")
Back to Journals » International Journal of General Medicine » Volume 15
Atrial Septal Defect Repair in Adolescent and Adult Patients, a Cross Sectional Study at Jordan University Hospital, a Tertiary Hospital in a Developing Country
Authors Bani Hani A , Salhiyyah K, Salameh M , Abu Abeeleh M, Al Smady M, Al Rawashdeh M, Abu Fares H, Al- Ammouri I
Received 13 January 2022
Accepted for publication 8 March 2022
Published 30 March 2022 Volume 2022:15 Pages 3517—3524
DOI https://doi.org/10.2147/IJGM.S356502
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Amjad Bani Hani,1 Kareem Salhiyyah,2 Mohammad Salameh,1 Mahmoud Abu Abeeleh,1 Moaath Al Smady,1 Mohammad Al Rawashdeh,3 Hala Abu Fares,3 Iyad Al- Ammouri3
1Department of General Surgery, Division of Cardiac Surgery, The University of Jordan, Amman, Jordan; 2Department of Cardiac Science, Middle East University, Amman, Jordan; 3Department of Pediatrics, Division of Pediatric Cardiology, The University of Jordan, Amman, Jordan
Correspondence: Amjad Bani Hani, Email [email protected]
Objective: We aim to report our heart team’s experience in repair of Secundum atrial septal defect (ASD) in adolescent and adult patients at Jordan University Hospital (JUH).
Methodology: A retrospective observational study of 44 patients who underwent secundum ASD closure by transcatheter closure (TCC) or Minimally Invasive Cardiac Surgery (MICS) at JUH. Patients who were treated at an age of 14 years or older regardless of the age of diagnosis were included. SPSS and Microsoft Excel were used to analyze the data.
Results: A total of 44 patients with secundum ASD were treated during the period of (January 2015 and December 2019). The mean age was 34.1 (± 14.3) years. Thirty-four patients underwent TCC, 9 underwent surgical closure and one had a hybrid procedure. We had no mortality and 2 minor morbidities. After a mean follow-up period of 13.2-/+13.6 months, most patients experienced improved symptoms, and there was a significant reduction of right ventricular dimension from 33.1 (± 8.74) to 24 (± 4.67) mm (p=0.0001).
Conclusion: ASD closure whether TCC or MICS is a safe procedure with very low morbidity. A heart team approach is a necessity in the era of advances in both MICS surgery and TCC approach. A heart team provides the patients with a variety of safe and cosmetic solutions that allow the patients to have a fast management and recovery phase in rapid time through providing the merits and avoiding the complications of each modality, the team allows low volume centers in developing countries to achieve an excellent outcome.
Keywords: atrial septal defect, ASD closure, heart team
Introduction
The incidence of congenital heart disease (CHD) is on the rise globally.1 Atrial Septal defect (ASD) is the second most common anomaly occurring in approximately 1.64 per 1000 live births (17.5% of all congenital heart diseases).1 Nearly 70% of all Atrial septal defects are of the secundum subtype. This is a sporadic incidence.2 It is usually asymptomatic during infancy and childhood and diagnosed incidentally. Most patients are expected to survive into adulthood when they become more symptomatic.3–5
The treatment of Secundum ASD has evolved over the last 2 decades. First, the surgical outcome of ASD repair through the classical median sternotomy (MS) approach has improved significantly becoming one of the safest operations,6,7 meanwhile two attractive strategies have been developed: minimally invasive cardiac surgery (MICS), and transcatheter occlusion devices (TCC). Both offer excellent clinical outcomes, and rapid recovery. This necessitated the development of a team that treats the patient in the best available manner.
Jordan, a middle income developing country has a high incidence of congenital heart diseases, particularly atrial septal defects with rates of about 12.3 and 2.5 cases per 1000 live births respectively.8 This puts high pressure on health care resources, especially in a developing country with limited resources. A new adolescent and adult Secundum ASD service was set up at our unit in 2017 to offer patients either MICS or TCC. Before the setup of the heart team service, the interventional cardiologist used to decide individually the therapeutic procedure of choice and refer the patients who need surgery for median sternotomy approach. This report describes our early experience in setting up this service using a heart team approach to facilitate decision making and ensure the best clinical outcome.
Materials and Methods
A retrospective analysis was performed for all the adolescent and adult patients (over 14-year- old) who underwent secundum ASD repair either TCC or MICS at our institute (JUH) after reforming the ASD services between (January 2017 to December 2019).
Data collected including preoperative demographics, intraoperative variables, and postoperative outcomes.
The heart team reviewed each case and joint decisions were made regarding the optimal treatment strategy. All patients underwent trans-esophageal echocardiography. The suitability of TCC of the secundum ASD was based on the following criteria, maximum defect size, presence of multiple defects, aneurysmal septum, and careful evaluation of the defect rims. Rims evaluated included superior, aortic, atrioventricular valve, inferior, and posterior rims. Appropriate rims were defined as >5 mm.9 With exception of deficient or absent aortic rim, transcatheter closure was not done if any other rim was deficient.
Techniques
Transcatheter ASD Closure (TCC)
The technique of ASD closure using double disc devices is extensively described in the literature.10 Device closure was done using a self-centering device in most cases, or a patent foramen ovale (PFO) occluder in selected cases (such as in multiple small defects, or presence of aneurysmal septum). The procedure is done with general anesthesia and trans-esophageal echocardiographic guidance. The selection of the device type and size depended on the anatomical features of the defect, including the maximum diameter of the defect, length of the rims, and the presence of single or multiple defects. The size of the self-centering device was selected to be 3–5 mm larger than the maximum diameter of the defect. The size of the PFO occluder device was selected so that the device would cover all the defects in case of multiple defects, or be sufficient to cover the dimension of the aneurysm in cases of aneurysmal atrial septum.
In large defects, or defects with deficient aortic rim, a number of techniques were used to assist deployment of occluder device and avoidance of prolapse of left atrial disc during deployment. In some patients, simple rapid deployment with counterclockwise tension was successful, in others, left or right upper pulmonary vein technique, or left atrial appendage techniques, where the left atrial disc is deployed first in the pulmonary vein or the atrial appendage, followed by rapid deployment of the right atrial disc resulted in successful delivery.
Minimally Invasive Surgical Technique (MICS)
Patients were operated on in a supine position with the right side elevated. A venous cannula (15F) was then inserted percutaneously through the right internal jugular vein using Seldinger technique. In all cases, cardiopulmonary bypass was instituted via the femoral vessels. A limited 5-cm skin incision was then made under the right nipple in men and the right inframammary groove in women. A video assisted working-port was made in the fourth intercostal space and the thoracic cage was embedded with CO2. The inferior venous cannula was positioned in the right atrium under transesophageal echocardiography guidance. The arterial cannulation (19–23F) was inserted using the same technique, both Caval veins were snared. External aortic cross clamp was applied. The right atrium was opened through a longitudinal incision. All defects were closed using Autologous Pericardium.
Data Analysis
Data were analyzed using SPSS software (version 20, Chicago, USA) and Microsoft Excel (version 365, Microsoft, California, USA). Continuous data were presented as mean, standard deviation, median and interquartile range (IQR), and were compared Student's t-test, Categorical data were expressed as percentages.
Results
Preoperative
During the study period, a total of 44 patients with Secundum ASD were treated by the heart team. The mean age was 34.1 (±14.3) years, range (13–64), 17 (39%) were males and 27 (61%) were females. Table 1 summarizes preoperative characteristics. Most patients were symptomatic 36 patients (85%) . The commonest symptoms were palpitation in 19 patients (45%), easy fatigability in 18 patients (42%), and chest pain in 11 patients (26%).
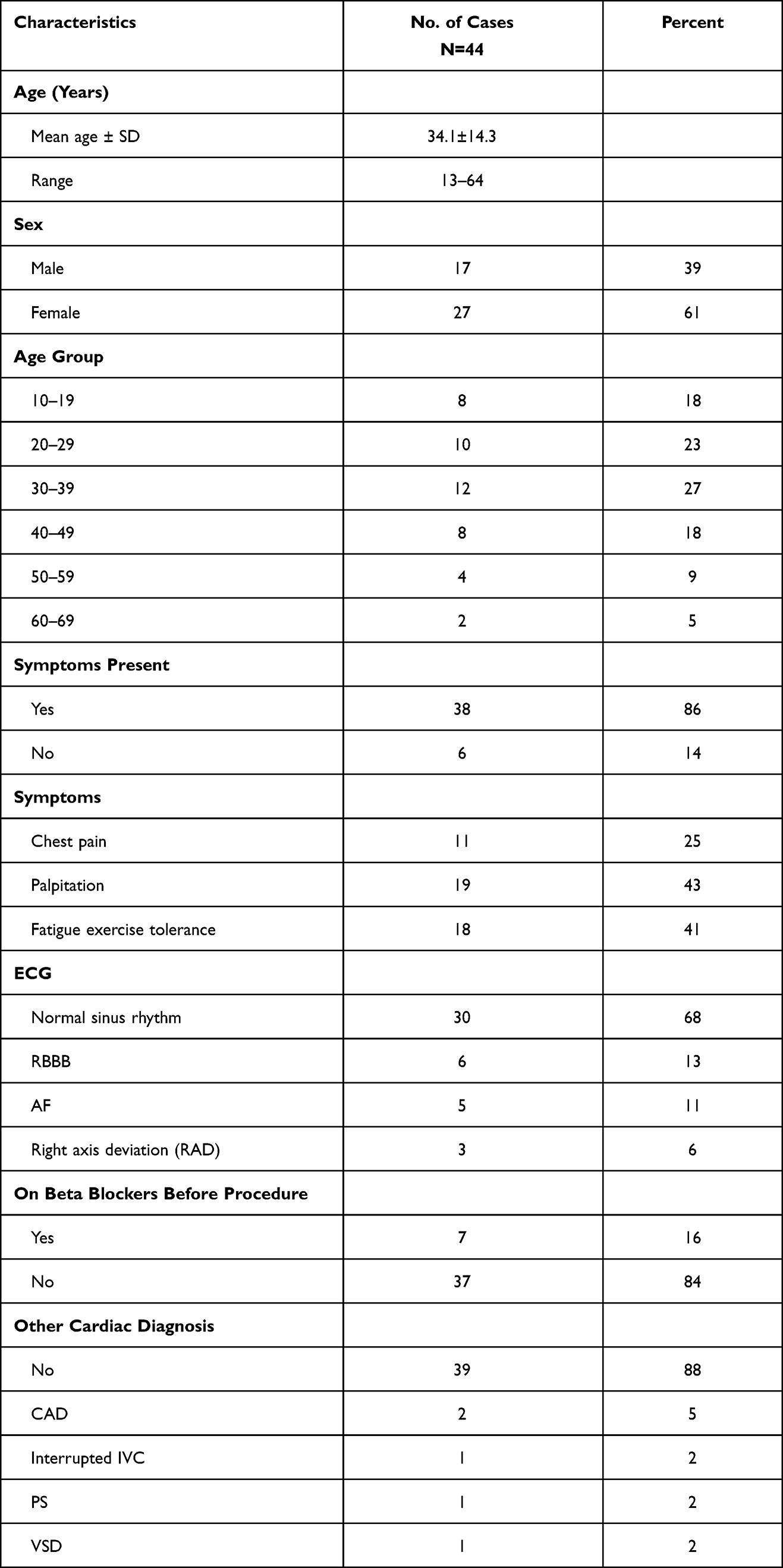 |
Table 1 Preoperative Patient Characteristics |
Atrial fibrillation was present in 5 patients (12.8%). Mean right ventricular dimension was 33.1 mm (±8.74). The mean defect size was 20.4 mm (± 9.5). Rim deficiency was present in 14 (33%) patients: Eight with deficient aortic rim, four posterior rim, and two inferior rim.
Other associated cardiac abnormalities were: coronary artery disease (CAD) in 2 patients (5.1%), interrupted inferior vena cava (IVC), pulmonary stenosis (PS) in one patient and ventricular septal defect (VSD) in one patient (2.6% each).
Operative
Thirty-four patients (77%) underwent TCC, 9 patients (20%) underwent surgical closure including one with hybrid surgery, and one patient had emergency surgery.
Trans-esophageal echocardiography guidance was done during the procedure. All patients had left to right shunt documented by color Doppler. Hemodynamic catheterization was done with measurement of the right ventricular (RV) pressure. Mean RV pressure was 30.6 (+-8.6). No patient had severe pulmonary hypertension to preclude closure. Calculations of shunting or Qp:Qs ratio was not routinely done. Devices used were self- centering device in 27 with a mean device size of 25.3± 9 mm, and PFO occluder in 7. Total devices used were 35 devices (34 TCC, and one Hybrid device closure using a 33 mm occlutech ASD occluder).
Devices used were Occlutech Figula Flex device (Occlutech, La CoursGata 2, Helsingborg, Sweden) 31, and Amplatzer septal occluders (Abbott. Abbott Park, Illinois, USA) in 4 Table 2.
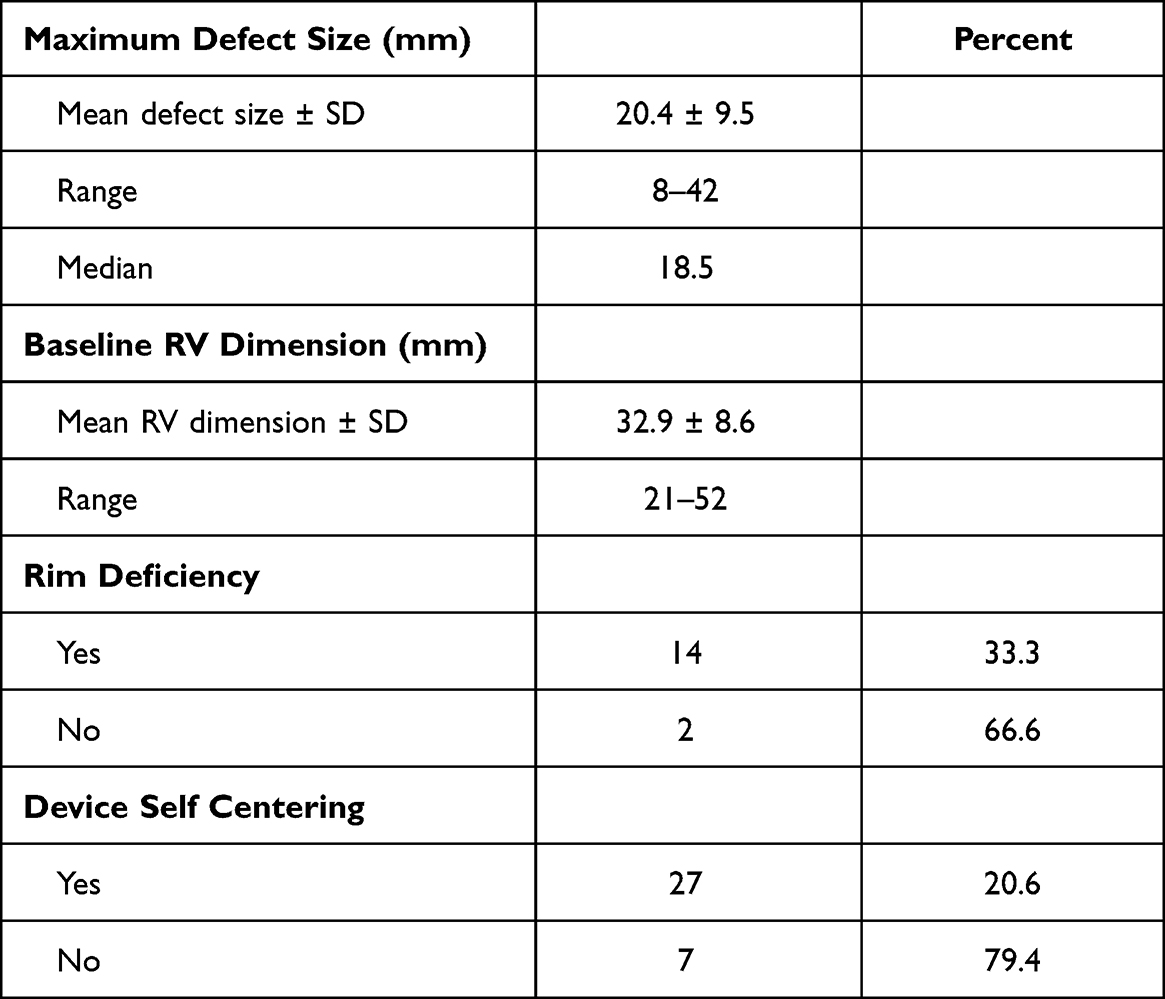 |
Table 2 Defect and Device Characteristics |
In one patient, there was device embolization, the patient was offered surgery from the beginning due to a large defect with suspicion of a small inferior rim. The Heart Team anticipated the possibility of device dislodgment but upon patient’s request TCC was performed and the device dislodged, he was operated upon promptly without any complications, confirmation of deficient inferior rim was done intra-operatively, this case was early in our experience with minimally invasive cardiovascular surgery therefore he was operated through standard median sternotomy.
Nine patients underwent surgical closure: eight of the patients with deficient inferior or posterior rims underwent primary surgical closure, and one underwent emergency closure following device embolization as mentioned above, where the diagnosis of deficient inferior rim was confirmed intra-operatively. In addition, patients who underwent primary surgical procedure due to deficient rims by echocardiography were confirmed to have deficient rims intra-operatively.
One patient underwent Hybrid device-closure of the defect due to interrupted inferior vena cava. A per-atrial puncture was done through a small lateral mini-thoracotomy in the 4th intercostal space. A delivery sheath was then inserted into the right atrium, then to the left atrium under trans-esophageal echocardiography guidance. Without using the Heart lung machine, we successfully deployed the occluder device (Bani Hani et al, 2020).
Postoperative
Most of our patients faced a smooth in hospital stay with a fast recovery postoperatively. We faced two minor morbidities; one of our patients developed a small right groin hematoma and soft palate hematoma due to trans-oesophageal echo probe that were managed conservatively. Another patient developed atrial fibrillation with rapid ventricular response after the TCC closure of the defect, controlled via chemical cardioversion. The major morbidity was to the patient with device embolization and was managed by emergent sternotomy and ASD repair with a pericardial patch.
Follow Up
The mean follow up period was 13.2-/+13.6 months (range 1–47) till the last follow up. All symptomatic patients reported subjective improvement of their symptoms, particularly exercise tolerance. No objective measure of exercise tolerance was done to confirm the finding. Additionally, patients who complained of palpitation before procedure reported improved symptom. However, of the 5 patients with AF, 4 remained in AF despite closure of defect.
The right ventricular dimension regressed from 33.1 ± 8.6 mm to 24.1 ± 4.5 mm (p=0.0001). A small residual shunt was present in 2 patients (5.1%) which were treated conservatively Table 3.
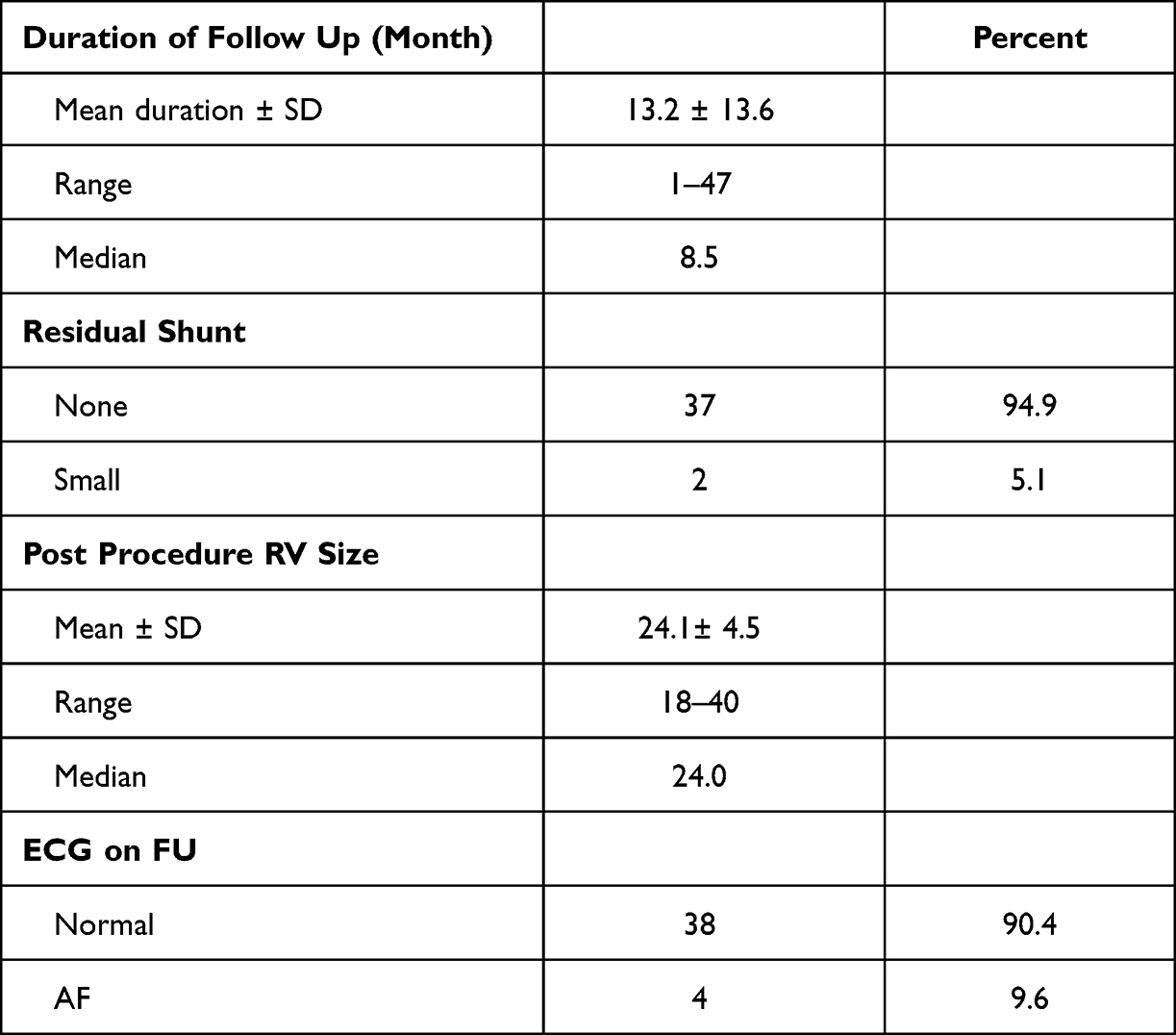 |
Table 3 Follow Up |
Discussion
Treatment of secundum ASD has seen significant changes over the past 2 decades MICS was introduced as an alternative to surgical repair through SMS and showed superior clinical and cosmetic results with earlier hospital discharge, and lower rates of surgical site infection and return to work.6,7,11,12
The other technical development was success of the TCC devices, first introduced in Japan in 2005. TCC was then approved for adult patients in 2011, before that it was only available for pediatric patients.13 TCC showed its superiority over the surgical approach of closing Secundum ASD.10,13
As these new technologies become widely available, few issues have risen; first the treatment decision making; not all cases could be treated with device closure, and some will still need surgery, second, the adoption of new techniques needs a learning curve for safe implementation, and third, the organizational arrangements for offering these procedures, for example, the need for surgical backup cover, provision of the other congenital services, and the case load recommended.
Success of TCC of secundum ASD depends mainly on two factors: Maximum size of the defect not exceeding 38–40 mm, and the presence of adequate rims (generally >5m)3. However, aortic rim deficiency is the only rim that is not necessary for successful device placement.
Several studies have compared standard surgical closure with percutaneous closure, they showed that both TCC and MICS are successful with no mortality,14–16 yet lower rates of complications and shorter hospital stay with transcatheter approach. Complications are mainly due to the lateral thoracotomy such as (right pleural effusion, right pneumothorax, and atelectasis of the right lung) in addition higher rates of atrial arrhythmias.13,14 On the other hand, some of the complications that might arise due to TCC of ASD are reported including cardiac erosion (incidence of 0.1–0.3%),17 device thromboembolism (incidence of 0.55% in the Amplatzer device proctors survey, mostly due to under sizing of the device and inadequate rims)18 and nickel allergy.13,19
In 2017, we had major reform to the Secundum ASD services at our hospital. Our surgical department covered adult service only with no congenital services. Pediatric cardiology offered a wide range of diagnostic services and interventional procedures that did not require surgical input. This included some highly selected secundum ASD transcatheter closure cases. With the service reform, MICS secundum ASD repair was introduced for cases which are not suitable for catheter intervention, and as surgical backup for more complex device closures. To ensure safety and efficiency of the new service, a heart team approach was adopted. The team included pediatric cardiologist, interventional pediatric cardiologist, cardiac anesthesiologist, and a cardiac surgeon specialised in minimally invasive cardiac surgery. The heart team made joint decisions about treatment options, and cross cover patient care and management.
Team concept is not a new concept in the medical field, it has been implemented in different specialties such as oncology and organ transplant19 Team based approach in cardiac field has garnered increasing interest after two achievements in the cardiovascular field, the Syntax score and the transcatheter aortic valve implantation.20
Multidisciplinary heart Team manages complex patient issues and gives complementary approach to patient care by joint decision of different medical specialties. By reviewing multiple options available and sharing them with patient and their family we can offer the best shared decision making and recommendations tailored to patient preference. It can encourage participation and commitment to excellence, and further drive innovation.19,21
This study shows our early experience in ASD service with excellent clinical outcome. There was no mortality, and low morbidity in both MICS and TCC groups. Medium term follow up showed significant improvement of symptoms, and reverse remodeling to the right ventricular dimensions. Heart rhythm has also improved. Aortic rim was the most common rim to be deficient in our cohort (20%). It is reported in other studies to be deficient in up to 40% of cases.9 All patients with deficient aortic rim in our cohort were successfully treated by device closure, the two discs of device are placed in a way that they hug the aortic root. Defects with deficient posterior or inferior rims are considered by most operators to be un-suitable for device closure, therefore they are best treated surgically, preferably using MICS.22
Heart team approach has proven essential in providing best care, and safeguard outcome in complex case. The size of the atrial septal defect and the rims are major points that decided the way of management, 6 of our patients were offered surgery from the beginning due to absent rim, one was large defect with suspicion of small inferior rim. Heart Team anticipated the possibility of device dislodgment but upon patient’s request transcatheter closure was performed and the device dislodged, he was taken promptly to surgery and operated without any complications, confirmation of deficient inferior rim was done intra-operatively, this was in our early experience with MICS therefore he was operated in standard median sternotomy. In another case for a patient with absent inferior vena cava we performed a hybrid minimally invasive procedure in which through a small lateral minithoracotomy in the 4th intercostal space we introduced a sheath into the right atrium. Without using the Heart lung machine, we successfully deployed the occluder device.23
Heart team fills the knowledge gap that might arise between different subspecialties, also it decreases unnecessary procedures. In general, the team physicians share the burden, and this might potentially minimize medical malpractice exposure, because there is a shared responsibility of recommending the most optimal therapy to the patient.19
We managed all our cases despite being allow volume center with limited resources in a developing country, we did not have to refer any case and we were able through the team approach to solve all unusual cases that we do not frequently encounter such as the absent inferior vena cava case.
Our observational study has a few important limitations including limited sample size, single- center data, and differences in follow-up duration.
Conclusion
ASD closure whether TCC or MICS is a safe procedure with very low morbidity. Heart Team approach is a necessity in the era of advances in Both MICS and TCC approach, A Heart team provides the patients with a variety of safe and cosmetic solutions that allows the patients to have a fast management and recovery phase in rapid time through providing the merits and avoiding the complications of each modality, the team allows low volume centers in developing countries to achieve excellent outcome.
Data Sharing Statement
All data are available with the corresponding author upon request.
All data is confident and no one allowed to disclose it apart from the research team.
Ethical Approval
The study was approved by the Institutional Review Board (IRB)Committee of the Jordan University Hospital under the registration number 67/2020/2114.
The consent to review the medical records is not required by the IRB committee.
Our IRB committee is compliant with declaration of Helsinki terms.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors declare no competing interest in this work.
References
1. Van Der Linde D, Konings EEM, Slager MA, et al. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol. 2011;58(21):2241–2247. doi:10.1016/j.jacc.2011.08.025
2. Helgason H, Jonsdottir G. Spontaneous closure of atrial septal defects. Pediatr Cardiol. 1999;20(3):195–199. doi:10.1007/s002469900439
3. Akagi T. Current concept of transcatheter closure of atrial septal defect in adults. J Cardiol. 2015;65(1):17–25. doi:10.1016/j.jjcc.2014.09.002
4. Suchon E, Pieculewicz M, Tracz W, Przewłocki T, Sadowski J, Podolec P. Transcatheter closure as an alternative and equivalent method to the surgical treatment of atrial septal defect in adults: comparison of early and late results. Med Sci Monit. 2009;15(12):612–617.
5. Moons P, Bovijn L, Budts W, Belmans A, Gewillig M. Temporal trends in survival to adulthood among patients born with congenital heart disease from 1970 to 1992 in Belgium. Circulation. 2010;122(22):2264–2272. doi:10.1161/CIRCULATIONAHA.110.946343
6. Yaliniz H, Topcuoglu MS, Gocen U, et al. Comparison between minimal right vertical infra-axillary thoracotomy and standard median sternotomy for repair of atrial septal defects. Asian J Surg. 2015;38(4):199–204. doi:10.1016/j.asjsur.2015.01.008
7. Yi K, Guo X, You T, et al. Standard median sternotomy, right minithoracotomy, totally thoracoscopic surgery, percutaneous closure, and transthoracic closure for atrial septal defects in children: a protocol for a network meta-analysis. Med (United States). 2019;98(38):0–3. doi:10.1097/MD.0000000000017270
8. Al-Ammouri I, Ayoub F. Heart disease in Syrian refugee children: experience at Jordan University Hospital. Ann Glob Health. 2016;82(2):300–306. doi:10.1016/j.aogh.2015.02.517
9. Vaidyanathan B, Simpson JM, Kumar RK. Transesophageal echocardiography for device closure of atrial septal defects. Case selection, planning, and procedural guidance. JACC Cardiovasc Imaging. 2009;2(10):1238–1242. doi:10.1016/j.jcmg.2009.08.003
10. Yang MC, Wu JR. Recent review of transcatheter closure of atrial septal defect. Kaohsiung J Med Sci. 2018;34(7):363–369. doi:10.1016/j.kjms.2018.05.001
11. Raslan S, Sharaa M, Refaie M, Ali WDK, Elhenawy AM. Outcome variables of right anterolateral mini-thoracotomy versus complete sternotomy in atrial septal defect closure: a randomized controlled trial. J Egypt Soc Cardio Thorac Surg. 2017;25(2):121–127. doi:10.1016/j.jescts.2017.03.004
12. Vistarini N, Aiello M, Mattiucci G, et al. Port-access minimally invasive surgery for atrial septal defects: a 10-year single-center experience in 166 patients. J Thorac Cardiovasc Surg. 2010;139(1):139–145. doi:10.1016/j.jtcvs.2009.07.022
13. Kodaira M, Kawamura A, Okamoto K, et al. Comparison of clinical outcomes after transcatheter vs minimally invasive cardiac surgery closure for atrial septal defect. Circ J. 2017;81(4):543–551. doi:10.1253/circj.CJ-16-0904
14. Butera G, Biondi-Zoccai G, Sangiorgi G, et al. Percutaneous versus surgical closure of secundum atrial septal defects: a systematic review and meta-analysis of currently available clinical evidence. EuroIntervention. 2011;7(3):377–385. doi:10.4244/EIJV7I3A63
15. Formigari R, Di Donato RM, Mazzera E, et al. Minimally invasive or interventional repair of atrial septal defects in children: experience in 171 cases and comparison with conventional strategies. J Am Coll Cardiol. 2001;37(6):1707–1712. doi:10.1016/s0735-1097(01)01213-x
16. Butera G, Carminati M, Chessa M, et al. Percutaneous versus surgical closure of secundum atrial septal defect: comparison of early results and complications. Am Heart J. 2006;151(1):228–234. doi:10.1016/j.ahj.2005.02.051
17. Crawford GB, Brindis RG, Krucoff MW, Mansalis BP, Carroll JD. Percutaneous atrial Septal Occluder devices and cardiac erosion: a review of the literature. Catheter Cardiovasc Interv. 2012;80(2):157–167. doi:10.1002/ccd.24347
18. Engelman RM, Engelman DT. Strategies and devices to minimize stroke in adult cardiac surgery. Semin Thorac Cardiovasc Surg. 2015;27(1):24–29. doi:10.1053/j.semtcvs.2015.03.001
19. Head SJ, Kaul S, MacK MJ, et al. The rationale for heart team decision-making for patients with stable, complex coronary artery disease. Eur Heart J. 2013;34(32):1–11. doi:10.1093/eurheartj/eht059
20. Cinteza M. Heart team: who is the captain? Maedica (Buchar). 2016;11(3):183–185.
21. Fleming M, Smith S, Slaunwhite J, Sullivan J. Investigating interpersonal competencies of cardiac surgery teams. Can J Surg. 2006;49(1):22–30.
22. Amedro P, Bayburt S, Assaidi A, et al. Should transcatheter closure of atrial septal defects with inferior-posterior deficient rim still be attempted? J Thorac Dis. 2019;11(3):708–716. doi:10.21037/jtd.2019.02.89
23. Bani Hani A, Abdullattif M, AL-Ammouri I. Hybrid closure of a large atrial septal defect using Occlutech Flex II septal occluder in a patient with interrupted inferior caval vein. Cardiol Young. 2020;1–3. doi:10.1017/S104795112000092X
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.