")
Back to Journals » Journal of Pain Research » Volume 15
Balloon Kyphoplasty vs Vertebroplasty: A Systematic Review of Height Restoration in Osteoporotic Vertebral Compression Fractures
Authors Patel N, Jacobs D, John J, Fayed M, Nerusu L, Tandron M, Dailey W, Ayala R, Sibai N, Forrest P, Schwalb J, Aiyer R
Received 24 October 2021
Accepted for publication 28 March 2022
Published 27 April 2022 Volume 2022:15 Pages 1233—1245
DOI https://doi.org/10.2147/JPR.S344191
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Michael A Ueberall
Nimesh Patel,1 David Jacobs,1 Jessin John,1 Mohamed Fayed,1 Lakshmi Nerusu,2 Marissa Tandron,2 William Dailey,2 Ricardo Ayala,2 Nabil Sibai,1,2 Patrick Forrest,1,2 Jason Schwalb,2,3 Rohit Aiyer1,2
1Department of Anesthesiology, Pain Management and Perioperative Medicine, Henry Ford Health System, Detroit, MI, USA; 2Department of School of Medicine, Wayne State University School of Medicine, Detroit, MI, USA; 3Department of Neurological Surgery, Henry Ford Health System, Detroit, MI, USA
Correspondence: Nimesh Patel, Department of Anesthesiology, Pain Management and Perioperative Medicine, Henry Ford Health System, 2799 W Grand Blvd, Detroit, MI, 48202, USA, Tel +1 313-932-5756, Fax +1 313-916-9434, Email [email protected]
Purpose of Review: This systematic review comprehensively compared balloon kyphoplasty and vertebroplasty with respect to height restoration and pain relief.
Recent Findings: PRISMA guidelines were utilized to compare balloon kyphoplasty and vertebroplasty, focusing on the primary outcome of height restoration and the secondary outcomes of pain relief and functionality. A total of 33 randomized controlled trials were included; 20 reviewed balloon kyphoplasty, 7 reviewed vertebroplasty, and 6 compared vertebroplasty to balloon kyphoplasty. Both treatments restored some vertebral body height and showed benefits in pain reduction and improved patient-reported functionality.
Summary: Balloon kyphoplasty and vertebroplasty are effective treatments for vertebral compression fractures and this review suggests that balloon kyphoplasty may be favored for vertebral height restoration. Further studies are needed to conclude whether balloon kyphoplasty or vertebroplasty is superior for alleviating pain.
Keywords: chronic pain, compression fracture, kyphoplasty, low back pain, pain management, post-operative pain, vertebroplasty
Introduction
Osteoporotic vertebral compression fractures (OVCF) are common sequelae of osteoporosis, accounting for 700,000 cases annually in the United States.1 Of these, about one-third are symptomatic, often presenting as acute or chronic low back pain.2
Conservative approaches such as non-steroidal anti-inflammatory drugs (NSAIDs), mild opioids, lumbosacral orthotic compressor belts, physical therapy, bed rest, and tincture of time are commonly used for OVCF management, unless there is neurological compromise or evidence of instability.3 However, for many patients, conservative management is often insufficient and results in significant morbidity, leading to loss of work hours, decreased functional independence, and chronic pain.4 Furthermore, insufficient vertebral height can cause sequelae of spinal deformities, reduced pulmonary function, depression, reduced mobility, and poorer quality of life, underscoring the importance of surgical correction.5–7
Balloon kyphoplasty and vertebroplasty have been found to be beneficial for restoration of bone height in chronic back pain refractory to conventional therapies. Tsoumakidou et al published guidelines in 2017 on vertebral augmentation indications. The indications for percutaneous vertebroplasty include painful vertebral compression fractures (either refractory to medical treatment or secondary to benign bone tumors), osteolytic processes, and osteonecrosis. Additional indications include symptomatic vertebra plana, acute stable fractures, chronic fractures with non-union or internal cystic changes, need for vertebral body or pedicle reinforcement prior to surgical stabilization, and traumatic acute vertebral compression fracture with a local kyphotic angle greater than 15 degrees.7,9
The placement of acrylic cement (specifically polymethylmethacrylate [PMMA]) percutaneously for diseases of the spine has been described since the 1980s. Vertebroplasty for osteoporotic compression fractures started developing in the 1990s, with case reports describing marked pain relief after the procedure with minimal complications.5 Multiple clinical trials have been conducted to determine the outcomes of vertebroplasty. A study published by Farrokhi et al in 2011 determined that vertebroplasty restored vertebral body height and provided significant pain relief compared to conservative management.6
Balloon kyphoplasty, a surgical process involving an inflatable balloon, is another method to treat vertebral compression fractures. This method was initially attempted in the 1990s by Dr. Mark Reiley using a Kyphx inflatable balloon tamp device.8 The procedure is generally performed through a unipedicular or bipedicular approach, where cannulas are placed percutaneously adjacent to each collapsed vertebral body. Studies have been conducted to determine the clinical outcome and effectiveness of balloon kyphoplasty compared to conservative treatment. Li et al found that patients who underwent kyphoplasty had decreased post-procedure pain scores and had statistically significant height restoration compared to preoperative measures and to patients who underwent conservative treatment.9 Jin et al found similar outcomes for height and pain scores in a study published in 2018.10 They determined that balloon kyphoplasty patients had greater improvement in pain scores, height restoration, and rate of bone union and lower kyphosis angles at 1-year follow-up compared to patients who had conservative treatment alone.10
Two major prospective, blinded, randomized trials failed to show any improvement in pain or physical function with cement injection over injection of local anesthetic into the zygapophysial joints up to 6 months after the procedure.11,12 Nonetheless, balloon kyphoplasty and vertebroplasty may be beneficial for restoration of bone height in patients with chronic back pain refractory to conventional therapies, or it may at least prevent future vertebral collapse and further deformity. There is justified hope that the long-term effects of vertebral augmentation may be better than conservative management in certain subpopulations.
This systematic review seeks to provide a comprehensive appraisal and comparison of balloon kyphoplasty and vertebroplasty, focusing on the primary outcome of height restoration as well as investigating the secondary outcomes of pain relief and functionality. This study is unique and robust for a variety of reasons. First, our study critically investigated whether there is any correlation between height restoration and pain relief. Second, we reviewed several secondary outcomes, including pain, functionality, kyphosis angle restoration, wedge angle restoration, cement leakage, Gardner’s angle, and Cobb’s angle. Third, we only included randomized controlled trials (RCTs) to make the analysis more robust and clinically applicable. Fourth, we aimed to provide an update on the literature that compares kyphoplasty versus vertebroplasty for height restoration as well as for pain relief and function. Finally, we searched 6 databases to ensure that this review was comprehensive.
Methods
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Protocols Statement issued in 2015.13
Literature Search
An initial literature search was performed on March 25, 2020 within the Henry Ford Health System library system to identify relevant studies in electronic databases, PubMed/MEDLINE (1946 to June 2020), Embase (1974 to June 2020), Web of Science (1954 to March 2020), Cochrane Library (including Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Reviews [1970 to June 2020]), ClinicalTrials.gov (2008 to March 2020), and CINAHL (1937 to June 2020) to retrieve RCTs. This identified 1752 articles with 504 duplicates between the databases, for a total of 1248 articles that were screened. The Mesh strategy that was used can be found in the appendices. An add-on literature search was performed on June 26, 2020, without the term height or height restoration. This resulted in an additional 4214 articles. When duplicates were removed 2899 articles were screened in addition to the 1248 previous articles for a total of 4147 that were screened.
The search was performed by the librarians using medical subject headings (MESH) of kyphoplasty, vertebroplasty, vertebral height restoration, vertebral height restoration, spinal fracture, and vertebral compression fracture. Two independent librarians completed a literature review of articles from 1937 to June 2020, with their results compiled. An example of one search strategy used is the following: (((((((“Kyphoplasty”[Mesh]) OR kyphoplasty)) OR ((“Vertebroplasty”[Mesh]) OR vertebroplasty))) AND (((((“vertebral height restoration”) OR vertebral-height-restoration) OR vertebral height restoration) OR restoration of vertebral height) OR vertebrae height restor*)) AND (((vertebral compression fracture) OR ((“Fractures, Compression”[Mesh]) AND (vertebr* OR spine OR spinal))) OR ((“Spinal Fractures”[Mesh]) AND (compress*)))). The full electronic search strings used by the research librarian staff to perform this search are included in Appendix 1. Add-on search included the same search string without height or height restoration, which is also provided in Appendix 1.
Study Selection
Only RCTs published in English was included in this systematic review. Exclusion criteria for this study were as follows: systematic reviews, observational studies, case reports, editorials, case series, non-human (animal) studies, cadaver models, non-English language studies, inclusion of patients with vertebral compression fractures other than osteoporosis, and studies of kyphoplasty and/or vertebroplasty that did not look at outcome measures of vertebral height restoration.
We pre-specified eligibility criteria using the population, intervention, comparator, and outcomes (PICO) approach as follows:
Participants: Only trials with participants above the age of 18 years with OVCF as the primary indication for treatment with balloon kyphoplasty and vertebroplasty were included in this systematic review.
Interventions and Comparators: Intervention was defined as balloon kyphoplasty or vertebroplasty. Comparators were any other intervention or surgical technique used for vertebral augmentation.
Outcomes: The primary outcome was height restoration with statistical significance. Secondary outcomes of pain relief, functionality, cement leakage, Cobb’s Angle, wedge angle restoration, kyphosis angle restoration, and Gardner’s angle.
Six authors (NP, JJ, MT, LN, WD, RA) reviewed all trials for screening selection and extraction. Any discrepancies for qualification for the systematic review between the six reviewers were discussed and resolved together, as well as further discussion and review with the primary investigator, RA if there were any secondary discrepancies. A total of 5966 articles were retrieved from the broad search terms used. Identifying and excluding duplicate records resulted in 4147 articles. Titles and abstracts were then screened, resulting in 3909 articles that were excluded. The full text of 238 articles was then assessed for eligibility, and all studies apart from RCTs for osteoporotic vertebral compression fractures without statistical analysis were removed. This resulted in a final number of 33 articles that were included in the study. The PRISMA flow diagram can be reviewed in Figure 1. We confirmed our search strategy by also reviewing all the studies identified by previous systematic reviews with a similar topic to ensure that no article was missed for inclusion.14–16
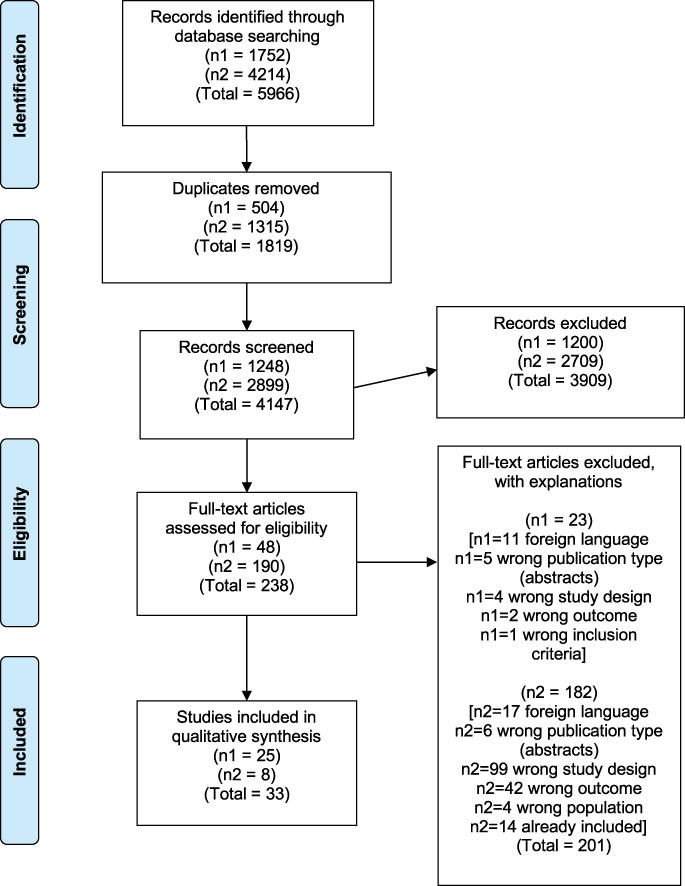 |
Figure 1 PRISMA flow chart of vertebral height restoration in osteoporotic vertebral compression fractures after vertebroplasty or kyphoplasty.19 |
Risk of Bias Assessment for Individual Trials
Two authors (NP and RA) independently assessed the risk of bias for each study included in this systematic review (Appendices 2 and 3). The risk of bias graph and summary were created with the use of RevMan 5.4.1 software, which was downloaded online.17 Creation of the graph was created by both authors classifying different specific biases to come up with an overall bias as either high, low, or unclear.
Data Extraction and Quality Assessment
Only RCTs were included in this systematic review. The Harden model was used to categorize studies into different levels of review.18 Only level II studies were included, which is defined as “one or more well powered randomized, controlled trials.” The purpose of this review was to present a comprehensive review of all the literature available for height restoration after vertebroplasty or kyphoplasty for patients with OVCF.
For all included studies, study characteristics and outcomes were placed into summary tables and independently extracted by at least 2 reviewers. Specifically, the primary author’s name, year, sample sizes, study duration, treatment and comparison group, mean age, type of fracture, fracture age, unipedicular versus bipedicular approach, cement volume, and incidence of cement extravasation were recorded. Recorded primary clinical outcome measures included the following: vertebral body height restoration (anterior, middle, posterior), wedge angle, kyphosis angle, and Cobb’s angle. Recorded secondary clinical outcome measures included the following: visual analogue scale (VAS), Oswestry Disability Index (ODI), life ability score, EQ5D, Roland-Morris Disability Questionnaire (RDQ), EuroQol Visual Analogue Scale (EQ-VAS), and Short Form-36 (SF-36) [PF, MH)]. Continuous data were reported with timeframes of post-operative 1, 6, 12, 24, and 36 months, when available.
Results
The comprehensive results of the data are summarized in Tables 1 and 2 and Supplementary Tables S1–S3 . A total of 33 RCTs were included in this study. Of the 33 studies, 20 reviewed balloon kyphoplasty, 7 reviewed vertebroplasty, and 6 compared vertebroplasty to balloon kyphoplasty head-to-head. It should be noted that the Noriega study (2019) is a 3-year follow-up of the original study published in 2016.
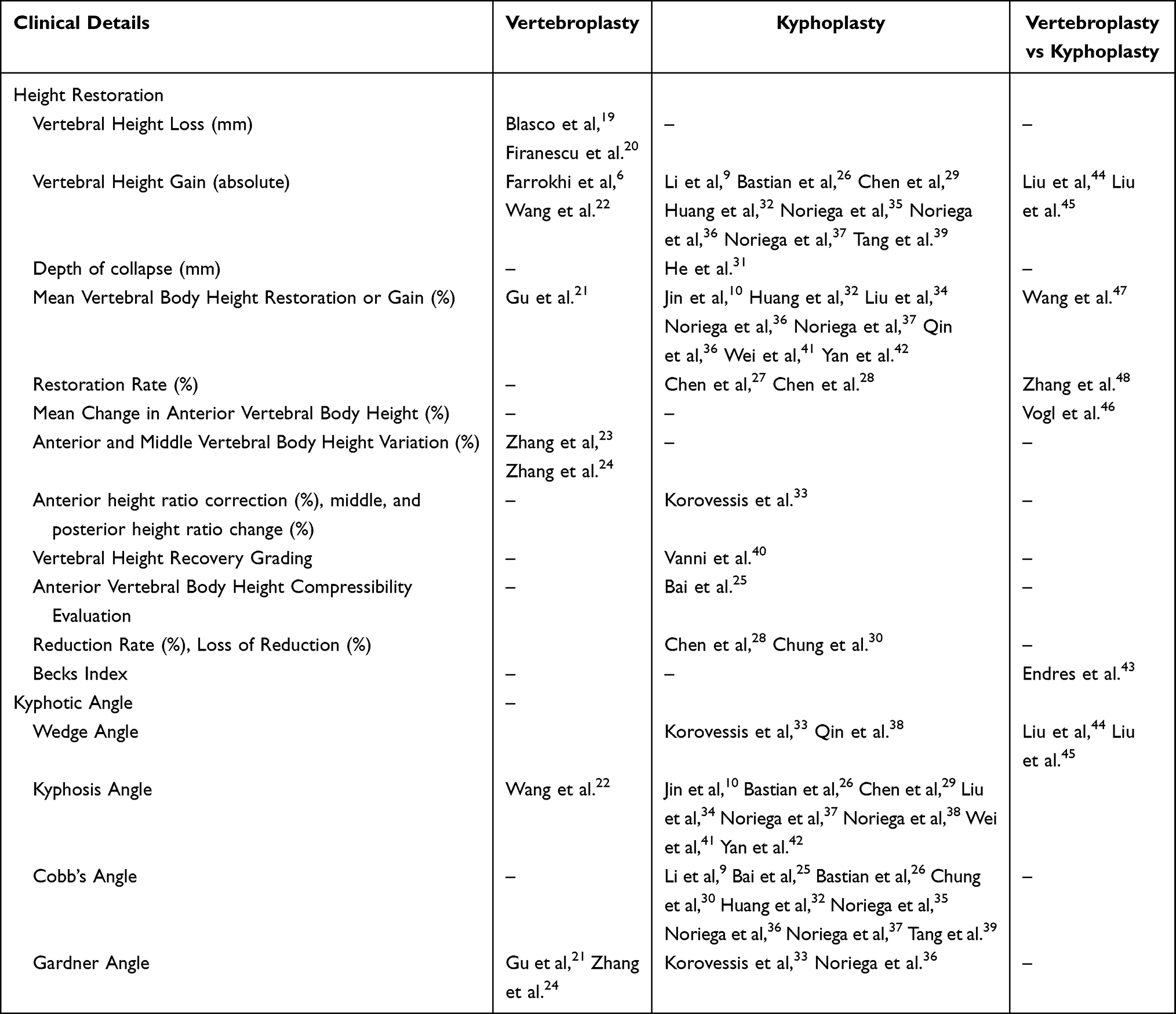 |
Table 1 Reference Guide for Citations and Outcome |
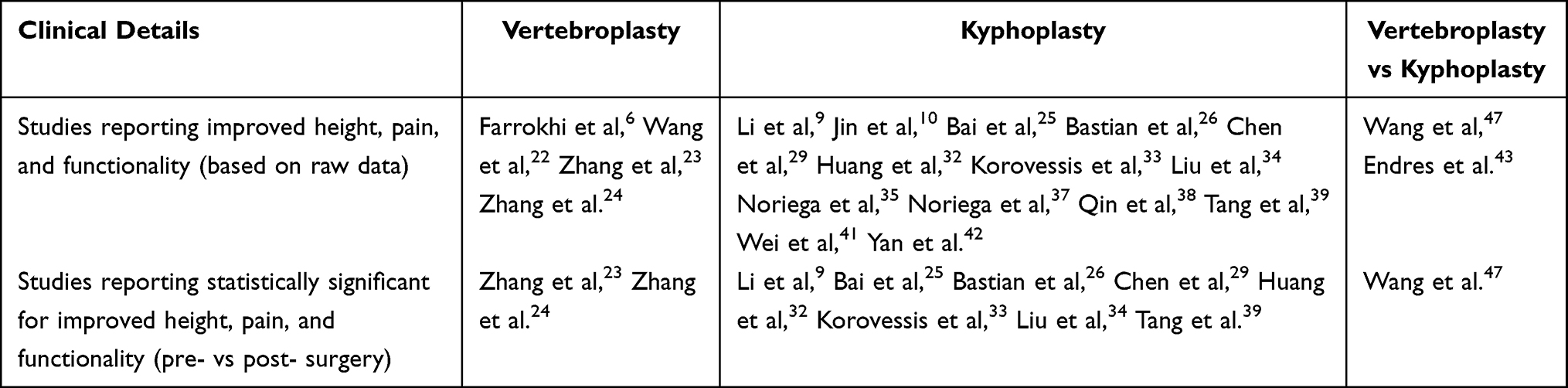 |
Table 2 Number of Studies with Improvements of Vertebral Height, Pain, and Functionality |
Primary Outcome
Vertebral Height Restoration
A total of 7 studies investigated vertebral height restoration in patients undergoing vertebroplasty.6,19–24 Of these studies, 2 reported vertebral height loss, 1 reported mean vertebral height restoration, 2 investigated vertebral body height variation, and 2 reported absolute vertebral height gain (Table 1).6,19–24 Wang et al reported a significantly greater vertebral height at 1 month post-procedure compared to conservative treatment.22 Farrohki et al reported significant height restoration that was maintained to 36 months.6 Firanescu et al reported that 118 vertebroplasty patients developed 0–3 mm of further height loss and did not specifically report height restoration.20 Blasco et al reported no significant height reduction in the vertebroplasty or conservative group at 12 months and did not specifically report height restoration.19 In 2 studies by Zhang et al from 2015, depending on the vertebroplasty technique used, post-operative anterior and middle vertebral body height variation ranged from 47.3–54.0% and 45.6%-59.6%, respectively.23,24 Gu et al reported significant postoperative increases in central and anterior mean vertebral body height compared to preoperative values (P < 0.005) but also reported significant decreases in central and anterior vertebral body height (P < 0.005) 2 years after treatment compared to immediately after treatment.21 Overall, the most favorable findings were reported in the 2 studies measuring absolute vertebral body height gain, which improved significantly after vertebroplasty.6,22
A total of 20 studies investigated vertebral height restoration with balloon kyphoplasty as at least one of the treatment arms.9,10,25–42 None of these studies reported vertebral height loss, 8 studies reported vertebral height restoration, 8 studies reported absolute vertebral height restoration, 2 studies reported restoration rate, 1 study reported vertebral height loss rate, 1 study reported post-operative reduction rate, 1 study reported anterior vertebral body height compressibility evaluation, 1 study reported vertebral height recovery grading, and 1 study reported anterior, middle, and posterior height ratio change.9,10,25–42 All studies with outcomes of vertebral height restoration reported improvements in vertebral height after balloon kyphoplasty, except in Vanni et al’s study where 16% of kyphoplasty patients had no change after their procedure.10,32,34,36–38,40–42 All but one study with pre- and postoperative outcomes of absolute height demonstrated significant improvements in kyphoplasty postoperatively, with Chen et al showing anterior and middle height improvements up to 24 months.9,26,29,32,35,39 Noriega et al’s 2016 paper did not report a significant postoperative correction in height for anterior, middle, and posterior height.36 Of note, one of Noriega et al’s 2019 studies presented the 3-year follow-up data from Noriega et al’s 2016 study.36,37
A total of 6 studies compared balloon kyphoplasty head-to-head with vertebroplasty and reported percent restoration, restoration recovery rate, absolute change in height, or Beck index.43–48 In Vogl et al’s study examining height maintenance, a mean cement volume of 3.77 ± 0.69 mL was injected in the kyphoplasty group compared to 3.99 ± 1.10 mL in the vertebroplasty group, and 3 months after treatment, vertebral body maintenance was equivalent in both groups and there was a smaller mean change in anterior height in the kyphoplasty arm, though this was not statistically significant compared to the vertebroplasty arm.46 Liu et al’s initial study in 2010 reported a mean cement volume of 5.56 ± 0.62 mL injected in the kyphoplasty group compared to 4.91 ± 0.65 mL in the vertebroplasty group, and there were statistically significant increases in vertebral body height in both the kyphoplasty and vertebroplasty group on post-operative day 3, with larger height gains in the kyphoplasty group.45 In Liu et al’s follow-up study, both groups had statistically significant improvements in mean vertebral body height 3 days, 1 year, 2 years, and 5 years postoperatively compared to preoperative values, with larger vertebral body height gains achieved in the kyphoplasty group.44 Wang et al reported a mean cement volume of 4.22 mL injected in the kyphoplasty group compared to 3.31 mL in the vertebroplasty group, and both the vertebroplasty and kyphoplasty groups demonstrated statistically significant improvements in vertebral height at 1-year follow-up, with a significantly greater mean restoration in the kyphoplasty group.47 Zhang et al’s study comparing vertebroplasty to kyphoplasty reported a mean cement volume of 4.60 ± 1.00 mL injected in the kyphoplasty group compared to 3.41 ± 1.30 mL in the vertebroplasty group, and at 1-year follow-up, the vertebral height recovery rate in the vertebroplasty group was 16.14 ± 3.33% compared to 26.24 ± 2.12% in the kyphoplasty group, which was a statistically significant difference.48 Endres et al reported a mean cement volume of 3.1 mL injected in the vertebroplasty group and 3.9 mL in the balloon kyphoplasty group and compared the pre- and postoperative Beck index (anterior edge height/posterior edge height) between balloon kyphoplasty, shield kyphoplasty, and vertebroplasty and did not find any significant change in the Beck index at 6-month follow-up, correlating with no significant increase in vertebral body height.43 Overall, 3 of the 6 head-to-head studies demonstrated a correlation between larger volume of cement injected and improved vertebral body height, favoring balloon kyphoplasty, and 5 of the 6 head-to-head studies favored balloon kyphoplasty for height restoration, with 2 of these studies showing a statistically significant between-group difference.44–48
Secondary Outcomes
Pain
A total of 6 studies reported preoperative and postoperative VAS scores for patients who received vertebroplasty.6,19,21–24 Collectively, all patients in the 6 vertebroplasty studies demonstrated reduced postoperative pain scores. Of note, 3 studies reported sustained pain relief to at least 12 months, with the longest duration of 36 months reported by Farrokhi et al.6,19,21,24
In our review, 18 of 20 balloon kyphoplasty studies reported preoperative and postoperative VAS scores.9,10,25,27–39,41,42 Of these 18 studies, 12 reported follow-up of 12 months or more, and 6 studies demonstrated sustained VAS score reductions at 12 months.10,28–30,33–37,41,42 Korovessis et al reported sustained VAS score reductions at 14 months, Chung et al reported sustained VAS score reductions at 16.6 months, Chen et al’s 2011 study and Chen et al reported sustained VAS score reductions at 24 months, and Noriega et al’s 2019 paper reported sustained VAS score reductions at 36 months.28–30,33,37
A total of 6 studies compared vertebroplasty head-to-head with balloon kyphoplasty and evaluated preoperative and postoperative pain scores.43–45,47,48 Liu et al’s 2010 paper, Endres et al, and Zhang et al reported no significant difference in 6-month postoperative VAS scores when comparing either system.43,45,48 Similarly, Lie et al’s 2015 paper and Wang et al reported no significant difference in postoperative VAS scores at 12 months between the 2 systems.44,47 In addition, Liu et al’s follow-up study in 2015 reported no significant difference in mean VAS scores between groups at 2- and 5-year follow-up.44 Overall, neither technique was favored in reducing postoperative pain scores after treatment.
Functionality
Functionality was assessed by the ODI in the majority of studies included in the review. For patients who underwent vertebroplasty, 3 studies examined pre- and postoperative ODI scores.6,23,24 All 3 studies demonstrated statistically significant improvements in ODI scores after treatment, with improvements ranging from 18 months to 36 months postoperatively.11,25
Of 20 studies, 13 evaluated ODI scores in patients undergoing balloon kyphoplasty.9,10,25,27,28,32–39 There was significant improvement in ODI scores reported at 12 months in 4 studies, 2 years in Chen et al and Qin et al, and 3 years in Noriega et al.28,34–37,41
There were 3 studies that examined ODI scores in head-to-head comparisons between balloon kyphoplasty and vertebroplasty, and follow-up ranged from 6 to 24 months.43,47,48 All 3 studies demonstrated significantly lower postoperative ODI scores in each group, though there was no significant between-group difference.43,47,48 One study demonstrated significantly lower ODI scores 1 month after treatment in the kyphoplasty group, though by 6 months, this between-group difference was not maintained.48 Overall, neither technique was favored in improving ODI scores after treatment.
Throughout the review the most common functionality scale was the ODI; however, other more subjective scales were also used, such as EQ-VAS, RDQ, EQ5, SF-36, clinical efficacy, and life ability scores.
Wedge Angle Restoration
Only 1 study investigated wedge angle after vertebroplasty.22 In Wang et al’s study, after vertebroplasty the wedge angle improved from 28.77° ± 3.49° preoperatively to 15.72° ± 2.19° postoperatively, which was a significant correction compared to the conservative treatment group.22 There were 2 studies that examined wedge angle correction in patients undergoing kyphoplasty.33,38 Korovessis et al demonstrated a non-significant improvement in wedge angle postoperatively compared to preoperative values.33 Qin et al reported an average wedge angle of 22.6° ± 12.2° preoperatively in the kyphoplasty group, which improved to 11.1 ± 7.1° up to 2 years postoperatively, but this study did not report whether this change was statistically significant.38
There were 2 studies that examined wedge angle restoration in head-to-head comparisons between balloon kyphoplasty and vertebroplasty. In Liu et al’s 2010 study, there were statistically significant reductions in wedge angle in both groups at 6 months, with a significantly larger reduction in the kyphoplasty group (P < 0.001).45 In Liu et al’s 2015 study, there was a statistically significant reduction in mean wedge angle 3 days, 1 year, 2 years, and 5 years postoperatively compared to preoperative values in both groups, with a mean reduction of 8.0° and 3.3° in the kyphoplasty and vertebroplasty groups, respectfully. This paper did not report on whether these differences between groups was statistically significant.44 Overall, of the 2 head-to-head studies investigating wedge angle restoration, both favored balloon kyphoplasty, but only one reported statistical significance.44,45
Kyphosis Angle Restoration
No studies examined kyphosis angle restoration in the vertebroplasty studies. A total of 7 studies investigated kyphosis angle correction after kyphoplasty.14,28–30,33–36 Two studies by Noriega et al did not demonstrate significant reductions in kyphosis angle, with results ranging from 12 months to 3 years after treatment.36,37 There were 3 studies that reported significant reductions in kyphosis angle.10,26,41 Significant improvements in kyphosis angle ranged from 3.72° ± 1.53° immediately after treatment in Wei et al’s study, 3° after 1 month in Bastian et al’s study, and 7.1° after 1 year in Jin et. al’s study10,26,41 There were 3 studies that compared unilateral kyphoplasty to bilateral kyphoplasty that reported kyphosis angle as an outcome.29,34,42 Liu et al and Chen et al reported significant reductions in the kyphosis angle at 12 months and 33.5 months after treatment, respectively, and did not find significant between-group differences.29,34,42 In contrast, Yan et al reported that both groups demonstrated significant improvements in postoperative kyphosis angle reduction at 12 months and reported a significantly greater reduction in the unilateral group.42 No studies directly compared kyphosis angle in kyphoplasty versus vertebroplasty. Overall, 3 kyphoplasty studies reported significant improvement in kyphosis angle after treatment, and 1 of 3 studies comparing unilateral to bilateral kyphoplasty favored unilateral kyphoplasty in reducing kyphosis angle.10,26,41,42
Cobb’s Angle Restoration
Only 2 studies examined Cobb’s angle for vertebroplasty procedures and reported significant improvement postoperatively.21,24 In Gu et al’s study, this improvement was reversed 2 years after treatment, where there was a significant increase (P < 0.005) in Cobb’s angle compared to immediately after treatment. Zhang et al reported a significant improvement (P < 0.01) in Cobb’s angle within 3 days after treatment.21,24 There were 6 studies that compared pre- and postoperative Cobb’s angle for kyphoplasty procedures.9,25,26,32,36,37 Bai et al reported significant improvement in Cobb’s angle 3 days and 6 months after treatment, Bastian et al reported significant improvement at 1 month after treatment, and Li et al found significant improvement at 6 months after treatment.9,25,26 In contrast, Noriega et al’s 2016 study reported no significant improvement 5 days, 6 months, and 12 months after treatment, while Noriega et al’s 2019 paper reported no significant improvement 3 years after treatment.36,37 Tang et al reported a significant difference (P < 0.05) in preoperative vs postoperative Cobb’s angle for unilateral and bilateral kyphoplasty but did not specify at what postoperative duration this significant difference occurred.39 There were no head-to-head studies investigating Cobb’s angle. Overall, there was conflicting evidence of whether either technique could lead to sustained improvement in Cobb’s angle after treatment.
Gardner Angle
Only 2 studies reported reduction in Gardner angle in the kyphoplasty arm.33,36 In Noriega et al’s 2016 study, there was no correction in the Gardner angle 5 days post-treatment, and at 6 and 12 months, worsening was observed by 2.2°± 4.0° and 0.95° ± 4.26°, respectively.36 Korovessis et al reported a non-significant reduction in Gardner angle of 6 ° ± 5 ° (P = 0.067) in the kyphoplasty arm.33
Cement Leakage
There were 6 of 7 studies with vertebroplasty as an investigational arm that reported on cement leakage.6,19–24 Firanescu et al reported the highest cement leakage, with 91.3% of patients demonstrating leakage and all events were asymptomatic.20 The following 3 studies also reported asymptomatic leakage: Zhang L, Liu et al 28%, Blasco et al 49%, and Zhang L et al 51.2%.19,23,24 Gu et al reported the lowest cement leakage rate at 10.8%.22 Farrokhi et al reported a cement leakage rate of 14%, and 1 patient developed epidural cement leakage necessitating immediate decompression and evacuation of bone cement.6
A total of 15 studies investigated cement leakage with kyphoplasty as the treatment arm.26,27,29–35,37–42 While 3 studies reported zero leakage events in the kyphoplasty arms, 7 studies reported asymptomatic leakage, and leakage rates ranged from 2.85% in Huang et al to 45.1% in Noriega et al26,29,30,32,34,35,37,39–41 Korovessis et al reported 2 events of acute paraplegia necessitating emergent decompression, and both patients recovered and were able to ambulate without an assistive device at 14-month follow-up.33
There were 6 studies that compared unilateral to bilateral kyphoplasty. Tang et al reported no extravasation events in both groups, and 2 studies reported more extravasation events in the unilateral kyphoplasty group; though the study did not report on statistical significance.27,29,30 There were 2 studies that reported significantly more leakage in the bilateral kyphoplasty group.34,42 Yan et al reported cement leakage in 7.6% of the patients in the unilateral group compared to 14.6% of patients in the bilateral group (P < 0.01), and Liu et al reported 7.1% of patients with extravasation relative to 23.3% of patients in the bilateral group (P < 0.05).34–42 Chen et al reported cement extravasation in 8.33% of patients in the unilateral group and 16.67% of patients in the bilateral group but did not report on statistical significance.29
A total of 4 studies directly compared cement extravasation head-to-head between kyphoplasty and vertebroplasty.43,46–48 Zhang et al and Endres et al reported no significant between-group difference in cement extravasation rates, and Zhang et al and Endres et al reported that all leakages were asymptomatic.43,48 In these 3 studies, cement extravasation ranged from 11.11–13.1% for kyphoplasty and 11.86–36.36% for vertebroplasty.43,48 Wang et al reported a significantly lower cement leakage rate (P < 0.05) in the vertebroplasty group, with 13.24% leakage compared to 30.56% in the kyphoplasty group; notably, all patients in the vertebroplasty group were asymptomatic as a result of the leakage.47 Vogl et al reported significantly less cement extravasation in the kyphoplasty groups.46
Overall, 6 studies included vertebroplasty in the treatment arm, and leakage occurred in 10.8–91.3% of patients.6,19–24 There were 15 studies that included kyphoplasty as a treatment arm, where 3 studies reported no leakage events while 8 studies reported asymptomatic leakage, which occurred in 2.85–45.1% of patients.26,27,29–35,37–42 In 6 studies comparing unilateral to bilateral kyphoplasty, 3 reported less leakage in the unilateral group, with 2 of them reporting statistical significance.27,29,30,34,39,42 Also, of the head-to-head studies, 2 reported no significant between-group difference in leakage rates while 2 studies reported significantly less leakage in the kyphoplasty arms.43,46–48
Discussion
Restoration of vertebral height remains a valuable quantitative measure to gauge the efficacy of vertebroplasty and balloon kyphoplasty. Our review demonstrated that the majority of patients who underwent vertebroplasty or balloon kyphoplasty had improved height restoration, except for 24 patients (16%) undergoing kyphoplasty in Vanni et al’s study.40 In contrast, Hulme et al’s systematic review of 69 articles concluded that height restoration was not achieved in 34% of kyphoplasty and 39% of vertebroplasty procedures.14 Our systematic review identified 6 head-to-head RCTs comparing vertebroplasty to balloon kyphoplasty that reported height outcomes, and 5 of these studies favored kyphoplasty over vertebroplasty.43–48 Additionally, in both groups, the mean vertebral body height at 1 and 5 years was relatively unchanged compared to the 3-day postoperative height, suggesting improved durability and resilience.44,45 Though 5 of 6 head-to-head RCTs in this review favored balloon kyphoplasty, more data are required before definitively stating that kyphoplasty or vertebroplasty is superior for height restoration: although both procedures do improve height restoration.
A more recent meta-analysis by Wang et al found that kyphoplasty significantly increased vertebral body height compared to vertebroplasty.49 However, both Wang et al and Hulme et al’s studies were limited by publication bias and the inclusion of low-quality studies, such as retrospective and prospective cohort studies.14,49 It should be noted that previous studies have also found several other factors that could affect postoperative vertebral body height restoration. For example, in vertebroplasty, preoperative dynamic mobility of bone has been identified as a good indicator of vertebral height restoration.50,51 Similarly, in balloon kyphoplasty, studies that showed improved height restoration included acute fractures or incompletely healed fractures that had edema, increasing the probability that kyphoplasty works better on mobile fractures.52 Some investigators have suggested that age of the fracture is an independent predictor for height restoration.53,54 Due to the lack of data available for fracture types in the studies included in our review, we were unable to evaluate an association between fracture type and height restoration rate. Nevertheless, our review supports previous research that shows that both vertebroplasty and balloon kyphoplasty are effective at height restoration.
Pain and functionality are important clinical indicators as they underscore the effectiveness of surgery and can be used as a surrogate on behalf of quality-of-life measures. In this review, VAS was used to assess pain and the ODI was used to assess patient functionality. Of 33 studies, 32 reported preoperative and postoperative VAS scores, with 4 studies reporting 24-month follow-up, and 1 study reporting 5-year follow-up.21,28,29,36,45 In all 6 RCTs that directly compared vertebroplasty to balloon kyphoplasty, improved postoperative VAS scores were seen, though there were no significant between-group differences, even at 5-year follow-up.43–45,47,48 Sustained improvement in function was seen for up to 3 years in both kyphoplasty and vertebroplasty.6,37 All 4 studies examining ODI scores in head-to-head comparisons between kyphoplasty and vertebroplasty demonstrated significantly lower postoperative ODI scores in both groups, though there was no significant between-group difference at sustained follow-up.25,43,47,48
Our review supports the findings from previous systematic reviews and meta-analyses, which showed that kyphoplasty and vertebroplasty had comparable beneficial effects on pain and disability.14,16,49 Furthermore, Table 2 shows that 11 studies examined all 3 parameters: vertebral height restoration, pain, and functionality. In our systematic review we only included studies that completed statistical analyses for height restoration. Therefore, not all studies in Table 2 were powered to determine statistical significance for secondary endpoints like pain and functionality. Therefore, while the majority of studies showed an improvement in all 3 outcomes, this suggests that vertebral height may be clinically correlated with improvement in pain and functionality. However, as the majority of studies did not perform statistical analyses for all 3 parameters, further research will need to be completed before we can definitively conclude the strength of this correlation.
Similar to vertebral height restoration, reduction of kyphotic and wedge angle has been studied extensively as a measure of vertebroplasty and kyphoplasty effectiveness. In a meta-analysis by Wang et al, the authors reported a significantly greater reduction of wedge angle in kyphoplasty patients than in vertebroplasty patients.49 Six studies in this review reported significant reductions in kyphosis angles from immediately postoperative until one year after treatment.10,26,29,34,41,42 Furthermore, a meta-analysis by Ma et al showed that there were significantly smaller kyphosis angles in the kyphoplasty groups compared to vertebroplasty groups during long-term follow-up in their RCT and cohort studies.55 Similarly, Wang et al reported a significant reduction in kyphosis angle in both short- and long-term follow-up data in kyphoplasty patients.56 In addition, Liu et al’s 2015 study reported a significant relationship between wedge angle and risk of adjacent fracture after vertebroplasty, which was hypothesized to be secondary to adjacent vertebrae bearing a larger transferred load.44 Greater angle restoration after kyphoplasty is thought to be due to the inflatable balloon creating a cavity that allows for a greater amount of cement to be injected. This could be especially helpful in patients with severe angle deformity caused by OVCF. However, we advise caution with interpretation of these results because the previous 6 systematic reviews and meta-analyses collectively included only 9 RCTs, and our review only included only 6 head-to-head trials.14–16,43–49,55,57
Cement leakage is a relatively common complication seen with both vertebroplasty and kyphoplasty. In this review, cement leakage rates ranged from 1.21% to 91.3% in vertebroplasty and from 0% to 45.1% in kyphoplasty.6,20,41,47 In a 2017 meta-analysis by Zhan et al, incidence rates were reported as 18.4% for kyphoplasty and 54.7% for vertebroplasty.57 Cement leakage is typically categorized as any event where the therapeutic cement is found outside of the target vertebral body. This includes leakage into the spinal canal or intervertebral foramina, which could result in neurological compromise; leakage into venous pathways, which could lead to clinically significant venous embolisms; or extracortical leakage, which may not have any clinical relevance. Zhan et al reported the following 3 risk factors that could lead to a higher incidence of cement leakage: intervertebral clefts, end-plate cortical disruptions, and procedure-related factors such as cement viscosity and injected volume.57 In both the Zhan et al meta-analysis and our own systematic review, the incidence of cement leakage occurred fewer times in the kyphoplasty groups than in the vertebroplasty groups.57 Although this could be due to a variety of factors, it is likely that the inflated balloon used in kyphoplasty creates a cavity for cement injection, thus allowing higher volume under less pressure.
As mentioned earlier, this systematic review is unique for various reasons. Hulme et al’s systematic review was comprehensive, as it included 69 studies, but it was published almost 15 years ago.14 Zhu et al recently published an updated, robust meta-analysis, but only 3 databases were reviewed, resulting in 6 RCTs in their analysis.16 Liang et al also published an extensive systematic review on this topic in 2016, but again, non-RCTs were included, and of the RCTs reviewed only 4 were included.15 It should be noted that since 2018, as per our review, 8 RCTs assessing kyphoplasty, vertebroplasty, and height restoration have been published, and therefore have added significantly to the literature on this topic. Our systematic review provides an updated, comprehensive review of height restoration, pain, and function.
Limitations
We recognize that this study does have some limitations. First, the inclusion of only RCTs may have been too restrictive as meaningful outcome measures and long-term data are difficult to measure with this study design. In addition, follow-up periods varied greatly from immediately postoperative to 5 years, which should be taken into consideration when clinicians read this review. Third, this review only included articles published in English and may have left out relevant studies. We also noticed that for the majority of RCTs, the surgeon was not blinded, which could have led to observer and detection bias. Furthermore, measurement of vertebral height restoration is dependent on the patient’s position, which was not uniformly measured among the studies reviewed or even within the same study. Another limitation is that among the studies included, the severity and age of fracture varied. It is also difficult to compare kyphoplasty to vertebroplasty given the variation in types of fractures that respond to the different treatments. We were unable to comment on whether the degree of compression was correlated with improved outcomes with vertebral augmentation, or if the amount of height restoration was correlated with pulmonary function or mortality, as these data were not uniformly reported in the studies included. Moreover, cement volume was correlated with improved height restoration in 3 head-to-head studies but was not widely reported in the studies included in this systematic review. Furthermore, not all studies reported on pain and functionality, which made broad recommendations difficult. Lastly, a meta-analysis was attempted however meaningful conclusions could not be drawn as the study’s variables are heterogenous with several different parameters, such as study size, patient age, study length, and different outcomes without a common endpoint. Therefore, we chose not to include those results in our study.
Conclusion
Our findings support the conclusion that balloon kyphoplasty and vertebroplasty are effective treatments for vertebral compression fractures. They may restore some vertebral body height loss and improve kyphosis, Cobb’s, and wedge angles. Both treatments show benefits in pain reduction and improve patient-reported functionality when correlated with height restoration; however, many studies that investigated all 3 variables did not report statistically significant results, and further robust studies and data analysis are needed to confirm this finding. As a result, we cannot definitively conclude whether balloon kyphoplasty or vertebroplasty is superior for alleviating pain and restoring functionality, though our review suggests that balloon kyphoplasty may be favored for vertebral height restoration. Nevertheless, both surgical techniques of vertebroplasty and balloon kyphoplasty should be considered for the treatment of vertebral compression fractures.
Acknowledgments
We thank Karla D. Passalacqua, Ph.D. at Henry Ford Hospital for her critical review of the manuscript. We are grateful to medical librarians Steven Moore and JoAnn Krzeminski for their assistance with the literature search and electronic search strings. The abstract of this paper was presented at PAINWeek 2020, as well as Midwestern Anesthesia Research Conference 2021, in the form of a poster presentation and oral presentation, respectively. The poster’s abstract was published in “PAINWeek Abstract Book 2020” in Postgraduate Medicine, 132:sup1, 1–76: DOI: 10.1080/00325481.2020.1824967.
Funding
There is no funding to report.
Disclosure
Dr Jason Schwalb reports grants from Medtronic, Inc, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Ensrud KE, Schousboe JT. Clinical practice. vertebral fractures. N Engl J Med. 2011;364(17):1634–1642. doi:10.1056/NEJMcp1009697
2. Longo UG, Loppini M, Denaro L, Maffulli N, Denaro V. Osteoporotic vertebral fractures: current concepts of conservative care. Br Med Bull. 2012;102(1):171–189. doi:10.1093/bmb/ldr048
3. Lee HM, Park SY, Lee SH, Suh SW, Hong JY. Comparative analysis of clinical outcomes in patients with osteoporotic vertebral compression fractures (OVCFs): conservative treatment versus balloon kyphoplasty. Spine J. 2012;12(11):998–1005. doi:10.1016/j.spinee.2012.08.024
4. Hallberg I, Rosenqvist AM, Kartous L, Löfman O, Wahlström O, Toss G. Health-related quality of life after osteoporotic fractures. Osteoporos Int. 2004;15(10):834–841. doi:10.1007/s00198-004-1622-5
5. Bostrom MP, Lane JM. Future directions. Augmentation of osteoporotic vertebral bodies. Spine. 1997;22(24 Suppl):38s–42s. doi:10.1097/00007632-199712151-00007
6. Farrokhi MR, Alibai E, Maghami Z. Randomized controlled trial of percutaneous vertebroplasty versus optimal medical management for the relief of pain and disability in acute osteoporotic vertebral compression fractures. J Neurosurg Spine. 2011;14(5):561–569. doi:10.3171/2010.12.SPINE10286
7. Tsoumakidou G, Too CW, Koch G, et al. CIRSE guidelines on percutaneous vertebral augmentation. Cardiovasc Intervent Radiol. 2017;40(3):331–342. doi:10.1007/s00270-017-1574-8
8. Mathis JM, Ortiz AO, Zoarski GH. Vertebroplasty versus kyphoplasty: a comparison and contrast. AJNR Am J Neuroradiol. 2004;25(5):840–845.
9. Li Y, Zhu J, Xie C. A comparative study of percutaneous kyphoplasty and conservative therapy on vertebral osteoporotic compression fractures in elderly patients. Int J Clin Exp Med. 2017;10(5):8139–8145.
10. Jin C, Xu G, Weng D, Xie M, Qian Y. Impact of magnetic resonance imaging on treatment-related decision making for osteoporotic vertebral compression fracture: a prospective randomized trial. Med Sci Monit. 2018;24:50–57. doi:10.12659/MSM.905729
11. Buchbinder R, Osborne RH, Ebeling PR, et al. A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures. N Engl J Med. 2009;361(6):557–568. doi:10.1056/NEJMoa0900429
12. Comstock BA, Sitlani CM, Jarvik JG, Heagerty PJ, Turner JA, Kallmes DF. Investigational vertebroplasty safety and efficacy trial (INVEST): patient-reported outcomes through 1 year. Radiology. 2013;269(1):224–231. doi:10.1148/radiol.13120821
13. Shamseer L, Moher D, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;350:g7647. doi:10.1136/bmj.g7647
14. Hulme PA, Krebs J, Ferguson SJ, Berlemann U. Vertebroplasty and kyphoplasty: a systematic review of 69 clinical studies. Spine. 2006;31(17):1983–2001. doi:10.1097/01.brs.0000229254.89952.6b
15. Liang L, Chen X, Jiang W, et al. Balloon kyphoplasty or percutaneous vertebroplasty for osteoporotic vertebral compression fracture? An updated systematic review and meta-analysis. Ann Saudi Med. 2016;36(3):165–174. doi:10.5144/0256-4947.2016.165
16. Zhu Y, Cheng J, Yin J, Zhang Z, Liu C, Hao D. Therapeutic effect of kyphoplasty and balloon vertebroplasty on osteoporotic vertebral compression fracture: a systematic review and meta-analysis of randomized controlled trials. Medicine. 2019;98(45):e17810. doi:10.1097/MD.0000000000017810
17. Review Manager (RevMan) [Computer program]. Version 5.4. The Cochrane Collaboration, 2020.
18. Harden RN, Oaklander AL, Burton AW, et al. Complex regional pain syndrome: practical diagnostic and treatment guidelines, 4th edition. Pain Med. 2013;14(2):180–229. doi:10.1111/pme.12033
19. Blasco J, Martinez-Ferrer A, Macho J, et al. Effect of vertebroplasty on pain relief, quality of life, and the incidence of new vertebral fractures: a 12-month randomized follow-up, controlled trial. J Bone Miner Res. 2012;27(5):1159–1166. doi:10.1002/jbmr.1564
20. Firanescu CE, De Vries J, Lodder P, et al. Percutaneous vertebroplasty is no risk factor for new vertebral fractures and protects against further height loss (VERTOS IV). Cardiovasc Intervent Radiol. 2019;42(7):991–1000. doi:10.1007/s00270-019-02205-w
21. Gu YT, Zhu DH, Liu HF, Zhang F, Mcguire R. Minimally invasive pedicle screw fixation combined with percutaneous vertebroplasty for preventing secondary fracture after vertebroplasty. J Orthop Surg Res. 2015;10:31. doi:10.1186/s13018-015-0172-1
22. Wang Q, Wang S, Li X, Wei Y, Ma X Clinical observation of percutaneous vertebroplasty in the treatment of senile osteoporosis complicated with vertebral compression fractures. 2018.
23. Zhang L, Liu Z, Wang J, et al. Unipedicular versus bipedicular percutaneous vertebroplasty for osteoporotic vertebral compression fractures: a prospective randomized study. BMC Musculoskelet Disord. 2015;16(1):145. doi:10.1186/s12891-015-0590-6
24. Zhang L, Wang J, Feng X, et al. A comparison of high viscosity bone cement and low viscosity bone cement vertebroplasty for severe osteoporotic vertebral compression fractures. Clin Neurol Neurosurg. 2015;129:10–16. doi:10.1016/j.clineuro.2014.11.018
25. Bai M, Yin H, Zhao J, Li Y, Yang Y, Wu Y. Application of PMMA bone cement composited with bone-mineralized collagen in percutaneous kyphoplasty. Regen Biomater. 2017;4(4):251–255. doi:10.1093/rb/rbx019
26. Bastian L, Schils F, Tillman JB, Fueredi G. A randomized trial comparing 2 techniques of balloon kyphoplasty and curette use for obtaining vertebral body height restoration and angular-deformity correction in vertebral compression fractures due to osteoporosis. AJNR Am J Neuroradiol. 2013;34(3):666–675. doi:10.3174/ajnr.A3363
27. Chen C, Chen L, Gu Y, et al. Kyphoplasty for chronic painful osteoporotic vertebral compression fractures via unipedicular versus bipedicular approachment: a comparative study in early stage. Injury. 2010;41(4):356–359. doi:10.1016/j.injury.2009.09.021
28. Chen C, Wei H, Zhang W, et al. Comparative study of kyphoplasty for chronic painful osteoporotic vertebral compression fractures via unipedicular versus bipedicular approach. J Spinal Disord Tech. 2011;24(7):E62–65. doi:10.1097/BSD.0b013e318228f470
29. Chen L, Yang H, Tang T. Unilateral versus bilateral balloon kyphoplasty for multilevel osteoporotic vertebral compression fractures: a prospective study. Spine. 2011;36(7):534–540. doi:10.1097/BRS.0b013e3181f99d70
30. Chung HJ, Chung KJ, Yoon HS, Kwon IH. Comparative study of balloon kyphoplasty with unilateral versus bilateral approach in osteoporotic vertebral compression fractures. Int Orthop. 2008;32(6):817–820. doi:10.1007/s00264-007-0439-1
31. He G, Yu Q, Yang K, Gao Z, Han A. Clinical application of percutaneous kyphoplasty under the guidance of DynaCT in the treatment of compression fractures of thoracolumbar. J Musculoskelet Neuronal Interact. 2019;19(2):229–233.
32. Huang Z, Zhang L. Treatment of osteoporotic vertebral compressive fractures with percutaneous kyphoplasty and oral Zishengukang. J Tradit Chin Med. 2012;32(4):561–564. doi:10.1016/S0254-6272(13)60071-0
33. Korovessis P, Vardakastanis K, Repantis T, Vitsas V. Balloon kyphoplasty versus KIVA vertebral augmentation–comparison of 2 techniques for osteoporotic vertebral body fractures: a prospective randomized study. Spine. 2013;38(4):292–299. doi:10.1097/BRS.0b013e31826b3aef
34. Liu MX, Xia L, Zhong J, Dou NN, Li B. Is it necessary to approach the compressed vertebra bilaterally during the process of PKP? J Spinal Cord Med. 2020;43(2):201–205. doi:10.1080/10790268.2018.1451238
35. Noriega D, Marcia S, Theumann N, et al. A prospective, international, randomized, noninferiority study comparing an implantable titanium vertebral augmentation device versus balloon kyphoplasty in the reduction of vertebral compression fractures (SAKOS study). Spine J. 2019;19(11):1782–1795. doi:10.1016/j.spinee.2019.07.009
36. Noriega DC, Ramajo RH, Lite IS, et al. Safety and clinical performance of kyphoplasty and SpineJack(®) procedures in the treatment of osteoporotic vertebral compression fractures: a pilot, monocentric, investigator-initiated study. Osteoporos Int. 2016;27(6):2047–2055. doi:10.1007/s00198-016-3494-x
37. Noriega DC, Rodrίguez-Monsalve F, Ramajo R, Sánchez-Lite I, Toribio B, Ardura F. Correction to: long-term safety and clinical performance of kyphoplasty and SpineJack® procedures in the treatment of osteoporotic vertebral compression fractures: a pilot, monocentric, investigator-initiated study. Osteoporos Int. 2019;30(3):647. doi:10.1007/s00198-018-04825-3
38. Qin J, Li J, Liu Y, et al. Clinical comparison between a percutaneous hydraulic pressure delivery system and balloon tamp system using high-viscosity cement for the treatment of osteoporotic vertebral compression fractures. Clinics. 2019;74:e741. doi:10.6061/clinics/2019/e741
39. Tang J, Guo WC, Hu JF, Yu L. Unilateral and bilateral percutaneous kyphoplasty for thoracolumbar osteoporotic compression fractures. J Coll Physicians Surg Pak. 2019;29(10):946–950. doi:10.29271/jcpsp.2019.10.946
40. Vanni D, Pantalone A, Bigossi F, Pineto F, Lucantoni D, Salini V. New perspective for third generation percutaneous vertebral augmentation procedures: preliminary results at 12 months. J Craniovertebr Junction Spine. 2012;3(2):47–51. doi:10.4103/0974-8237.116537
41. Wei P, Yao Q, Xu Y, Zhang H, Gu Y, Wang L. Percutaneous kyphoplasty assisted with/without mixed reality technology in treatment of OVCF with IVC: a prospective study. J Orthop Surg Res. 2019;14(1):255. doi:10.1186/s13018-019-1303-x
42. Yan L, Jiang R, He B, Liu T, Hao D. A comparison between unilateral transverse process-pedicle and bilateral puncture techniques in percutaneous kyphoplasty. Spine. 2014;39(26 Spec No.):B19–26. doi:10.1097/BRS.0000000000000493
43. Endres S, Badura A. Shield kyphoplasty through a unipedicular approach compared to vertebroplasty and balloon kyphoplasty in osteoporotic thoracolumbar fracture: a prospective randomized study. Orthop Traumatol Surg Res. 2012;98(3):334–340. doi:10.1016/j.otsr.2011.11.010
44. Liu JT, Li CS, Chang CS, Liao WJ. Long-term follow-up study of osteoporotic vertebral compression fracture treated using balloon kyphoplasty and vertebroplasty. J Neurosurg Spine. 2015;23(1):94–98. doi:10.3171/2014.11.SPINE14579
45. Liu JT, Liao WJ, Tan WC, et al. Balloon kyphoplasty versus vertebroplasty for treatment of osteoporotic vertebral compression fracture: a prospective, comparative, and randomized clinical study. Osteoporos Int. 2010;21(2):359–364. doi:10.1007/s00198-009-0952-8
46. Vogl TJ, Pflugmacher R, Hierholzer J, et al. Cement directed kyphoplasty reduces cement leakage as compared with vertebroplasty: results of a controlled, randomized trial. Spine. 2013;38(20):1730–1736. doi:10.1097/BRS.0b013e3182a14d15
47. Wang CH, Ma JZ, Zhang CC, Nie L. Comparison of high-viscosity cement vertebroplasty and balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures. Pain Physician. 2015;18(2):E187–194.
48. Zhang P, Zhong ZH, Yu HT, Zhou W, Li J. Therapeutic effects of new-type hydraulic delivery vertebroplasty, balloon kyphoplasty and conventional pusher-type vertebroplasty on single segmental osteoporotic vertebral compression fracture. Exp Ther Med. 2018;16(4):3553–3561. doi:10.3892/etm.2018.6624
49. Wang B, Zhao CP, Song LX, Zhu L. Balloon kyphoplasty versus percutaneous vertebroplasty for osteoporotic vertebral compression fracture: a meta-analysis and systematic review. J Orthop Surg Res. 2018;13(1):264. doi:10.1186/s13018-018-0952-5
50. Carlier RY, Gordji H, Mompoint DM, Vernhet N, Feydy A, Vallée C. Osteoporotic vertebral collapse: percutaneous vertebroplasty and local kyphosis correction. Radiology. 2004;233(3):891–898. doi:10.1148/radiol.2333030400
51. Mckiernan F, Jensen R, Faciszewski T. The dynamic mobility of vertebral compression fractures. J Bone Miner Res. 2003;18(1):24–29. doi:10.1359/jbmr.2003.18.1.24
52. Faciszewski T, Mckiernan F. Calling all vertebral fractures classification of vertebral compression fractures: a consensus for comparison of treatment and outcome. J Bone Miner Res. 2002;17(2):185–191. doi:10.1359/jbmr.2002.17.2.185
53. Berlemann U, Franz T, Orler R, Heini PF. Kyphoplasty for treatment of osteoporotic vertebral fractures: a prospective non-randomized study. Eur Spine J. 2004;13(6):496–501.
54. Phillips FM, Ho E, Campbell-Hupp M, Mcnally T, Todd Wetzel F, Gupta P. Early radiographic and clinical results of balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures. Spine. 2003;28(19):
55. Ma XL, Xing D, Ma JX, Xu WG, Wang J, Chen Y. Balloon kyphoplasty versus percutaneous vertebroplasty in treating osteoporotic vertebral compression fracture: grading the evidence through a systematic review and meta-analysis. Eur Spine J. 2012;21(9):1844–1859. doi:10.1007/s00586-012-2441-6
56. Wang H, Sribastav SS, Ye F, et al. Comparison of percutaneous vertebroplasty and balloon kyphoplasty for the treatment of single level vertebral compression fractures: a meta-analysis of the literature. Pain Physician. 2015;18(3):209–222.
57. Zhan Y, Jiang J, Liao H, Tan H, Yang K. Risk factors for cement leakage after vertebroplasty or kyphoplasty: a meta-analysis of published evidence. World Neurosurg. 2017;101:633–642. doi:10.1016/j.wneu.2017.01.124
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.