")
Back to Journals » International Journal of General Medicine » Volume 12
Atrial Fibrillation Post Coronary Artery Graft Surgery: A Review Of Literature
Authors Jannati M
Received 19 August 2019
Accepted for publication 30 September 2019
Published 7 November 2019 Volume 2019:12 Pages 415—420
DOI https://doi.org/10.2147/IJGM.S227761
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mansour Jannati
Cardiovascular Surgery Ward, Shiraz University of Medical Sciences, Shiraz, Iran
Correspondence: Mansour Jannati
Cardiovascular Surgery Ward, Shiraz University of Medical Sciences, Central Building of Shiraz University of Medical Sciences, Zand Street, Shiraz, Iran
Tel + 989171122759 Email [email protected]
Abstract: Atrial fibrillation (AF) is a failure that is observed in heart disease and is also known to be the most common heart rhythm disturbance post coronary artery bypass surgery. Although AF is considered a transient problem, it is usually accompanied with a variety of complications and morbidity for patients and may result in death. In the present study, pre- and post-operative considerable factors which may increase the risk and mortality of AF, and possible treatments have been concisely reviewed.
Keywords: atrial fibrillation, cardiac surgery, mortality, risk factor, prophylaxis
Introduction
Atrial fibrillation (AF) is a failure that is observed in heart diseases such as rheumatic and ischemic, as well as thyrotoxicosis and hypertension,1–3 and it is also known to be the most common heart rhythm disturbance post coronary artery bypass surgery (CABS).4 The incidence probability of AF is controversial; for example, of 700 000 patients who undergo open cardiac surgery in the US annually,5 11%–40% have AF.6 Also, based on the results obtained with continuous electrocardiographic monitoring, the incidence range of postoperative AF has been reported to be 25%–40%, and up to 62% after a coronary artery bypass surgery or combined coronary artery bypass surgery and valve procedure.4,7,8 On the other hand, according to the report of the Cleveland Clinic Foundation the prevalence of preoperative electrocardiogram AF incidence ws very low (0.96%).9 Nonetheless, AF still exists and its incidence has not decreased, in spite of the advancement of surgery, anesthesia and care methods post surgery.10,11
Although AF is often benign and transient, various factors, including prolonged length of stay, intensive care unit readmission, a greater need for reintubation, persistent congestive heart failure, stroke, and increased overall costs, have been recognized as associated with postoperative AF.12–16 Typical conditions associated with the serious complications of AF include hemodynamic disorders, hypotension caused by the rapid ventricular response, myocardial infarction, cerebral apoplexy, increased length of hospitalization, and death.17–22
The etiology of AF does not indicate a specific factor and there are a number of factors which might lead to the incidence of AF. Potential factors that have been shown to play a role in the creation of atrial susceptibility to AF include: pericarditis, atrial injury from surgical handling or cannulation, atrial suture lines, acute atrial enlargement from pressure or volume overload, inadequate myocardial protection during cardiopulmonary bypass, atrial ischemia, long bypass and aortic cross-clamp times, hyperadrenergic states (such as the use of postoperative inotropic medications), pulmonary complications, hypoxemia, inflammation,23,24 hypokalemia, and hypomagnesemia.25–27
Since the rate of AF incidence is considerably high and it could come with morbidities that annoy patients, it is a hot point of research in the field of cardiac science. Hence, in the present study we review some aspects of AF disorder after cardiac bypass surgery, including potential pre- and post-operative factors that might play a role in AF incidence, complications that arise with AF, risk of mortality, and management and treatment of AF such as prophylaxis procedures.
Pre-Operative And Post-Operative Considerations Of AF
An understanding of the preoperative factors concerned with the incidence of AF would be helpful to minimize morbidities followed by AF, or even to assist prevention. Although some patients develop AF after cardiac surgery without showing any apparent predisposing factors, most patients present at least one clinical predictor. The main preoperative factors which enhance the risk of AF incidence have been summarized in Table 1. These risk factors include increasing age,1,28–31 gender,32 previous history of AF, increased left atrial size or cardiomegaly, mitral valvular disease (particularly mitral stenosis), previous cardiac surgery, chronic obstructive pulmonary disease (COPD), low-intensity physical activity in the year prior to surgery, elevated preoperative hemoglobin A1c,26,33 obesity,34,35 and Caucasian race. Other factors which are as significant as the former include absence of beta-blocker or angiotensin converting enzyme inhibitor (ACE inhibitor), preoperative digoxin use,36 low-dose dopamine,37 higher preoperative plasma concentration of brain natriuretic peptide (BNP),1 severe right coronary artery stenosis, preoperative increase in P wave duration on surface (>116 msec)38 or on signal-averaged (> 140 msec) ECG.29,39
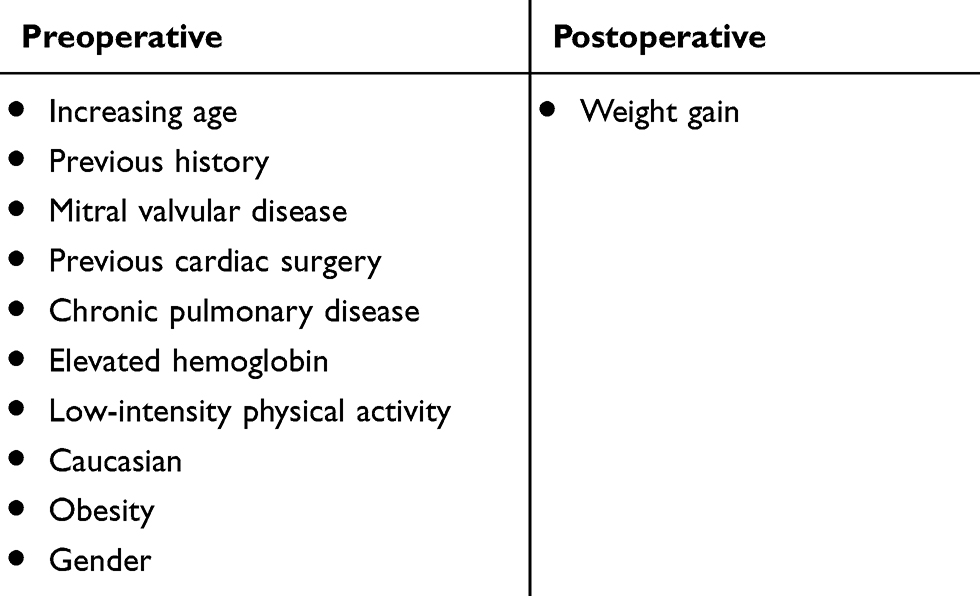 |
Table 1 Potential Pre- And Post-Operative Factors Which Increase The Risk Of AF Incidence |
Also, as potential predicting factors, time of onset (elapsed time), weight gain, fluid distribution, and recovered hematocrit were compared between control and experimental groups.32 In terms of elapsed time, it was shown that approximately 70% of patients experienced AF on either the third or fourth postoperative day. In terms of weight gain, 64% of patients gained between 2 and 8 pounds. By looking only at those patients who gained weight and excluding those who remained the same and those who lost weight, the percentage of weight gain rises to 72%. The results of the subject of fluid distribution showed that 66% of patients had a positive fluid balance which means patients gained more fluid than lost it. It might be regarding that 55% of patients with a positive fluid balance had 1000 mL, or more surplus, at the time of atrial arrhythmia. Concerning the hematocrit factor, 76% of patients with AF were able to recover a range of 70 –100% of their original erythrocyte count.32 Based on these results, excluding weight gain, fluid distribution and hematocrit recovery were similar between the two groups.
Mortality As A Result Of AF
Although age is one of the factors that increases the risk of AF incidence and AF seems to be more dominant among older people, using appropriate and applicable statistical methods for studying large population (such as Framingham study) has demonstrated that postoperative AF is associated with reduced survival, independent of age.40 AF incidence will be accompanied by morbidity and complications. According to the comparison between AF and non-AF patients, the length of hospital stay was demonstrated to be significantly longer in the AF group. Also, reports indicate a higher rate of early death and stroke in AF patients.12
Retrospective analysis on in-hospital outcomes of AF patients showed that these complications are not just excluded for myocardial infarction, but the probability of occurrence of other complications like stroke, respiratory failure, renal failure, hypotension requiring pressors, multisystem failure, shock, CP arrest, discharge on anticoagulants, and discharge on any antiarrhythmics was significantly higher in AF patients compared to non-AF groups.40
It has been shown that AF is associated with an increased risk of both early and late mortality. Albeit early death in the postoperative period dominates, late mortality is also shown to be statistically significant. This finding was more obvious after exclusion of early mortality cases from the analysis and was even further strengthened by consistent findings in a simultaneous case-matched population.40
It should be noted that the mechanism of each of short- and long-term mortality as a result of postoperative AF is not similar. In short term mortality, the main AF incidence mechanism is the loss of atrial transport function directly followed by hemodynamic compromise and congestive heart failure (CHF). On the other hand, in the long term mortality, there is no clear mechanistic link and the most probable include adverse drug effect, the occurrence of disabling stroke and embolic catastrophes.41
Management, Prevention, And Treatment
Postoperative AF is usually associated with a higher risk of stroke,42 thus, strategies for preventing stroke should be considered seriously in this setting. Also, clinicians need to pay careful attention to the risk of hemorrhage following surgery, especially when they are going to consider anticoagulation in patients who have not been actively cardioverted. For patients who have been recognized cardioverted within the first 48 h of AF diagnosis with no more recurrence of the arrhythmia, the anticoagulation treatment is not necessary.43
Regarding the high probability of AF after cardiac surgeries, prophylaxis treatment has been strongly recommended especially when there is a risk factor.44 Pieces of evidences have introduced class II β-blockers calcium channel controllers and also amiodarone (an antiarrhythmic drugs agent) as the effective prophylactic drug in controlling and reducing the risk of AF incidence after surgery.6,10 Although several different strategies have been studied to reduce the incidence of AF after cardiac surgery, here, we mainly focus on the role of ADDs and B-adrenergic blocking agents (BBs) because they are widely available and have been proven efficient. Overall advantage and disadvantages of amiodarone treatment, as a model of a therapeutic agent, have been presented in Table 2.
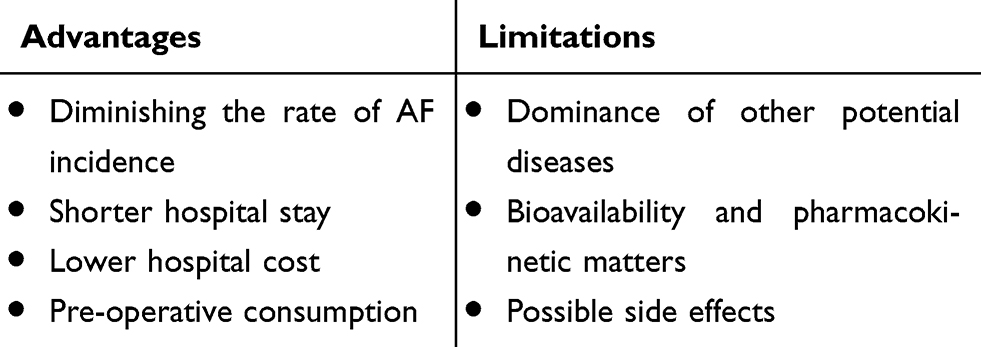 |
Table 2 Overall View Of The Advantages And Limitations Of Drug Treatment |
According to the 2006 American College of Cardiology guidelines, the American Heart Association, and the European Society of Cardiology for the management of AF, BBs was introduced as an impressive agent to prevent postoperative AF.45 The effectiveness of BBs in diminishing the risk of postoperative AF has been supported in a large body of evidence. Atenolol, metoprolol, timolol, propranolol, and carvedilol are among the most studied agents in the postoperative setting and significant differences have been observed in relative efficacy of each of these agents. Based on contemporary practices, BBs can lower the risk of postoperative AF by approximately 30%, which means despite treatment, many patients would still develop AF.42
Among antiarrhythmic agents, amiodarone and sotalol are known to be more safe and efficacious in diminishing the risk of postoperative AF. Sotalol requires daily monitoring during the first five doses. Also, sotalol is dominantly cleared renally, and its use is not feasible in patients with renal dysfunction. In addition, in patients with complications like severe left ventricular dysfunction or congestive heart failure, amiodarone can be the drug of choice.43 Comparative studies between amiodarone and placebo demonstrated that the initial treatment with amiodarone reduced the risk of postoperative AF compare with the placebo group. Also, amiodarone groups showed significantly shorter hospital stays and lower total hospital cost compared to the placebo group.46 In another study, treatment of amiodarone significantly reduced atrial tachyarrhythmias and the risk of sustained ventricular arrhythmias.47 In addition, it has been demonstrated that post-operative prophylaxis with intravenous infusion of amiodarone, followed by oral administration, significantly reduced the incidence of postoperative AF, total costs of care, length of intensive care unit and hospital stay.48,49 Even, oral doses of amiodarone are sufficient to control cardiac arrhythmia.50 It is worth noting that the possible difference in results between therapeutic treatments depends on dosage, duration of treatment, method of consumption (ie, injection, oral), cardiopulmonary bypass, and methods of stopping and continuing β-blocker consumption near surgery.50
However, in spite of the considerable positive outcomes of AADs in patients undergoing cardiac surgery, there are some significant clinical difficulties which limit the use of these agents. It is a fact that patients who undergo cardiac surgery usually have problems such as structural heart disease, coronary artery disease, or impaired left ventricular systolic function. Moreover, there are other factors which might impact bioavailability and pharmacokinetics of ADDs agents in the early postoperative period; factors such as drug–drug interactions, first-pass metabolism, alterations in absorption, protein binding, impairment of elimination pathways and volumes of distribution. For example, in the case of amiodarone, drug–drug interactions are a major concern and need more attention to be paid. The above-mentioned factors contribute to the arrhythmia risk associated with sodium and potassium channel blockers.43
Also, pre-operative amiodarone prophylaxis has been shown to be useful to prevent AF occurrence in high-risk patients.51 Oral consumption of amiodarone for a period of one week before surgery was stated to reduce AF manifestation by 50% and to decrease hospital cost and hospitalization duration by 25%.52 On the other hand, consumption of amiodarone may be accompanied by side effects including bradycardia, ventricle arrhythmia, cardio block, interstitial pneumonia, and liver poisoning. Although the exact mechanism of the drug effects on AF after surgery is not clearly known, its effect is postulated to be in relation with the combination of antiadrenergic and Class I and II antiarrhythmic effects.53 Overall effects of prophylactic methods on the term of hospitalization depend on the balance between decreasing the AF incidence, and as a result, decreasing the hospitalization duration on one hand, and increasing the side effects of the drug on the other hand.50
Conclusion
Atrial fibrillation is a prevalent consequence of coronary bypass surgery which results in complications and morbidity for patients. Mortality outcome of AF might be present both long- and short-term, each followed by a different mechanism. Pre-operative factors such as age, gender, ethnicity, previous history of AF, and obesity can increase the risk of AF incidence. Also, post-operative factors like weight gain might be helpful to predict the risk of AF occurrence and to provide adequate precautions and care. Moreover, prophylaxis treatments, especially with antiarrhythmic drugs (AAD) and B-adrenergic blocking agents (BBs), have been shown as the most effective and available treatments which decrease the risk of AF incidence as well as length and cost of hospitalization. Prophylaxis treatments need specific consideration, regarding each agent, and might be accompanied with limitations and side effects; e.g. sotalol is not recommended for patients with renal failure and drug–drug interaction is of concern in the case of amiodarone. Nonetheless, amiodarone has shown an inhibitory role against AF incidence and duration of hospitalization, even with oral administration and before surgery.
Acknowledgment
The author thanks all the participants, especially Sasan Afifi.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Pires LA, Wagshal AB, Lancey R, Huang SK. Arrhythmias and conduction disturbances after coronary artery bypass graft surgery: epidemiology, management, and prognosis. Am Heart J. 1995;129:799–808.
2. Mendes LA, Connelly GP, McKenney PA, et al. Right coronary artery stenosis: an independent predictor of atrial fibrillation after coronary artery bypass surgery. J Am Coll Cardiol. 1995;25:198–202. doi:10.1016/0735-1097(94)00329-o
3. Crosby LH, Pifalo WB, Woll KR, Burkholder JA. Risk factors for atrial fibrillation after coronary artery bypass grafting. Am J Cardiol. 1990;66:1520–1522.
4. Lauer MS, Eagle KA, Buckley MJ, DeSanctis RW. Atrial fibrillation following coronary artery bypass surgery. Prog Cardiovasc Dis. 1989;31:367–378. doi:10.1016/0033-0620(89)90031-5
5. Mason JW. Amiodarone. N Engl J Med. 1987;316:455–466. doi:10.1056/NEJM198702193160807
6. Faniel R, Schoenfeld P. Efficacy of i.v. amiodarone in converting rapid atrial fibrillation and flutter to sinus rhythm in intensive care patients. Eur Heart J. 1983;4:180–185.
7. Cox JL. A perspective of postoperative atrial fibrillation in cardiac operations. Ann Thorac Surg. 1993;56:405–409. doi:10.1016/0003-4975(93)90871-e
8. Vecht RJ, Nicolaides EP, Ikweuke JK, Liassides C, Cleary J, Cooper WB. Incidence and prevention of supraventricular tachyarrhythmias after coronary bypass surgery. Int J Cardiol. 1986;13:125–134. doi:10.1016/0167-5273(86)90137-3
9. Quader MA, McCarthy PM, Gillinov AM, et al. Does preoperative atrial fibrillation reduce survival after coronary artery bypass grafting? Ann Thorac Surg. 2004;77:1514–1522. discussion 22-4. doi:10.1016/j.athoracsur.2003.09.069
10. Alboni P, Shantha N, Pirani R, et al. Effects of amiodarone on supraventricular tachycardia involving bypass tracts. Am J Cardiol. 1984;53:93–98. doi:10.1016/0002-9149(84)90690-8
11. Kojuri J, Mahmoodi Y, Jannati M, Shafa M, Ghazinoor M, Sharifkazemi MB. Ability of amiodarone and propranolol alone or in combination to prevent post-coronary bypass atrial fibrillation. Cardiovasc Ther. 2009;27:253–258. doi:10.1111/j.1755-5922.2009.00100.x
12. Tamis JE, Steinberg JS. Atrial fibrillation independently prolongs hospital stay after coronary artery bypass surgery. Clin Cardiol. 2000;23:155–159. doi:10.1002/clc.4960230305
13. Abreu JE, Reilly J, Salzano RP, Khachane VB, Jekel JF, Clyne CA. Comparison of frequencies of atrial fibrillation after coronary artery bypass grafting with and without the use of cardiopulmonary bypass. Am J Cardiol. 1999;83:775–6,A9. doi:10.1016/S0002-9149(98)00988-6
14. Almassi GH, Schowalter T, Nicolosi AC, et al. Atrial fibrillation after cardiac surgery: a major morbid event? Ann Surg. 1997;226:501–511. discussion 11-3. doi:10.1097/00000658-199710000-00011
15. Creswell LL, Schuessler RB, Rosenbloom M, Cox JL. Hazards of postoperative atrial arrhythmias. Ann Thorac Surg. 1993;56:539–549. doi:10.1016/0003-4975(93)90894-n
16. Weintraub WS, Jones EL, Craver J, Guyton R, Cohen C. Determinants of prolonged length of hospital stay after coronary bypass surgery. Circulation. 1989;80:276–284. doi:10.1161/01.cir.80.2.276
17. Galloway AC, Shemin RJ, Glower DD, et al. First report of the port access international registry. Ann Thorac Surg. 1999;67:51–56. discussion 7-8. doi:10.1016/s0003-4975(98)01265-x
18. Dimmer C, Tavernier R, Gjorgov N, Van Nooten G, Clement DL, Jordaens L. Variations of autonomic tone preceding onset of atrial fibrillation after coronary artery bypass grafting. Am J Cardiol. 1998;82:22–25. doi:10.1016/s0002-9149(98)00231-8
19. Borzak S, Tisdale JE, Amin NB, et al. Atrial fibrillation after bypass surgery: does the arrhythmia or the characteristics of the patients prolong hospital stay? Chest. 1998;113:1489–1491. doi:10.1378/chest.113.6.1489
20. Stafford PJ, Kolvekar S, Cooper J, et al. Signal averaged P wave compared with standard electrocardiography or echocardiography for prediction of atrial fibrillation after coronary bypass grafting. Heart. 1997;77:417–422. doi:10.1136/hrt.77.5.417
21. Zipes DP. Braunwald’s Heart Disease: a Textbook of Cardiovascular Medicine. W.B. Saunders; 2005.
22. Redle JD, Khurana S, Marzan R, et al. Prophylactic oral amiodarone compared with placebo for prevention of atrial fibrillation after coronary artery bypass surgery. Am Heart J. 1999;138:144–150. doi:10.1016/s0002-8703(99)70260-7
23. Bramer S, van Straten AH, Soliman Hamad MA, Berreklouw E, Martens EJ, Maessen JG. The impact of new-onset postoperative atrial fibrillation on mortality after coronary artery bypass grafting. Ann Thorac Surg. 2010;90:443–449. doi:10.1016/j.athoracsur.2010.03.083
24. Korantzopoulos P, Kolettis TM, Galaris D, Goudevenos JA. The role of oxidative stress in the pathogenesis and perpetuation of atrial fibrillation. Int J Cardiol. 2007;115:135–143. doi:10.1016/j.ijcard.2006.04.026
25. Wahr JA, Parks R, Boisvert D, et al. Preoperative serum potassium levels and perioperative outcomes in cardiac surgery patients. Multicenter study of perioperative ischemia research group. JAMA. 1999;281:2203–2210.
26. Zaman AG, Alamgir F, Richens T, Williams R, Rothman MT, Mills PG. The role of signal averaged P wave duration and serum magnesium as a combined predictor of atrial fibrillation after elective coronary artery bypass surgery. Heart. 1997;77:527–531. doi:10.1136/hrt.77.6.527
27. Aglio LS, Stanford GG, Maddi R, Boyd JL
28. Mathew JP, Fontes ML, Tudor IC, et al. A multicenter risk index for atrial fibrillation after cardiac surgery. JAMA. 2004;291:1720–1729. doi:10.1001/jama.291.14.1720
29. Zaman AG, Archbold RA, Helft G, Paul EA, Curzen NP, Mills PG. Atrial fibrillation after coronary artery bypass surgery: a model for preoperative risk stratification. Circulation. 2000;101:1403–1408. doi:10.1161/01.cir.101.12.1403
30. Asher CR, Miller DP, Grimm RA, Cosgrove DM
31. Aranki SF, Shaw DP, Adams DH, et al. Predictors of atrial fibrillation after coronary artery surgery. Current trends and impact on hospital resources. Circulation. 1996;94:390–397.
32. Premaratne S, Premaratne ID, Fernando ND, Williams L, Hasaniya NW. Atrial fibrillation and flutter following coronary artery bypass graft surgery: a retrospective study and review. JRSM Cardiovasc Dis. 2016;5:2048004016634149.
33. Kinoshita T, Asai T, Suzuki T, Kambara A, Matsubayashi K. Preoperative hemoglobin A1c predicts atrial fibrillation after off-pump coronary bypass surgery. Eur J Cardiothorac Surg. 2012;41:102–107. doi:10.1016/j.ejcts.2011.04.011
34. Bramer S, van Straten AH, Soliman Hamad MA, Berreklouw E, van den Broek KC, Maessen JG. Body mass index predicts new-onset atrial fibrillation after cardiac surgery. Eur J Cardiothorac Surg. 2011;40:1185–1190. doi:10.1016/j.ejcts.2011.02.043
35. Zacharias A, Schwann TA, Riordan CJ, Durham SJ, Shah AS, Habib RH. Obesity and risk of new-onset atrial fibrillation after cardiac surgery. Circulation. 2005;112:3247–3255. doi:10.1161/CIRCULATIONAHA.105.553743
36. Deliargyris EN, Raymond RJ, Guzzo JA, et al. Preoperative factors predisposing to early postoperative atrial fibrillation after isolated coronary artery bypass grafting. Am J Cardiol. 2000;85:763–764. doi:10.1016/S0002-9149(99)00857-7
37. Argalious M, Motta P, Khandwala F, et al. “Renal dose” dopamine is associated with the risk of new-onset atrial fibrillation after cardiac surgery. Crit Care Med. 2005;33:1327–1332. doi:10.1097/01.ccm.0000166876.41694.ca
38. Buxton AE, Josephson ME. The role of P wave duration as a predictor of postoperative atrial arrhythmias. Chest. 1981;80:68–73. doi:10.1378/chest.80.1.68
39. Steinberg JS, Zelenkofske S, Wong SC, Gelernt M, Sciacca R, Menchavez E. Value of the P-wave signal-averaged ECG for predicting atrial fibrillation after cardiac surgery. Circulation. 1993;88:2618–2622. doi:10.1161/01.cir.88.6.2618
40. Villareal RP, Hariharan R, Liu BC, et al. Postoperative atrial fibrillation and mortality after coronary artery bypass surgery. J Am Coll Cardiol. 2004;43:742–748. doi:10.1016/j.jacc.2003.11.023
41. Loubani M, Hickey MS, Spyt TJ, Galinanes M. Residual atrial fibrillation and clinical consequences following postoperative supraventricular arrhythmias. Int J Cardiol. 2000;74:125–132. doi:10.1016/s0167-5273(00)00229-1
42. Burgess DC, Kilborn MJ, Keech AC. Interventions for prevention of post-operative atrial fibrillation and its complications after cardiac surgery: a meta-analysis. Eur Heart J. 2006;27:2846–2857. doi:10.1093/eurheartj/ehl272
43. Rho RW. The management of atrial fibrillation after cardiac surgery. Heart. 2009;95:422–429. doi:10.1136/hrt.2007.132795
44. Rosenbaum MB, Chiale PA, Ryba D, Elizari MV. Control of tachyarrhythmias associated with Wolff-Parkinson-White syndrome by amiodarone hydrochloride. Am J Cardiol. 1974;34:215–223. doi:10.1016/0002-9149(74)90200-8
45. European Heart Rhythm A, Heart Rhythm S; Fuster V, Ryden LE, Cannom DS, et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation–executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation). J Am Coll Cardiol. 2006;48:854–906.
46. Daoud EG, Strickberger SA, Man KC, et al. Preoperative amiodarone as prophylaxis against atrial fibrillation after heart surgery. N Engl J Med. 1997;337:1785–1791. doi:10.1056/NEJM199712183372501
47. Mitchell LB, Exner DV, Wyse DG, et al. Prophylactic oral amiodarone for the prevention of arrhythmias that begin early after revascularization, valve replacement, or repair: PAPABEAR: a randomized controlled trial. JAMA. 2005;294:3093–3100. doi:10.1001/jama.294.24.3093
48. Zebis LR, Christensen TD, Kristiansen IS, Hjortdal VE. Amiodarone cost effectiveness in preventing atrial fibrillation after coronary artery bypass graft surgery. Ann Thorac Surg. 2008;85:28–32. doi:10.1016/j.athoracsur.2007.07.060
49. Zebis LR, Christensen TD, Thomsen HF, et al. Practical regimen for amiodarone use in preventing postoperative atrial fibrillation. Ann Thorac Surg. 2007;83:1326–1331. doi:10.1016/j.athoracsur.2006.09.096
50. Habibollahi P, Jam SH, Vahdati SS, Baghi HM, Amiri H. Amiodaron in atrial fibrillation: post coronary artery bypass graft. World J Emerg Med. 2016;7:250–254. doi:10.5847/wjem.j.1920-8642.2016.04.002
51. Budeus M, Hennersdorf M, Perings S, et al. Amiodarone prophylaxis for atrial fibrillation of high-risk patients after coronary bypass grafting: a prospective, double-blinded, placebo-controlled, randomized study. Eur Heart J. 2006;27:1584–1591. doi:10.1093/eurheartj/ehl082
52. Hohnloser SH, Meinertz T, Dammbacher T, et al. Electrocardiographic and antiarrhythmic effects of intravenous amiodarone: results of a prospective, placebo-controlled study. Am Heart J. 1991;121:89–95. doi:10.1016/0002-8703(91)90960-p
53. Zipes DP, Libby P, Bonow RO, Braunwald E. (2004). Heart Disease: A Textbook of Cardiovascular Medicine. 7th Edition. Philadelphia: Elsevier Science. E. B. Heart Disease.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.