")
Back to Journals » Research Reports in Clinical Cardiology » Volume 13
Baseline Characteristics, Risk Factors and Etiology of Heart Failure Among Patients Hospitalized at a Teaching Hospital in Somalia: Cross-Sectional Study
Authors Farah Yusuf Mohamud M , Jeele MOO , Cetinkaya O, Goitom Sereke S , Bongomin F , AM Ahmed M
Received 26 June 2022
Accepted for publication 3 September 2022
Published 13 September 2022 Volume 2022:13 Pages 63—71
DOI https://doi.org/10.2147/RRCC.S380136
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Kones
Mohamed Farah Yusuf Mohamud,1 Mohamed Osman Omar Jeele,1 Osman Cetinkaya,1 Senai Goitom Sereke,2 Felix Bongomin,3 Mohamed AM Ahmed4– 6
1Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia; 2School of Medicine, College of Health Sciences, Makerere University, Kampala, Uganda; 3Department of Medical Microbiology and Immunology, Faculty of Medicine, Gulu University, Gulu, Uganda; 4Department of Paediatrics, Faculty of Medicine and Surgery, Mogadishu University, Mogadishu, Somalia; 5Department of Paediatric Cardiology, Uganda Heart Institution, Kampala, Uganda; 6Basaksehir Cam ve Sakura Sehir Hospital, University of Health Sciences, Istanbul, Turkey
Correspondence: Mohamed Farah Yusuf Mohamud, Mogadishu Somali Turkey Education and Research Hospital, Thirty Street, Alikamin, Wartanabada District, Mogadishu, Somalia, Tel +252615591689, Email [email protected]
Introduction: Heart failure (HF) is a heterogeneous syndrome and growing global epidemic estimated to affect over 26-million people worldwide. The aim of this study is to investigate baseline characteristics, risk factors, and etiology of HF among patients admitted to a tertiary hospital in Somalia.
Methods: Between May and October 2021, data on epidemiological characteristics, risk factors, and etiology of HF among patients admitted to an emergency unit of a teaching hospital in Mogadishu, Somalia were retrospectively collected and analyzed.
Results: A total of 155 patients were disgnosed with HF, their mean age was 65.9 ± 14 years, 46.5% (n = 72) were aged 65 years or older, and 58.7% (n=91) were female. The prevalence of HF was 3.4% (n = 155); 47.7% (n = 74) had HF with preserved ejection fraction (HFpEF), 34.9% HF with reduced ejection fraction (HFrEF), and 17.4% HF with mildly reduced ejection fraction (HFmrEF). More females than males had HFrEF and HFmrEF (77.8% vs 59.3%, p < 0.01). In contrast, HFpEF was more frequent in males (55.4% vs 44.6%, p < 0.01). Regarding cardiovascular disease risk factors, patients with HFpEF had advanced age (≥ 65), were male, and had co-morbid hypertensive heart disease (HHD) and thyroid disease. On the other hand, patients with HFrEF were more in older age (50– 64 years), were women, and frequently had ischemic heart disease and diabetes mellitus compared to patients with HFpEF and HFmrEF. Among participants with HFpEF, HHD (58.1%) was the most common etiologies of HF, whereas in HFrEF, ischemic heart disease (38.9%) was prominent.
Conclusion: HF in Somalia, different risk factors and etiologies were found in three groups of HF patients. Hypertension plays a predominant role both in its risk factors and the underlying cause of HF. We recommend implementation of specialized cardiac centers for the adult patients with cardiovascular diseases and promotion of the awareness of cardiovascular risk factors.
Keywords: heart failure, ejection fraction, hypertension, diabetes, emergency unit, Somalia
Introduction
According to the American College of Cardiology/American Heart Association (ACC/AHA) and the European Society of Cardiology (ESC) guidelines for the diagnosis and treatment of chronic heart failure (CHF), heart failure (HF) is a combined clinical syndrome that results from various anatomical or physiological cardiac dysfunction that impairs the ability of the ventricles to be supplied with or eject blood.1,2 HF has emerged as a global pandemic affecting over 26 million people worldwide, and it is expected that by 2030 more than 8 million people will develop HF.3,4
The prevalence and incidence of HF in developed countries range from 1–2% of the adult population and 5–10 per 1000 population per year, respectively.5,6 Although there are no population-based studies about incidence and prevalence in sub-Saharan Africa (SSA), studies reported from SSA hospital indicates that HF is responsible for about 9.4–42.5% of all medical admissions and 25.6–30.0% of admissions into the cardiac units.7,8 Therefore, HF is an important cause of morbidity in SSA and yet heavily under recognized and probably underdiagnosed, and the true burden of the syndrome in the region remains unknown.9
Several underlying cardiac and extracardiac disease predispose to HF. However, ischemic heart disease (IHD), hypertension, diabetes mellitus, and valvular heart disease (VHD) are the most common risk factors for HF, globally.10 In SSA, rheumatic heart disease (RHD) is the most common risk factor for HF, however, other risk factors such as ischemic heart disease (IHD), non-RHD VHD, hypertensive heart disease (HHD), dilated cardiomyopathy (DCMP), and cor-pulmonale are becoming increasingly common.11,12 Regardless of the cause, patients with HF commonly presents with exertional dyspnea, orthopnea, paroxysmal nocturnal dyspnea, fatigue, and peripheral edema.1,2
Hospitalization for decompensated HF carries a poor prognosis with high mortality rates.13,14 Predictors of poor prognosis includes advanced age, lower systolic blood pressure, elevated blood urea nitrogen (BUN), and impaired renal function.15–17 However, racial, and ethnic difference is also thought to contribute to HF clinical outcomes.
There is a paucity of studies on clinical characteristics, risk factors, and etiology of different phenotypes of HF among patients from Somalia. This study therefore aimed to investigate baseline characteristics, risk factors, and etiology of different types ofHFamong patients admitted to an emergency unit of a teaching hospital in Mogadishu, Somalia.
Method
Study Design and Setting
This was a hospital-based retrospective study conducted in Mogadishu, Somalia, between May and October 2021. We used the recently established hospital information system (FONET) of the Emergency Unit in Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia. The FONET database was made possible due to collaboration with the Ministry of health Somalia, the Ministry of Health of Turkey, and sağlık bilimleri üniversitesi.
Study Population
This cross-sectional observational study enrolled heart failure patients visiting in the emergency department at Mogadishu Somalia Turkish Training and Research Hospital from May 2021 to October 2021. A total of 4500 patients were screened in the emergency unit, 155 patients were diagnosed heart failure (HFpEF, HFrEF, and HFmrEF).
More than 50 cardiac patients are seen per day in the hospital. Cardiologists diagnosed HF as fulfilling the Framingham criteria. The criteria included in the list were physician assessments of neck-vein distension, rales, S3 gallop, venous pressure >16cm of water, hepatojugular reflux, and weight loss of 4.5 kg in 5 days due to diuretic therapy (major criteria). Minor criteria were ankle edema, night cough, dyspnea on exertion, tachycardia, hepatomegaly, and weight loss.
“Definite heart failure” was defined as having at least two major criteria or one major criterion and two minor criteria, if the minor criteria could not be attributed to any other condition.
The baseline characteristics of the participants included age and gender, and the risk factors included hypertension, diabetes mellitus, ischemic heart disease, dyslipidemia, thyroid diseases, underlying diseases, and HF was classified according to the left ventricular ejection fraction (LVEF).
Sample Size
Patients hospitalized within the study population constituted the study population.
Study Procedure
From the clinical and echocardiographic data in the medical records, we attempted to determine the cause of HF. Ischemic heart disease was defined as (a) a clinical diagnosis of myocardial infarction or (b) an electrocardiographic (ECG) finding of Q-wave myocardial infarction, (c) a history of coronary angioplasty or coronary artery bypass graft, and (d) ECG stress test which is considered positive for ischemia if there is at least a 1-mm horizontal or down-sloping ST-segment depression. Up-sloping ST-segment depression is not considered a positive finding. An ST-segment elevation greater than 1 mm is highly suggestive of significant ischemia. Echocardiographic findings were defined as the diagnosis of valvular and congenital heart disorders and pulmonary arterial pressure (PAP). Moreover, measurement of PAP on echocardiography by using tricuspid valve velocity (4v2 = TV pressure gradient).
HHD was defined as a clinical history of hypertension and left ventricular hypertrophy (LVH) determined from echocardiographic or ECG findings. The criteria for cardiomyopathy (CM) comprised the absence of signs of ischemic, hypertensive, valvular, or congenital heart disease and the presence of global Left ventricular dilation with impaired systolic function or LVH with diastolic dysfunction in the absence of a known cardiac or systemic cause.
Classification of patients with HF according to left ventricular ejection fraction (LVEF), from those with normal LVEF (≥50%) considered as HF with preserved EF (HFpEF), to those with reduced LVEF (40%) recognized as HF with reduced EF (HFrEF), those Patients with an LVEF in the range of 40–49% define as HF with mildly reduced EF (HFmrEF), and HF with improved EF (HFmrEF): HF with a baseline LVEF≤40%, a ≥10-point increase from baseline LVEF, and a second measurement of LVEF>40%.18 This classification is essential due to different demographics, co-morbidities, underlying etiologies, and responses to therapies.19
The study protocol was approved by the local Institutional Review Board Committee of Ethics from the Mogadishu Somali Turkish Training and research Hospital, Mogadishu, Somalia (Approval number: MSTH/6383), which also provided a waiver of consent given the retrospective nature of the study. Nonetheless, all patient records/information were anonymized before analysis.
Statistical Analysis
Microsoft Excel software was used to create the database and cleaned data was analyzed using STATA version 16.0. Continuous variables are presented as mean ± standard deviation and categorical variables as the observed number of patients (percentage). The Mann–Whitney U-test was used for continuous variables and Fisher's exact test was utilized for categorical variables to compare patient characteristics between groups (HFpEF, HFmrEF, and HFrEF). P-value<0.05 was considered statistically significant.
Results
Demographic Characteristics, Prevalence and Classification of Heart Failure
A total of 4500 patients were screened in the emergency unit, 155 patients were diagnosed heart failure (HFpEF, HFrEF, and HFmrEF). The median age of the participants was 65.9 ± 14 years, 46.5 (n=72) were aged 65 years or older, and 58.7% (n=91) were female.
Of the 4500 participants, 3.4% (n=155) met the author-defined definition of definitive HF. Of this, the classification of heart failure was based purely on clinical assessment and echocardiography without the use of brain natriuretic peptide (BNP). The prevalence of HFpEF, HFrEF, and HFmrEF was 47.7% (74/155), 34.9% (54/155), and 17.4% (27/155), respectively.
Risk Factors for Heart Failure
Table 1 summarizes the risk factors for HF among the participants. Most (66%, n=102) of participants with HF had a history of hypertension. Forty-seven (30.3%) had at least one cardiovascular disease, 36 (23.2%) had diabetes mellitus, 36 (23.2%) hyperlipidemia, and 25 (16.1%) thyroid disease.
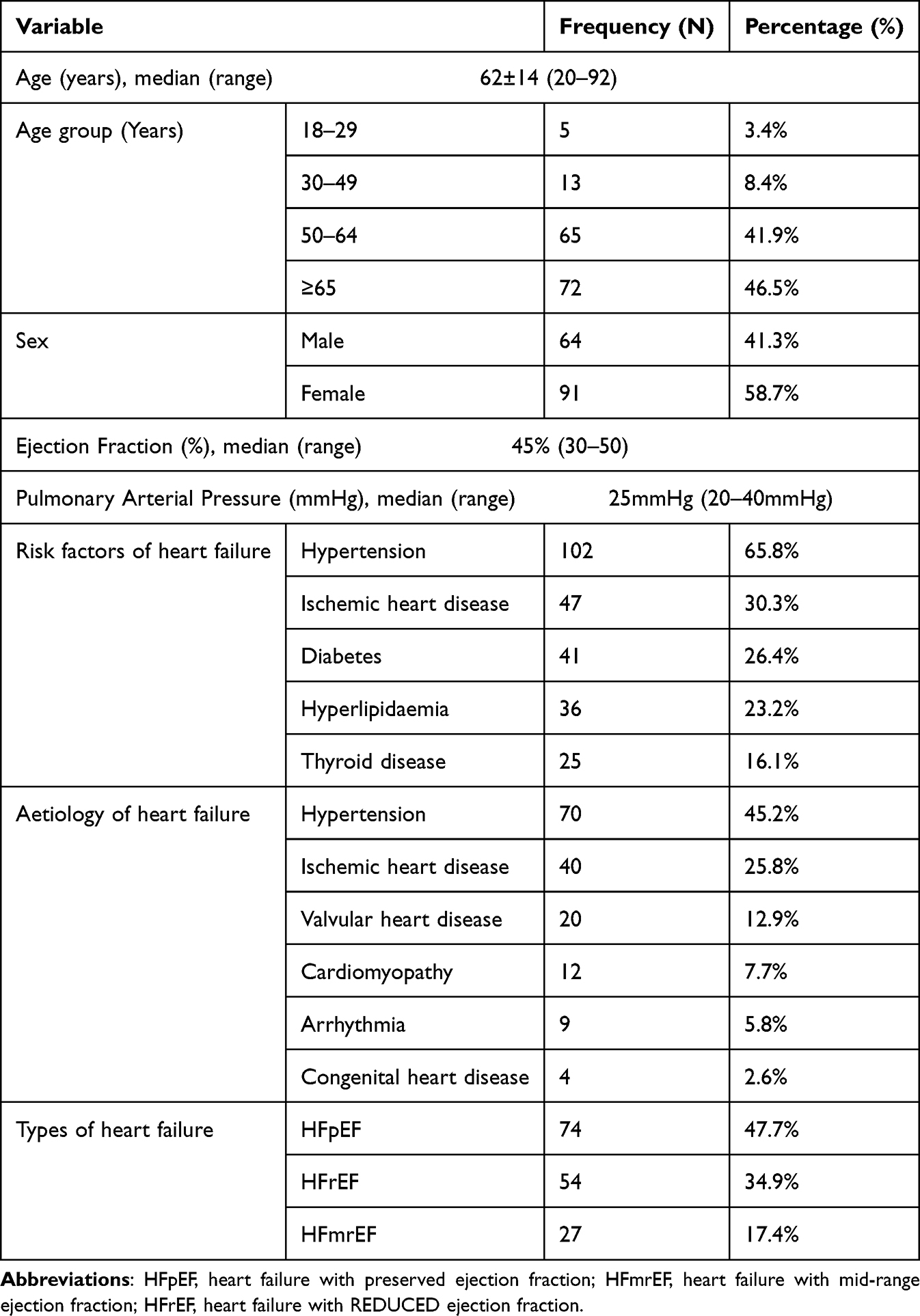 |
Table 1 Epidemiological Characteristics, Risk Factors, and Aetiology of Different Types of Heart Failure Patients, MSTERH, Somalia from May to October 2021 |
Etiology of Heart Failure
Hypertension was the leading cause of HF (45.1%, n=70), followed by IHD (25.8%, n= 40), VHD (12.9%, n= 20), cardiomyopathy (7.7%, n= 12), arrhythmias (5.8%, n= 9), and congenital heart disease (2.6%, n=4), Table 1.
A higher proportion of females than males hadHFrEF or HFmrEF (77.8% versus 59.3%, p< 0.01). In contrast, HFpEF was more common among males (55.4% versus 44.6%, p< 0.01), Table 2.
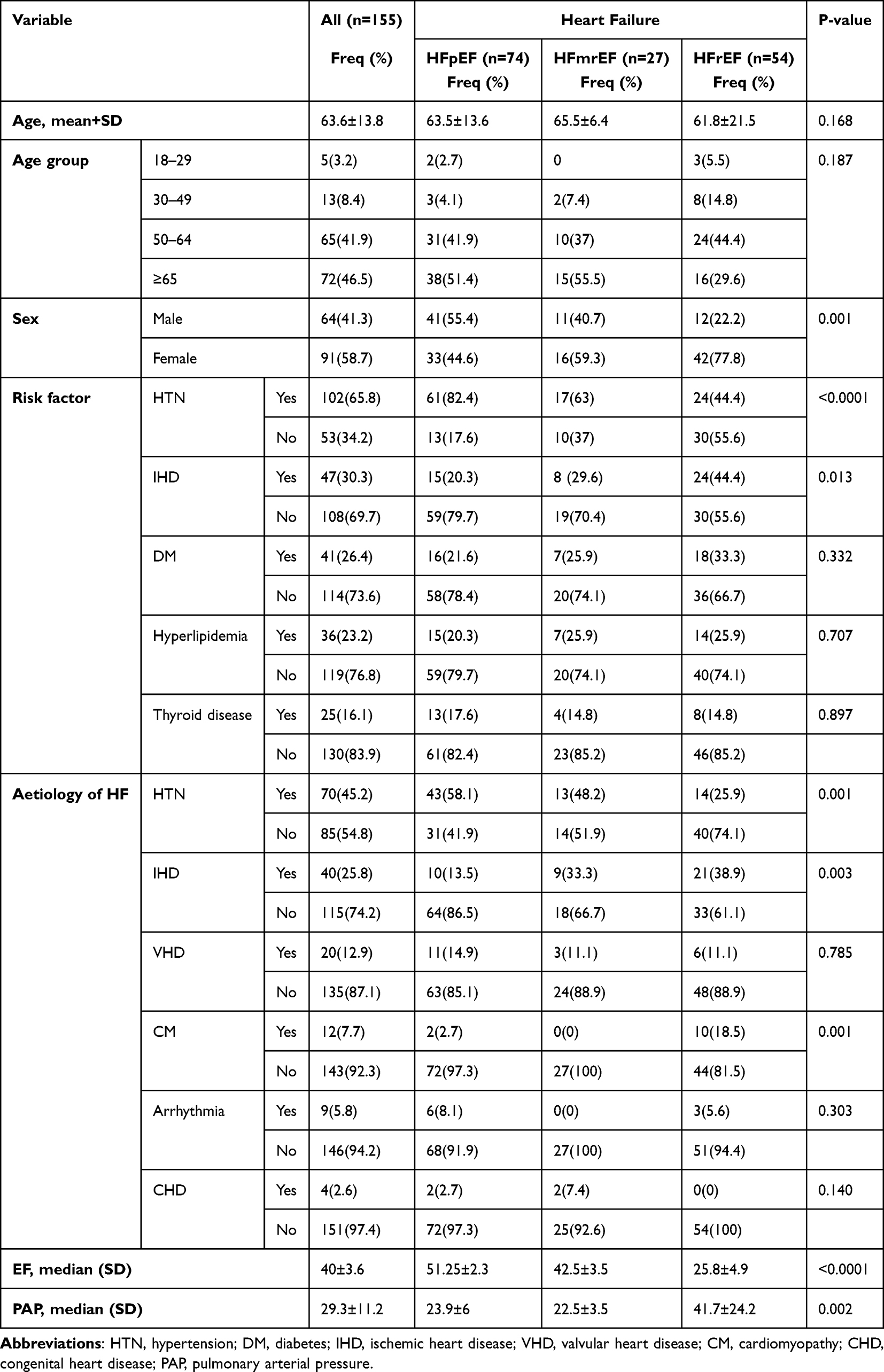 |
Table 2 Epidemiological Characteristics, Risk Factors, and Aetiology of Study Participants Illustrating the Differences Between HFpEF, HFmrEF and HFrEF |
Stratification of Risk Factors Across Ejection Fractions
As compared to those with HFrEF, participants with HFmrEF or HFpEF mostly had ischemic heart disease (44.4% versus 29.6% versus 20.3%, p< 0.05) and diabetes mellitus (33.3% versus 25.9% versus 21.6%%, p=0.3), but a lower proportion of participants with hypertension (44.4 versus 63% versus 82.4%, p<0.0001). There was no statistically significant difference in hyperlipidemia and thyroid disease rates between HF subtypes.
Participants with HFmrEF and HFrEF had a lower prevalence of hypertension (58.1% versus 48.2% versus 26.9%, p=0.003), VHD (14.9% vs 11.1% vs 11.1% P=0.3), and arrhythmia (8.1% versus 0%, versus 5.6%, p<0.1) but a lower extent of ischemic heart disease (13.5% versus 33.3% versus 38.9%, p=0.003) compared to those with HFpEF. As compared to participants with HFpEF and HFmrEF, a higher proportion of those with HFrEF had pulmonary arterial pressure (PAP) (23.9±6 versus 22.5±3.5 versus 41.7±24.2, p= 0.002) (Table 2).
Discussion
HF has emerged as a global pandemic affecting over 26 million people worldwide, and it is expected that by 2030 more than 8 million people will develop HF.3,4 Even though HF affects large numbers of patients and the morbidity and mortality are striking. Therefore, it is of critical importance to analyze the data of HF patients in routine clinical practice on a national basis and to form a database for future investigations.
In this cohort of patients, the mean age of the study population was 65.9 ± 14 years, years with 46.5% of patients being 65 years and older. In sharp contrast to the present study, a Survey of Heart Failure (THESUS-HF), which included 1006 patients hospitalized for acute heart failure in nine Sub-Saharan African nations, reported mean age of 52.3 years.20 However, similarly to the demographic pattern observed in the developed countries where the most usually affected age group is those over 65.21–23
HF is well-known in the Western world as a major public health issue linked to a high risk of morbidity and mortality, especially among the elderly.8
According to hospital prevalence surveys in SSA, HF accounts for 9.4–42.5% of all medical hospitalizations and 25.6–30.0% of cardiac unit admissions.8 In contrast, there is a lack of previous population-based incidence and prevalence studies on heart failure in Somalia.
In the present study, the prevalence of heart failure in Somalia was 3.4%. A study conducted by Massoure et al found that the prevalence of HF in Djibouti was 2.7%.23 A recent study conducted from Sudan found that the prevalence of HFpEF was 15%.24 Another study reported from Ethiopia determined that HFis the third most common reason for admission to the medical wards of Saint Paul Medical College Hospital (SPMCH), accounting for 16% of all admissions.25 In developed countries, the prevalence of HFpEF is increasing over time.26,27 In the current study, the prevalence of HFpEF was 47.7%, which was consistent with other studies from Ethiopia, Saudi, and the USA.12,28,29 According to a recent study conducted by Martinez-Brana et al, 72.2% of Spaniards have HFpEF.12 Kaneko et al observed a prevalence of HFpEF of 72% in a study conducted in Japan.30
On the other hand, the prevalence of HFmrEF in the present investigation was 17.4%. According to the HESUSHF registry, the prevalence of HFmrEF was 19.6% in one of 12 hospitals in nine countries.16 On the contrary, the prevalence of HFrEF was 34.9% which was in alignment with another study from African countries.12,31
In this study, as compared to males, female patients had a greater prevalence of HFrEF and HFmrEF. In contrast, HFpEF were more prominent to male gender. Most of the cases had a prior history of hypertension, IHD, and diabetes mellitus. Previous studies in patients with HFpEF were at an advanced age, women, and more frequently have hypertension compared to patients with HFmrEF and HFrEF.30,32,33 Patients with HFpEF were advanced age (≥65), male sex, and more often to have hypertension and thyroid disease than patients with HFpEF and HFmrEF, according to the present study.
In the current analysis, patients with HFrEF were more in elder age (50–64), women, and frequently have IHD and diabetes compared to patients with HFpEF and HFmrEF. In a meta-analysis study, compared with patients with HFpEF, those with HFrEF were younger and more often men, and have a history of CAD.34 In general, hypertension, IHS, and VHD were the most common causes of heart failure in our study. This was a similar finding in other studies.12,23,35 Regarding the present study, the etiology of HF specifically in patients with HFpEF, hypertensive heart disease (HHD), and VHD is more prevalent. Whereas, patients with HFrEF, the most common causes were IHD and cardiomyopathies. Similar findings were documented in previous studies.36–39
Limitations and Strengths
Our study had several limitations. First, because this study was conducted in a single medical center, the findings could not be generalized. Second, because the study was retrospective, several participants had to drop out due to a missing document. Third, the study population’s sample size may not be large enough to detect statistically significant differences. Despite these limitations, we believe that our study provided first and vital information on the baseline characteristics, risk factors, and etiology of different types of heart failure among patients in the emergency department at a single teaching hospital in Mogadishu, Somalia. It will also serve as a blueprint for future clinical research in the field.
Conclusion
In conclusion, we report a substantial burden of HF among patients acutely hospitalized in a Somalian emergency unit. Hypertension plays a predominant role both in its risk factors and the underlying cause of HF. There is a potential sex-difference in the subtype of HF, warranting further studies. We recommend implementation of specialized cardiac centers for the adult patients with cardiovascular diseases and promotion of awareness on the importance of HF and cardiovascular risk factors.
Data Sharing Statement
All data generated or analyzed during this study are included in this article.
Ethics Approval and Consent to Participate in This Study
Approval for conducting the study was obtained from Mogadishu Somali Turkish Training and Research Hospital (Reference number –MSTH/6383). We used the electronic medical records in the hospital information system and written informed consent was waived, while the patient’s data confidentiality was respected. This study was carried out in accordance to the Helsinki Declaration contents.
Acknowledgments
We thank Mogadishu Somali Turkish training and research hospital, department of medicine and emergency unit for providing a conducive environment for our research activities.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hunt SA, Abraham WT, Chin MH; American College of Cardiology; American Heart Association Task Force on Practice Guidelines; American College of Chest Physicians; International Society for Heart and Lung Transplantation; Heart Rhythm Society. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to update the 2001 guidelines for the evaluation and management of Heart Failure). Circulation. 2005;112:e154–e235. doi:10.1161/CIRCULATIONAHA.105.167586
2. Swedberg K, Cleland J, Dargie H, et al. Guidelines for the diagnosis and treatment of chronic heart failure: executive summary (update 2005) The Task Force for the diagnosis and treatment of chronic heart failure of the European Society of Cardiology. Eur Heart J. 2005;26(11):1115–1140. doi:10.1093/eurheartj/ehi204
3. Ponikowski P, Anker SD, AlHabib KF, et al. Heart failure: preventing disease and death worldwide. ESC Heart Fail. 2014;1(1):4–25. doi:10.1002/ehf2.12005
4. Mozaffarian D, Benjamin EJ, Go AS, et al. Executive summary: heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. 2016;133(4):447–454. doi:10.1161/CIR.0000000000000366
5. Mosterd A, Hoes AW. Clinical epidemiology of heart failure. Heart. 2007;93(9):1137–1146. doi:10.1136/hrt.2003.025270
6. Cowie MR, Wood DA, Coats AJ, et al. Incidence and aetiology of heart failure; a population-based study. Eur Heart J. 1999;20(6):421–428. doi:10.1053/euhj.1998.1280
7. Mendez GF, Cowie MR. The epidemiological features of heart failure in developing countries: a review of the literature. Int J Cardiol. 2001;80(2–3):213–219. doi:10.1016/S0167-5273(01)00497-1
8. Ogah OS, Adebiyi A, Sliwa K. Heart failure in sub-saharan Africa. InTopics in heart failure management. IntechOpen. 2019;61. doi:10.5772/intechopen.82416
9. Bloomfield GS, Barasa FA, Doll JA, Velazquez EJ. Heart failure in sub-Saharan Africa. Curr Cardiol Rev. 2013;9(2):157–173. doi:10.2174/1573403X11309020008
10. Mosterd A, Hoes AW, De Bruyne MC, et al. Prevalence of heart failure and left ventricular dysfunction in the general population; The Rotterdam Study. Eur Heart J. 1999;20(6):447–455. doi:10.1053/euhj.1998.1239
11. Ntusi NB, Mayosi BM. Epidemiology of heart failure in sub-Saharan Africa. Expert Rev Cardiovasc Ther. 2009;7(2):169–180. doi:10.1586/14779072.7.2.169
12. Abebe TB, Gebreyohannes EA, Tefera YG, Abegaz TM. Patients with HFpEF and HFrEF have different clinical characteristics but similar prognosis: a retrospective cohort study. BMC Cardiovasc Disord. 2016;16(1):232. doi:10.1186/s12872-016-0418-9
13. Madsen BK, Hansen JF, Stokholm KH, Brøns J, Husum D, Mortensen LS. Chrome congestive heart failure: description and survival of 190 consecutive patients with a diagnosis of chronic congestive heart failure based on clinical signs and symptoms. Eur Heart J. 1994;15(3):303–310. doi:10.1093/oxfordjournals.eurheartj.a060495
14. Croft JB, Giles WH, Pollard RA, Keenan NL, Casper ML, Anda RF. Heart failure survival among older adults in the United States: a poor prognosis for an emerging epidemic in the Medicare population. Arch Intern Med. 1999;159(5):505–510. doi:10.1001/archinte.159.5.505
15. Fonarow GC, Adams KF, Abraham WT, Yancy CW, Boscardin WJ; ADHERE Scientific Advisory Committee. Risk stratification for in-hospital mortality in acutely decompensated heart failure: classification and regression tree analysis. JAMA. 2005;293(5):572–580. doi:10.1001/jama.293.5.572
16. Pocock SJ, Ariti CA, McMurray JJ, et al. Predicting survival in heart failure: a risk score based on 39 372 patients from 30 studies. Eur Heart J. 2013;34(19):1404–1413. doi:10.1093/eurheartj/ehs337
17. Gioli-Pereira L, Marcondes-Braga FG, Bernardez-Pereira S, et al. Predictors of one-year outcomes in chronic heart failure: the portrait of a middle income country. BMC Cardiovasc Disord. 2019;19(1):1–7. doi:10.1186/s12872-019-1226-9
18. Bozkurt B, Coats AJ, Tsutsui H, et al. Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur J Heart Fail. 2021;23(3):352–380. doi:10.1002/ejhf.2115
19. Butler J, Fonarow GC, Zile MR, et al. Developing therapies for heart failure with preserved ejection fraction: current state and future directions. JACC. 2014;2(2):97–112. doi:10.1016/j.jchf.2013.10.006
20. Damasceno A, Mayosi BM, Sani M, et al. The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries: results of the sub-Saharan Africa survey of heart failure. Arch Intern Med. 2012;172(18):1386–1394. doi:10.1001/archinternmed.2012.3310
21. Gheorghiade M, Abraham WT, Albert NM, et al. OPTIMIZE-HF investigators and coordinators. Systolic blood pressure at admission, clinical characteristics, and outcomes in patients hospitalized with acute heart failure. JAMA. 2006;296(18):2217–26. doi:10.1001/jama.296.18.2217
22. Adams JKF, Fonarow GC, Emerman CL, et al.; ADHERE Scientific Advisory Committee and Investigators. Characteristics and outcomes of patients hospitalized for heart failure in the United States: rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J. 2005;149(2):209–216. doi:10.1016/j.ahj.2004.08.005
23. Massoure PL, Roche NC, Lamblin G, et al. Heart failure patterns in Djibouti: epidemiologic transition. Medecine Et Sante Tropicales. 2013;23(2):211–216.
24. Omer A, Mohemed E, Abdulrahman A, Yousuf J, Mohammed M. Studying of heart disease prevalence, distribution and co-factors in Sudanese population. Int J Res Med Sci. 2016;4(1):206. doi:10.18203/2320-6012.ijrms20160032
25. Bane A, Bayisa T, Adamu F, Abdissa SG. Medical admissions and outcomes at Saint Paul’s Hospital, Addis Ababa, Ethiopia: a retrospective study. Ethiopian J Health Dev. 2016;30(1):50–56.
26. Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355(3):251–259. doi:10.1056/NEJMoa052256
27. Roger VL, Weston SA, Redfield MM, et al. Trends in heart failure incidence and survival in a community-based population. JAMA. 2004;292(3):344–350.
28. ElShaer F, Hassan W, Fawzy ME, et al. The prevalence, clinical characteristics, and prognosis of diastolic heart failure: a clinical study in Elderly Saudi patients with up to 5 years follow‐up. Congestive Heart Fail. 2009;15(3):117–122. doi:10.1111/j.1751-7133.2008.00043.x
29. Punnoose LR, Givertz MM, Lewis EF, Pratibhu P, Stevenson LW, Desai AS. Heart failure with recovered ejection fraction: a distinct clinical entity. J Card Fail. 2011;17(7):527–532. doi:10.1016/j.cardfail.2011.03.005
30. Kaneko H, Suzuki S, Yajima J, et al. Clinical characteristics and long-term clinical outcomes of Japanese heart failure patients with preserved versus reduced left ventricular ejection fraction: a prospective cohort of Shinken Database 2004–2011. J Cardiol. 2013;62(2):102–109. doi:10.1016/j.jjcc.2013.03.013
31. Dzudie A, Hongieh Abanda M, Nkoke C, et al.; THEUS‐HF investigators, Damasceno A. Clinical characteristics and outcomes of black African heart failure patients with preserved, mid‐range, and reduced ejection fraction: a post hoc analysis of the THESUS‐HF registry. ESC Heart Fail. 2021;8(1):238–249. doi:10.1002/ehf2.12903
32. Ho JE, Gona P, Pencina MJ, et al. Discriminating clinical features of heart failure with preserved vs. reduced ejection fraction in the community. Eur Heart J. 2012;33(14):1734–1741. doi:10.1093/eurheartj/ehs070
33. Lee DS, Gona P, Vasan RS, et al. Relation of disease pathogenesis and risk factors to heart failure with preserved or reduced ejection fraction: insights from the Framingham heart study of the national heart, lung, and blood institute. Circulation. 2009;119(24):3070–3077. doi:10.1161/CIRCULATIONAHA.108.815944
34. Meta-analysis Global Group in Chronic Heart Failure (MAGGIC). The survival of patients with heart failure with preserved or reduced left ventricular ejection fraction: an individual patient data meta-analysis. Eur Heart J. 2012;33(14):1750–1757. doi:10.1093/eurheartj/ehr254
35. Kennedy N, Miller P. The spectrum of paediatric cardiac disease presenting to an outpatient clinic in Malawi. BMC Res Notes. 2013;6(1):1–4. doi:10.1186/1756-0500-6-53
36. Martínez-Braña L, Mateo-Mosquera L, Bermúdez-Ramos M, et al. Clinical characteristics and prognosis of heart failure in elderly patients. Revista Portuguesa de Cardiologia. 2015;34(7–8):457–463. doi:10.1016/j.repc.2015.02.002
37. Mori Y, Nishikawa Y, Kobayashi F, Hiramatsu K. Clinical status and outcome of Japanese heart failure patients with reduced or preserved ejection fraction treated with carvedilol. Int Heart J. 2013;54(1):15–22. doi:10.1536/ihj.54.15
38. Macín SM, Perna ER, Canella JP, et al. Differences in clinical profile and outcome in patients with decompensated heart failure and systolic dysfunction or preserved systolic function. Revista Española de Cardiología. 2004;57(1):45–51. doi:10.1016/S0300-8932(04)77060-8
39. Ojeda S, Anguita M, Muñoz JF, et al. Clinical characteristics and medium-term prognosis of patients with heart failure and preserved systolic function. Do they differ in systolic dysfunction? Revista Espanola de cardiologia. 2003;56(11):1050–1056.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.