")
Back to Journals » Clinical Ophthalmology » Volume 14
Bacterial Detection Rate and Surgical Outcome in Povidone-Iodine Irrigation After Nasolacrimal Duct Intubation
Authors Ishikawa S, Shoji T , Yamada N, Shinoda K
Received 28 May 2019
Accepted for publication 20 December 2019
Published 23 January 2020 Volume 2020:14 Pages 205—211
DOI https://doi.org/10.2147/OPTH.S217484
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sho Ishikawa,1 Takuhei Shoji,1 Norihiro Yamada,2 Kei Shinoda1
1Department of Ophthalmology, Saitama Medical University, Saitama, Japan; 2Department of Ophthalmology, Yokohama City University, Kanagawa, Japan
Correspondence: Sho Ishikawa
Department of Ophthalmology, Saitama Medical University, 38 Morohongo, Moroyama, Saitama 350-0495, Japan
Tel +81-4-9276-1250
Fax +81-4-9295-8002
Email [email protected]
Purpose: In various ophthalmic surgical procedures, 0.25% povidone-iodine (PI) solution is used to prevent infections. This study examined the bacterial colonisation before and after endoscopic nasolacrimal duct intubation irrigated with PI solution and investigated the relationship between bacterial detection and surgical failure.
Methods: A retrospective study at Saitama Medical University Hospital. We enrolled 113 patients (33 men, 80 women) who underwent lacrimal intubation surgery between April 2016 and December 2018. Preoperatively, the lacrimal pathways were washed with normal saline solution, which was subsequently cultured. The sites of obstruction in the lacrimal pathway were endoscopically determined, perforated, and intubated. The tubes were afterward either irrigated with 0.25% PI or normal saline every 2 weeks. After 8 weeks, a piece of the removed lacrimal tube was cultured. We characterized the pre- and postoperative bacterial cultures.
Results: We enrolled 54 and 52 patients in PI and saline groups (mean age: 69.1± 9.2 and 73.2± 7.2 years), respectively. In the PI group, Staphylococcus epidermidis was less frequently detected postoperatively than preoperatively. S. oralis and Candida parapsilosis were identified more often postoperatively (P=0.02, P=0.01, respectively). The PI group had significantly lower bacterial detection rate than the saline group (P=0.01). However, the surgical failure rates did not differ between groups. In surgical failure patients, the postoperative rate of Pseudomonas aeruginosa was very high (75%).
Conclusion: PI reduces the bacterial detection rate but does not improve the surgical success rate. P. aeruginosa is associated with an increased risk of surgical failure.
Keywords: nasolacrimal intubation, povidone-iodine, syringing, bacterial population, lacrimal obstructive disease
Introduction
Obstruction or stenosis of the nasolacrimal system causes lacrimation, so generally, either topical antibiotics or surgical treatment is chosen. Dacryocystorhinostomy (DCR) restores the drainage of tears by bypassing a blockage in the nasolacrimal duct through the creation of a bony ostium and is the primary treatment choice for cases with primary acquired nasolacrimal duct obstruction. Silicone tube intubation was first introduced by Keith1 who used the technique in patients with nasolacrimal duct obstruction as an alternative to DCR. Since then silicone intubation has become an established alternative treatment option. The reported success rate of silicone tube intubation in patients with nasolacrimal duct stenosis ranges from 40% to 75%.2–6 The timing of the tube removal is reportedly between 1 week and several years, with 2- to 6-months post intubation being the most common removal period.6–8 Many hospitals prescribe antibiotic eye drops while the silicone tube is retained, which carries the risk of creating resistant bacteria. Additionally, patients with nasolacrimal duct obstruction do not have normal conjunctival flora because of chronic dacryocystitis9 and the long-term use of antibiotics. In DCR surgery, it is reported that Pseudomonas infection of the silicone tube is significantly higher in cases with revision than in those without revision, but this is not the case in endoscopic nasolacrimal duct intubation.10
Preoperative povidone-iodine (PI) solution is strongly recommended to prevent bacterial endophthalmitis in cataract surgery.11 Shimada et al reported that irrigating the operative field with 0.25% PI during cataract surgery resulted in a reduction of the bacterial detection rate to 0%.12 After this report, PI was included in various ophthalmic surgical procedures.13–16 A meta-analysis of non-ophthalmic surgical procedures revealed that PI significantly reduces the postoperative infection rate in clean but not in dirty or contaminated wounds.17 However, the efficacy of PI after intubation surgery has not been reported yet. In the present study, we retrospectively compared bacterial cultures before and after endoscopic nasolacrimal duct intubation in patients irrigated with either 0.25% PI solution or normal saline solution.
Materials and Methods
This retrospective study was approved by the Ethical Committee of Saitama Medical University Hospital (18152.01, clinical trial number was UMIN000031981) and was conducted in accordance with the provisions of the Declaration of Helsinki. All subjects had given written informed consent to the surgical procedure. The need for additional informed consent apart from that for the surgical procedures was waived by the Ethical Committee of Saitama Medical University because of the study’s retrospective design. Patient data was used only for this study and patient confidentiality was preserved. The datasets generated and/or analysed during the current study are available only this study.
We enrolled 113 patients (33 men, 80 women) who underwent lacrimal intubation surgery at Saitama Medical University Hospital between April 2016 and December 2018. All patients with a history of lacrimal surgery, trauma of the eyelid, or hypersensitivity or allergic reactions to PI were excluded. Additionally, patients affected by epiphora not caused by a lacrimal obstructive disease, eg, patients with lid position anomalies, eyelash anomalies, blepharitis, allergic conjunctivitis, infectious conjunctivitis, conjunctivochalasis, facial palsy, or punctal stenosis or obstruction were also excluded.
The detailed procedure was as follows. First, all patients underwent comprehensive ophthalmologic examinations, including slit-lamp examinations. We excluded all patients with no obstruction of the nasolacrimal system.
Second, using a 23G Nakamura’s lacrimal washing single-size needle® (Inami, Tokyo, Japan) filled with saline solution, the lacrimal pathway was washed to determine whether it was obstructed. The diagnosis of a lacrimal obstructive disease was made when the saline solution did not reach the nasal cavity. The epiphora severity was scored as follows: Munk score 0, no watering; 1, occasional watering requiring dabbing less than twice a day; 2, watering requiring dabbing 2–4 times a day; 3, watering requiring dabbing 5–10 times a day; 4, watering requiring dabbing more than 10 times a day or constant watering.18 Other symptoms, such as irritation and foreign body sensation, were scored using the ocular surface disease index (OSDI). The OSDI provides a tool for the rapid assessment of the symptoms of ocular irritation consistent with dry eye disease and their impact on vision-related functions, scoring from 0–100.19
Third, we performed lacrimal intubation surgery. Prior to surgery, we washed the lacrimal pathway with normal saline solution and cultured the reflux from the lacrimal pathway (1st bacterial examination; preoperative). The lacrimal surgery to perforate the obstruction using the lacrimal endoscope (Fibertech, Chiba, Japan) and to intubate the lacrimal pathway was successful in all cases. The site of obstruction of the lacrimal pathway was localized during this surgical procedure. For intubation, we used LACRIFAST® (Kaneka Medical Products, Osaka, Japan) with a lacrimal tube.
Fourth, after the lacrimal surgery, patients were assigned to the 0.25% PI solution group (PI group) or the normal saline group (saline group) according to the surgeon’s preference. Either PI or saline was used as an irrigating solution to wash the lacrimal pathway. We syringed the lacrimal pathway every 2 weeks to prevent occlusion and lacrimal tube infection for 8 weeks. We syringed with 5mL in both groups. All patients received 0.3% gatifloxacin and 0.1% fluorometholone topically four times a day for 8 weeks.
Fifth, 8 weeks later, we removed the lacrimal tube after syringed the lacrimal pathway. The extracted lacrimal tube was divided into three parts based on the distance from the punctal portion: up to 20 mm (from the puncta to the lacrimal sac), up to 40 mm (in the nasolacrimal duct), and above 40 mm (in the nasal cavity) immediately after removed lacrimal tube. We cultured the second piece (2nd bacterial examinations; postoperative).
Finally, we evaluated the success of the procedure 3 months after the surgery. Surgical success was defined as successful fluid irrigation of the lacrimal pathway without reflux during this procedure. Surgical failure was established by the absence of fluid in the nasal cavity during the irrigation of the lacrimal pathway.
All statistical analyses were performed using the software JMP version 11® (SAS Institute, Tokyo, Japan). All data are expressed as means ± SD. The Mann–Whitney U-test was applied for the comparison of Munk scores between the PI group and the saline group. The unpaired t-test was applied for the age between both groups. The chi-square test was used for the comparison of sex and the bacterial detection rate before and after surgery. Statistical significance was set at P<0.05. Note that P-values smaller than 0.001 are presented as P<0.001.
Results
A total of 113 patients were enrolled. Of these, 7 patients were excluded (5 cases with hypersensitivity to or irritation by PI and 1 case with lack of informed consent). Thus, 54 patients in the PI group and 52 patients in the saline group were included in this study. The mean ages of the study participants were 69.1±9.2 years in the PI group and 73.2±7.2 years in the saline group. The mean age of the saline group was significantly higher than that of the PI group (P=0.01). The sex distribution of the groups was not statistically significantly different. The obstruction sites in patients of the PI group and the saline group were determined as the nasolacrimal duct in 43 and 39 patients, the common canaliculus in 8 and 12 patients, and the superior canaliculus in 2 and 1 patients, respectively. One patient of the PI group presented an obstruction of the inferior canaliculus. The Munk and OSDI scores were not different between the PI group (3.72±1.45 and 28.25±14.90, respectively) and the saline group (3.46±1.50 and 20.63±10.33, respectively; see Table 1).
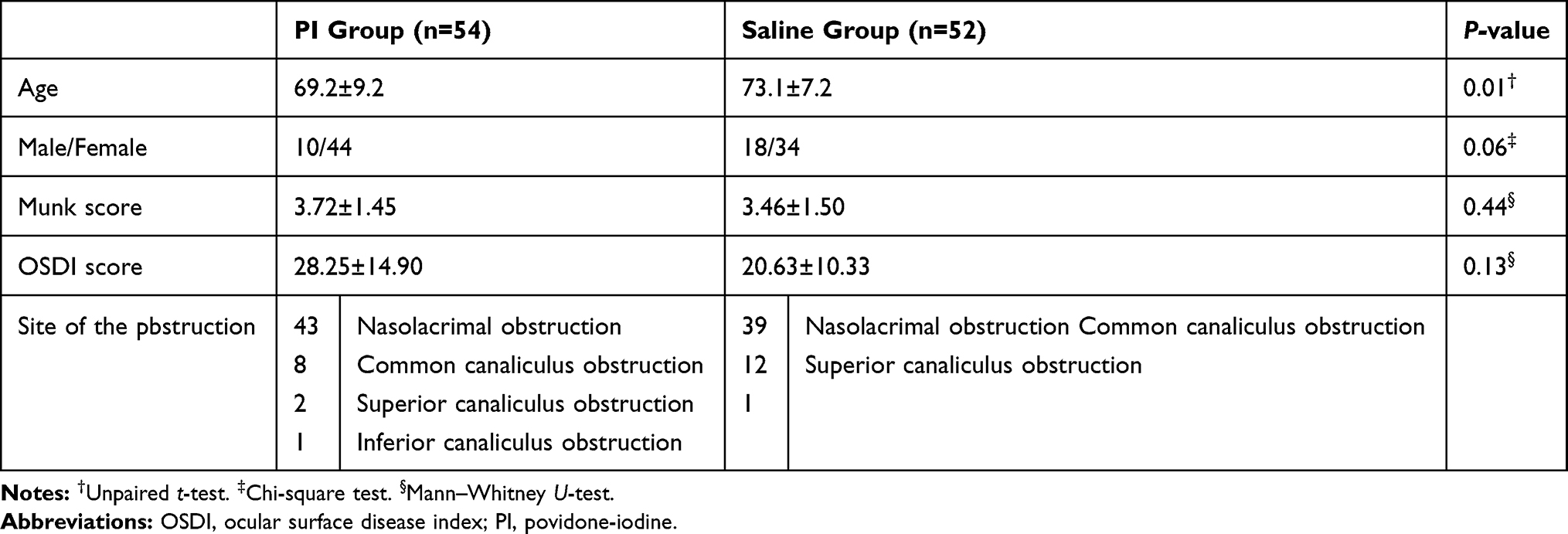 |
Table 1 Profile of the PI and the Saline Group |
Table 2 shows the pre- and postoperative detection of bacterial species in the PI and the saline group. Importantly, the rates of patients without detected bacteria were preoperatively similar for both groups. However, postoperatively, the rate was significantly lower in the PI group than in the saline group (PI, 14/54 vs saline, 4/52; p=0.01 in Table 2). In the PI group, Staphylococcus epidermidis was less frequently detected after surgery than before surgery (P = 0.02). S. oralis and C. parapsilosis were discovered postoperatively more often than preoperatively (P=0.02 and P=0.01, respectively). In the saline group, S. epidermidis was less frequent after surgery than before surgery (P<0.01). S. oralis and Corynebacterium species were identified more often postoperatively than preoperatively (both P<0.01). The postoperative bacterial detection rate was significantly lower in the PI group than in the saline group (P=0.01).
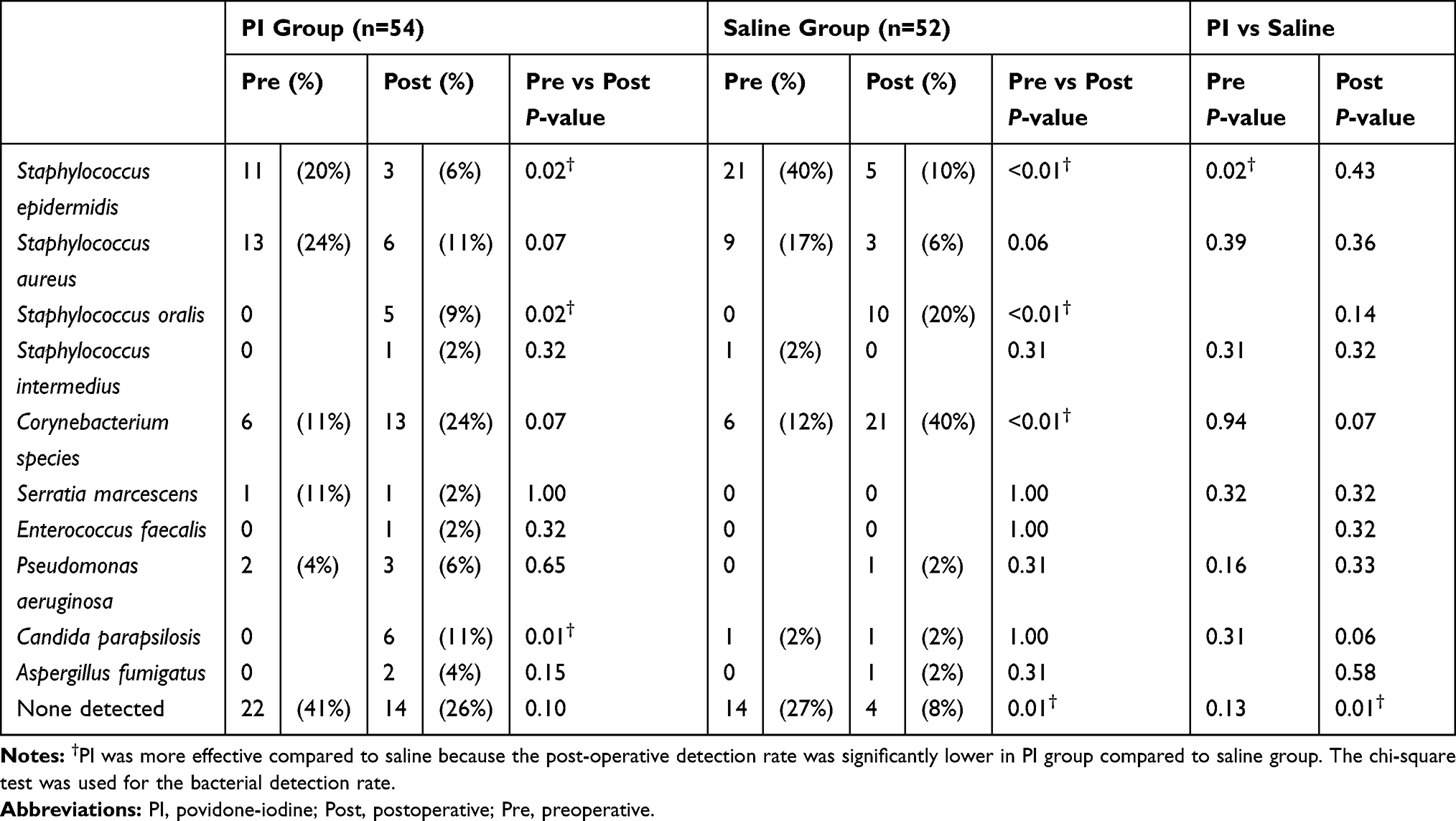 |
Table 2 Pre- and Postoperative Detection of Bacterial Species |
Three months after surgery, surgical failure occurred in 3 and 4 patients of the PI and the saline group, respectively. The frequencies of surgical failures did not differ between the PI group (6%) and the saline group (8%, P=0.65). The mean OSDI score in the surgical failure group was significantly higher than that in the surgical success group in both the PI and saline groups (both P<0.01). Between the PI and saline groups, there were no differences in age, sex, and Munk score (Table 3). The profiles of the patients with surgical failure are shown for the PI and saline groups in Table 4. In patients with a surgical failure outcome, the postoperative detection rate of Pseudomonas aeruginosa was very high (75%) regardless of the group (PI group, 67%; saline group, 100%).
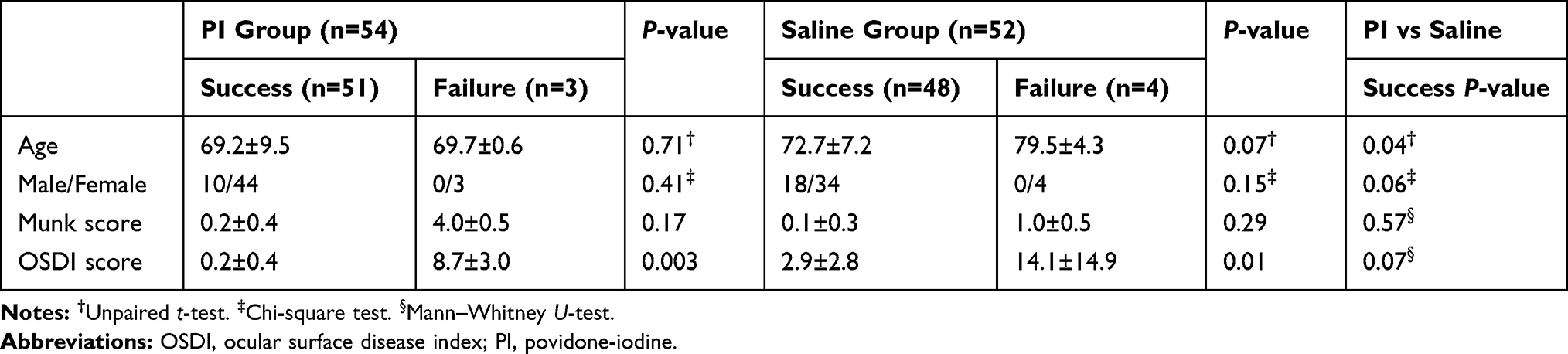 |
Table 3 Profile of the PI and Saline Groups 8 Weeks Postoperatively |
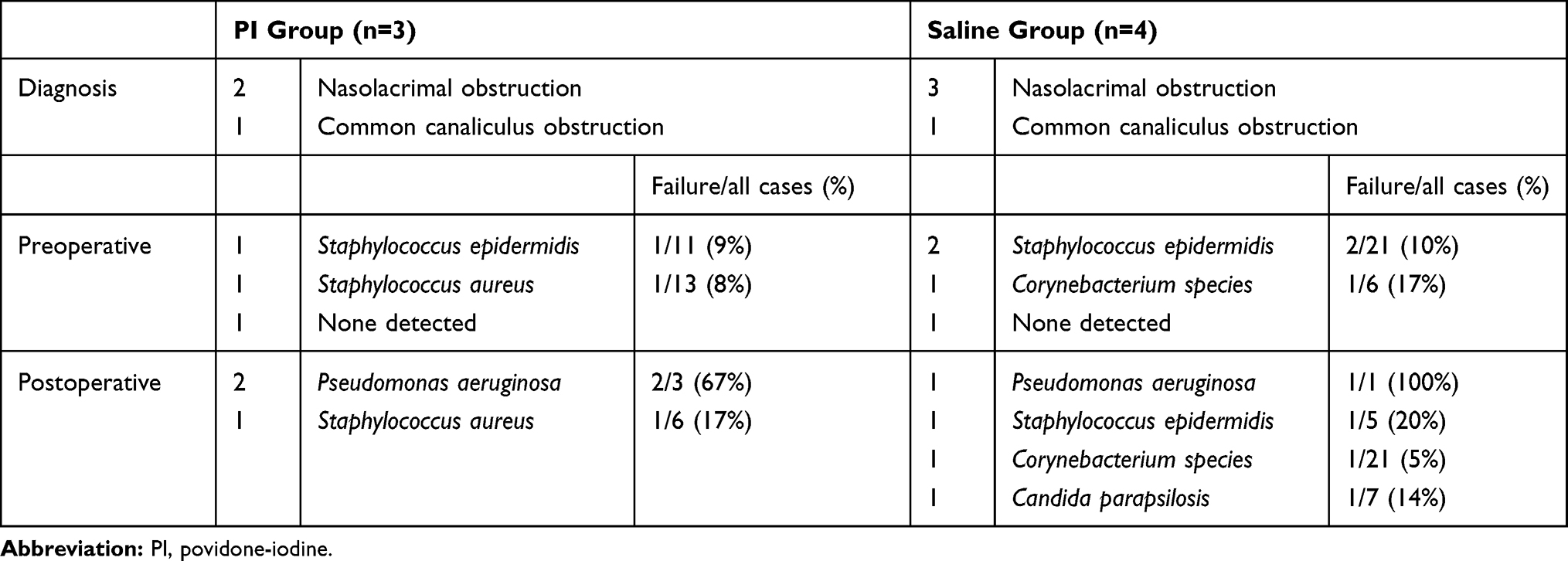 |
Table 4 Profile of Patients with Surgical Failure in the PI and Saline Groups |
We syringed the lacrimal pathway every 2 weeks and recorded unwanted effects. Although no patient of the PI group or the saline group felt ocular pain or experienced conjunctival redness, 2 patients of the PI group felt a slight throat irritation.
Discussion
In the present study, we showed that washing the lacrimal pathway with PI solution reduces the detection rate of bacteria but does not improve the surgical success rate compared to saline solution. The detection rate of S. epidermidis was reduced postoperatively in both the PI group and the saline group. On the other hand, the detection rate of S. oralis was increased postoperatively in both groups, and Corynebacterium species were more often observed in the saline group, whereas C. parapsilosis was more frequently identified in the PI group. The postoperative detection of P. aeruginosa was associated with a high risk of surgical failure.
Previous studies have suggested that postoperative infection and inflammation such as Pseudomonas infection,10 lacrimal scarring,20 and fibrosis due to prolonged silicone intubation10,20 might be associated with result of nasolacrimal surgery. An inflammation may either be caused by bacterial contamination or by mechanical stress induced by the tube. It was reported that silicone tube intubation does not induce significant histopathological changes of the lacrimal sac.21 Moreover, in chronic dacryocystitis patients, chronic inflammation with fibrosis is the most commonly revealed histopathological finding in biopsies of the lacrimal sac wall.22 For these reasons, we suggest that the most frequent cause of postoperative lacrimal obstruction is not the tube itself but its bacterial contamination.
In this study, S. epidermidis was less frequently detected after than before surgery in both the PI and saline groups. The detection rates of S. oralis and C. parapsilosis were increased postoperatively in comparison to their preoperative rates, and we suppose these bacteria are derived from the nasal cavity. By contrast, Corynebacterium species were identified more often after than before surgery but only in the saline group. We assume that the topical gatifloxacin administration effectively reduced a Staphylococcus epidermidis contamination but that the Corynebacterium species were resistant to this drug. In this study, all Corynebacterium species detected in tube samples were resistant to quinolone antibiotics. PI solution has the advantage that it does not induce bacterial resistance.
In the present study, the P. aeruginosa detection rate was high in the surgical failure group. In DCR surgery, it has been reported that the Pseudomonas infection rate of silicone tubes is significantly higher in cases with revision than in those without revision.10 Moreover, isolation of P. aeruginosa from silicone tube biofilms is associated with a high rate (50%) of surgical failure.23 In in vitro experiments, only S. aureus and P. aeruginosa formed after 12 weeks biofilms on silicon tubes incubated in culture media with various bacteria.24 We suggest that the formation of a biofilm is correlated with surgical failure. In the current study, we prescribed prophylactically antibiotic eye drops (0.3% gatifloxacin), but all detected P. aeruginosa strains were resistant to gatifloxacin in drug susceptibility tests. In the case of drug-resistant bacteria, PI might be helpful in preventing the formation of a biofilm.
Several limitations of the present study should be noted. First, the pre- and postoperative samples differed. The preoperative sample was acquired from the reflux discharge representing the lacrimal pathway and the conjunctival sac, whereas the postoperative sample consisted of the tube representing the bacteria of the nasolacrimal duct. Since the resident bacteria of these anatomical sites differ, we did not strictly compare the same things, but it was reported that there is a statistically significant similarity between isolates from lacrimal and nasal/conjunctival samples in patients with dacryocystitis and lacrimal obstruction.25,26 We tried to get postoperative samples from the reflux discharge, but there was no reflex all the cases after intubation surgery. Additionally, it was difficult to collect a sample of the lacrimal mucosa or lacrimal discharge during endoscopic surgery; hence, we cultured the tube instead of the reflex discharge. Second, we did not consider the side effects of PI affecting the lacrimal mucosa. PI is more easily absorbed by the mucosa than the skin, so PI administration might induce lacrimal mucosa changes. However, we did see the lacrimal mucosa during endoscopy, and we did not observe any changes after tube removal. Anaphylaxis can occur when PI is used for mucosa disinfection,27 but no cases of anaphylaxis related to its ophthalmic use have been reported yet. If the mucosa is exposed to PI for a long time, it can cause a chemical burn.28 Therefore, we excluded all patients who described an irritation or hypersensitivity to PI. Finally, this study only validates the short-term effects of the lacrimal surgery procedure. In a longer observation period, other factors might cause surgery failure, so long-term studies are needed in the future.
Conclusions
We demonstrate that compared to saline solution, 0.25% PI solution reduces the detection rate of bacterial contamination but does not improve the surgical success rate. P. aeruginosa isolated from the silicone tube is associated with an increased risk of surgical failure.
Abbreviations
DCR, dacryocystorhinostomy; PI, povidone-iodine.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this article.
References
1. Keith CG. Intubation of the lacrimal passages. Am J Ophthalmol. 1968;65:70–74. doi:10.1016/0002-9394(68)91031-3
2. Angrist RC, Dortzbach RK. Silicone intubation for partial and total nasolacrimal duct obstruction in adults. Ophthalmic Plast Reconstr Surg. 1985;1:51–54. doi:10.1097/00002341-198501000-00008
3. Connell PP, Fulcher TP, Chacko E, O’ Connor MJ, Moriarty P. Long term follow up of nasolacrimal intubation in adults. Br J Ophthalmol. 2006;90:435–436. doi:10.1136/bjo.2005.084590
4. Shah A, Tekriwal AK, Drummond PM, Woodruff G. Long-term results of closed nasolacrimal intubation in adults. Eur J Ophthalmol. 2007;17:490–493. doi:10.1177/112067210701700402
5. Mimura M, Ueki M, Oku H, Sato B, Ikeda T. Indications for and effects of Nunchaku-style silicone tube intubation for primary acquired lacrimal drainage obstruction. Jpn J Ophthalmol. 2015;59:266–272. doi:10.1007/s10384-015-0381-5
6. Inatani M, Yamauchi T, Fukuchi M, Denno S, Miki M. Direct silicone intubation using Nunchaku-style tube (NST-DSI) to treat lacrimal passage obstruction. Acta Ophthalmol Scand. 2000;78:689–693. doi:10.1034/j.1600-0420.2000.078006689.x
7. Demirci H, Elner VM. Double silicone tube intubation for the management of partial lacrimal system obstruction. Ophthalmology. 2008;115:383–385. doi:10.1016/j.ophtha.2007.03.078
8. Kabata Y, Goto S, Takahashi G, Tsuneoka H. Vision-related quality of life in patients undergoing silicone tube intubation for lacrimal passage obstructions. Am J Ophthalmol. 2011;152:147–150. doi:10.1016/j.ajo.2011.01.022
9. Shahraki K, Makateb A, Shirzadi K, Khosravifard K. Frequency of bacterial samples from patients with chronic acquired nasolacrimal duct obstruction. Med Arch. 2016;70:433–436. doi:10.5455/medarh.2016.70.433-436
10. Kim SE, Lee SJ, Lee SY, Yoon JS. Clinical significance of microbial growth on the surfaces of silicone tubes removed from dacryocystorhinostomy patients. Am J Ophthalmol. 2012;153:253–257. doi:10.1016/j.ajo.2011.06.030
11. Ciulla TA, Starr MB, Masket S. Bacterial endophthalmitis prophylaxis for cataract surgery: an evidence-based update. Ophthalmology. 2002;109:13–24. doi:10.1016/S0161-6420(01)00899-5
12. Shimada H, Arai S, Nakashizuka H, Hattori T, Yuzawa M. Reduction of anterior chamber contamination rate after cataract surgery by intraoperative surface irrigation with 0.25% povidone-iodine. Am J Ophthalmol. 2011;151:11–17. doi:10.1016/j.ajo.2010.07.002
13. Shimada H, Hattori T, Mori R, Nakashizuka H, Fujita K, Yuzawa M. Minimizing the endophthalmitis rate following intravitreal injections using 0.25% povidone-iodine irrigation and surgical mask. Graefes Arch Clin Exp Ophthalmol. 2013;251:1885–1890. doi:10.1007/s00417-013-2274-y
14. Shimada H, Nakashizuka H, Hattori T, et al. Prophylaxis for acute scleral buckle infection using 0.25 % povidone-iodine ocular surface irrigation during surgery. Int Ophthalmol. 2014;34:211–216. doi:10.1007/s10792-013-9816-5
15. Otani K, Shimada H, Nakashizuka H, Okubo H. Capsular bag irrigation using 0.025% povidone-iodine in balanced salt solution PLUS for the treatment of postoperative endophthalmitis. Int Ophthalmol. 2018;38:1787–1790. doi:10.1007/s10792-017-0645-9
16. Nakashizuka H, Shimada H, Hattori T, Tanaka K, Kitagawa Y, Shinoda K. Intravitreal injection of 1.25% povidone iodine followed by vitrectomy using 0.025% povidone iodine irrigation for treating endophthalmitis. Transl Vis Sci Technol. 2019;8:21. doi:10.1167/tvst.8.1.21
17. López-Cano M, Kraft M, Curell A, et al. A Meta-analysis of prophylaxis of surgical site infections with topical application of povidone iodine before primary closure. World J Surg. 2019;43:374–384. doi:10.1007/s00268-018-4798-0
18. Munk PL, Lin DT, Morris DC. Epiphora: treatment by means of dacryocystoplasty with balloon dilatation of the nasolacrimal drainage apparatus. Radiology. 1990;177:687–690.
19. Schiffman RM, Christianson MD, Jacobsen G, Hirsch JD, Reis BL. Reliability and validity of the ocular surface disease index. Arch Ophthalmol. 2000;118:615–621. doi:10.1001/archopht.118.5.615
20. Allen K, Berlin AJ. Dacryocystorhinostomy failure: association with nasolacrimal silicone intubation. Ophthalmic Surg. 1989;20:486–489.
21. Ciftci F, Erşanli D, Civelek L, Baloglu H, Karadayi K, Güngör A. Histopathologic changes in the lacrimal sac of dacryocystorhinostomy patients with and without silicone intubation. Ophthalmic Plast Reconstr Surg. 2005;21:59–64. doi:10.1097/01.IOP.0000148408.51615.FE
22. Amin RM, Hussein FA, Idriss HF, Hanafy NF, Abdallah DM. Pathological, immunohistochemical and microbiologicalal analysis of lacrimal sac biopsies in patients with chronic dacrocystitis. Int J Ophthalmol. 2013;6:817–826. doi:10.3980/j.issn.2222-3959.2013.06.14
23. Kim SH, Park CY, Hwang SW, Chang M. Clinical significance of biofilm on silicone tubes removed from patients with nasolacrimal duct stenosis. J Craniofac Surg. 2018;29:462–465. doi:10.1097/SCS.0000000000004191
24. Kim DJ, Park JH, Chang M. Species-specific characteristics of the biofilm generated in silicone tube: an in vitro study. BMC Ophthalmol. 2018;18:85. doi:10.1186/s12886-018-0750-1
25. Bale RN. Dacryocystitis: bacteriological study and its relation with nasal pathology. Indian J Ophthalmol. 1987;35:178–182.
26. Pradeep AV, Patil SS, Koti SV, Arunkumar JS, Garag SS, Hegde JS. Clinico-bacteriological study of chronic dacryocystitis cases in northern Karnataka, India. J Clin Diagn Res. 2013;7:2502–2504. doi:10.7860/JCDR/2013/6636.3590
27. Waran KD, Munsick RA. Anaphylaxis from povidone-iodine. Lancet. 1995;345:1506. doi:10.1016/S0140-6736(95)91063-8
28. Wykoff CC, Flynn HW
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.