")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Benzodiazepine and Z-Drug Use in Switzerland: Prevalence, Prescription Patterns and Association with Adverse Healthcare Outcomes
Authors Landolt S, Rosemann T , Blozik E , Brüngger B, Huber CA
Received 3 November 2020
Accepted for publication 2 March 2021
Published 12 April 2021 Volume 2021:17 Pages 1021—1034
DOI https://doi.org/10.2147/NDT.S290104
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Roger Pinder
Salome Landolt,1 Thomas Rosemann,1 Eva Blozik,1,2 Beat Brüngger,2 Carola A Huber1,2
1Institute of Primary Care, University of Zürich, University Hospital Zürich, Zürich, Switzerland; 2Department of Health Sciences, Helsana Insurance Group, Zürich, Switzerland
Correspondence: Carola A Huber
Helsana Insurance Group, P.O. 8081, Zürich, Switzerland
Tel + 41 43 340 6341
Fax +41 43 340 0434
Email [email protected]
Purpose: This study aimed to give a nationwide comprehensive picture of the prevalence and prescription patterns of benzodiazepines (BZ) and Z-drugs (ZD) in Switzerland and to analyze the association with adverse health care outcomes.
Patients and Methods: A population-based, cross-sectional study was conducted, using a large health insurance database in Switzerland. Records from all adult patients with ≥ 1 prescription for a benzodiazepine and/or a Z-drug in 2018 were included. We calculated the prevalence of BZ and ZD user (extrapolated to the Swiss general population), the number of prescriptions and the type of provider (among each BZ and ZD only user). Multivariate logistic regression models were performed to estimate the association between drug prescription and the risk of hospitalization in different healthcare settings.
Results: Of a total of 844ʹ692 patients, 95ʹ179 had ≥ 1 BZ and/or ZD prescription in 2018. The extrapolated one-year prevalence for the general Swiss population was 8.1% for a BZ prescription, 3.5% for a ZD prescription, and 10.5% for a BZ and/or ZD prescription, and continuously increased with age. The majority of the elderly (over 65 years) had ≥ 1 prescription (BZ: 51.9%; ZD: 56.9%; BZ and/or ZD: 53.5). The proportion of patients with ≥ 6 prescriptions per year was 23.1% for BZ only user and 35.2% for ZD only user. Most patients had ≥ 1 prescription from a general practitioner. Regression models showed a higher likelihood to be admitted to acute care, psychiatry, rehabilitation, or nursing home with ≥ 1 prescription for a benzodiazepine and/or a Z-drug.
Conclusion: This study is the first to give a nationwide overview of the current use of benzodiazepines and Z-drugs in Switzerland based on health insurance claims data. The results revealed a remarkably high prevalence among the general Swiss population, especially in older generations. The negative consequences of heavy BZ and ZD use are a crucial public health problem, that should be addressed.
Keywords: anxiolytics, sedatives, pharmacoepidemiology, health insurance claims data
Introduction
Introduced into clinical medicine in 1961, benzodiazepines can be categorized as short-acting (half-life (t1/2) <24 h) and long-acting (t1/2 >24 h).1 Benzodiazepines sedate the patient by decreasing activity and arousal and thereby facilitate falling asleep. Furthermore, they have anticonvulsive and muscle-relaxant activity. These effects are caused by the binding of the inhibitory neurotransmitter gamma-aminobutyric acid “GABA” to the GABAA receptor, for which benzodiazepines increase the affinity. The Z-drugs (zolpidem and zopiclone) also bind to the GABAA receptor and lead to an increased affinity for GABA, but are structurally different from benzodiazepines.1 Benzodiazepines and Z-drugs are primarily prescribed for the treatment of insomnia, with benzodiazepines additionally being used for the treatment of anxiety.2,3
Benzodiazepines and Z-drugs are some of the most frequently prescribed drugs in several health care systems, although their continued use is not supported by evidence and medical recommendations.4–8 European guidelines for the diagnosis and treatment of insomnia recommend the use of benzodiazepines and Z-drugs only as effective short-term treatments of insomnia (<4 weeks), if cognitive behavioral therapy is not sufficient or available (first-line treatment).9 In the treatment of anxiety disorders, benzodiazepines are important due to their fast onset of action, but are usually a second-line option and used as short-term or additional therapy.10 Both national and international recommendations like the updated “AGS Beers Criteria for Potentially Inappropriate Medication Use in Older Adults” or the “Choosing wisely Switzerland” campaign even postulate that benzodiazepine and Z-drug use should be avoided, especially in the elderly.7,8 Nevertheless, results from international studies showed a high prevalence of benzodiazepine use ranging from 2.1% up to 5.2% in the general population, and among older populations a prevalence ranging from 30.0% to 35.1% in a 12-month period.4,5,11–13 There exist only a few studies on the use of benzodiazepines in Switzerland.14–20 For example, one study, which was based on claims data from the elderly (≥65 years), showed that approximately 20% had at least one benzodiazepine prescription. However, this study included only the elderly and represented only a small part of Switzerland (nine out of 26 cantons).14 Furthermore, previous research reported a benzodiazepine prescription prevalence of 9% (within 6 months) and 11% (within 1 year).15–20 These studies, however, were based on pharmacy dispensing, self-reported and outdated data. There is no study in Switzerland that provides a comprehensive overview of benzodiazepine prescription patterns including prescriber information of nationwide data.
Additionally, guideline recommendations were based on the fact that the use of benzodiazepines and Z-drugs can have several severe side effects. Various studies have shown an association with cognitive decline in older people, although the underlying mechanisms are still unclear.21–25 There is also a higher risk to be hospitalized for fall-related injuries after taking benzodiazepines or Z-drugs among elderly people.26,27 Furthermore, hospital patients who were prescribed benzodiazepines during their stay had a higher likelihood to have more bed days in the hospital.28 There is very little research about the association of benzodiazepine use and adverse health care outcome in Switzerland. To the best of our knowledge, only Luta and colleagues have investigated that benzodiazepine users had a higher probability of being hospitalized for any cause and trauma in comparison to non-users.14 However, this study included only residents from a small part of Switzerland and estimated the effect of benzodiazepine use only on one healthcare outcome.
Therefore, the aims of this study were to give a current and comprehensive overview of the use of benzodiazepines and Z-drugs in Switzerland. Furthermore, we aimed to estimate the association between benzodiazepine and Z-drug use and various adverse health care outcomes.
Patients and Methods
Study Design and Data Source
This cross-sectional study was based on health insurance claims data from the Helsana Group in the 1-year period of 2018. The Helsana Group is one of Switzerland’s largest health insurance companies, covering about 1.18 million people, which comprises about 14% of the entire Swiss population in all 26 cantons of Switzerland. The data is considered almost representative of the general Swiss population. Every resident in Switzerland contracts mandatory health insurance on the private insurance market (controlled by federal authorities) to cover medical treatment. Our claims data are highly reliable as the recorded data comprises almost all pharmacy and health care invoices. Health care costs are shared by insurants and health care insurance companies. The insured person must pay an annual deductible of between 300 and 2500 Swiss francs per year (chosen by the insured person) and a premium monthly. A higher annual deductible results in a lower monthly premium. The insured person can choose between the care models of standard care and managed care, which also includes telemedical models and family doctor models.
Following the national ethical and legal regulation, ethical approval by the local Ethics Committee of the Canton of Zurich and patient consent were not needed for this study. All data accessed complied with relevant data protection and privacy regulations.
Identification of Study Participants and Drug Classification
All enrolled persons ≥18 years, which were prescribed at least one benzodiazepine or Z-drug in 2018, were included. Benzodiazepines and Z-drugs are available only by prescription in Switzerland. Prescribers do not have any information about prescription from other physicians. Every prescribed drug purchased in a pharmacy is charged to the health insurance company. Benzodiazepines and Z-drugs were classified based on their therapeutic and chemical properties according to the Anatomical Therapeutic Chemical (ATC) classification system of the World Health Organization.29 Anxiolytic benzodiazepines were classified under N05BAxx, sedative benzodiazepines were classified under N05CDxx and Z-drugs under N05CFxx. Benzodiazepines, which were used for the treatment of epilepsy (clonazepam (N03AE01), midazolam (N03AE02)), were excluded.
Additionally, benzodiazepines were categorized as short-acting for a half-life (t1/2) <24 h and long-acting for a half-life (t1/2) >24 h.1 According to the Ashton Manual classification of long-acting and short-acting benzodiazepines and similar drugs were defined as follows: Oxazepam (N05BA04), Lorazepam (N05BA06), Bromazepam (N05BA08), Alprazolam (N05BA12), Triazolam (N05CD05), Lormetazepam (N05CD06), Temazepam (N05CD07), Midazolam (N05CD08), Zopiclone (N05CF01) and Zolpidem (N05CF02) were classified as short-acting agents. Diazepam (N05BA01), Chlordiazepoxid (N05BA02), Clorazepate (N05BA05), Clobazam (N05BA09), Ketazolam (N05BA10), Prazepam (N05BA11), Flurazepam (N05CD01), Nitrazepam (N05CD02) and Flunitrapezam (N05CD03) were classified as long-acting agents.30
Patient and Provider Characteristics
Patient characteristics included gender, age, language region (German including Rhaeto-Romanic, French, Italian) and residence. The national community typology provided by the Swiss Federal Office of Statistics was used to categorize the region of residence as “urban” and “rural”.31 The type of health insurance coverage (standard or managed care) and the level of the deductible class (low rated as ≤500 CHF and high rated as >500 CHF) were evaluated. The presence of comorbid chronic conditions was identified by a proxy variable on the basis of drug prescriptions related to chronic conditions. Twenty-two comorbid chronic conditions were classified.32
To calculate the proportion of patients with a single chronic condition in 2018, we divided the number of patients with at least one ATC-group defined medication prescription by all insured persons of the study.
Furthermore, the type of physician (provider), who is exclusively authorized to prescribe medication in Switzerland, was analyzed. Four provider categories were defined: general practitioner only, psychiatrist only, other medical specialists only, and combination of providers. In the latter category, all patients were included, who received their benzodiazepine prescription from at least two different kinds of providers.
Objectives
To determine the current prevalence of benzodiazepine and Z-drugs by measuring unadjusted and extrapolated proportions of persons with prescribed drugs within 1 year.
To determine the prescription patterns of benzodiazepine and Z-drug use by drug classes, number of prescriptions and type of provider.
To determine the association between benzodiazepine and Z-drug use and health care outcomes.
Statistical Analyses and Outcomes
We calculated the prevalence of benzodiazepine and/or Z-drug prescription by dividing the number of persons with at least one prescription of benzodiazepines and/or Z-drugs in 2018 by the total number of persons ≥18 years insured by the Helsana Group. The prevalences were also calculated by age and sex. Additionally, we examined the prevalence of individuals with drug prescription extrapolated for the adult Swiss population. For the extrapolation, we used census data provided by the Swiss Federal Office of Statistics. We could test the applicability and representativeness of our data to the adult Swiss population by a direct comparison between the raw and extrapolated results. Sex, age and canton of residence were adjusted through the procedure of extrapolation.
Patient characteristics of “benzodiazepine/Z-drug user” and “benzodiazepine/Z-Drug non-user” were compared by Fisher’s exact test (dichotomous characteristics), chi-squared test (>2 characteristics), and Kruskal–Wallis test (continuous characteristics). Furthermore, we analyzed the number of prescriptions and type of provider in the following subsamples: “benzodiazepine user only” the group “Z-drug user only” and “benzodiazepines and/or Z-drug user only”. As the last step, we provided group comparisons between patients with a prescription for a short-acting and a long-acting benzodiazepine.
Finally, logistic regression models were performed to estimate the association between benzodiazepine and Z-drug use and adverse health care outcomes. The outcomes included hospitalization in acute care, hospitalization in psychiatry, admission in a rehabilitation facility, and admission in a nursing home within 2018. The logistic regression models were controlled for age groups (18–25, 25–35, 35–45, 55–65, 65–74 (reference group), 75–85, ≥85), gender (male (reference group) and female), insurance model (managed care or standard model (reference group)), type of annual deductible (high (reference group) or low deductible), residential area (rural or urban (reference group)), language region (German (reference group), French, Italian) and the number of comorbid conditions (no comorbid conditions as the reference group). We provided our estimations as odds ratios (ORs) with a confidence interval of 95% (CIs). For all analyses, the R version 3.6.1 (R Development Core Team 2019) was used. Statistical significance was defined for a p-value <0.05.
Results
Prescription Prevalence by Population Characteristics
Of a total of 844ʹ692 patients, 8.7% had a prescription for benzodiazepines, 3.7% for Z-drugs, and 11.3% for benzodiazepines and/or Z-drugs in 2018 (Table 1). The extrapolated prevalence of the general Swiss population was 8.1% for benzodiazepines, 3.5% for Z-drugs, and 10.5% for benzodiazepines and/or Z-drugs (results not shown). Figures 1–3 show the extrapolated prevalence of use by sex and age groups (in 2-year categories). Women had a higher extrapolated prevalence than men for benzodiazepine use, for Z-drug use, and benzodiazepine and/or Z-drug use in all age groups. Comparable with the unadjusted medication groups, the majority of the drug user were female (65.5% of benzodiazepines recipients, 66.7% of Z-drugs recipients, 65.6% of benzodiazepines and/or Z-drugs recipients; Table 1).
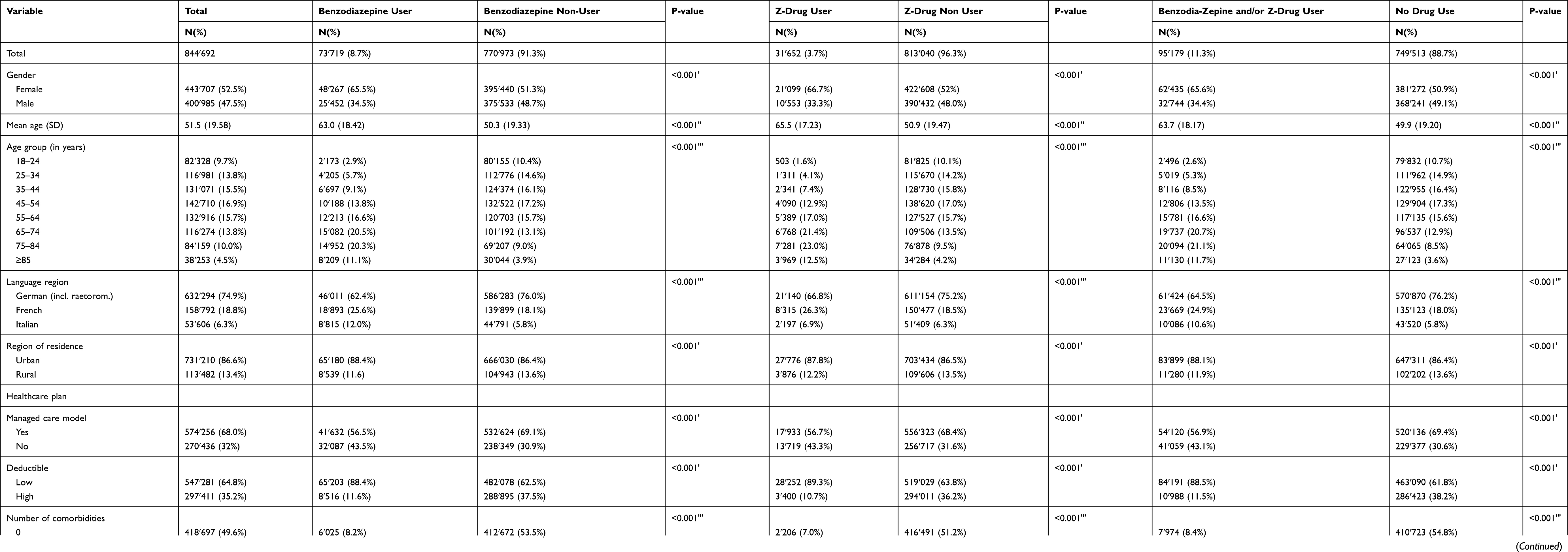 |
Table 1 Characteristics of the Study Population with and without Benzodiazepine and Z-Drug Use in 2018 |
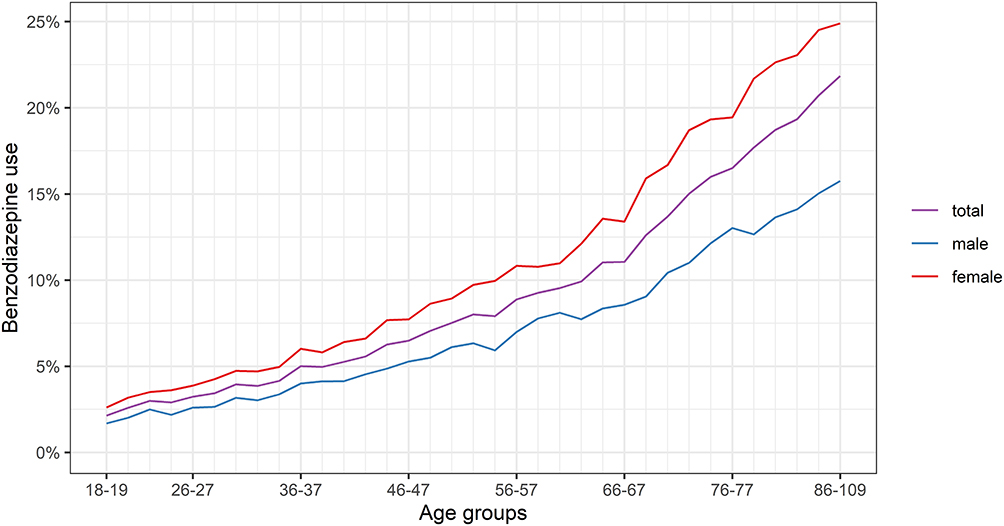 |
Figure 1 Extrapolated prevalence of benzodiazepine use in the Swiss adult population by sex and age in 2018. |
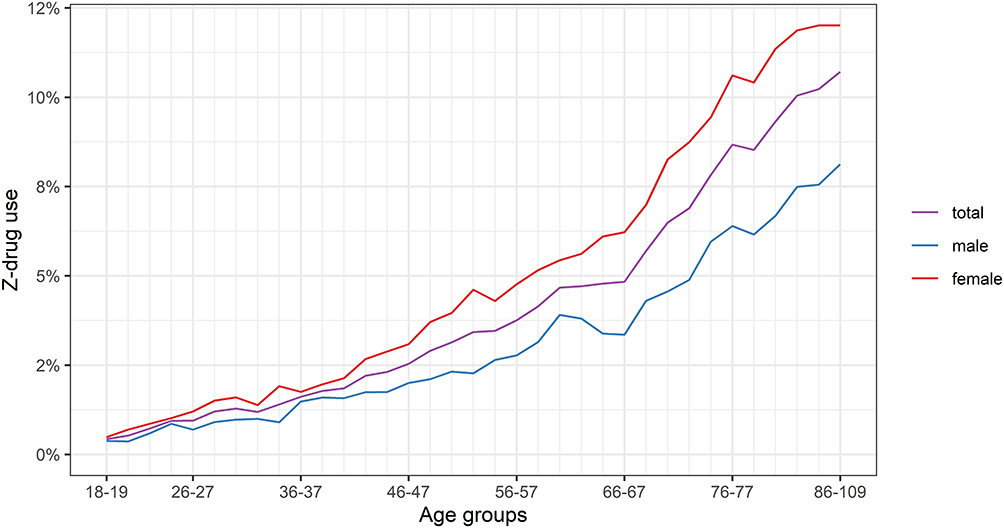 |
Figure 2 Extrapolated prevalence of Z-drug use in the Swiss adult population by sex and age in 2018. |
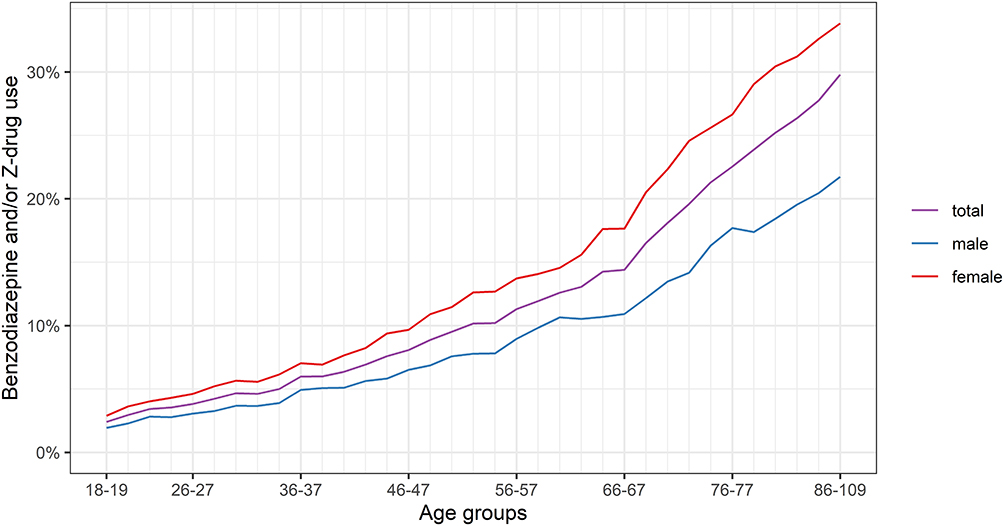 |
Figure 3 Extrapolated prevalence of benzodiazepine and/or Z-drug use in the Swiss adult population by sex and age in 2018. |
The unadjusted and the extrapolated prevalence increased continuously with age in all medication groups (Figures 1–3, Table 1). The mean age in the unadjusted medication groups was between 63.0 years (standard deviation, SD: 18.4) in the benzodiazepine group, 63.7 years (SD: 18.2) in benzodiazepine and/or Z-drug group and 65.5 years (SD: 17.2) in the Z-drug group (Table 1). A prevalence of about 30% was found in the middle-aged group “45–64 years” for all three medication groups (30.4% for benzodiazepines, 29.9% for Z-drugs, and 30.1% for benzodiazepines and/or Z-drugs). Over 50% of the patients aged ≥65 years received at least one prescription in the three medication groups (51.9% for benzodiazepines, 56.9% for Z-drugs and 53.5% for benzodiazepines and/or Z-drugs). In the age group “18–24 years” up to the age group “45–54 years” the prevalence of benzodiazepine prescription was higher than the prevalence of Z-drug prescription. From the age group “55–64 years” up to the age group “≥85 years” the prevalence of Z-drug prescription was higher than the prevalence of benzodiazepine prescription.
In the German-speaking part, the prevalence of prescription in the three medication groups was remarkably higher (62.4% for benzodiazepines, 66.8% for Z-drugs, and 64.5% for benzodiazepines and/or Z-drugs) than in the French-speaking part (25.6% for benzodiazepines, 26.3% for Z-drugs, and 24.9% for benzodiazepines and/or Z-drugs) and the Italian speaking part (12.0% for benzodiazepines, 6.9% for Z-drugs, and 10.6% for benzodiazepines and/or Z-drugs; Table 1). In all medication groups, almost 90% of the medication users lived in an urban region (88.4% for benzodiazepines, 87.8% for Z-drugs, and 88.1% for benzodiazepines and/or Z-drugs). Additionally, more than half of the patients were enrolled in a managed care model (56.5% for benzodiazepines, 56.7% for Z-drugs, 56.9% for benzodiazepines and/or Z-drugs, which is less than in non-user groups. In almost two thirds of all cases persons with ≥3 comorbidities had a benzodiazepine and/or Z-drug prescription (58.6% for benzodiazepines, 63.0% for Z-drugs, and 58.6% for benzodiazepines and/or Z-drugs).
Number of Prescriptions and Provider
In all medication groups, the highest proportion of medication users received only one prescription (48.8% for benzodiazepines only, 35.8% for Z-drugs only, and 41.0% for benzodiazepines and/or Z-drugs; Table 2). However, the group with the second-highest proportion were users with ≥6 prescriptions in 1 year (23.1% for benzodiazepines only, 35.2% for Z-drugs only, and 30.1% for benzodiazepines and/or Z-drugs). The prevalence of ≥6 prescriptions was higher in the Z-drugs only group than in the benzodiazepines only group (35.2% vs 23.1%, respectively).
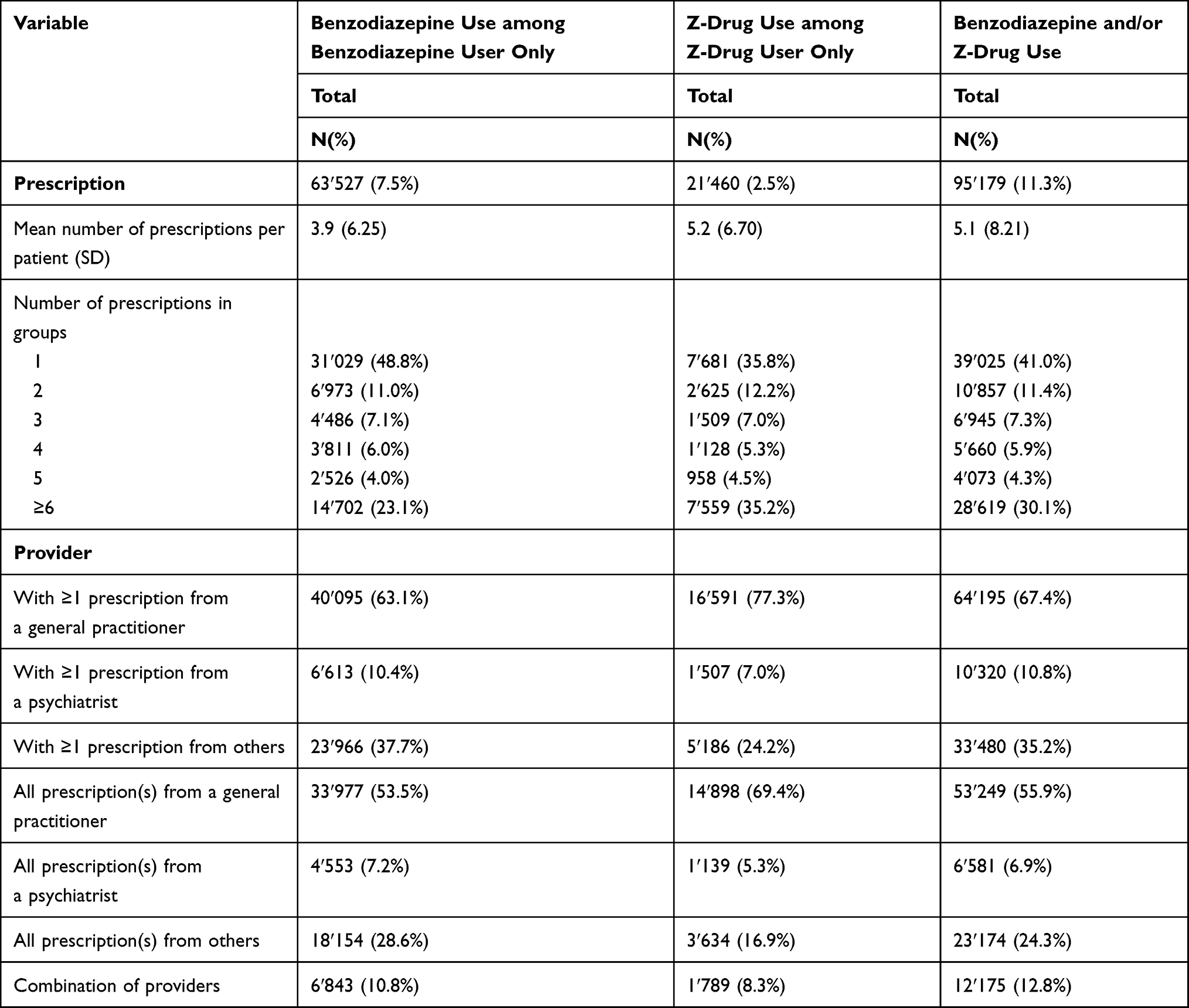 |
Table 2 Number of Prescriptions and Prescription by Type of Provider among Benzodiazepine and Z-Drug User in 2018 |
The mean number of prescriptions per patient in 2018 was 3.9 (SD: 6.3) for benzodiazepines only, 5.2 (SD: 6.7) for Z-drugs only, and 5.1 (SD: 8.2) for benzodiazepines and/or Z-drugs: Table 2). In all medication groups, more than two-thirds of all users had at least one prescription from a general practitioner (63.1% for benzodiazepines only, 77.3% for Z-drugs only, and 67.4% for benzodiazepines and/or Z-drugs) and a majority had all prescriptions from a general practitioner (53.5% for benzodiazepines only, 69.4% for Z-drugs only and 55.9% for benzodiazepines and/or Z-drugs). 10.8% of benzodiazepine users, 8.3% of Z-drug users, and 12.8% of benzodiazepine and/or Z-drug users had a combination of providers.
Type of Benzodiazepines (Short and Long Acting)
About 86% of the patients used short-acting benzodiazepines only, 9.9% long-acting benzodiazepines only, and 4.0% a combination of short- and long-acting benzodiazepines in 2018 (Table S1). The proportion of females was in the short-acting group 65.9%, in the long-acting group 59.0%, and in the combined group 62.3%. About 55% of the patients using short-acting benzodiazepines only had ≥3 comorbid diseases, 58% among long-acting users and 74.5% among those using short- and long-acting agents combined.
The mean number of prescriptions per patient was 4.5 (SD: 6.5) among long-acting benzodiazepines only users, 3.5 (SD: 5.3) among short-acting benzodiazepines only users, and 11.8 (SD:13.9) among short- and long-acting users within 1 year (Table 3). Among both the short- and long-acting benzodiazepine users, the majority of patients had at least one prescription (short-acting: 51.4%; long-acting: 43.1%). In the group using short- and long-acting benzodiazepine combined, 60.0% of the patients had equal or more than six prescriptions per year.
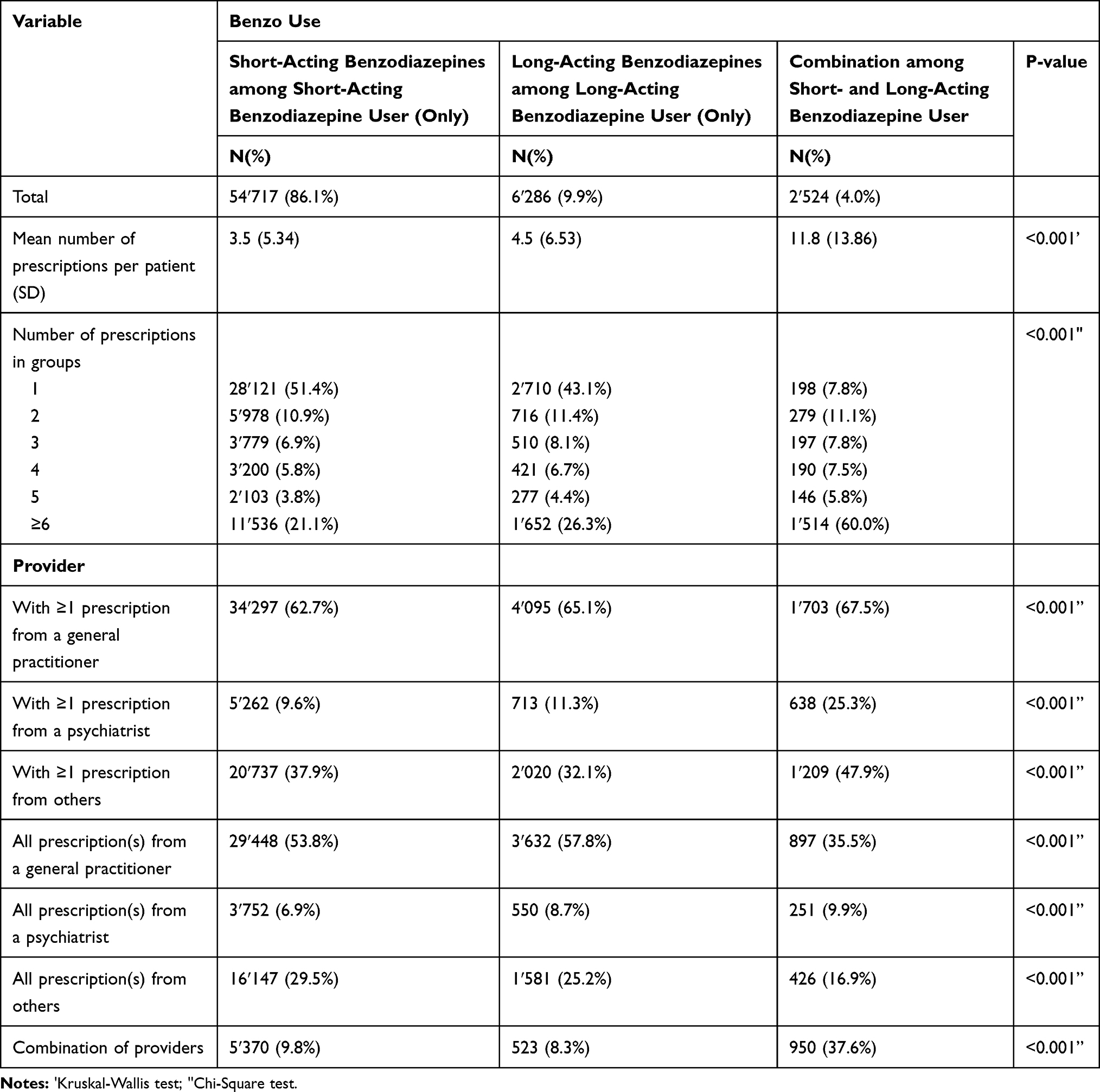 |
Table 3 Number of Prescriptions and Prescription by Type of Provider among Benzodiazepine Short- and Long-Acting User in 2018 |
The main provider was a general practitioner with 62.7% for users of short-acting benzodiazepines only, 65.1% for those of long-acting benzodiazepines only, and 67.5% for combined users of short- and long-acting benzodiazepine (Table 3). A combination of different providers was used most among patients with short- and long-acting benzodiazepines with 37.6%, compared to 9.8% among those with short-acting benzodiazepines, and 8.3% among patients with long-acting benzodiazepines.
Adverse Health Care Outcome
In the three medication groups, patients with at least one prescription were more likely to be admitted to acute care than without respective drug prescription (OR: 1.21, 95%-CI: 1.19–1.23 for benzodiazepine and/or Z-drug prescription; Tables S2–S4).
Patients with at least one prescription were also more likely to be admitted to psychiatry (OR: 6.23, 95%-CI: 5.85–6.63 for benzodiazepine and/or Z-drug prescription). The highest likelihood of admission to a psychiatric hospital had patients with a prescription in the age group 18–24 (OR: 12.13, 95%-CI: 10.68–13.77 for benzodiazepine and/or Z-drug prescription), compared to patients in the age group “64–75 years”. This trend continues to be up to the age group “55–65 years”, but with steadily decreasing frequency. Patients aged “75–84 years” and “≥85 years” had the highest likelihood to enter acute care, rehabilitation, or nursing home in all three medication groups. The likelihood to be admitted to a nursing home was especially high for patients aged ≥85 years (OR: 21.93, 95%-CI: 20.61–23.33 for benzodiazepine and/or Z-drug prescription) (reference group “64–75 years”). The odds of admission to rehabilitation or nursing home were higher in all three groups with a prescription than without respective drug prescriptions.
Women with a prescription were more likely to be admitted to acute care than men with a prescription in all three medication groups (OR: 1.09, 95%-CI 1.07–1.10 benzodiazepine and/or Z-drugs) and they were also more likely to be hospitalized in a nursing home than men (OR: 1.51, 95%-CI 1.45–1.57 for benzodiazepines and/or Z-drugs).
The likelihood of admission in acute care, psychiatry, rehabilitation, or nursing home was higher for all patients with comorbidities who had a prescription for benzodiazepines and/or Z-drugs than patients without any comorbidities. The probability was notably higher to enter a rehabilitation facility for a person with ≥3 comorbidities than for a person without comorbidities (OR: 18.04, 95%-CI 15.87–20.52 for benzodiazepines and/or Z-drugs). The results of the logistic regression models for benzodiazepines and Z-drug prescription separately did not significantly differ from the results of the combined drug classed and are also shown in Tables S2–S4.
Discussion
This population-based cross-sectional study is the first to systematically investigate the use and prescription patterns of benzodiazepines and/or Z-drugs as well its associations with different adverse healthcare outcomes in Switzerland using nationwide claims data. There were three main findings of this study. First, the extrapolated prevalence of use was remarkably high in 2018, ranging from 3.5% for Z-drugs, 8.1% for benzodiazepines to 10.5% for benzodiazepines and/or Z-drugs in Switzerland. Second, analyzing prescription patterns revealed that the main provider was a general practitioner and that a small but remarkable proportion of drug users had ≥6 prescriptions in 1 year. Third, receiving a prescription for a benzodiazepine and/or a Z-drug was strongly associated with a higher likelihood of various adverse health care outcomes.
Our findings of the remarkable high prevalence of drug use are comparable with previous research.11,14,15 International studies showed a prevalence between 2.06% and 7.5% in the general population.5,11,12 Among adults aged 65 years and older, a Swiss study including data from nine of the 26 cantons of Switzerland found a prevalence of about 20% of users with at least one prescription for a benzodiazepine, with a higher prevalence for women than men.14 This is in line with international studies showing also that older age groups were consistently having higher prescription rates, ranging from 8.7% to 21.5%, than younger age groups.33–36 This finding is of critical importance, especially when considering the classification of benzodiazepines and Z-drugs as potentially inappropriate medication in the elderly on the PRISCUS List (an overview of unsuitable medications in older age groups and recommendations for alternatives), due to an increased risk of adverse drug events in this patient group.37 The authors of the PRISCUS List make no distinction between short- and long-acting benzodiazepines and warn against both benzodiazepine types in the elderly. Additionally, our findings are also in line with previous research showing a higher prevalence of prescription among women.11,14,38–41 This higher prevalence of use for women can be partly explained by the association of poor sleep and insomnia with menopause.42 This correlates with our finding of a remarkable prevalence difference for men and women around perimenopausal age. Another possible explanation is that men are less likely than women to seek help from health care providers for mood and anxiety disorders.43
We found that the main prescription provider was a general practitioner, which is consistent with previous research.12,34,44,45 Our finding that 8.3% to 12.8% of users had a combination of providers, is comparable with other study findings showing that 12.7% had two or more providers in 1 year.46 This is very crucial, as a combination of providers can result in a loss of control over the number of prescriptions and, thus, potentially provide incentives for substance abuse, dependence and drug interactions. This problem is especially known as the so-called phenomenon of “doctor shopping”, defined as seeing multiple prescribers, often under false pretenses and care-seeking behavior.47,48 Additionally, we found that the largest proportion of users received only one prescription, but the second-largest group, interestingly, was the group with ≥6 prescriptions with a prevalence of 23.1% to 35.2%. This finding is in line with previous studies showing that long-term use of benzodiazepine and/or Z-drugs is common, even though the existing guidelines are clearly against long-term treatment.7,8,35,45,46 We assume that the guidelines are very challenging to implement and insufficiently practicable in their current form. The discontinuation of such therapy could impact the physician–patient relationship, one of the main pillars of medicine, negatively. There are concerns about whether an end of the therapy will be successful.49,50 Furthermore, general practitioners reported insufficient knowledge and confidence in the provision and use of alternative psychological therapies in the management of insomnia.51
Due to changes in pharmacokinetics and pharmacodynamics resulting from older age, the risk of benzodiazepine side effects increases in the elderly and is especially related to long-acting agents (eg sedation, psychomotor disorders).52 This qualifies long-acting benzodiazepines as a potentially inappropriate medication in the elderly.37 In our study, the vast majority of users with a benzodiazepine prescription had a prescription for a short-acting benzodiazepine, only about one-tenth had a prescription for a long-acting benzodiazepine. Our prevalence finding is lower than in the previous international research, where around one-quarter had a prescription for a long-acting benzodiazepine agent.11,13 A recent study found a prevalence of 25% for long-acting agents, 67.7% for intermediate-acting benzodiazepine agents and 7.4% for short-acting benzodiazepine agents in the elderly in Switzerland.14 One potential explanation for this difference can be the classification of benzodiazepines as intermediate-acting agents in the study, as we used a long-and short-acting definition for benzodiazepines in our study.
In our analysis, we found a higher likelihood of admission in acute care, psychiatry, rehabilitation, and a nursing home in individuals with at least one benzodiazepine prescription compared to non-users. This can partly be explained by the various side effects and withdrawal symptoms that come with the use of a benzodiazepine and/or a Z-drug. Previous research also found that benzodiazepine recipients were higher users of medical care, had more emergency department visits, and were hospitalized more frequently.53,54 In a Swiss study analyzing emergency department presentations for symptoms consistent with acute toxicity, the most frequently reported drugs were benzodiazepines.55 Previous research found an influence on balance during nighttime awakening with Z-drug use and it was stated multiple times that the use of benzodiazepine and/or Z-drugs correlates with increased risk of falls.56–59 Various studies showed an association of benzodiazepine and/or Z-drug use with cognitive decline in the elderly.22–24 An elevated risk for the development of Alzheimer’s is being discussed, but the findings of the according studies are not conclusive.60–62
The likelihood for hospitalization in a psychiatric facility was especially high among the youngest age group (18–24 years) and decreased within older age groups. This could be partly explained as benzodiazepines are often used in the treatment of psychiatric disorders treated in psychiatric facilities.63 A recent study found that among individuals with a benzodiazepine prescription aged 0–24 years (with the highest prevalence clearly in young adults), 45.3% had a record of a psychiatric disorder diagnosed within 6 months of benzodiazepine dispensation. The most common diagnoses were anxiety and depression.64 The lowering likelihood for psychiatric hospitalization in the elderly can partly be explained by the finding that the prevalence of anxiety disorders declines with older age compared to younger age groups.65
Strengths and Limitations
This study has several strengths and limitations. The main strength of our study is the nationwide claims-based approach which allows us to provide a nationwide overview of the prescription prevalence of benzodiazepines and/or Z-drugs and its effect on healthcare outcomes in Swiss adults. Moreover, we were able to calculate representative results in the general population, since estimates were additionally extrapolated to the Swiss population-based on federal data.
This study has also several limitations. We have no information on the reasons for a benzodiazepine and/or Z-drug prescription by using health insurance claims data since medical diagnoses are not systematically recorded in the Swiss ambulatory setting. Additionally, we defined comorbid chronic conditions by prescriptions related to those conditions, which represent proxies for medical diagnoses. Further, the number of prescriptions might be slightly underestimated since about 3% of the entire claims were not reimbursed and paid out-of-pocket by the patients. On the other hand, based on prescription data, we are not able to evaluate the actual medication intake, which can lead to an overestimation of the actual drug intake. Additionally, our database has some minor differences in sex, age and region and is, therefore, not entirely representative of the Swiss population. As we used extrapolated claims data, our results represent an approximation of the real number of users. However, a large dataset was included, which was based on data of one of the largest health insurance companies, which covers a total of 1.18 million residents, about 14% of the Swiss population in 2018. Furthermore, even though we found an association between benzodiazepine and/or Z-drug prescription with adverse health care outcomes, we are not able to state a causal effect.
Conclusion
This study is the first to give a nationwide overview of the current use of benzodiazepines and Z-drugs in Switzerland based on health insurance claims data. The results revealed a remarkably high prevalence among the general Swiss population, especially in older generations. Furthermore, we found a significant association between benzodiazepine and/or Z-drugs use, and several adverse health care outcomes, which reflects that the negative consequences of BZ and ZD use are a crucial public health problem. Further efforts should be focused on establishing alternative therapies.
Disclosure
Dr Eva Blozik reports personal fees from Swiss National Fonds, during the conduct of the study; grants from MSD, Amgen, Novartis Pharma, and Vifor, outside the submitted work. Mr Beat Brüngger reports grants from MSD Merck Sharp & Dohme AG (Switzerland), Vifor Pharma (Switzerland), and Swiss National Science Foundation (SNSF), outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Mihic SJ, Mayfield J, Harris RA. Hypnotics and sedatives. In: Brunton LL, Hilal-Dandan R, Knollmann BC, editors. Goodman & Gilman’s: The Pharmacological Basis of Therapeutics.
2. Lader MH. Limitations on the use of benzodiazepines in anxiety and insomnia: are they justified? Eur Neuropsychopharmacol. 1999;9:S399–S405. doi:10.1016/S0924-977X(99)00051-6
3. Hollingworth SA, Siskind DJ. Anxiolytic, hypnotic and sedative medication use in Australia. Pharmacoepidemiol Drug Saf. 2010;19(3):280–288. doi:10.1002/pds.1899
4. Hwang SH, Han S, Choi H, Park C, Kim SM, Kim TH. Trends in the prescription of benzodiazepines for the elderly in Korea. BMC Psychiatry. 2017;17(1):303. doi:10.1186/s12888-017-1467-z
5. Li C, Santaella-Tenorio J, Mauro PM, Martins SS. Past-year use of prescription opioids and/or benzodiazepines among adults in the United States: estimating medical and nonmedical use in 2015–2016. Drug Alcohol Depend. 2019;204:107458. doi:10.1016/j.drugalcdep.2019.04.029
6. Tardelli VS, Fidalgo TM, Santaella J, Martins SS. Medical use, non-medical use and use disorders of benzodiazepines and prescription opioids in adults: differences by insurance status. Drug Alcohol Depend. 2019;204:107573. doi:10.1016/j.drugalcdep.2019.107573
7. Schweizerische Fachgesellschaft für Geriatrie [homepage on the Internet]. Bern: Benzodiazepine nur in Ausnahmefällen [Benzodiazepines only in exceptional cases]. Smarter medicine - choosing wisely Switzerland. Available from: https://www.smartermedicine.ch/de/datensammlung/detail/empfehlung/fachperson/17.html.
8. By the 2019 American Society Beers Criteria® Update Expert Panel. American geriatrics society 2019 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;67(4):674–694. doi:10.1111/jgs.15767
9. Riemann D, Baglioni C, Bassetti C, et al. European guideline for the diagnosis and treatment of insomnia. J Sleep Res. 2017;26(6):675–700. doi:10.1111/jsr.12594
10. Murrough JW, Yaqubi S, Sayed S, Charney DS. Emerging drugs for the treatment of anxiety. Expert Opin Emerg Drugs. 2015;20(3):393–406. doi:10.1517/14728214.2015.1049996
11. Olfson M, King M, Schoenbaum M. Benzodiazepine Use in the United States. JAMA Psychiatry. 2015;72(2):136–142. doi:10.1001/jamapsychiatry.2014.1763
12. Akpinar A, Yaman AR, Karakuş K, Atay I, Demirci K. The frequency of benzodiazepine use in the Isparta Province. Klinik Psikofarmakol Bülteni. 2016;26(2):169–174. doi:10.5455/bcp.20150707103818
13. Préville M, Bossé C, Vasiliadis HM, et al. Correlates of potentially inappropriate prescriptions of benzodiazepines among older adults: results from the ESA study. Can J Aging. 2012;31(3):313–322. doi:10.1017/S0714980812000232
14. Luta X, Bagnoud C, Lambiris M, et al. Patterns of benzodiazepine prescription among older adults in Switzerland: a cross-sectional analysis of claims data. BMJ Open. 2020;10(1):e031156. doi:10.1136/bmjopen-2019-031156
15. Petitjean S, Ladewig D, Meier CR, Amrein R, Wiesbeck GA. Benzodiazepine prescribing to the Swiss adult population: results from a national survey of community pharmacies. Int Clin Psychopharmacol. 2007;22(5):292–298. doi:10.1097/YIC.0b013e328105e0f2
16. Gmel G, Kuendig H, Maffli E, et al. Suchtmonitoring Schweiz/Jahresbericht [addiction monitoring Switzerland/annual report]. - daten 2011, Bern 2012. Schweiz, German.
17. Gmel G, Notari L, Gmel C. Suchtmonitoring Schweiz–Einnahme von psychoaktiven und anderen Medikamenten in der Schweiz im Jahr 2012 [addiction monitoring Switzerland – Use of psychoactive and other drugs in Switzerland in 2012]. Sucht Schweiz, Lausanne. Schweiz, German; 2013.
18. Gmel G, Notari L, Gmel C. Suchtmonitoring Schweiz–Vertiefende Analysen zur Einnahme von Schlafmitteln, Beruhigungsmitteln sowie Psychostimulanzien im Jahr 2014 [addiction monitoring Switzerland - in-depth analyses of the use of sleeping pills, tranquilizers and psychostimulants in 2014]. Sucht Schweiz, Lausanne. Schweiz, German; 2015.
19. Gmel G, Notari L, Gmel C. Suchtmonitoring Schweiz–Einnahme von psychoaktiven Medikamenten in der Schweiz im Jahr 2015 [addiction monitoring Switzerland – Intake of psychoactive drugs in Switzerland in 2015]. Sucht Schweiz, Lausanne. Schweiz, German; 2016.
20. Gmel G, Notari L, Gmel C. Suchtmonitoring Schweiz–Einnahme von psychoaktiven Medikamenten in der Schweiz im Jahr 2016 [addiction monitoring Switzerland – Intake of psychoactive drugs in Switzerland in 2016]. Sucht Schweiz, Lausanne. Schweiz, German; 2018.
21. Bierman EJM, Comijs HC, Gundy CM, Sonnenberg C, Jonker C, Beekman ATF. The effect of chronic benzodiazepine use on cognitive functioning in older persons: good, bad or indifferent? Int J Geriatr Psychiatry. 2007;22(12):1194–1200. doi:10.1002/gps.1811
22. Wu C-S, Wang S-C, Chang IS, Lin K-M. The association between dementia and long-term use of benzodiazepine in the elderly: nested case–control study using claims data. Am J Geriatr Psychiatry. 2009;17(7):614–620. doi:10.1097/JGP.0b013e3181a65210
23. Gomm W, von Holt K, Thomé F, et al. Regular benzodiazepine and Z-substance use and risk of dementia: an analysis of German claims data. J Alzheimers Dis. 2016;54(2):801–808. doi:10.3233/JAD-151006
24. Billioti de Gage S, Bégaud B, Bazin F. Benzodiazepine use and risk of dementia: prospective population based study. BMJ. 2012;345:e6231–e6231. doi:10.1136/bmj.e6231
25. Islam MM, Iqbal U, Walther B, et al. Benzodiazepine use and risk of dementia in the elderly population: a systematic review and meta-analysis. Neuroepidemiology. 2016;47(3–4):181–191. doi:10.1159/000454881
26. Schroeck JL, Ford J, Conway EL, et al. Review of safety and efficacy of sleep medicines in older adults. Clin Ther. 2016;38(11):2340–2372. doi:10.1016/j.clinthera.2016.09.010
27. Yu N-W, Chen P-J, Tsai H-J, et al. Association of benzodiazepine and Z-drug use with the risk of hospitalisation for fall-related injuries among older people: a nationwide nested case-control study in Taiwan. BMC Geriatr. 2017;17(1):140. doi:10.1186/s12877-017-0530-4
28. Nakao M, Sato M, Nomura K, Yano E. Benzodiazepine prescription and length of hospital stay at a Japanese university hospital. Biopsychosoc Med. 2009;3(1):10. doi:10.1186/1751-0759-3-10
29. WHO. Collaborating Centre for Drug Statistics Methodology, Guidelines for ATC Classification and DDD Assignment, 2020. Oslo; 2019.
30. Ashton H. (2002) [homepage on the Internet]. Benzodiazepines: how they work and how to withdraw. The Ashton Manual. Newcastle upon Tyne, England, UK: New Castle University; 2002. Available from: https://benzo.org.uk/index.htm.
31. Bundesamt für Statistik (2019) [homepage on the Internet]. Raumgliederung der Schweiz [regional division of Switzerland]. Gemeindetypologie und Stadt/Land-Typologie; 2019. Available from: https://www.bfs.admin.ch/bfs/de/home/grundlagen/raumgliederungen.assetdetail.9046166.html2019.
32. Huber CA, Szucs TD, Rapold R, Reich O. Identifying patients with chronic conditions using pharmacy data in Switzerland: an updated mapping approach to the classification of medications. BMC Public Health. 2013;13(1):1030. doi:10.1186/1471-2458-13-1030
33. Lagnaoui R, Depont F, Fourrier-Réglat A, et al. Patterns and correlates of benzodiazepine use in the French general population. Eur J Clin Pharmacol. 2004;60(7):523–529. doi:10.1007/s00228-004-0808-2
34. Donato F, Samani F, Marini M, et al. Across-sectional survey on benzodiazepine use among older people in an Italian region. Ital J Public Health. 2005;2.
35. Egan M, Moride Y, Wolfson C, Monette J. Long-term continuous use of benzodiazepines by older adults in Quebec: prevalence, incidence and risk factors. J Am Geriatr Soc. 2000;48(7):811–816. doi:10.1111/j.1532-5415.2000.tb04758.x
36. Bachhuber MA, Hennessy S, Cunningham CO, Starrels JL. Increasing benzodiazepine prescriptions and overdose mortality in the United States, 1996–2013. Am J Public Health. 2016;106(4):686–688. doi:10.2105/AJPH.2016.303061
37. Holt S, Schmiedl S, Thürmann PA. Potentially inappropriate medications in the elderly: the PRISCUS list. Dtsch Arztebl. 2010;107(131–132):543.
38. Verthein U, Buth S, Holzbach R, Neumann-Runde E, Martens MS. Benzodiazepine und Z-substanzen - Analyse der kassenärztlichen Verschreibungen von 2006 bis 2015. Psychiatr Prax. 2019;46(7):399–405. doi:10.1055/a-0961-2371
39. Sonnenberg CM, Bierman EJ, Deeg DJ, Comijs HC, van Tilburg W, Beekman AT. Ten-year trends in benzodiazepine use in the Dutch population. Soc Psychiatry Psychiatr Epidemiol. 2012;47(2):293–301. doi:10.1007/s00127-011-0344-1
40. Kassam A, Patten SB. Hypnotic use in a population-based sample of over thirty-five thousand interviewed Canadians. Popul Health Metr. 2006;4(1):15. doi:10.1186/1478-7954-4-15
41. Fourrier-Réglat A, Letenneur L, Dartigues J, Moore N, Begaud B. Benzodiazepine use in an elderly community-dwelling population. Eur J Clin Pharmacol. 2001;57(5):419–425. doi:10.1007/s002280100326
42. Nowakowski S, Meliska CJ, Fernando Martinez L, Parry BL. Sleep and menopause. Curr Neurol Neurosci Rep. 2009;9(2):165–172. doi:10.1007/s11910-009-0025-6
43. Susukida R, Mojtabai R, Mendelson T. Sex differences in help seeking for mood and anxiety disorders in the national comorbidity survey-replication. Depress Anxiety. 2015;32(11):32. doi:10.1002/da.22366
44. Cascade E, Kalali AH. Use of benzodiazepines in the treatment of anxiety. Psychiatry. 2008;5(9):21–22.
45. Jacob L, Rapp MA, Kostev K. Long-term use of benzodiazepines in older patients in Germany: a retrospective analysis. Ther Adv Psychopharmacol. 2017;7(6–7):191–200. doi:10.1177/2045125317696454
46. Neutel C. The epidemiology of long-term benzodiazepine use. Int Rev Psychiatry. 2005;17(3):189–197. doi:10.1080/09540260500071863
47. Ong MS, Olson KL, Cami A, et al. Provider patient-sharing networks and multiple-provider prescribing of benzodiazepines. Int J Gen Med. 2016;31(2):164–171. doi:10.1007/s11606-015-3470-8
48. Worley J, Hall JM. Doctor shopping: a concept analysis. Res Theory Nurs Pract. 2012;26(4):
49. Cook J, Marshall R, Masci C, Coyne J. Physicians’ perspectives on prescribing benzodiazepines for older adults: a qualitative study. J Gen Intern Med. 2007;22(3):303–307. doi:10.1007/s11606-006-0021-3
50. Cook J, Biyanova T, Masci C, Coyne J. Older patient perspectives on long-term anxiolytic benzodiazepine use and discontinuation: a qualitative study. J Gen Intern Med. 2007;22(8):1094–1100. doi:10.1007/s11606-007-0205-5
51. Everitt H, McDermott L, Leydon G, Yules H, Baldwin D, Little P. GPs’ management strategies for patients with insomnia: a survey and qualitative interview study. Br J Gen Pract. 2014;64(619):e112–9. doi:10.3399/bjgp14X677176
52. Madhusoodanan S, Bogunovic OJ. Safety of benzodiazepines in the geriatric population. Expert Opin Drug Saf. 2004;3(5):485–493. doi:10.1517/14740338.3.5.485
53. Alvarenga J, Loyola Filho A, Firmo J, Lima-Costa M, Uchoa E. A population based study on health conditions associated with the use of benzodiazepines among older adults (The Bambui health and aging study). Cad Saude Publica. 2009;25:605–612. doi:10.1590/S0102-311X2009000300015
54. Kroll D, Reyes Nieva H, Barsky A, Linder J. Benzodiazepines are prescribed more frequently to patients already at risk for benzodiazepine-related adverse events in primary care. J Gen Intern Med. 2016;31(9):31. doi:10.1007/s11606-016-3740-0
55. Scholz I, Schmid Y, Exadaktylos A, Haschke M, Liechti M, Liakoni E. Emergency department presentations related to abuse of prescription and over-the-counter drugs in Switzerland: time trends, sex and age distribution. Swiss Med Wkly. 2019;149:149. doi:10.4414/smw.2019.20056
56. Frey D, Ortega J, Wiseman C, Farley C, Wright K. Influence of zolpidem and sleep inertia on balance and cognition during nighttime awakening: a randomized placebo-controlled trial. J Am Geriatr Soc. 2011;59(1):73–81. doi:10.1111/j.1532-5415.2010.03229.x
57. Finkle W, Der J, Greenland S, et al. Risk of fractures requiring hospitalization after an initial prescription for zolpidem, alprazolam, lorazepam, or diazepam in older adults. J Am Geriatr Soc. 2011;59(10):1883–1890. doi:10.1111/j.1532-5415.2011.03591.x
58. Lai -M-M, Lin -C-C, Lin -C-C, Liu C-S, Li T-C, Kao C-H. Long-term use of zolpidem increases the risk of major injury: a population-based cohort study. Mayo Clin Proc. 2014;89(5):89. doi:10.1016/j.mayocp.2014.01.021
59. Markota M, Rummans TA, Bostwick JM, Lapid MI. Benzodiazepine use in older adults: dangers, management, and alternative therapies. Mayo Clin Proc. 2016;91(11):1632–1639. doi:10.1016/j.mayocp.2016.07.024
60. Imfeld P, Bodmer M, Jick SS, Meier CR. Benzodiazepine use and risk of developing alzheimer’s disease or vascular dementia: a case–control analysis. Drug Saf. 2015;38(10):909–919. doi:10.1007/s40264-015-0319-3
61. Biétry FA, Pfeil AM, Reich O, Schwenkglenks M, Meier CR. Benzodiazepine use and risk of developing alzheimer’s disease: a case-control study based on Swiss claims data. CNS Drugs. 2017;31(3):245–251. doi:10.1007/s40263-016-0404-x
62. Billioti de Gage S, Moride Y, Ducruet T. Benzodiazepine use and risk of Alzheimer’s disease: case-control study. BMJ. 2014;349:g5205–g5205. doi:10.1136/bmj.g5205
63. Panes A, Fourrier-Réglat A, Verdoux H, Tournier M. Usages et mésusages des benzodiazépines chez les patients souffrant de troubles psychiatriques [Use and misuse of benzodiazepines in patients with psychiatric disorders]. Presse Med. 2018;47(10):886–891. doi:10.1016/j.lpm.2018.10.003
64. Sidorchuk AA-O, Isomura K, Molero YA-O, et al. Benzodiazepine prescribing for children, adolescents, and young adults from 2006 through 2013: a total population register-linkage study. PLoS Med. 2018;15(8):e1002635. doi:10.1371/journal.pmed.1002635
65. Wolitzky-Taylor KB, Castriotta N, Lenze EJ, Stanley MA, Craske MG. Anxiety disorders in older adults: a comprehensive review. Depress Anxiety. 2010;27(2):190–211. doi:10.1002/da.20653
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.