")
Back to Journals » OncoTargets and Therapy » Volume 11
Better efficacy of intrapleural infusion of bevacizumab with pemetrexed for malignant pleural effusion mediated from nonsquamous non-small cell lung cancer
Authors Song X , Chen D , Guo J, Kong L, Wang H , Wang Z
Received 15 August 2018
Accepted for publication 23 October 2018
Published 27 November 2018 Volume 2018:11 Pages 8421—8426
DOI https://doi.org/10.2147/OTT.S184030
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Federico Perche
Xinyu Song,1,2,* Dawei Chen,3,* Jun Guo,1 Li Kong,3 Haiyong Wang,1 Zhehai Wang1
1Department of Medical Oncology, Shandong Cancer Hospital Affiliated to Shandong University, Jinan, Shandong, People’s Republic of China; 2School of Medicine and Life Sciences, University of Jinan-Shandong Academy of Medical Sciences, Jinan, Shandong, People’s Republic of China; 3Department of Radiation Oncology, Shandong Cancer Hospital Affiliated to Shandong University, Jinan, Shandong, People’s Republic of China
*These authors contributed equally to this work
Background and objective: Several clinical trials have reported that intrapleural infusion of bevacizumab with or without cisplatin exhibits encouraging efficacy in nonsquamous non-small cell lung cancer (NS-NSCLC) patients with malignant serous cavity effusion. However, most of the studies included a number of different types of cancers or different hydrops types rather than focusing on one. In addition, no study reported the efficacy and toxicity of intrapleural infusion of bevacizumab and pemetrexed for advanced NS-NSCLC patients with malignant pleural effusion (MPE).
Patients and methods: We retrospectively collected patients with MPE mediated from NS-NSCLC who underwent intrapleural infusion of bevacizumab between August 2012 and February 2017. According to the different combined agents with bevacizumab, we divide patients into two groups: Group 1 (BP Group) intrapleural infusion of bevacizumab combined with pemetrexed and Group 2 (BD group) intrapleural infusion of bevacizumab combined with cisplatin.
Results: A total of 45 patients were enrolled in this study. Twenty-two of them received intrapleuralinfusion of bevacizumab and pemetrexed every 2 weeks, 23 received bevacizumab and cisplatin after draining effusion as much as possible. The progression-free survival for patients in BP group was significantly higher than BD group (P < 0.05) while the overall survival between the two groups was not significantly different (P > 0.05). In addition, there was no statistical difference in adverse effects between two groups.
Conclusion: Intrapleural infusion of bevacizumab and pemetrexed is effective and tolerable for patients with MPE mediated from NSCLC.
Keywords: NS-NSCLC, MPE, bevacizumab, pemetrexed
Introduction
Lung cancer is the main cause of cancer-related deaths, and non-small cell lung cancer (NSCLC) accounts for ~85% of all new lung cancer cases.1 Most NSCLC patients suffer serious syndromes, and malignant pleural effusion (MPE) is one of the most common syndrome, seriously influencing patients’ quality of life (QoL) and management.2 In clinic, thoracentesis and then intracavitary infusion of agents is a common treatment to control symptomatic MPE. Traditional intracavitary agents include cytogenesis, biological response modifiers, sclerosis agents, and so on. However, the efficacies and toxicities are unsatisfactoried.3
In recent years, several clinical trials have revealed that intrapleural infusion of bevacizumab (BEV) with or without cisplatin controls malignant serous cavity effusion effectively.4–7 Kitamura et al demonstrated a disease control rate (DCR) of 92.3% and median progression-free survival (mPFS) of 312 days in MPE patients treated with intravenous BEV plus chemotherapy, without obvious treatment-related toxicity.8 In addition, Chen et al reported an objective response rate (ORR) of 65.21%, DCR of 86.96%, and mPFS of 6 months in patients with MPE due to mesothelioma.9 However, most of the studies included a number of different types of cancers or different hydrops types rather than focusing on one. According to previous studies, the administration of intrapleural BEV was in 5 mg/kg every 3 or 4 weeks,10–12 and Chen et al found that intrapleural infusion of BEV in lower dose was effective to control MPE in NSCLC patients, not only in curative effect, but also the toxicity.7 Pemetrexed plus cisplatin is the first-line chemotherapy for nonsquamous NSCLC (NS-NSCLC) in clinical practice.13 Considering the evidence above, we suppose that intrapleural infusion of BEV and pemetrexed is an effective treatment for MPE mediated from NS-NSCLC.
Thus, in this study, we used a retrospective setting to compare the effectiveness of intrapleural infusion of BEV and pemetrexed versus BEV and cisplatin in patients with MPE mediated from NS-NSCLC.
Patients and methods
Patients
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Committee Board of Shandong Cancer Hospital (Jinan, People’s Republic of China). Written informed consent was obtained from all patients. Inclusion criteria were: advanced NS-NSCLC confirmed with histological or pathological examinations; malignant cells were found in pleural precipitation by cytological examination or pathological changes of malignant tumors were observed in pleural biopsy tissues; ultrasonic and computed tomography examinations confirmed an increased amount of pleural effusion; no pleurodesis were delivered within 2 month before the study; Karnofsky Performance Score (KPS) >60 and a predicted survival time longer than 2 months; no major organ dysfunction, heart rate, liver, and kidney test all resulted within normal range. The exclusion criteria were: allergic reactions to BEV, cisplatin, or pemetrexed; major organ dysfunctions or detectable internallesions; pregnancy or breastfeeding; metastasis to the central nervous system; history of refractory psychiatric disease; respiratory failure or severe chronic pulmonary disease; uncontrolled active infection; MPE was not accurately measured due to various reasons.
Methods
Thoracentesis was performed for all patients with the aid of ultrasound. After thoracentesis and pleural fluid drained as much as possible, patients received intrapleural infusion of agents. We divided patients with two groups. BP group: BEV 200 mg and pemetrexed 400–600 mg were dissolved in 40 mL normal saline. BD group: BEV 200 mg and cisplatin 40–60 mg were dissolved in 40 mL normal saline. Then patients were asked for a bed rest of 1–2 hours and turn over every 20 minutes to encourage the uniform distribution of drugs in pleural cavity. Treatments were repeated every 2 weeks with the maximum of three courses per patient. In addition, all patients were accompanied by platinum-based systematic chemotherapy.
Efficacy evaluation
Primary monitoring parameters
The response evaluation was performed after the completion of at least one course of treatment. Evaluation of immediate response was determined according to previous studies and WHO therapeutic criteria for pleural effusion.4–7 Complete remission (CR): accumulated effusion had disappeared and remained stable for at least 4 weeks; partial remission (PR): accumulated effusion had decreased by 50%, associated with improved symptoms with no increased accumulation of fluid, and remained stable for at least 4 weeks; remission not obvious (NC): <50% of the pleural effusion had disappeared, or then was no noticeable change in symptoms; progressive disease (PD): the amount of accumulated effusion had increased with worsening of symptoms. The ORR was calculated as CR plus PR; DCR was calculated by taking the sum of CR, PR, and NC. Progression-free survival (PFS) was defined as the interval between the initiation of intrapleural infusion and the time of either effusion progression or death. Overall survival (OS) was measured from the date of initial intrapleural infusion to the date of death from any cause or the last known follow-up.
Adverse events
Treatment-related adverse events were evaluated by the Common Toxicity Evaluation Criteria according to the National Cancer Institute and classified as grade 1–5.11 Grade 1 adverse events are mild adverse reactions that are usually asymptomatic and do not require intervention or medication. Grade 2 adverse events refer to moderate adverse reactions, usually with clinical symptoms and requiring local drug or other interventions. Such reactions may affect the body’s functions, but do not impair daily life and activities. Grade 3 adverse events refer to relatively serious adverse reactions that may cause adverse consequences, usually with complex symptoms, requiring active intervention such as surgery or hospitalization. Grade 4 adverse events are those that may pose a potential threat to life. Such reactions are often disabling or even leading to organ damage or loss of function. Grade 5 adverse events are death.
Quality of life
QoL is referred to the change of KPS and classified as improvement (KPS score increasing ≥10 points), stabilization (KPS score no increasing or decreasing), and reduction (KPS score decreasing ≥10 points).
Statistical analysis
All cases were followed-up through telephone, outpatient service, or hospitalization until May 2018, with the death of the patient as the end of the follow-up. SPSS 19.0 software was applied. The difference between different treatments was studied via t-test, whereas chi-squared test was applied for enumeration data. P-value < 0.05 was considered as of statistical significance.
Results
Demographic characteristics
A total of 45 patients were enrolled in our study. Of which, 22 of them received intrapleural infusion of BEV and pemetrexed every 2 weeks, 23 received BEV and cisplatin. Patients’ demographic characteristics are listed in Table 1. Characteristics were similar between the two treatment groups and no significant difference was reported. All 45 patients completed the treatments. The patients included 24 males and 21 females with an average age of 56 (range from 32 to 72) years.
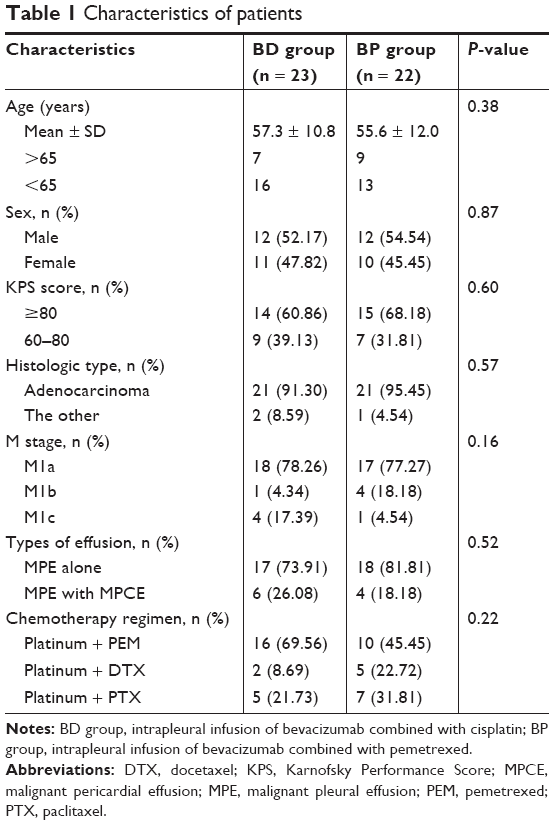 | Table 1 Characteristics of patients |
Response evaluation
In BD group, two patients presented with CR, 11 with PR, five with NC, and five patients with PD. Thus, ORR in BP group was 56.52% (13/23) and DCR 78.26% (18/23). In BP group, two patients had CR, 17 had PR, two had NC, and one had PD. ORR was 86.36% (19/22) and DCR was 95.45% (21/22). Thus, the ORR of patients in BP group were significantly higher than that of BP group (P < 0.05; Table 2).
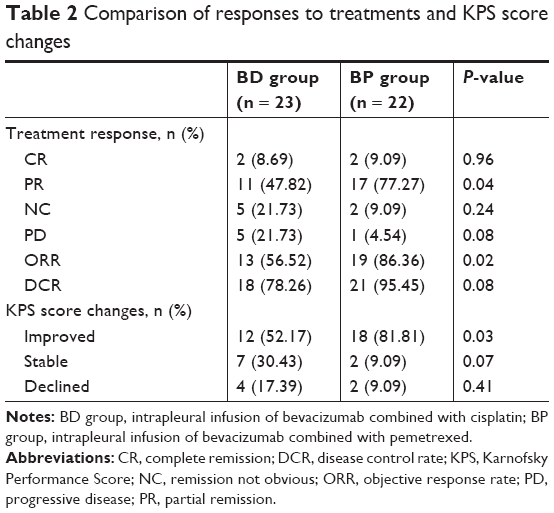 | Table 2 Comparison of responses to treatments and KPS score changes |
PFS and OS
The median PFS was 5.4 months in BP group, and the median OS was 10.5 months. In BD group, the median PFS was 4.0 months and the OS was 10.3 months. The PFS for BP group was significantly higher than the BD group (P < 0.05; Figure 1), whereas the OS between the two groups was not significantly different (P > 0.05; Figure 2).
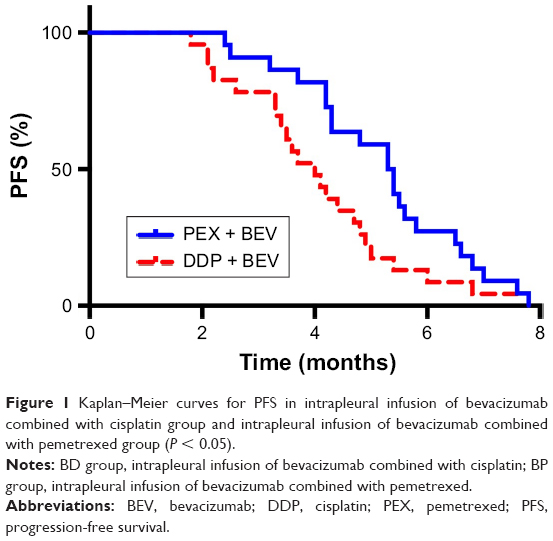 | Figure 1 Kaplan–Meier curves for PFS in intrapleural infusion of bevacizumab combined with cisplatin group and intrapleural infusion of bevacizumab combined with pemetrexed group (P < 0.05). |
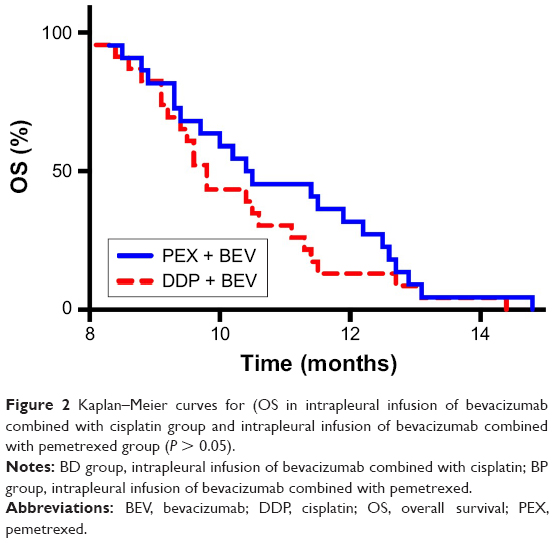 | Figure 2 Kaplan–Meier curves for (OS in intrapleural infusion of bevacizumab combined with cisplatin group and intrapleural infusion of bevacizumab combined with pemetrexed group (P > 0.05). |
Adverse events
No treatment-related deaths occurred in both treatments. The common untoward reactions of chemotherapeutics and BEV that occurred in both groups are listed in Table 3. The major adverse reactions in both groups comprised neutropenia, thrombopenia, anemia, fatigue, fever, hepatic damage adrenal damage. The incidence of adverse events was comparable in both groups. Moreover, only few of them are ranged from grade 3 to 4 according to WHO guideline. BEV-related adverse events mainly include hypertension, proteinuria, thrombus, hemorrhage, electrocardiograph change, and perforations, and no statistical difference exists between the two groups. Only some individual patients had these side effects, and these conditions did not require special treatment. A few patients of BP group showed slight proteinuria. However, this adverse effect was diminished after appropriate renal protection treatment and no significant difference presented in the two groups.
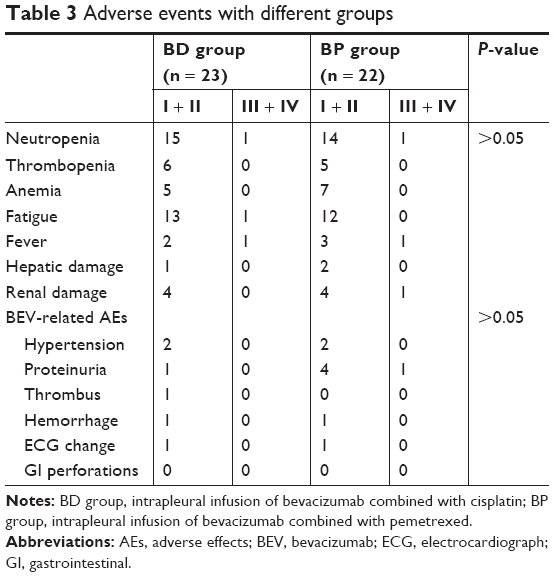 | Table 3 Adverse events with different groups |
Quality of life
QoL was improved in 81.81% (18/22) of the patients in the BP group and 52.17% (12/23) patients in BD group, and this difference was statistically significant (P < 0.05; Table 2).
Discussion
MPE plays a major role in QoL and survival for NSCLC patients, which can cause stethalgia, cough, and disturbance in respiration.3 Thoracocentesis and intrapleural infusion of drugs can relieve the symptoms, but MPE will occur frequently in a short period. In addition, pleural effusion has high concentration of nutriment such as carotenoid,14 lipid-soluble vitamin and protein,15 etc. Hence, thoracocentesis or persistent pleural drainage might lead to cachexia. To date, in clinic, common treatment methods for MPE include intrapleural infusion of chemotherapeutic agents, biological response modifiers, or simple thoracocentesis. However, all these treatments have unsatisfactory efficacy or severe adverse reactions.
VEGF is a main factor in the increase of the permeability of small vessels, which plays a significant role in the formation of MPE.16,17 Previous studies have discovered the relationship between the quantity of malignant serous cavity effusion and VEGF level in tumor-burdened animals.18,19 But there is lack of correlation between pleural VEGF levels and response.20 BEV, a humanized antihuman VEGF-A monoclonal antibody, is the most popular anti-VEGF agent in clinic. Nowadays, intrapleural infusion of BEV combined with chemotherapeutic agents to treat with MPE has been demonstrated to be an effective method in many studies.6,7,21–23 Given the anti-VEGF effect of BEV, for the small vessels in pleural cavity, the permeability will be evaluated and the pleural pressure will be decreased. Thus, chemotherapeutic agents could pass through the pleural barrier and encourage it to reach a relative high concentration for a longer time, then kill tumor cells and decrease pleural effusion formation.
BEV has been demonstrated necessary in the treatment of many types of advanced cancers, including of the colorectal, kidney, breast, and glioblastoma. And it is functional in suppressing pleural, peritoneal, and pericardial effusion in combination with cisplatin was appreciated relatively recently.4–7,21–24 However, most of the studies included a number of different types of cancers or different hydrops types rather than focusing on one. In addition, cisplatin is a broad-spectrum antitumor drug, while pemetrexed is a relatively special agent for NSCLC in the first line chemotherapy.
Our study showed that the ORR for intrapleural BEV combined with pemetrexed was 86.36%, that is statistically higher than the 56.52% by BEV and cisplatin (P < 0.05). This result accorded with a recent study by Chen et al treating patients with MPE using intrapleural injection of pemetrexed 500 mg and BEV 300 mg had an ORR of 65.21% and DCR of 86.96%.7 The difference in response between that study and ours was possibly due to the different tumor types and the dose of the agents. Jiang et al compared the efficacy of intrapleural infusion of BEV and cisplatin with cisplatin alone.25 The ORR and DCR of BEV and cisplatin were significant superior than that of cisplatin alone. In another report, BEV combined with cisplatin obviously controlled MPE in a lung cancer patient. Similarly, intrapericardial, intraperitoneal, or intravenous administration of BEV has been demonstrated to effectively control malignant serous cavity effusion. Chen et al used BEV to treat a 45-year-old patient with refractory malignant pericardial effusion (MPCE) due to NSCLC. MPCE had complete response and the PFS of the patient was 4 months.26 El-Shami et al10 reported that nine patients with malignant ascites who received intraperitoneal BEV got long-lasting control in all cases.
In our study, the ORR and DCR of patients treated with intrapleural infusion of BEV combined with pemetrexed was superior to that of these treated with BEV and cisplatin. The BEV and pemetrexed group also showed statistical difference in PFS compared with the group treated with BEV and cisplatin. Regarding adverse events, there was no significant difference in two groups and no obvious severe advents occurred. However, the present study included a relatively small number of patients and even difficult for multivariate analysis.
Conclusion
Intrapleural infusion of pemetrexed and BEV is an efficient, safe, and novel treatment for MPE with NS-NSCLC. More clinical studies are required to explore the require dosage of the agents used in the treatment.
Acknowledgments
The authors would like to express their gratitude to the enrolled patients and to the members of the Shandong Cancer Hospital Affiliated to Shandong University.
Disclosure
The authors report no conflicts of interest in this work.
References
Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893–2917. | ||
Sugiura S, Ando Y, Minami H, Ando M, Sakai S, Shimokata K. Prognostic value of pleural effusion in patients with non-small cell lung cancer. Clin Cancer Res. 1997;3(1):47–50. | ||
Ayantunde AA, Parsons SL. Pattern and prognostic factors in patients with malignant ascites: a retrospective study. Ann Oncol. 2007;18(5):945–949. | ||
Chen D, Li X, Zhao H, et al. The efficacy of pemetrexed and bevacizumab intrapleural injection for malignant pleural mesothelioma-mediated malignant pleural effusion. Indian J Cancer. 2014;51 Suppl 3(Suppl 3):e82–e85. | ||
Tamiya M, Tamiya A, Yamadori T, et al. Phase 2 study of bevacizumab with carboplatin-paclitaxel for non-small cell lung cancer with malignant pleural effusion. Med Oncol. 2013;30(3):676. | ||
Ishimoto O, Saijo Y, Narumi K, et al. High level of vascular endothelial growth factor in hemorrhagic pleural effusion of cancer. Oncology. 2002;63(1):70–75. | ||
Chen D, Song X, Zhang Y, Kong L, Wang H, Yu J. Optimizing intrapleural bevacizumab dosing in non-small-cell lung cancer-mediated malignant pleural effusion: less is more. Future Oncol. 2018;14(21):2131–2138. | ||
Kitamura K, Kubota K, Ando M, et al. Bevacizumab plus chemotherapy for advanced non-squamous non-small-cell lung cancer with malignant pleural effusion. Cancer Chemother Pharmacol. 2013;71(2):457–461. | ||
Chen D, Song X, Shi F, et al. Greater efficacy of intracavitary infusion of bevacizumab compared to traditional local treatments for patients with malignant cavity serous effusion. Oncotarget. 2017;8(21):35262–35271. | ||
El-Shami K, Elsaid A, El-Kerm Y. Open-label safety and efficacy pilot trial of intraperitoneal bevacizumab as palliative treatment in refractory malignant ascites. J Clin Oncol. 2007;25(18S):9043. | ||
Bellati F, Napoletano C, Ruscito I, et al. Complete remission of ovarian cancer induced intractable malignant ascites with intraperitoneal bevacizumab. Immunological observations and a literature review. Invest New Drugs. 2010;28(6):887–894. | ||
Hamilton CA, Maxwell GL, Chernofsky MR, Bernstein SA, Farley JH, Rose GS. Intraperitoneal bevacizumab for the palliation of malignant ascites in refractory ovarian cancer. Gynecol Oncol. 2008;111(3):530–532. | ||
Wu YL, Lu S, Lu Y, et al. Results of PROFILE 1029, a Phase III comparison of first-line crizotinib versus chemotherapy in East Asian patients with ALK-positive advanced non-small cell lung cancer. J Thorac Oncol. 2018;13(10):S155630721–S155630724. | ||
Martínez-Moragón E, Aparicio J, Sanchis J, Menéndez R, Cruz Rogado M, Sanchis F. Malignant pleural effusion: prognostic factors for survival and response to chemical pleurodesis in a series of 120 cases. Respiration. 1998;65(2):108–113. | ||
Heffner JE, Klein JS. Recent advances in the diagnosis and management of malignant pleural effusions. Mayo Clin Proc. 2008;83(2):235–250. | ||
Ruiz E, Aleman C, Alegre J, Soriano T, Fernandez deSevilla T. Angiogenic factors and angiogenesis inhibitorsin exudative pleural effusions. Lung. 2005;183:185–195. | ||
Hamed EA, El-Noweihi AM, Mohamed AZ, Mahmoud A, Mediators MV. Vasoactive mediators (VEGF and TNF-alpha) in patients with malignant and tuberculous pleural effusions. Respirology. 2004;9(1):81–86. | ||
Jia L, Du Y, Li T, et al. Differential expression of vascular endothelial growth factor-A, -C and -D for the diagnosis and prognosis of cancer patients with malignant effusions. Oncol Lett. 2015;10(2):667–674. | ||
Zhao H, Li X, Chen D, et al. Intraperitoneal administration of cisplatin plus bevacizumab for the management of malignant ascites in ovarian epithelial cancer: results of a phase III clinical trial. Med Oncol. 2015;32(2):292. | ||
Hsu LH, Hsu PC, Liao TL, Feng AC, Chu NM, Kao SH. Pleural fluid osteopontin, vascular endothelial growth factor, and urokinase-type plasminogen activator levels as predictors of pleurodesis outcome and prognosticators in patients with malignant pleural effusion: a prospective cohort study. BMC Cancer. 2016;16(1):463. | ||
Thickett DR, Armstrong L, Millar AB. Vascular endothelial growth factor (VEGF) in inflammatory and malignant pleural effusions. Thorax. 1999;54(8):707–710. | ||
Grove CS, Lee YC. Vascular endothelial growth factor: the key mediator in pleural effusion formation. Curr Opin Pulm Med. 2002;8(4):294–301. | ||
Ribeiro SC, Vargas FS, Antonangelo L, et al. Monoclonal anti-vascular endothelial growth factor antibody reduces fluid volume in an experimental model of inflammatory pleural effusion. Respirology. 2009;14(8):1188–1193. | ||
Oida T, Mimatsu K, Kano H, et al. Pericardiocentesis with cisplatin for malignant pericardial effusion and tamponade. World J Gastroenterol. 2010;16(6):740–744. | ||
Jiang L, Li P, Gong Z, et al. Effective treatment for malignant pleural effusion and ascites with combined therapy of bevacizumab and cisplatin. Anticancer Res. 2016;36(3):1313–1318. | ||
Chen D, Zhang Y, Shi F, et al. Sustained response of malignant pericardial effusion to intrapericardial bevacizumab in an advanced lung cancer patient: a case report and literature review. Onco Targets Ther. 2015;8:2767–2770. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.