected safety concerns to the fetus. Also similar to vedolizumab, minimal amounts of ustekinumab are found in breast milk (peak amounts 2–3 days after infusion), so breastfeeding is expected to be safe with ustekinumab. An additional meta-analysis also recently demonstrated the safety of ustekinumab with no difference in pooled prevalence between pregnant women with IBD using ustekinumab and the general population in the rates of early pregnancy loss, risk of preterm birth, low birth weight, and congenital malformations.96
Dupilumab in Pregnancy
Dupilumab is expected to cross the placental barrier and be excreted in breast milk like other IgG antibodies. Clinical data, although limited, have been described in pregnancy and have not shown a drug-associated risk of major birth defects, miscarriages, or adverse maternal or fetal outcomes.95
Conclusion
Several biologic therapies have been approved for enteric disease, mostly for inflammatory bowel disease. Because these therapies differ in efficacy, safety, and mode of administration, each individual patient’s disease severity, comorbidities, and preference for route of administration should be considered when making a decision on the best biologic option (see Table 1). Overall, we have had many years of data, both in clinical trials and in real-world experience, to show improvement in disease outcomes with the use of these therapies. Many biologic therapies are still under clinical trials for more enteric disease indications and may contribute to the growing armamentarium of treatment options for our patients.
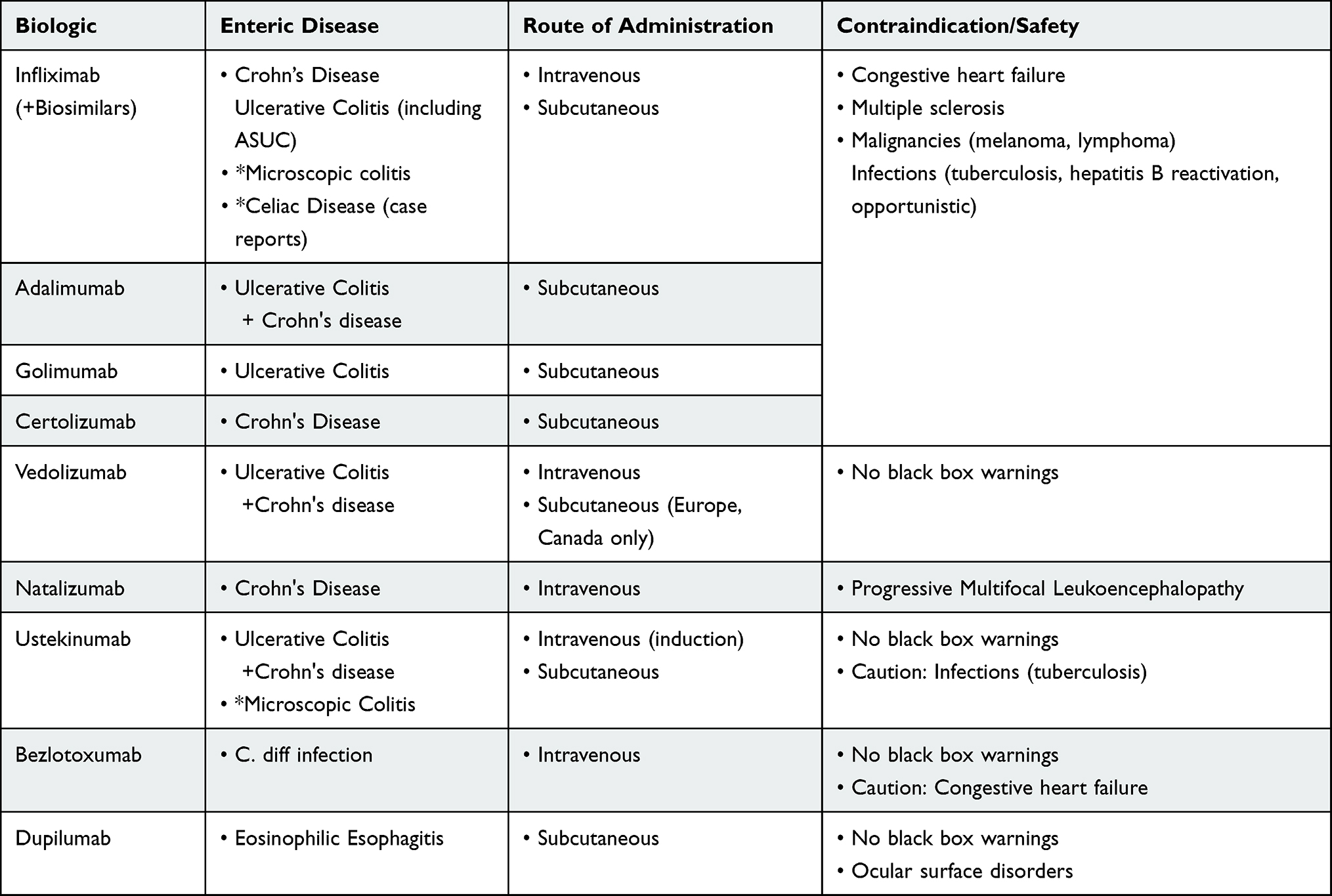 |
Table 1 Contraindications and Routes of Administration for the Use of Biologics in Enteric Disease |
Disclosure
Dr. Abraham reports research funding from Janssen, Celgene, Genentech, Gilead, AbbVie, Takeda, and Lilly, and has been a paid consultant/speaker for AbbVie, BMS, Takeda, Janssen, Pfizer, Lilly, and Medtronics. The authors report no other conflicts of interest in this work.
References
1. Sandborn WJ, Hanauer SB. Antitumor necrosis factor therapy for inflammatory bowel disease: a review of agents, pharmacology, clinical results, and safety. Inflamm Bowel Dis. 1999;5(2):119–133. doi:10.1097/00054725-199905000-00008
2. Targan SR, Hanauer SB, van Deventer SJ, et al. A short-term study of chimeric monoclonal antibody cA2 to tumor necrosis factor alpha for Crohn’s disease. Crohn’s Disease cA2 Study Group. N Engl J Med. 1997;337(15):1029–1035. doi:10.1056/NEJM199710093371502
3. Present DH, Rutgeerts P, Targan S, et al. Infliximab for the treatment of fistulas in patients with Crohn’s disease. N Engl J Med. 1999;340(18):1398–1405. doi:10.1056/NEJM199905063401804
4. Hanauer SB, Feagan BG, Lichtenstein GR, et al. Maintenance infliximab for Crohn’s disease: the ACCENT I randomised trial. Lancet. 2002;359(9317):1541–1549. doi:10.1016/S0140-6736(02)08512-4
5. Sands BE, Blank MA, Patel K, van Deventer SJ, Study AI. Long-term treatment of rectovaginal fistulas in Crohn’s disease: response to infliximab in the ACCENT II Study. Clin Gastroenterol Hepatol. 2004;2(10):912–920. doi:10.1016/S1542-3565(04)00414-8
6. Colombel JF, Sandborn WJ, Reinisch W, et al. Infliximab, azathioprine, or combination therapy for Crohn’s disease. N Engl J Med. 2010;362(15):1383–1395. doi:10.1056/NEJMoa0904492
7. Feagan BG, McDonald JW, Panaccione R, et al. Methotrexate in combination with infliximab is no more effective than infliximab alone in patients with Crohn’s disease. Gastroenterology. 2014;146(3):681–688 e681. doi:10.1053/j.gastro.2013.11.024
8. Narula N, Peyrin-Biroulet L, Colombel JF. Combination therapy with methotrexate in inflammatory bowel disease: time to COMMIT? Gastroenterology. 2014;146(3):608–611. doi:10.1053/j.gastro.2014.01.040
9. Davidov Y, Ungar B, Bar-Yoseph H, et al. Association of induction infliximab levels with clinical response in perianal Crohn’s Disease. J Crohns Colitis. 2017;11(5):549–555. doi:10.1093/ecco-jcc/jjw182
10. Yarur AJ, Kanagala V, Stein DJ, et al. Higher infliximab trough levels are associated with perianal fistula healing in patients with Crohn’s disease. Aliment Pharmacol Ther. 2017;45(7):933–940. doi:10.1111/apt.13970
11. Hanauer SB, Sandborn WJ, Rutgeerts P, et al. Human anti-tumor necrosis factor monoclonal antibody (Adalimumab) in Crohn’s disease: the CLASSIC-I trial. Gastroenterology. 2006;130(2):
12. Sandborn WJ, Hanauer SB, Rutgeerts P, et al. Adalimumab for maintenance treatment of Crohn’s disease: results of the CLASSIC II trial. Gut. 2007;56(9):1232–1239. doi:10.1136/gut.2006.106781
13. Colombel JF, Sandborn WJ, Rutgeerts P, et al. Adalimumab for maintenance of clinical response and remission in patients with Crohn’s disease: the CHARM trial. Gastroenterology. 2007;132(1):52–65. doi:10.1053/j.gastro.2006.11.041
14. Rutgeerts P, Van Assche G, Sandborn WJ, et al. Adalimumab induces and maintains mucosal healing in patients with Crohn’s disease: data from the EXTEND trial. Gastroenterology. 2012;142(5):1102–1111 e1102. doi:10.1053/j.gastro.2012.01.035
15. Panaccione R, Sandborn WJ, D’Haens G, et al. Clinical benefit of long-term adalimumab treatment in patients with Crohn’s disease following loss of response or intolerance to infliximab: 96-week efficacy data from GAIN/ADHERE trials. J Crohns Colitis. 2018;12(8):930–938. doi:10.1093/ecco-jcc/jjy050
16. Schreiber S, Rutgeerts P, Fedorak RN, et al. A randomized, placebo-controlled trial of certolizumab pegol (CDP870) for treatment of Crohn’s disease. Gastroenterology. 2005;129(3):807–818. doi:10.1053/j.gastro.2005.06.064
17. Sandborn WJ, Feagan BG, Stoinov S, et al. Certolizumab pegol for the treatment of Crohn’s disease. N Engl J Med. 2007;357(3):228–238. doi:10.1056/NEJMoa067594
18. Schreiber S, Khaliq-Kareemi M, Lawrance IC, et al. Maintenance therapy with certolizumab pegol for Crohn’s disease. N Engl J Med. 2007;357(3):239–250. doi:10.1056/NEJMoa062897
19. Colombel JF, Sandborn WJ, Allez M, et al. Association between plasma concentrations of certolizumab pegol and endoscopic outcomes of patients with Crohn’s disease. Clin Gastroenterol Hepatol. 2014;12(3):423–431 e421. doi:10.1016/j.cgh.2013.10.025
20. Feagan BG, Sandborn WJ, Wolf DC, et al. Randomised clinical trial: improvement in health outcomes with certolizumab pegol in patients with active Crohn’s disease with prior loss of response to infliximab. Aliment Pharmacol Ther. 2011;33(5):541–550. doi:10.1111/j.1365-2036.2010.04568.x
21. Binion DG, West GA, Volk EE, et al. Acquired increase in leucocyte binding by intestinal microvascular endothelium in inflammatory bowel disease. Lancet. 1998;352(9142):1742–1746. doi:10.1016/S0140-6736(98)05050-8
22. Sandborn WJ, Colombel JF, Enns R, et al. Natalizumab induction and maintenance therapy for Crohn’s disease. N Engl J Med. 2005;353(18):1912–1925. doi:10.1056/NEJMoa043335
23. Targan SR, Feagan BG, Fedorak RN, et al. Natalizumab for the treatment of active Crohn’s disease: results of the ENCORE Trial. Gastroenterology. 2007;132(5):1672–1683. doi:10.1053/j.gastro.2007.03.024
24. Sakuraba A, Annunziata ML, Cohen RD, Hanauer SB, Rubin DT. Mucosal healing is associated with improved long-term outcome of maintenance therapy with natalizumab in Crohn’s disease. Inflamm Bowel Dis. 2013;19(12):2577–2583. doi:10.1097/MIB.0b013e3182a8df32
25. Wyant T, Fedyk E, Abhyankar B. An overview of the mechanism of action of the monoclonal antibody vedolizumab. J Crohns Colitis. 2016;10(12):1437–1444. doi:10.1093/ecco-jcc/jjw092
26. Sandborn WJ, Feagan BG, Rutgeerts P, et al. Vedolizumab as induction and maintenance therapy for Crohn’s disease. N Engl J Med. 2013;369(8):711–721. doi:10.1056/NEJMoa1215739
27. Sands BE, Van Assche G, Tudor D, Akhundova-Unadkat G, Curtis RI, Tan T. Vedolizumab in combination with corticosteroids for induction therapy in Crohn’s disease: a post hoc analysis of GEMINI 2 and 3. Inflamm Bowel Dis. 2019;25(8):1375–1382. doi:10.1093/ibd/izy384
28. Lowenberg M, Vermeire S, Mostafavi N, et al. Vedolizumab induces endoscopic and histologic remission in patients with Crohn’s Disease. Gastroenterology. 2019;157(4):997–1006 e1006. doi:10.1053/j.gastro.2019.05.067
29. Luo J, Wu SJ, Lacy ER, et al. Structural basis for the dual recognition of IL-12 and IL-23 by ustekinumab. J Mol Biol. 2010;402(5):797–812. doi:10.1016/j.jmb.2010.07.046
30. Feagan BG, Sandborn WJ, Gasink C, et al. Ustekinumab as induction and maintenance therapy for Crohn’s Disease. N Engl J Med. 2016;375(20):1946–1960. doi:10.1056/NEJMoa1602773
31. Hanauer SB, Sandborn WJ, Feagan BG, et al. IM-UNITI: three-year efficacy, safety, and immunogenicity of ustekinumab treatment of Crohn’s Disease. J Crohns Colitis. 2020;14(1):23–32. doi:10.1093/ecco-jcc/jjz110
32. Feagan BG, Sandborn WJ, D’Haens G, et al. Induction therapy with the selective interleukin-23 inhibitor risankizumab in patients with moderate-to-severe Crohn’s disease: a randomised, double-blind, placebo-controlled phase 2 study. Lancet. 2017;389(10080):1699–1709. doi:10.1016/S0140-6736(17)30570-6
33. Feagan BG, Panes J, Ferrante M, et al. Risankizumab in patients with moderate to severe Crohn’s disease: an open-label extension study. Lancet Gastroenterol Hepatol. 2018;3(10):671–680. doi:10.1016/S2468-1253(18)30233-4
34. Billmeier U, Dieterich W, Neurath MF, Atreya R. Molecular mechanism of action of anti-tumor necrosis factor antibodies in inflammatory bowel diseases. World J Gastroenterol. 2016;22(42):9300–9313. doi:10.3748/wjg.v22.i42.9300
35. Rubin DT, Ananthakrishnan AN, Siegel CA, Sauer BG, Long MD. ACG clinical guideline: ulcerative colitis in adults. Am J Gastroenterol. 2019;114(3):384–413. doi:10.14309/ajg.0000000000000152
36. Rutgeerts P, Sandborn WJ, Feagan BG, et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2005;353(23):2462–2476. doi:10.1056/NEJMoa050516
37. Reinisch W, Sandborn WJ, Hommes DW, et al. Adalimumab for induction of clinical remission in moderately to severely active ulcerative colitis: results of a randomised controlled trial. Gut. 2011;60(6):780–787. doi:10.1136/gut.2010.221127
38. Sandborn WJ, Feagan BG, Marano C, et al. Subcutaneous golimumab induces clinical response and remission in patients with moderate-to-severe ulcerative colitis. Gastroenterology. 2014;146(1):
39. Sandborn WJ, Feagan BG, Marano C, et al. Subcutaneous golimumab maintains clinical response in patients with moderate-to-severe ulcerative colitis. Gastroenterology. 2014;146(1):96–109 e101. doi:10.1053/j.gastro.2013.06.010
40. Singh S, Allegretti JR, Siddique SM, Terdiman JP. AGA technical review on the management of moderate to severe ulcerative colitis. Gastroenterology. 2020;158(5):1465–1496 e1417. doi:10.1053/j.gastro.2020.01.007
41. Lasa JS, Olivera PA, Danese S, Peyrin-Biroulet L. Efficacy and safety of biologics and small molecule drugs for patients with moderate-to-severe ulcerative colitis: a systematic review and network meta-analysis. Lancet Gastroenterol Hepatol. 2022;7(2):161–170. doi:10.1016/S2468-1253(21)00377-0
42. Singh S, Andersen NN, Andersson M, Loftus EV
43. Singh S, Proudfoot JA, Dulai PS, et al. Comparative efficacy and speed of onset of action of infliximab vs golimumab in ulcerative colitis. Clin Gastroenterol Hepatol. 2020;18(2):424–431 e427. doi:10.1016/j.cgh.2019.05.019
44. Panaccione R, Ghosh S, Middleton S, et al. Combination therapy with infliximab and azathioprine is superior to monotherapy with either agent in ulcerative colitis. Gastroenterology. 2014;146(2):392–400 e393. doi:10.1053/j.gastro.2013.10.052
45. Kaniewska M, Moniuszko A, Rydzewska G. The efficacy and safety of the biosimilar product (Inflectra((R))) compared to the reference drug (Remicade((R))) in rescue therapy in adult patients with ulcerative colitis. Prz Gastroenterol. 2017;12(3):169–174. doi:10.5114/pg.2017.70468
46. Merck Sharp & Dohme Corp. Renflexis (Package Insert); 2017. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/761054orig1s000lbl.pdf.
47. Pfizer. Ixifi (Infliximab-qbtx) package insert; 2017. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/761072s000lbl.pdf.
48. Amgen Inc. Amjevita (Adalimumab-atto) package insert; 2016. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/761024lbl.pdf.
49. Boehringer Ingelheim Pharmaceuticals, Inc. Cyltezo (Adalimumab-adbm) package insert; 2017. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/761058s003lbl.pdf.
50. Ye BD, Pesegova M, Alexeeva O, et al. Efficacy and safety of biosimilar CT-P13 compared with originator infliximab in patients with active Crohn’s disease: an international, randomised, double-blind, phase 3 non-inferiority study. Lancet. 2019;393(10182):1699–1707. doi:10.1016/S0140-6736(18)32196-2
51. Meyer A, Rudant J, Drouin J, Weill A, Carbonnel F, Coste J. Effectiveness and safety of reference infliximab and biosimilar in Crohn disease: a French Equivalence Study. Ann Intern Med. 2019;170(2):99–107. doi:10.7326/M18-1512
52. Colombel JF, Sands BE, Rutgeerts P, et al. The safety of vedolizumab for ulcerative colitis and Crohn’s disease. Gut. 2017;66(5):839–851. doi:10.1136/gutjnl-2015-311079
53. Wang MC, Zhang LY, Han W, et al. PRISMA–efficacy and safety of vedolizumab for inflammatory bowel diseases: a systematic review and meta-analysis of randomized controlled trials. Medicine. 2014;93(28):e326. doi:10.1097/MD.0000000000000326
54. Pulusu SSR, Srinivasan A, Krishnaprasad K, et al. Vedolizumab for ulcerative colitis: real world outcomes from a multicenter observational cohort of Australia and Oxford. World J Gastroenterol. 2020;26(30):4428–4441. doi:10.3748/wjg.v26.i30.4428
55. Hu A, Kotze PG, Burgevin A, et al. Combination therapy does not improve rate of clinical or endoscopic remission in patients with inflammatory bowel diseases treated with vedolizumab or ustekinumab. Clin Gastroenterol Hepatol. 2021;19(7):1366–1376 e1362. doi:10.1016/j.cgh.2020.07.012
56. Sands BE, Peyrin-Biroulet L, Loftus EV
57. Scott FI, Shah Y, Lasch K, Luo M, Lewis JD. Assessing the optimal position for vedolizumab in the treatment of ulcerative colitis: a simulation model. Inflamm Bowel Dis. 2018;24(2):286–295. doi:10.1093/ibd/izx045
58. Sands BE, Sandborn WJ, Panaccione R, et al. Ustekinumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2019;381(13):1201–1214. doi:10.1056/NEJMoa1900750
59. Panaccione R, Danese S, Sandborn WJ, et al. Ustekinumab is effective and safe for ulcerative colitis through 2 years of maintenance therapy. Aliment Pharmacol Ther. 2020;52(11–12):1658–1675. doi:10.1111/apt.16119
60. Rubin DT, Dotan I, DuVall A, et al. Etrolizumab versus Adalimumab or placebo as induction therapy for moderately to severely active ulcerative colitis (HIBISCUS): two phase 3 randomised, controlled trials. Lancet Gastroenterol Hepatol. 2022;7(1):17–27. doi:10.1016/S2468-1253(21)00338-1
61. Agrawal M, Verstockt B. Etrolizumab for ulcerative colitis: beyond what meets the eye. Lancet Gastroenterol Hepatol. 2022;7(1):2–4. doi:10.1016/S2468-1253(21)00369-1
62. An induction study of mirikizumab in participants with moderately to severely acute ulcerative colitis (LUCENT 1); 2022. Available from: https://clinicaltrials.gov/ct2/show/NCT03518086.
63. Choy MC, Seah D, Faleck DM, et al. Systematic review and meta-analysis: optimal salvage therapy in acute severe ulcerative colitis. Inflamm Bowel Dis. 2019;25(7):1169–1186. doi:10.1093/ibd/izy383
64. Laharie D, Bourreille A, Branche J, et al. Long-term outcome of patients with steroid-refractory acute severe UC treated with ciclosporin or infliximab. Gut. 2018;67(2):237–243. doi:10.1136/gutjnl-2016-313060
65. Chapin RW, Lee T, McCoy C, Alonso CD, Mahoney MV. Bezlotoxumab: could this be the answer for clostridium difficile recurrence? Ann Pharmacother. 2017;51(9):804–810. doi:10.1177/1060028017706374
66. Orth P, Xiao L, Hernandez LD, et al. Mechanism of action and epitopes of Clostridium difficile toxin B-neutralizing antibody bezlotoxumab revealed by X-ray crystallography. J Biol Chem. 2014;289(26):18008–18021. doi:10.1074/jbc.M114.560748
67. Wilcox MH, Gerding DN, Poxton IR, et al. Bezlotoxumab for prevention of recurrent clostridium difficile infection. N Engl J Med. 2017;376(4):305–317. doi:10.1056/NEJMoa1602615
68. Merck Sharp and Dohme Corp. Zinplava (bezlotoxumab) package insert; 2016. Available from: https://accessdata.fda.gov/drugsatfda_docs/label/2016/761046s000lbl.pdf.revised.
69. Esteve M, Mahadevan U, Sainz E, Rodriguez E, Salas A, Fernandez-Banares F. Efficacy of anti-TNF therapies in refractory severe microscopic colitis. J Crohns Colitis. 2011;5(6):612–618. doi:10.1016/j.crohns.2011.05.001
70. Munch A, Ignatova S, Strom M. Adalimumab in budesonide and methotrexate refractory collagenous colitis. Scand J Gastroenterol. 2012;47(1):59–63. doi:10.3109/00365521.2011.639079
71. Pola S, Fahmy M, Evans E, Tipps A, Sandborn WJ. Successful use of infliximab in the treatment of corticosteroid dependent collagenous colitis. Am J Gastroenterol. 2013;108(5):857–858. doi:10.1038/ajg.2013.43
72. Hirano I, Collins MH, Assouline-Dayan Y, et al. RPC4046, a monoclonal antibody against IL13, reduces histologic and endoscopic activity in patients with eosinophilic esophagitis. Gastroenterology. 2019;156(3):592–603 e510. doi:10.1053/j.gastro.2018.10.051
73. Dellon ES, Collins MH, Rothenberg ME, et al. Long-term efficacy and tolerability of RPC4046 in an open-label extension trial of patients with eosinophilic esophagitis. Clin Gastroenterol Hepatol. 2021;19(3):473–483 e417. doi:10.1016/j.cgh.2020.03.036
74. Assa’ad AH, Gupta SK, Collins MH, et al. An antibody against IL-5 reduces numbers of esophageal intraepithelial eosinophils in children with eosinophilic esophagitis. Gastroenterology. 2011;141(5):1593–1604. doi:10.1053/j.gastro.2011.07.044
75. Stein ML, Collins MH, Villanueva JM, et al. Anti-IL-5 (mepolizumab) therapy for eosinophilic esophagitis. J Allergy Clin Immunol. 2006;118(6):1312–1319. doi:10.1016/j.jaci.2006.09.007
76. Straumann A, Conus S, Grzonka P, et al. Anti-interleukin-5 antibody treatment (mepolizumab) in active eosinophilic oesophagitis: a randomised, placebo-controlled, double-blind trial. Gut. 2010;59(1):21–30. doi:10.1136/gut.2009.178558
77. Spergel JM, Rothenberg ME, Collins MH, et al. Reslizumab in children and adolescents with eosinophilic esophagitis: results of a double-blind, randomized, placebo-controlled trial. J Allergy Clin Immunol. 2012;129(2):
78. Ludvigsson JF, Leffler DA, Bai JC, et al. The Oslo definitions for coeliac disease and related terms. Gut. 2013;62(1):43–52. doi:10.1136/gutjnl-2011-301346
79. Raiteri A, Granito A, Giamperoli A, Catenaro T, Negrini G, Tovoli F. Current guidelines for the management of celiac disease: a systematic review with comparative analysis. World J Gastroenterol. 2022;28(1):154–175. doi:10.3748/wjg.v28.i1.154
80. Gillett HR, Arnott ID, McIntyre M, et al. Successful infliximab treatment for steroid-refractory celiac disease: a case report. Gastroenterology. 2002;122(3):800–805. doi:10.1053/gast.2002.31874
81. Rawal N, Twaddell W, Fasano A, Blanchard S, Safta A. Remission of refractory celiac disease with infliximab in a pediatric patient. ACG Case Rep J. 2015;2(2):121–123. doi:10.14309/crj.2015.25
82. Costantino G, Della Torre A, Lo Presti MA, Caruso R, Mazzon E, Fries W. Treatment of life-threatening type I refractory coeliac disease with long-term infliximab. Dig Liver Dis. 2008;40(1):74–77. doi:10.1016/j.dld.2006.10.017
83. Vivas S, de Morales JMR, Ramos F, Suárez-Vilela D. Alemtuzumab for refractory celiac disease in a patient at risk for enteropathy-associated T-cell lymphoma. N Engl J Med. 2006;354(23):2514–2515. doi:10.1056/NEJMc053129
84. Castillo EF, Schluns KS. Regulating the immune system via IL-15 transpresentation. Cytokine. 2012;59(3):479–490. doi:10.1016/j.cyto.2012.06.017
85. Sestak K, Dufour JP, Liu DX, et al. Beneficial effects of human anti-interleukin-15 antibody in gluten-sensitive rhesus macaques with celiac disease. Front Immunol. 2018;9:1603. doi:10.3389/fimmu.2018.01603
86. Lahdeaho ML, Scheinin M, Vuotikka P, et al. Safety and efficacy of AMG 714 in adults with coeliac disease exposed to gluten challenge: a phase 2a, randomised, double-blind, placebo-controlled study. Lancet Gastroenterol Hepatol. 2019;4(12):948–959. doi:10.1016/S2468-1253(19)30264-X
87. Kirchgesner J, Lemaitre M, Carrat F, Zureik M, Carbonnel F, Dray-Spira R. Risk of serious and opportunistic infections associated with treatment of inflammatory bowel diseases. Gastroenterology. 2018;155(2):337–346 e310. doi:10.1053/j.gastro.2018.04.012
88. Lemaitre M, Kirchgesner J, Rudnichi A, et al. Association between use of thiopurines or tumor necrosis factor antagonists alone or in combination and risk of lymphoma in patients with inflammatory bowel disease. JAMA. 2017;318(17):1679–1686. doi:10.1001/jama.2017.16071
89. Lichtenstein GR, Feagan BG, Cohen RD, et al. Infliximab for Crohn’s Disease: more than 13 years of real-world experience. Inflamm Bowel Dis. 2018;24(3):490–501. doi:10.1093/ibd/izx072
90. Hisamatsu T, Suzuki Y, Kobayashi M, et al. Long-term safety and effectiveness of Adalimumab in Japanese patients with Crohn’s disease: 3-year results from a real-world study. Intest Res. 2021;19(4):408–418.
91. Curtis JR, Mariette X, Gaujoux-Viala C, et al. Long-term safety of certolizumab pegol in rheumatoid arthritis, axial spondyloarthritis, psoriatic arthritis, psoriasis and Crohn’s disease: a pooled analysis of 11 317 patients across clinical trials. RMD Open. 2019;5(1):e000942. doi:10.1136/rmdopen-2019-000942
92. Dulai PS, Singh S, Jiang X, et al. The real-world effectiveness and safety of vedolizumab for moderate-severe Crohn’s Disease: results from the US VICTORY consortium. Am J Gastroenterol. 2016;111(8):1147–1155. doi:10.1038/ajg.2016.236
93. Rutgeerts P, Gasink C, Chan D, et al. Efficacy of ustekinumab for inducing endoscopic healing in patients with Crohn’s Disease. Gastroenterology. 2018;155(4):1045–1058. doi:10.1053/j.gastro.2018.06.035
94. Harris RJ, McDonnell M, Young D, et al. Early real-world effectiveness of ustekinumab for Crohn’s disease. Frontline Gastroenterol. 2020;11(2):111–116. doi:10.1136/flgastro-2019-101237
95. Hirano I, Dellon ES, Hamilton JD, et al. Efficacy of dupilumab in a Phase 2 randomized trial of adults with active eosinophilic esophagitis. Gastroenterology. 2020;158(1):111–122 e110. doi:10.1053/j.gastro.2019.09.042
96. Nielsen OH, Gubatan JM, Juhl CB, Streett SE, Maxwell C. Biologics for inflammatory bowel disease and their safety in pregnancy: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2022;20(1):74–87 e73. doi:10.1016/j.cgh.2020.09.021
97. Mariette X, Forger F, Abraham B, et al. Lack of placental transfer of certolizumab pegol during pregnancy: results from CRIB, a prospective, postmarketing, pharmacokinetic study. Ann Rheum Dis. 2018;77(2):228–233. doi:10.1136/annrheumdis-2017-212196
98. Clowse ME, Forger F, Hwang C, et al. Minimal to no transfer of certolizumab pegol into breast milk: results from CRADLE, a prospective, postmarketing, multicentre, pharmacokinetic study. Ann Rheum Dis. 2017;76(11):1890–1896. doi:10.1136/annrheumdis-2017-211384
99. Narula N, Al-Dabbagh R, Dhillon A, Sands BE, Marshall JK. Anti-TNFalpha therapies are safe during pregnancy in women with inflammatory bowel disease: a systematic review and meta-analysis. Inflamm Bowel Dis. 2014;20(10):1862–1869. doi:10.1097/MIB.0000000000000092
100. Moens A, van der Woude CJ, Julsgaard M, et al. Pregnancy outcomes in inflammatory bowel disease patients treated with vedolizumab, anti-TNF or conventional therapy: results of the European CONCEIVE study. Aliment Pharmacol Ther. 2020;51(1):129–138. doi:10.1111/apt.15539
101. Gisbert JP, Chaparro M. Safety of new biologics (Vedolizumab and Ustekinumab) and small molecules (Tofacitinib) during pregnancy: a review. Drugs. 2020;80(11):1085–1100. doi:10.1007/s40265-020-01346-4
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.