")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 13
Attitudes toward antipsychotic treatment among patients with bipolar disorders and their clinicians: a systematic review
Authors Sajatovic M, DiBiasi F , Legacy SN
Received 13 April 2017
Accepted for publication 10 July 2017
Published 30 August 2017 Volume 2017:13 Pages 2285—2296
DOI https://doi.org/10.2147/NDT.S139557
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Wai Kwong Tang
Martha Sajatovic,1 Faith DiBiasi,2 Susan N Legacy3
1Departments of Psychiatry and Neurology, Case Western Reserve University School of Medicine, Cleveland, OH, USA; 2US Medical Affairs, Neuroscience, Otsuka Pharmaceutical Development & Commercialization, Inc., Rockville, MD, USA; 3US Medical Affairs, Neuroscience, Otsuka Pharmaceutical Development & Commercialization, Inc., Princeton, NJ, USA
Introduction: Antipsychotics are recommended as first-line therapy for acute mania and maintenance treatment of bipolar disorder; however, published literature suggests their real-world use remains limited. Understanding attitudes toward these medications may help identify barriers and inform personalized therapy. This literature review evaluated patient and clinician attitudes toward the use of antipsychotics for treating bipolar disorder.
Materials and methods: A systematic search of the Cochrane Library, Ovid MEDLINE, Embase, and BIOSIS Previews identified English language articles published between January 1, 2000, and June 15, 2016, that reported attitudinal data from patients, health care professionals, or caregivers; treatment decision-making; or patient characteristics that predicted antipsychotic use for bipolar disorder. Results were analyzed descriptively.
Results: Of the 209 references identified, 11 met the inclusion criteria and were evaluated. These articles provided attitudinal information from 1,418 patients with bipolar disorder and 1,282 treating clinicians. Patients’ attitudes toward antipsychotics were generally positive. Longer duration of clinical stability was associated with positive attitudes. Implementation of psychoeducational and adherence enhancement strategies could improve patient attitudes. Limited data suggest clinicians’ perceptions of antipsychotic efficacy and tolerability may have the greatest impact on their prescribing patterns. Because the current real-world evidence base is inadequate, clinician attitudes may reflect a relative lack of experience using antipsychotics in patients with bipolar disorder.
Conclusion: Although data are very limited, perceived tolerability and efficacy concerns shape both patient and clinician attitudes toward use of antipsychotic drugs in bipolar disorder. Additional studies are warranted.
Keywords: bipolar disorder, antipsychotics, systematic review, attitudes
Introduction
Bipolar spectrum disorders (BSDs) consist of many cycling mood disorders, with an estimated prevalence ranging from 2.4% to 15.1%,1,2 comprising bipolar I disorder (BD-I), bipolar II disorder, cyclothymic disorder, and other related disorders. BSD is often complicated by many other comorbidities such as anxiety, substance abuse, and personality disorders3,4 and is associated with a high suicide rate relative to other types of depression.5 Poor treatment adherence and frequent discontinuation of treatment among patients with BSD are common clinical problems and may be responsible for illness chronicity, comorbidity complications, and increased economic burden.3,4 Since the year 2000, numerous second-generation antipsychotics (SGAs) have received US Food and Drug Administration approval for first-line treatment of BD-I.6–9 These treatments are approved either as monotherapies or in combination with lithium and/or anticonvulsants.6–8 The most recent guidelines for the treatment of bipolar disorder recommend antipsychotics as first-line therapy for acute mania and maintenance treatment.4,10–13 Although trends in prescribing patterns show an increase in prescribing of antipsychotics for bipolar disorder over the past decade,14 their real-world use remains limited, and lithium and anticonvulsant mood stabilizers remain the standard of care.15–17
Barriers to use of second-generation antipsychotic medications (APs) in bipolar disorder may exist for reasons related to the patient,18,19 clinician,20,21 or health care system.22,23 It is possible that patients and clinicians generally avoid antipsychotics in bipolar disorder because of early reports that described dysphoria or subjective discomfort with first-generation compounds.24–27 Patient- or clinician-related barriers may include tolerability concerns, specifically the increased risk of adverse effects, such as weight gain, metabolic syndrome, hypertension, dyslipidemia, and QT prolongation.28–31 Further, formulary restrictions may lead to prescribing barriers.22,23
Studies have shown that medication satisfaction is positively correlated with treatment adherence, and better adherence is associated with symptom reduction.32,33 However, choosing treatment that is the best fit for patients is a complex process. Clinicians must weigh efficacy benefits versus tolerability concerns based on their familiarity with the drug and available clinical data.20,21,34 Individual patient factors, including preference for a specific treatment modality, treatment history, comorbidities, and adherence history, all need to be considered.34 Factors that affect patient attitudes toward treatment include duration of untreated disease, insight, and past treatment experience.19 This systematic review evaluated the published literature on patient and clinician attitudes toward the use of antipsychotics for the treatment of bipolar disorder. Findings on what patients and clinicians believe to be factors that encourage or discourage the use of this class of drugs may help in understanding the place of these compounds in the bipolar disorder treatment armamentarium and inform personalized therapy for patients with bipolar disorder.
Materials and methods
Search methodology
Systematic searches were performed focused on identifying original research studies and reviews that described barriers and facilitators to prescribing or taking AP for the treatment of bipolar disorder. The Cochrane Library; Ovid MEDLINE® In-Process & Other Non-Indexed Citations; Ovid MEDLINE 1996 to June 15, 2016; Embase 1974 to June 15, 2016; and BIOSIS Previews 1993 to 2016 Week 29 were searched using the following search string: (“bipolar disorder” AND “antipsychotic” NOT “lithium” NOT “valproate”) AND (“barriers” OR “attitudes” OR “prescribing patterns” OR “treatment planning” OR “prescribing” OR “decision-making” OR “treatment choice” OR “awareness” OR “perception” OR “knowledge” OR “experience” OR “treatment satisfaction” OR “stigma”). The searches were limited to English language articles published in peer-reviewed journals between January 1, 2000, and June 15, 2016. The year 2000 was chosen as a cutoff date to ensure clinical relevance of the included articles based on the availability of multiple APs. Eligible articles were also searched by hand to see if there were any additional publications in their reference list that met the initial inclusion criteria.
Article selection process
Authors independently evaluated the articles for eligibility, beginning with the titles (performed by two authors), proceeding to abstracts (each abstract reviewed by two authors, all authors participated), and, lastly, full text (each full-text article reviewed by two authors, all authors participated). Disagreements were resolved by discussion among all authors. Only those articles containing either primary or secondary analyses specific to the bipolar disorder population, including any subgroup analyses specific to patients with this diagnosis, were included. Studies that reported only efficacy or safety, or adherence behavior information without specific attitudinal data from patients, health care professionals, or caregivers were excluded. Review articles and opinion pieces not containing original research data were excluded after their reference lists were searched to identify any new/original research articles not previously identified. Preclinical research, case reports, policy-focused articles, studies in pediatric patients, or those that reported use of antipsychotics in other psychiatric conditions without including bipolar disorder were excluded as well. Descriptive analysis of the selected articles was performed.
Results
Article selection
The initial database search retrieved 270 references with another 12 records identified through other sources, including a search by hand (Figure 1). After duplicates were removed, 209 unique references were screened, and 172 references were excluded after the title and abstract review. The remaining 37 articles were subjected to a full-text review, and 11 articles with attitudinal information from patients with bipolar disorder or clinicians treating patients with bipolar disorder were identified and subsequently analyzed.
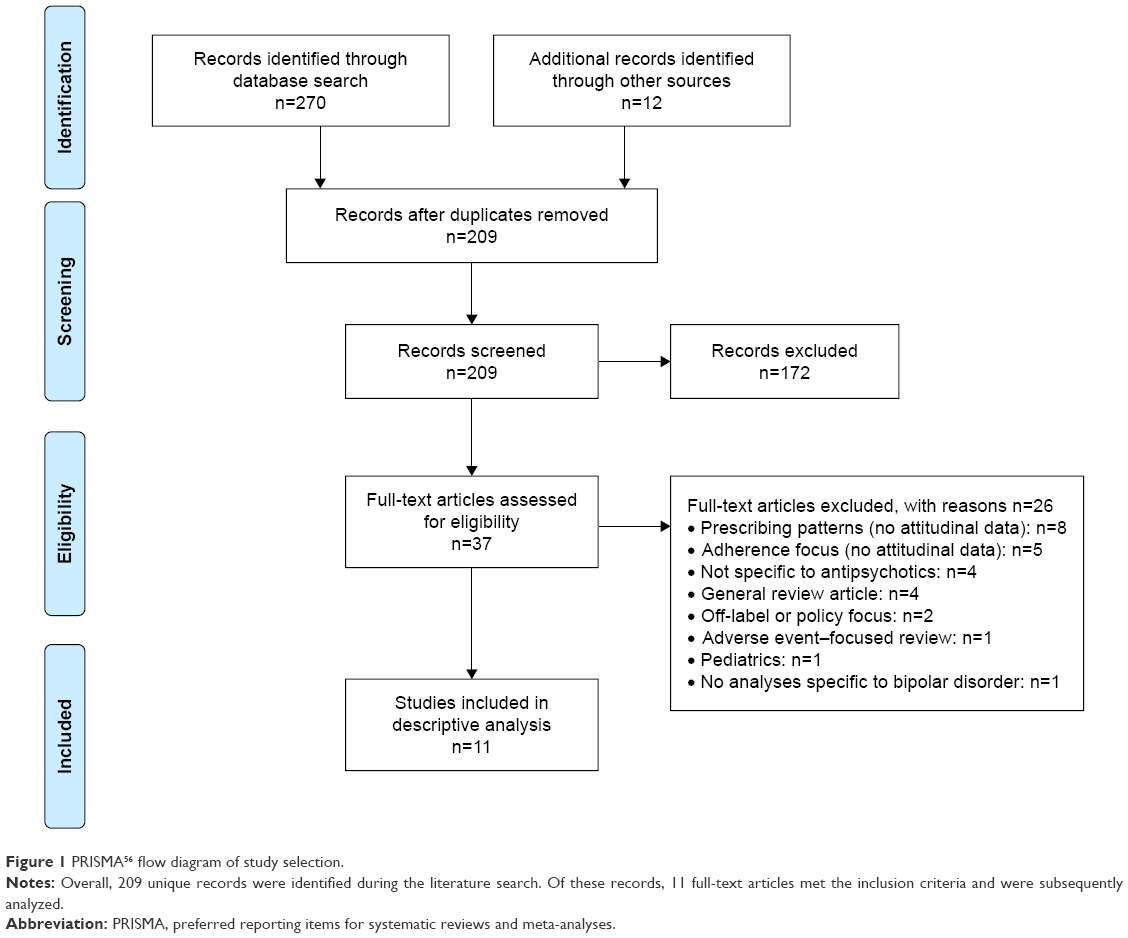 | Figure 1 PRISMA56 flow diagram of study selection. |
Study characteristics
Overall, 11 articles reported attitudinal information, representing a total of 1,418 patients with bipolar disorder (Table 1)18,19,32,35–37 and 1,282 treating clinicians (Table 2)20,34,38–40 from the US, Argentina, and Europe (Figure 2).18–20,32,34–40 All studies assessing patient attitudes used surveys or validated questionnaires, such as the Drug Attitude Inventory (DAI) and the Attitudes toward Mood Stabilizers Questionnaire (AMSQ). The articles pertaining to clinicians primarily determined attitudes using nonstandardized surveys developed to characterize the decision-making process during drug selection. All standardized instruments used for assessing attitudes toward APs in the studies identified by this search are summarized in Table 3.35,41–45
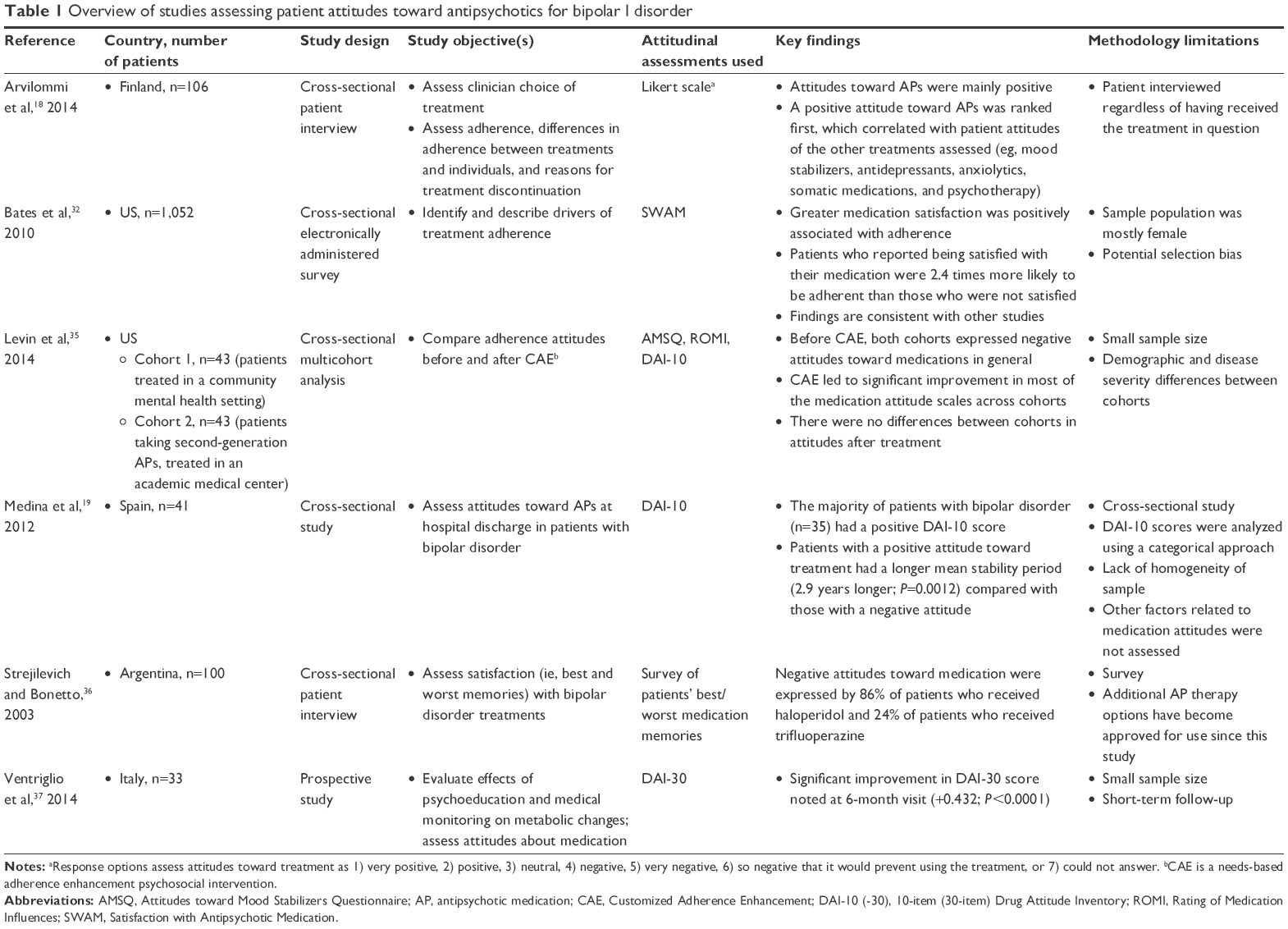 | Table 1 Overview of studies assessing patient attitudes toward antipsychotics for bipolar I disorder |
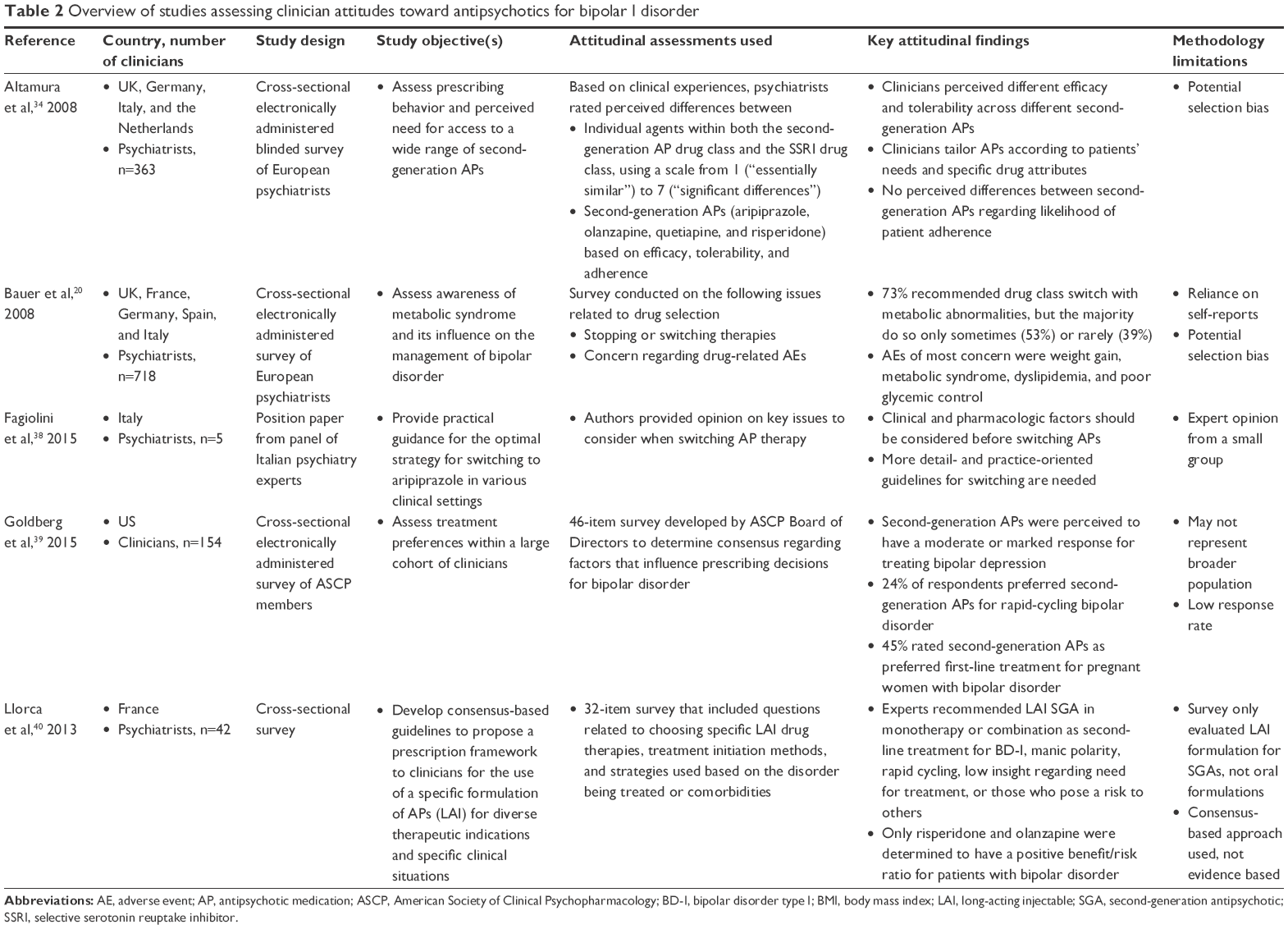 | Table 2 Overview of studies assessing clinician attitudes toward antipsychotics for bipolar I disorder |
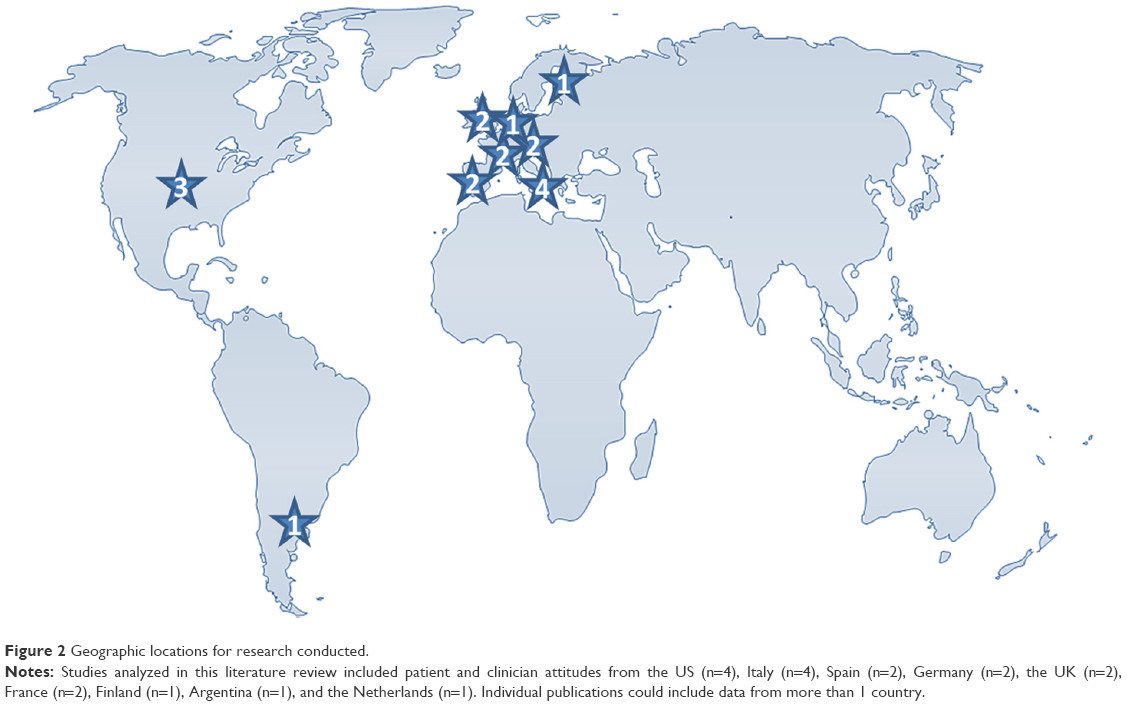 | Figure 2 Geographic locations for research conducted. |
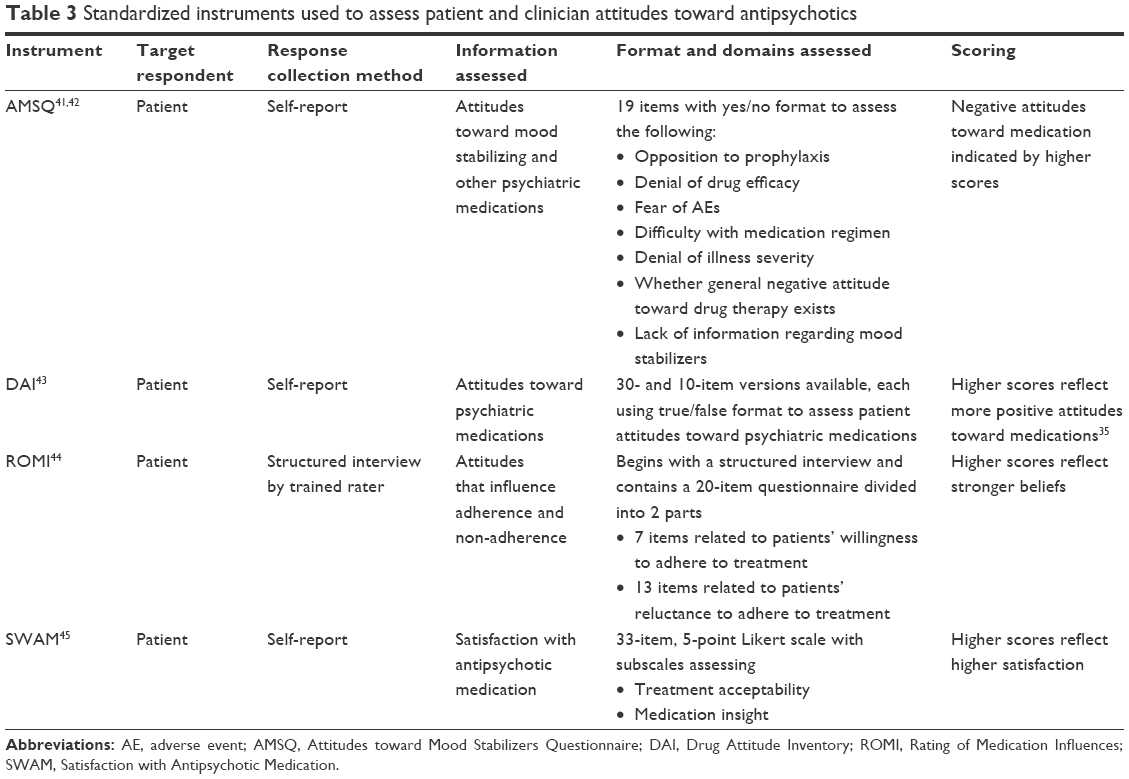 | Table 3 Standardized instruments used to assess patient and clinician attitudes toward antipsychotics |
Patient attitudes
Although the data are limited, articles reporting patient attitudes suggest that the majority of patients with bipolar disorder have positive attitudes toward antipsychotic treatment18 and that negative attitudes are generally held by those who have poor insight regarding their illness or less stable disease.19 Available data also indicate that positive attitudes toward medications are associated with better adherence32 and that educational strategies may improve attitudes toward medication and, in turn, improve adherence.35,37
The Jorvi Bipolar Study,18 a naturalistic study conducted in Finnish patients with bipolar disorder type I or II, assessed patient attitudes toward various types of treatment, including antipsychotics. For the 176 patients followed during the first 6 months of this study, most (86.9%) received mood stabilizers or SGAs. Of 106 patients who provided responses, 7.5% reported having a negative attitude toward antipsychotics that would prevent them from using this treatment. At 18 months of follow-up, ~29% of those taking antipsychotics reported nonadherence, of which >20% was attributed to a generally negative attitude toward treatment. Results from this study suggest that negative attitudes toward antipsychotic treatment can increase the likelihood of nonadherence more than sevenfold, based on an odds ratio comparing those with negative versus positive attitudes. However, overall, patients reported positive attitudes toward antipsychotics, similar to their attitudes regarding other treatments for bipolar disorder (eg, mood stabilizers, antidepressants, and anxiolytics).
Bates et al32 found that patient satisfaction with medication, as assessed by the Satisfaction with Antipsychotic Medication (SWAM) scale, was positively associated with treatment adherence. These investigators recruited patients who participated in the 2006 and 2007 US National Health and Wellness Survey. A total of 1,052 patients who self-reported a diagnosis of bipolar disorder and had a Composite International Diagnostic Interview–bipolar disorder score of ≥7 (indicating higher risk for bipolar disorder) and did not have schizophrenia were surveyed to determine attitudes toward current medication. Patient adherence was measured using the Morisky Medication Adherence Scale. The majority of patients in this cross-sectional sample, both adherent and nonadherent, were female (>75%), and 47% and 2% were being treated with second- and first-generation antipsychotics, respectively. Overall, patients who reported satisfaction with their AP, as measured by the SWAM, were 2.4 times as likely to be adherent as patients who were dissatisfied.
In a cross-sectional study conducted in Spain, Medina et al19 assessed attitudes toward antipsychotics among inpatients with schizophrenia or bipolar disorder. Forty-one patients with bipolar disorder who were admitted for an acute manic episode were included, though only limited results were reported separately for this group. Using the 10-item DAI (DAI-10), a true–false self-report instrument that assesses patients’ experience with psychotropic medications,43,46,47 and the Rating of Medication Influences (ROMI), a scale that assesses subjective reasons for adherence or nonadherence,44 these investigators found that patients with bipolar disorder who exhibited positive attitudes toward treatment (n=35) had a significantly longer duration of clinical stability (ie, an event-free period) versus those with negative attitudes (n=6; mean difference in stability time, 2.9 years; P=0.0012).
Only one study reported negative attitudes toward specific psychotropic drugs.36 In a letter to the editor, Strejilevich and Bonetto36 briefly described subjective findings from a survey they conducted among 100 Argentinian patients with bipolar disorder. When patients were asked about their experience related to treatment, haloperidol and trifluoperazine were the drugs most commonly associated with the worst memories (86% and 24% of patients, respectively). The authors note, however, that more recent data suggest better subjective tolerability with newer SGAs.
Two studies monitored patients’ attitudes toward medication before and after specific psychosocial and educational interventions.35,37 Ventriglio et al37 used the 30-item DAI (DAI-30) to prospectively evaluate the effects of psychoeducation on medication attitudes among 33 patients with BD-I and 33 with schizophrenia from a single center in Italy. Education was aimed at increasing awareness of the patient’s respective psychiatric illness as well as general health, diet, exercise, weight control, and current treatment. Results following the intervention were reported separately for the two diagnoses. Most of the patients with BD-I were receiving antipsychotics (97.0%), and no change in mean dosing was observed during the study. At the 6-month follow-up assessment, patients with BD-I showed a significantly improved DAI-30 score (+0.432; P<0.0001).
In the second study, Levin et al35 conducted an analysis of medication adherence and attitudes assessed before and after Customized Adherence Enhancement (CAE), a needs-based adherence enhancement psychosocial intervention. Data were extracted from three studies, two of which each enrolled 43 poorly adherent patients with bipolar disorder, each from different clinical settings in the US (ie, a community mental health center or an academic medical center), who were receiving SGAs and/or mood stabilizers, as well as a third cohort of patients with schizophrenia (n=10) or schizoaffective disorder (n=20).48,49 Medication adherence and attitudes assessed before and after CAE using the Tablet Routines Questionnaire, AMSQ, the ROMI, and the DAI-10, demonstrated improvements in medication adherence and in most of the medication attitude scales.35
Our review found seven articles (64%) that included attitudinal data pertaining to patients with bipolar disorder in addition to patients with other psychiatric illnesses,19,34,35,37–40 yet only five of these included survey questions or statistical analyses in the subgroup of patients with bipolar disorder.19,34,37,39 The remaining two articles provided only descriptive attitudinal data specific to patients with bipolar disorder, without further analyses in this subgroup.35,38 Two of the articles that assessed patients’ subjective attitudes toward antipsychotics offered overarching conclusions for patients with bipolar disorder combined with those with schizophrenia or schizoaffective disorder despite inherent differences in these conditions,19,35 though Levin et al35 performed analyses of covariance confirming no significant effect of diagnosis on any of the attitudinal measures.35
Clinician attitudes
Based on the articles identified in this search, information regarding clinician attitudes toward APs appears to be limited and comes largely from surveys that did not use standardized instruments. The literature suggests that clinicians perceive antipsychotic efficacy and tolerability as varying across patients and that there is a need for personalization of treatment regimens based on patient clinical needs.34,38
A European survey of psychiatrists in the UK, Germany, Italy, and the Netherlands examined perceptions about antipsychotic drug therapy among 363 psychiatrists from a variety of practice settings, primarily offices/private consulting (31%), hospitals (23%), and outpatient clinics (20%).34 Responses were based on physicians’ notes from 1,442 patients with schizophrenia (53%) or bipolar disorder (47%). Results suggested that, overall, physicians perceive significant differences in efficacy and tolerability between the SGAs, and the most common reasons for sequential prescribing of these drugs in patients with bipolar disorder were avoidance of specific side effects (90%), consideration of treatment history (92%), patient discontinuation or nonadherence (84%), and the presence of specific clinical symptoms (80%). Overall, the authors concluded that tailoring therapy should involve consideration of a variety of factors, including a patient’s previous medication experience, comorbidities, current symptoms, environment, and medication tolerability.
In a position paper published by a panel of Italian psychiatry experts, guidance is offered regarding the optimal strategy for switching to the SGA aripiprazole.38 Similar to the findings from the survey research described earlier, these authors highlight the need to consider factors such as patient characteristics, illness, medication, and environment, and note that medications should be evaluated individually when making the decision to switch between antipsychotics.
A survey of 718 European psychiatrists in the UK, Germany, France, Italy, and Spain, 67% of whom were practicing in the hospital setting, specifically assessed how metabolic concerns influence psychiatrists’ opinions regarding the treatment of bipolar disorder.20 The potential for weight gain was identified as the most common concern, and respondents reported this was also their patients’ top concern. The majority of psychiatrists associated several of the evaluated antipsychotics with weight gain, most often olanzapine (94%) and risperidone (72%). The authors note this is a significant finding not only because of increased cardiovascular risk but because weight gain can lead to nonadherence.
Two additional articles provide further insight regarding factors that drive psychiatrists’ pharmacotherapy decision-making in the treatment of bipolar disorder.39,40 Goldberg et al39 conducted a survey of the membership of the American Society of Clinical Psychopharmacology to determine consensus on sequential treatment steps for major depression and bipolar disorder. A total of 154 responses were received, primarily from clinicians who were directly involved in patient care ≥75% of their time (71%).39 All respondents reported prescribing SGAs for bipolar depression, and 90% believed they provide a moderate to marked response. When asked which clinical factors influenced prescribers away from using an antidepressant for bipolar depression, 89% indicated rapid cycling was a key consideration, and SGAs were a preferred first-line treatment in this patient group by 24% of respondents. In addition, when asked about preferred first-line agents for treating bipolar disorder during pregnancy, SGAs were most commonly selected (45% of respondents); the next most frequently selected first-line treatments were lamotrigine (35%) and FGAs (21%).
In the second article, Llorca et al40 report results from a 32-item questionnaire completed by experts from the French Association for Biological Psychiatry and Neuropsychopharmacology during development of treatment guidelines for the use of long-acting injectable (LAI) antipsychotics in serious mental illnesses, specifically schizophrenia, schizoaffective disorder, delusional disorder, and bipolar disorder.40 A consensus rating scale was used in which respondents expressed levels of agreement or disagreement with survey questions, and these responses were then interpreted as recommended indications for first-, second-, or third-line treatment strategies for each diagnosis. The majority of respondents (54.8%) felt that patients with bipolar disorder could benefit from a second-generation LAI (monotherapy or in combination) as second-line therapy. These guidelines specifically recommended second-generation LAI antipsychotics as second-line treatment for patients with BD-I, manic polarity, rapid-cycling bipolar disorder, and low insight as well as those who pose a risk to others. First- or second-generation LAI antipsychotics were recommended as first-line treatment for patients who exhibited partial/full nonadherence and those who preferred these therapies.
Similarly, among the articles describing clinician attitudes, one provided overall conclusions that combined patients with bipolar disorder and those with schizophrenia,34 but did include a separate discussion of the top considerations for psychiatrists choosing between SGAs for bipolar disorder, namely, side effects, and patient treatment history.
Discussion
Our review suggests that assessing patient attitudes toward medication and implementing strategies to combat those that may be based on inaccurate or inadequate knowledge could help maintain adherence and improve long-term outcomes. Two studies reported in this review found that specific educational strategies can improve patient attitudes toward medications.35,37 Targeting specific negative attitudes or reasons for poor adherence can potentially improve attitudes and may ultimately lead to better adherence, as highlighted by the two longitudinal studies of Levin et al,50 which demonstrated that patients whose medication attitudes improved became more adherent to treatment.
It is important to note that caregiver attitudes toward treatment can also play a key role in medication attitudes and adherence in general,51,52 as reported by Chang et al51 who in a cross-sectional study investigated 200 outpatients with a chronic psychiatric disorder and their caregivers about their attitudes toward psychotropic medications. This study revealed that additional factors that shape both patient and caregiver attitudes toward medications include perceived risks and benefits of the treatment, necessity for taking medication, and costs. In another cross-sectional analysis, Chang et al51 evaluated the relationship between medication attitudes and a number of patient-related variables. Patients with more positive attitudes toward medication had better social support and believed more strongly that others, such as family or clinicians, determine their health outcomes. Although further work is needed to assess how both patient and caregiver medication attitudes directly affect adherence,51,52 current evidence generally suggests that it is beneficial to include caregivers in education and support focused on medication prescribing and medication taking.
This review found that clinician perceptions of drug-specific efficacy, tolerability, and adverse effects impact their attitudes toward antipsychotics. It is worth noting, however, that clinician attitudes were not specifically assessed using standardized attitude questionnaires. Although none of the articles used an attitude-specific measure for evaluation, general perceptions in the form of recommendations39,40 and prescribing behaviors34 gave some insight into clinicians’ attitudes toward antipsychotic use for bipolar disorder. Clinicians mainly focused on drug characteristics (eg, efficacy, pharmacologic activity, and tolerability20,38) and patient comorbidities and potential propensity to experience side effects (eg, weight, medical history20,38) to guide their treatment decisions and prescribing patterns.20 Perceived tolerability of individual treatments, particularly potential metabolic risks, strongly affected treatment choice.
Overall, this review found few published studies addressing patient or clinician attitudes toward antipsychotics in the treatment of bipolar disorder. Many articles did not include attitudinal data as a primary outcome, and all had methodological limitations such as cross-sectional design, which prohibits causal interpretation, or a relatively short follow-up period, which precludes generalization to long-term treatment regimens that are the norm for bipolar disorder.
Although one study in this review reported negative patient attitudes associated with specific first-generation antipsychotics (haloperidol and trifluoperazine),36 it should be noted that this study may have limited current clinical relevance since it was conducted in 1999 and published over a decade ago. Numerous SGA treatments have been approved for use in bipolar disorder in the past 15 years. The bipolar clinical trial evidence base for the second-generation compounds is robust, and these agents generally have a decreased risk of extrapyramidal symptoms compared with first-generation compounds.6,28,53 Several of the articles identified in this review failed to distinguish between first-generation antipsychotics and SGAs. Interpretations regarding patient attitudes specific to first-generation antipsychotics are especially limited because in the two articles that assessed attitudes toward these agents either few patients were taking this class of antipsychotics (1.7% of the patient sample)32 or the data were derived >15 years ago with little detail on study methodology.36 Clinician attitude articles similarly had limited focus on first-generation drugs. Importantly, because of the overall lack of distinction between older and newer antipsychotics, along with the overall limited number of studies identified, some of which included very small numbers of patients with bipolar disorder, findings from this review may not be generalizable to the first-generation antipsychotics.
More than half of the articles identified in this review did not distinguish the subtypes of bipolar disorder in the patient sample (54.5%).19,20,32,34–36 This is a well-known limitation of the available literature, as noted in treatment guidelines, leading to uncertainty regarding whether subtypes of patients with bipolar disorder may respond differently to treatments.12 Likewise, it is unclear whether patients with different subtypes of bipolar disorder may have differing attitudes toward antipsychotic treatment. For example, individuals with a history of manic psychosis and hospitalization might potentially have negative thoughts or memories of antipsychotics, while individuals with no history of frank mania who are receiving antipsychotic treatment for long-term mood stabilization may have a very different experience. In addition, the inclusion of patients with a self-reported diagnosis of bipolar disorder32 adds uncertainty to generalization of the findings.
Given that data specific to the use of antipsychotics for bipolar disorder are limited, it is possible that the findings regarding clinician attitudes may, in part, reflect a relative lack of experience using antipsychotics in this patient population, drawing attention to the larger issue that few data are available to support evidence-based decisions in this area. As prescribing patterns for bipolar disorder are reported to be changing in some settings, with antipsychotics increasingly prescribed,14,54 additional evidence on both patient and clinician attitudes toward antipsychotic drugs in the treatment of bipolar disorder will likely accumulate over time.
After performing this systematic review of current literature, numerous research gaps were identified. As newer SGAs become approved for treating people with bipolar disorder, there remain scant high-quality data regarding patient, provider, or caregiver attitudes toward their use. The majority of the literature regarding attitudes toward bipolar disorder treatments is focused on lithium and anticonvulsants, while attitudes toward antipsychotics are primarily found in the schizophrenia literature. Although this review of the literature provides some insight into current patient and clinician attitudes, a comprehensive and prospective evaluation of factors that influence antipsychotic drug attitudes in bipolar disorder has not been conducted. There is a need for well-designed, real-world studies using standardized, validated questionnaires to collect additional attitudinal data that can be placed into clinical context, with an emphasis on understanding how medication attitudes influence treatment decisions in bipolar disorder. Additional studies that evaluate clinician and patient attitudes toward specific drugs, drug classes, and different drug formulations (eg, LAI antipsychotics) in bipolar disorder may help to identify ways to optimize adherence, satisfaction with care, and long-term outcomes.
As with any systematic review, our analysis had several limitations. Our search was limited to articles written in English; potentially relevant articles published in other languages were not captured. Although a comprehensive list of search terms was designed to retrieve all publications regarding attitudes toward antipsychotics for bipolar disorder, a search done by hand retrieved additional pertinent references, indicating that some publications meeting our search criteria may not have been captured and evaluated. Although there were few articles meeting the predefined inclusion criteria, we believe that the risk of publication bias with a broad, drug-class wide attitudinal analysis such as ours is likely lower compared to publications on studies focused on efficacy or safety of specific drugs. Moreover, the results are specific to antipsychotics in bipolar disorder and cannot be compared with or generalized to attitudes toward other treatments for bipolar disorder. Further, the articles could not be directly compared because their studies had varying designs, endpoints, and attitude evaluation methods (eg, surveys versus interviews; numerous questionnaires [DAI, ROMI, SWAM, AMSQ]). Lastly, given the limited quantity of data and the lack of consistent methodology, a meta-analysis could not be performed to quantify differences. We used the preferred reporting items for systematic reviews and meta-analyses (PRISMA) approach55 to guide our literature review, although there are other guidelines that may have been appropriate as well, such as enhancing transparency in reporting the synthesis of qualitative research (ENTREQ).56
Conclusion
In conclusion, there remains a dearth of information regarding patient and clinician attitudes toward the use of antipsychotics for the treatment of bipolar disorder. Understanding attitudes may help overcome barriers, meet treatment expectations, and confer greater treatment adherence. Additional real-world studies are warranted.
Acknowledgments
This research was supported by Otsuka Pharmaceutical Development & Commercialization, Inc. Editorial support for the preparation of this manuscript was provided by Jessica Holzhauer, DVM, and Sheri Arndt, PharmD, of C4 MedSolutions, LLC (Yardley, PA), a CHC Group company, with funding from Otsuka Pharmaceutical Development & Commercialization, Inc.
Disclosure
Martha Sajatovic has received research support from the National Institutes of Health, Centers for Disease Control and Prevention, Janssen, Merck, Pfizer, Reinberger Foundation, Reuter Foundation, and the Woodruff Foundation; has been a consultant for Bracket, Neurocrine, Otsuka, Pfizer, Prophase, and Supernus; has received royalties from Johns Hopkins University Press, Lexicomp, Oxford University Press, Springer Press, and UpToDate; and has participated in CME activities for the American Physician Institute, CMEology, and MCM Education. Faith DiBiasi and Susan N Legacy are employees of Otsuka Pharmaceutical Development & Commercialization, Inc. The authors report no other conflicts of interest in this work.
References
Dell’Aglio JC Jr, Basso LA, Argimon II, Arteche A. Systematic review of the prevalence of bipolar disorder and bipolar spectrum disorders in population-based studies. Trends Psychiatry Psychother. 2013;35(2):99–105. | ||
Merikangas KR, Jin R, He JP, et al. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch Gen Psychiatry. 2011;68(3):241–251. | ||
Fagiolini A, Forgione R, Maccari M, et al. Prevalence, chronicity, burden and borders of bipolar disorder. J Affect Disord. 2013;148(2–3):161–169. | ||
Fountoulakis KN, Grunze H, Vieta E, et al. The International College of Neuro-Psychopharmacology (CINP) treatment guidelines for Bipolar disorder in adults (CINP-BD-2017), part 3: the clinical guidelines. Int J Neuropsychopharmacol. Epub 2016 Dec 10. | ||
Latalova K, Kamaradova D, Prasko J. Suicide in bipolar disorder: a review. Psychiatr Danub. 2014;26(2):108–114. | ||
Ketter TA, Citrome L, Wang PW, Culver JL, Srivastava S. Treatments for bipolar disorder: can number needed to treat/harm help inform clinical decisions? Acta Psychiatr Scand. 2011;123(3):175–189. | ||
Abilify® (aripiprazole) [prescribing information]. Tokyo, Japan: Otsuka Pharmaceutical Co., Ltd.; 2016. | ||
Saphris® (asenapine) [prescribing information]. St. Louis, MO: Forest Pharmaceuticals, Inc.; 2015. | ||
US Food and Drug Administration. Approval package for: application number NDA 20-592/S-006 Zyprexa oral tablets. 2000 Available from: http://www.accessdata.fda.gov/drugsatfda_docs/nda/2000/020592_S006_ZUPREXA_ORAL_TABS_AP.pdf. Accessed December 1, 2016. | ||
Goodwin GM, Consensus Group of the British Association for Psychopharmacology. Evidence-based guidelines for treating bipolar disorder: revised second edition – recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2009;23(4):346–388. | ||
Malhi GS, Bassett D, Boyce P, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Aust N Z J Psychiatry. 2015;49(12):1087–1206. | ||
American Psychiatric Association. Practice guideline for the treatment of patients with bipolar disorder, second edition; 2002. Available from: http://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/bipolar.pdf. Accessed July 21, 2016. | ||
American Psychiatric Association. Guideline watch: practice guideline for the treatment of patients with bipolar disorder, second edition; 2005. Available from: http://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/bipolar-watch.pdf. Accessed November 22, 2016. | ||
Kessing LV, Vradi E, Andersen PK. Nationwide and population-based prescription patterns in bipolar disorder. Bipolar Disord. 2016;18(2):174–182. | ||
Hirschowitz J, Kolevzon A, Garakani A. The pharmacological treatment of bipolar disorder: the question of modern advances. Harv Rev Psychiatry. 2010;18(5):266–278. | ||
Karanti A, Kardell M, Lundberg U, Landen M. Changes in mood stabilizer prescription patterns in bipolar disorder. J Affect Disord. 2016;195:50–56. | ||
Miura T, Noma H, Furukawa TA, et al. Comparative efficacy and tolerability of pharmacological treatments in the maintenance treatment of bipolar disorder: a systematic review and network meta-analysis. Lancet Psychiatry. 2014;1(5):351–359. | ||
Arvilommi P, Suominen K, Mantere O, Leppamaki S, Valtonen H, Isometsa E. Predictors of adherence to psychopharmacological and psychosocial treatment in bipolar I or II disorders – an 18-month prospective study. J Affect Disord. 2014;155:110–117. | ||
Medina E, Salva J, Ampudia R, Maurino J, Larumbe J. Short-term clinical stability and lack of insight are associated with a negative attitude towards antipsychotic treatment at discharge in patients with schizophrenia and bipolar disorder. Patient Prefer Adherence. 2012;6:623–629. | ||
Bauer M, Lecrubier Y, Suppes T. Awareness of metabolic concerns in patients with bipolar disorder: a survey of European psychiatrists. Eur Psychiatry. 2008;23(3):169–177. | ||
Campbell EC, DeJesus M, Herman BK, et al. A pilot study of antipsychotic prescribing decisions for acutely-Ill hospitalized patients. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(1):246–251. | ||
Seabury SA, Goldman DP, Kalsekar I, Sheehan JJ, Laubmeier K, Lakdawalla DN. Formulary restrictions on atypical antipsychotics: impact on costs for patients with schizophrenia and bipolar disorder in Medicaid. Am J Manag Care. 2014;20(2):e52–e60. | ||
Vogt WB, Joyce G, Xia J, Dirani R, Wan G, Goldman DP. Medicaid cost control measures aimed at second-generation antipsychotics led to less use of all antipsychotics. Health Aff (Millwood). 2011;30(12):2346–2354. | ||
Hogan TP, Awad AG, Eastwood MR. Early subjective response and prediction of outcome to neuroleptic drug therapy in schizophrenia. Can J Psychiatry. 1985;30(4):246–248. | ||
Awad AG, Hogan TP, Voruganti LN, Heslegrave RJ. Patients’ subjective experiences on antipsychotic medications: implications for outcome and quality of life. Int Clin Psychopharmacol. 1995;10(Suppl 3):123–132. | ||
Awad AG, Voruganti LN. Impact of atypical antipsychotics on quality of life in patients with schizophrenia. CNS Drugs. 2004;18(13):877–893. | ||
Voruganti LN, Awad AG. Subjective and behavioural consequences of striatal dopamine depletion in schizophrenia – findings from an in vivo SPECT study. Schizophr Res. 2006;88(1–3):179–186. | ||
Haddad PM, Sharma SG. Adverse effects of atypical antipsychotics: differential risk and clinical implications. CNS Drugs. 2007;21(11):911–936. | ||
Muench J, Hamer AM. Adverse effects of antipsychotic medications. Am Fam Physician. 2010;81(5):617–622. | ||
Centorrino F, Masters GA, Talamo A, Baldessarini RJ, Ongur D. Metabolic syndrome in psychiatrically hospitalized patients treated with antipsychotics and other psychotropics. Hum Psychopharmacol. 2012;27(5):521–526. | ||
Gentile S. Long-term treatment with atypical antipsychotics and the risk of weight gain: a literature analysis. Drug Saf. 2006;29(4):303–319. | ||
Bates JA, Whitehead R, Bolge SC, Kim E. Correlates of medication adherence among patients with bipolar disorder: results of the Bipolar Evaluation of Satisfaction and Tolerability (BEST) study: a nationwide cross-sectional survey. Prim Care Companion J Clin Psychiatry. 2010;12(5). | ||
Liu-Seifert H, Osuntokun OO, Godfrey JL, Feldman PD. Patient perspectives on antipsychotic treatments and their association with clinical outcomes. Patient Prefer Adherence. 2010;4:369–377. | ||
Altamura AC, Armadoros D, Jaeger M, Kernish R, Locklear J, Volz HP. Importance of open access to atypical antipsychotics for the treatment of schizophrenia and bipolar disorder: a European perspective. Curr Med Res Opin. 2008;24(8):2271–2282. | ||
Levin JB, Seifi N, Cassidy KA, et al. Comparing medication attitudes and reasons for medication nonadherence among three disparate groups of individuals with serious mental illness. J Nerv Ment Dis. 2014;202(11):769–773. | ||
Strejilevich S, Garcia Bonetto G. Subjective responses to pharmacological treatments in bipolar patients. J Affect Disord. 2003;77(2):191–192. | ||
Ventriglio A, Gentile A, Baldessarini RJ, et al. Improvements in metabolic abnormalities among overweight schizophrenia and bipolar disorder patients. Eur Psychiatry. 2014;29(7):402–407. | ||
Fagiolini A, Brugnoli R, Di Sciascio G, De Filippis S, Maina G. Switching antipsychotic medication to aripiprazole: position paper by a panel of Italian psychiatrists. Expert Opin Pharmacother. 2015;16(5):727–737. | ||
Goldberg JF, Freeman MP, Balon R, et al. The American Society of Clinical Psychopharmacology survey of psychopharmacologists’ practice patterns for the treatment of mood disorders. Depress Anxiety. 2015;32(8):605–613. | ||
Llorca PM, Abbar M, Courtet P, Guillaume S, Lancrenon S, Samalin L. Guidelines for the use and management of long-acting injectable antipsychotics in serious mental illness. BMC Psychiatry. 2013;13:340. | ||
Harvey NS. The development and descriptive use of the Lithium Attitudes Questionnaire. J Affect Disord. 1991;22(4):211–219. | ||
Scott J, Pope M. Nonadherence with mood stabilizers: prevalence and predictors. J Clin Psychiatry. 2002;63(5):384–390. | ||
Awad AG. Subjective response to neuroleptics in schizophrenia. Schizophr Bull. 1993;19(3):609–618. | ||
Weiden P, Rapkin B, Mott T, et al. Rating of medication influences (ROMI) scale in schizophrenia. Schizophr Bull. 1994;20(2):297–310. | ||
Rofail D, Gray R, Gournay K. The development and internal consistency of the satisfaction with Antipsychotic Medication Scale. Psychol Med. 2005;35(7):1063–1072. | ||
Hogan TP, Awad AG. Drug attitude inventory. In: Rush A, editor. Handbook of Psychiatric Measures. Arlington, VA: American Psychiatric Association Publishing; 2000. | ||
Teter CJ, Falone AE, Bakaian AM, Tu C, Ongur D, Weiss RD. Medication adherence and attitudes in patients with bipolar disorder and current versus past substance use disorder. Psychiatry Res. 2011;190(2–3):253–258. | ||
Sajatovic M, Levin J, Fuentes-Casiano E, Cassidy KA, Tatsuoka C, Jenkins JH. Illness experience and reasons for nonadherence among individuals with bipolar disorder who are poorly adherent with medication. Compr Psychiatry. 2011;52(3):280–287. | ||
Sajatovic M, Levin J, Tatsuoka C, et al. Six-month outcomes of customized adherence enhancement (CAE) therapy in bipolar disorder. Bipolar Disord. 2012;14(3):291–300. | ||
Levin JB, Tatsuoka C, Cassidy KA, Aebi ME, Sajatovic M. Trajectories of medication attitudes and adherence behavior change in non-adherent bipolar patients. Compr Psychiatry. 2015;58:29–36. | ||
Chang CW, Sajatovic M, Tatsuoka C. Correlates of attitudes towards mood stabilizers in individuals with bipolar disorder. Bipolar Disord. 2015;17(1):106–112. | ||
Grover S, Chakrabarti S, Sharma A, Tyagi S. Attitudes toward psychotropic medications among patients with chronic psychiatric disorders and their family caregivers. J Neurosci Rural Pract. 2014;5(4):374–383. | ||
Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet. 2013;382(9896):951–962. | ||
Walpoth-Niederwanger M, Kemmler G, Grunze H, et al. Treatment patterns in inpatients with bipolar disorder at a psychiatric university hospital over a 9-year period: focus on mood stabilizers. Int Clin Psychopharmacol. 2012;27(5):256–266. | ||
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. | ||
Tong A, Flemming K, McInnes E, Oliver S, Craig J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med Res Methodol. 2012;12:181. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.