")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Autoimmune Glial Fibrillary Acidic Protein Astrocytopathy: To Identify Its Diagnosis, Management and Prognosis (GFAP-AID) Registry: Study Protocol for an Ambispective, Multicenter Registry in China
Authors Yang J , Jiang L, Yao H, Huang L, Long Y
Received 28 February 2022
Accepted for publication 6 May 2022
Published 1 June 2022 Volume 2022:18 Pages 1099—1105
DOI https://doi.org/10.2147/NDT.S364246
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Jie Yang,1,2 Lihong Jiang,1,2 Haiyan Yao,1,2 Li Huang,1,2 Youming Long1,2
1Department of Neurology, The Second Affiliated Hospital of GuangZhou Medical University, Guangzhou, Guangdong Province, People’s Republic of China; 2Key Laboratory of Neurogenetics and Channelopathies of Guangdong Province and The Ministry of Education of China, Institute of Neuroscience and the Second Affiliated Hospital of GuangZhou Medical University, Guangzhou, Guangdong Province, People’s Republic of China
Correspondence: Youming Long, Tel/Fax +86-20-34153147, Email [email protected]
Purpose: Currently, no uniform diagnostic criteria or treatment consensus is available for patients with autoimmune glial fibrillary acidic protein astrocytopathy (GFAP-A). The aim of this registry is to develop diagnostic and therapeutic recommendations for GFAP-A based on clinical features, neuroimaging, neuroelectrophysiological examinations, laboratory tests, specific antibody tests, immunotherapy, and prognosis.
Patients and methods: This multicenter, nationwide ambispective registry includes twenty-seven hospitals in China. From January 2020 to December 2022, consecutive hospitalized patients with symptoms of meningoencephalitis, as well as GFAP-IgG positive cerebrospinal fluid (CSF) or serum will be invited to join this study. It is conservatively estimated that over 300 patients will join the study. Data on demographics, medical history, treatment details and imaging features will be collected after discharge. Outcome events of interest will include modified Rankin Scale (mRS) and Expanded Disability Status Scale (EDSS), readmission with relapsed meningoencephalomyelitis, all-cause mortality, and mortality resulting from complications of GFAP-A. The follow-up will be conducted at six months and twelve months after discharge. Univariate and multivariate regression models will be used to calculate identify independent predictors of outcomes. Stratification analysis will be used to test whether results are similar between key subgroups.
Discussion: This study will describe the risk factors, disease course, response to immunotherapy, and long-term prognosis of a large cohort of GFAP-A patients. By using these data, a relatively rational recommendation process for the diagnosis and treatment of GFAP-A will be developed.
Trial Registration Number: ChiCTR2000041291.
Keywords: glial fibrillary acidic protein, astrocytopathy, antibody, diagnosis, prognosis
Introduction
In 2016, a new form of meningoencephalitis known as autoimmune glial fibrillary acidic protein (GFAP) astrocytopathy (GFAP-A) was described.1 Additional cases were subsequently confirmed internationally.2 GFAP-A is a form of meningoencephalomyelitis or limited meningoencephalomyelitis associated with binding of IgG to GFAP.3 The disease is characterized by meningitis, encephalitis, and myelitis symptoms as well as vision abnormalities.2,4 Predominance of CD8+ T cells may be an important pathological and diagnostic feature of this disease.5
Currently, no uniform diagnostic criteria are available for GFAP astrocytic lesions; additionally, coexisting neuroautoantibodies have been detected in some patients, making diagnosis difficult.6 Standard treatment protocols have not yet been developed. Although some patients are prone to relapse or even death, most patients with GFAP-A respond well to steroid treatment. Lack of response to corticosteroid should prompt evaluation for co-morbid malignancies.7 Notably, 38% of patients with GFAP-A are diagnosed with a tumor within 3 years of onset of neurological symptoms.1
Research related to GFAP-A has gradually received more attention, but most previous studies have had relatively small sample sizes,2,4,8 retrospective designs,4 or short follow-up periods.9 Thus, there is a lack of data in support of evidence-based medical decision-making to enable early diagnosis, effective treatment, and long-term prognostic assessment of the disease.
In this study, we will use an ambispective, multicenter design to recruit approximately 300 patients with GFAP-A, and analyze clinical data, magnetic resonance imaging (MRI) features, CSF examinations, and outcome events. These data will provide additional insight into the diagnosis, treatment, and prognosis of GFAP-A.
Methods
Study Design
This is a multicenter, nationwide, ambispective, observational, open-cohort study. The study was launched in January 2020 and will end in December 2022, with enrollment to be completed by December 2021. Follow-up will be conducted until December 2022. Between November 2020 and December 2021, patients were prospectively selected for observation from the Second Affiliated Hospital of Guangzhou Medical University, and other twenty-six tertiary hospitals in China. (See details in Acknowledgments). In total, about 300 patients are expected to be included in the study. After providing written informed consent, patients will be required to complete baseline data collection as specified in the study protocol. For the retrospective study, researchers will recruit patients from January 2020 to October 2020, and all enrolled patients must meet the inclusion criteria.
Inclusion Criteria
- Patients with a potential diagnosis of autoimmune encephalitis, central nervous demyelinating disease, or other autoimmune diseases of the central nervous system at screening.
- Positive detection of GFAP antibodies in CSF or serum.
- Ability to understand and comply with the research protocol.
- Written informed consent by the patient or the patient’s legally authorized representative after reviewing information about the study.
Exclusion Criteria
- Patients with a contraindication for lumbar puncture.
- Patients participating in other clinical trials.
- Patients who are unwilling or unable to provide informed consent for the study.
Outcome Measurement
Primary Outcome
The primary outcome in this study is the development of diagnostic and therapeutic recommendations for GFAP-A based on clinical features, neuroimaging, neuroelectrophysiological examinations, laboratory tests, specific antibody tests, immunotherapy, and prognosis.
Secondary Outcomes
- Rates of disability, modified Rankin Score (mRS), and expanded disability status scale 6 months and 1 year after symptom onset.
- Relapses, defined as hospital readmission for meningoencephalomyelitis.
- Newly diagnosed tumors confirmed by a specialist’s certificate of diagnosis based on pathology and/or imaging data.
- Mortality: all-cause mortality and mortality associated with the complications of GFAP-A.
Data Collection
To address these objectives, we meticulously designed a case report form (CRF) to collect the necessary information. The CRF consists of nine parts, as described below (Table 1).
- Demographic information and disease history: age, sex, length of hospital stays, familial disease history, concomitant diseases.
- Clinical features: history of precursor infections and information on causative pathogens, onset characteristics, clinical manifestations (eg, fever, headache, encephalopathy, involuntary movement, myelitis, abnormal vision, ataxia, mental disorder, epilepsy, and abnormal autonomic nervous function) and other symptoms and signs of meningoencephalomyelitis.
- Laboratory tests: blood tests (routine blood tests, biochemical investigations, tumor marker evaluations, thyroid function markers, and rheumatic disease markers) and spinal fluids tests (biochemical, cytologic, and bacteriologic analyses).
- GFAP antibody screening tests: detection of GFAP antibody in CSF or serum by indirect immunofluorescence assay. Patients will be divided into two cohorts.Cohort A include patients who was retrospectively recruited from January 2020 to October 2020 in the Second Affiliated Hospital of Guangzhou Medical University in whom GFAP IgG is detected by indirect immunofluorescence assay using rat/mouse brain samples and using an in-house cell-based assay (CBA) as described previously.2Cohort B include patients who was prospectively recruited from November 2020 to December 2021 from all twenty-seven centers. They are tested for GFAP-IgG using a tissue-based assay as well as a CBA by a commercial diagnostics company (Guangzhou KingMed Diagnostics Group Co., Ltd.), which is similar as previously published method, including our own center2 and other center.4For the tissue-based IFA, antibody detection was performed with an indirect immunofluorescence assay using standard rat cerebellar tissues. Briefly, serum (1: 50) or CSF (1: 1) samples were allowed to react with these tissue sections on glass slides for 3 hours at room temperature. The slides were then rinsed twice with phosphate-buffer saline (PBS) before being incubated with fluorescein-conjugated goat anti-human IgG for 1 hours. Finally, the slides were rinsed with PBS and the fluorescence pattern was examined under a microscope. For CBA, HEK293T cells were transfected with a human targeting GFAPαcDNA plasmid. At 36h after transfection, HEK293T cells were fixed with 4% paraformaldehyde. Cells were incubated with serum (1:10) or CSF (1:1) from patient for 1 h at room temperature, and then incubated for 1 h with CY3 conjugated goat anti-human IgG. Images were taken using a fluorescence microscope.
- Antibody screening tests. An indirect immunofluorescence assay or a cell-based assay will be used to assess the presence of GFAP-IgG in both serum and CSF for each patient. Furthermore, antibodies to Hu, Yo, Ri, CRMP5, amphiphysin, Ma2, NMDAR, AMPA1, AMPA2, CASPR2, LGI1, GABA receptor, and GAD65 will be detected.
- Pathological examinations. Patients with challenging differential diagnosis will undergo brain biopsy to detect whether there is an inflammatory reaction dominated by CD8 + T cells near neurons and astrocytes.
- Auxiliary examinations. Plain and enhanced MRI scans of the brain and spine, as well as positron emission tomography/computed tomography examinations, will be performed when necessary. Lesion location and number will be recorded. Neuroelectrophysiological examinations including electroencephalograms and evoked potentials will be performed as routine examinations. B-ultrasound examinations of abdominal organs will be performed for all patients and examinations of pelvic organs will be performed for female patients.
- Immunomodulatory therapy options will be recorded, including intravenous methylprednisolone, intravenous immunoglobulin, plasma exchange, immunoadsorption, oral corticosteroids, and immunosuppressive medications.
- Outcomes. Post-discharge follow-up will be performed by trained investigators at the outpatient clinic at 6 months and 12 months after discharge. The follow-up period will end in December 2022. During the follow-up period, patients will undergo physical examinations and laboratory tests. Brain and spinal MRI scans will be conducted for selected patients. Laboratory tests will include routine blood examinations and blood biochemistry. Outcome events of interest will include mRS and EDSS, readmission with relapsed meningoencephalomyelitis, all-cause mortality, and mortality resulting from complications of GFAP-A. Patients who cannot be visited at follow-up time points will be connected by telephone.
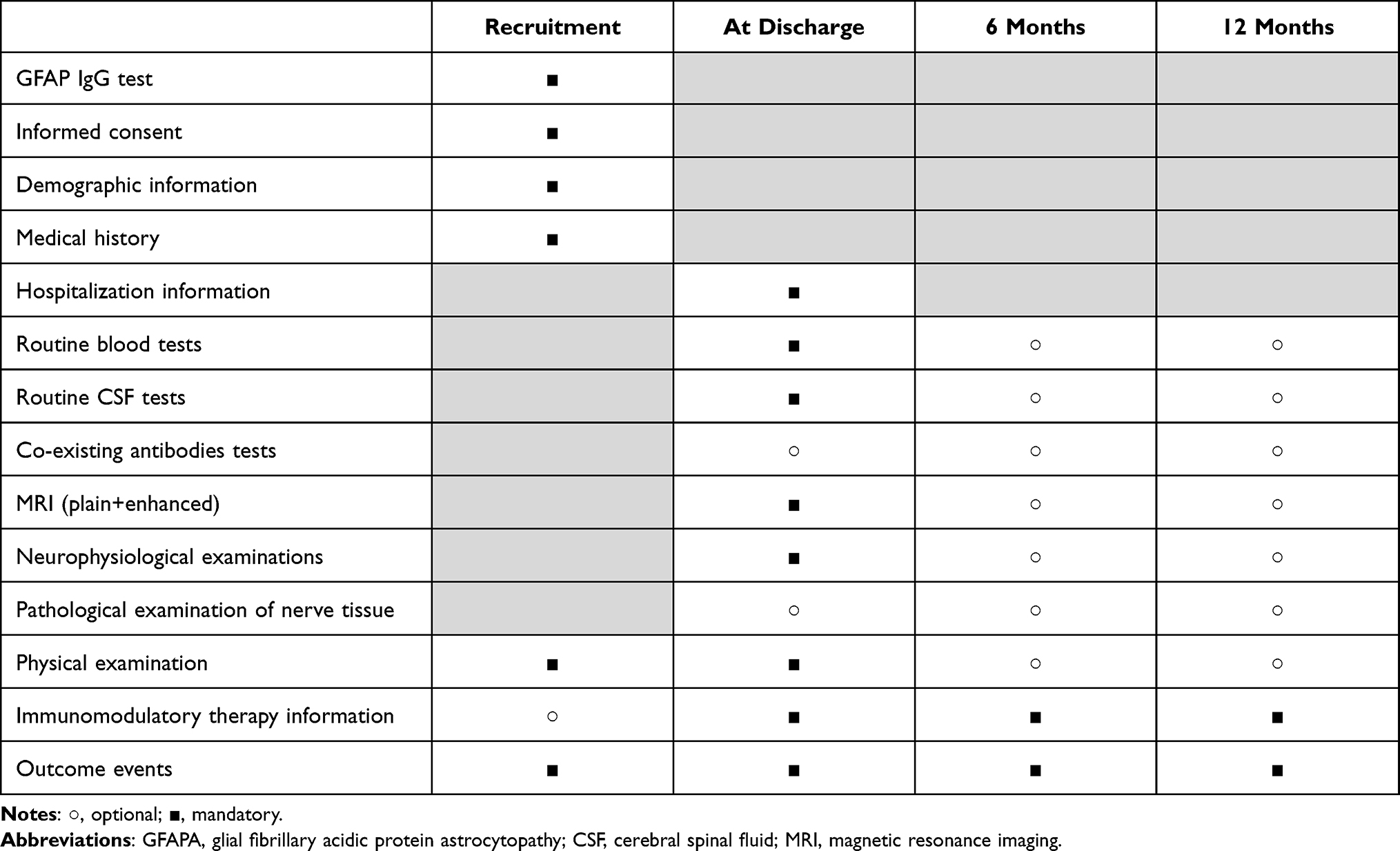 |
Table 1 Checklist for the Collection of Necessary Clinical Data and Follow-Up Scheme of Enrolled Patients with GFAP-A |
Research Supervision Committee
The supervisory committee will consist of a team responsible for data management and data checks as well as a methodological team. All committee members will have clearly divided roles and responsibilities and good cooperation. Each part of this study will have a standard operating procedure to ensure homogeneity of the study. Furthermore, dedicated staff will be assigned for data collection, data entry, data checking, data cleaning, and follow up. When analyzing multiple timepoint data after study entry, quality check results and data modification traces will be recorded in the online electronic data capture system (www.medresman.org). The supervisory committee requires an annual report on the progress of the study.
Statistical Analysis
SPSS 21.0 (IBM Corp., Armonk, NY, USA), R statistical software (http://www.R-project.org, The R Foundation), and Free Statistics software version 1.4 will be used for statistical analysis. Quantitative variables will be described as means ± standard deviations or medians (interquartile ranges). Categorical variables will be described as frequencies (N) and percentages (%); differences between categorical variables will be assessed using χ2 or Fisher’s exact tests. Ranked data will be expressed as frequencies and percentages; differences between ranked variables will be assessed using the Kruskal–Wallis H-test. The Kaplan-Meier method will be used to prepare survival curves. For the multivariable analysis, missing values will be imputed using multiple imputation. Univariate and multivariate regression models will be used to calculate identify independent predictors of outcomes. Stratification analysis will be used to test whether results are similar between key subgroups. All statistical tests will be two-sided, and values of P < 0.05 will be considered statistically significant.
Determination of Sample Size
Given that GFAP-A is a new form of encephalitis that was first described only 5 years ago, there are no definitive epidemiological data available at this time. Thus, this exploratory observational study will attempt to provide initial epidemiological data. We therefore propose a reasonable estimate of an appropriate sample size based on the number of GFAP-positive patients in our center and other subcenters over the past 2 years (approximately 300 patients recruited within 3 years). To our knowledge, this is the largest sample size for a study of GFAP-A to date.
Dissemination of Results
Dissemination in professional peer-reviewed journals is expected to begin in 2023 to promote awareness of GFAP disease diagnosis and treatment.
All personal data, such as name and gender, will be replaced by statistical codes or numbers during and after the study and will be kept strictly confidential. All clinical data will be analyzed anonymously through the CRF and EDC systems to protect patient privacy. Articles published on the basis of the data in this registry will not disclose any personal information.
Strengths and Limitations
- This will be the largest study of GFAP-A to date.
- The first study to propose recommendations for diagnosis and treatment of GFAP-A based on a clinical registry.
- This will be a multi-center ambispective study that minimizes the enrollment biases of single-center studies and the lack of data of retrospective studies.
- This registry focuses on Chinese patients with GFAP-A and the results should be cautiously generalized to other ethnic groups. A more scientific interpretation of the findings needs to be combined with future studies of other races of the same type like the current one.
- This will be an observational and partially retrospective study, there may be limitations related to inadequate data recording. However, because of the low incidence of the disease, this reasonable measure is necessary to include more cases.
Abbreviations
GAP-A, autoimmune glial fibrillary acidic protein astrocytopathy; CSF, cerebrospinal fluid; MRI, magnetic resonance imaging; mRS, modified Rankin Score; CRF, case report form; CBA, cell-based assay; CRMP5, collapsin response mediator protein 5; NMDAR, N-methyl-D-aspartate receptor; AMPA, alpha-amino-3- hydroxy-5-methyl-4 isoxazolepropionic acid; CASPR2, contactin-associated protein-like 2; LGI1, leucine-rich glioma-inactivated 1, GABA, gamma- aminobutyric acid; GAD65, The 65-KD isoform of glutamic acid decarboxylase.
Data Sharing Statement
We will transfer the CRFs to the EDC (www.medresman.org), which will be stored in a hard disk and cloud system. The data are available from the corresponding author upon reasonable request. Detailed results will be openly shared after study completion.
Ethics Approval and Consent to Participate
The study protocol (2020-hs-54) was approved by the Ethics Committee of the Second Affiliated Hospital of Guangzhou Medical University (Guangzhou, China). The study was designed as an ambispective, observational registry and all information will be collected after discharge. Clinical practice will therefore not be affected by the study. Patients diagnosed with GFAP-A before November 2020 will be contacted by telephone to obtain verbal consent. We will obtain written informed consent from patients diagnosed with GFAP-A after November 1, 2020. The study will be performed in accordance with the principles laid out in the Declaration of Helsinki. The latest protocol version is version 1.0 in Nov 2020.
Acknowledgments
Twenty-seven tertiary hospitals in China are participating in this study. We would like to thank the investigators from the collaborating centers: Aiqun Liu (the First Affiliated Hospital of Guangdong Pharmaceutical University), Daishi Tian (Tongji Hospital), Ying Fu (the First Affiliated Hospital of Fujian Medical University), Sheng Chen (Ruijin Hospital), Cunjin Zhang (Nanjing Drum Tower Hospital), Yulan Tang (the First Affiliated Hospital of Guangxi Medical University), Jun Guo (Tangdu Hospital), Weian Chen (the First Affiliated Hospital of Wenzhou Medical University), Han Lin (Dongguan Houjie Hospital), Ding Liu (the Third Xiangya Hospital of Central South University), Suhua Yao (Dali People’s Hospital), Wei Qiu (the Third Affiliated Hospital of Sun Yat-sen University), Xiuling Wu (Tangshan Workers Hospital), Huan Yang (XiangYa Hospital of Central South University), Chunmei Duan (the Second Affiliated Hospital of Army Medical University), Lizhu Wu (the Central Hospital of Jiangmen), Huiyu Feng (the First Affiliated Hospital of Sun Yat-sen University), Xiaoqiong Yan (Hubei Province Hospital of the Integrated Chinese and Western Medicine), Hongli Liu (Qinhuangdao First Hospital), Qianhui Xv (Shenzhen People’s Hospital), Jinlong Ye (Guang Dong 999 Brain Hospital), Yong You (the Second Affiliated Hospital of Hainan Medical University), Xiao Yang (General Hospital of Ningxia Medical University), Haiyang Wang (Jining NO.1 People’s Hospital), Tengfei Ou (Foshan Second People’s Hospital) and Bo Wang (the First People’s Hospital of Bijie).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project is supported by the following two funding: 1. The Research Project on New Technologies and New Business Applications of the Second Affiliated Hospital of Guangzhou Medical University (2020-10); 2. The National Natural Science Foundation of China (81771302). The funder had no influence in the design of this trial nor in the writing of manuscript and presenting the study outcomes, and also have no role in collection, analysis and interpretation of data.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fang B, McKeon A, Hinson SR, et al. Autoimmune glial fibrillary acidic protein astrocytopathy: a novel meningoencephalomyelitis. JAMA Neurol. 2016;73(11):1297–1307. doi:10.1001/jamaneurol.2016.2549
2. Long Y, Liang J, Xu H, et al. Autoimmune glial fibrillary acidic protein astrocytopathy in Chinese patients: a retrospective study. Eur J Neurol. 2018;25(3):477–483. doi:10.1111/ene.13531
3. Shan F, Long Y, Qiu W. Autoimmune glial fibrillary acidic protein astrocytopathy: a review of the literature. Front Immunol. 2018;9:2802. doi:10.3389/fimmu.2018.02802
4. Flanagan EP, Hinson SR, Lennon VA, et al. Glial fibrillary acidic protein immunoglobulin G as biomarker of autoimmune astrocytopathy: analysis of 102 patients. Ann Neurol. 2017;81(2):298–309. doi:10.1002/ana.24881
5. Yuan ZM, Li HL, Huang L, et al. CD8(+) T-cell predominance in autoimmune glial fibrillary acidic protein astrocytopathy. Eur J Neurol. 2021;28(6):2121–2125. doi:10.1111/ene.14778
6. Yang XG, Xu HM, Ding ML, et al. Overlapping autoimmune syndromes in patients with glial fibrillary acidic protein antibodies. Front Neurol. 2018;9. doi:10.3389/fneur.2018.00251
7. Dubey D, Hinso SR, Jolliffe EA, et al. Autoimmune GFAP astrocytopathy: prospective evaluation of 90 patients in 1 year. J Neuroimmunol. 2018;321:157–163. doi:10.1016/j.jneuroim.2018.04.016
8. Iorio R, Damato V, Evoli A, et al. Clinical and immunological characteristics of the spectrum of GFAP autoimmunity: a case series of 22 patients. J Neurol Neurosur Ps. 2018;89(2):138–146. doi:10.1136/jnnp-2017-316583
9. Yang XG, Liang JY, Huang QM, et al. Treatment of autoimmune glial fibrillary acidic protein astrocytopathy: follow-up in 7 cases. Neuroimmunomodulat. 2017;24(2):113–119. doi:10.1159/000479948
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.