")
Back to Journals » International Journal of General Medicine » Volume 13
Atypical Proximal Cervical Spondylotic Amyotrophy: Case Report Demonstrating Clinical/Imaging Discrepancy
Authors Feng S, Fan Z, Yang Y, Fei Q , Li X
Received 24 October 2020
Accepted for publication 12 November 2020
Published 2 December 2020 Volume 2020:13 Pages 1367—1372
DOI https://doi.org/10.2147/IJGM.S288588
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Shitong Feng,* Zihan Fan,* Yong Yang, Qi Fei, Xiang Li
Department of Orthopaedics, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiang Li; Yong Yang
Department of Orthopaedics, Beijing Friendship Hospital, Capital Medical University, Beijing 100050, People’s Republic of China
Tel +86-10-63138353; +86-13641225060
Fax +86-10-83911029
Email [email protected]; [email protected]
Purpose: The aim of this study was to present a novel case of unilateral proximal cervical spondylotic amyotrophy (CSA) with contralateral spinal cord compression, which is subject to misdiagnosis and missed diagnosis.
Background: CSA is the rare form of cervical spondylosis, which is characterized by severe muscle atrophy in the upper extremities. It can be classified in the proximal subtype and the distal subtype. The etiology, pathophysiology and treatment of CSA are still controversial.
Methods: A rare case of atypical proximal CSA, who presented with left shoulder and arm weakness, but cervical magnetic resonance imaging (MRI) showed large right paracentral disc herniation in the C4-5 level. Twelve weeks after undergoing anterior cervical discectomy and fusion technique in C4-5 level, the patient’s symptoms obviously recovered.
Conclusion: The opposite sides between disc herniation and clinical symptoms of upper extremity may be attributed to C5 ventral rootlet becoming stretched caused by spinal cord rotation or shift to the opposite side.
Keywords: cervical spondylotic amyotrophy, muscle atrophy, anterior decompression
Introduction
Cervical spondylotic amyotrophy (CSA) as the rare form of cervical spondylosis is characterized by severe muscle atrophy in the upper extremities, with or without sensory or lower limb involvement. It can be classified in the proximal subtype and the distal subtype.1 Proximal type CSA is typical by weakness in deltoids and biceps while the distal type CSA is characterized by weakness in forearms and hand muscles.2 In patients with proximal type CSA, impairment of shoulder abduction and elbow flexion are commonly found because of C5 or C6 segmental disorders. Patients with CSA have always been described as unilateral symptoms, but bilateral disease has also been presented occasionally.3 Though the exact incidence of CSA has yet to be established, literature has reported that the incidence of distal subtype is lower than proximal subtype.4 To the best of our knowledge, previous reports all described the same side between spinal cord compression and unilateral motor amyotrophy. Here we present a novel case of unilateral proximal CSA with contralateral spinal cord compression, which is subject to misdiagnosis and missed diagnosis.
Case Report
A 63-year-old female presented with a one-month history of left shoulder and arm weakness. She denied any history of numbness, paresthesia, pain, trauma, stretch injuries, or constitutional symptoms. Examination of her left shoulder showed marked atrophy of the C5 musculature, especially the deltoid, biceps. The strength of wrist extensor in both sides was normal. Passive range of motion was unrestricted in all planes, which means no evidence of capsular tightness. Medical Research Council grade strength of deltoid 1/5, biceps 1/5, triceps 4/5. (Figure 1) Other neurologic function was normal. Magnetic resonance imaging (MRI) of left shoulder showed no obvious evidence of a rotator cuff tear. MRI of the cervical spine indicated multilevel spondylotic changes, both C4–5 level and C5–6 level were included. While the C4–5 level was the most severe segment. The axial MRI of C5–6 level revealed that the space on both sides of neural foramina were acceptable. MRI T2-weighted imaging and CT myelography axial imaging at the C4–5 level showing large right paracentral disc herniation without myelomalacia. There was direct compression of the right anterior horn of the spinal cord on axial images. What is noteworthy was that the left neural foramen seemed to be narrower than the right one. (Figure 2) Electromyography (EMG) changes of denervation were most prominent in the left deltoid and biceps, while the thoracic paraspinal muscles and lower limb muscles were not involved obviously. Neurology consultation excluded amyotrophic lateral sclerosis (ALS) and other neurology-related diseases.
 |
Figure 1 Patient’s positive and behind appearance before surgery on presentation. |
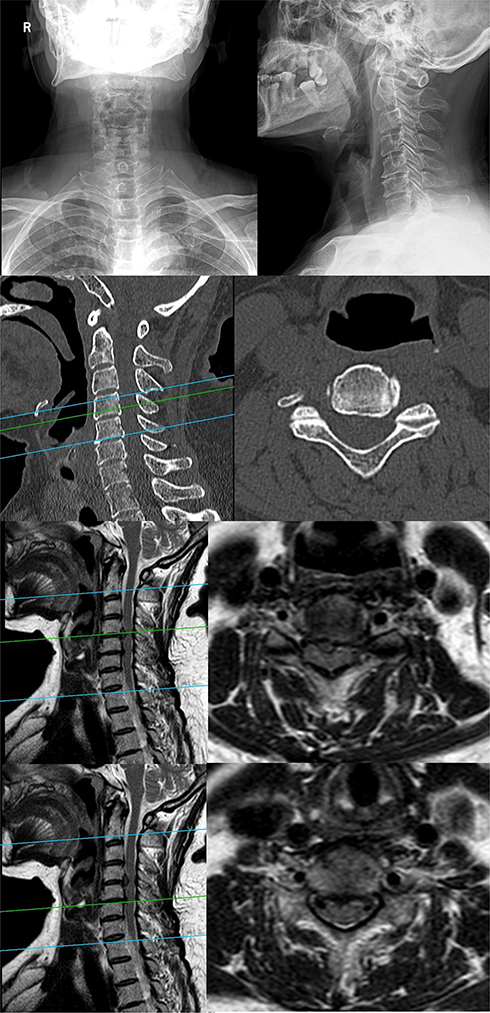 |
Figure 2 Preoperative imaging on presentation. |
This atypical case is different from the CSA prior reported study, but large right paracentral disc herniation in C4–5 level was diagnosed clearly. We speculated that there was some relationship between disc herniation in C4–5 level and clinical symptoms to some extent. After obtaining informed consent, the patient underwent anterior cervical discectomy and fusion technique in C4–5 level. Six weeks postoperatively, the patient’s biceps recovered some strength. Physical examination demonstrated elbow flexion of grade 4/5, deltoid function 2/5, and external rotation 1/5. Twelve weeks postoperatively, patient’s symptoms obviously recovered. Physical examination demonstrated elbow flexion of grade 5/5, deltoid function 3/5, and external rotation 3/5. Atrophy of the deltoid and biceps showed notable improvement. Contour of biceps was clearly visible when compared to preoperation. (Figure 3)
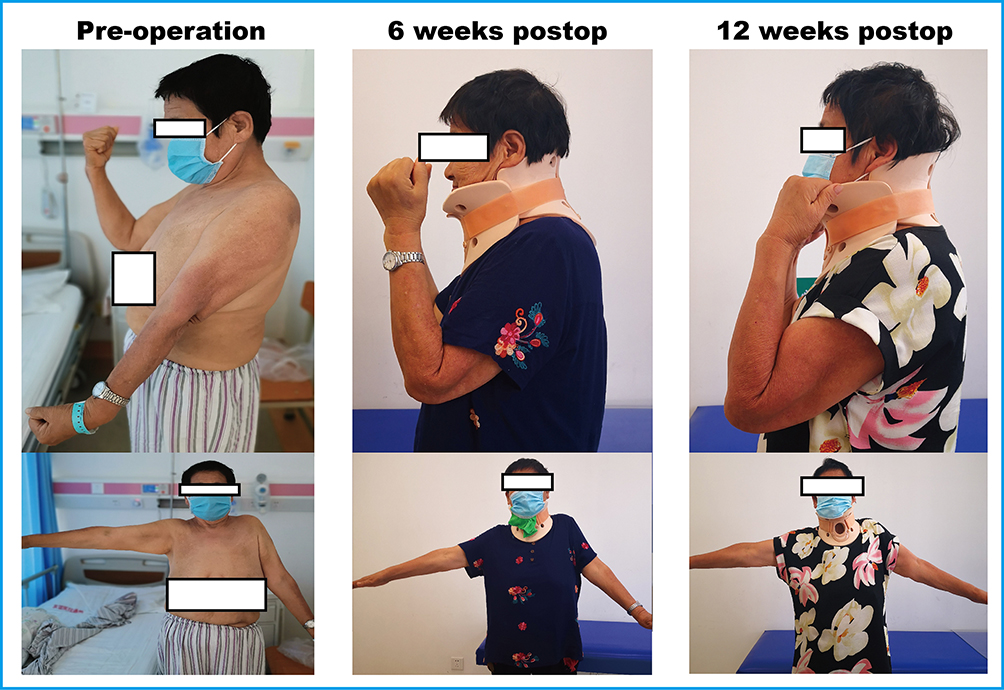 |
Figure 3 Change of upper limb muscle strength in different periods from preoperative to postoperative. |
MRI of the cervical spine at 12 weeks after operation revealed the compression of the spinal cord was removed, and the compressed dural sac notably recovered. Both neural foramens were apparently enlarged than pre-operation. (Figure 4)
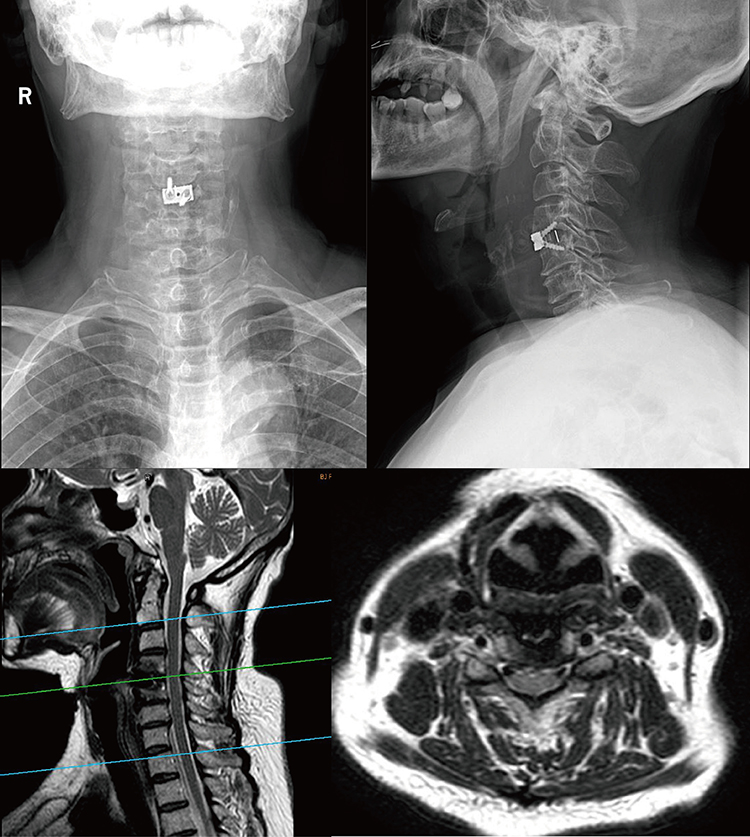 |
Figure 4 Postoperative imaging on presentation. |
The patient was pleased with her functional improvement, and was now able to perform activities of daily living including feeding and personal hygiene.
Discussion
The etiology and pathophysiology of CSA are still controversial. Prior study supposed that the posterolateral osteophytes selectively pressure on intradural ventral nerve root (VNR) might result in related symptoms.5 However, the intrinsic injury to the anterior horn (AH) of the spinal cord was also accepted by some researchers.6 Moreover, the literature had reported the injury to the intradural anterior rootlets was another cause of CSA.7 In addition, a case series proposed that the Luschka’s joint hyperplasia (51%) and disc herniation (30%) were the main etiologies of CSA.8 A recent article has introduced the research progress of CSA in detail.9
However, the above factors cannot provide a convincing explanation in our case. The large disc herniation in C4–5 level was on the right side, which meant the intrinsic injury to the AH of the spinal cord was supposed to have occurred on the right side theoretically, while the clinical symptoms involved the left upper extremity. No compression on the left intradural VNR caused by osteophytes showed in the CT scan. But the MRI revealed the left neural foramen was narrower than the right one, which was consistent with the clinical presentation. These imaging features were rarely mentioned in previous reports.
We speculate that the anatomical features of C5 ventral rootlets might be the entry point to explain the pathogenic factor in this case. Short C5 ventral rootlets appeared to become taut and easily injured when hemilateral anterior compression is performed. Shinomiya et al performed an anatomical study of 36 embalmed adult human cadavers, they supposed that nerve root compromise correlated with spinal cord rotation or shift to the opposite side.10 In this case, the right paracentral disc herniation led to the anterior spinal cord flattening. The nerve roots of opposite side, left C5 ventral rootlet, were tightly stretched due to the spinal cord rotation or shift, while the right C5 ventral rootlet seemed uninjured under certain conditions. This indirect injury mechanism resulted in delays or blocks in the left C5 ventral rootlet conduction and the weakness of deltoid and bicep muscles.
Besides, according to international standards for neurological classification of spinal cord injury (revised 2011), the wrist extensor is the key muscle for the C6 segment. In our case, the strength of wrist extensor in both sides was normal. Therefore, we speculated that C6 impingement was not involved.
Although the involved neurological level was consistent with the demonstration of MRI examination, the diagnosis was still undefined due to inconsistency between the side of compression of spinal cord and clinical symptoms before the operation. Given the deterioration of neurological function, we performed surgical treatment for this patient. We thought it was not a routine medical procedure.
Fortunately, the final clinical results justified our speculations to some extent. That is, the spinal cord rotation or shift was recovered after decompression was removed, which resulted in stretched left C5 ventral rootlet being released shown by postoperative MRI.
A recent systematic review pointed out that MRI showed “snake-eye” appearance on axial images in some of patients who were diagnosed with CSA,11 which indicated intrinsic AH pathology. But this imaging change did not appear in our case. There was no direct evidence to verify the association between AH and CSA by our case. The injury of VNR might be the more convincing factor in this case.
The significance of our case is that no previous reports emphasized the different sides between spinal cord compression and unilateral motor amyotrophy. These studies were too general when describing the symptoms and imaging features. Most of prior report series introduced the same sides between imaging features and symptoms of motor amyotrophy. This interesting case provided a unique view of rare CSA. We admitted that as a simple CSA case, our patient was not rare. But the discrepancy between clinical presentation and radiological finding was the most important point for our case. To the best of our knowledge, no study on this topic has been reported.
Despite the limitations of the short-term follow-up, a favorable result was obtained for weakness of deltoid and bicep muscles in the present case. This case was limited by a lack of measuring blood flow in the anterior spinal artery at the level of the cervical spine. AH appeared in which sides could not be confirmed without cytological examination or autopsy.
Conclusion
In conclusion, the opposite sides between disc herniation and clinical symptoms of upper extremity may be attributed to C5 ventral rootlet being stretched caused by spinal cord rotation or shift to the opposite side. Anterior cervical discectomy and fusion for similar cases may be a feasible option.
Ethical and Consent
The study was approved by the ethics committee of Beijing Friendship Hospital. The patient provided written informed consent to have the case details and any accompanying images published. This study was conducted in accordance with the latest version of the Declaration of Helsinki. This subject was ensured anonymity, which was maintained by using subject-specific numeric code on the record, including registration card.
Funding
The study was funded by the Program of Scientific Research Cultivation in Beijing Municipal Hospitals (PX2020003), Beijing, China.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yanagi T, Kato H, Sobue I. [Clinical characteristics of cervical spondylotic amyotrophy]. Rinsho Shinkeigaku. 1976;16(7):520–528. Japanese.
2. Jiang SD, Jiang LS, Dai LY. Cervical spondylotic amyotrophy. Eur Spine J. 2011;20(3):351–357. doi:10.1007/s00586-010-1544-1
3. Gebere-Michael SG, Johnston JC, Metaferia GZ, et al. Bilaterally symmetric cervical spondylotic amyotrophy: a novel presentation and review of the literature. J Neurol Sci. 2010;290(1–2):142–145. doi:10.1016/j.jns.2009.12.009
4. Tauchi R, Imagama S, Inoh H, et al. Risk factors for a poor outcome following surgical treatment of cervical spondylotic amyotrophy: a multicenter study. Eur Spine J. 2013;22(1):156–161. doi:10.1007/s00586-012-2506-6
5. Imajo Y, Kato Y, Kanchiku T, et al. Pathology and prognosis of proximal-type cervical spondylotic amyotrophy: new assessment using compound muscle action potentials of deltoid and biceps brachii muscles. Spine. 2011;36(7):E476–481. doi:10.1097/BRS.0b013e3181e08d93
6. Zhang J, Cui C, Liu Z, et al. Predisposing factors for poor outcome of surgery for cervical spondylotic amyotrophy: a multivariate analysis. Sci Rep. 2016;6:39512. doi:10.1038/srep39512
7. Tauchi R, Imagama S, Inoh H, et al. Characteristics and surgical results of the distal type of cervical spondylotic amyotrophy. J Neurosurg Spine. 2014;21(3):411–416. doi:10.3171/2014.4.SPINE13681
8. Shinomiya K, Komori H, Matsuoka T, et al. Neuroradiologic and electrophysiologic assessment of cervical spondylotic amyotrophy. Spine. 1994;19(1):21–25. doi:10.1097/00007632-199401000-00005
9. Takahashi T, Hanakita J, Minami M, et al. Cervical spondylotic amyotrophy: case series and review of the literature. Neurospine. 2019;16(3):579–588. doi:10.14245/ns.1938210.105
10. Shinomiya K, Okawa A, Nakao K, et al. Morphology of C5 ventral nerve rootlets as part of dissociated motor loss of deltoid muscle. Spine. 1994;19(22):2501–2504. doi:10.1097/00007632-199411001-00002
11. Luo W, Li Y, Xu Q, et al. Cervical spondylotic amyotrophy: a systematic review. Eur Spine J. 2019;28(10):2293–2301. doi:10.1007/s00586-019-05990-7
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.