")
Back to Journals » Open Access Emergency Medicine » Volume 14
Atypical High-Altitude Cerebral Edema Presentation at an Altitude of Less Than 3000 Meters Elevation: A Case Report
Authors Bolotin T, Prokopakis KE, Becker B
Received 31 August 2021
Accepted for publication 15 March 2022
Published 29 March 2022 Volume 2022:14 Pages 119—122
DOI https://doi.org/10.2147/OAEM.S336951
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Hans-Christoph Pape
Todd Bolotin,1,2 Kayla E Prokopakis,1 Bruce Becker2
1Department of Emergency Medicine, Mercy Health St. Elizabeth Boardman Hospital, Boardman, OH, USA; 2Department of Emergency Medicine, Centura Health St. Anthony Breckenridge Mountain Clinic, Breckenridge, CO, USA
Correspondence: Kayla E Prokopakis, Department of Emergency Medicine, Mercy Health St Elizabeth Boardman Hospital, 11 Ashli Lane, Boardman, OH, 44408, USA, Tel +1 740 512 8498, Email [email protected]
Introduction: Atypical presentations of high altitude cerebral edema may have a stuttering course that can be similar to more common and benign pathology at a lower altitude than typically causes high altitude cerebral edema.
Case Report: A healthy 27-year-old male presented to a medical clinic situated at an altitude of 2829 meters with a “migraine” headache and nausea. He reported several episodes of ‘blurry vision’ each lasting seconds to a minute over the previous day. Symptoms had started four to five days after ascending from his home at sea level. The visual symptoms did not recur while he was in the clinic and his headache and nausea improved after oral medication. The physician recommended advanced imaging at the local hospital, but he declined and was discharged. The following day while riding a ski lift between 2830 and 3782 meters, he had a one-hour episode of visual disturbance with an intense headache. He was directed to proceed to the hospital for magnetic resonance imaging of the brain which demonstrated changes in his corpus callosum consistent with high altitude cerebral edema and he was evacuated to 1609 meters.
Conclusion: An index of suspicion for high altitude cerebral edema must be maintained for any new neurological symptoms in unacclimatized individuals presenting to high alpine environments even those lower than typically associated with this high mortality condition.
Keywords: high altitude cerebral edema, HACE, altitude, cerebral edema
Introduction
Altitude related illness is prevalent in visitors to high alpine environments in the United States and world-wide. Twenty-five percent of individuals ascending from sea level to moderate elevations of 1920 to 2956 meters in Colorado develop some form of acute mountain sickness.1 High altitude pulmonary edema (HAPE), which is noncardiogenic pulmonary edema usually presenting with cough or dyspnea, has an incidence of 0.01–0.1% in Colorado above 2700 meters.2 The incidence can be as great as 15% in the Himalayas at altitudes of 3300 meters or more.3 The incidence high altitude cerebral edema (HACE), defined as symptoms of acute mountain sickness with coinciding ataxia or altered mental status, is significantly lower. HACE has been reported in unacclimatized persons at altitudes above 2000m, but this is exceedingly rare. Due to differences in definition and clinical diagnosis, limited epidemiological research, and significant variability in rates of ascent, the exact incidence of HACE remains unclear. Hackett and Rennie reported HACE in 1.0% of all trekkers between 4243 and 5500 m in Nepal while Wu et al found an incidence of 0.26% in China.4,5 Bärtsch noted an incidence of 0.5% in 5355 visitors to 4555 m in Tibet, based on data reported to him by Tianyi Wu.6 A thirteen year case series documented only thirteen total HACE cases in Colorado visitors who are only able to reach a maximum elevation of 4401m.7 The study participant has given consent to participate and publish the report. Approval was also obtained from the CommonSpirit Health Research Institute, Englewood, CO institutional review board to publish the case details.
Case Report
The patient in this case was a 27-year-old male, native to New York State, who had driven across the country by himself to snowboard in Colorado. His ascent seemed to be rapid as he made the trip in 2 days where he arrived at an altitude of 2773m. While in the state, at this elevation and snowboarded at a maximum elevation of 3962 m. He was in his normal state of good health during the drive and for the first several days after arrival at high altitude. He was snowboarding at a local resort with a summit elevation of 3782 m when he had a sudden onset of transient visual blurring which compromised his ability to snowboard for minutes at a time. These symptoms recurred throughout the day (with and without activity) and were accompanied by a mild headache and a feeling of nausea. He was anorectic but did not vomit. That night he was asymptomatic. The next day while snowboarding the visual symptoms recurred lasting a minute and were followed by a significant headache. He presented to a medical clinic situated at 2829 meters complaining of a ‘migraine’ headache. Initial set of vital signs revealed a blood pressure of 160/97, heart rate of 96, respiratory rate of 17, a temperature of 98.4 and a pulse oximeter reading 92% on room air. The patient noted that his father had a history of migraine headaches and typically reported blurry vision followed by headache and nausea. His family history was significant only for migraine headaches; his personal medical history was negative. He was treated with oral ibuprofen and ondansetron and improved. The physician treating him suggested transfer to the local hospital for advanced imaging, but the patient declined and was discharged. The next day the patient had another episode with more significant visual symptoms that lasted an hour and then resolved while ascending a ski lift between 2830 and 3782 meters. His visual symptoms gradually resolved, but he was left with a severe persistent occipital headache, nausea, and an episode of vomiting. He called the medical clinic and was directed to the local Emergency Department (ED). He presented to the ED at an altitude of 2773 m with the chief complaint of headache and visual changes. He was noted to have a normal physical exam including normal vital signs except for a mildly elevated blood pressure of 153/99, a normal neurologic exam, normal vision, and a normal fundoscopic exam without signs of papilledema or retinal hemorrhage. Lab work was also obtained and was unremarkable. He did not have evidence of hyponatremia or hypoglycemia. The complete blood count, basic metabolic panel and liver function test were all with normal limits. Given the recurrent visual disturbances and headache, a magnetic resonance image (MRI) of the brain was obtained (Figure 1). The MRI showed signs consistent with high altitude cerebral edema. He was given 10 mg of intravenous dexamethasone and transferred to a hospital in Denver at an altitude of 1682 m. He was asymptomatic except for a mild headache after arriving in Denver. He was seen by neurology and observed in the hospital overnight. The following day he was asymptomatic and was discharged after being counseled about proper acclimatization procedures.
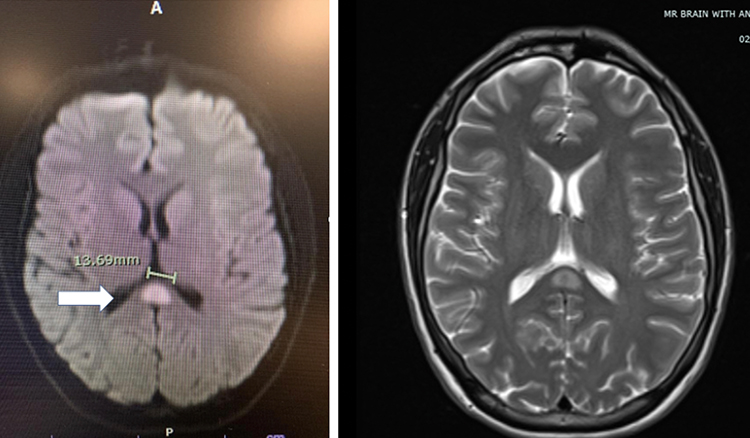 |
Figure 1 Magnetic resonance image of brain with restricted diffusion in splenium of corpus callosum (arrow) on T2 weighted axial image with and without enhancement. |
Discussion
HACE is a severe and potentially fatal form of acute mountain sickness. It is typically characterized by fatigue, headache, altered mental status, and ataxia. Unrecognized and untreated, these patients can proceed to coma and death in less than 24 hours.6 This case represents an atypical presentation as the patient experienced intermittent headache and transient visual changes without the persistent headache, ataxia or alteration in mental status which are the normal manifestations of this form of cerebral edema.6,8,9 This was not the typical HACE presentation as the symptomatology was different as well as the waxing and waning of symptoms rather than their persistence. Usually HACE is progressive and symptoms tend to worsen. The patient presented with a chief complaint of intermittent migraine without any neurologic findings.
The mechanism of injury is thought to be hypoxia induced neurohormonal and hemodynamic changes leading to increased capillary pressure and leakage.8 HACE appears to be a pathophysiologic process caused by cytotoxic and vasogenic edema that can proceed to microvascular disruption and microbleeds. The splenium of the corpus callosum is particularly susceptible to reversible restricted diffusion changes seen on FLAIR and T2 MR imaging.10 These changes in the corpus callosum are demonstrated in our patient in Figure 1. The treatment of HACE involves supplemental oxygen, dexamethasone, and descent. In lieu of descent, a portable hyperbaric chamber may be used.9
As mentioned previously, the patient did present with a headache. A broad differential was considered including a migraine. Diagnosis of a migraine versus HACE may be difficult as a headache can be a symptom of HACE and altitude may also trigger a migraine.11 In our patient, MRI findings confirmed our HACE diagnosis as corpus callosum change would not be seen in a migraine.
Conclusion
This case underlines how important it is that clinicians practicing in mountain environments, where visitors frequently arrive from lower altitudes without acclimatization, have an understanding of HACE, its diagnosis and treatment, and morbidity and mortality if untreated; furthermore, these clinicians must embrace the possibility of atypical presentations that may mimic more benign conditions such as ‘migraines’. HACE should be in the differential diagnosis for any patient recently arrived at high altitude with new onset, unexplained neurologic symptoms. Early diagnosis and treatment can be lifesaving.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Honigman B, Theis MK, Kozoil-McLain J, et al. Acute mountain sickness in a general tourist population at moderate altitudes. Ann Intern Med. 1993;118(8):587–592. doi:10.7326/0003-4819-118-8-199304150-00003
2. Sophocles AM. High-altitude pulmonary edema in Vail, Colorado, 1975–1982. West J Med. 1986;144(5):569–573.
3. Singh I, Roy SB. High altitude pulmonary edema: clinical, hemodynamic, and pathologic studies. In: Command UA, Ra D, editors. Biomedicine of High Terrestrial Elevation Problems. Washington D.C:US Army Research and Development Command; 1969:108–120.
4. Hackett PH, Rennie D, Levine HD. The incidence, importance, and prophylaxis of acute mountain sickness. Lancet. 1976;2(7996):1149–1155. doi:10.1016/S0140-6736(76)91677-9
5. Wu T, Ding S, Liu J, et al. Ataxia: an early indicator in high altitude cerebral edema. High Alt Med Biol. 2006;7(4):275–280. doi:10.1089/ham.2006.7.275
6. Bartsch P, Swenson ER. Acute high altitude illnesses. N Engl J Med. 2013;368(24):2294–2302. doi:10.1056/NEJMcp1214870
7. Yarnell PR, Heit J, Hackett PH. High-altitude cerebral edema (HACE): the Denver/Front Range experience. Semin Neurol. 2000;20(2):209–217. doi:10.1055/s-2000-9830
8. Jensen JD, Vincent AL. High altitude cerebral edema. In: Stat Pearls. Treasure Island (FL): StatPearls Publishing; 2021.
9. Luks AM, McIntosh SE, Grissom CK, et al. Wilderness Medical Society consensus guidelines for the prevention and treatment of acute altitude illness: 2019 update. Wilderness Environ Med. 2019;30(4S):S3–S18. doi:10.1016/j.wem.2019.04.006
10. Hackett PH, Yarnell PR, Weiland DA, et al. Acute and evolving MRI of high altitude cerebral edema: microbleeds, edema and pathophysiology. Am J Neuroradiol. 2019;40(3):464–469. doi:10.3174/ajnr.A5897
11. Hornbein T, Schoene R. High altitude: an exploration of human adaptation. In: Effect of Altitude on Common Medical Conditions, Dekker. New York, NY: CRC Press; 2001:839–886.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.