")
Back to Journals » International Journal of General Medicine » Volume 15
Bilateral Lower Limbs Cellulitis: A Narrative Review of an Overlooked Clinical Dilemma
Authors Chuang YC , Liu PY , Lai KL, Tseng CH
Received 19 January 2022
Accepted for publication 24 May 2022
Published 9 June 2022 Volume 2022:15 Pages 5567—5578
DOI https://doi.org/10.2147/IJGM.S356852
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yu-Chuan Chuang,1 Po-Yu Liu,2– 4 Kuo-Lung Lai,5,* Chien-Hao Tseng2,*
1Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan; 2Division of Infectious Disease, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan; 3Rong Hsing Research Center for Translational Medicine, National Chung Hsing University, Taichung, Taiwan; 4Ph.D. Program in Translational Medicine, National Chung Hsing University, Taichung, Taiwan; 5Division of Allergy, Immunology and Rheumatology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
*These authors contributed equally to this work
Correspondence: Chien-Hao Tseng, Division of Infectious Disease, Department of Internal Medicine, Taichung Veterans General Hospital, No. 1650, Sec. 4, Taiwan Blvd., Xitun Dist, Taichung City, 407219, Taiwan, Tel +886 4 2359 2525 Extension 3081, Email [email protected]
Abstract: Bilateral lower limbs cellulitis is a rare clinical condition, which has been overlooked for a long time. In daily clinical practice, bilateral cellulitis is a sporadically encountered condition; however, it remains a clinical challenge. There is a broad differential diagnosis for this clinical entity, and there is a lack of accepted international diagnostic criteria. Unnecessary antibiotic prescription is common, which has led to an emerging problem. In this review, we summarize case reports of bilateral lower limbs cellulitis and common pathogens that have been documented.
Keywords: cellulitis, bilateral, legs, lower limbs, lower extremities
Introduction
Cellulitis, a common bacterial skin infection, typically presents with a poorly demarcated erythematous skin lesion, edema, warmth, and tenderness. When the skin barrier is breached, microorganisms may enter via skin integrity defects and cause infections.1 Sometimes cellulitis may be secondary to hematogenous seeding of causative pathogens, or it results from direct spread of subjacent infections, such as subcutaneous abscesses, fistulas or osteomyelitis.2
It is a well-known fact that cellulitis is most often unilateral. Although it may affect any part of the body, the lower extremities are involved most frequently.3 Bilateral involvement should always prompt consideration of other diagnoses. In fact, in the absence of specific risk factors such as skin trauma, bilateral involvement is usually rare.1,4 Lower extremity cellulitis is caused by direct invasion of the affected limb by the offending organism. As a result, bilateral cellulitis tends to indicate the existence of an identifiable predisposing risk factor, either an independent invasion of both legs by bacteria or underlying comorbidities. Thus, bilateral lower limbs cellulitis must be distinguished from other noninfectious causes. We should take all possible alternative diagnosis into careful consideration.
Materials and Methods
Systematic Review
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines,5 we conducted a review of all studies on patients with bilateral lower limbs cellulitis. However, since all the collected literatures are case reports, there will be a significant degree of bias. It is reasonable that we have only completed a narrative review.
Literature Search Strategy and Case Report Selection
We performed a thorough literature search using PubMed. The available data were identified by searching PubMed (from 1990 until March 2022), current contents, and references from relevant articles. For the bibliographic search, MeSH terminology was used using the following search strategy: [(cellulitis) AND (bilateral) AND (Legs OR “Lower Extremity” [Mesh] OR lower extremities OR lower limb)]. The bibliographic search was done by two researchers. All duplicates were eliminated. Two independent researchers reviewed the chosen contents and determined whether these articles met all inclusion criteria. For documents where there was no consensus, we consulted a third researcher to help reach a consensus.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) the final diagnosis was categorized as cellulitis; (2) it included bilateral leg involvement; (3) the date of publication was between January 1, 1990 and March 16, 2022; and (4) the language of publication was English or there were English abstracts with enough important information on PubMed.
Study Selection
Our search uncovered 126 bibliographic references to articles published between January 1, 1990 and March 16, 2022. There were no duplicate references so the selection of articles was determined according to the inclusion criteria set forth above. The PRISMA 2020 flow diagram for literature screening can be viewed in Figure 1. After screening of records, 81 records did not meet the inclusion criteria. Hence, 45 full-text articles were assessed for eligibility. Twenty-seven of them were excluded because the final diagnosis was not cellulitis and 5 of them were excluded due to the lack of emphasis on “simultaneous infection” in both lower extremities, which did not meet the inclusion criteria. Finally, 13 documents were selected for analysis, which comprised a total of 13 cases.
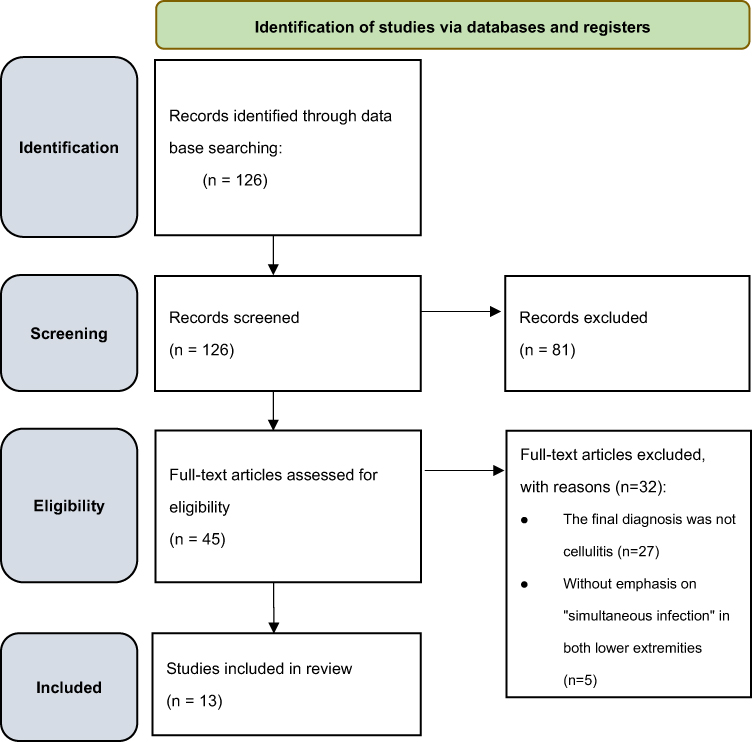 |
Figure 1 Flow diagram of the study selection process. |
Data Extraction
We extracted data from all selected case reports using a standardized table. The data were grouped as follows: author, year of publication, countries, age, gender, the diagnosis of bilateral lower limbs cellulitis, comorbid conditions, causative organism, antimicrobial treatment, and outcome. The collected data were entered into standardized data extraction sheets using Microsoft Excel 2019 (Microsoft Corp, Seattle, WA) for data extraction.
Results and Discussion
Epidemiology
Cellulitis is a common clinical problem with an incidence of around 200 per 100,000 person-years.6 The incidence of cellulitis has been associated with age, and therefore the elderly are disproportionately affected; however, there was no obvious gender difference among patients with cellulitis.6
In our research, 13 documents were selected for analysis with a total of 13 cases. In this study, our search uncovered 126 bibliographic references. Figure 2 shows the distribution of bilateral leg cellulitis by year of reporting. Only 13 cases with definite bilateral cellulitis have been reported since 1990. The 13 cases came from only three countries: six in the United States, six in Japan, and one in Australia. More than half of the reported cases occurred after 2016. There has been an increase in published cases of bilateral cellulitis since 2010; however, the number of reported cases remains sparse.
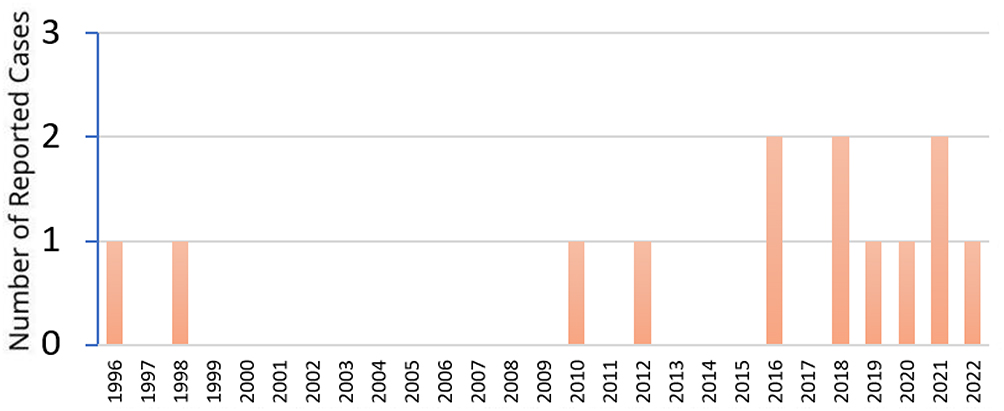 |
Figure 2 Distribution of bilateral leg cellulitis by year of reporting. |
Many experts and researchers have suggested that bilateral lower legs cellulitis is a rare clinical condition.7 Physicians may encounter a clinical challenge in diagnosing lower limb cellulitis. Since misdiagnosis is common, it is difficult to accurately calculate the incidence of bilateral lower legs cellulitis. Many patients with an alternative diagnosis initially presented with features of typical cellulitis.8 Further investigation was necessary so as to determine the true incidence.
Microbiology
When it comes to cellulitis, the usual pathogens are beta-hemolytic streptococci (groups A, B, C, F, and G), with group A Streptococcus (Streptococcus pyogenes) being the most common. Staphylococcus aureus is another common cause that the physician should be considered.1 Moreover, gram-negative organisms also occupy a certain proportion in patients with cellulitis.9 In immunocompromised patients, the spectrum of potential pathogens is much broader, and rare opportunistic pathogens (eg, Helicobacter cinaedi, Cryptococcus species, Fusarium species) should be alerted.10
For bilateral lower limbs cellulitis, common pathogens of cellulitis should also be taken into priority consideration. For instance, beta-hemolytic streptococci and Staphylococcus aureus may still cause most bilateral lower limbs cellulitis. However, individualized consideration should be established, since different risk factors are linked to specific pathogens. Clarifying the underlying comorbidities and structural anomalies is important in a clinical setting. We summarize the special considerations for patients with underlying comorbid conditions in Table 1.
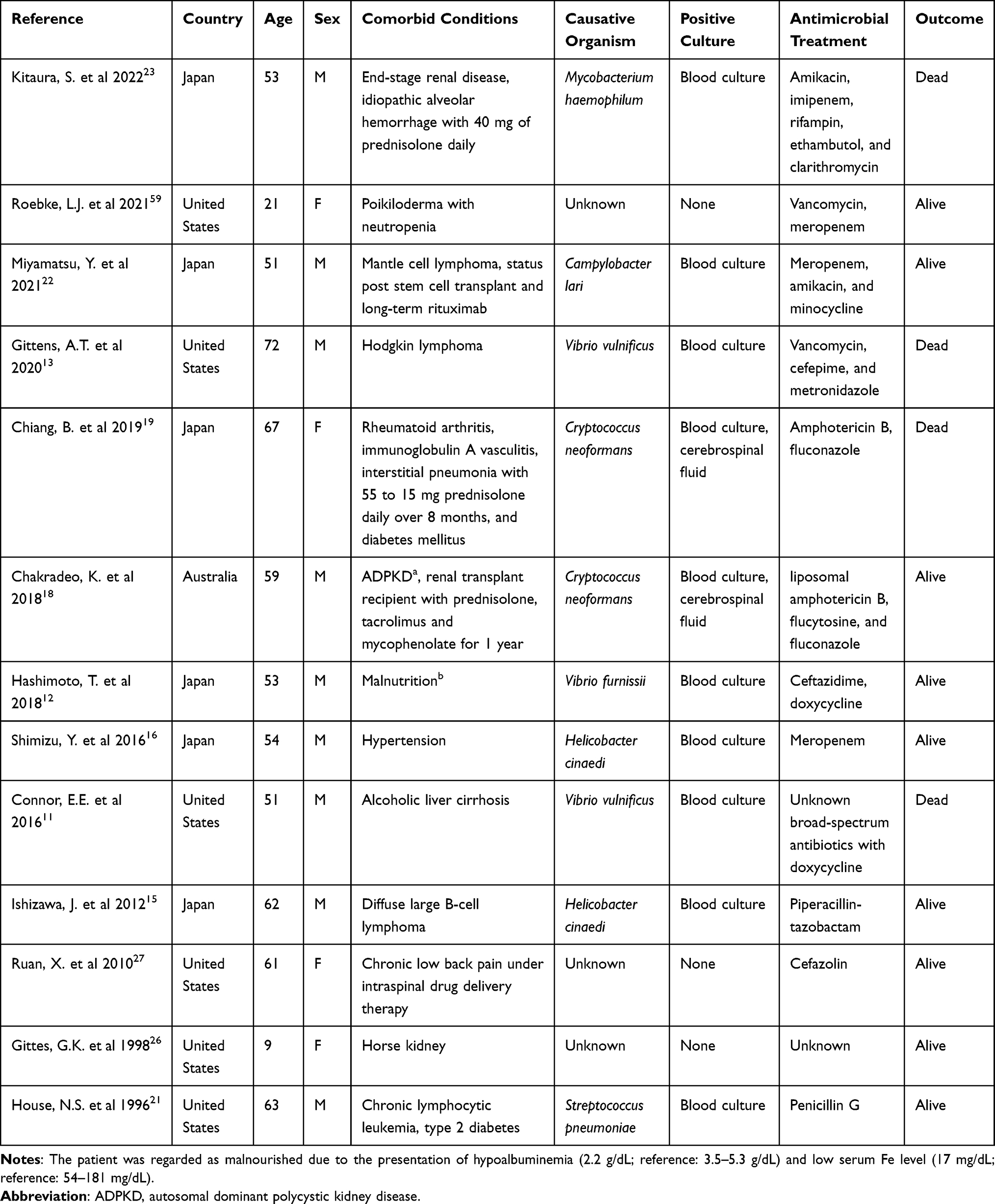 |
Table 1 The Characteristics of the Patients with Bilateral Cellulitis |
Definite pathogens were isolated in 10 cases with Vibrio species in 3 of all cases.11–13 Vibrio vulnificus accounted for 2 cases and Vibrio furnissii was responsible for 1 case. V. vulnificus potentially infects wounds that have been exposed to estuarine or sea water, shellfish, or fish. In these reported cases, immunocompromised status, especially liver cirrhosis, is a major risk factor that should be recognized. Most soft tissue infections from V. vulnificus and V. furnissii had a contact history of saltwater or undercooked seafood.10,13,14 However, in the 3 cases of Vibrio related bilateral lower limbs cellulitis, no one could be traced to seawater or seafood exposure. Although 2 cases had diarrhea a few days before admission.
Helicobacter cinaedi was noted in 2 cases.15,16 Indeed, H. cinaedi, a fastidious bacterium that grows slowly and requires strict culture conditions, is not a common organism in cellulitis; patients who are immunocompromised are vulnerable, nonetheless.17 The diagnosis of H. cinaedi infection is difficult, so it is important to be alert to the possibility of bilateral lower limbs cellulitis caused by this pathogen.
Cryptococcus neoformans also accounted for 2 cases.18,19 They are both immunocompromised patients with long-term immunosuppressive agents. One had rheumatoid arthritis with interstitial pneumonia and was treated with oral prednisolone from 55 to 15 mg per day over 8 months. Another one had received a kidney transplant and was on immunosuppression including prednisolone, tacrolimus and mycophenolate about 1 year. They were both diagnosed with disseminated cryptococcosis with positive blood culture and cerebrospinal fluid culture. Disseminated cryptococcal infection in immunosuppressed patients most commonly presents with pulmonary or central nervous system (CNS) symptoms initially. Cutaneous symptoms occur as a secondary manifestation of hematogenous spread and present different clinical morphologies, including ulcers, acneiform papules, subcutaneous nodules, and cellulitis.20 However, in these two cases, there are no clinical symptoms to suggest either pulmonary or CNS involvement at first. Cellulitis as the initial presenting symptom in disseminated cryptococcal infection is rare but exists.
In the remaining cases of bilateral cellulitis, several less common causative organisms were also documented, including Streptococcus pneumoniae, Campylobacter lari, and Mycobacterium haemophilum.21–23 However, isolation of these pathogens may be difficult not only due to the low organism yield rate in the cellulitis but also because of the lack of reliable methods for detecting pathogens such as C. lari.
Previous literature indicated that the proportion of cellulitis with positive blood culture results was quite low, generally less than ten percent.10 However, in the thirteen case reports we found with cellulitis of both lower extremities, ten were with positive blood cultures. It may be a hypothesis that cellulitis in both lower extremities is associated with an increased rate of positive blood cultures. And the reason may be that the bilateral cellulitis was secondary to disseminated disease or that the large infectious burden (bilateral) made it became bloodstream infection easily.
Risk Factors
There are various predisposing factors linked to lower limb cellulitis. Several important factors identified in previous studies can be categorized into systemic and local factors. Systemic factors include a history of cellulitis, elderly, obesity, venous insufficiency, saphenous venectomy for coronary artery bypass surgery, edema, and lymphedema. In contrast, local factors involve skin surface disruption, which can be related to trauma, ulceration, or inflammatory diseases of the skin, such as atopic dermatitis, contact dermatitis, and venous eczema.24,25
In cases of bilateral cellulitis, several comorbid conditions were reported. Malignancy including lymphoma and leukemia was noted in 4 cases.13,15,21,22 In brief, immunosuppressed hosts with malignancy, diabetes mellitus, liver cirrhosis, or organ transplant recipient, seemed to have a higher risk of bilateral involvement with cellulitis. Four cases had long-term use of immunosuppressive agents, including prednisolone, tacrolimus, mycophenolate and rituximab.18,19,22,23 Moreover, it is important to pay attention to anatomical deformity in cases of bilateral leg cellulitis. For instance, urinary tract anomaly in a patient with inferior vena cava obstruction from a horseshoe kidney was also related to the occurrence of bilateral cellulitis.26 Underlying comorbidity of liver cirrhosis is another risk factor. Bilateral lower limbs cellulitis with pathogens of Vibrio vulnificus was reported in patients with underlying liver cirrhosis.11
A special consideration in bilateral cellulitis is long-term intrathecal morphine administration. Several side effects have been associated with long-term use of intrathecal morphine, and leg edema is a complication that is increasingly being recognized. Accordingly, it is crucial that the treating physician be alert to this possibility in bilateral cellulitis patients with a history of long-term intrathecal morphine administration.27
Although not emphasized by these case reports, local factors involving skin surface disruption should be carefully examined during history taking and physical examination. Trauma with environmental exposure or bilateral abrasion due to improper shoe size or ill-fitting shoes must be discerned.28 Inflammatory diseases of the skin play a key role in the development of cellulitis.24,25 For example, a patient with stasis dermatitis may develop a secondary infection. Stasis dermatitis is a well-known mimicker of cellulitis, especially when there is bilateral involvement. Nevertheless, patients may develop concomitant superficial infection when an acute flare occurs.
Clinical Manifestations
Cellulitis typically presents with certain features, as follows: “rubor,” “dolor,” “calor,” and “tumor” or erythema, pain, warmth, and edema. The classic presentation of the borders in cellulitis are ill-defined and relatively smooth.29 Local features also include petechiae and hemorrhage, as well as superficial bullae, which may occur in the involved skin region. In contrast, for patients with sensation of pruritus or burning, which is less common in cellulitis, other diagnoses should be considered in the first differential diagnosis.25
In our review of the literature, we found several cases with a diagnosis of bilateral lower limbs cellulitis, and although it is less common, true infection should be taken into consideration, especially in patients with underlying immunosuppression. In cases of bilateral cellulitis, not only typical features may be seen but also other systemic manifestations. For instance, in the cases we analyzed, most of the patients presented with fever and chills. The physician should arrange blood culture for further bacterial investigation, especially in cases with systemic symptoms other than local presentation of cellulitis. Some patients also presented with gastrointestinal symptoms, such as nausea and vomiting.13 A few patients had prolonged symptoms with the presentation of pain in both legs and erythema for more than one month.16,18 Another important presentation with bilateral lower leg involvement is recurrent episodes that were observed in several patients. If the predisposing factors are not removed, these patients might suffer recurrent infection. A case of 61-year-old woman with intractable chronic low back pain who was treated with intrathecal morphine use, developed recurrent cellulitis.27 In another case, a patient with urinary tract anomaly and inferior vena cava obstruction from a horseshoe kidney also suffered recurrent bilateral cellulitis.26 When a patient with recurrent episodes is encountered, it is important to search for modifiable risk factors.
We paid attention to the early clinical signs from cellulitis to necrotizing fasciitis, which was associated with higher mortality and required emergent surgical intervention. Marked pain or tenderness out of proportion, the rapidly progressive extent of swelling or redness, violaceous bullae, shock, necrosis of skin and subcutaneous tissue were the clinical clues for us to be alert to necrotizing fasciitis.1,10,30 For 13 cases of bilateral lower limbs cellulitis in Table 1, three cases had the necessary of surgical debridement.11,13,21 Vibrio vulnificus accounted for 2 cases and Streptococcus pneumoniae was responsible for 1 case. All three cases were compatible with most symptoms or signs described above, either presenting initially or developing during hospitalization.
Differential Diagnosis
It is not uncommon to mistake a noninfectious disorder or an inflammatory dermatologic disorder as cellulitis.31 Lower leg erythema with bilateral distribution should prompt an alternative diagnosis, particularly in patients without other symptoms of cellulitis. The differential diagnosis of bilateral lower limbs cellulitis is presented in Table 2.
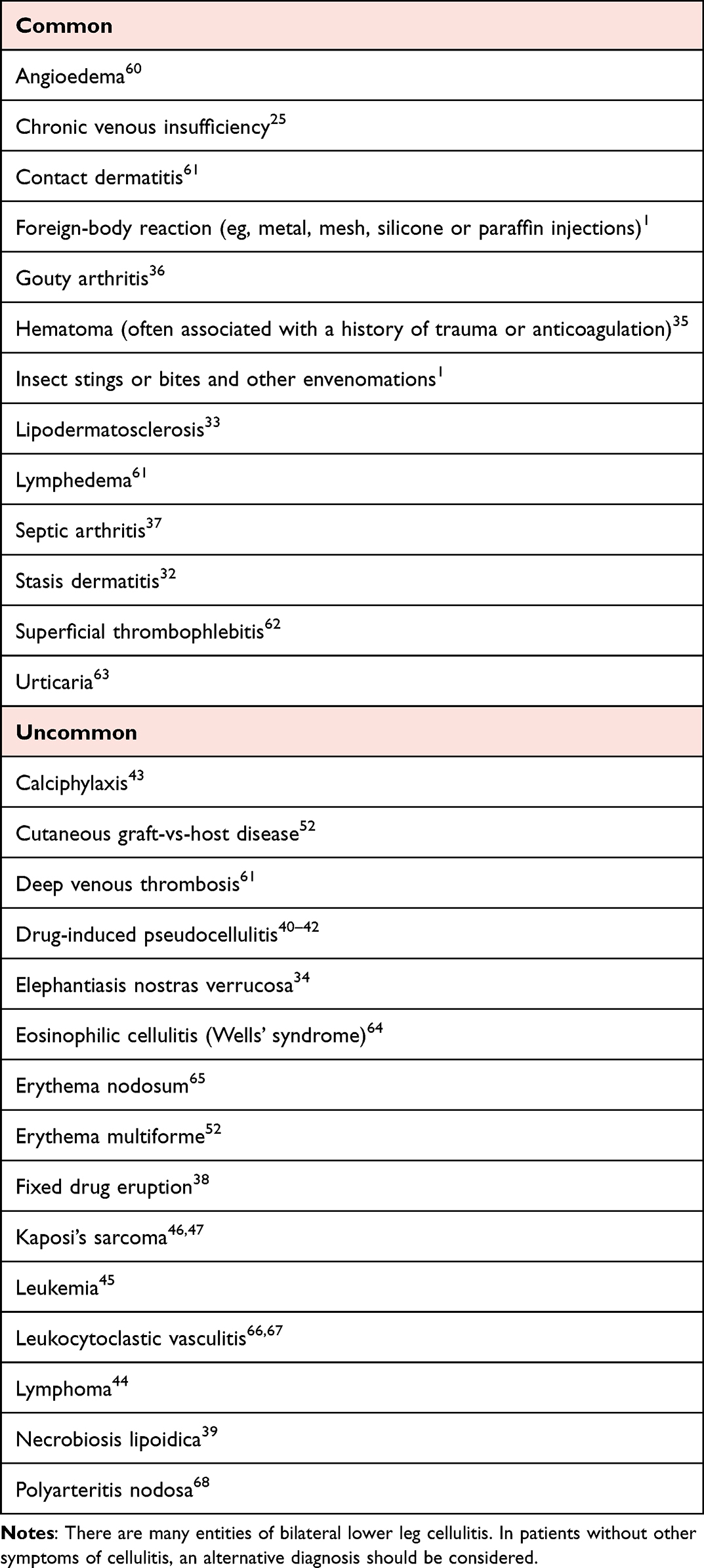 |
Table 2 Common Differential Diagnosis of Bilateral Lower Legs Cellulitis |
Stasis dermatitis is the most common condition to be misdiagnosed as cellulitis.32 Stasis dermatitis can be distinguished by its bilateral nature in a condition without bilateral involvement; however, this may be difficult since bilateral cellulitis and stasis dermatitis share many common features. A history of lower extremity chronic venous disease raises the possibility of a differential diagnosis of chronic venous insufficiency, lipodermatosclerosis, or less commonly, elephantiasis nostras verrucosa.25,33,34 Although it is important to distinguish these venous-related diseases from bilateral cellulitis, it should be borne in mind that these patients are more prone to concomitant cellulitis. Another common condition that is generally misdiagnosed as bilateral cellulitis is hematoma, which is often associated with a history of anticoagulation medication use or trauma.35 Gouty arthritis and septic arthritis also mimic bilateral cellulitis when multiarticular involvement is noted.36,37 Serum uric acid level as well as arthrocentesis may be useful in such cases, especially when the erythema region overlaps the joints. Several dermatologic diseases are also frequently seen, such as contact dermatitis, urticaria, angioedema, or superficial thrombophlebitis. Insect stings or bites, other envenomations, and foreign-body reactions (eg, metal, mesh, silicone or paraffin injections) can be determined by thorough history taking.1
Less common dermatologic diseases included fixed drug eruption, eosinophilic cellulitis (also known as Wells’ syndrome), erythema nodosum, erythema multiforme, and necrobiosis lipoidica. Fixed drug eruption has the classical manifestation of localized erythematous patches, which recur in the same area whenever the patient is exposed to the offending drug.38 Necrobiosis lipoidica is a rare disease commonly seen in patients with diabetes mellitus. The disease usually causes bilateral lesions with the lower extremities being the most commonly involved region.39 Drug-induced pseudocellulitis should also be taken into consideration. In previous studies, some patients who were treated with gemcitabine or pemetrexed suffered from drug-induced pseudocellulitis.40–42 This is an underrecognized situation and may cause unnecessary antibiotic treatment. A skin biopsy from these patients may reveal drug hypersensitivity reactions. In patients who have end-stage renal disease or are on dialysis, calciphylaxis is an important disease that should not be missed. It is a rare but serious disorder which manifests as skin ischemia and necrosis. The involvement is usually bilateral with the lower extremities most commonly involved.43
In patients with hematologic malignancies such as lymphoma and leukemia, patients may present with cutaneous manifestations. Careful physical examinations and laboratory findings, as well as skin histopathology of the lesions, are crucial for diagnosis.44,45 Kaposi sarcoma usually occurs over the distal portion of the lower extremities. Nevertheless, the initial lesion may present at unusual locations without distal extremity involvement.46,47
Assessment and Diagnosis
There is no consensus regarding the diagnosis of cellulitis and specific diagnostic criteria do not exist, but the alert physician can find clues in the history and physical examination that point toward cellulitis.7 Symptoms of pain and erythema with laboratory findings of leukocytosis are usually suggestive of cellulitis, especially in patients with a history of trauma. Since the diagnosis of cellulitis is usually based on clinical manifestations, there is no difference in the diagnosis of bilateral cellulitis. However, diagnosing cellulitis is not as easy as previously thought. A previous study in the UK demonstrated a high rate of misdiagnosis. In the study, patients who were admitted with the presentation of erythematous change of bilateral legs were misdiagnosed as bilateral cellulitis in 15 out of 50 patients.48 Similarly, in a previous study carried out in the United States, misdiagnosis occurred in around 28% of patients.32
Misdiagnosis of bilateral cellulitis is a common problem that can lead to overuse of antibiotics and subject patients to potentially unnecessary hospital stays.31 In cases of cellulitis of bilateral lower legs as well as unilateral lower extremity, the physician should perform a thorough history taking and physical examination. Detailed history collection may help upon differentiating the bilateral cellulitis from its mimicking conditions.49 Chemotherapeutic agents such as gemcitabine and pemetrexed were reported to cause pseudocellulitis. It is important to clarify whether the patient was under treatment by these chemotherapeutic agents because the treatment may differ from the infectious-related condition. In the setting of drug-induced cellulitis, the symptoms are resolved with discontinuation or dose reduction of the treatment. Moreover, these patients might not respond well to the antibiotic treatment and might benefit from systemic or topical steroid use.41,42 Previous surgical history should be collected: for instance, patients who received bilateral total knee replacements were predisposed to cellulitis, arthritis, or deep vein thrombosis.50,51 In addition to the classic presentation with erythema, swollen, local heat, and tenderness, the physician should look for other risk factors, including the absence of dorsalis pedis and posterior tibial pulses, lower limbs edema, clinical signs of venous disease, and fissuring, scaling, or maceration over the interdigital toe spaces.52
Bilateral lesions on the legs are frequently treated with antibiotics for presumed cellulitis. Nevertheless, it is important to perform a wound culture, pus or discharge culture, blood culture, or even culture of a skin biopsy in the setting of bilateral involvement. Definite culture reports are cardinal in guiding the appropriate antibiotic adjustment. A 53-year-old man with a diagnosis of disseminated Mycobacterium haemophilum infection initially presented as cellulitis of bilateral lower extremities. The mycobacterial blood culture turned positive after 24 days. However, the skin biopsy revealed abundant acid-fast bacilli in Ziehl-Neelsen stain with negative result of polymerase chain reaction for Mycobacterium tuberculosis. The patient was therefore treated as nontuberculous mycobacteria infection quite earlier.23 It is essential to arrange a biopsy of the involved skin region if the lesions are not responding to the empirical antibiotic administration, or if, there is another differential diagnosis that can better explain the clinical condition.46
Due to the aforementioned dilemma, it may be helpful to consult with a dermatologist in the early stage of the disease; moreover, pathology studies may also be needed. Consultation is essential so as to avoid misdiagnosis and to prescribe the treatment accurately diagnosed with a proper treatment plan.31,46 The role of a dermatologist in diagnosing cellulitis has been widely discussed. Some experts have suggested the development of algorithms to help provide an accurate diagnosis, which may also be useful in cases with bilateral involvement.53 The differential diagnosis of bilateral lower limbs cellulitis encompasses a broad range of conditions and diseases, which are predominantly dermatologic diseases. Teledermatology may provide benefits for affected patients.53
Since bilateral lower limbs cellulitis is more complicated, it is crucial to follow up carefully to monitor disease progression and treatment response. The efficacy of the treatment gives a clue as to whether the current diagnosis is accurate. It may also prompt the physician to search for an alternative diagnosis if the presentation does not match expectations.49
Treatment
It is often difficult to obtain a definitive bacterial report in cases of cellulitis, mostly due to the low yield rate from skin biopsy, needle aspiration, and blood culture. As a consequence, most patients were treated with a course of empirical treatment.54
In the situation of bilateral lower limbs involvement, there is no consensus nor treatment guideline. Nevertheless, the concepts related to and the criteria used for typical cases of cellulitis may help. For instance, it is still possible to initially categorize whether the lesion is purulent or non-purulent. In patients with purulent skin and soft tissue infection, the physician should consider performing incision and drainage and arranging bacterial culture before prescribing antibiotic treatment.55 Regarding cases of non-purulent skin and soft tissue infections, systemic antibiotics are also necessary. Initial evaluation may take advantage of the clinical criteria for systemic inflammatory response syndrome (SIRS). For instance, a patient who meets only one SIRS criterion is more likely to respond to oral agents. In contrast, for patients meeting two or more SIRS criteria, an intravenous regimen should be considered.1 It is also essential to assess the risk and the likelihood of resistant pathogens for individual patients.
Other considerations for specific antibiotic use include the occurrence of cellulitis following exposure to human or animal bite or exposure to estuarine or sea waters, shellfish, or fish. A 72-year-old man with Hodgkin lymphoma had bilateral lower extremities cellulitis with hemorrhagic bullae. Empirical treatments with broad-spectrum antibiotics were given, including meropenem, vancomycin and metronidazole, but without any tetracycline. The patient worsened quickly and died. Blood cultures isolated V. vulnificus from anaerobic bottles posthumously.13 The combinations of a third-generation cephalosporin with doxycycline had lower mortality rates than monotherapy in Vibrio infections.56,57 For patients with a presumptive diagnosis of Vibrio septicemia, empirical treatment should be a combination therapy including doxycycline. Moreover, patients with certain underlying conditions such as immunocompromised status and splenectomy require broad-spectrum antibiotics.52 In the thirteen cases, we analyzed, empirical treatment with meropenem was seen in three cases with one of them suffering from the comorbid condition of mantle cell lymphoma. Piperacillin-tazobactam was also reported in patients with diffuse large B-cell lymphoma. Patients with multiple co-morbidities or immunocompromised status, are more likely to be infected by a broad range of organisms. These patients should empirically be treated with broad-spectrum antibiotics initially.29 For example, the use of vancomycin with either piperacillin-tazobactam, imipenem, or meropenem is a reasonable recommendation as the initial empiric regimen for severe infection.52
Treatment response should be followed closely and the antibiotic adjusted according to the bacterial report if possible. If the treatment response is not as favorable as anticipated, further adjustment should be considered, and it should always be kept in mind that an alternative diagnosis of bilateral lower limbs cellulitis may mislead our clinical decision. There is no known optimal duration of antibiotic use for cellulitis cases with bilateral involvement. Traditionally, most patients with uncomplicated cellulitis are treated for roughly one to two weeks. However, there is evidence supporting the notion that prolonged antibiotic treatment may be unnecessary. A five-day treatment course should have similar efficacy in cases of uncomplicated cellulitis.58 The physician should also survey for possible predisposing factors, such as tinea pedis or stasis dermatitis, in order to prevent the recurrence of bilateral lower limbs cellulitis.52
Conclusion
Research has suggested that bilateral lower leg cellulitis is very rare; however, a number of cases of bilateral lower limbs cellulitis were identified in our review of the literature. Misdiagnosis of bilateral cellulitis can lead to overuse of antibiotics and may subject patients to potentially unnecessary hospital stays. Local characteristics of the affected area, systemic signs, laboratory tests, and, in some cases, skin biopsy can be helpful in determining the correct diagnosis. It is important to recognize bilateral limb cellulitis, especially in patients with underlying immunocompromised conditions, which may place the patient at risk of developing clinical emergency. Upon encountering patients with suspected bilateral lower limbs cellulitis, it is crucial to obtain bacterial reports if possible. A definitive identification of pathogens collected via needle aspiration, pus culture, tissue culture, blood culture, or even skin biopsy may help guide the antibiotic choice. Our review comes with great limitations: we only summarize case reports, and there may be many inherent biases. However, there is not much attention or related literature on bilateral lower limbs cellulitis. Further investigation of true bilateral lower limbs cellulitis is necessary, particularly with respect to diagnosis and management. We hope this review can attract more people to pay attention to this topic.
Funding
CH Tseng was supported in part by the Taichung Veterans General Hospital (TCVGH-DYU118302).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Raff AB, Kroshinsky D. Cellulitis: a Review. JAMA. 2016;316(3):325–337. doi:10.1001/jama.2016.8825
2. Pasternack MS, Swartz MN. Cellulitis, Necrotizing Fasciitis, and Subcutaneous Tissue Infections. In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases.
3. Lazzarini L, Conti E, Tositti G, de Lalla F. Erysipelas and cellulitis: clinical and microbiological spectrum in an Italian tertiary care hospital. J Infect. 2005;51(5):383–389.
4. Dupuy A, Benchikhi H, Roujeau J-C, et al. Risk factors for erysipelas of the leg (cellulitis): case-control study. BMJ. 1999;318(7198):1591–1594.
5. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
6. McNamara DR, Tleyjeh IM, Berbari EF, et al. Incidence of lower-extremity cellulitis: a population-based study in Olmsted County, Minnesota. Mayo Clin Proc. 2007;82(7):817–821.
7. Keller EC, Tomecki KJ, Alraies MC. Distinguishing cellulitis from its mimics. Cleve Clin J Med. 2012;79(8):547–552.
8. Patel M, Lee SI, Thomas KS, Kai J. The red leg dilemma: a scoping review of the challenges of diagnosing lower-limb cellulitis. Br J Dermatol. 2019;180(5):993–1000.
9. Gunderson CG, Martinello RA. A systematic review of bacteremias in cellulitis and erysipelas. Journal of Infection. 2012;64(2):148–155.
10. Swartz MN. Clinical practice. Cellulitis. N Engl J Med. 2004;350(9):904–912. doi:10.1056/NEJMcp031807
11. Connor EE, Jackson NR, McGoey RR. Pathology Image Of the Month: rapidly Progressive Hemorrhagic Cellulitis of Bilateral Lower Extremities with Subsequent Septic Shock and Death. J La State Med Soc. 2016;168(3):109–112.
12. Hashimoto T, Takaya S, Kutsuna S, et al. A case report of Vibrio furnissii bacteremia and cellulitis in a malnourished patient without an apparent site of entry. J Infect Chemother. 2018;24(1):65–67.
13. Gittens AT, Clarke JD, Abdelbaki S, Kwon JS. A 72-Year-Old Man With a Violaceous Rash and Sepsis. Chest. 2020;157(2):e41–e45.
14. Ballal M, Shetty V, Bangera SR, Prabhu M, Umakanth S. Vibrio furnissii, an emerging pathogen causing acute gastroenteritis: a Case Report. JMM Case Rep. 2017;4(9):e005111.
15. Ishizawa J, Mori T, Tsukada Y, et al. [Recurrent cellulitis due to Helicobacter cinaedi after chemotherapy for malignant lymphoma]. Rinsho Ketsueki. 2012;53(6):623–627.
16. Shimizu Y, Gomi H, Ishioka H, Isono M. Refractory to treat Helicobacter cinaedi bacteremia with bilateral lower extremities cellulitis in an immunocompetent patient. IDCases. 2016;5:9–11.
17. Kawamura Y, Tomida J, Morita Y, Fujii S, Okamoto T, Akaike T. Clinical and bacteriological characteristics of Helicobacter cinaedi infection. J Infect Chemother. 2014;20(9):517–526.
18. Chakradeo K, Paul Chia YY, Liu C, Mudge DW, De Silva J. Disseminated cryptococcosis presenting initially as lower limb cellulitis in a renal transplant recipient - A case report. BMC Nephrol. 2018;19(1):18.
19. Chiang B, Kamiya K, Sato A, et al. Rapid diagnosis by mass spectrometry of disseminated cryptococcosis clinically mimicking refractory bilateral cellulitis. J Dermatol. 2019;46(10):e345–e346.
20. Valente ES, Lazzarin MC, Koech BL, et al. Disseminated Cryptococcosis Presenting as Cutaneous Cellulitis in an Adolescent With Systemic Lupus Erythematosus. Infect Dis Rep. 2015;7(2):5743.
21. House NS, Helm KF, Marks JG. Acute onset of bilateral hemorrhagic leg lesions. Pneumococcal cellulitis. Arch Dermatol. 1996;132(1):
22. Miyamatsu Y, Tanizaki R, Yamada S, Tsujimura I, Wakabayashi H. Cellulitis with persistent bacteremia caused by Campylobacter lari in a patient with mantle-cell lymphoma. IDCases. 2021;23:e01053.
23. Kitaura S, Okamoto K, Wakabayashi Y, et al. A Cold-Blooded Tiptoer: nonresolving Cellulitis in an Immunocompromised Patient. Open Forum Infect Dis. 2022;9(4):ofac074.
24. Bjornsdottir S, Gottfredsson M, Thorisdottir AS, et al. Risk factors for acute cellulitis of the lower limb: a prospective case-control study. Clin Infect Dis. 2005;41(10):1416–1422.
25. Hirschmann JV, Raugi GJ. Lower limb cellulitis and its mimics: part I. Lower limb cellulitis. J Am Acad Dermatol. 2012;67(2):163 e161–112.
26. Gittes GK, Snyder CL, Murphy JP, Ashcraft KW. Inferior vena caval obstruction from a horseshoe kidney: report of a case with operative decompression. J Pediatr Surg. 1998;33(5):764–765.
27. Ruan X, Liu H, Couch JP, Wang F, Chiravuri S. Recurrent cellulitis associated with long-term intrathecal opioid infusion therapy: a case report and review of the literature. Pain Med. 2010;11(6):972–976.
28. Ikpeze TC, Omar A, Elfar JH. Evaluating Problems With Footwear in the Geriatric Population. Geriatr Orthop Surg Rehabil. 2015;6(4):338–340.
29. Bailey E, Kroshinsky D. Cellulitis: diagnosis and management. Dermatol Ther. 2011;24(2):229–239.
30. Yildiz H, Yombi JC. Necrotizing Soft-Tissue Infections. N Engl J Med. 2018;378(10):970.
31. Weng QY, Raff AB, Cohen JM, et al. Costs and Consequences Associated With Misdiagnosed Lower Extremity Cellulitis. JAMA Dermatol. 2017;153(2):141–146.
32. David CV, Chira S, Eells SJ, et al. Diagnostic accuracy in patients admitted to hospitals with cellulitis. Dermatol Online J. 2011;17(3):1.
33. Galsinh H, Singh K, Smith L. Lipodermatosclerosis: the common skin condition often treated as cellulitis. J R Coll Physicians Edinb. 2019;49(1):41–42.
34. Hadian Y, Link D, Dahle SE, Isseroff RR. Elephantiasis nostras verrucosa: an atypical presentation following intrapelvic lymphoma. Dermatol Online J. 2019;25:12.
35. Baek YS, Song JY, Jeong KM, Jeon J. Late-onset extensive haematoma mimicking cellulitis. Int Wound J. 2019;16(1):297–299.
36. Blumberg G, Long B, Koyfman A. Clinical Mimics: an Emergency Medicine-Focused Review of Cellulitis Mimics. J Emerg Med. 2017;53(4):475–484.
37. Long B, Koyfman A, Gottlieb M. Evaluation and Management of Septic Arthritis and its Mimics in the Emergency Department. West J Emerg Med. 2019;20(2):331–341.
38. Ai Van H, Wu Y-H. Neutrophilic fixed drug eruption: a case report and literature review. Dermatologica Sinica. 2020;38(3):190–191.
39. Gupta P, Saikia U, Arora S, De D, Radotra B. Panniculitis: a dermatopathologist’s perspective and approach to diagnosis. Indian J Dermatopathol Diagnostic Dermatol. 2016;3(2):29–41.
40. Gill D, Schrader J, Kelly M, Martinez F, Syed W, Wright J. Gemcitabine associated pseudocellulitis: a missed diagnosis. J Oncol Pharm Pract. 2018;24(7):550–552.
41. Lo Y, Wu WH. Pemetrexed-induced pseudocellulitis. Kaohsiung J Med Sci. 2020;36(11):953–954.
42. Katsenos S, Psara A, Panagou C. Pemetrexed-induced cellulitis: a rare toxicity in non-small cell lung cancer treatment. J Oncol Pharm Pract. 2013;19(1):93–94.
43. Chang JJ. Calciphylaxis: diagnosis, Pathogenesis, and Treatment. Adv Skin Wound Care. 2019;32(5):205–215.
44. Scott JF, Honda K, Lu K. Seemed Like Cellulitis: intravascular Large B-Cell Lymphoma. Am J Med. 2016;129(7):685–687.
45. Chavez MA, Heidari B, Thacker S, Samuel LL, Ogbonna M. Acute Promyelocytic Leukemia Presenting as Bilateral Acute Limb Ischemia and ST Elevation Myocardial Infarction: a Case Report. Cureus. 2020;12(6):e8495.
46. Batra V, Baras A. Bilateral cellulitis. BMJ Case Rep. 2015;2015:bcr2015211117.
47. Khattak M. Bilateral Chest X-Ray Shadowing and Bilateral leg lesions - A case of Pulmonary Kaposi Sarcoma. Webmedcentral. 2016;7(2):548.
48. Elwell R. Developing a nurse-led ‘red legs’ service. Nurs Older People. 2015;27(10):23–27.
49. Hepburn MJ, Dooley DP, Ellis MW. Alternative diagnoses that often mimic cellulitis. Am Fam Physician. 2003;67(12):2471.
50. Rodriguez JA, Ranawat CS, Maniar RN, Umlas ME. Incisional cellulitis after total Hip replacement. J Bone Joint Surg Br. 1998;80(5):876–878.
51. Heo SM, Harris I, Naylor J, Lewin AM. Complications to 6 months following total Hip or knee arthroplasty: observations from an Australian clinical outcomes registry. BMC Musculoskelet Disord. 2020;21(1):602.
52. Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the infectious diseases society of America. Clin Infect Dis. 2014;59(2):147–159.
53. Imadojemu S, Rosenbach M. Dermatologists Must Take an Active Role in the Diagnosis of Cellulitis. JAMA Dermatol. 2017;153(2):134–135.
54. Jeng A, Beheshti M, Li J, Nathan R. The role of beta-hemolytic streptococci in causing diffuse, nonculturable cellulitis: a prospective investigation. Medicine. 2010;89(4):217–226.
55. Sullivan T, de Barra E. Diagnosis and management of cellulitis. Clin Med. 2018;18(2):160–163.
56. Kim SE, Shin SU, Oh TH, et al. Outcomes of Third-Generation Cephalosporin Plus Ciprofloxacin or Doxycycline Therapy in Patients with Vibrio vulnificus Septicemia: a Propensity Score-Matched Analysis. PLoS Negl Trop Dis. 2019;13(6):e0007478.
57. Liu JW, Lee IK, Tang HJ, et al. Prognostic factors and antibiotics in Vibrio vulnificus septicemia. Arch Intern Med. 2006;166(19):2117–2123.
58. Hepburn MJ, Dooley DP, Skidmore PJ, Ellis MW, Starnes WF, Hasewinkle WC. Comparison of short-course (5 days) and standard (10 days) treatment for uncomplicated cellulitis. Arch Intern Med. 2004;164(15):1669–1674.
59. Roebke LJ, Vander Maten JW, Alkhoury G. Hyperbaric oxygen management of recurrent cellulitis in poikiloderma with neutropenia. Am J Med Genet A. 2021;185(7):2150–2152.
60. Nedelea I, Deleanu D. Isolated angioedema: an overview of clinical features and etiology. Exp Ther Med. 2019;17(2):1068–1072.
61. Hirschmann JV, Raugi GJ. Lower limb cellulitis and its mimics: part II. Conditions that simulate lower limb cellulitis. J Am Acad Dermatol. 2012;67(2):
62. Hocevar A, Suput Skvarca D, Tomsic M, Perdan Pirkmajer K. Multifocal Thrombophlebitis and Orbital Cellulitis. Am J Case Rep. 2020;21:e919715.
63. Falagas ME, Vergidis PI. Narrative review: diseases that masquerade as infectious cellulitis. Ann Intern Med. 2005;142(1):47–55.
64. Tan LYC, Wang D, Lee JSS, Ho BWY, Lim JHL. Eosinophilic cellulitis secondary to occult strongyloidiasis, case report. AME Medical Journal. 2021;6:9.
65. Requena L, Requena C. Erythema nodosum. Dermatol Online J. 2002;8(1):4.
66. McCann SE, Dalton SR, Kobayashi TT. Histopathology of bilateral lower extremity inflammatory lymphedema in military basic trainees: a leukocytoclastic vasculitis of the deep vascular plexus. J Cutan Pathol. 2017;44(5):500–503.
67. Buck M, Dumic I, McDermott W, et al. Leukocytoclastic vasculitis as a rare dermatologic manifestation of Crohn’s disease mimicking cellulitis: a case report. BMC Gastroenterol. 2020;20(1):240.
68. Hughes LB, Bridges SL. Polyarteritis nodosa and microscopic polyangiitis: etiologic and diagnostic considerations. Curr Rheumatol Rep. 2002;4(1):75–82.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.