")
Back to Journals » Infection and Drug Resistance » Volume 15
Bacterial Vaginosis and Associated Factors Among Pregnant Women Attending Antenatal Care in Harar City, Eastern Ethiopia
Authors Ahmed M , Ayana DA , Abate D
Received 26 February 2022
Accepted for publication 10 June 2022
Published 16 June 2022 Volume 2022:15 Pages 3077—3086
DOI https://doi.org/10.2147/IDR.S364229
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Mohammed Ahmed, Desalegn Admassu Ayana, Degu Abate
Department of Medical Laboratory Science, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Correspondence: Mohammed Ahmed Aliyi, Department of Medical Laboratory Science, College of Health and Medical Sciences, Haramaya University, P.O. Box 235, Harar, Ethiopia, Tel +251-921-658-970, Email [email protected]
Background: Bacterial vaginosis is one of the most common causes of abnormal vaginal discharge in women of reproductive age, especially pregnant women. It is characterized by the decrement of lactobacilli and increasing proliferation of diverse anaerobic bacteria. The prevalence of bacterial vaginosis and contributing factors vary between countries, within the same country, and among different populations.
Objective: The purpose of this study was to determine the prevalence of bacterial vaginosis and associated factors among pregnant women attending antenatal care from May 5–July 15, 2021 in health-care facilities found in Harar town, eastern Ethiopia.
Methods and Materials: An institutional-based cross-sectional study was conducted among 248 pregnant women attending antenatal care through systematic random sampling. Data were collected using a structured questionnaire and two vaginal swabs were collected using sterile swabs and transported to the microbiology laboratory. Samples were analyzed using Amsel’s criteria or using Nugent scoring criteria and culture. Data were entered into EpiData version 3.1 and transferred to SPSS version 25 for analysis. Binary logistic regression was used to identify variables associated with bacterial vaginosis. P-value < 0.05 was considered statistically significant.
Results: Altogether 248 pregnant women were included in the study. Overall, 21.4% (95% CI: 16, 27) of study participants had bacterial vaginosis. History of sexually transmitted infection (AOR = 6.0, 95% CI: 1.94, 19.07; P = 0.002), history of spontaneous abortion (AOR = 5.8, 95% CI: 1.55, 22.02; P = 0.009), multiple sex partners (AOR = 8.6, 95% CI: 2.93, 25.79; P = 0.000) and having vaginal discharge (AOR = 5.5, 95% CI: 2.48, 12.41; P = 0.000) were significantly associated with bacterial vaginosis.
Conclusion: The prevalence of bacterial vaginosis is higher among symptomatic pregnant women and associated with a history of sexually transmitted infection, vaginal discharge, multiple sexual partners and spontaneous abortion.
Keywords: bacterial vaginosis, lactobacilli, G. vaginalis, Amsel’s criteria, Nugent scoring system
Introduction
Bacterial vaginosis (BV) is one of the most common causes of vaginitis in women of reproductive age, resulting from decrement of lactobacilli and increasing proliferation of diverse anaerobic bacteria.1,2 Bacterial vaginosis is the most common vaginal dysbiosis that affects women of childbearing age and comprises around 50% of all cases of vaginitis worldwide.3,4
About 50–75% of women with BV are asymptomatic,5 however, some women with BV experience symptoms such as thin grayish-white discharge, itching, vaginal irritation, and malodorous fishy odor during sexual intercourse which have a significant negative impact on a woman’s self-esteem, sexual relationships and quality of life.6–8
BV is associated with adverse outcomes, including spontaneous abortion, preterm birth, stillbirth, low birth weight, chorioamnionitis, postpartum endometritis, increased risk of pelvic inflammatory disease and it facilitates the transmission of sexually transmitted infection.9–11 In addition, BV increases the risk of acquiring human immunodeficiency virus infection by 40–60%.12,13 BV is also associated with a history of sexually transmitted infection and the number of sex partners.14
Globally, the burden of BV infection among reproductive age women varies from country to country, being most common in Africa and less common in America, Europe and Asia, which ranges from 5–70%.15 The incidence of BV is higher among low socioeconomic countries including Ethiopia. A few previous studies showed that the prevalence of BV in Ethiopia ranges from 2.8–19.4%, with only a single study among pregnant women.16,17 Using different methods to diagnose BV may result in variation among the prevalence reports.18
Bacterial vaginosis can be diagnosed clinically using Amsel’s criteria or through the laboratory using the Nugent scoring system.19 A combination of both Amsel’s clinical criteria and Nugent grade scoring system of Gram stain is better for an accurate diagnosis of BV. A few previous studies conducted used either Amsel’s clinical criteria or Nugent grade scoring system only, however, none of the previous researchers used culture to isolate G. vaginalis; which accelerates formation of the biofilm that largely contributes to the development of BV in combination with other anaerobic organisms. Overall, to the researchers’ knowledge, there has been limited information about BV among pregnant women in Ethiopia. Furthermore, bacterial vaginosis is linked to a number of pregnancy complications that warrant global consideration; Ethiopia has neither an intensive analysis nor successful control systems. In order to prevent complications of BV among pregnant women, early diagnosis and treatment are crucial.
Therefore, this study aimed to determine the prevalence of bacterial vaginosis and associated factors among pregnant women attending antenatal clinics (ANC) using clinical and different laboratory diagnostic techniques including microbial culture.
Methods and Materials
Study Setting, Design, and Duration
The study was conducted in Harar city, a capital city of the Harari regional state, in the eastern part of Ethiopia. Harar is found 550 km away from the capital Addis Ababa. Based on population projections, the estimated total population of Harar was 226,412 (Central Statistical Agency 2007) and 4300 pregnant women in 2020. The study was conducted in two selected health facilities; Hiwot Fana Specialized University Hospital and Family Guidance Association of Ethiopia (FGAE) from May 5 to July 15, 2021.
An institutional-based cross-sectional study was conducted among pregnant women attending ANC follow up in health facilities in Harar city. Those who had taken antibiotics in the preceding two weeks were excluded from the study.
Sample Size and Sampling Technique
The sample size (n = 248) was calculated using a single population proportion formula with the following assumptions: confidence level of 95%, margin of error 5%, prevalence of bacterial vaginosis among pregnant women 19.4% in Addis Ababa17 Ethiopia, and 10% non-response rate. Health facilities (hospitals and clinic) in Harar City were stratified to governmental health facilities and non-governmental health facilities. One governmental and one non-governmental health facility were selected using the lottery method. The sample size was proportionally allocated to the selected health facility based on the average ANC follow up in the previous three months. An eligible pregnant woman was included in the study using a systematic random sampling technique.
Data Collection Method
Training was given to nurses recruited as data collectors. The trained nurses completed the standardized questionnaire after informed, voluntary, written and signed consent was obtained. Data were collected regarding socio-demographic characteristics and associated factors, such as history of spontaneous abortion, previous usage of IUCDs, vaginal discharge, history of preterm birth, number of lifetime sex partners and previous history of an STI. Trained nurses collected two vaginal swabs from the lateral and the posterior vaginal fornix while observing for consistency and color of vaginal discharge. One swab was used for analysis of Amsel’s criteria and the second swab was used for Gram staining and culture. The collected swab specimens were tested for PH; then immediately dipped into Amies transport media and transported to the microbiology laboratory.
Diagnostic Method of Bacterial Vaginosis
In this study, two main diagnostic methods of bacterial vaginosis were applied; clinical criteria and laboratory-based method. The most widely used clinical criteria are Amsel’s clinical criteria which include PH measurement (using a Whatman PH meter that measures pH from 1–14), saline wet mount (for clue cells) and for whiff test (to see for fishy or amine odor) as one indicator of BV by the addition of 10% KOH. Bacterial vaginosis is clinically diagnosed by Amsel’s criteria by at least fulfilling three out of four of the following criteria: homogeneous thin gray or white vaginal discharge, positive whiff test, high vaginal PH >4.5 and presence of clue cell.20
Diagnosis of BV was also conducted by the Nugent grade scoring system of Gram stain of vaginal discharge. In BV diagnosis, Gram staining classified the bacteria as Lactobacillus morphotypes for large Gram-positive bacilli, Mobiluncus morphotypes for curved Gram-negative while Gardnerella vaginalis (Bacteroides morphotypes) were reported as small Gram-variable rod/coccobacilli as indicated in Table 1. The Nugent scoring system is a gold standard test that involves grading of Gram staining of vaginal smear; and Amsel’s clinical criteria are non-quantifiable and non-reproducible clinical symptoms.21–23 The Nugent score is based on the idea that having high numbers of Lactobacillus spp. are indicative of health, and their depletion with increased proportions of morphotypes resembling Gardnerella, Bacteroides spp., and curved Gram-variable rods is indicative of bacterial vaginosis.24
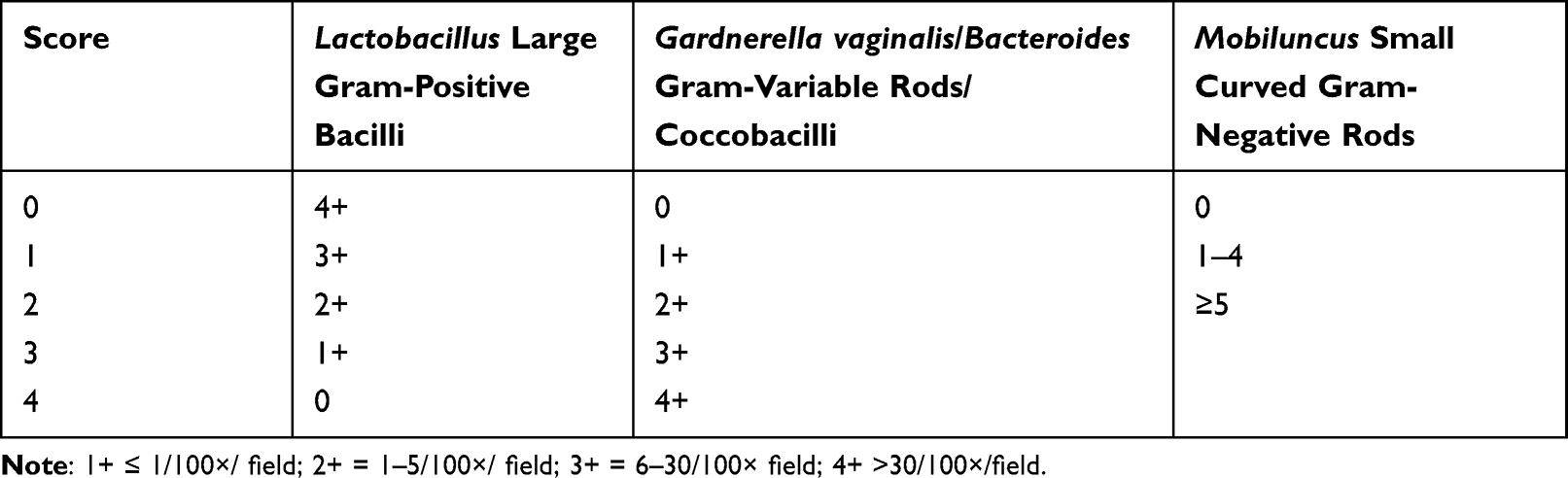 |
Table 1 Summary of the Nugent Grade Scoring System |
Morphotypes were scored as average number of each morphotype seen after examining at least 10–20 high power (oil immersion) fields. The total score of the Gram stain results were added together to get the final score as summarized below.
(Lactobacillus spp. + G. vaginalis/Bacteroides + mobiluncus spp). “0” score, no morphotypes present; 1, ≤1 morphotype present; 2, 1–5 morphotypes present; 3, 6–30 morphotypes present; 4, >30 morphotypes present (Table 1). All morphotypes added together to give a final score ranging from 0–10. Nugent score of 7–10 was considered positive for BV, a score of 0–3 was considered “normal”, and a score of 4–6 was considered “intermediate flora”.25,26
Those samples that were classified as bacterial vaginosis by either Amsel’s criteria or Nugent grading system of Gram stain or both were cultured on blood agar and De Man Rogosa Sharpe (MRS) agar27 and incubated at 37°C, with 5% CO2 for 24–48 hours. MRS is a selective culture medium designed to favor the growth of Lactobacilli. Gardnerella vaginalis was identified by beta-hemolytic appearance of the transparent colonies on 5% sheep blood agar plate with 5% CO2 in a candle jar as a facultative anaerobe. For beta-hemolytic organisms, catalase test was performed to identify species of interest. For the catalase negatives, starch hydrolysis and oxidase tests were conducted. G. vaginalis was recognized by a positive beta-hemolysis on blood agar and starch hydrolysis test, as well as catalase and oxidase negative. Starch hydrolysis test for G. vaginalis culture was inoculated onto starch medium and incubated at 37°C. After overnight incubation, the plate was flooded with Lugol’s iodine solution. Presence of clear, colorless zone indicates starch hydrolysis.28
Data and Sample Quality Control
The questionnaire was prepared in English and translated into the local language (Afaan Oromo, and Amharic), as the study subject speaks Afaan Oromo & Amharic. Then the questionnaire was translated back into English to check for consistency. A questionnaire was pretested on 5% of pregnant women attending ANC at Jugal hospital to check for comprehensiveness, order, validity, and reliability. Quality of samples was maintained following aseptic procedure during sample collection, using sterile applicator sticks for sample collection and Amies transport media for transportation to the microbiology laboratory. Quality control of Gram stain was checked using known control slides to ensure the quality of reagents as well as the efficacy of staining procedures. Culture media were tested for sterility and performance tests. The performance test for culture was improved by strictly following the manufacturer’s instructions. Equipment used in the microbiology laboratory such as autoclave, incubators, refrigerator, and other instruments was monitored using standard procedures and by performing proper routine maintenance, maintaining optimum temperature, humidity, and other condition to ensure the results are accurate and reproducible. Sterility of culture media was assessed by incubating 3–5% of batches of prepared culture media at 35–37° for 24 hours and checked for any growth.
Methods of Data Analysis
Collected data were checked for completeness and consistency and entered into EpiData3.1 and transferred into SPSS version 25 for analysis. Bivariate analysis was used to identify variables associated with bacterial vaginosis. Variables with no missing value and having no multicollinearity were included in bivariate analyses. All variables which were shown to be P<0.25 on bivariate analysis were selected for multivariable analysis to check for possible association with bacterial vaginosis by controlling potential confounding factors through backward LR (likelihood ratio). Model fitness for application of multivariate analysis was checked by using Hosmer-Lemeshow goodness of fit model. AOR and P-values <0.05 were considered statistically significant.
Ethical Considerations and Informed Consent
Ethical approval was obtained from Haramaya University College of Health and Medical Sciences’ Institutional Health Research Ethics Review Committee (IHRERC) with Ref. No. IHRERC/057/2021. This study was conducted in accordance with the Declaration of Helsinki. Prior to data collection, written informed consent was obtained from participants. The objective of the study was explained to the participants, and those who agreed to participate were included in the study. A female nurse collected the vaginal swab in a separate room to ensure the participant’s privacy and confidentiality. Unauthorized persons were unable to access the obtained data. Participants who tested positive for BV by either Amsel’s criteria or Nugent grading system of Gram stain or by both methods were immediately reported to their service provider, who gave them recommended therapy. Covid-19 prevention and control measures were briefly addressed with data collectors, and protective equipment (face masks and sanitizer) was provided to data collectors during the data collection process to protect them from Covid-19.
Results
Socio-Demographic and Health-Related Characteristics of Study Participants
The study included a total of 248 pregnant women from two health facilities, of which 55.2% were living in rural areas, 97.6% were married and 31.5% had attended primary education. Participants’ age ranged from 17–43 years, with mean (±SD) age of 26.29 (±4.54) years. Most of the study participants (60.5%) were within the 25–34 age group and 51.6% were housewives. Of the total participants, 37.9% had vaginal discharge and a majority (58.9%) were multigravida (Table 2).
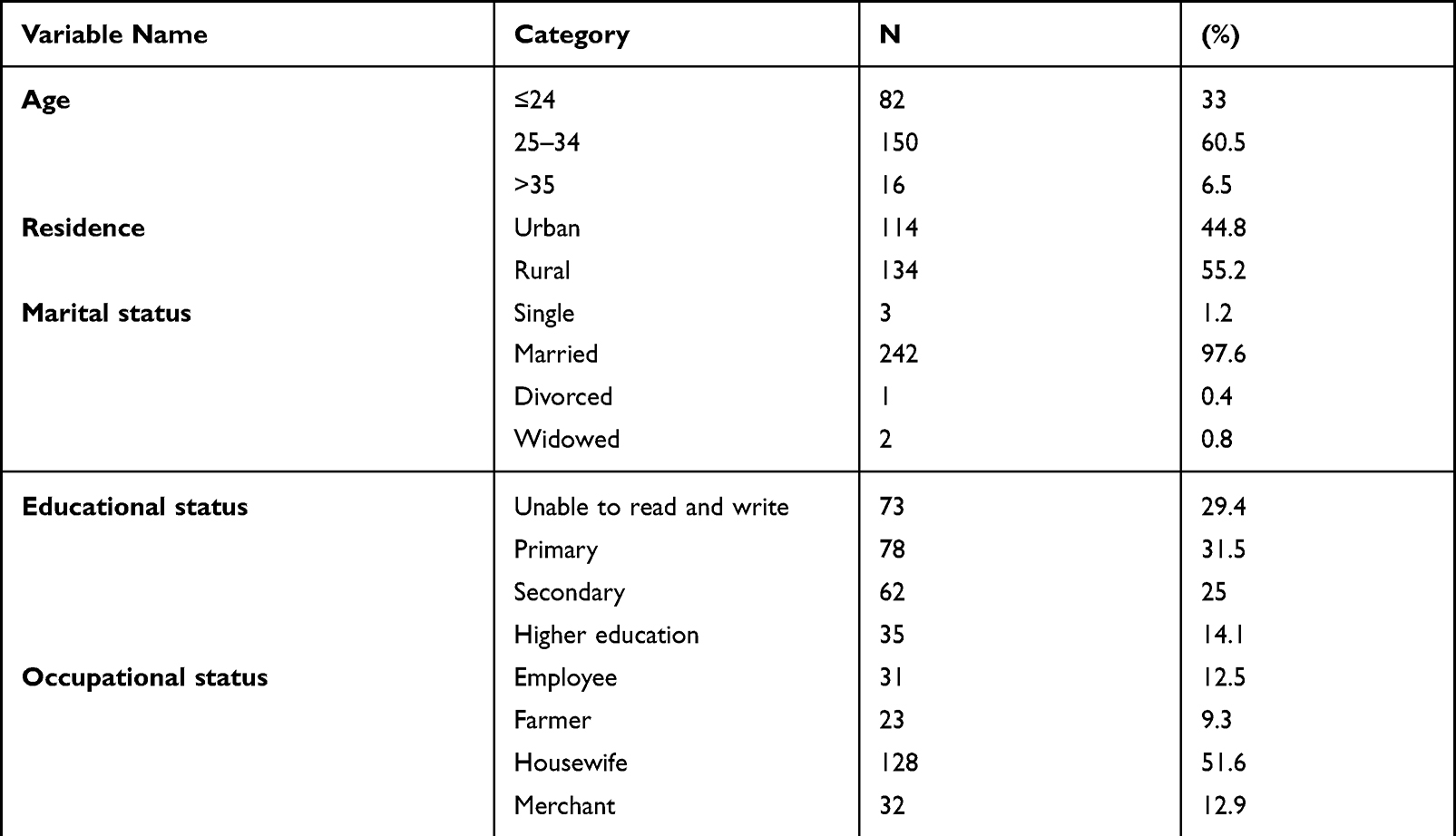 |
Table 2 Socio-demographic and Health Related Characteristics of Study Participants |
Magnitude of Bacterial Vaginosis and Associated Factors
In this study the overall prevalence of bacterial vaginosis by Nugent grade scoring system or Amsel’s criteria was 21.4% (53/248) (95% CI: 16, 27). G. vaginalis was isolated in 25 from the total BV case by the culture method. This accounts for 10.1% of study participants.
According to Nugent’s scoring system, of the 248 study participants, 51/248 (20.6%) were diagnosed as bacterial vaginosis with a Nugent score of 7–10, and 37/248 (14.9%) as intermediate with a Nugent score of 4–6. The implications of “intermediate flora” are unclear; however, it might proceed to BV or to normal flora. Using Amsel’s criteria, 48/248 (19.35%) of the pregnant women were diagnosed with bacterial vaginosis. Only 25/53 of the participants with bacterial vaginosis were found to have Gardnerella vaginalis on culture.
Of the 53 BV cases, 46 were positive by both Nugent grade scoring system and Amsel’s criteria, 5 were reported as BV by the Nugent grade scoring system, but negative by Amsel’s criteria; and 2 were positive by Amsel’s criteria, but classified as intermediate (score 4–6) by the Nugent scoring system. From the 53 BV cases, 36/53 (67.9%) pregnant women had vaginal discharge and clue cells were present in 90.6% (48/53) (Table 3).
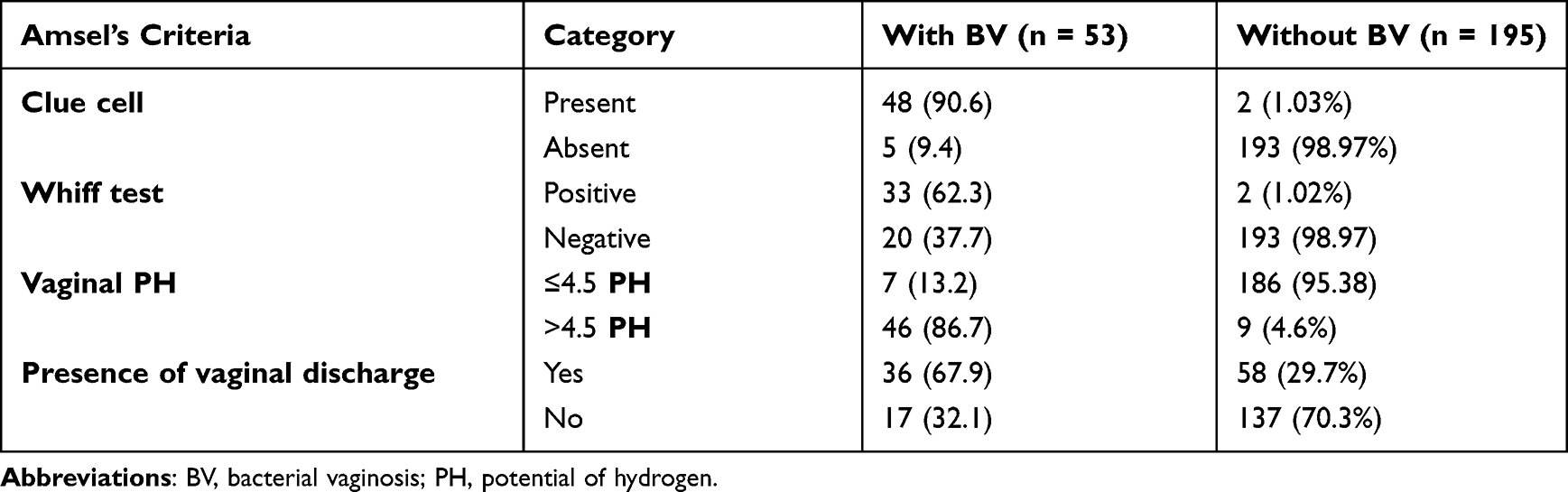 |
Table 3 Frequency Distribution of Amsel’s Criteria of Study Participants |
A total of 53 samples were classified as bacterial vaginosis by Amsel’s criteria and Nugent grading system of Gram stain was cultured on blood agar and MRS agar. G. vaginalis was recognized by beta-hemolysis on blood agar, positive starch hydrolysis test, catalase and oxidase negative tests. G. vaginalis was isolated in 25 of the BV cases by culture.
With bivariable analysis, history of an STI, history of spontaneous abortion, history of preterm delivery, previous IUCD use, vaginal discharge, number of prior pregnancies, and multiple sexual partners were associated (P <0.25) with bacterial vaginosis by a Nugent score system. In the multivariable analysis, history of an STI, vaginal discharge, history of spontaneous abortion and a number of sexual partners were found to be statistically significantly associated with BV (P <0.05). Pregnant women who have a history of STI were 6 times more likely to develop bacterial vaginosis than their counterparts (AOR = 6.0, 95% CI: 1.94, 19.07; P = 0.002) (Table 4).
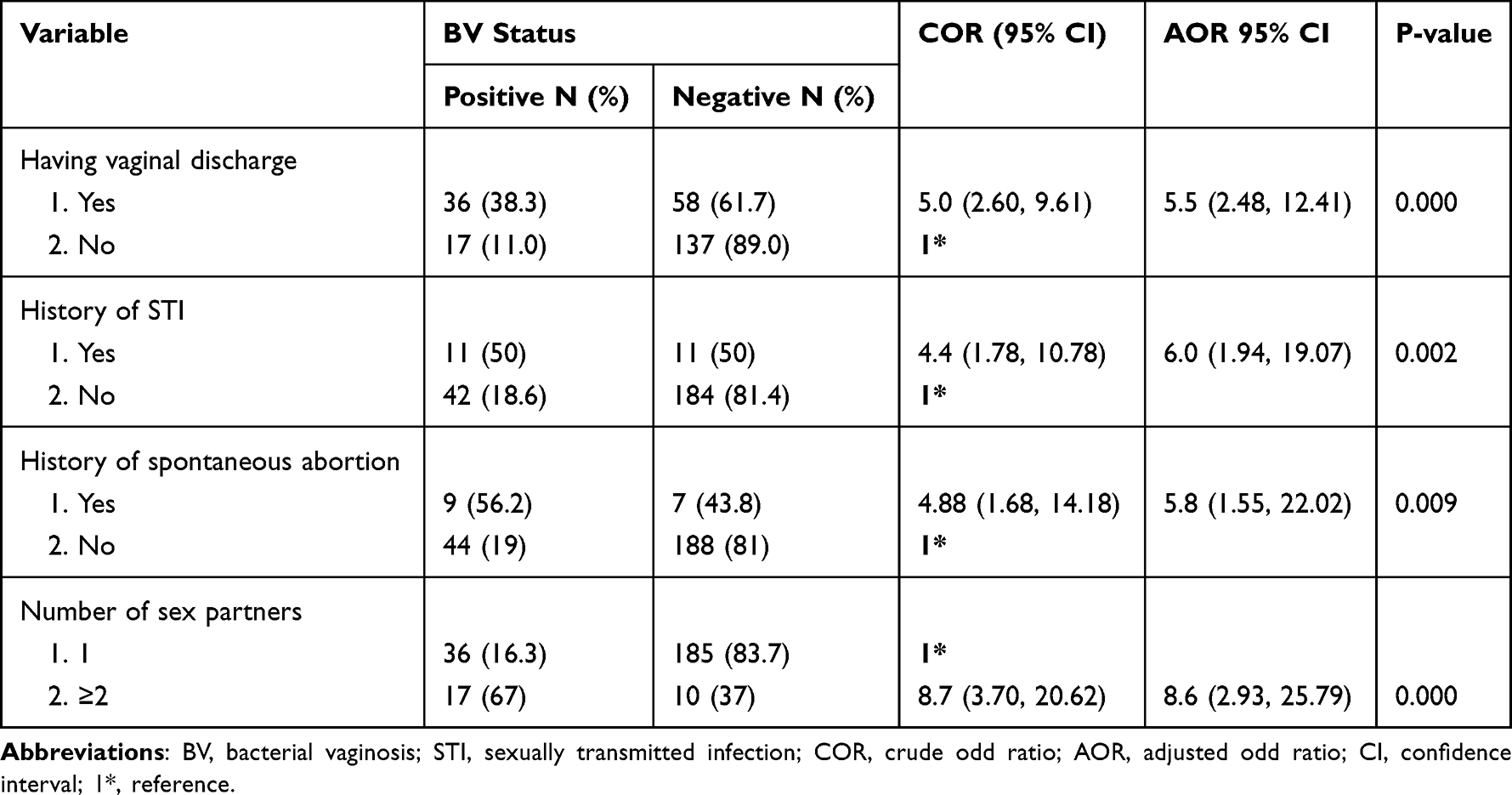 |
Table 4 Logistic Regression Analysis of Factors Associated with Bacterial Vaginosis Among Pregnant Women Attending ANC at HFSUH and FGAE from May 5-July 15, 2021 |
Discussion
According to the current study, the overall prevalence of bacterial vaginosis among pregnant women attending ANC at selected health facility in Harar city was 21.4% (95% CI; 16, 27) by Nugent scoring system or Amsel’s criteria. History of STI, history of spontaneous abortion, having vaginal discharge and having multiple sexual partners were factors associated with bacterial vaginosis.
This study found a consistent finding with a study done in India that reported 19%.29 Another study conducted in North India showed a prevalence of 20.5%30 and a study conducted in Brazil reported 22%.31 The prevalence of bacterial vaginosis found in this study is also comparable with the 17.3% in North‑Eastern Nigeria,32 17.7% (95% CI 12.9, 23.4) in South Africa33 and 19.3% (95% CI 15.7, 27.0) in Kenya.34 It is also more or less comparable with 24.8% pooled prevalence report of BV in Africa.14 A similar study finding was also reported from Ethiopia, Addis Ababa of 19.4%.17 This comparable sample size, method used and similarity of study population may contribute to the very close findings among different studies.14
In contrast to the current study, lower bacterial vaginosis prevalence of 3.88% was reported from Portugal,35 13% from Lucknow30 and 8.6% from India.36 This might be related to the nature of bacterial vaginosis, which greatly varied by geographical distribution, socioeconomic and behavioral differences of the study population.14,15
However, this study found a lower prevalence of bacterial vaginosis compared with a study done in Brazil, Ouro Preto 32.5% (95% CI: 27.7, 37.7),37 Tanzania 28.5%,38 Ghana 30.9%,39 Zimbabwe 32.6%,40 Nigeria 38%41 and Sudan 49.8%.2 The lower prevalence of BV in the current study might be attributed to the difference in sampling techniques, sample size difference and other sociodemographic characteristics of the participants.42–45
Despite the fact that many laboratories utilize non-culture-based approaches, isolation of G. vaginalis is critical. It is usually difficult to isolate and identify G. vaginalis from a polymicrobial sample such as a vaginal swab containing vaginal microbiota. Culture-based identification is challenging and time-consuming when dealing with slow-growing and fastidious organisms.46
In the current study G. vaginalis were isolated from 10.1% of pregnant women. This is consistent with studies reported from different countries: 8.7% in Northeast India,47 9.6% in Boston, USA,48 8% in England49 and 10.2% in Turkey.50 However, it is lower than some studies conducted in India 16.7%, Pakistan 17%, and 38.7% in central Nigeria.29,51–53 The prevalence of G. vaginalis worldwide ranges from 6–94%.49,54 Low isolation rate of Gardnerella vaginalis might be attributed to the poor viability and fastidiousness of the organism to grow in various media.47 To grow G. vaginalis and other anaerobic bacteria species involved in bacterial vaginosis through culture is difficult and it was not a satisfactory diagnostic tool for bacterial vaginosis.29,55
In this study, there were no statistically significant association between bacterial vaginosis and sociodemographic characteristics of participants such as age, marital status, residence, occupation and level of education (P>0.05). This is in line with studies conducted in Tanzania,38 Brazil37 and Turkey.56 But, studies conducted in the USA, Poland, China, Indonesia and Nigeria32,57–60 revealed an association between BV and different sociodemographic characteristics such as marital status, age, level of education and occupational status. This might be due to the variation in prevalence of bacterial vaginosis by the community, which could be attributed to factors such as hygiene practices and difference in sociodemographic characteristics.58,61,62
Factors that are statistically associated with BV were multiple sexual partners and history of sexually transmitted disease (P<0.05). This is consistent with earlier studies performed in Germany, Australia, Cameroon, Ethiopia and Nigeria.17,61–65 Even if the mechanism is unknown, having multiple sexual partners and a history of STI can upset/disturb the normal flora of the vagina (lactobacilli) and facilitate the growth of diverse anaerobic bacteria.14
Pregnant women with vaginal discharge were among the factors statistically associated with bacterial vaginosis (P<0.05). This is comparable with studies conducted in Brazil, the USA, Botswana and Nigeria.31,66–68 The results of this study indicated that pregnant women with vaginal discharge have a high diagnostic value, since nearly two-thirds (67.9%) of BV positive individuals reported vaginal discharge in this study. This might be because the most prevalent clinical sign and symptom of BV infection is abnormal vaginal discharge.1,8 History of spontaneous abortion was also an independent predictor of bacterial vaginosis in this study (P<0.05). This is consistent with studies performed in Belgium, Burkina Faso, Nigeria and Ethiopia.16,52,69,70 This might be related to lytic enzymes produced by BV-associated bacteria, such as proteases and phospholipase, which cause lysis of phospholipids in fetal membranes and cell membranes of clue cells. Arachidonic acid is generated during phospholipid lysis; this acid induces prostaglandin induction (PGs). PGs cause uterine muscle contraction, sulfated glycosaminoglycan (GAG) reduction, collagen fibril restructuring, and cervical resistance reduction. In addition, PGs stimulate the release of metalloproteinases from neutrophils via inducing the release of inflammatory cytokines. Metalloproteinases break down connective tissue such as the chorioamniotic membrane, which leads to spontaneous abortion.71–73
Limitations of the Study
Lack of gas producing kits for cultivation of strictly anaerobic bacteria such as Bacteroides species, Prevotella, A. vaginae and others. Some confidence intervals were wide due to the small sample size.
Drug susceptibility was not conducted for G. vaginalis due to lack of antibiotic drugs in powder form.
Conclusion
The overall prevalence of bacterial vaginosis among pregnant women is higher than found in previous studies conducted by Nugent’s scoring system and Amsel’s criteria. The prevalence of bacterial vaginosis is higher among symptomatic pregnant women and associated with a previous history of sexually transmitted infection, vaginal discharge, multiple sexual partners and history of spontaneous abortion. Therefore, as BV is common in pregnant women, early diagnosis of pregnant women with the above factors should be an integral part of the laboratory investigation, which is vital for good pregnancy outcomes and necessary to reduce the complications.
Data Sharing Statement
Due to the privacy policy, the datasets are not publicly available. On reasonable request, the corresponding author will provide the data that support the findings of this study.
Acknowledgment
We are thankful to all our microbiology staff for their excellent technical support. We are grateful to Family Guidance Association of Ethiopia and Hiwot Fana Specialized University Hospital management and study participants for their kind cooperation. Finally, we would like to thank Haramaya University for financial support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting the manuscript, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. In the amended draft, the English version was edited.
Disclosure
The authors declare that they have no conflicts of interests.
References
1. Drew RJ, Murphy T, Broderick D, O’Gorman J, Eogan M. An interpretation algorithm for molecular diagnosis of bacterial vaginosis in a maternity hospital using machine learning: proof-of-concept study. Diagn Microbiol Infect Dis. 2020;96(2):114950. doi:10.1016/j.diagmicrobio.2019.114950
2. Abdelaziz ZA, Ibrahim ME, Bilal NE, Hamid ME. Vaginal infections among pregnant women at Omdurman Maternity Hospital in Khartoum, Sudan. J Infect Dev Ctries. 2014;8(4):490–497. doi:10.3855/jidc.3197
3. Marrazzo JM, Martin DH, Watts DH, et al. Bacterial vaginosis: identifying research gaps proceedings of a workshop sponsored by DHHS/NIH/NIAID November 19–20, 2008. Sex Transm Dis. 2010;37(12):732. doi:10.1097/OLQ.0b013e3181fbbc95
4. Turovskiy Y, Sutyak Noll K, Chikindas ML. The aetiology of bacterial vaginosis. J Appl Microbiol. 2011;110(5):1105–1128. doi:10.1111/j.1365-2672.2011.04977.x
5. Bautista CT, Wurapa E, Sateren WB, Morris S, Hollingsworth B, Sanchez JL. Bacterial vaginosis: a synthesis of the literature on etiology, prevalence, risk factors, and relationship with chlamydia and gonorrhea infections. Mil Med Res. 2016;3(1):1–10. doi:10.1186/s40779-016-0074-5
6. Gajdács M, Zsoldiné Urbán E. Epidemiology and resistance trends of Staphylococcus aureus isolated from vaginal samples: a 10-year retrospective study in Hungary. Acta Dermatovenerol Alp PanonAdriat. 2019;28(4):143–147. doi:10.15570/actaapa.2019.35
7. Jones A. Bacterial vaginosis: a review of treatment, recurrence, and disparities. J Nurse Pract. 2019;15(6):420–423. doi:10.1016/j.nurpra.2019.03.010
8. Bilardi JE, Walker S, Temple-Smith M, et al. The burden of bacterial vaginosis: women’s experience of the physical, emotional, sexual and social impact of living with recurrent bacterial vaginosis. PLoS One. 2013;8(9):e74378. doi:10.1371/journal.pone.0074378
9. Ugwumadu A. Role of antibiotic therapy for bacterial vaginosis and intermediate flora in pregnancy. Best Pract Res Clin Obstet Gynaecol. 2007;21(3):391–402. doi:10.1016/j.bpobgyn.2007.01.001
10. Işik G, Demirezen Ş, Dönmez HG, Beksaç MS. Bacterial vaginosis in association with spontaneous abortion and recurrent pregnancy losses. J Cytol. 2016;33(3):135. doi:10.4103/0970-9371.188050
11. Mehta SD, Agingu W, Nordgren RK, et al. Characteristics of women and their male sex partners predict bacterial vaginosis among a prospective cohort of Kenyan women with nonoptimal vaginal microbiota. Sex Transm Dis. 2020;47(12):840. doi:10.1097/OLQ.0000000000001259
12. Cohen CR, Lingappa JR, Baeten JM, et al. Bacterial vaginosis associated with increased risk of female-to-male HIV-1 transmission: a prospective cohort analysis among African couples. PLoS Med. 2012;9(6):e1001251. doi:10.1371/journal.pmed.1001251
13. Atashili J, Poole C, Ndumbe PM, Adimora AA, Smith JS. Bacterial vaginosis and HIV acquisition: a meta-analysis of published studies. AIDS. 2008;22(12):1493. doi:10.1097/QAD.0b013e3283021a37
14. Tesfay G, Deekonda K, Paramasivam R, Muthupandian S. Prevalence and associated risk factors of bacterial vaginosis among pregnant women in Africa: a systematic review; 2020.
15. Kenyon C, Colebunders R, Crucitti T. The global epidemiology of bacterial vaginosis: a systematic review. Am J Obstet Gynecol. 2013;209(6):505–523. doi:10.1016/j.ajog.2013.05.006
16. Mulu W, Yimer M, Zenebe Y, Abera B. Common causes of vaginal infections and antibiotic susceptibility of aerobic bacterial isolates in women of reproductive age attending at Felegehiwot referral Hospital, Ethiopia: a cross sectional study. BMC Women’s Health. 2015;15(1):42. doi:10.1186/s12905-015-0197-y
17. Mengistie Z, Woldeamanuel Y, Asrat D, Adera A. Prevalence of bacterial vaginosis among pregnant women attending antenatal care in Tikur Anbessa University Hospital, Addis Ababa, Ethiopia. BMC Res Notes. 2014;7(1):822. doi:10.1186/1756-0500-7-822
18. Chavoustie SE, Eder SE, Koltun WD, et al. Experts explore the state of bacterial vaginosis and the unmet needs facing women and providers. Int J Gynecol Obstet. 2017;137(2):107–109. doi:10.1002/ijgo.12114
19. Bautista CT, Wurapa EK, Sateren WB, Morris SM, Hollingsworth BP, Sanchez JL. Association of bacterial vaginosis with chlamydia and gonorrhea among women in the US Army. Am J Prev Med. 2017;52(5):632–639. doi:10.1016/j.amepre.2016.09.016
20. Amsel R, Totten PA, Spiegel CA, Chen KC, Eschenbach D, Holmes KK. Nonspecific vaginitis: diagnostic criteria and microbial and epidemiologic associations. Am J Med. 1983;74(1):14–22. doi:10.1016/0002-9343(83)91112-9
21. Amegashie CP, Gilbert NM, Peipert JF, Allsworth JE, Lewis WG, Lewis AL. Relationship between nugent score and vaginal epithelial exfoliation. PLoS One. 2017;12(5):e0177797. doi:10.1371/journal.pone.0177797
22. Antonucci F, Mirandola W, Fontana C, Fontana C. Comparison between Nugent’s and Hay/Ison scoring criteria for the diagnosis of bacterial vaginosis in WASP prepared vaginal samples. Clin Investig. 2017;7:89–93.
23. Coleman JS, Gaydos CA. Molecular diagnosis of bacterial vaginosis: an update. J Clin Microbiol. 2018;56(9):e00342–e00318. doi:10.1128/JCM.00342-18
24. Martin DH, Ferris MJ. Endogenous microbiota of the genitourinary tract. In: Mucosal Immunology. Elsevier; 2015:95–107.
25. Nugent RP, Krohn MA, Hillier SL. Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J Clin Microbiol. 1991;29(2):297–301. doi:10.1128/jcm.29.2.297-301.1991
26. Spiegel CA, Amsel R, Holmes K. Diagnosis of bacterial vaginosis by direct gram stain of vaginal fluid. J Clin Microbiol. 1983;18(1):170–177. doi:10.1128/jcm.18.1.170-177.1983
27. Rogosa M, Sharpe ME. Species differentiation of human vaginal lactobacilli. Microbiology. 1960;23(1):197–201.
28. Sigmon J. The Starch Hydrolysis Test. American Society for Microbiology; 2008.
29. Bhat G, Kotigadde S, Shenoy S. Comparison of the methods of diagnosis of bacterial vaginosis. J Clin Diagnostic Res. 2011;5(3):498–501.
30. Lata I, Pradeep Y, Sujata AJ. Estimation of the incidence of bacterial vaginosis and other vaginal infections and its consequences on maternal/fetal outcome in pregnant women attending an antenatal clinic in a tertiary care hospital in North India. IJCM. 2010;35(2):285. doi:10.4103/0970-0218.66855
31. Simoes J, Discacciati M, Brolazo E, Portugal P, Dini D, Dantas M. Clinical diagnosis of bacterial vaginosis. Int J Gynecol Obstet. 2006;94(1):28–32. doi:10.1016/j.ijgo.2006.04.013
32. Ibrahim S, Bukar M, Galadima G, Audu B, Ibrahim H. Prevalence of bacterial vaginosis in pregnant women in Maiduguri, North Eastern Nigeria. Niger J Clin Pract. 2014;17(2):154–158. doi:10.4103/1119-3077.127424
33. Redelinghuys MJ, Ehlers MM, Dreyer AW, Lombaard H, Olorunju SA, Kock MM. A cross-sectional study on the relationship of age, gestational age and HIV infection to bacterial vaginosis and genital mycoplasma infection. BMJ Open. 2015;5(10):e008530. doi:10.1136/bmjopen-2015-008530
34. Masha SC, Wahome E, Vaneechoutte M, Cools P, Crucitti T, Sanders EJ. High prevalence of curable sexually transmitted infections among pregnant women in a rural county hospital in Kilifi, Kenya. PLoS One. 2017;12(3):e0175166. doi:10.1371/journal.pone.0175166
35. Machado D, Castro J, Martinez-de-oliveira J, Nogueira-Silva C, Cerca N. Prevalence of bacterial vaginosis in Portuguese pregnant women and vaginal colonization by Gardnerella vaginalis. PeerJ. 2017;5:e3750. doi:10.7717/peerj.3750
36. Dadhwal V, Hariprasad R, Mittal S, Kapil A. Prevalence of bacterial vaginosis in pregnant women and predictive value of clinical diagnosis. Arch Gynecol Obstet. 2010;281(1):101–104. doi:10.1007/s00404-009-1089-x
37. Teixeira PM, Vital WC, Lima AA, et al. Bacterial vaginosis: prevalence, risk profile and association with sexually transmitted infections. J Epidemiol Infect. 2020;10(3). doi:10.17058/jeic.v10i3.14984.
38. Shayo PA, Kihunrwa A, Massinde AN, et al. Prevalence of bacterial vaginosis and associated factors among pregnant women attending at Bugando Medical Centre, Mwanza, Tanzania. Tanzan J Health Res. 2012;14(3):175–182. doi:10.4314/thrb.v14i3.3
39. Konadu DG, Owusu-Ofori A, Yidana Z, et al. Prevalence of vulvovaginal candidiasis, bacterial vaginosis and trichomoniasis in pregnant women attending antenatal clinic in the middle belt of Ghana. BMC Pregnancy Childbirth. 2019;19(1):341. doi:10.1186/s12884-019-2488-z
40. Kurewa NE, Mapingure MP, Munjoma MW, Chirenje MZ, Rusakaniko S, Stray-Pedersen B. The burden and risk factors of sexually transmitted infections and reproductive tract infections among pregnant women in Zimbabwe. BMC Infect Dis. 2010;10(1):127. doi:10.1186/1471-2334-10-127
41. Olowe O, Makanjuola O, Olowe R, Adekanle D. Prevalence of vulvovaginal candidiasis, trichomoniasis and bacterial vaginosis among pregnant women receiving antenatal care in Southwestern Nigeria. Eur J Microbiol Immunol. 2014;4(4):193–197. doi:10.1556/EUJMI-D-14-00027
42. Waters TP, Denney JM, Mathew L, Goldenberg RL, Culhane JF. Longitudinal trajectory of bacterial vaginosis during pregnancy. Am J Obstet Gynecol. 2008;199(4):
43. Bartellas E, Crane JM, Daley M, Bennett KA, Hutchens D. Sexuality and sexual activity in pregnancy. BJOG: Int J Obstet Gynaecol. 2000;107(8):964–968. doi:10.1111/j.1471-0528.2000.tb10397.x
44. Uwapusitanon W, Choobun T. Sexuality and sexual activity in pregnancy. J Med Assoc Thai. 2004;87 Suppl 3:S45–S49.
45. Verstraelen H, Verhelst R, Vaneechoutte M, Temmerman M. The epidemiology of bacterial vaginosis in relation to sexual behaviour. BMC Infect Dis. 2010;10(1):1–11. doi:10.1186/1471-2334-10-81
46. Rumyantseva TA, Bellen G, Romanuk TN, et al. Utility of microscopic techniques and quantitative real-time polymerase chain reaction for the diagnosis of vaginal microflora alterations. J Low Genit Tract Dis. 2015;19(2):124–128. doi:10.1097/LGT.0000000000000060
47. Baruah FK, Sharma A, Das C, Hazarika NK, Hussain JH. Role of Gardnerella vaginalis as an etiological agent of bacterial vaginosis. Iran J Microbiol. 2014;6(6):409.
48. Delaney ML, Onderdonk AB; Microbiology and Prematurity Study Group. Nugent score related to vaginal culture in pregnant women. Obstet Gynecol. 2001;98(1):79–84.
49. Bramley H, Dixon R, Jones B. Haemophilus vaginalis (Corynebacterium vaginale, Gardnerella vaginalis) in a family planning clinic population. Sex Transm Infect. 1981;57(1):62–66. doi:10.1136/sti.57.1.62
50. Buyukbayrak EE, Kars B, Karsidag AYK, et al. Diagnosis of vulvovaginitis: comparison of clinical and microbiological diagnosis. Arch Gynecol Obstet. 2010;282(5):515–519. doi:10.1007/s00404-010-1498-x
51. Mehreen I, Nuzhat S, Saadia D, Muhammad Z, Shazia T. Comparison of vaginal culture and pap smear in the diagnosis of bacterial vaginosis; 2017.
52. Damen JG, Suleiman SZ, Vem ST, Goltong J, Kahansim M. Microbiological diagnosis of bacterial vaginosis in pregnant women in a resource limited setting in north central Nigeria. Am J Life Sci. 2014. 2(6):356. doi:10.11648/j.ajls.20140206.15.
53. Rao P, Devi S, Shriyan A, Rajaram M, Jagdishchandra K. Diagnosis of bacterial vaginosis in a rural setup: comparison of clinical algorithm, smear scoring and culture by semiquantitative technique. Indian J Med Microbiol. 2004;22(1):47–50. doi:10.1016/S0255-0857(21)02951-0
54. Pheifer TA, Forsyth PS, Durfee MA, Pollock HM, Holmes KK. Nonspecific vaginitis: role of Haemophilus vaginalis and treatment with metronidazole. N Engl J Med. 1978;298(26):1429–1434. doi:10.1056/NEJM197806292982601
55. Easmon C, Hay P, Ison C. Bacterial vaginosis: a diagnostic approach. Genitourin Med. 1992;68(2):134. doi:10.1136/sti.68.2.134
56. Demirezen Ş, Küçük A, Beksaç MS. The association between copper containing IUCD and bacterial vaginosis. Cent Eur J Public Health. 2006;14(3):138–140. doi:10.21101/cejph.a3339
57. Ness RB, Hillier S, Richter HE, et al. Can known risk factors explain racial differences in the occurrence of bacterial vaginosis? J Natl Med Assoc. 2003;95(3):201.
58. Kalinka J, Hanke W, Wasiela M, Laudański T. Socioeconomic and environmental risk factors of bacterial vaginosis in early pregnancy. J Perinatal Med. 2002;30(6):467–475. doi:10.1515/JPM.2002.073
59. Li X-D, Wang -C-C, Zhang X-J, et al. Risk factors for bacterial vaginosis: results from a cross-sectional study having a sample of 53, 652 women. Eur J Clin Microbiol Infect Dis. 2014;33(9):1525–1532. doi:10.1007/s10096-014-2103-1
60. Ocviyanti D, Rosana Y, Olivia S, Darmawan F. Risk factors for bacterial vaginosis among Indonesian women. Med J Indones. 2010;19(2):130–135. doi:10.13181/mji.v19i2.396
61. Smart S, Singal A, Mindel A. Social and sexual risk factors for bacterial vaginosis. Sex Transm Infect. 2004;80(1):58–62. doi:10.1136/sti.2003.004978
62. Allsworth JE, Peipert JF. Prevalence of bacterial vaginosis: 2001–2004 national health and nutrition examination survey data. Obstet Gynecol. 2007;109(1):114–120. doi:10.1097/01.AOG.0000247627.84791.91
63. Brotman RM, Klebanoff MA, Nansel TR, et al. A longitudinal study of vaginal douching and bacterial vaginosis—A marginal structural modeling analysis. Am J Epidemiol. 2008;168(2):188–196. doi:10.1093/aje/kwn103
64. Kamga YM, Ngunde JP, Akoachere J-FK. Prevalence of bacterial vaginosis and associated risk factors in pregnant women receiving antenatal care at the Kumba Health District (KHD), Cameroon. BMC Pregnancy Childbirth. 2019;19(1):166. doi:10.1186/s12884-019-2312-9
65. Durugbo II, Nyengidiki TK, Bassey G, Wariso KT. Bacterial vaginosis among women with tubal factor infertility in Nigeria. Int J Gynecol Obstet. 2015;131(2):133–136. doi:10.1016/j.ijgo.2015.05.031
66. Aduloju OP, Akintayo AA, Aduloju T. Prevalence of bacterial vaginosis in pregnancy in a tertiary health institution, south western Nigeria. Pan Afr Med J. 2019;33. doi:10.11604/pamj.2019.33.9.17926
67. Paavonen J, Brunham RC. Bacterial vaginosis and desquamative inflammatory vaginitis. N Engl J Med. 2018;379(23):2246–2254. doi:10.1056/NEJMra1808418
68. Romoren M, Velauthapillai M, Rahman M, Sundby J, Klouman E, Hjortdahl P. Trichomoniasis and bacterial vaginosis in pregnancy: inadequately managed with the syndromic approach. Bull World Health Organ. 2007;85:297–304. doi:10.2471/BLT.06.031922
69. Kirakoya-Samadoulougou F, Nagot N, Defer M-C, Yaro S, Meda N, Robert A. Bacterial vaginosis among pregnant women in Burkina Faso. Sex Transm Dis. 2008;35(12):985–989. doi:10.1097/OLQ.0b013e3181844f22
70. Donders GG, Van Bulck B, Caudron J, Londers L, Vereecken A, Spitz B. Relationship of bacterial vaginosis and mycoplasmas to the risk of spontaneous abortion. Am J Obstet Gynecol. 2000;183(2):431–437. doi:10.1067/mob.2000.105738
71. Govender L, Hoosen AA, Moodley J, Moodley P, Sturm AW. Bacterial vaginosis and associated infections in pregnancy. Int J Gynecol Obstet. 1996;55(1):23–28. doi:10.1016/0020-7292(96)02744-0
72. Imseis HM, Greig PC, Livengood CH, Shunior E, Durda P, Erikson M. Characterization of the inflammatory cytokines in the vagina during pregnancy and labor and with bacterial vaginosis. J Soc Gynecol Investig. 1997;4(2):90–94. doi:10.1177/107155769700400208
73. Ji H, Dailey TL, Long V, Chien EK. Prostaglandin E2–regulated cervical ripening: analysis of proteoglycan expression in the rat cervix. Am J Obstet Gynecol. 2008;198(5):
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.