")
Back to Journals » Open Access Journal of Sports Medicine » Volume 14
Awareness and Knowledge of Medical Issues Related to Female Athletes Among Track and Field Coaches
Authors Tsukahara Y , Kamada H, Torii S, Yamamoto H, Yamasawa F
Received 5 January 2023
Accepted for publication 15 March 2023
Published 23 March 2023 Volume 2023:14 Pages 9—19
DOI https://doi.org/10.2147/OAJSM.S403703
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Andreas Imhoff
Yuka Tsukahara,1,2 Hiroshi Kamada,2,3 Suguru Torii,2,4 Hiroshi Yamamoto,5 Fumihiro Yamasawa2
1Department of Sports Medicine, Tokyo Women’s College of Physical Education, Kunitachi, Japan; 2Medical Committee, Japan Association of Athletics Federations (JAAF), Tokyo, Japan; 3Department of Orthopaedic Surgery, University of Tsukuba, Tsukuba, Japan; 4Faculty of Sport Sciences, Waseda University, Tokorozawa, Japan; 5School of Sports and Health, Hosei University, Tokyo, Japan
Correspondence: Yuka Tsukahara, Department of Sports Medicine, Tokyo Women’s College of Physical Education, 4-30-1 Fujimidai, Kunitachi, Japan, Email [email protected]
Introduction: Little is known regarding medical knowledge pertaining to female athletes among track and field coaches and their interactions with female athletes regarding medical problems.
Methods: Participants were track and field coaches (369 males and 43 females) with Japan Sport Association certification and they completed an anonymous survey on their knowledge of medical problems pertinent to female athletes including whether the coaches knew about the female athlete triad and relative energy deficiency in sports; their feelings about female athletes’ use of contraceptive pills; whether they speak about menses with the female athletes; and whether they have a gynecologist for consultation regarding their medical problems.
Results: Females coaches were significantly more likely to be aware of the triad (odds ratio (OR), 3.44; p = 0.003); to have access to a physician able to address the gynecological problems of female athletes (OR, 9.22; p < 0.001); and to talk to their female athletes about menses (OR, 2.30; p = 0.015) than their male counterparts. Coaches with more experience tended to be aware of the triad and relative energy deficiency in sports compared with those with ≤ 5 years of experience.
Conclusion: Females coaches are aware of the triad, talk about menses with their female athletes, and have access to a physician who can address gynecological problems with compared to male counterparts. Educating all coaches on these problems is essential to provide adequate support to female athletes.
Keywords: track and field, relative energy deficiency in sports, female athlete triad syndrome
Introduction
Track and field is a multievent sport that includes both power events, such as jumping, throwing, and sprinting, and endurance events, such as long-distance running. Thus, there is potential for a wide range of injuries and illnesses. According to the Japan Association of Athletics Federations (JAAF), the most common injury was tendon and ligament injuries in track and field athletes who compete at the national level and 15.9% of sprinters and 19% of long-distance runners experienced stress fractures in college.1 Furthermore, 62.3% of national-level collegiate long-distance runners have been found to have anemia, and more than half of female national-level high school long-distance runners have amenorrhea.1 However, unfortunately, many of them answered that they have never received medical attention for them.1 Both athletes and coaches should be aware of these common injuries and illnesses and how to prevent and treat them. Such knowledge keeps athletes healthy and could enhance their performance levels.2 However, a Canadian study on soccer coaches found that only 29.8% used existing injury prevention programs.3 Furthermore, although it has been well-established that balance programs prevent injuries, less than 30% of coaches were found to include a balance program in their warm-up.4 Brown et al revealed that only 30% of coaches have heard of the female athlete triad (the triad) which is an interrelationship of low energy availability with or without disordered eating, menstrual irregularities or amenorrhea and low bone mineral density.5 Moreover, less than 25% of female adolescent non-athletes seek medical attention for secondary amenorrhea in Japan,6,7 and a previous study demonstrated that although 40% of the elite-level female track and field athletes had menstrual disorders including oligomenorrhea, none sought medical attention.8 This suggests that some athletes are not being diagnosed even if they have symptoms that require medical attention, including the triad, owing to a lack of medical knowledge in both the athletes and their coaches. Moreover, low estrogen pills are often used by female athletes to treat dysmenorrhea and delay menstruation to prevent its interference with competitive events. However, a survey in Japan found that many coaches object to their female athletes using low estrogen pills owing to potential weight gain.9,10 Yet, without sufficient medical knowledge, coaches’ decisions could risk endangering their athletes.
A good coach–athlete relationship is important for both parties because they spend a large amount of time together and often share values and feelings. Mottaghi and others have reported a significant positive relationship between the anxiety levels of athletes and their coaches.5,11–15 Although sports coaching is still male dominant, sex is an important factor in the coach–athlete relationships, and it has been conjectured that the lack of understanding on how to engage with female athletes exacerbates male dominance in sports.16 Thus, several studies have emphasized the need for more female sports coaches, although the numbers remain far from equal.17,18
To the best of our knowledge, there have been no previous studies on track and field coaches’ medical knowledge or awareness of problems affecting female athletes or of differences in this knowledge according to the coach's characteristics in Japan.
Thus, this study aimed to investigate the medical knowledge and awareness pertaining to female athletes among track and field coaches and their interactions with female athletes regarding medical problems. The objective of this study was also to determine the characteristics, including sex of the coaches with and without such knowledge and awareness.
Materials and Methods
This was a cross-sectional study in which an online anonymous survey was disseminated to track and field coaches in Japan via email, who were found through the mailing list of JAAF. A panel of experts, including the Chair of the Coaching Committee and the Chair of the Medical Committee of JAAF, reviewed the survey, which was revised based on the advice of the panel. The participants were the same as those in a previous study and the survey was distributed in spring of 2021.19
A total of 5241 track and field coaches with Japan Sport Association certification were invited to participate in the study. The distributed survey gathered demographic information from participants regarding their sex, affiliations, years of coaching, whether the coaches themselves were athletes and the level they had attained as an athlete if they were one, and their coaching environment including what event they coach and the sex of their athletes. Although the numbers were small, because there are few national events for elementary school athletes, we included those elementary school coaches too. The main part of the survey consisted of questions regarding respondents’ awareness of the triad and relative energy deficiency in sports (RED-S), their opinions on the use of low estrogen pills by female athletes, the gynecological medical attention received by the female athletes, and whether they had easy access to physicians able to address gynecological problems including team physicians. Answers were selected from a scale of set responses, with “Often” and “Sometimes” being considered as positive responses and “Rarely” and “Never” as negative responses.
Statistical Analysis
All data were analyzed using Stata 16.1 (Stata Corporation, TX, USA). A p-value <0.05 was considered statistically significant. Chi-squared tests were performed to investigate the differences between male and female coaches. Multivariate logistic regression was utilized to determine the independent variables and coaches’ backgrounds were included in the model. Odds ratios (OR) and associated 95% confidence intervals (CIs) were calculated to determine the strength of the model.
Results
A total of 412 coaches participated in the study (response rate 7.9%). Of the participants, 89.6% were males and 10.4% were females. Affiliations varied, but 57.8% of the coaches were affiliated with schools. We found that 71.4% of respondents had coached athletes on a national level and 93.5% used to be track and field athletes themselves. Moreover, 55.5% of the coaches trained athletes who had competed at a national or international level, and 91% coached both male and female athletes. Details of the participants are listed in Table 1.
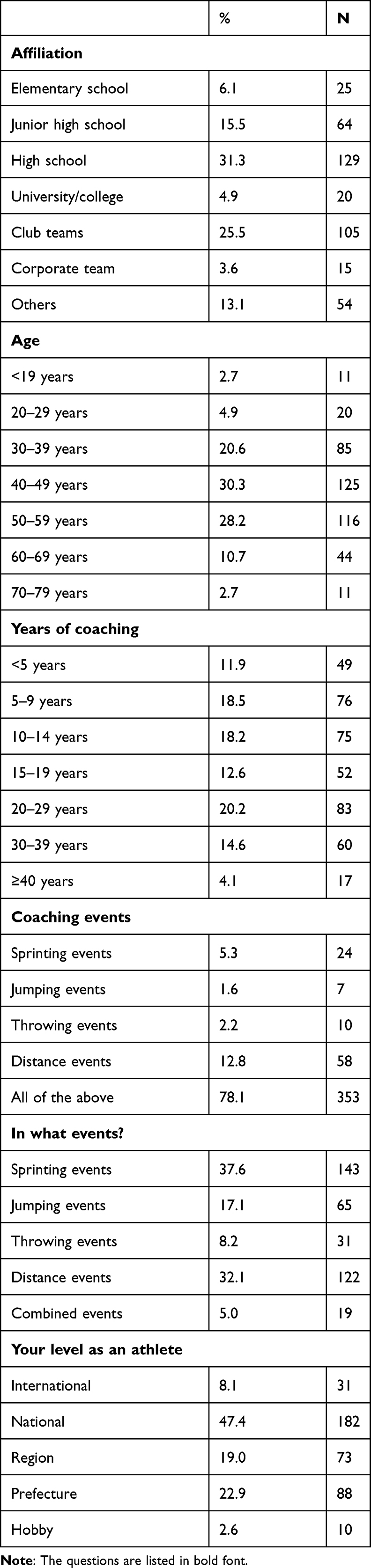 |
Table 1 Characteristics of the Participants |
Furthermore, 58.0% and 53.5% coaches were familiar with the triad and RED-S, respectively. In addition, 74.4% and 82% of female and male coaches, respectively, were not hesitant that their female athletes sought medical attention for gynecological problems, such as amenorrhea and dysmenorrhea. However, 32.6% and 16.8% female and male coaches, respectively, were reluctant for their female athletes to use low estrogen pills. The complete survey results are presented in Table 2 and chi-squared analysis revealed considerably more female than male coaches to be aware of the triad, to talk about problems regarding menses with athletes, and to have a physician able to discuss gynecological problems with female athletes including a team physician.
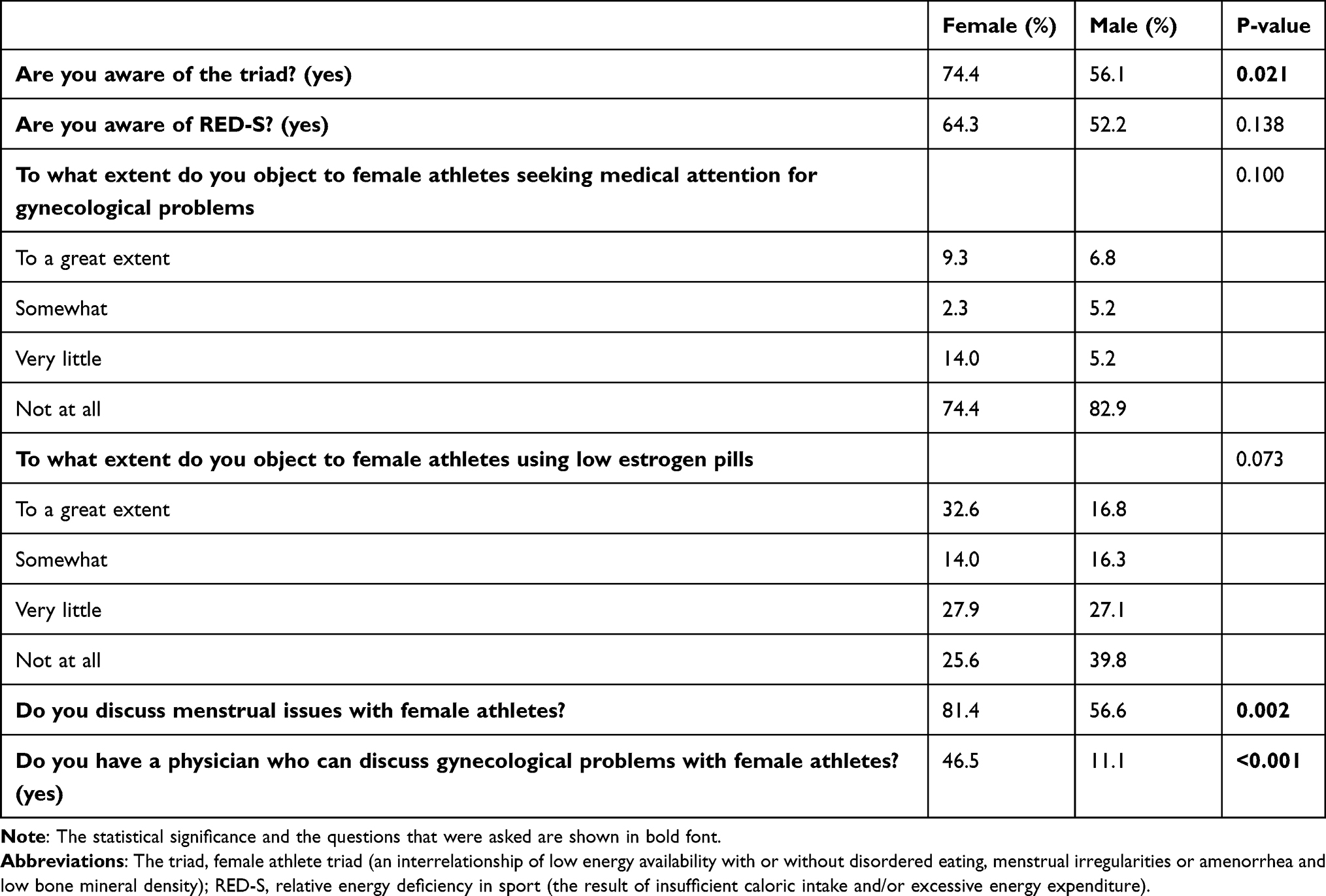 |
Table 2 Summary of Sex Differences in the Survey Responses of Sports Coaches |
The results of the logistic regression analysis for each of the main survey questions are described below and summarized in Table 3.
 |
Table 3 Results of the Logistic Regression Analysis (Statistically Significant Data Only) |
Awareness of the Triad
Significantly more female than male coaches were aware of the triad (OR, 3.59; p = 0.002). Considerably more coaches under the age of 30 years were aware of the triad than those aged 30 years and more. Coaches affiliated with high schools (OR, 2.30; p = 0.015), universities/colleges (OR, 9.02; p = 0.008), and club teams knew significantly more and those affiliated with elementary schools (OR, 0.31; p = 0.039) knew less compared to those affiliated with club teams. Those with less than 5 years of coaching experience were less likely to be aware of the triad than those with more than 5 years of coaching experience. Those who used to be a jumper had significantly lower awareness of the triad compared to those who used to be a sprinter (OR, 0.37; p = 0.004).
Awareness of RED-S
Neither the sex nor the age of coaches was related to their knowledge of RED-S. Coaches affiliated with a university/college (OR, 4.18; p = 0.042) were aware of RED-S than those affiliated with a club team. Significantly fewer number of coaches who used to compete in jumping (OR, 0.52; p = 0.045) and combined (OR, 0.33; p = 0.041) events were aware of RED-S than those who were former sprinters.
Opposed to Female Athletes Seeking Medical Attention for Gynecological Problems
Those with a coaching experience of 10–19 years and more than 30 years were significantly less opposed to athletes seeking medical attention for gynecological problems than those with less than 5 years of experience.
Opposed to Female Athletes’ Use of Low Estrogen Pills
Neither the sex nor the age of coaches was associated with their opposition to female athletes’ use of low estrogen pills. Coaches of high school athletes (OR, 0.45; p = 0.017) were less opposed than coaches of club teams. Also, compared to those with less than 5 years of coaching experience, those with 10–14 years (OR, 0.38; p = 0.028) and more than 30 years (OR, 0.32; p = 0.040) of coaching experience were less likely to be opposed to female athletes’ use of low estrogen pills.
Discussion of Menses with Female Athletes
Female coaches were significantly more likely than their male counterparts to talk about menses with their female athletes (OR, 5.07, p = 0.001). Coaches of high school (OR, 3.01; p = 0.003) and university/college teams (OR, 5.80; p = 0.031) were significantly more likely to talk about menses with their female athletes than coaches of club teams. Those with more than 10 years of coaching experience were significantly more likely to discuss menses with their female athletes than coaches with less than 5 years’ experience.
Access to a Physician (Including Having a Team Physician) Able to Address the Gynecological Problems of Female Athletes
Female coaches were significantly more likely than their male counterparts to have access to a physician able to address the gynecological problems of female athletes (OR, 9.22; p <0.001). Coaching at a university/college (OR, 8.28; p = 0.002) or for a corporate team (OR, 11.30; p = 0.001) was also positively related to the likelihood of having access to such a physician.
Discussion
In this study, we surveyed sports coaches to determine their medical knowledge, awareness and attitudes toward female athletes. A total of 412 coaches responded to our survey, 89.6% of whom were males. This reflects the sex imbalance among track and field coaches, both in Japan and internationally.20,21 Our participants were Japan Sport Association-certified sports instructors who had attended seminars on medical problems affecting female athletes. However, less than 60% of the coaches we surveyed were aware of the triad and RED-S. A previous study on American collegiate coaches found that 63.7% had heard of the triad, and 48.3% were able to identify the three components of the triad.22 Our results indicated that female coaches are considerably more aware of the triad than their male counterparts. This suggests that female coaches are generally more knowledgeable about medical problems that affect female athletes. Our regression analysis found a positive relationship between the female sex and knowledge of the triad. Since RED-S was defined later than the triad, awareness of the triad was higher than that of RED-S.23,24 Coaching high school and college teams was also positively related to knowledge of the triad. This may be because coaches affiliated with high schools and higher education institutions are more exposed to learning. Although, long-distance runners are more prone to encounter the triad than track and field athletes those coaches who were long-distance runners during their own athletic careers were no more likely to be aware of the triad than sprinters.25,26 This is problematic because although the respondents were mostly males (89.6%), we would still expect those who had previously been involved in an event where the triad is common to be more aware of the problem than other coaches.25,26 An age of 20–29 years was positively related to knowledge of the triad and RED-S, suggesting greater awareness among younger coaches. This is a positive sign for future coaching.
A total of 11.9% of coaches indicated that they were opposed to their female athletes seeking medical attention for gynecological problems “to a great extent” or “somewhat”. This is concerning because it could have significant detrimental effects on the health of female athletes. Moreover, 34.3% of coaches were opposed to their female athletes using low estrogen pills “to a great extent” or “somewhat”. Surprisingly, although there was only a small number of female coaches and there were no statistical differences between coach sexes, female coaches were considerably more opposed than their male counterparts to their female athletes using low estrogen pills. Low estrogen pills are often prescribed for dysmenorrhea which is prevalent among young females and in fact, Sundell et al reported that 67% of the women experienced dysmenorrhea at 24 years of age.27,28 It is speculated that coaches who object to low estrogen pills do so because of potential side effects such as nausea and weight gain due to water retention.29–31 Female athletes can also use low estrogen pills to manipulate their menstrual cycle so that it will not interfere with their games or training, which may be beneficial. Use of low estrogen pills is low in Japan compared with western countries possibly because of cultural differences and concerns about side effects.29–31 However, this is changing, and use of low estrogen pills among Japanese female athletes increased from 7% of those who participated in the 2012 London Olympics to 27% of those who participated in the 2016 Rio Olympics although this is still low compared with other countries.32,33 We also found a higher proportion of coaches with less than 5 years of coaching experience who objected to their athletes seeking gynecological medical attention and using low estrogen pills than the proportion of more experienced coaches. Thus, these also reflect the fact that the coaches gain knowledge by coaching experiences.
Because the prevalence of dysmenorrhea is high in young females, coaches should know that advising young female athletes not to take low estrogen pills or other medications for its treatment is unethical. Although fear of the possible side effects is understandable; it is important to be aware that their incidence differs between individuals and coaches should not interfere with an athlete’s medical decisions or the advice of medical professionals without sufficient knowledge.30–34
Significantly more female coaches (81.4%) than male coaches (56.6%) discussed about menses with female athletes. This possibly arises from the taboo against bringing up this topic with men, which makes it harder for male coaches.35–37 Coaching at high schools and colleges was positively related to discussing menses with female athletes. This may be because these coaches spend time with the athletes outside of training because the majority of coaches in Japanese schools are faculty members.38 Less experience in coaching was negatively related to menses discussion. We speculate that more recently qualified coaches may be reluctant to bring up the topic until they have built relationships with their athletes. Female coaches were significantly more likely than male coaches to have a physician with whom female athletes could discuss gynecological problems, and female sex showed a positive correlation with this in logistic regression analysis. This is possibly because female coaches have more easy access to gynecologists or feel more comfortable than their male counterparts discussing gynecological problems with their team physician if they have one. This is important for the health of female athletes.
This study had several limitations that should be noted. Because we did not test to the respondents’ knowledge of what exactly the triad and RED-S are, it is possible that some coaches who claimed to know about these did not. Because the survey was sent to officially licensed coaches, our respondents would have received some education on relevant subjects, making them more knowledgeable than coaches who are not officially licensed and there could have been a selection bias. Thus, future studies should focus on coaches at different professional levels, including those who are not officially licensed as those who are not officially licensed may not have much knowledge because they have not taken the lectural courses required to be licensed. In addition, the majority of our survey respondents were males, reflecting the high sex imbalance in this profession in Japan and future studies with more female coaches are essential. Unfortunately, most aspects of sports and roles associated with it are male-dominated, both in Japan and internationally and future studies should endeavor to include a broader demographic of coaches and should expand the survey outside of Japan.39 In addition to the existence of a pay gap and fewer female events in the Olympics,40,41 the lack of female coaches in most sports is a global problem. In this study, although it turned out that female coaches were more aware of medical issues related to female athletes compared to male counterparts, the percentage of female coaches was only 10.4%. Thus, it is possible that many female athletes may not be getting medical attention because of the lack of coaches’ knowledge and awareness of medical problems related to female athletes. In order to promote sex equality in sports, it is important for both male and female coaches to have knowledge and awareness regarding medical problems related to female athletes and have to have more female coaches in the field to support female athletes. Thus, educating coaches by providing the opportunity to attend courses to obtain such knowledge is essential.
Conclusions
In this study, we found that more female than male coaches are aware of the triad, talk about menses with their female athletes, and have access to a physician who can address gynecological problems. Having access to a physician, including a team physician, who can discuss gynecological problems with coaches and athletes is vital to the health and wellbeing of female athletes. While the necessity and importance of female coaches have been demonstrated in research dating back to 2009, sex imbalance remains and only 10.4% of the respondents in this study were female coaches. Our survey results also indicated that many coaches are not comfortable with their athletes seeking medical attention for gynecological problems or using low estrogen pills. It is apparent that coaches could benefit from more training and education to ensure they are fully equipped with the medical knowledge needed to support their athletes.
Abbreviations
OR, Odds ratios; CIs, associated 95% confidence intervals; JAAF, the Japan Association of Athletics Federations; the triad, female athlete triad; RED-S, relative energy deficiency in sports.
Ethics Statement
The study was approved by the Ethics Review Procedures Concerning Research with Human Subjects Group of the authors’ affiliated institutions (approval number, 20190170). Signed statements of informed consent to participation and publication were obtained from the participants before the study.
Acknowledgments
The authors thank all the coaches who answered the survey.
Funding
This work was supported by JKA and its promotion funds from KEIRIN RACE. Article processing charge was funded by JSPS KAKENHI Number 21K17571.
Disclosure
The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.
References
1. Japan Association of Athletics Federations. Surveillance of injuries and illnesses of Collegiate athletes. “On the internet”. Available from: https://www.jaaf.or.jp/files/upload/202005/16_125001.pdf.
2. Hamer J, Desbrow B, Irwin C. A review exploring coach knowledge, attitudes/beliefs and behaviours towards low energy availability in athletes. Int J Sports Sci Coach. 2022;2022:17479541221140188.
3. Mawson R, Creech MJ, Peterson DC, Farrokhyar F, Ayeni OR. Lower limb injury prevention programs in youth soccer: a survey of coach knowledge, usage, and barriers. J Exp Orthop. 2018;5(1):43. doi:10.1186/s40634-018-0160-6
4. Räisänen AM, Owoeye OBA, Befus K, van den Berg C, Pasanen K, Emery CA. Warm-ups and coaches’ perceptions: searching for clues to improve injury prevention in youth basketball. Front Sports Act Living. 2021;3:619291. doi:10.3389/fspor.2021.619291
5. Brown KN, Wengreen HJ, Beals KA. Knowledge of the female athlete triad, and prevalence of triad risk factors among female high school athletes and their coaches. J Pediatr Adolesc Gynecol. 2014;27(5):278–282. doi:10.1016/j.jpag.2013.11.014
6. Tosi M, Maslyanskaya S, Dodson NA, Coupey SM. The female athlete triad: a comparison of knowledge and risk in adolescent and young adult figure skaters, dancers, and runners. J Pediatr Adolesc Gynecol. 2019;32(2):165–169. doi:10.1016/j.jpag.2018.10.007
7. Tsujioka M, Gemba M, Ono K, Saito I, Shimoyama C. Secondary amenorrhea in high school girls. Bull Keio Univ Health Center. 2003;21(1):27–31. Article in Japanese.
8. Tsukahara Y, Torii S, Yamasawa F, et al. Bone parameters of elite athletes with oligomenorrhea and prevalence seeking medical attention: a cross-sectional study. J Bone Miner Metab. 2021;39:1009–1018. doi:10.1007/s00774-021-01234-1
9. Lopez LM, Ramesh S, Chen M, et al. Progestin-only contraceptives: effects on weight. Cochrane Database Syst Rev. 2016;2016(8):Cd008815. doi:10.1002/14651858.CD008815.pub4
10. Fujii T, Osuga Y, Obayashi S, et al. Survey on menstrual disorders in athletes and coaches. J Obstet Gynaecol Res. 2016;68(4):38–47.
11. Wrisberg CA. Quality of life for male and female athletes. Quest. 1996;48(3):392–408. doi:10.1080/00336297.1996.10484205
12. Mottaghi M, Atarodi A, Rohani Z. The relationship between coaches’ and athletes’ competitive anxiety, and their performance. Iran J Psychiatry Behav Sci. 2013;7(2):68–76.
13. Verschueren K. Attachment, self-esteem, and socio-emotional adjustment: there is more than just the mother. Attach Hum Dev. 2020;22(1):105–109. doi:10.1080/14616734.2019.1589066
14. Peng J, Zhang J, Zhao L, Fang P, Shao Y. Coach-athlete attachment and the subjective well-being of athletes: a multiple-mediation model analysis. Int J Environ Res Public Health. 2020;17(13):4675. doi:10.3390/ijerph17134675
15. Ramis Y, Torregrosa M, Viladrich C, Cruz J. The effect of coaches’ controlling style on the competitive anxiety of young athletes. Front Psychol. 2017;8:572. doi:10.3389/fpsyg.2017.00572
16. Norman L. The coaching needs of high performance female athletes within the coach-athlete Dyad. Int Sport Coach J. 2015;2(1):15. doi:10.1123/iscj.2013-0037
17. Greenhill J, Auld C, Cuskelly G, Hooper S. The impact of organisational factors on career pathways for female coaches. Sport Manage Rev. 2009;12(4):229–240. doi:10.1016/j.smr.2009.03.002
18. Ladda S. Where are the female coaches? J Phys Educ Recreation Dance. 2015;86(4):3–4. doi:10.1080/07303084.2015.1009804
19. Tsukahara Y, Kamada H, Torii S, et al. Controlling behavior, sex bias and coaching success in Japanese track and field. Sports. 2023;11(2):32. doi:10.3390/sports11020032
20. Norman L, Rankin-Wright A. Surviving rather than thriving: understanding the experiences of women coaches using a theory of gendered social well-being. Int Rev Sociol Sport. 2018;53(4):424–450. doi:10.1177/1012690216660283
21. Kubayi A, Coopoo Y, Morris-Eyton H. Work-related constraints in sports coaching: perceptions of South African female coaches. Int J Sports Sci Coach. 2017;12(1):103–108. doi:10.1177/1747954116684391
22. Pantano KJ. Current knowledge, perceptions, and interventions used by collegiate coaches in the u.s. Regarding the prevention and treatment of the female athlete triad. N Am J Sports Phys Ther. 2006;1(4):195–207.
23. Matzkin E, Curry EJ, Whitlock K. Female athlete triad: past, present, and future. J Am Acad Orthop Surg. 2015;23(7):424–432. doi:10.5435/JAAOS-D-14-00168
24. Mountjoy M, Sundgot-Borgen J, Burke L, et al. The IOC consensus statement: beyond the female athlete triad--relative energy deficiency in sport (RED-S). Br J Sports Med. 2014;48(7):491–497. doi:10.1136/bjsports-2014-093502
25. Mudd LM, Fornetti W, Pivarnik JM. Bone mineral density in collegiate female athletes: comparisons among sports. J Athl Train. 2007;42(3):403–408.
26. Rauh MJ, Barrack M, Nichols JF. Associations between the female athlete triad and injury among high school runners. Int J Sports Phys Ther. 2014;9(7):948–958.
27. Sundell G, Milsom I, Andersch B. Factors influencing the prevalence and severity of dysmenorrhoea in young women. Br J Obstet Gynaecol. 1990;97(7):588–594. doi:10.1111/j.1471-0528.1990.tb02545.x
28. Ju H, Jones M, Mishra G. The prevalence and risk factors of dysmenorrhea. Epidemiol Rev. 2014;36:104–113. doi:10.1093/epirev/mxt009
29. Cea-Soriano L, García Rodríguez LA, Machlitt A, Wallander MA. Use of prescription contraceptive methods in the UK general population: a primary care study. Bjog. 2014;121(1):53–60;discussion–1−. doi:10.1111/1471-0528.12465
30. Martin D, Sale C, Cooper SB, Elliott-Sale KJ. Period prevalence and perceived side effects of hormonal contraceptive use and the menstrual cycle in elite athletes. Int J Sports Physiol Perform. 2018;13(7):926–932. doi:10.1123/ijspp.2017-0330
31. Yoshida H, Sakamoto H, Leslie A, Takahashi O, Tsuboi S, Kitamura K. Contraception in Japan: current trends. Contraception. 2016;93(6):475–477. doi:10.1016/j.contraception.2016.02.006
32. Rechichi C, Dawson B, Goodman C. Athletic performance and the oral contraceptive. Int J Sports Physiol Perform. 2009;4(2):151–162. doi:10.1123/ijspp.4.2.151
33. Nose S, Dohi M, Namba A. Rate of low-dose estrogen progestin (LEP) use in elite Japanese female athletes and issues concerning LEP use. Japan J Clin Sports. 2014;22:122–127. Article in Japanese.
34. Parker MA, Sneddon AE, Arbon P. The menstrual disorder of teenagers (MDOT) study: determining typical menstrual patterns and menstrual disturbance in a large population-based study of Australian teenagers. Bjog. 2010;117(2):185–192. doi:10.1111/j.1471-0528.2009.02407.x
35. McKeever P. The perpetuation of menstrual shame: implications and directions. Women Health. 1984;9(4):33–47. doi:10.1300/J013v09n04_04
36. Stubbs ML. Cultural perceptions and practices around menarche and adolescent menstruation in the United States. Ann N Y Acad Sci. 2008;1135:58–66. doi:10.1196/annals.1429.008
37. Whisnant L, Zegans L. A study of attitudes toward menarche in white middle-class American adolescent girls. Am J Psychiatry. 1975;132(8):809–814.
38. Agency JS. General guideline regarding sports club activities. “On the internet”. Available from: https://www.mext.go.jp/sports/b_menu/shingi/013_index/toushin/__icsFiles/afieldfile/2018/03/19/1402624_1.pdf.
39. World Economic Forum. Global gender gap report 2022. “On the internet”. Available from: https://www.weforum.org/reports/global-gender-gap-report-2022/.
40. Archer A, Prange M. ‘Equal play, equal pay’: moral grounds for equal pay in football. J Philosophy Sport. 2019;46(3):416–436. doi:10.1080/00948705.2019.1622125
41. World Athletics. Olympic game 2021: “On the internet”. Available from: https://worldathletics.org/competitions/olympic-games/the-xxxii-olympic-games-athletics-7132391/timetable/bydiscipline.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.