")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Behavioral Response to HIV/AIDS Prevention Messages Among Students in Selected Universities of Amhara Region, Northwest Ethiopia: An Extended Parallel Process Model
Authors Afenigus AD , Mulugeta H , Tsehay B, Gedfew M , Ayenew T , Getnet A
Received 5 November 2020
Accepted for publication 30 December 2020
Published 2 February 2021 Volume 2021:13 Pages 115—124
DOI https://doi.org/10.2147/HIV.S288297
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Abebe Dilie Afenigus,1 Henok Mulugeta,1 Binalfew Tsehay,2 Mihretie Gedfew,1 Temesgen Ayenew,1 Asmamaw Getnet1
1Department of Nursing, College of Health Sciences, Debre Markos University, Debre Markos, Gojjam, Ethiopia; 2Department of Biomedical Sciences, School of Medicine, Debre Markos University, Debre Markos, Ethiopia
Correspondence: Abebe Dilie Afenigus
Department of Nursing, College of Health Sciences, Debre Markos University, PO Box 269, Debre Markos, Gojjam, Ethiopia
Email [email protected]
Background: HIV/AIDS is a global pandemic. Sub-Saharan Africa accounts for two-thirds of the newly HIV-infected cases in the world. Similarly, the prevalence of HIV infections among Ethiopian university students has also increased as HIV prevention was not sufficiently prioritized. In order to decrease the surge of the HIV pandemic, prevention messages that encourage individuals to reduce sexual and risk behaviors still remain a key intervention strategy. Besides this, the behavioral response to HIV prevention messages among Ethiopian universities is not well studied.
Objective: To assess students’ behavioral response to HIV/AIDS prevention messages in selected universities of the Amhara region using an extended parallel process model (EPPM), in 2019.
Methods: A facility-based cross-sectional study was employed among 423 eligible students from January to February, 2019 using a stratified sampling technique. The dependent variable is response to HIV/AIDS prevention messages (danger control and fear control) which is addressed by EPPM. The model explains the components of threat (perceived susceptibility and perceived severity) and efficacy (response efficacy and self-efficacy). Subtracting wings of threat component score from efficacy wings score gives the critical value. If the critical value had positive scores, it showed responses of danger control; if the critical value was negative, it showed response of fear control. A logistic regression model was fitted to assess the association between the dependent and independent variables.
Results: The response rate of this study was 94.6%. Among 400 respondents, 263 (65.8%; 95%CI: 61– 70) of them were in the danger control response whereas 137 (34.2%; 95%CI: 30– 39) were in fear control response. Moreover, 200 (50%) of the participants had adequate knowledge and 180 (45%) had a favorable attitude towards HIV/AIDS prevention messages. Danger control response for HIV prevention messages was higher among first-year students (AOR=5.5; 95%CI: 1.5– 19) and third-year students (AOR=3.9; 95%CI: 2– 14) compared with fifth-year students. Similarly, those students who reside on the campus were 60% times less likely to develop danger control when compared with students who live with their family (AOR=0.4; 95%CI: 0.2– 0.9). Besides this, students who had adequate knowledge (AOR=2.6; 95%CI: 1.5– 4.5) and students who receive fear-inducer messages (AOR=4.5; 95%CI: 3– 25] were more likely to develop danger control responses.
Conclusion and Recommendation: Nearly two-thirds of the participants were in the danger control response. Year of study, with whom students currently live, type of message they received, and the knowledge level of respondents were the factors associated with students’ response to HIV/AIDS prevention messages. Therefore, the messages must aim at enhancing threat component perception with appropriate efficacy messages to control danger and promote behavioral change.
Keywords: behavioral response, HIV prevention messages, extended parallel process model
Introduction
HIV destroys the CD4 cells and consequently, the body is exposed to conditions called opportunistic infections. An estimated 1.7 million and 37.9 million individuals were newly infected and live with HIV, respectively in the world by 2018.1,2
HIV/AIDS is one of the pandemics that are distributed all over the world. The pandemic has affected all regions of the globe although there are variations among regions on the level of burden of the pandemic. Around 25.6 million people were living with HIV in Sub-Saharan Africa. Sub-Saharan Africa, which is the hardest-hit region worldwide, accounts for two-thirds of the newly HIV infected cases in the world. Although a couple of countries have achieved a decline in new HIV infections among adults, most countries have not made significant progress, and yet others have experienced worrying surges in HIV infection. For instance, individuals who acquire new HIV infections in Ethiopia has increased because HIV prevention was not sufficiently prioritized.3–5
AIDS has become one of the most serious threats to life, education, social, and economic progress of nations and causes significant individual morbidity and mortality. Among AIDS-associated mortality around the globe, the majority (70%) resided in the African region. In Ethiopia, HIV/AIDS-related mortality among the youth population was 34% and it also accounted for 66% of all deaths in the reproductive age-group of urban dwellers. Consistent with the EDHS 2016, the national HIV prevalence is 0.9%; of this, the urban prevalence was 2.9% whereas the rural prevalence is 0.4%. The prevalence varies from region to region. The annual new HIV infection proportion by regions in Ethiopia within the same year is highest (26%) within the Amhara region.6,7
Many studies demonstrated a high prevalence of HIV seropositivity among Ethiopian university students with a prevalence of 1.2%, 14.5%, 12.5%, and 3.8% for Bahir Dar, Dire Dawa, Jimma, and St Mary's Universities respectively.8–11
In Africa, the susceptibility of university students to HIV/AIDS is due to high mating prevalence, inconsistent and incorrect condom utilization, and sexual promiscuity.12 As a result of substance use, living far from family without supervision, and sexual activity, university students in Ethiopia are also vulnerable to acquire HIV infection.13
Controlling activities which expose to HIV infection is the focus of HIV infection prevention strategy. If university students get attention to the health threat messages (HIV/AIDS) they received, the subsequent step is delivering methods/solutions to that threat. Delivering fear arousing messages enhance students to focus on strategies of response efficacy and self-efficacy by changing their behavior.14
All countries need to intensify HIV prevention mechanisms to end the AIDS pandemic. Ethiopia has also developed an HIV/AIDS prevention, care, and treatment strategic plan in an investment case approach which is being implemented from 2015–2020. One among the objectives of this plan is to implement high impact and targeted prevention programs through behavior change communication programs, condom distribution and use, prevention and control of sexually transmitted infections, and ensuring blood safety. Therefore, the cheapest HIV prevention activities are also important to realize the possibility of an AIDS-free generation by 2030.3,4
Efficacy beliefs (response efficacy, self-efficacy) and fear of a health threat (severity and susceptibility of threat) combined to form behavioral response can be explained by EPPM. In this model, the receivers (university students) must believe the health threat (HIV/AIDS) as severe (perceived severity). Besides this, the students must feel susceptible/liable to HIV (perceived susceptibility). Subsequently, students should perceive that the suggested activity is efficacious in keeping the health threat (perceived response efficacy). Moreover, the students are able to act based on recommended suggestions/responses (perceived self-efficacy). If perceived threat and efficacy is high among the students, they easily accept the messages and therefore perform the required activity to avoid the threat which is called “danger control”. Alternatively, if the perceived threat is stronger than efficacy, the students might involve in “fear control”. In this case, they avoid fear by reducing the messages rather than preventing the threat. Generally, for a low perceived threat, the students/receivers do not operate the message prior to considering efficacy. This is called “ no response”.15,16
EPPM showed components of threat and efficacy. In EPPM, when people encounter a health threat, they either control the danger or control their fear. Besides this, the model explains threat as the danger to which one feels vulnerable/susceptible to a significant health problem. This threat has two components called susceptibility to threat (the perceived likelihood of experiencing the threat (one’s vulnerability to a treat) and severity of the threat (the degree of harm that would possibly be experienced if a threat is encountered). Efficacy is also explained as the perception that an individual effectively performs the suggested response to avoid a health problem/threat. It has components of response efficacy (the perception of an individual regarding the effectiveness the recommended action to avoid a threat) and self-efficacy (the belief that an individual is able to act based on recommended action).16
Both perception of threat and efficacy can affect an individual behavior. Based on these appraisals, at the end one of the three (no response, a danger control, or fear control) results might occur after providing a message to certain threats in EPPM (Figure 1). Based on EPPM, initially, individuals evaluate the threat of danger. The higher the believed threat; the more inspired individuals start to judge the efficacy of the endorsed response. When individuals view the threat as trivial/insignificant (perceived as low), there is no need to further proceed with the message; with little concern of efficacy and no response made. The level of perception of a certain threat might determine the behavior change of persons.15–17
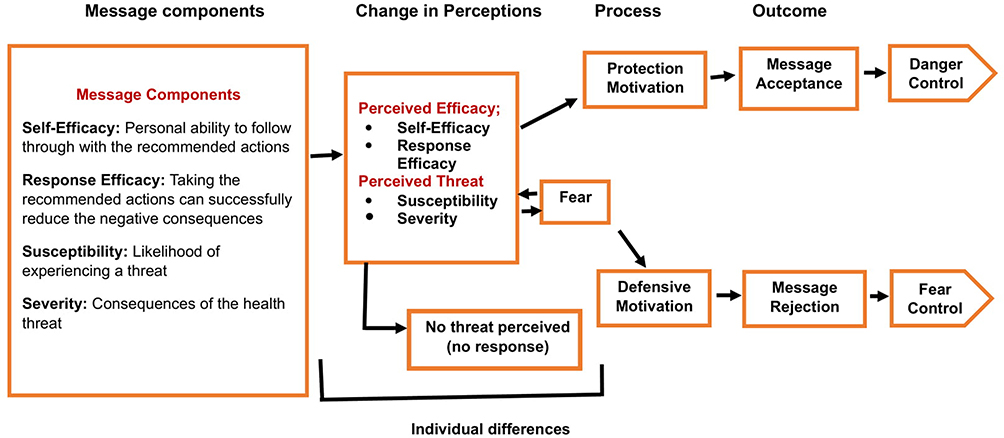 |
Figure 1 Theoretical framework of the extended parallels process model (EPPM). |
Methods
Study Design, Area and Period
A facility-based cross-sectional study design was implemented to assess behavioral response to HIV prevention messages among students in selected universities (Bahir Dar, Injibara and Debre Markos universities) of Amhara region from January to April 2019.
Eligibility Criteria, Sample Size Determination and Sampling Procedure
All regular students in in selected Amhara region universities who were available during data collection period were included in the study. However, students who were unable to communicate were excluded from this study.
Single population proportion formula was used to determine sample size with the assumption of 5% marginal error, 95% confidence interval and by considering proportion (p) of danger control response 48% from study conducted at Hosanna colleges.18 Moreover, by accounting 10% nonresponse rate, 423 eligible students were included in the study. By considering heterogeneity among selected Amhara region universities stratified sampling was used as a sampling technique. Finally, systematic random sampling technique was applied to select students from the registered list at each university after the participants were proportionally allocated to size (Figure 2).
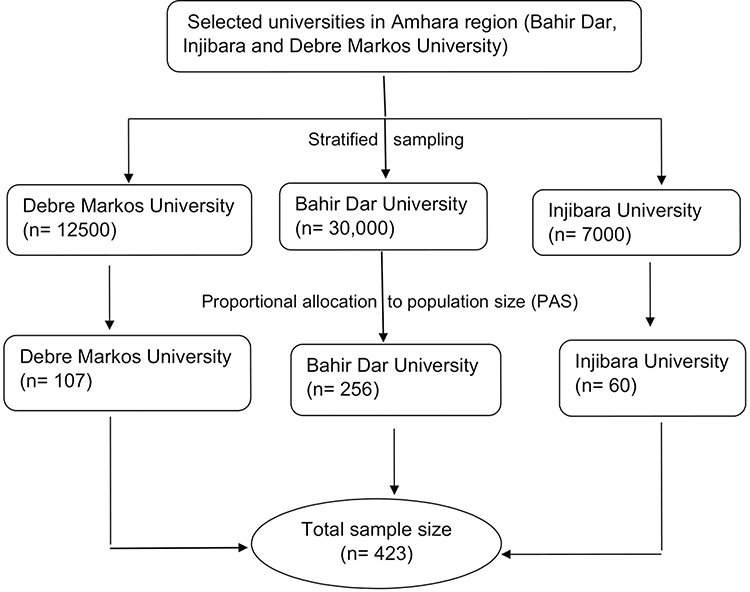 |
Figure 2 Sampling procedure schematic presentations among students in universities, 2019. |
Study Variables and Operational Definitions
The independent variables are sociodemographic variables (age, sex, marital status, religion, residence, and income), message component, individual differences (past sexual behaviors, knowledge and attitude about HIV/AIDS) and distal factors (Preference of source, message and channel) while the outcome variable is behavioral response to HIV prevention messages. In this study, the terms listed below were explained in such a way.
Behavioral Response to HIV/AIDS Prevention Messages
The response is danger control and fear control which is determined by calculating critical value.
Critical Value
Subtracting wings of threat (perceived susceptibility and perceived severity) component score from efficacy wings (response efficacy, self-efficacy) score is the critical value. If the critical value is zero, it indicates no response.
Danger Control
If the critical value had positive scores, it shows responses of danger control (requires threat to inspire with high efficacy messages); When humans perceive they are at-risk for a certain threat such as HIV (ie, high perceived threat), and that they perceive as able to efficaciously prevent it from taking place (ie, high perceived efficacy), they are prompted to control the danger/threat.
Fear Control Responses
If the critical value is negative, it shows response of fear control (require only efficacy messages without threat); if individuals perceive they are in significant risk or threat like HIV/AIDS (ie, high perceived threat), with perceptions of incapable to act the suggested response (ie, low perceived efficacy), then they are prompted to control fear.
Knowledge
Respondents who answered greater than or equal to the mean of knowledge-related questions were categorized as knowledgeable whereas those who answered less than the mean of knowledge-related questions were categorized as having inadequate knowledge.
Attitude
Students who scored above the median were categorized as having favorable attitude while those who scored less than the median score were considered as having an unfavorable attitude.
Data Collection Procedure, Quality Assurance and Analysis
The data were collected by using structured self-administered questionnaire after reviewing literature of comparable research using extended parallel process model.
Data were collected by using the English version questionnaire after carefully designing the tool. Besides this, a pretest was done on 5% of the total sample at Finote Selam teacher’s college. Data collectors, supervisors, and principal investigator checked data for completeness, and data were cleaned, entered into EpiData version 4.2 software, and then exported to Statistical Package and Service Solution (SPSS) version 25 for final analyses.
Percentage and frequency tables were used to describe the data. To identify factors associated with response to HIV prevention messages, bivariate and multivariable logistic regression analyses were conducted. All variables with p-value less than 0.2 on bivariate analyses were entered into multivariable logistic regression analyses to adjust the effects of confounding. Statistical significance was set at p-value less than 0.05 and Hosmer and Lemeshow statistical test was used to test for model fit.
Ethical Considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Ethical clearance was obtained from ethical review committee of Debre Markos University, College of Health Sciences. Participants were informed about the purpose, procedure of data collection, confidentiality, and privacy before the actual data collection. Data were collected after obtaining a verbal informed consent from study participants which is approved by the ethical review committee of Debre Markos University.
Results
Sociodemographic Characteristics
A total of 400/423 eligible students were included in the study with a response rate of 94.6%. Among 400 respondents, 293 (73.2%) were males. Similarly, their age ranged from 19 to 47 years with mean of 27.93 (SD=±6.596) years. Among the students who participate in the study, 370 (92.5%) were single in relationship and 283 (70.8%) were living on campus while attending their education (Table 1).
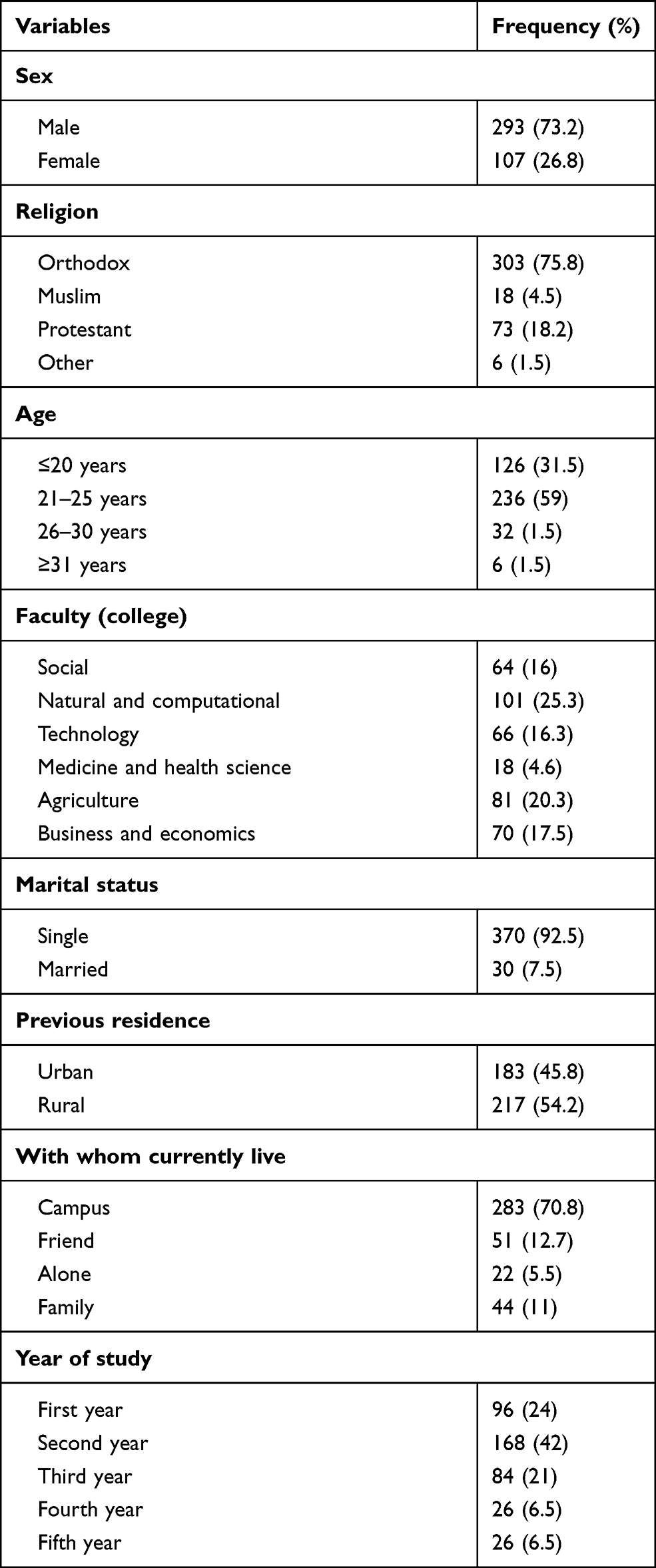 |
Table 1 Sociodemographic Characteristics of Students in Selected Universities, 2019 (n=400) |
Knowledge and Attitude of Students Towards HIV/AIDS Prevention Messages
Eighteen questions that aimed to assess the knowledge of students towards HIV/AIDS were provided to the students (Table 2). Based on the operational definition stated in the methods section, 200 (50%; 95%CI 45.3–55) of were knowledgeable whereas the remaining half of the respondents had inadequate knowledge towards HIV/AIDS prevention messages. Moreover, a total of 10 questions were used to assess attitude of students towards HIV/AIDS prevention (Table 3). Based on the operational definition stated in the methods section, 180 (45%; 95%CI: 39.8–50.2) of the participants had favorable attitude while 220 (55%; 95%CI: 49.8–60.2) had unfavorable attitude toward HIV prevention messages.
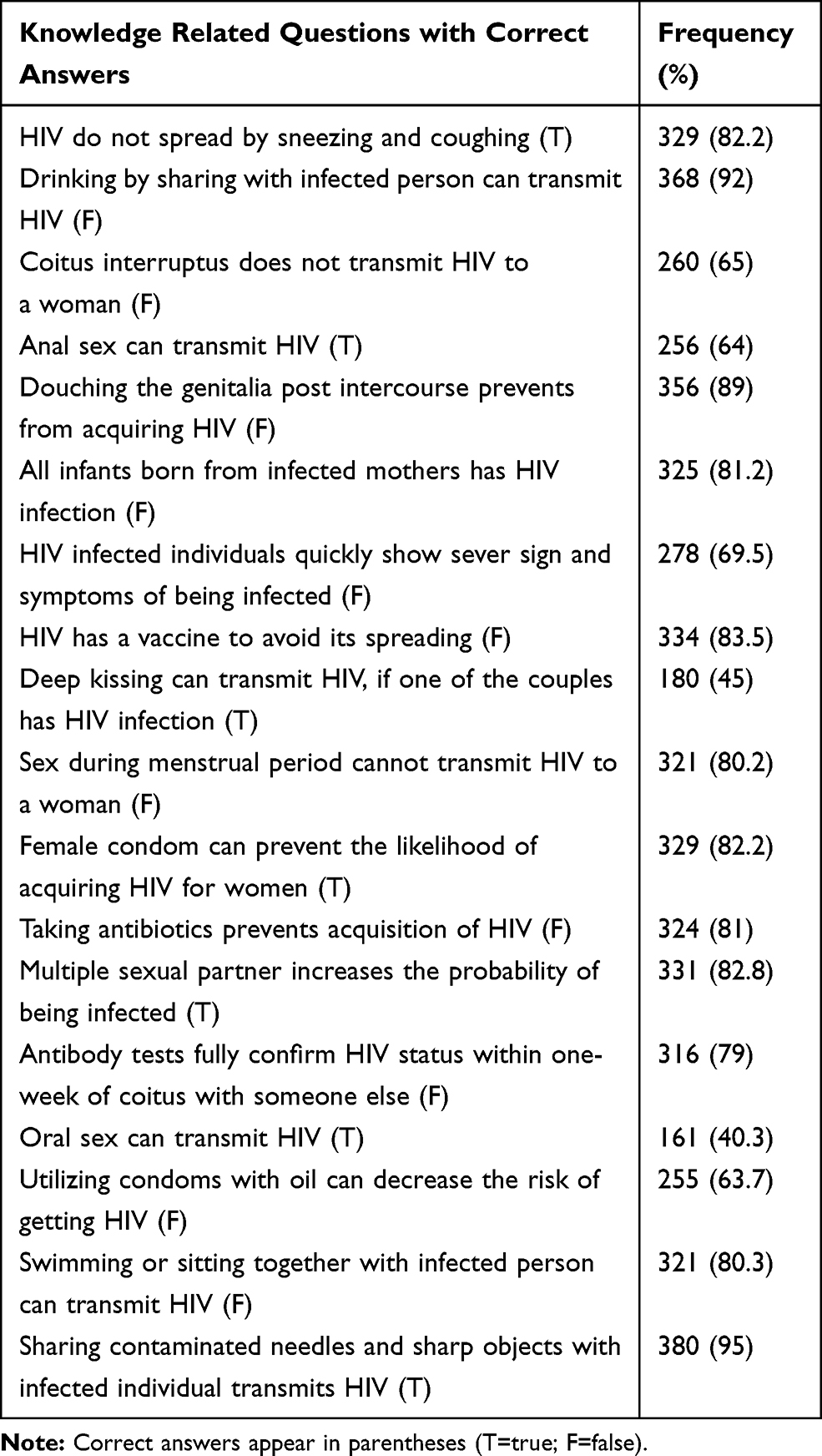 |
Table 2 Distribution of Correct Answers About Knowledge Related Questions Among Students in Selected Universities of Northwest Ethiopia, 2019 |
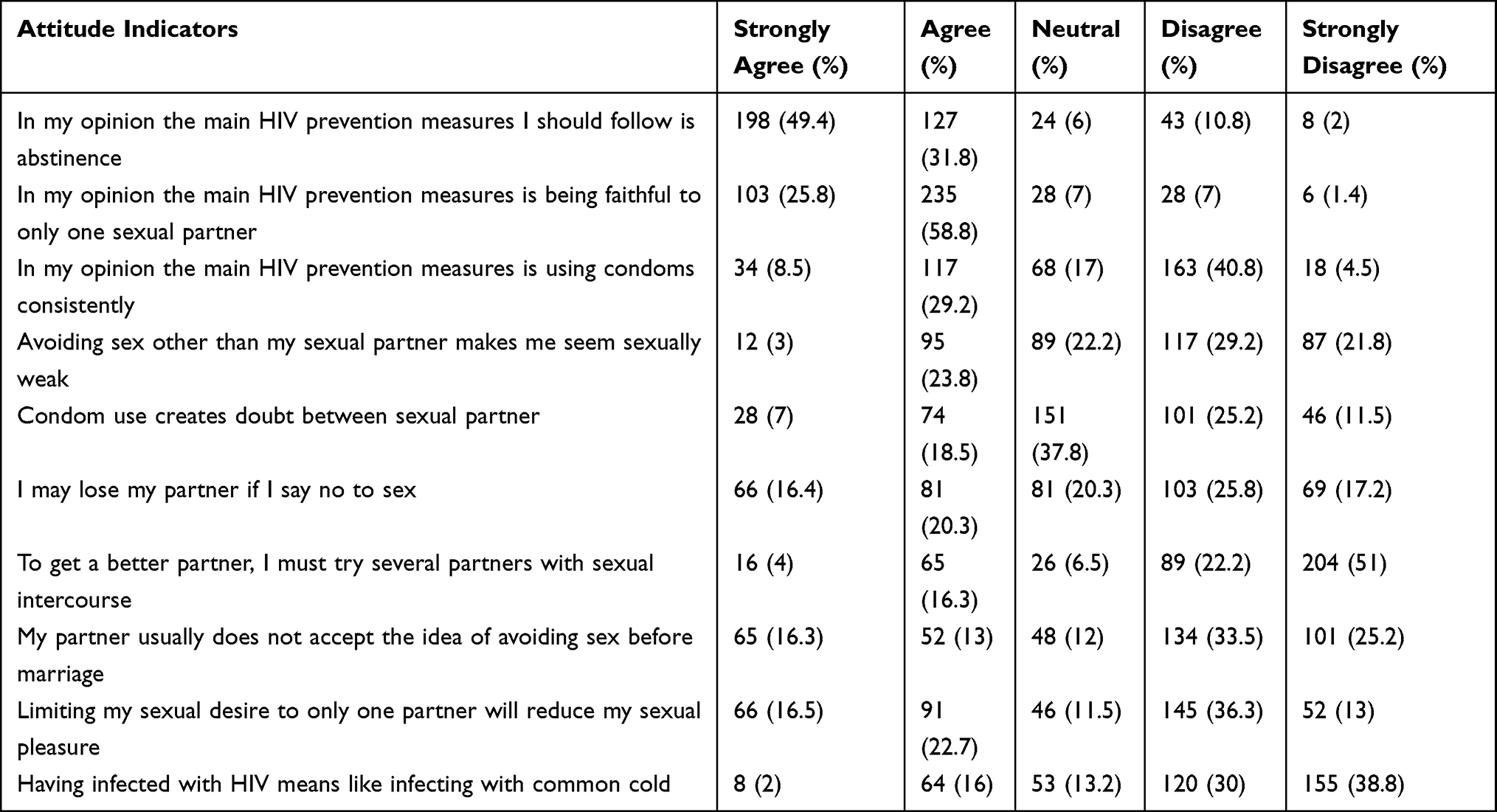 |
Table 3 Attitude Towards HIV Prevention Messages Among University Students in North West, Ethiopia, 2019 |
Perceptions of Threat and Efficacy on HIV/AIDS
A total of 12 questions were used to assess efficacy and threat perceptions; of which the first six questions assess students’ perceived threat (perceived susceptibility, perceived severity) whereas the last six questions assess students’ perceived efficacy (response efficacy, self-efficacy) (Table 4). Based on the operational definition, 263 (65.8%; 95%CI: 61–70) of the students were in danger control (positive critical value) whereas 137 (34.2%; 95%CI: 30–39) were in fear control response having negative critical value whereas no individuals have zero critical value.
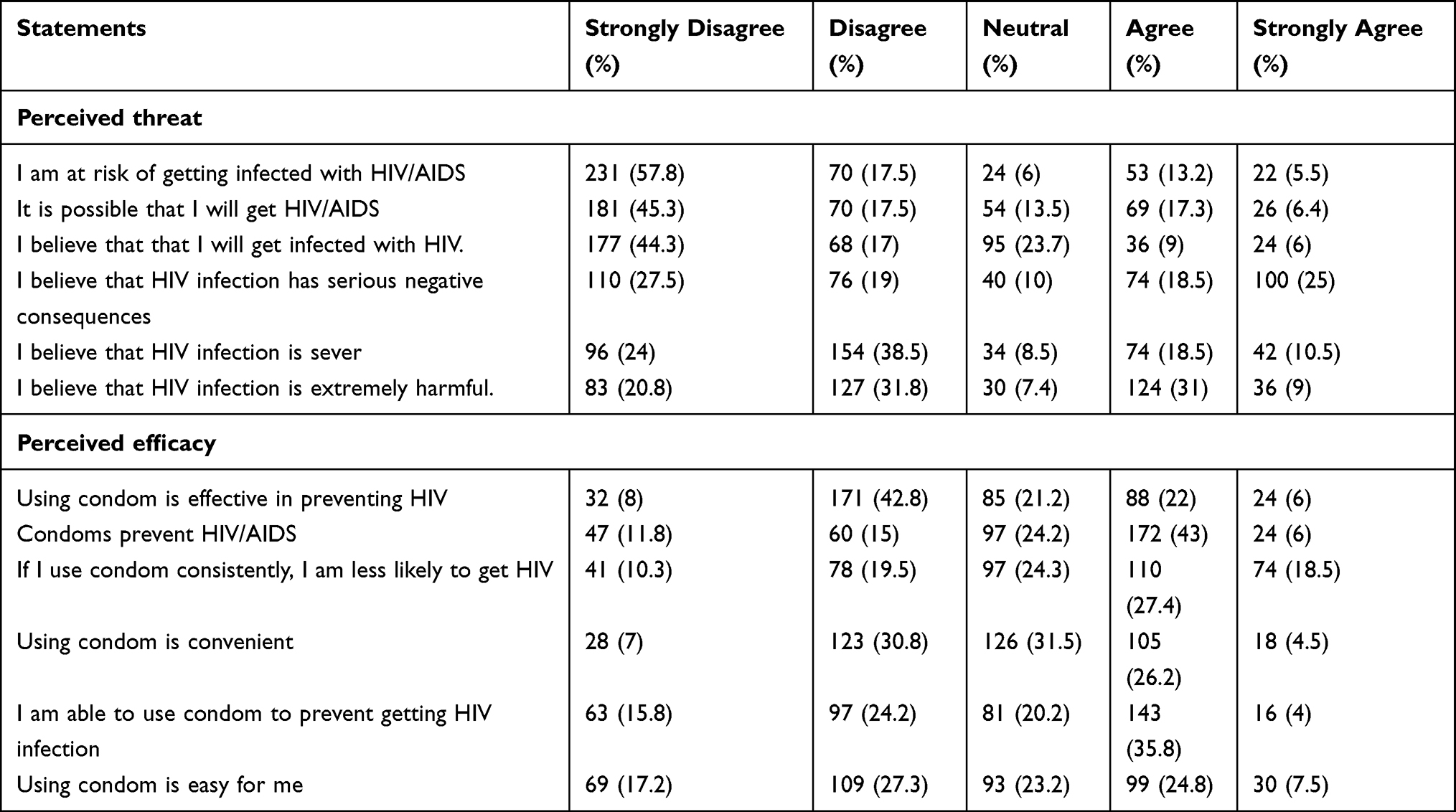 |
Table 4 Perception of Threat and Efficacy Among University Students, in North West Ethiopia, 2019 |
Factors Affecting Response to HIV Prevention Messages
In bivariable logistic regression analysis, sex of the respondent, year of the study, previous residence, with whom they currently live, type of message they received, attitude and knowledge were statistically associated with response of students towards HIV prevention messages with p-value less than 0.05 at 95% confidence interval. However, only year of the study, with whom they currently live, type of message they received, and knowledge level of respondents were significantly associated with the response of students towards HIV prevention messages in multivariable analysis (Table 5). First-year students were 5.5 times more likely to develop danger control as compared to fifth-year students (AOR=5.5; 95%CI: 1.5–19). Similarly, third-year students were 3.9 times more likely to develop danger control than fifth-year students (AOR=3.9; 95%CI: 2–14).
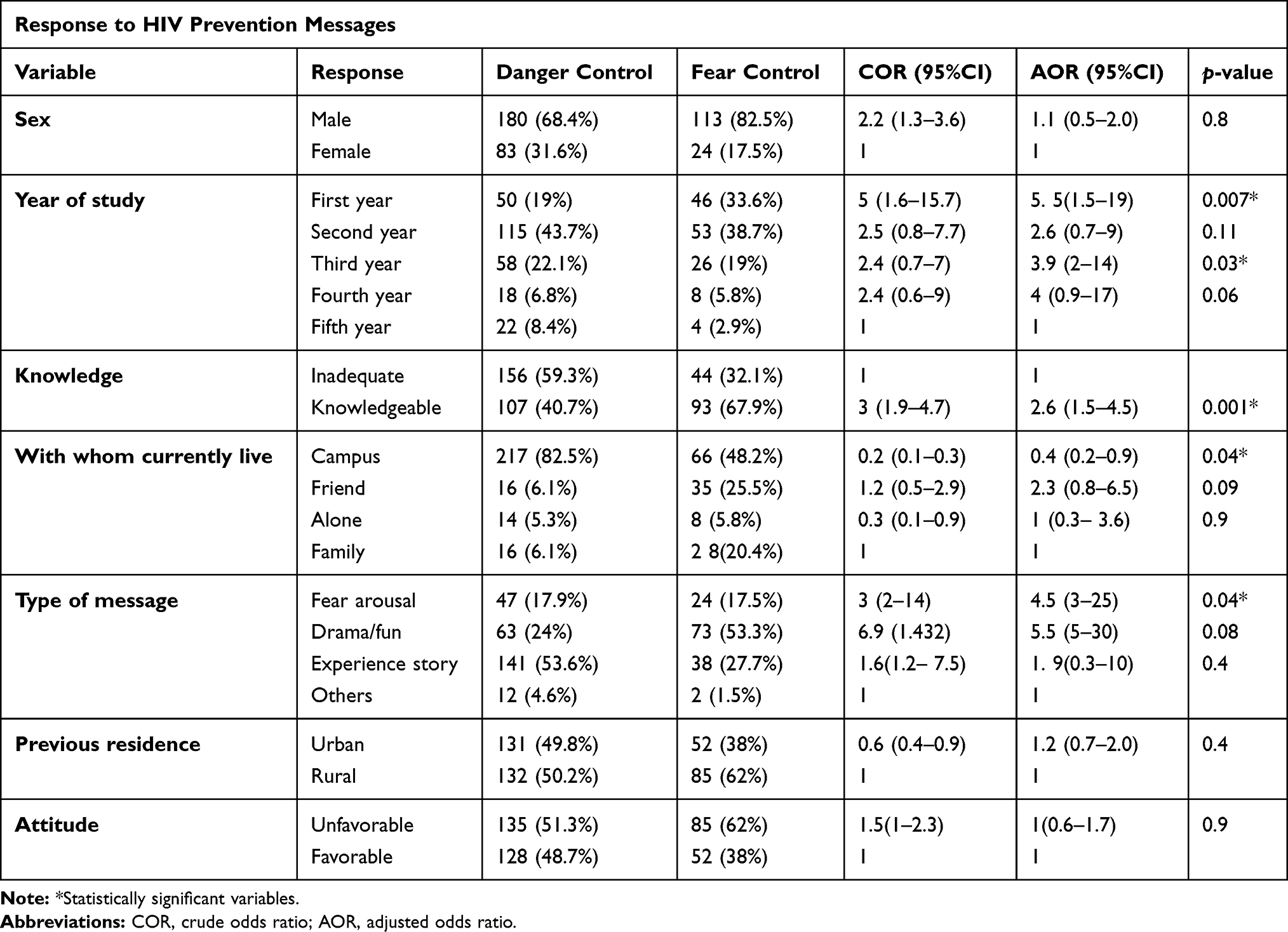 |
Table 5 Factors Associated with Response of Students Toward HIV Prevention Messages in Selected Universities of Northwest Ethiopia, 2019 |
In addition, students who live on the campus were 60% times less likely to develop danger control as compared to students who live with the family (AOR=0.4; 95%CI: 0.2–0.9). Moreover, students who had adequate knowledge were 2.6 times more likely to develop danger control as compared to students who had inadequate knowledge (AOR=2.6; 95%CI: 1.5– 4.5).
Similarly, students who receive fear arousal messages were 4.5 times more likely to develop danger control as compared to students who received other type of messages (AOR=4.5; 95%CI: 3–25).
Source and Type of Message
Among the respondents 168 (42%), 132 (33%), 40 (10%), 24 (6%), 18 (4.5%), and 18 (4.5%), were received messages about HIV/AIDS prevention from health-care workers, radio/television, religious leader, other (clubs) sources, friend/parent, and people living with HIV respectively. Besides this, about 179 (44.7%) of the respondents like to receive life experience messages in the form of story and 136 (34%) of the respondents like to receive messages in the form of fun or drama (Figure 3).
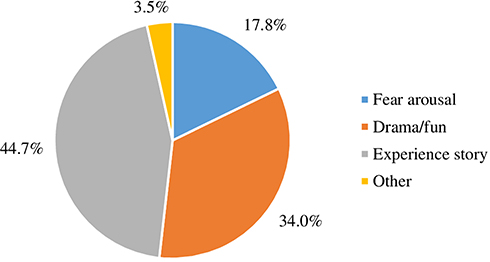 |
Figure 3 Type of HIV prevention messages that the students like to receive, 2019. |
Discussion
In this study, extended parallel process model was used to assess the response of students towards HIV/AIDS prevention messages. In this study, 65.8% with 95%CI: 61–70 of the respondents were in danger control responses, whereas 34.2% with 95%CI: 30–39 were in fear control response. However, a study conducted in Hosanna, Ethiopia showed that, 48.1% of the respondents were in danger control response and 51.9% were found in fear control response.18 Another study in Iran also showed that 31.3% and 68.7% of the respondents were in the fear control and danger control respectively towards HIV prevention messages.19 This might be because in danger control, the participants may consider alternatives to avert a health threat (HIV/AIDS) whereas in fear control, they denied danger and focus on controlling fear by not processing the risk.
In this study, only half with 95%CI: 45.3– 55 of the respondents had adequate knowledge towards HIV/AIDS prevention messages. This is relatively lower than a study conducted in United Arab Emirates, where 61% of them had adequate knowledge.20 The reason for this discrepancy might be lack of accessibility of adequate trainings on HIV/AIDS prevention methods for university students in Ethiopia.
Year of the study was significantly associated with students’ response to HIV/AIDS prevention messages in this study; of whom first-year students (AOR=5.5; 95%CI: 1.5–19) and third-year students (AOR=3.9; 95%CI: 2–14) were more likely to develop danger control as compared to fifth-year students which is in line with a study conducted in Bahir Dar among private college students, where third-year students committed 4.98 times more risky sexual behaviors than first-year students.21 This further justifies that as year of study increases the risk of having multiple sexual partners is increased which in turn leads to acquisition health threat (HIV) due to alcohol and substance use, peer pressure and increased level of extroversion.
The students who live in the campus were 60% times less likely to develop danger control as compared to students who live with the family (AOR=0.4; 95%CI: 0.2–0.9) which is in line with a study done in Bahir Dar, where university students are susceptible to acquire HIV infections due to exposure to substances, sexual promiscuity and living far from the family without family supervision.13 This might be because of peer pressure, far away from family, intake of alcohol and substance causes sense of relaxation and impair cognitive capacity that ultimately lead to not perceiving HIV as health risk.
Similarly, students who receive fear arousal message were 4.5 times more likely to develop danger control as compared to students who received other type of messages (AOR=4.5; 95%CI: 3–25) which is also supported by review studies conducted in different countries, in which students danger control response is enhanced by delivering fear arousal messages.22,23 This might be because of when a serious personally relevant threat is elicited to a person by fear arousal messages; they tried to avert that threat by performing recommended actions.
Strengths and Limitations of the Study
The main strength of this study is assessing behavioral response towards HIV prevention messages by using the extended parallel process model. However, the quantitative results are not supported with qualitative findings and it does not include the response of other HIV prevention messages such as abstinence and being faithful to once sexual partner.
Conclusion and Recommendation
Nearly one-third of the students were in fear control response while the remaining two-thirds of the respondents were in danger control response. Year of study, with whom students currently live, type of message they received and knowledge level of respondents were the factors associated with students’ response to HIV/AIDS prevention messages. Therefore, the messages must aim at enhancing threat components with appropriate efficacy messages in danger control response, whereas the messages must aim at efficacy alone in fear control response to promote behavioral change among students. Besides this, all concerned bodies should increase students’ awareness to HIV/AIDS prevention messages, monitor, and evaluate those students who live in the campus.
Abbreviations
EPPM, extended parallel process model; CD4, Cluster of Differentiation 4.
Data Sharing Statement
All data pertaining to this study are contained and presented in this document.
Acknowledgments
Authors would like to thank Debre Markos University, Injibara University, Bahir Dar University, data collectors, and supervisors.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work. There is no conflict of interest regarding the publication of this paper. The abstract of this paper was submitted at the 31st EPHA annual Conference under the theme of Health service delivery for oral presentation with interim findings. However, due to the emerging of the COVID-19 pandemic the conference was officially cancelled and not yet presented. The submitted abstract was found in the 31st EPHA annual conference presentation and authors data set list via the following link: https://etpha.org/conference/index.php/31stConference/31stConference/schedConf/presentations.
References
1. Morris M. Aidsmap.com: a comprehensive HIV/AIDS information resource. J Consum Health Internet. 2017;21(4):402–409. doi:10.1080/15398285.2017.1377545
2. WHO. HIV/AIDS key facts report. July, 2019. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids.
3. Kharsany AB, Karim QA. HIV infection and AIDS in sub-Saharan Africa: current status, challenges and opportunities. Open AIDS J. 2016;10:34. doi:10.2174/1874613601610010034
4. HIV prevention 2020 road map — accelerating HIV prevention to reduce new infections by 75%. October, 2017. Available from: https://www.unaids.org/en/resources/documents/2017/hiv-prevention-2020-road-map.
5. Group GHPW. HIV prevention in the era of expanded treatment. 2004. Available from: http//wwwgatesfoundationorg/nr/downloads/globalhealth/aids/PWG2004Reportpdf.
6. Susuman AS. HIV/AIDS in Ethiopia: health View. J Asian Afr Stud. 2017;52(3):302–313. doi:10.1177/0021909615570957
7. National consolidated guidelines for comprehensive HIV prevention, care and treatment. August, 2018.
8. Mulu W, Abera B, Yimer M. Prevalence of human immunodeficiency virus infection and associated factors among students at Bahir Dar University. Ethiop J Health Dev. 2016;28(3).
9. Belachew Y. HIV sero-prevalence among students of Jimma University, Southwest Ethiopia. Ethiop J Health Sci. 2004;14(2):65–74.
10. Shewangizaw Z, Girma M, Endazenaw G. Assessment of HIV sero-prevalence among St. Marry University Students, Ethiopia. Science. 2015;3(4):468–477.
11. Mengistu B. P3. 303 HIV prevalence and associated risk factors among University Students in Eastern Ethiopia, 2009. Sex Transm Infect. 2013;89(Suppl1):A243–A. doi:10.1136/sextrans-2013-051184.0758
12. Peltzer K, Seoka P. Evaluation of HIV/AIDS prevention intervention messages on a rural sample of South African youth’s knowledge, attitudes, beliefs and behaviours over a period of 15 months. J Child Adolesc Ment Health. 2004;16(2):93–102. doi:10.2989/17280580409486576
13. Mulu W, Abera B, Yimer M. Prevalence of human immunodeficiency virus infection and associated factors among students at Bahir Dar University. Prevalence. 2014;28(3).
14. Casey MK, Timmermann L, Allen M, Krahn S, Turkiewicz KL. Response and self-efficacy of condom use: a meta-analysis of this important element of AIDS education and prevention. South Commun J. 2009;74(1):57–78. doi:10.1080/10417940802335953
15. Witte K. Putting the fear back into fear appeals: the extended parallel process model. Commun Monogr. 1992;59(4):329–349. doi:10.1080/03637759209376276
16. Witte K, Meyer G, Martell D. Effective Health Risk Messages: A Step-By-Step Guide. Sage; 2001.
17. Witte K. Fear control and danger control: a test of the extended parallel process model (EPPM). Commun Monogr. 1994;61(2):113–134. doi:10.1080/03637759409376328
18. Feleke D, Zewdie B, Yohannes K, Tariku D, Dube J. Are people controlling the danger or fear for condom use as HIV/AIDS preventive message? An evaluative type of study based on extended parallel process model. J AIDS Clin Res. 2013;4(12).
19. Esmaeilzadeh S, Allahverdipour H, Fathi B, Shirzadi S. Risk perception of HIV/AIDS and low self-control trait: explaining preventative behaviors among Iranian university students. Glob J Health Sci. 2016;8(4):44. doi:10.5539/gjhs.v8n4p44
20. Haroun D, El Saleh O, Wood L, Mechli R, Al Marzouqi N, Anouti S. Assessing knowledge of, and attitudes to, HIV/AIDS among university students in the United Arab Emirates. PLoS One. 2016;11(2):e0149920. doi:10.1371/journal.pone.0149920
21. Alamrew Z, Bedimo M, Azage M. Risky sexual practices and associated factors for HIV/AIDS infection among private college students in Bahir Dar City, Northwest Ethiopia. ISRN Public Health. 2013;2013.
22. Popova L. The extended parallel process model: illuminating the gaps in research. Health Educ Behav. 2012;39(4):455–473. doi:10.1177/1090198111418108
23. Maloney EK, Lapinski MK, Witte K. Fear appeals and persuasion: a review and update of the extended parallel process model. Soc Personal Psychol Compass. 2011;5(4):206–219. doi:10.1111/j.1751-9004.2011.00341.x
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.