")
Back to Journals » Drug Design, Development and Therapy » Volume 11
Baracle® vs Baraclude® for 48 weeks in patients with treatment-naïve chronic hepatitis B: a comparison of efficacy and safety
Authors Kim DY , Kim JH, Tak WY , Yeon JE, Lee JH, Yoon JH, Lee YJ, Lee BS, Han BH, Lee HC
Received 15 August 2017
Accepted for publication 20 September 2017
Published 31 October 2017 Volume 2017:11 Pages 3145—3152
DOI https://doi.org/10.2147/DDDT.S149199
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Manfred Ogris
Do Young Kim,1 Ju Hyun Kim,2 Won Young Tak,3 Jong Eun Yeon,4 Joon Hyeok Lee,5 Jung Hwan Yoon,6 Youn Jae Lee,7 Byung Seok Lee,8 Byung Hoon Han,9 Han Chu Lee10
1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, 2Department of Gastroenterology, Gachon University Gil Medical Center, Incheon, 3Department of Internal Medicine, Kyungpook National University Hospital, Daegu, 4Department of Internal Medicine, Korea University Guro Hospital, Seoul, 5Department of Gastroenterology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, 6Department of Internal Medicine, Seoul National University Hospital, Seoul, 7Department of Gastroenterology, Inje University Busan Paik Hospital, Busan, 8Department of Gastroenterology, Chungnam National University Hospital, Daejeon, 9Department of Gastroenterology, Kosin University Gospel Hospital, Busan, 10Department of Internal Medicine, Asan Medical Center, Ulsan University, Seoul, Republic of Korea
Background and objective: Entecavir (ETV) is a standard of care for chronic hepatitis B (CHB). In a bioequivalence study, ETV from Dong-A ST (Baracle®) was found to have a pharmacokinetic profile equivalent to ETV from Bristol-Myers Squibb (BMS) (Baraclude®). The present study was conducted to evaluate the antiviral activity and safety of ETV from Dong-A ST in comparison to ETV from BMS in patients with CHB.
Methods: In this multicenter, double-blind, active-controlled, stratified-randomized, parallel group, comparative trial, 118 treatment-naïve patients with CHB were randomly assigned to receive either 0.5 mg of ETV from Dong-A ST or ETV from BMS once daily for 48 weeks. The primary efficacy endpoint was virologic improvement (a mean reduction from baseline in serum HBV DNA levels) at 24 weeks. Secondary efficacy endpoints included a mean reduction in serum HBV DNA levels at 48 weeks, proportion of patients with undetectable levels of serum HBV DNA, rates of hepatitis B e antigen (HBeAg) loss and seroconversion, rates of HBsAg loss and seroconversion, and rates of normalization of alanine aminotransferase (ALT) levels.
Results: From baseline to week 24, HBV DNA levels (log10) decreased by 4.81 and 4.63 with ETV from Dong-A ST and with ETV from BMS, respectively. The upper limit of two-sided 95% confidence intervals (CI) (equivalent to one-sided 97.5% CIs) for the difference between the treatment groups was 0.208, which was below the noninferiority margin of 1, thus supporting the noninferiority of ETV from Dong-A ST in comparison to ETV from BMS. No statistically significant differences were noted between the treatment groups in all secondary and tertiary efficacy endpoints. Safety profiles were also similar between the two groups.
Conclusion: In patients with previously untreated HBeAg-positive or negative HBV infection, the efficacy of ETV from Dong-A ST was noninferior to that of ETV from BMS, and there were no significant differences in efficacy or safety between two groups.
Keywords: chronic hepatitis B, generic, ETV from Dong-A ST (Baracle®)
Introduction
Hepatitis B is a chronic liver disease caused by hepatotrophic hepatitis B virus (HBV) infection. Approximately 2 billion people worldwide are exposed to HBV and more than 350 million people are chronically infected therewith.1 HBV is also a major cause of cirrhosis and hepatocellular carcinoma (HCC). The prevalence of HBV infection worldwide differs among geographic areas, and proportions of carriers vary from 0.1% to 15%. In Korea, HBV infections have gradually decreased since commercialization of the hepatitis B vaccine (1990s), although 3.7% of the population is still infected.2–4
The goal of chronic hepatitis B (CHB) treatment is to suppress the proliferation of HBV. By inhibiting HBV proliferation, inflammation is relieved, and fibrosis, cirrhosis, liver failure, or HCC can be prevented. Thereby, it is possible to reduce mortality due to liver disease and to improve the survival rate thereof.5 Although the ideal treatment goal is loss of hepatitis B surface antigen (HBsAg), complete treatment of HBV is almost impossible, because nuclear covalently closed circular DNA (cccDNA) remains after treatment. In clinical practice, alanine aminotransferase (ALT) normalization, nondetection of serum HBV DNA, serum hepatitis B e antigen (HBeAg) loss or seroconversion, and histologic improvement are used as treatment response indicators.6
Entecavir (ETV) is a deoxyguanosine nucleoside analog that is converted to its active form, ETV-triphosphate, in vivo. ETV-triphosphate exerts antiviral effects by inhibiting three steps of replication: priming of HBV DNA polymerase, reverse transcription of the HBV DNA negative strand from pregenomic mRNA, and synthesis of the HBV DNA positive strand.7,8
In a Phase III clinical trial, ETV was shown to be superior to lamivudine in terms of histologic improvement, reduction of HBV DNA levels from baseline, proportion of patients with undetectable HBV DNA, and ALT normalization.9,10 ETV is now widely used as a standard therapeutic agent for CHB and is recommended as a first-line treatment by international and domestic guidelines, including the American Association for the Study of Liver Diseases (AASLD), European Association for the Study of the Liver (EASL), Asian Pacific Association for the Study of the Liver (APASL), and Korean Association for the Study of the Liver (KASL).6,11,12
Baracle® is a ETV product developed by Dong-A ST based on a pharmacokinetic profile equivalent to ETV from BMS in bioequivalence tests. However, studies have yet to demonstrate the efficacy and safety of ETV from Dong-A ST in comparison with ETV from BMS for CHB patients. Therefore, the current study was designed to compare the antiviral efficacy and safety between ETV from Dong-A ST (Baracle) and ETV from BMS (Baraclude®) in patients with CHB.
Patients and methods
Study design
This study was conducted as a multicenter, double-blind, active-controlled, randomized with stratification, parallel group, and comparative trial at 18 sites in South Korea from September 2013 to November 2015. As patients with HBeAg positivity or negativity may differ in their responses to antiviral therapy, a stratified randomization was performed to ensure balance between treatment groups.
All subjects who consented to participate in the present trial provided written informed consent and were subjected to screening tests. Within 4 weeks after screening, subjects who were determined to be eligible for the study were randomized with stratification 1:1 to Baracle (ETV 0.5 mg; Dong-A ST Co., Seoul, Republic of Korea) or Baraclude (ETV 0.5 mg; Bristol-Myers Squibb Korea) treatment groups based on HBeAg status (positive/negative). After stratified randomization, subjects were administered either ETV from Dong-A ST or ETV from BMS via one tablet once daily on an empty stomach (2 hours after taking meal or at least 2 hours before taking meal). Each subject took the investigational products (IP) for 48 weeks, during which the subjects visited the clinical trial institution according to the schedule specified in the study protocol, to receive the planned efficacy and safety assessments.
Patients
Inclusion criteria were male and female patients of ages 18–65 years who were diagnosed as HBsAg-positive at the screening visit and had a medical record of CHB for at least 6 months. For those who were diagnosed as HBeAg-positive at the screening visit, HBV DNA levels were ≥1×105 copies/mL, which was quantified through real-time PCR, and for those who were diagnosed as HBeAg-negative, HBV DNA levels were ≥1×104 copies/mL. Subjects were to have ALT levels between 2 times and 10 times the upper limit of the normal (ULN) levels at the screening visit. Subjects with compensated cirrhosis were eligible for the study if their ALT levels were between the ULN and 10 times the ULN levels. Subjects were not administered any antiviral agents, including interferon or pegylated interferon agents, for at least 12 weeks and within 24 weeks prior to screening.
Exclusion criteria included infection with hepatitis C virus (HCV), hepatitis D virus (HDV), human immunodeficiency virus (HIV), decompensated diseases, hematochromatosis, Wilson’s disease, alcoholic liver disease, autoimmune liver disease, and α-1 antitrypsin deficiency. Subjects who were administered immunosuppressive agents or systemic corticosteroids for more than 4 weeks within 24 weeks prior to screening were excluded. Subjects with less than 50 mL/min of creatinine clearance (body weight and age were adjusted by the Cockgraft–Gault method) at the screening visit or subjects with greater than 50 mL/min of α-fetoprotein at the screening visit, who were presumed to have HCC based on the result of the relevant imaging test, were also excluded.
Study assessments
Efficacy
The primary efficacy endpoint was virologic improvement, defined as a change in HBV DNA level (log10) from baseline to week 24 after IP administration.
Secondary efficacy endpoints included virologic endpoints (the proportion of subjects whose HBV DNA levels were less than 300 copies/mL at week 24 and week 48, change in HBV DNA levels [log10] from baseline to week 48), biochemical endpoints (the proportion of subjects whose ALT levels become normal at week 24 and week 48, the proportion of subjects whose HBV DNA levels were less than 300 copies/mL and whose ALT levels became normal at week 48), and serologic endpoints (the proportion of subjects who were HBeAg-positive at the screening visit, but lost HBeAg at week 24 and week 48; the proportion of subjects who were HBeAg-positive at the screening visit, but showed HBeAg seroconversion at week 24 and week 48; the proportion of subjects who showed loss of HBsAg and emergence of anti-HBs at week 48).
The tertiary efficacy endpoint was the proportion of subjects who expressed HBV DNA gene mutations after IP administration, which was confirmed by HBV DNA sequencing.
Safety
Adverse events, such as subjective and objective symptoms, and abnormalities in clinical laboratory tests and vital signs, were assessed. The number and percentage of subjects who experienced ALT flare (≥10X ULN and ≥2X baseline) were also assessed.
Statistical analysis
All efficacy analyses were performed on the full analysis set (FAS) and per-protocol set (PPS). The FAS population included all randomized subjects who received at least one dose of the study drug and had at least one valid post-baseline efficacy evaluation. The PPS population was defined as a subset of the FAS population who completed the study without any major protocol violations.
Assuming a one-sided α level of 0.025 and 80% power, a sample size of 92 patients was estimated with a noninferiority margin of 1. Considering a 20% drop-out rate, the study required a total of 116 patients. For the primary efficacy endpoint, the noninferiority of ETV from Dong-A ST to ETV from BMS was to be supported if the upper limit of the two-sided 95% CI (equivalent to one-sided 97.5% CI) was below the prespecified noninferiority margin of 1.9,10,13,14 Other secondary and tertiary efficacy endpoints were compared between the two treatment groups using Cochran–Mantel–Haenszel test adjusted for a stratification factor, HBeAg (positive/negative), respectively. Differences in the HBV DNA levels (log10) from baseline to week 48 between the two treatment groups were analyzed using ANCOVA with HBeAg (positive/negative) as a stratification factor.
The number (N) and proportion (%) of subjects who lost HBeAg at week 24 and week 48 were compared between the two treatment groups using χ2 test or Fisher’s exact test.
The difference between the two groups with respect to the incidences of adverse events (AEs), adverse drug reactions (ADRs), serious adverse events (SAEs), and serious adverse drug reactions (SADRs) was analyzed using χ2 test of Fisher’s exact test. The number (N) and proportion (%) of subjects with ALT flare (≥10X ULN and ≥2X baseline) were compared using χ2 test or Fisher’s exact test to determine if there was a statistically significant difference between the two groups.
All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Ethics statement
The study was approved by the Institutional Review Boards of each of the 18 participating institutions, including Asan Medical Center (IRB approval number: 2013-0660), The Catholic University of Korea Seoul St Mary’s Hospital (KC13MSMV0402), Gachon University Gil medical Center (GAIRB2013-170), Keimyung University Dongsan Medical Center (DSMC2013-06-034), Konkuk University Medical Center (KUH1010498), Kyungpook National University Hospital (KNUH2013-06-025), Korea University Guro Hospital (KUGH13089), Dong-A University Hospital (13-090), Samsung Medical Center (SMC2013-06-059), Seoul National University Hospital (H-1306-079-498), Severance Hospital Yonsei University (4-2013-0333), Ulsan University Hospital (UUH2013-07-061), Inje University Busan Paik Hospital (13-100), Chonbuk National University Hospital (CUH2013-06-024), Chungnam National University Hospital (CNUH2013-06-007), Kosin University Gospel Hospital (KUGH2014-02-018), Presbyterian Medical Center (2014-06-026), and Hanyang University Medical Center (HYUH2014-05-024). The study was performed in compliance with good clinical practices, according to ICH guidelines.
Results
Baseline characteristics
The mean age of the included patients was 45.8±11.0 years, and male sex was predominant (67.8%). The mean prevalent period of CHB was 11.4±10.8 years, and all patients were treatment-naïve. Forty-seven (39.8%) patients had compensated cirrhosis, and the rate of HBeAg positivity was 59.3%. HBV genotype was C in all patients. There was no significant difference in the baseline characteristics between the ETV from Dong-A ST and ETV from BMS treatment groups (Table 1).
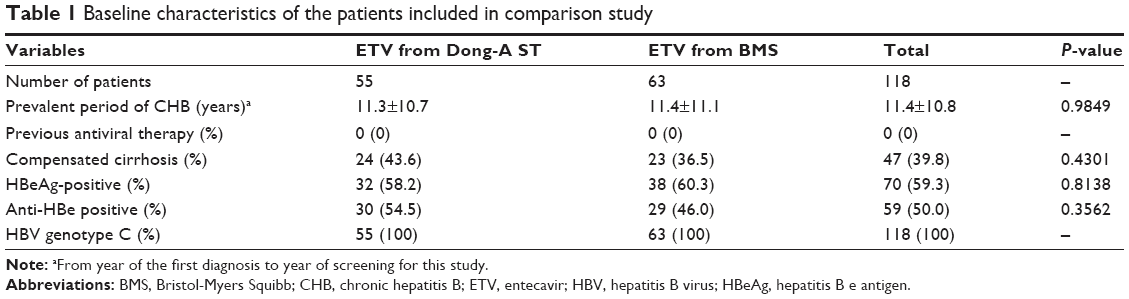 | Table 1 Baseline characteristics of the patients included in comparison study |
Comparison of HBV DNA declines at weeks 24 and 48
Serum HBV DNA levels declined equally at 24 and 48 weeks in both groups. Using the full analysis set, at week 24, the declines in HBV DNA levels from baseline were 4.79 log10 in ETV from Dong-A ST and 4.64 log10 in ETV from BMS group. In ANCOVA analysis with HBeAg as a covariate, which was also a stratification factor, HBV DNA declines from baseline to week 24 were 4.81 log10 in ETV from Dong-A ST and 4.63 log10 in ETV from BMS group. Regarding the differences in HBV decline, the upper limit of two-sided 95% CI (ie, 97.5% one-sided CI) was 0.208, which is less than the noninferiority margin of 1. At week 48, the covariate analysis with HBeAg as a covariate also revealed that HBV DNA decline was not significantly different between the two groups (P=0.6440): 5.0 log10 in ETV from Dong-A ST and 4.9 log10 in ETV from BMS group (Table 2).
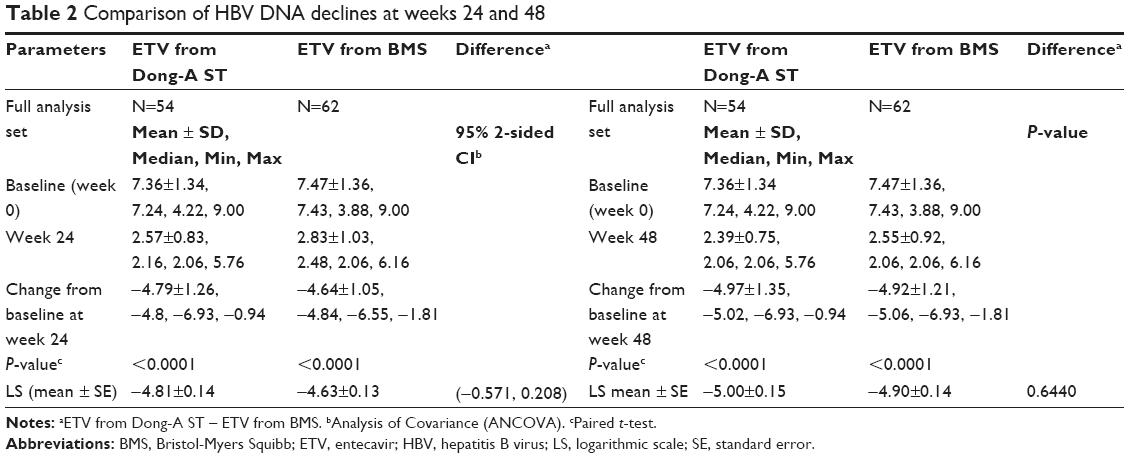 | Table 2 Comparison of HBV DNA declines at weeks 24 and 48 |
Proportion of patients with HBV DNA levels <300 copies/mL at week 48
Figure 1 shows the mean decreases of serum HBV DNA levels during the study period in patients who received either ETV from Dong-A ST or ETV from BMS. There was no significant difference in HBV decline between the two groups during the entire study period. At week 24, 36 (66.7%) patients in ETV from Dong-A ST and 31 (50.0%) in ETV from BMS group achieved HBV DNA less than 300 copies/mL. At week 48, 44 (81.5%) patients in the ETV from Dong-A ST group and 44 (71.0%) in the ETV from BMS group achieved HBV DNA levels less than 300 copies/mL. After adjustment of HBeAg status, we found no significant difference in the proportion of patients with HBV DNA <300 copies/mL at both weeks 24 and 48 (respectively, P=0.0530 and P=0.2128) (Figure 2).
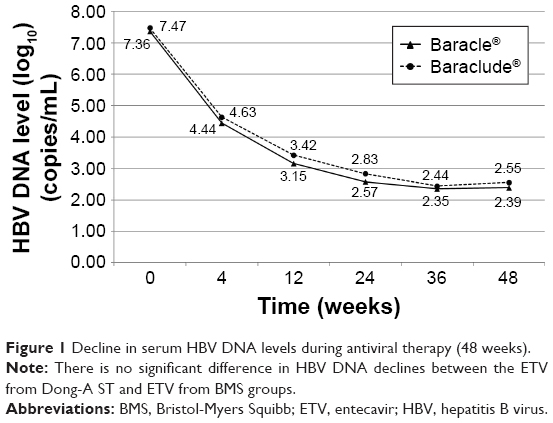 | Figure 1 Decline in serum HBV DNA levels during antiviral therapy (48 weeks). |
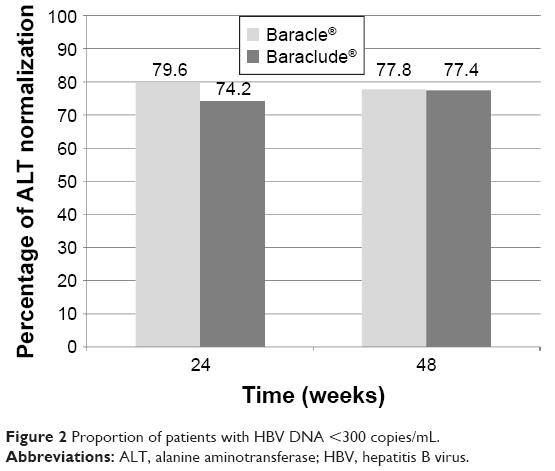 | Figure 2 Proportion of patients with HBV DNA <300 copies/mL. |
ALT normalization and HBeAg loss
For all included patients, the rates of ALT normalization were 79.6% in the ETV from Dong-A ST group and 74.2% in the 3 ETV from BMS group at week 24, which was not statistically different (P=0.5131). At week 48, the rates were 77.8% in the ETV from Dong-A ST group and 77.4% in the ETV from BMS group (P=0.9851) (Figure 3). Regarding HBeAg loss during antiviral therapy, 3 (10.0%) patients in the ETV from Dong-A ST group and 3 (8.3%) patients with HBeAg-positive in the ETV from BMS group showed HBeAg loss at week 24. No other patients achieved HBeAg loss or seroconversion thereafter (Figure 4).
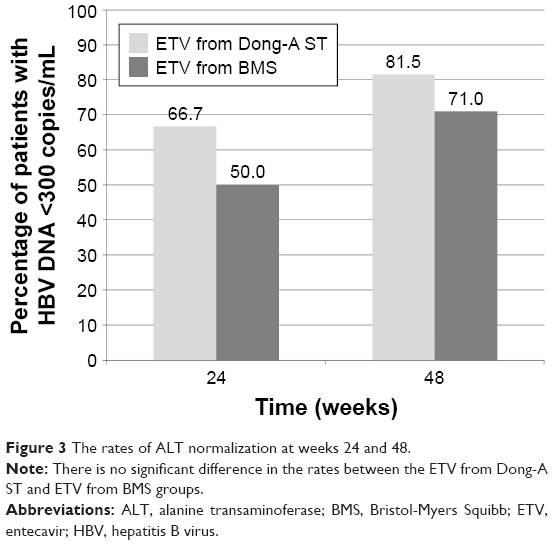 | Figure 3 The rates of ALT normalization at weeks 24 and 48. |
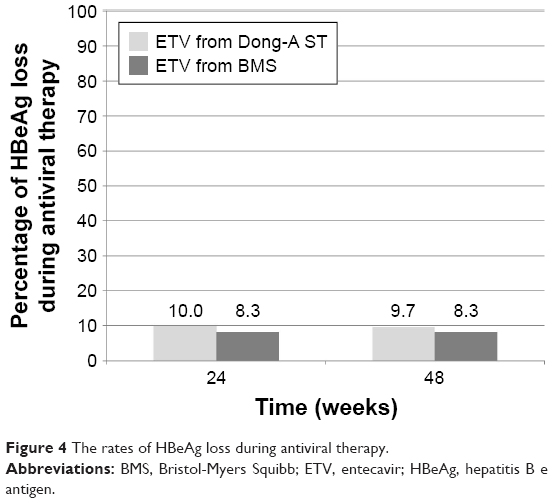 | Figure 4 The rates of HBeAg loss during antiviral therapy. |
Adverse events
All adverse events were presented after standardization into system organ classes (SOC) and preferred terms (PT) using MedDRA (Version 16.0) (Table 3). There was a total of 47 adverse events (AE; Any untoward medical occurrence in a patient or clinical investigation subject administered a pharmaceutical product, which does not necessarily have a causal relationship with this treatment) from 24 (43.6%) patients in the ETV from Dong-A ST group and 73 AEs from 31 (50.0%) patients in the ETV from BMS group (P=0.4912). Mild, moderate, and severe AEs occurred in 37, 8, and 2 cases in the ETV from Dong-A ST group and in 62, 9, and 2 cases in the ETV from BMS group. Adverse drug reactions (ADRs; All noxious and unintended responses to a medicinal product related to any dose) were observed in one case in the ETV from Dong-A ST group and two cases (from 1 patient) in the ETV from BMS group. There were four cases of serious AEs (SAEs; AE which results in death, life-threatening conditions, inpatient hospitalization, prolongation of existing hospitalization, persistent/significant disability/incapacity, or a congenital anomaly/birth defect) seen in three patients (5.5% and 4.8%) in each of the ETV from Dong-A ST and ETV from BMS groups. There was no serious ADR (SADR; ADR which results in death, life-threatening condition, inpatient hospitalization, prolongation of existing hospitalization, persistent/significant disability/incapacity, or a congenital anomaly/birth defect) in either group.
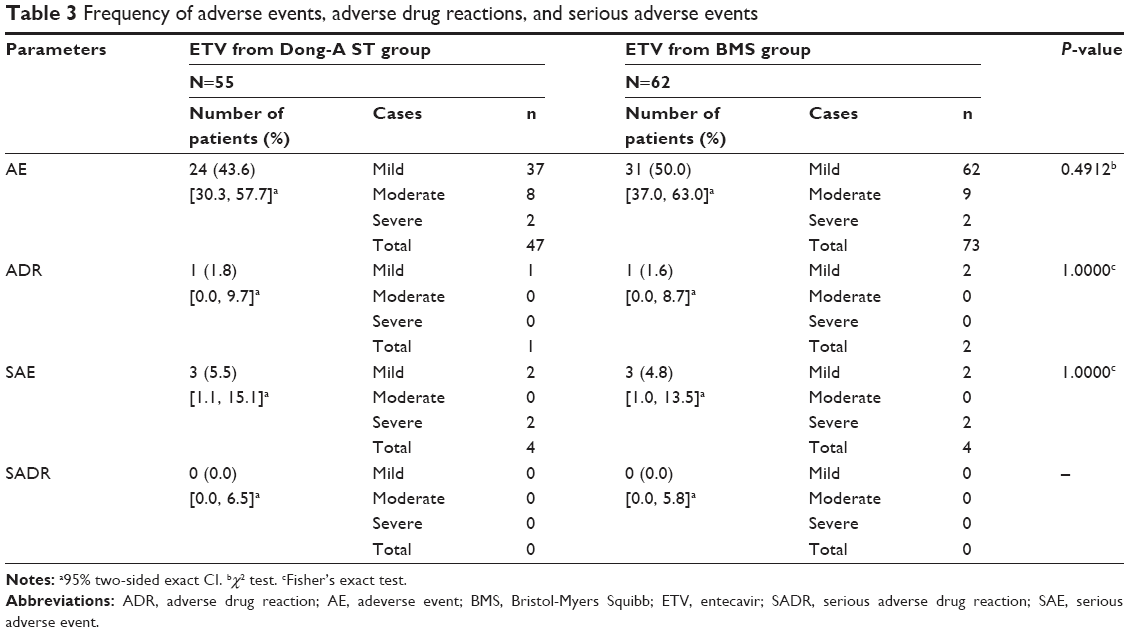 | Table 3 Frequency of adverse events, adverse drug reactions, and serious adverse events |
Discussion
CHB imposes a significant global health care burden; approximately 5% of individuals throughout the world are estimated to be infected with HBV, and the annual mortality associated with persistent HBV infection is about 1.2 million.15 International guidelines recommend ETV together with tenofovir (TDF) as the first-line therapy in the treatment of naïve CHB patients because of its potent antiviral activity and higher genetic barrier.9,10,12 Continuous suppression of HBV replication is clinically important as the risk of cirrhosis and/or HCC in CHB patients increases proportionally with increases in serum HBV DNA concentrations.16,17 Indeed, since the introduction of ETV in clinical practice, there have been many studies showing the long-term clinical benefits of ETV in terms of prevention of CHB progression (ie, cirrhosis or HCC).18,19
In the current study, we observed no differences in suppression of HBV replication and safety between those taking ETV from Dong-A ST and ETV from BMS. The change in HBV DNA levels (log10) from baseline to week 24, which was the primary endpoint of study, was 4.81 log10 in ETV from Dong-A ST and 4.63 log10 in ETV from BMS group, confirming that ETV from Dong-A ST is not inferior to ETV from BMS. At week 48, declines in HBV DNA were also not significantly different between the two groups (P=0.6440): 5.0 log10 in the ETV from Dong-A ST and 4.9 log10 in the ETV from BMS group. The proportions of patients with HBV DNA <300 copies/mL at weeks 24 and 48 were also not different between the two groups (66.7% vs 50.0% at week 24, 81.5% vs 71.0% at week 48). Thus, the overall antiviral activity was deemed to be comparable between ETV from Dong-A ST and ETV from BMS. In particular, the rates of undetectable serum HBV DNA levels in the present study were similar with ETV pivotal clinical trials, wherein the rates were 67% in HBeAg-positive patients and 90% in HBeAg-negative patients.9,10
Because of relatively short treatment period of 1 year, the rates of HBeAg loss might not be fully evaluated or compared in HBeAg-positive patients. Nonetheless, the HBeAg loss rates at week 48 were not different between two groups: 9.7% in ETV from Dong-A ST and 8.3% in ETV from BMS group.
A major concern regarding generic antiviral agent for HBV infection would be whether it can show bioequivalence, comparable efficacy, and safety in real patients. First, ETV from Dong-A ST demonstrated an equivalent pharmacokinetic profile to ETV from BMS in bioequivalence tests. When ETV from Dong-A ST or ETV from BMS 0.5 mg Tab was administered in 36 healthy male adults, the two-sided 90% CI of Cmax and AUCt were 1.0366–1.1740 and 0.9605–1.1149, respectively. Thus, it was confirmed that they were within the acceptable bioequivalence range of 0.80–1.25. Second, in this multicenter, prospective randomized trial, antiviral potency indicated by serum HBV DNA declines at weeks 24 (primary endpoint) and 48 (secondary endpoint) and the proportions of patients with HBV DNA <300 copies/mL (secondary endpoint) were not different between the two drugs. Lastly, there was a similar safety profile in the ETV from Dong-A ST and ETV from BMS groups. Most of adverse events were mild, and there were rare ADRs or SAEs. In addition, there was no case of SADR. In particular, ETV is known not to be related to nephrotoxicity or loss of bone density. In our study, both ETV from Dong-A ST and from BMS did not result in elevation of serum creatinine or decrease of glomerular filtration rate (GFR) during study period (data not shown).
Although regulation authority does not request a manufacturer to conduct clinical trials to approve a generic drug, data comparing efficacy and safety between generic and branded drugs are sometimes necessary. This is because, in a survey, 25% of physicians stated that they would only increase prescribing generic drugs if additional clinical trials were presented.20
This study has a strength in that efficacy and safety were compared between original and generic anti-HBV drugs by a well-designed randomized trial. This is the first report to show the comparable efficacy and safety of generic anti-HBV drug. A limitation of this study is a relative short (1 year) duration of drug administration, which may not allow for the comparison of long-term virologic and/or biochemical responses between the two drugs.
Conclusion
In conclusion, we demonstrated that ETV from Dong-A ST is not inferior to ETV from BMS in treatment-naïve HBeAg (+) or HBeAg (−) patients in terms of HBV DNA reduction, rates of HBeAg seroconversion, ALT normalization, and efficacy profile.
Acknowledgments
This study was sponsored by Dong-A ST Co., the manufacturer of Baracle®. Dong-A ST Co. made significant contributions to the design and analysis of the study, and assisted in preparation of research grant applications. The following investigators and institutions participated in the study: Han Chu Lee (Asan Medical Center), Si Hyun Bae (The Catholic University of Korea Seoul St Mary’s Hospital), Ju Hyun Kim (Gachon University Gil medical Center), Jae Seok Hwang (Keimyung University Dongsan Medical Center), So Young Kwon (Konkuk University Medical Center), Won Young Tak (Kyungpook National University Hospital), Jong Eun Yeon (Korea University Guro Hospital), Sang Young Han (Dong-A University Hospital), Joon Hyeok Lee (Samsung Medical Center), Jung Hwan Yoon (Seoul National University Hospital), Do Young Kim (Severance Hospital Yonsei University), Neung Hwa Park (Ulsan University Hospital), Youn Jae Lee (Inje University Busan Paik Hospital), Sung Hoon Kim (Chonbuk National University Hospital), Byung Seok Lee (Chungnam National University Hospital), Byung Hoon Han (Kosin University Gospel Hospital), Yong Geun Cho (Presbyterian Medical Center), and Dae Won Chun (Hanyang University Medical Center). None of the investigators have a conflict of interest with regard to this study.
Disclosure
The authors report no conflicts of interests in this work.
References
Papatheodoridis GV, Idilman R, Dalekos GN, et al. The risk of hepatocellular carcinoma is decreasing after the first 5 years of entecavir or tenofovir in Caucasians with chronic hepatitis B. Hepatology. Epub 2017 Jun 16. | ||
Chae HB, Kim JH, Kim JK, Yim HJ. Current status of liver diseases in Korea: hepatitis B. Korean J Hepatol. 2009;15(Suppl 6):S13–S24. | ||
Korea Centers for Disease Control and Prevention. 2006 disease Control White Paper. Cheongju: Korea Centers for Disease Control and Prevention; 2007:144. | ||
Ministry of Health & Welfare, Korea Centers for Disease Control and Prevention. The third Korea National Health and Nutrition Examination Survey (KNHANES III). 2005: Health Examination. Ministry of Health & Welfare; 2006:68. | ||
Sohn W, Cho JY, Kim JH, et al. Risk score model for the development of hepatocellular carcinoma in treatment-naive patients receiving oral antiviral treatment for chronic hepatitis B. Clin Mol Hepatol. 2017;23(2):170–178. | ||
KASL clinical practice guidelines: management of chronic hepatitis B. Clin Mol Hepatol. 2016;22(1):18–75. | ||
Soriano V, Barreiro P, Benitez L, Pena JM, de Mendoza C. New antivirals for the treatment of chronic hepatitis B. Expert Opin Investig Drugs. 2017;26(7):843–851. | ||
Seifer M, Hamatake RK, Colonno RJ, Standring DN. In vitro inhibition of hepadnavirus polymerases by the triphosphates of BMS-200475 and lobucavir. Antimicrob Agents Chemother. 1998;42(12):3200–3208. | ||
Chang TT, Gish RG, de Man R, et al. A comparison of entecavir and lamivudine for HBeAg-positive chronic hepatitis B. N Engl J Med. 2006;354(10):1001–1010. | ||
Lai CL, Shouval D, Lok AS, et al. Entecavir versus lamivudine for patients with HBeAg-negative chronic hepatitis B. N Engl J Med. 2006;354(10):1011–1020. | ||
Terrault NA, Bzowej NH, Chang KM, Hwang JP, Jonas MM, Murad MH. AASLD guidelines for treatment of chronic hepatitis B. Hepatology. 2016;63(1):261–283. | ||
European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67(2):370–398. | ||
Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al. Adefovir dipivoxil for the treatment of hepatitis B e antigen-negative chronic hepatitis B. N Engl J Med. 2003;348(9):800–807. | ||
Marcellin P, Chang TT, Lim SG, et al. Adefovir dipivoxil for the treatment of hepatitis B e antigen-positive chronic hepatitis B. N Engl J Med. 2003;348(9):808–816. | ||
World Health Organization. Hepatitis B. World Health Organization Fact Sheet 204 (Revised October 2000). Geneva: WHO; 2000. | ||
Chen CJ, Yang HI, Su J, et al. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. Jama. 2006;295(1):65–73. | ||
Iloeje UH, Yang HI, Su J, Jen CL, You SL, Chen CJ. Predicting cirrhosis risk based on the level of circulating hepatitis B viral load. Gastroenterology. 2006;130(3):678–686. | ||
Yang SC, Lee CM, Hu TH, et al. Virological response to entecavir reduces the risk of liver disease progression in nucleos(t)ide analogue-experienced HBV-infected patients with prior resistant mutants. J Antimicrob Chemother. 2013;68(9):2154–2163. | ||
Zoutendijk R, Reijnders JG, Zoulim F, et al. Virological response to entecavir is associated with a better clinical outcome in chronic hepatitis B patients with cirrhosis. Gut. 2013;62(5):760–765. | ||
Kersnik J, Peklar J. Attitudes of Slovene general practitioners towards generic drug prescribing and comparison with international studies. J Clin Pharm Ther. 2006;31(6):577–583. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.