")
Back to Journals » Cancer Management and Research » Volume 9
Bidirectional risk between venous thromboembolism and cancer in East Asian patients: synthesis of evidence from recent population-based epidemiological studies
Authors Kok VC
Received 14 September 2017
Accepted for publication 9 November 2017
Published 5 December 2017 Volume 2017:9 Pages 751—759
DOI https://doi.org/10.2147/CMAR.S151331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Victor C Kok1,2
1Division of Medical Oncology, Cancer Center, Kuang Tien General Hospital, 2Asia University, Taichung, Taiwan
Background: Unprovoked (idiopathic) venous thromboembolism (VTE) with no obvious antecedent risk factors, is associated with a significant risk of subsequent occult cancer. Conversely, there is a heightened risk of VTE in cancer patients. This bidirectional risk can be estimated from population-based cohort studies conducted in East Asians.
Methods: A literature search using medical subject heading terms and Boolean logic in PubMed and MedLine was performed in April 2017. Twenty-two papers reported from East Asia were retrieved for study and data synthesis. Proportional meta-analysis with a random-effects model was used to synthesize data with 95% confidence intervals (CIs) when appropriate.
Results: Synthesis of data on VTE incidence in the East Asian population (I2 = 76.2%) showed that pooled incidence was 20.3 (95% CI, 11.2–32) per 100,000 person-years. VTE incidence steadily increased with age. Unprovoked VTE accounted for 35% (95% CI, 24%–48%) of all cases of incident VTE (I2 = 99.7%). The overall cancer risk was significantly higher (2.3-fold) in the VTE cohort than in comparators. Among the patients with unprovoked VTE, approximately 7% had a subsequent cancer diagnosis within 2 years of the first episode of idiopathic VTE. The risk of VTE recurrence was increased in cancer patients (adjusted odds ratio, 1.64; 95% CI, 1.26–1.99). VTE incidence was 9.9 per 1,000 person-years in cancer patients, particularly in liver, pancreas, and lung cancer patients.
Conclusion: Newly diagnosed VTE incidence is estimated at approximately 4,400 new cases annually in Taiwan and 7,100 in South Korea. Similar to the trend in VTE incidence among the general population, VTE risk in East Asian cancer patients is markedly lessened.
Keywords: venous thromboembolism, cancer, East Asian, bidirectional relationship, epidemiological study
Introduction
Venous thrombosis is defined as a blood clot (thrombus) forming in a vein or in multiple veins. Classically, venous thromboembolism (VTE) incorporates two clinical entities: deep vein thrombosis (DVT) and pulmonary embolism. The causes of VTE can be categorized into two groups of hypercoagulable states (also referred to as thrombophilia): hereditary or acquired, according to its etiology. In the clinical settings, it is more useful to categorize VTE into idiopathic (a term equivalent to unprovoked) and provoked types. In provoked VTE, there is an obvious precedent risk factor for thrombosis. Patients with unprovoked VTE, who are subsequently diagnosed with a malignancy usually within a year of follow-up, are retrospectively regarded as having overt cancer-associated VTE. Although unprovoked VTE is a diagnosis made at the initial presentation of venous thrombosis when no obvious etiology is discovered, in the real world, any unprovoked VTE that precedes a malignancy can be retrospectively categorized as an overt cancer-associated type, regardless of the length of the follow-up interval.
The causes of inherited thrombophilia, which is a lifelong genetic predisposition to thrombosis, are markedly different between the Western and the Asian patients. In a small study of 50 Taiwanese adult patients with sonogram-proved VTE, protein S deficiency was the most common cause of hereditary VTE.1 The most common causes of hereditary VTE in Western countries are factor V Leiden (FVL; FV R506Q), which is associated with activated protein C resistance, and factor II G20210A polymorphism, both of which are extremely rare in Asian populations.2
Provoked-type VTE can result from an obvious preceding event, such as surgery (particularly orthopedic surgery), endoscopic submucosal dissection for superficial gastric neoplasm,3 trauma, pregnancy, presence of an indwelling central venous catheter, immobilization, or neoadjuvant (preoperative) chemotherapy.4–8 It is noteworthy that several VTE patients have more than one provoking risk factor; a clear example would be immobilization after orthopedic surgery with an indwelling central venous catheter.9–14 Idiopathic or unprovoked VTE is the focus of this study. This is mainly because clinicians should maintain a high index of suspicion of occult cancer, practically defined in epidemiologic studies as cancer developing within 1 year after the diagnosis of unexplained VTE, which is the underlying etiology.
VTE has been considered rarer in East Asian populations than in Caucasians.14–19 White et al20 utilized the California Discharge Data Set to identify a cohort of incident VTE patients in 1996. After adjusting for the misclassification of race, investigators calculated VTE incidence to be highest in African-Americans, with 141 per 100,000, followed by 104 per 100,000 in Caucasians; 55 per 100,000 in Hispanics; and 21 per 100,000 in Asian/Pacific Islanders. Idiopathic VTE incidence was significantly lower among both Hispanics and Asian/Pacific Islanders than among Caucasians or African-Americans (p < 0.001).21
Several epidemiologic studies of VTE have been conducted in the past decade in East Asian patients.16–18 An evidence-based analytic approach with data synthesis is required to improve our knowledge of issues related to the bidirectional relationship regarding incidence rate (IR) or risks such as relative risk (RR) or hazard ratio (HR) from VTE to cancer development and from cancer diagnosis to an episode of VTE in East Asian patients.
Materials and methods
Ethical statement
This study is an expert review of the current published epidemiologic studies on the bidirectional relationship between VTE and cancer, and thus was classified as research exempt from review by the institutional review board of the Kuang Tien General Hospital.
Literature search
Peer-reviewed clinical reports in the English language indexed in PubMed were included. Two explicit statements of questions being addressed with reference to participants, interventions, comparisons, outcomes, type of question, and study design were established as follows:22 the first explicit foreground question of cancer risk from an episode of VTE: patients (P), adult East Asian patients; exposure (E), patients who developed VTE; comparison (C), comparators without VTE; outcomes (O), risk of cancer development (IR, RR, or HR); type of question (T), prognosis-type question; and study design (S), population-based longitudinal studies. The second question of risk of VTE development from cancer was as follows: P, adult East Asian patients; E, patients who have cancer; C, comparators without cancer; O, risk of VTE development (IR, RR, or HR); T, prognosis-type question; and S, population-based longitudinal studies.
A comprehensive literature search strategy was established with the following details to search the PubMed literature database using medical subject headings (MeSHs) and qualified Boolean search terms: “Venous Thrombosis”[MeSH] AND “Neoplasms”[MeSH] AND “Taiwan”[MeSH] OR “Taiwan”[All Fields], the results revealed 50 articles, of which three qualified articles were selected; “Venous Thrombosis”[MeSH] AND (population-based[All Fields] AND study[All Fields]) OR cohort[All Fields]) AND (“Taiwan”[MeSH] OR “Taiwan”[All Fields]), the results revealed 41 articles, but none were selected; and (“Venous Thromboembolism”[MeSH] OR (“Venous”[All Fields] AND “Thromboembolism”[All Fields]) OR “Venous Thromboembolism”[All Fields]) AND (“Taiwan”[MeSH] OR “Taiwan”[All Fields]), the results revealed 97 articles, of which nine were qualified to be reviewed. Using a similar search strategy, the search terms were then extended from Taiwan to Korea, Japan, China, and finally to East Asia. Similar literature search strategy with no regard to countries or geographical regions was employed for selecting the comparator studies conducted in non-Asian or mixed populations.
Statistical analysis
Proportional meta-analysis was performed to derive a pooled proportion of the development of incident cancer in VTE patients. The method adopted was Stuart-Ord (inverse double arcsine square root).23 Noncombinability of studies was examined with the decision to choose either fixed or random effects based upon I2.24 We used the StatsDirect software (http://www.statsdirect.com, England: StatsDirect Ltd., 2017) to perform all pooled meta-analyses.
Results and discussion
Estimation of VTE incidence in the East Asian population
VTE incidence of any etiology is much less in the East Asian population than in Caucasians.
Combining the data for VTE incidence from Taiwanese, Korean, and Hong Kong Chinese studies16–18 using proportional meta-analysis with the random-effects model (because I2 = 76.2%) showed that the pooled proportion was 20.3 (95% CI, 11.2–32) per 100,000 person-years (Figure 1).25 This pooled East Asian IR estimation is approximately one-tenth to one-sixth of that in the community-based Framingham Heart Study, which is 203 (95% CI, 179–226) per 100,000 person-years. Comparing the present current East Asian estimation with the result of another relevant epidemiological study conducted in Auckland, New Zealand, in an ethnically diverse population, the age-adjusted annual rate of VTE per 100,000 person-years in all Asian populations (including India, and South East Asia) in New Zealand was estimated at 25.3, which is within the 95% CI of the results of the current study.26 In the Auckland study, people of European descent had a fourfold increased risk of VTE (RR = 4.02; 95% CI, 3.34–4.84) compared with those of Asian descent.26
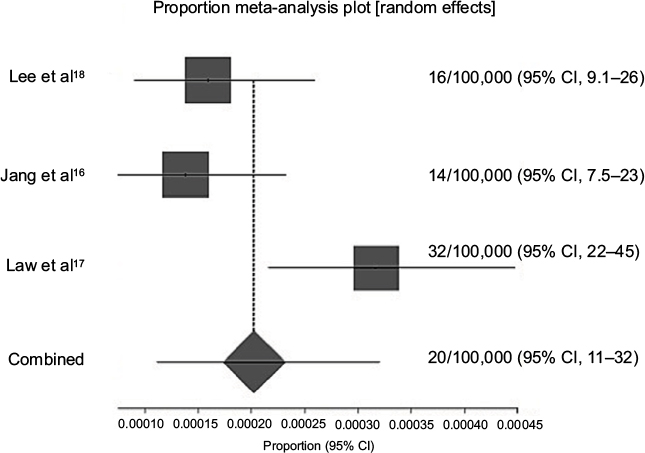 | Figure 1 Proportional meta-analysis synthesizing the IR of VTE in three East Asian studies to derive a combined result. Note: A random-effects model was used with I2 = 76.2%. Abbreviations: CI, confidence interval; IR, incidence rate; VTE, venous thromboembolism. |
A retrospective population-based study in Taiwan by Lee et al18 has shown that in women VTE incidence per 100,000 person-years markedly increased from 2.0 events in those aged <30 years to 118.2 in those aged >80 years; similarly, in men, the incidence increased from 3.0 events in those aged <30 years to 83.1 in those aged >80 years. The recurrence rate of VTE is estimated at 5.1% per person-year.18
Newly diagnosed VTE incidence is estimated at approximately 4,400 new cases each year in Taiwan and 7,100 (13.8 per 100,000 per annum times a population of 51.25 million) in South Korea. The crude incidence of VTE in Taiwanese patients steadily increases with age, ranging from 4 per 100,000 in patients aged <40 years to 108 in those aged ≥80 years.18
Table 1 compares estimated IRs of overall and unprovoked VTE in the general population in five Asia–Pacific (including four East Asian) and two Western countries. Unprovoked (idiopathic) VTE accounts for approximately 34% (95% CI, 19.8%–50.6%; random-effects model using DerSimonian–Laird methods) of all cases of VTE in East Asia.14,18,19 These are synthetic data constructed after the author performed a proportional meta-analysis using a random-effects model after pooling three relevant studies.
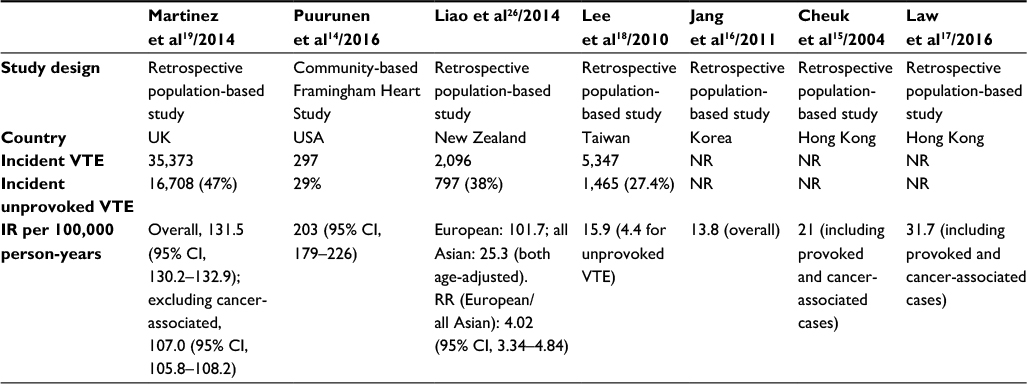 | Table 1 Estimated IR of overall and unprovoked VTE in the general population compared between five Asia-Pacific and two Western studies Abbreviations: CI, confidence interval; IR, incidence rate; NR, not reported; RR, relative risk; VTE, venous thromboembolism. |
To calculate the proportion of unprovoked VTE among the entire cohort of patients with VTE, it is appropriate to combine data from four studies.14,18,19,26 A proportional meta-analysis with a random-effects model under an I2 of 99.8% derived a pooled proportion of 35% with a 95% CI of 24%–48% (Table 1, Figure 2).
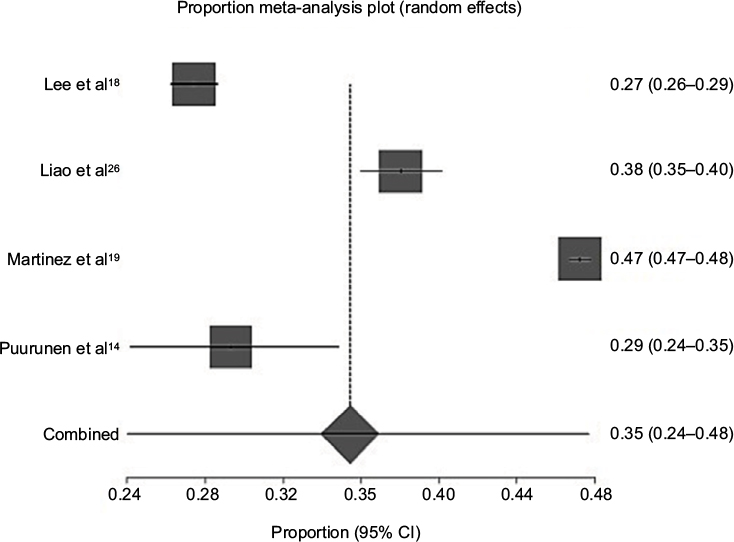 | Figure 2 Meta-analysis of the proportion of unprovoked VTE pooling four relevant epidemiologic studies with a random-effects model with I2 = 99.7% gives a pooled proportion of 35% (95% CI, 24%–48%). Abbreviations: CI, confidence interval; VTE, venous thromboembolism. |
There is an interesting observation that there is seasonal variation in VTE occurrence among Korean patients, regardless of whether it is unprovoked or non-cancer associated. Jang et al27 have reported in their series of 1,495 VTE patients that VTE incidence peaked in December and was the lowest in July (χ2 = 11.83, p = 0.008). This difference in VTE incidence between winter and summer in East Asia provides a new perspective on VTE prevention strategy, particularly in regions where seasons can bring sharp changes in the ambient temperature. Winter is associated with a decreased mobility.
Risk of occult cancer in East Asian patients with unprovoked VTE
A prospective trial conducted in Canada (854 patients with unprovoked VTE) provided reliable data on the incidence of occult cancer during a 1-year follow-up period, which was 3.9 per 100 patient-years.28 The Tromso survey of 733 Norwegians found that the incidence of occult cancer after VTE was 5.5 per 100 patient-years during a 1-year follow-up.29 The IR of cancer in Taiwanese patients with unprovoked VTE was estimated at 2.2–4.5 per 100 patient-years (Table 2).10,30
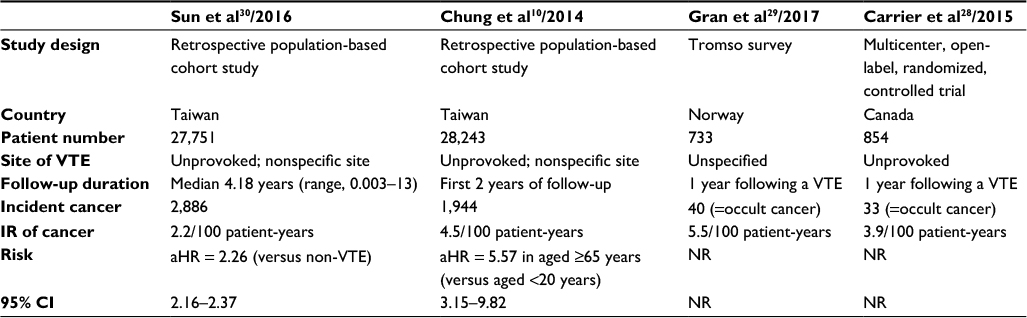 | Table 2 Epidemiologic studies showing the incidence of cancer in patients with VTE Note: In contrast, Carrier et al’s28 prospective clinical trial data are also extracted for direct comparison. Abbreviations: aHR, adjusted hazard ratio; CI, confidence interval; IR, incidence rate; NR, not reported; VTE, venous thromboembolism. |
Population-based observation studies sometimes come up with interesting study results. In a population-based study with 2-year follow-up conducted in Taiwan, the study results imply that the risk of occult cancer is higher in older patients with VTE than young patients. Compared with patients aged below 40 years, those aged ≥65 years with unprovoked VTE had a nearly sixfold increased risk of subsequent cancer development.10 Among patients with unprovoked VTE, 7% of them would receive a diagnosis of cancer within 2 years after the first idiopathic VTE episode. The three most common cancers after unprovoked VTE in Taiwanese patients were lung, liver, and colorectal cancers, with rates of 18.3%, 12.3%, and 10.9%, respectively.30
Risk of VTE in East Asian patients with all-site malignancy and by specific site
Cancer induces a hypercoagulable state.12 The risk of cancer-associated thrombosis is determined by patient-related factors, such as the state of hypercoagulability; medical comorbidities; ambulation; prior personal history of venous thrombosis; tumor-related factors, such as cancer type, early versus advanced stage, extent of disease, and tumor grade; cancer-derived circulating tissue factor-containing microvesicles;31,32 and treatment-emergent causes, including surgery, chemotherapy, antiangiogenic agent use, and hormonal treatment. The discussion of cancer-associated procoagulants, such as tissue factors that are present in blood or tissue, is beyond the scope of this study. According to their tendency to develop venous thrombosis, cancers can be categorized as having high, medium, or low thrombotic risk. Cancers originating in the chest and abdomen are particularly associated with high absolute rates of VTE.33
A retrospective population-based study of 83,203 cancer patients at unspecified sites found an IR of VTE of 13.9 per 1,000 patient-years (95% CI, 13.4–14.4), representing an adjusted HR of 4.7 (95% CI, 4.5–4.9), compared with patients without cancer.33 The risk of VTE in cancer patients is markedly decreased in East Asians; two recent Taiwanese studies found IRs of 1.9 and 3.4 per 1,000 person-years (Table 3).9,34
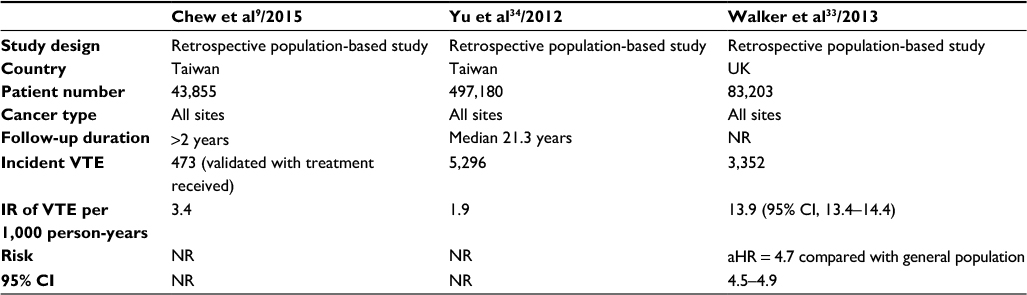 | Table 3 Epidemiologic studies showing the incidence of VTE in patients with cancer Abbreviations: aHR, adjusted hazard ratio; CI, confidence interval; IR, incidence rate; NR, not reported; VTE, venous thromboembolism. |
Table 4 shows VTE incidence in East Asian patients with various types of cancer reported in epidemiologic studies published after 2010. The risk is commonly represented as the cumulative IR (CIR) of VTE. Yokoyama et al35 have reported a CIR of 11% in a single-institution observational study of patients with newly diagnosed diffuse large B-cell lymphoma. Lee et al36 have reported a 2-year CIR of 9.2% in Korean patients with pancreatic adenocarcinoma. A prospective cohort study of patients with newly diagnosed lymphoma across Asia found a 1-year actuarial incidence of 7.9%.37 Lee et al38 have found a 2-year CIR of 6.6% in a single-institution observational study of Korean patients with non-small-cell lung cancer. A retrospective population-based cohort study conducted in 1,013 Taiwanese patients with uterine cervix cancer found a 5-year CIR of 3.3%.39 Ye et al,40 in a single-institution observational study of gynecological cancer patients in China, have reported a 10-year CIR of 2% for the entire cohort, 3.7% for vulvar cancer, and 2.5% for ovarian cancer. Kang et al,41 in a single-institution study of inoperable gastric cancer patients in Korea, have found a 1-year CIR of 3.5%.
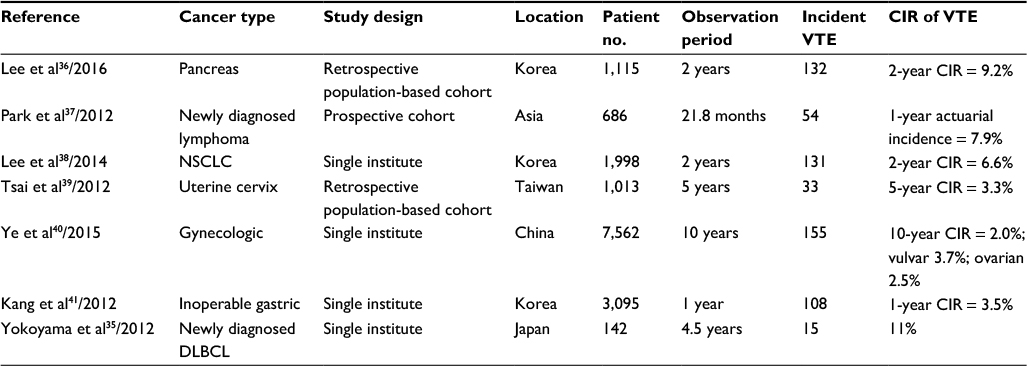 | Table 4 Epidemiologic studies published after 2010 showing the incidence of VTE in East Asian patients with various types of cancer Abbreviations: CIR, cumulative incidence rate; DLBCL, diffuse large B-cell lymphoma; NSCLC, non-small-cell lung cancer; VTE, venous thromboembolism. |
To determine whether there is a similar pattern in the occurrence of VTE in specific cancer types that are more common in the Asian population, it will be worthwhile for this study to perform a head-to-head comparison of studies between East Asian and Western countries using esophageal cancer and the stomach cancer as examples (Table 5). The incidence of VTE in East Asian patients with esophageal cancer is quite similar to those reported in the Western countries.4,5,7,42 However, in stomach cancer, the risk of VTE is lower in East Asians with advanced cancer.41,43,44 For advanced stomach cancer, the 1-year cumulative incidence is 9% in the American patients as reported by Fuentes et al.45 A Denmark study demonstrates that perioperative chemotherapy administered in the group of patients with gastric cancer will raise the incidence of VTE to 37%.7 In contrast, a South Korean prospective database research shows that the 2-year cumulative incidence in patients with metastatic stage IV gastric cancer is 24.4%.44 Another Japanese study on advanced-stage gastric cancer treated with palliative chemotherapy reveals that the 1-year cumulative incidence of VTE is 13.6%, much lower than those reported in Western countries.43 The difference in the occurrence pattern may be site specific or resulted from different working definitions of VTE adopted in different studies.
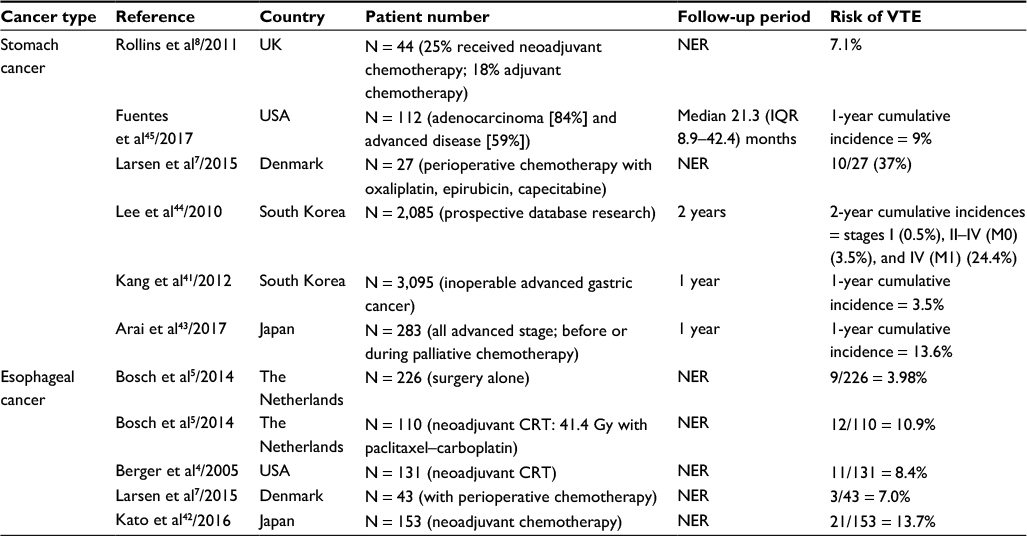 | Table 5 Head-to-head comparison of studies conducted in the East Asian or Western countries on the risk of VTE in gastric and esophageal cancers which are more common in the Asian population Abbreviations: CRT, chemoradiotherapy; IQR, interquartile range; M0, no distant metastasis; M1, at least one distant metastasis; NER, not explicitly reported; VTE, venous thromboembolism. |
Upper extremity DVT, although much less common, is more related to malignancy and thrombophilia than is lower extremity DVT. In a population-based thrombophilia study involving a total of 1,203 VTE patients in Malmö, Sweden, 63 (5.2%) had upper extremity DVT.46 At diagnosis, 30% of the patients with upper extremity DVT had active malignancy, and thrombophilia accounted for 29% of the patients with upper extremity VTE. Among the patients with thrombophilia, 66% were heterozygous and 17% were homozygous for the FVL mutation, 10% were heterozygous for the prothrombin mutation, and 6% were both heterozygous for the FVL mutation and had lupus anticoagulant antibodies.46
A brief discussion on thrombophilia is warranted to understand the scope of the problems. An earlier Japanese study reported that 8 (2%) of 392 otherwise healthy subjects had protein S deficiency and two (0.5%) had protein C deficiency.47 Compared with the Japanese results, Zhu et al2 have reported much lower frequencies of genetic deficiency in the three main natural anticoagulants – antithrombin, protein C, and protein S – which are rare in Western countries but are important risk factors for VTE in Asian countries. This cross-sectional survey aiming to establish sex- and age-related normal ranges for activity levels of the three main natural anticoagulants in 3,493 healthy Han Chinese patients found that 15 (4.3 per 1,000) harbored a genetic variant detected by direct sequencing.2
Conclusion
Recent population-based cohort studies conducted in East Asia have provided an opportunity for us to understand the bidirectional relationship of VTE and cancer in the region. The IR of VTE of any etiology in East Asians is much less than in Caucasians. Combining the data for VTE incidence in the general population from Taiwanese, Korean, and Hong Kong Chinese studies using proportional meta-analysis revealed that the pooled proportion was 20.3 (95% CI, 11.2–32) per 100,000 person-years. Newly diagnosed VTE incidence is estimated at least 4,400 new cases each year in Taiwan and 7,100 in South Korea, because it is hard to pick up cases of silent VTE in retrospective cohort studies. Unprovoked VTE accounts for approximately 34% (95% CI, 19.8%–50.6%) of all cases of VTE in East Asia. The IR of cancer in Taiwanese patients with unprovoked VTE was estimated at 2.2–4.5 per 100 patient-years. Similar to the trend in general population, the risk of VTE in cancer patients is markedly lessened in East Asians than in Caucasians, with an IR of 1.9–3.4 per 1,000 person-years in the region.
The implications of the findings reported in this paper are as follows: knowledge translation can be realized by extracting published results from relevant epidemiological research. Second, robust estimation derived from the statistical synthesis gives a clearer picture of the bidirectional risk of VTE and cancer in East Asia. Last but not least, future research can be more efficient via deepening the regional collaboration to establish an international prospective data collection.
Disclosure
The author reports no conflicts of interest in this work.
References
Ho CH, Chau WK, Hsu HC, Gau JP, Yu TJ. Causes of venous thrombosis in fifty Chinese patients. Am J Hematol. 2000;63(2):74–78. | ||
Zhu T, Ding Q, Bai X, et al. Normal ranges and genetic variants of antithrombin, protein C and protein S in the general Chinese population. Results of the Chinese Hemostasis Investigation on Natural Anticoagulants Study I Group. Haematologica. 2011;96(7):1033–1040. | ||
Kusunoki M, Miyake K, Shindo T, et al. The incidence of deep vein thrombosis in Japanese patients undergoing endoscopic submucosal dissection. Gastrointest Endosc. 2011;74(4):798–804. | ||
Berger AC, Scott WJ, Freedman G, et al. Morbidity and mortality are not increased after induction chemoradiotherapy followed by esophagectomy in patients with esophageal cancer. Semin Oncol. 2005;32(6 suppl 9):S16–S20. | ||
Bosch DJ, Van Dalfsen QA, Mul VE, Hospers GA, Plukker JT. Increased risk of thromboembolism in esophageal cancer patients treated with neoadjuvant chemoradiotherapy. Am J Surg. 2014;208(2):215–221. | ||
Kimura Y, Oki E, Ando K, Saeki H, Kusumoto T, Maehara Y. Incidence of venous thromboembolism following laparoscopic surgery for gastrointestinal cancer: a single-center, prospective cohort study. World J Surg. 2016;40:309–314. | ||
Larsen AC, Frokjaer JB, Fisker RV, et al. Treatment-related frequency of venous thrombosis in lower esophageal, gastro-esophageal and gastric cancer – a clinical prospective study of outcome and prognostic factors. Thromb Res. 2015;135(5):802–808. | ||
Rollins KE, Peters CJ, Safranek PM, Ford H, Baglin TP, Hardwick RH. Venous thromboembolism in oesophago-gastric carcinoma: incidence of symptomatic and asymptomatic events following chemotherapy and surgery. Eur J Surg Oncol. 2011;37(12):1072–1077. | ||
Chew TW, Gau CS, Wen YW, Shen LJ, Mullins CD, Hsiao FY. Epidemiology, clinical profile and treatment patterns of venous thromboembolism in cancer patients in Taiwan: a population-based study. BMC Cancer. 2015;15:298. | ||
Chung WS, Lin CL, Hsu WH, Sung FC, Li RY, Kao CH. Idiopathic venous thromboembolism: a potential surrogate for occult cancer. QJM. 2014;107(7):529–536. | ||
Heit JA, Spencer FA, White RH. The epidemiology of venous thromboembolism. J Thromb Thrombolysis. 2016;41:3–14. | ||
Ikushima S, Ono R, Fukuda K, Sakayori M, Awano N, Kondo K. Trousseau’s syndrome: cancer-associated thrombosis. Jpn J Clin Oncol. 2016;46(3):204–208. | ||
Liew NC, Alemany GV, Angchaisuksiri P, et al. Asian venous thromboembolism guidelines: updated recommendations for the prevention of venous thromboembolism. Int Angiol. 2017;36(1):1–20. | ||
Puurunen MK, Gona PN, Larson MG, Murabito JM, Magnani JW, O’Donnell CJ. Epidemiology of venous thromboembolism in the Framingham Heart Study. Thromb Res. 2016;145:27–33. | ||
Cheuk BL, Cheung GC, Cheng SW. Epidemiology of venous thromboembolism in a Chinese population. Br J Surg. 2004;91(4):424–428. | ||
Jang MJ, Bang SM, Oh D. Incidence of venous thromboembolism in Korea: from the Health Insurance Review and Assessment Service database. J Thromb Haemost. 2011;9(12):85–91. | ||
Law Y, Chan YC, Cheng SW. Epidemiological updates of venous thromboembolism in a Chinese population. Asian J Surg. Epub 2016 Dec 21. | ||
Lee CH, Lin LJ, Cheng CL, Kao Yang YH, Chen JY, Tsai LM. Incidence and cumulative recurrence rates of venous thromboembolism in the Taiwanese population. J Thromb Haemost. 2010;8(7):1515–1523. | ||
Martinez C, Cohen AT, Bamber L, Rietbrock S. Epidemiology of first and recurrent venous thromboembolism: a population-based cohort study in patients without active cancer. Thromb Haemost. 2014;112:255–263. | ||
White RH, Zhou H, Murin S, Harvey D. Effect of ethnicity and gender on the incidence of venous thromboembolism in a diverse population in California in 1996. Thromb Haemost. 2005;93(2):298–305. | ||
White RH, Keenan CR. Effects of race and ethnicity on the incidence of venous thromboembolism. Thromb Res. 2009;123(suppl 4): S11–S17. | ||
Kok VC, Kuo JT. Pazopanib as a second-line treatment for non-cytokine-treated metastatic renal cell carcinoma: a meta-analysis of the effect of treatment. BMC Urol. 2016;16:34. | ||
Stuart A, Ord K. Kendall’s Advanced Theory of Statistics: Distribution Theory. 6th ed. London: Edward Arnold; 1994. | ||
Nikolakopoulou A, Mavridis D, Salanti G. Demystifying fixed and random effects meta-analysis. Evid Based Ment Health. 2014;17(2):53–57. | ||
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558. | ||
Liao S, Woulfe T, Hyder S, Merriman E, Simpson D, Chunilal S. Incidence of venous thromboembolism in different ethnic groups: a regional direct comparison study. J Thromb Haemost. 2014;12:214–219. | ||
Jang MJ, Kim HJ, Bang SM, et al. Seasonal variation in the occurrence of venous thromboembolism: a report from the Korean Venous Thromboembolism Working Party. Thromb Res. 2012;130(4):e199–e202. | ||
Carrier M, Lazo-Langner A, Shivakumar S, et al. Screening for occult cancer in unprovoked venous thromboembolism. N Engl J Med. 2015;373(8):697–704. | ||
Gran OV, Braekkan SK, Paulsen B, Skille H, Rosendaal FR, Hansen JB. Occult cancer-related first venous thromboembolism is associated with an increased risk of recurrent venous thromboembolism. J Thromb Haemost. 2017;15(7):1361–1367. | ||
Sun LM, Chung WS, Lin CL, Liang JA, Kao CH. Unprovoked venous thromboembolism and subsequent cancer risk: a population-based cohort study. J Thromb Haemost. 2016;14:495–503. | ||
Bang OY, Chung JW, Lee MJ, et al. Cancer cell-derived extracellular vesicles are associated with coagulopathy causing ischemic stroke via tissue factor-independent way: the OASIS-CANCER study. PLoS One. 2016;11(7):e0159170. | ||
Ettelaie C, Collier ME, Featherby S, Benelhaj NE, Greenman J, Maraveyas A. Analysis of the potential of cancer cell lines to release tissue factor-containing microvesicles: correlation with tissue factor and PAR2 expression. Thromb J. 2016;14:2. | ||
Walker AJ, Card TR, West J, Crooks C, Grainge MJ. Incidence of venous thromboembolism in patients with cancer – a cohort study using linked United Kingdom databases. Eur J Cancer. 2013;49(6):1404–1413. | ||
Yu YB, Gau JP, Liu CY, et al. A nation-wide analysis of venous thromboembolism in 497,180 cancer patients with the development and validation of a risk-stratification scoring system. Thromb Haemost. 2012;108(2):225–235. | ||
Yokoyama K, Murata M, Ikeda Y, Okamoto S. Incidence and risk factors for developing venous thromboembolism in Japanese with diffuse large b-cell lymphoma. Thromb Res. 2012;130(1):7–11. | ||
Lee JC, Ro YS, Cho J, et al. Characteristics of venous thromboembolism in pancreatic adenocarcinoma in East Asian Ethnics: a large population-based observational study. Medicine. 2016;95(17):e3472. | ||
Park LC, Woo SY, Kim S, et al. Incidence, risk factors and clinical features of venous thromboembolism in newly diagnosed lymphoma patients: results from a prospective cohort study with Asian population. Thromb Res. 2012;130(3):e6–e12. | ||
Lee YG, Kim I, Lee E, et al. Risk factors and prognostic impact of venous thromboembolism in Asian patients with non-small cell lung cancer. Thromb Haemost. 2014;111:1112–1120. | ||
Tsai SJ, Ruan YX, Lee CC, et al. The incidence of venous thromboembolism in cervical cancer: a nationwide population-based study. BMC Res Notes. 2012;5:316. | ||
Ye S, Zhang W, Yang J, et al. Pattern of venous thromboembolism occurrence in gynecologic malignancy: incidence, timing, and distribution a 10-year retrospective single-institutional study. Medicine. 2015;94:e2316. | ||
Kang MJ, Ryoo BY, Ryu MH, et al. Venous thromboembolism (VTE) in patients with advanced gastric cancer: an Asian experience. Eur J Cancer. 2012;48(4):492–500. | ||
Kato F, Takeuchi H, Matsuda S, Kawakubo H, Omori T, Kitagawa Y. Incidence of and risk factors for venous thromboembolism during surgical treatment for esophageal cancer: a single-institution study. Surg Today. 2016;46(4):445–452. | ||
Arai H, Hironaka S, Minashi K, Denda T, Shimokawa M, Yamaguchi T. Cumulative incidence, risk factors and prognostic impact of venous thromboembolism in Japanese patients with advanced gastric cancer. Jpn J Clin Oncol. 2017;47(10):942–948. | ||
Lee KW, Bang SM, Kim S, et al. The incidence, risk factors and prognostic implications of venous thromboembolism in patients with gastric cancer. J Thromb Haemost. 2010;8(3):540–547. | ||
Fuentes HE, Oramas DM, Paz LH, Wang Y, Andrade XA, Tafur AJ. Venous thromboembolism is an independent predictor of mortality among patients with gastric cancer. J Gastrointest Cancer. Epub 2017 Jun 21. | ||
Isma N, Svensson PJ, Gottsater A, Lindblad B. Upper extremity deep venous thrombosis in the population-based Malmo thrombophilia study (MATS). Epidemiology, risk factors, recurrence risk, and mortality. Thromb Res. 2010;125(6):e335–e338. | ||
Suehisa E, Nomura T, Kawasaki T, Kanakura Y. Frequency of natural coagulation inhibitor (antithrombin III, protein C and protein S) deficiencies in Japanese patients with spontaneous deep vein thrombosis. Blood Coagul Fibrinolysis. 2001;12(2):95–99. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.