")
Back to Journals » Patient Preference and Adherence » Volume 10
Better health-related quality of life (mental component summary), having a higher level of education, and being less than 75 years of age are predictors of hospital admission among cognitively intact nursing home residents: a 5-year follow-up study
Authors Drageset J, Eide GE, Ranhoff A
Received 10 July 2015
Accepted for publication 9 January 2016
Published 7 March 2016 Volume 2016:10 Pages 275—282
DOI https://doi.org/10.2147/PPA.S92135
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Jorunn Drageset,1,2 Geir Egil Eide,3,4 Anette Hylen Ranhoff5,6
1Department of Nursing, Faculty for Health and Social Science, Bergen University College, Bergen, Norway; 2Department of Public Health and Primary Care, University of Bergen, Bergen, Norway; 3Centre for Clinical Research, Western Norway Health Region Authority, Bergen, Norway; 4Research Group for Lifestyle Epidemiology, Department of Public Health and Primary Care, University of Bergen, Bergen, Norway; 5Kavli Research Centre for Ageing and Dementia, Haraldsplass Hospital, Bergen, Norway; 6Department of Clinical Science, University of Bergen, Bergen, Norway
Objective: To study whether health-related quality of life (HRQOL), activities of daily living (ADL), and anxiety and depression symptoms affect the risk of hospital admission and potential interactions with having a cancer diagnosis.
Methods: This study was a prospective observational study with 5-year follow-up and analyzed the follow-up data on hospital admissions until 2010 using baseline data from 227 cognitively intact nursing home (NH) residents (60 of whom had cancer) in 2004–2005. Data on HRQOL were collected by using the Short Form-36 Health Survey, divided into physical component summary (PCS) and mental component summary (MCS), and symptoms of anxiety and depression were collected by using the Hospital Anxiety and Depression Scale (HADS). ADL were obtained from registered observation and sociodemographic variables, diagnoses, and hospital admissions from the NH records. Personal identification numbers were linked to the record systems of the hospitals, thereby registering all hospital admissions. We analyzed the time elapsing between inclusion and the first hospital admission.
Results: Residents with higher HRQOL (MCS) had significantly more hospital admissions after adjustment for age, sex, marital status, education, and comorbidity. HRQOL (PCS), ADL, depression, and anxiety symptoms were not associated with hospital admissions. Cancer increased the risk after adjustment for all other risk factors but did not increase the effects of MCS, PCS, ADL, or depression or anxiety symptoms. Having a higher level of education and being less than 75 years of age were associated with hospitalization. The residents diagnosed with cancer had the most days in hospital related to diseases of the respiratory system and cancer, and diseases of the circulatory and respiratory systems were more frequent among the residents without a cancer diagnosis.
Conclusion: Better self-reported HRQOL (MCS) was associated with hospital admissions, whereas self-reported HRQOL (PCS), ADL, and depression and anxiety symptoms were not. Cancer increased the risk but not the effects of MCS, PCS, ADL, or depression or anxiety symptoms. Having a higher level of education and being less than 75 years of age were also associated with hospitalization.
Keywords: mental health, cancer, nursing homes, older people, hospital admission
Introduction
Many older people in residential care are hospitalized.1–4 Some hospitalization, such as for hip fractures and major gastrointestinal bleeding, is unavoidable.4
Previous studies on hospital admission of residents from nursing homes (NHs) have predominantly focused on physical and cognitive disability2 and specific diagnoses such as congestive heart failure, infections, and fractures and mental health disorders,2,3,5,6 with varying numbers of days spent in hospital. Health-related quality of life (HRQOL), activities of daily living (ADL), and anxiety and depression symptoms related to hospital admissions among cognitively intact NH residents with cancer have been given less attention.
Background
Most people living in NHs are old, physically impaired, and have short survival time after admission to the NH.7 Furthermore, NH residents are characterized by chronic illnesses, multiple diagnoses,8 and symptoms such as fatigue, pain, appetite loss,7 anxiety, and depression.7,9 Most (80%) of the NH residents in Norway have dementia;10 consequently, the cognitively intact NH residents represent a small group.
Among the NH residents, 10%–26% have been diagnosed with cancer at admission,11,12 and more NH residents will be diagnosed with cancer in the years ahead.13 Symptoms of pain, anorexia, vomiting, nausea, and fatigue are prevalent,14,15 and pain is often untreated.14 NH residents with a diagnosis of cancer are often dependent in ADL, have unstable health,13,16 report more depression and anxiety symptoms than other residents,16 and rated their HRQOL as being lower than those without a diagnosis of cancer.11
NH residents are, therefore, a vulnerable group with complex needs who require advanced care and treatment. If they need more advanced care and treatment than the NH can provide, hospital admission may be necessary.12
Few studies have examined the association between self-reported HRQOL, ADL, symptoms of anxiety and depression, and hospital admission among NH residents.2,17–19 A systematic review17 in which one study explicitly focused on ADL limitation reported that African–American NH residents with more ADL limitation were more likely to be hospitalized in the last 90 days of life compared to white NH residents. Miu and Chan19 found that depressive symptoms were associated with hospital admission among community-dwelling older people, and Becker et al17 found that serious mental disorder was associated with hospital admission among NH residents. In adults with diabetes who had been admitted to hospital, Li et al20 found significantly poorer mean scores on each of the physical dimensions of the physical component summary (PCS) of the Short Form-36 Health Survey (SF-36) at baseline.
ADL and symptoms of anxiety and depression may worsen over time and interact with HRQOL. Accordingly, one can question whether ADL, anxiety, depression, and HRQOL might be contributing factors to hospitalization. Although there is evidence related to hospital admission among NH residents, associations between HRQOL, ADL, anxiety and depression, and hospital admission among cognitively intact NH residents have been poorly studied. Promoting HRQOL is a recognized objective for older people21 that is fundamental in nursing and a crucial nursing concern in long-term care.7,22 Enabling NH residents to maintain HRQOL is therefore vital.
Based on our literature review,2,17–19 we hypothesized that HRQOL, ADL, and anxiety and depression symptoms are correlated with the rate of hospital admissions among cognitively intact NH residents with and without a diagnosis of cancer.
The specific aims of the study were as follows:
- To investigate whether self-reported mental and physical health, ADL, and anxiety and depression symptoms are correlated with the rate of hospital admissions among NH residents who are cognitively intact, and whether a diagnosis of cancer may influence the effects of these variables adjusted for age, sex, marital status, education, and comorbidity.
- To describe the hospital stay according to the diagnosis at discharge, number of admissions, and the total number of days spent in hospital during the follow-up period.
Materials and methods
The baseline data were obtained from a prospective cohort study that included NH residents without cognitive impairment in 30 NHs in Bergen, Norway, in 2004–2005 and with follow-up to 2010.1,11 The main study investigated HRQOL among NH residents without cognitive impairment. For the purpose of this study, we collected information about hospital admissions during 5 years after inclusion.
Study setting
Most NHs in Norway are owned and operated by the public sector. Few NHs are privately owned, and municipalities fund them. Local boards determine all admissions to private and public NHs. Further, most NHs offer regular units or special care units for people with dementia, and some have rehabilitation units. The regulations for NHs and living arrangements for 24-hour care and nursing govern the education of the professionals in NHs.23 The education required in NHs is equivalent to registered nurse or state-enrolled nurse (licensed practical nurse). The quality of care of NHs in Norway is regulated by the Municipal Health Act and the Social Services Act24 and by the professional code of ethics for nurses, which complies with the International Council of Nurses guidelines.25 If the legal requirements and norms are met, the NHs have great autonomy in organizing nursing and health care.
Study cohort
The inclusion criteria were as follows: cognitively intact and able to converse, 65 years or older, and had lived in the NH for a minimum of 6 months.
We defined cognitively intact as a score of 0.5 or less on the Clinical Dementia Rating Scale (CDR),26 a widely used clinical tool to grade dementia: severe (3), moderate (2), mild (1), questionable (0.5), and no (0) dementia. A standard algorithm determines the overall level of dementia.26 The scoring is based on trained nurses observing the residents for a minimum of 4 weeks. The CDR shows high inter-rater reliability for doctors and specialized nurses.1,27
A total of 252 of the 2,042 NH residents complied with the criteria for inclusion, and their primary-care nurse invited them to participate. We obtained the data on HRQOL, depression, and anxiety through individual personal interviews taking place in the NH. The principal investigator (JD) recorded the demographic information and interviewed the NH residents, reading the questions aloud and placing a circle around the resident’s answer. We found this necessary, because many residents of NH cannot easily hold a pen and have vision impairment. Each participant was given a large-type version of the questionnaire so that they could see the questions. The interviewer made sure that the respondents understood all questions. Two hundred and twenty seven residents provided informed consent to participate. Of these, 60 (26%) had cancer.
The Norwegian Social Science Data Services and the Western Norway Regional Committee for Medical and Health Research Ethics (REK Vest number 162.03/2009/1550) approved this study.
Data sources
We used NH medical records to identify the 227 respondents. We linked their identification numbers to the records of the hospital to ensure that we captured all hospital admissions (unplanned or planned admissions). We used the hospital’s patient administrative system for information about dates of admission, dates of discharge, diagnoses at discharge, and dates of death in hospital. The primary diagnoses at discharge from hospital were classified in accordance with the tenth revision of the International Classification of Diseases (ICD-10). We classified the diagnoses according to the main ICD-10 chapters. We calculated the length of stay by using the dates of admission and discharge. We confirmed the date of death by linking the National Population Registry and the patient’s journal. We based the residents’ diagnoses on when the resident was discharged, the incidence of hospital admissions, in-hospital mortality, and length of stay on this information.1 All admissions were recorded.
Variables and measurements
Outcome variables
The main outcome was the time elapsed after the person was included in the sample in 2004–2005 until the first time the person was admitted to hospital. For NH residents not admitted to hospital after being included, we recorded the time elapsed before follow-up ended (in 2010). We defined these time periods as being censored admission times. Further, for people who died while residing in the NH before being admitted to hospital for the first time, we recorded how much time elapsed before the resident died and treated this as a censored time of admission.1 Secondary outcomes were diagnosis at discharge, the number of admissions, and the total days spent in hospital during the follow-up period. Residents admitted and discharged on the same day were recorded as having 0 days in hospital.
Exposure variables
Health-related quality of life
We used the SF-36 to measure HRQOL. SF-36 is not specific to age, disease, or treatment and is widely used in health surveys measuring how people function physically and the social and mental aspects of HRQOL.28 The SF-36 has 36 questions (items) in eight dimensions: physical functioning (ten items), role limitation related to physical problems (four items), bodily pain (two items), general health (five items), vitality (four items), social functioning (two items), role limitation related to emotional problems (three items), and mental health (five items). An additional item, reported health transition, measures changes in general health during the past year. The response scores for each dimension are added, giving a score between 0 and 100 (highest).28 Higher scores indicate better HRQOL. The SF-36 has been used in many studies with older people and is reliable and valid.29 The eight dimensions are summarized in two scales: PCS: 0–100 and mental component summary (MCS: 0–100).28 In this study, we used PCS and MCS. The PCS and MCS were derived from the dataset by using the recommended procedures.28
Activities of daily living
We used the Modified Katz Index of Independence in ADL to assess ADL.30 This is based on assessing a person’s functional independence for six nominal variables (dressing, bathing, transferring from bed to chair, going to the toilet, eating, and continence) and focuses on basic or primary ADL functions. The index is based on a person’s actual performance in care situations and is mainly designed for nurses to observe.30 The reliability and scalability (a measure of construct validity) of the Modified Katz Index has been satisfactory in various populations including older people.30 This study used the Modified Katz Index with six nominal variables of ADL.
ADL was scored from 1 (independent) to 3 (fully dependent) on six daily activities (bathing, dressing, going to the toilet, transferring, continence, and eating), and we applied the mean score for the statistical analysis.
Hospital Anxiety and Depression Scale
The Hospital Anxiety and Depression Scale (HADS) has 14 items and subscales for depression (HADS-D, seven items) and anxiety (HADS-A, seven items).31 Each item is scored from 0 to 3. The subscales have a maximum score of 21, and a higher score indicates a higher symptom load. The scores 0–7 are considered normal, scores of 8–10 indicate possible cases of anxiety or depression, and scores exceeding 11 indicate anxiety or depression that requires further investigation and possibly treatment.31 The HADS in a Norwegian version has been validated for use in older people32 and is reliable and valid among NH residents.33 In this study, we used HADS-D and HADS-A sum scores. Cronbach’s alpha was 0.85 for HADS total score, 0.83 for HADS-A, and 0.75 for HADS-D.33
Potential confounders
The demographic variables were sex, age group, educational level, having a cancer diagnosis when included, and marital status. We obtained information about cancer from the records and included all types of active cancer and cancer previously treated.
We used Groll’s Functional Comorbidity Index (FCI) to describe morbidity. The FCI includes 18 disease categories scored as present (score 1) and not present (score 0) and cannot exceed 18.34
The diagnoses in the index correspond with the ICD-10 diagnosis codes except for obesity. The FCI includes physical and mental diagnoses such as osteoporosis and depression. The FCI has been used previously in studies of NH residents.1,22,35
Statistical analysis
We used descriptive statistics (medians, means and standard deviations, proportions, and interquartile ranges) to describe the distribution of the recorded variables. We compared residents with (n=60; 26%) and without cancer (n=167) regarding categorical variables by using the exact chi-square test36 and by using continuous variables with Student’s t-test.37 We analyzed the time elapsed between inclusion in 2004–2005 until the first hospital admission with survival analysis, defining the time to death or the end of follow-up (February 2, 2010) as censored observation times. We used the Kaplan–Meier procedure38,39 to perform unadjusted survival analysis, to compare residents who had cancer with those who did not by using the log-rank test and simple Cox regression analysis.40 Demographic variables (age, sex, and length of NH stay) and specific diagnoses are potentially correlated with hospitalization.2 We, therefore, adjusted for these variables in a backward stepwise Cox regression analysis. We reported the fully adjusted model (first step) and final model (last step) and tested how cancer versus no cancer interact with ADL, HADS-A, HADS-D, MCS, and PCS, respectively.
We chose P≤0.05 as the criterion for statistical significance. We performed the statistical analysis using SPSS (version 21).
Results
Drageset et al1 previously reported the baseline characteristics of the study sample. Of the 60 residents with a cancer diagnosis, 26 (43%) were hospitalized, 30 (50%) died without hospitalization, and four (7%) had no hospitalization and were still alive at the end of follow-up. Of the 167 residents without a cancer diagnosis, 55 (33%) were hospitalized, 88 (53%) died without hospitalization, and 24 (14%) had no hospitalization and were still alive at the end of follow-up. Table 1 presents descriptive statistics for ADL, HADS-A, HADS-D, MCS, and PCS according to cancer at baseline. ADL, HADS-A, and HADS-D had skewed distributions (Shapiro-Wilk’s test of normality P<0.001) with medians (interquartile range) of 2.0 (1.7–2.3), 3.0 (0.3–6.0), 6.0 (3.0–9.0) for residents with cancer and 2.2 (1.7–2.3), 3.0 (1.0–6.0), 6.0 (2.3–8.0) for residents without cancer, respectively.
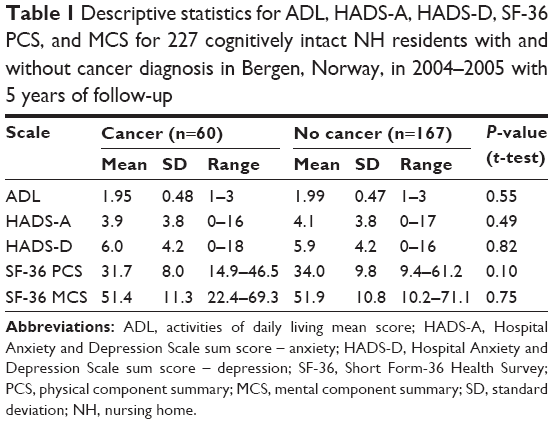 | Table 1 Descriptive statistics for ADL, HADS-A, HADS-D, SF-36 PCS, and MCS for 227 cognitively intact NH residents with and without cancer diagnosis in Bergen, Norway, in 2004–2005 with 5 years of follow-up |
Table 2 gives descriptive statistics for the days in hospital according to diagnosis at discharge from hospital for residents with and without cancer at the interview. Residents admitted and discharged on the same day were recorded as having 0 days in hospital. The residents diagnosed with cancer had the most days in hospital related to diseases of the respiratory system and cancer (mean 4.7 and 4.6, respectively). Days in hospital related to diseases of the circulatory and respiratory systems were most frequent among the residents without a cancer diagnosis (mean 2.2 and 4.8, respectively). The number of days in hospital did not differ significantly between the diagnosis groups (P=0.10).
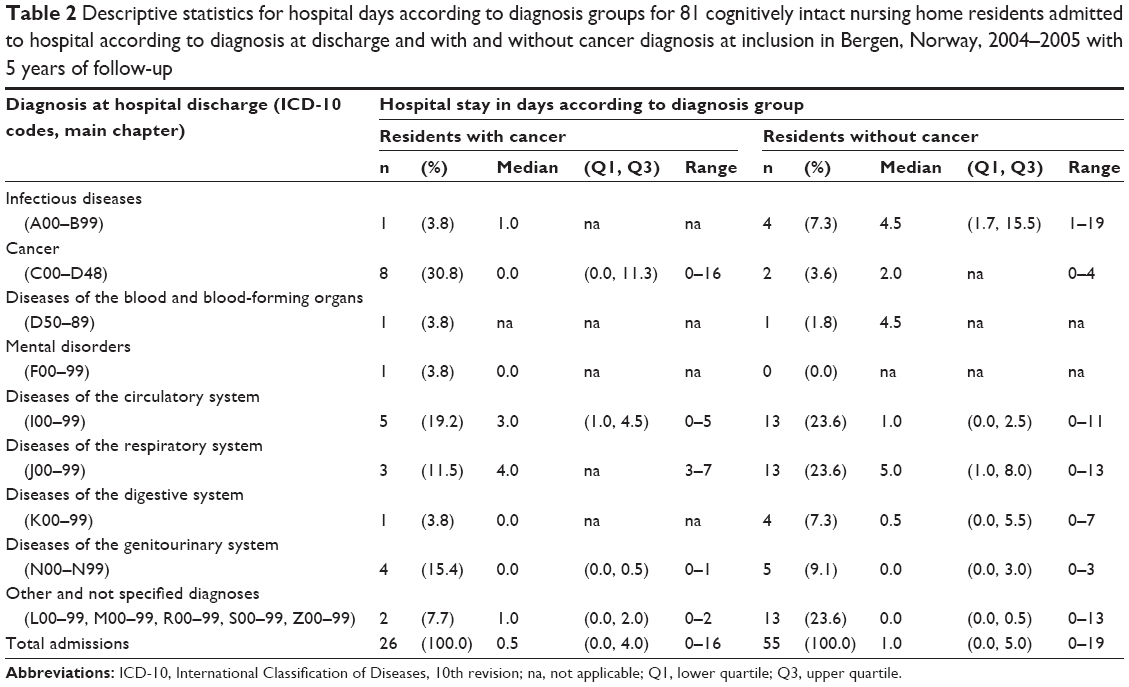 | Table 2 Descriptive statistics for hospital days according to diagnosis groups for 81 cognitively intact nursing home residents admitted to hospital according to diagnosis at discharge and with and without cancer diagnosis at inclusion in Bergen, Norway, 2004–2005 with 5 years of follow-up |
Table 3 shows the results of the Cox proportional hazards regression analysis. Admissions were considerably more frequent among NH residents with cancer than among those without cancer. In the adjusted analysis, independent of cancer, residents with the most education and those 65–74 years old had more hospital admissions. MCS was statistically significant only in the final model. After adjusting for age, education, and MCS, residents who had cancer at inclusion had 1.9 times more hospital admissions than did residents without cancer (P=0.01). Cancer did not interact with the MCS (P=0.52), PCS (P=0.57), ADL (P=0.78), HADS-A (P=0.16), or HADS-D (P=0.83). Symptoms of anxiety and depression and ADL were not significantly associated with hospital admission. The significant hazard ratios in the fully adjusted model remained essentially the same in the final model after backward elimination.
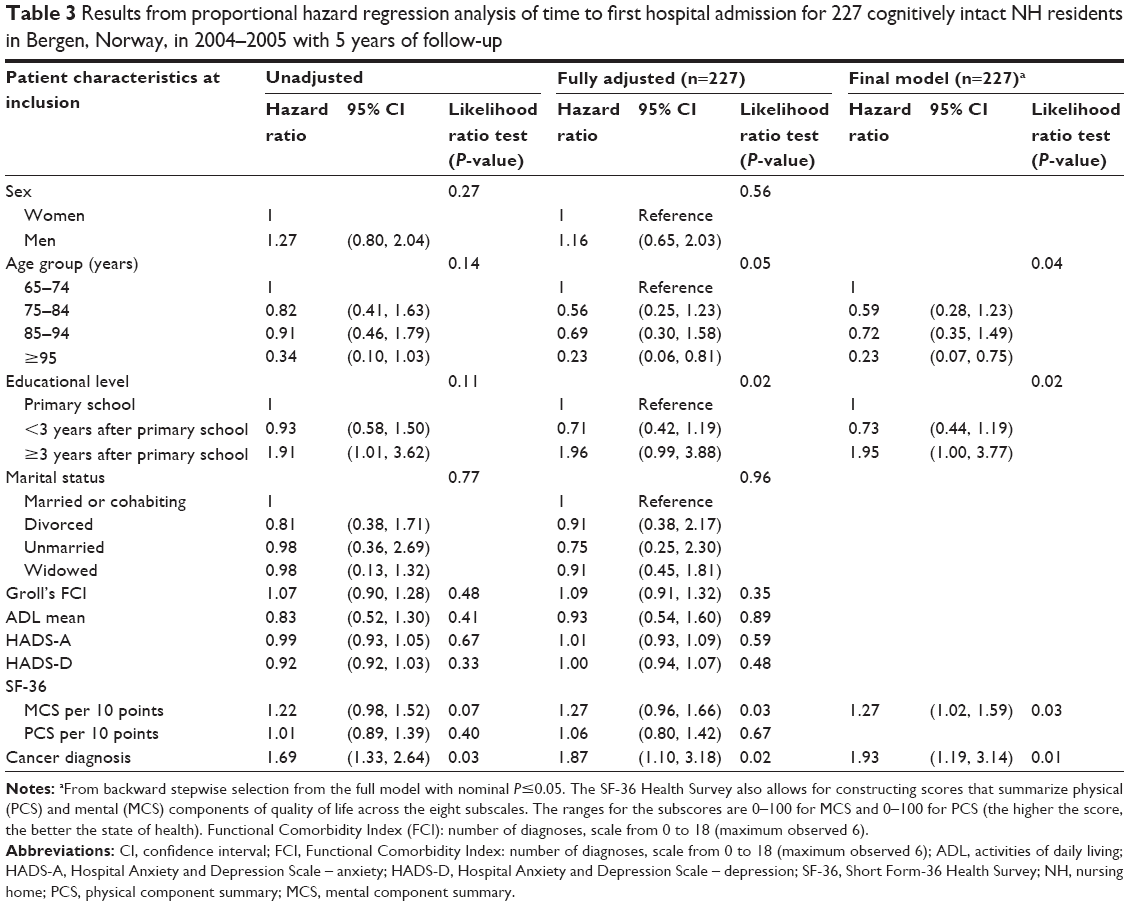 | Table 3 Results from proportional hazard regression analysis of time to first hospital admission for 227 cognitively intact NH residents in Bergen, Norway, in 2004–2005 with 5 years of follow-up |
Discussion
Better HRQOL (MCS), having a higher level of education, and low age were correlated with hospital admission among NH residents. Residents who had cancer had nearly twice the risk for hospital admission (1.9 times) as residents without cancer.
NH residents with cancer had the most days in hospital related to respiratory diseases and cancer. Hospital stays were mostly related to circulatory and respiratory diseases among the residents without a diagnosis of cancer. In our study, many residents had brief admissions, and many were discharged on the same day (median length of stay 0), in contrast to other studies3,6,17 in which stay in hospital related to cancer among NH residents had a median of 1–6 days. These studies also included residents with cognitive impairment and residents staying short term. Other studies have also shown that cognitive disability is correlated with more frequent hospitalization.2,17 The difference in the median number of days in hospital may reflect the difference in study populations. One explanation could be that many people were sent to a hospital for diagnostic clarification rather than treatment and care or for evaluation or planned treatment (cancer therapy) and not really admitted. This difference may also be explained by other studies not considering 1-day stays in hospital as admissions.3,5,6,17 The difference between the long-term care system in Norway and in other countries could also contribute to the differences in the practices for admission. Konetzka et al4 and Kirsebom et al6 reported that NHs run by private for-profit providers are more likely to send residents to hospital than public or private nonprofit providers.
For residents without cancer, circulatory diseases (median 1 day) and respiratory diseases (median 5 day) accounted for the most hospital days, in accordance with other studies.3,5,6,17
An important finding was that a higher MCS (better mental health) was associated with hospital admissions regardless of cancer. This finding is surprising, since the co-occurrence of poorer mental health and physical disorders has more commonly been found to be associated with increased risk for hospitalization.4,12 One explanation of our results could be that residents with more available personal coping resources and social network support report better mental health,35 which leads to better communication between residents, the family and caregivers and other health personnel in decisions about hospital admission. Wilkes et al41 reported that people whose family members visited often received better care and that the relatives were more connected to the residents and the staff. Social support is also related to more frequent hospitalization for NH residents.1 Other explanations could be that residents with worse mental health could be generally more frail and have decided together with a physician and their family to not be hospitalized but to receive palliative care and were treated in the NH. Or, residents could have fewer resources such as social network support1 and problems in communicating their needs. Mental health and hospital admission need to be studied further among NH residents.
In contrast to other studies,2,19,42 we found no associations between ADL, symptoms of anxiety and depression, and hospital admission. One explanation for our findings may be the available resources of nursing personnel and physicians in NHs. The residents who receive satisfactory assistance in performing ADL, treatment, and care in NHs will probably also feel safer. Continuity of care, high staff ratio, and competence have been shown to lead to better quality of care and less likelihood of being hospitalized.2,6,17 The causes of hospital admission in relation to self-reported HRQOL need to be studied further.
Strengths and limitations
The major strengths of our study are that we prospectively followed up all subjects from the 30 NHs for 5 years and that one author (JD) obtained all the interviews and obtained medical and demographic variables from the records. Other strengths include an excellent response rate (90%) and equivalent methods for comparing the people with and without cancer.
The main shortcoming is that no information was available about the decisions about referral to hospital, neither about whether some of the residents had signed advanced directives nor about their comprehensive care plans. Other shortcomings include no information on change in variables and the symptoms preceding and the causes of hospital admission (except for discharge diagnoses), no information on whether the admissions were planned or unplanned, and no data about the stage of cancer (during or after treatment) and the length of time elapsed since cancer was diagnosed. However, the purpose of the study was to use the baseline data of the study to assess the risk for hospital admission. We have no information about the staffing of physicians and nurses, which might influence the frequency of hospital admission4 or about the influence of family members. Our study included cognitively intact NH residents, whereas other studies on hospital admission have not focused especially on cognitive status.
Conclusion
Better self-reported HRQOL (MCS) was associated with hospital admissions, whereas self-reported physical health, ADL, and depression and anxiety symptoms were not. Cancer increased the risk after adjustment for all other risk factors but did not increase the effects of MCS, PCS, ADL, or depression or anxiety symptoms. Having a higher level of education and being less than 75 years of age were associated with hospitalization.
Relevance to clinical practice
Since residents with lower HRQOL (MCS) are less likely to be admitted to hospital, special attention should be given to them, regardless of whether they have cancer or not, to help them to communicate their needs. This information could be gathered by observing, asking the residents and close family, and gathering information from staff reports and medical reports. Clinical personnel should also give attention to residents, regardless of their HRQOL, ensuring that they receive proper treatment and care based on symptoms and perceived diseases. Clinical personnel should be aware of residents with fewer available resources, such as education, and of residents who have cancer and observe them to determine whether they have cancer-related symptoms that require intervention before hospital admission is required.
Acknowledgment
This work was supported by the Norwegian Cancer Society under grant number 59084001.
Disclosure
The authors report no conflicts of interest in this work.
References
Drageset J, Eide GE, Harrington C, Ranhoff AH. Acute hospital admission for nursing home residents without cognitive impairment with a diagnosis of cancer. Eur J Cancer Care. 2015;24:147–154. | ||
Grabowski DC, Stewart KA, Broderick SM, Coots LA. Predictors of nursing home hospitalization: a review of the literature. Med Care Res Rev. 2008;65:3–39. | ||
Graverholt B, Riise T, Jamtvedt G, Ranhoff AH, Kruger K, Nortvedt MW. Acute hospital admissions among nursing home residents: a population-based observational study. BMC Health Serv Res. 2011;11:126. | ||
Konetzka RT, Spector W, Limcangco MR. Reducing hospitalizations from long-term care settings. Med Care Res Rev. 2008;65:40–66. | ||
Kruger K, Jansen K, Grimsmo A, Eide GE, Geitung JT. Hospital admissions from nursing homes: rates and reasons. Nurs Res Pract. 2011;2011:247623. | ||
Kirsebom M, Hedstrom M, Wadensten B, Poder U. The frequency of and reasons for acute hospital transfers of older nursing home residents. Arch Gerontol Geriatr. 2014;58:115–120. | ||
Haugan G. Meaning-in-life in nursing-home patients: a correlate with physical and emotional symptoms. J Clin Nurs. 2014;23:1030–1043. | ||
Linton A, Lach H. Matteson & McConnell’s Gerontological Nursing: Concepts and Practice. Philadelphia: Saunders; 2007. | ||
Smalbrugge M, Pot AM, Jongenelis K, Beekman AT, Eefsting JA. Prevalence and correlates of anxiety among nursing home patients. J Affect Disord. 2005;88:145–153. | ||
Selbaek G, Kirkevold O, Engedal K. The prevalence of psychiatric symptoms and behavioural disturbances and the use of psychotropic drugs in Norwegian nursing homes. Int J Geriatr Psychiatry. 2007;22:843–849. | ||
Drageset J, Eide GE, Ranhoff AH. Cancer in nursing homes: characteristics and health-related quality of life among cognitively intact residents with and without cancer. Cancer Nurs. 2012;35:295–301. | ||
Rodin MB. Cancer patients admitted to nursing homes: what do we know? J Am Med Dir Assoc. 2008;9:149–156. | ||
Bourbonniere M, Van Cleave JH. Cancer care in nursing homes. Semin Oncol Nurs. 2006;22:51–57. | ||
Duncan JG, Bott MJ, Thompson SA, Gajewski BJ. Symptom occurrence and associated clinical factors in nursing home residents with cancer. Res Nurs Health. 2009;32:453–464. | ||
Jordhoy MS, Saltvedt I, Fayers P, Loge JH, Ahlner-Elmqvist M, Kaasa S. Which cancer patients die in nursing homes? Quality of life, medical and sociodemographic characteristics. Palliat Med. 2003;17:433–444. | ||
Buchanan RJ, Barkley J, Wang S, Kim M. Analyses of nursing home residents with cancer at admission. Cancer Nurs. 2005;28:406–414. | ||
Becker MA, Boaz TL, Andel R, Gum AM, Papadopoulos AS. Predictors of preventable nursing home hospitalizations: the role of mental disorders and dementia. Am J Geriatr Psychiatry. 2010;18:475–482. | ||
Liu LF, Wen MJ. A longitudinal evaluation of residents’ health outcomes in nursing homes and residential care homes in Taiwan. Qual Life Res. 2010;19:1007–1018. | ||
Miu DK, Chan CK. Prognostic value of depressive symptoms on mortality, morbidity and nursing home admission in older people. Geriatr Gerontol Int. 2011;11:174–179. | ||
Li CL, Chang HY, Lu JR. Health-related quality of life predicts hospital admission within 1 year in people with diabetes: a nationwide study from Taiwan. Diabet Med. 2009;26:1055–1062. | ||
Borowiak E, Kostka T. Predictors of quality of life in older people living at home and in institutions. Aging Clin Exp Res. 2004;16:212–220. | ||
Drageset J, Natvig GK, Eide GE, Bondevik M, Nortvedt MW, Nygaard HA. Health-related quality of life among old residents of nursing homes in Norway. Int J Nurs Pract. 2009;15:455–466. | ||
Ministry of Health and Care Services. FOR 1988-11-14 nr. 932: forskrift for sykehjem og boform for heldøgns omsorg og pleie av lov av 14. november 1988 med hjemmel i lov af 19. november 1982 nr. 66 om helsetjenestene i kommunene m.v. [FOR 1988-11-14 no. 932: regulations for nursing homes and living arrangements for 24-hour care and nursing pursuant to the Act of 14 November 1988 in accordance with the Municipal Health Act, Act No. 66 of 19 November 1982]. Oslo: Ministry of Health and Care Services; 1988. Norwegian. | ||
Ministry of Health and Care Services. FOR 2003-06-27 nr. 792: forskrift om kvalitet i pleie-og omsorgstjenestene for tjenesteyting etter lov av 19. november 1982 nr. 66 om helsetjenesten i kommune og etter lov av 13. desember 1991 nr. 81 om sosiale tjenester m.v. [FOR 2003-06-27 nr. 792: regulation of the quality of care in health and social services regulated by the Municipal Health Act, Act No. 66 of 19 November 1982 and the Social Services Act, Act No. 81 of 13 December 1991]. Oslo: Ministry of Health and Care Services; 2003. Norwegian. | ||
International Council of Nurses. The ICN Code of Ethics for Nurses. Geneva: International Council of Nurses; 2006. | ||
Hughes CP, Berg L, Danziger WL, Coben LA, Martin RL. A new clinical scale for the staging of dementia. Br J Psychiatry. 1982;140:566–572. | ||
McCulla MM, Coats M, Van Fleet N, Duchek J, Grant E, Morris JC. Reliability of clinical nurse specialists in the staging of dementia. Arch Neurol. 1989;46:1210–1211. | ||
Ware JE. SF-36 Health Survey Manual and Interpretation Guide. Boston: Medical Outcomes Trust; 2005. | ||
Lyons RA, Perry HM, Beverley N, Littlepage C. Evidence for the validity of the Short-form 36 Questionnaire (SF-36) in an elderly population. Age Ageing. 1994;23:182–184. | ||
Katz S, Akpom CA. A measure of primary sociobiological functions. Int J Health Serv. 1976;6:493–508. | ||
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67:361–370. | ||
Stordal E, Bjelland I, Dahl AA, Mykletun A. Anxiety and depression in individuals with somatic health problems. The Nord-Trondelag Health Study (HUNT). Scand J Prim Health Care. 2003;21:136–141. | ||
Haugan G, Drageset J. The hospital anxiety and depression scale – dimensionality, reliability and construct validity among cognitively intact nursing home patients. J Affect Disord. 2014;165:8–15. | ||
Groll DL, To T, Bombardier C, Wright JG. The development of a comorbidity index with physical function as the outcome. J Clin Epidemiol. 2005;58:595–602. | ||
Drageset J, Eide GE, Nygaard HA, Bondevik M, Nortvedt MW, Natvig GK. The impact of social support and sense of coherence on health-related quality of life among nursing home residents – a questionnaire survey in Bergen, Norway. Int J Nurs Stud. 2009;46:65–75. | ||
Lydersen S, Fagerland MW, Laake P. Recommended tests for association in 2×2 tables. Stat Med. 2009;28:1159–1175. | ||
Student. The probable error of a mean. Biometrika. 1908;V1:1–25. | ||
Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Soc. 1958;53:457–481. | ||
Mantel N. Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother Rep. 1966;50:163–170. | ||
Cox DR. Regression models and life tables. J R Stat Soc B. 1972;189:504–513. | ||
Wilkes L, Jackson D, Vallido T. Placing a relative into a nursing home: family members’ experiences after the move. A review of the literature. Geriaction. 2008;26:24–29. | ||
Mor V, Papandonatos G, Miller SC. End-of-life hospitalization for African American and non-Latino white nursing home residents: variation by race and a facility’s racial composition. J Palliat Med. 2005;8:58–68. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.