")
Back to Journals » International Journal of General Medicine » Volume 9
Atrial fibrillation among the black population in a Ugandan tertiary hospital
Authors Lugero C, Kibirige D, Kayima J, Kizza Mondo C, Freers J
Received 16 November 2015
Accepted for publication 11 February 2016
Published 8 June 2016 Volume 2016:9 Pages 191—198
DOI https://doi.org/10.2147/IJGM.S100637
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Charles Lugero,1,2 Davis Kibirige,3 James Kayima,1,2 Charles Kizza Mondo,2 Jurgen Freers,2
1Division of Adult Cardiology, Uganda Heart Institute, 2Department of Medicine, Makerere University College of Health Sciences, Kampala, 3Department of Medicine, Our Lady of Consolata Hospital, Kisubi, Uganda
Background: Atrial fibrillation (AF) is the most common type of sustained cardiac arrhythmia in adults, accounting for one-third of hospitalizations due to arrhythmia and related complications worldwide. Previously, rheumatic heart disease was documented as the commonest cause of AF in sub-Saharan Africa. However, due to the prevailing epidemiological transition in sub-Saharan Africa, the risk factors and ensuing complications of AF have changed and are on the increase.
Methods: This was a descriptive cross-sectional study involving 102 patients presenting with AF who were recruited from the cardiology unit of Mulago National Referral Hospital, Uganda, over 3 months. Sociodemographic, medical history, and clinical data were obtained.
Results: The mean age of study participants was 52±21.3 years with a female predominance (58 [56.9%]). The commonest coexisting medical conditions were hypertension in 42% and rheumatic heart disease in 32% of the patients. The commonest echocardiographic abnormality was chamber dilation, noted in 76.8% of all patients. Heart failure was the most frequent complication encountered (50%) followed by left ventricular diastolic dysfunction and acute thromboembolic stroke documented in 19.6% and 12.8% of the study participants, respectively. Of the enrolled patients, ten (9.8%) died within 3 days of admission.
Conclusion: AF tends to occur at a younger age in Ugandan patients. The commonest underlying medical conditions among these patients were hypertension and rheumatic heart disease. Hence, all patients with hypertension and rheumatic heart disease should be meticulously screened for AF.
Keywords: atrial fibrillation, clinical profile, complications, Uganda
Introduction
In developed countries, atrial fibrillation (AF) is the most common sustained cardiac arrhythmia with an exponential increase with advancing age.1 It is strongly associated with an increased risk of stroke, hospitalization, and mortality.2 With the existing epidemiological transition from communicable to noncommunicable diseases, AF is a growing public health problem in sub-Saharan Africa (SSA).3 Use of anticoagulants, accessibility and costs of monitoring, poor drug compliance, and nonadherence to existing treatment guidelines are key challenges in managing patients with AF in this region.4,5
Data derived from studies in SSA in comparison to those derived from the developed countries have revealed that majority of patients presenting with AF have very severe disease and are comparatively younger with a higher frequency of concomitant complications.6–10
In Uganda, there is no literature on the clinical profile, complications, and outcome of patients presenting with AF. This was the basis of performing this contemporary cross-sectional study to describe the clinical characteristics and complications of patients presenting with AF at the cardiology unit of Mulago National Referral and Teaching Hospital, Kampala, Uganda.
Study methods
This was a descriptive cross-sectional study performed at the cardiology unit of Mulago National Referral and Teaching hospital in Kampala, the capital city of Uganda. This is the largest national referral hospital, teaching and health care research facility in Uganda with a 1,600 bed capacity.
Eligible patients presenting with AF to the cardiology unit, who were ≥13 years old, and had offered written informed consent or assent were consecutively recruited over a period of 3 months (April to June 2012) until the desired sample size was attained. Caregivers of patients <16 years old gave written consent and assent. Patients with atrial flutter and other rhythm disorders were excluded. AF was confirmed by a resting electrocardiography (ECG) done at the time of admission and interpreted by an experienced cardiologist.
The desired sample size of a minimum of 95 patients was obtained using the modified Kish Leslie (1965) formula:
N=Z2pq/e2, where N= required sample size, Z= standard normal value corresponding to the set level of confidence at 95% (1.96), P= estimated frequency of outcome factor in the population (the study used as a reference was by Karen Sliwa in South Africa where 56% of patients with AF had concomitant heart failure),8 q=1–P (0.44), and e= precision (0.1).
After obtaining informed consent or assent, pretested questionnaires were used to collect the patients’ information on the sociodemographic characteristics, presenting symptoms, presence and type of underlying heart diseases, thyroid status, history of excessive alcohol intake, and drug history (anti-arrhythmic and anticoagulation therapy). All participants had baseline anthropometric measurements of weight and height for the calculation of body mass index (BMI). Standard procedures for measuring blood pressure were also done on all patients after a 30-minute rest using a manual Dekamet Accoson MK3 mercury sphygmomanometer machine.
A two-dimensional Doppler transthoracic echocardiography (ECHO) was performed by an experienced cardiologist on all the patients with particular interest given to the left atrial size; left ventricular systolic and diastolic function; and the presence of valvular heart disease, hypertensive heart disease, and myocardial infarction. On ECHO, measurements of the inter-ventricular septum (IVS) or left ventricular posterior (LVP) wall >11 mm were considered to signify presence of left ventricular hypertrophy (LVH).11 Left ventricular function was defined as preserved when the left ventricular ejection fraction (LVEF) was ≤35% and depressed when LVEF <35%.
Diagnosis of hypertensive heart disease required the presence of at least one of the following conditions: 1) LVH on echocardiography (septum and posterior wall thickness 11 mm) and/or systolic or diastolic dysfunction or 2) signs of LVH on the 12-lead resting ECG using Sokolow–Lyon criteria and persistent elevation of blood pressure (≥140/90 mmHg) despite antihypertensive drug therapy.11,12
Using the validated congestive heart failure-hypertension-age ≥75 years-diabetes-prior stroke/transient ischemic attack (CHADS2) score, stroke risk stratification was performed for all the enrolled patients.13 This index measures stroke risk by assigning one point each for congestive heart failure, hypertension, age ≥75 years, and diabetes mellitus, with two points added for a history of stroke or transient ischemic attack. According to the American College of Cardiology, American Heart Association and the European Society of Cardiology guidelines, a CHADS2 score of ≥2 is considered as a marker of high risk of stroke and an indication for oral anticoagulation (OAC) therapy. A CHADS2 score of 1 is considered as a marker of moderate risk and an indication for OAC or cardiac aspirin.14
Laboratory analysis
Blood was then drawn from all the participants to assess serum urea, creatinine, electrolytes, and thyroid function tests. The collected blood samples were centrifuged and the extracted plasma was stored at –20°C. The analysis was done in the clinical chemistry laboratory of Mulago hospital by two experienced laboratory technicians using a fully automated COBAS® Integra 400 (Roche Diagnostics, Hoffman-La Roche Ltd., Basel, Switzerland) machine.
Statistical analysis
All the data collected on the pretested data collection sheet were entered into Epidata and thereafter exported to Stata version 10 for statistical analysis. Patient characteristics were reported as frequency and percentage for categorical variables, mean and standard deviation (SD) for the normally distributed continuous variables, and median and interquartile range (IQR) for continuous variables that were not normally distributed. Chi-square tests or Fischer’s exact test, where appropriate, were used to compare the categorical variables. Only variables with a P-value of <0.05 were considered significant.
Ethical consideration
The study was approved by the Department of Internal Medicine, Makerere College of Health Sciences and Makerere University School of Medicine Research and Ethics Committee. All patients gave informed consent and assent prior to enrollment into the study.
Results
Sociodemographic, clinical, and laboratory characteristics of the patients
Sociodemographic characteristics of the study participants
Of the 102 patients enrolled, majority were females (58 [56.9%]). The overall mean age was 52±21.3 years and did not differ with sex. The youngest participant was 13 years and the oldest was 88 years old. Majority of the study participants were employed (52.9%) and had attained some level of education (85 [83.3%]) (Table 1).
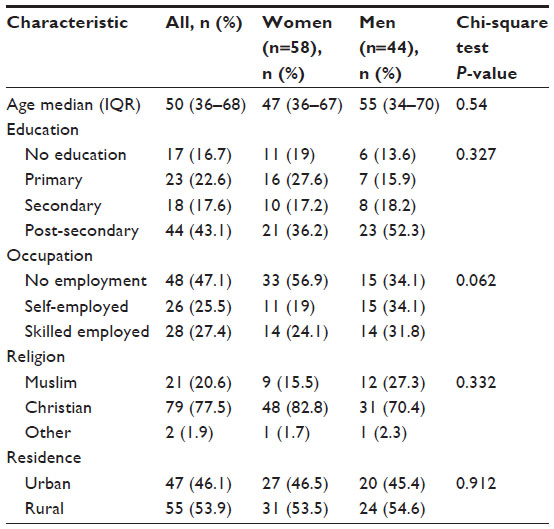 | Table 1 Sociodemographic characteristics of admitted patients presenting with AF |
Clinical features of the study participants
Majority of the participants presented with palpitations (86 [84%]) and dyspnea (70 [68.6%]). There was no difference in the presenting symptoms according to sex. Approximately, 57% of the patients had a normal BMI, defined as 18.5–25 kg/m2. Obesity, overweight, and underweight were documented in 9.8%, 24.5%, and 8.8% of the participants, respectively.
Laboratory characteristics of the study participants
Thyroid dysfunction among the study participants was very infrequent. Overt and subclinical hyperthyroidism and hypothyroidism were both documented in 2.9% of the participants. There was no significant difference noted in regards to sex. Renal derangements were also uncommon in this study population. Only 31.7% and 37.6% of the participants had elevated serum creatinine and blood urea nitrogen (BUN) levels on assessment, respectively. Hypocalcemia (uncorrected for serum albumin levels) was very frequent, occurring in 51 (50.5%) participants (Table 2).
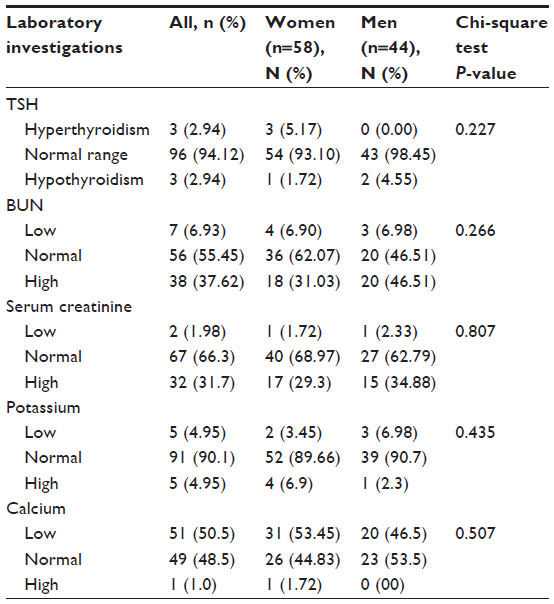 | Table 2 Laboratory findings of the study participants |
Underlying medical conditions associated with AF
The commonest underlying medical condition in the study participants was hypertension, documented in 43 (42.2%) participants. Rheumatic heart disease, diabetes mellitus, and congenital heart diseases were noted in 32.4%, 9.8%, and 5.9% of the study participants, respectively. A significant proportion of the participants (n=79 [77.4%]) had at least one cardiac condition combined. The documented combined cardiac conditions included hypertensive heart disease, congenital heart diseases, myocardial infarction, and rheumatic heart disease, and they were more prevalent in females compared to males (86.2% vs 65.9%, P=0.015) (Table 3).
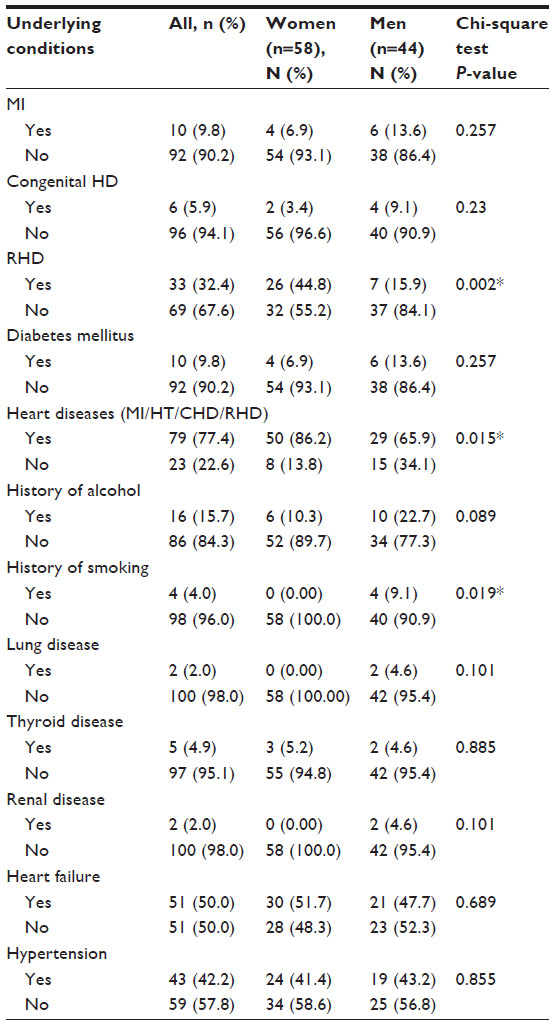 | Table 3 Underlying medical conditions associated with atrial fibrillation |
Five (4.9%) patients presented with “lone” AF (ie, no other diagnoses or evidence of underlying cardiac dysfunction). These were mostly males (64.7%) and were younger with a mean age of 46.1±18.7 years. In terms of ventricular response, over 86% of patients had uncontrolled AF (ventricular rate >90 beats per min [bpm]) and this was equally distributed between the males and females studied. Of the four patients with a heart rate <50 bpm, two had sick sinus syndrome.
Echocardiographic findings of the study participants
An ECHO examination was done in all the participants. The commonest abnormality was chamber dilation (dilation of ≥1 chambers) documented in 76.8% of all patients. Preserved left ventricular systolic function and diastolic dysfunction were noted in 93 (91.2%) and 27 (26.5%) patients, respectively.
Other ECHO findings in the study participants were rheumatic heart disease in 35 (34.3%), mitral stenosis in 33 (32.3%), dilated cardiomyopathy in 14 (13.7%), ischemic heart disease in eleven (10.8%), and LVH in 35 (34.3%) patients.
Both rheumatic heart disease and mitral stenosis were more prevalent in female participants compared to male participants and this finding was statistically significant (48.3% vs 15.9%, P=0.001 and 46.6% vs 13.6%, P<0.001, respectively) (Table 4).
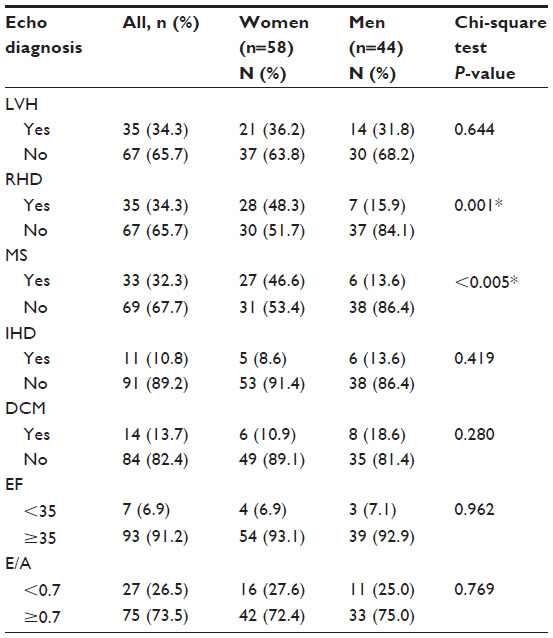 | Table 4 Echocardiographic findings of the study participants |
Complications attributable to AF
Heart failure was the commonest complications encountered among the study participants (51 [50%]). Acute thromboembolic stroke and left ventricular systolic and diastolic dysfunction were documented in 13 (12.8%), 7 (6.9%), and 20 (19.6%) patients, respectively. Forty one (40.2%) patients had a history of readmission due to AF. Of the enrolled patients, ten (9.8%) died within 3 days following admission (Table 5).
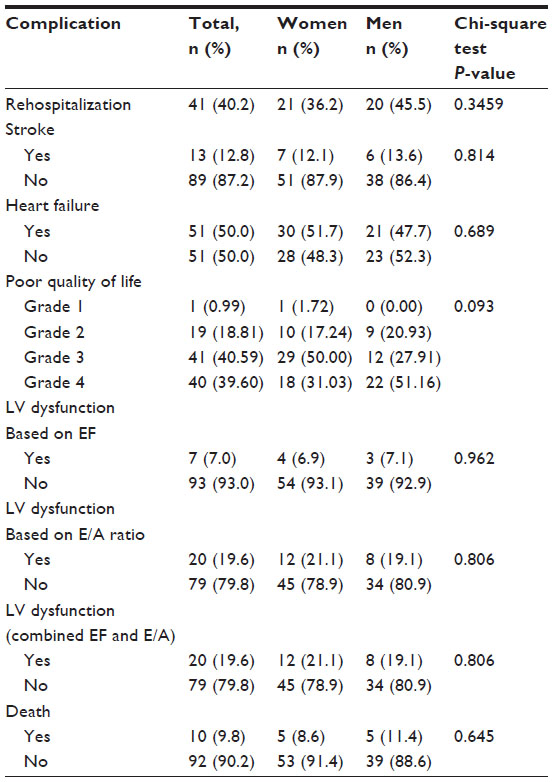 | Table 5 Complications of patients with AF admitted at Mulago Hospital medical wards |
Stroke risk stratification
We used the recently validated CHADS2 score to stratify patients for stroke risk. Out of 102 participants, the majority had moderate risk (58 [56.9%]). High stroke risk was noted in 18 (17.7%) patients while 26 (25.5%) had a low risk. A secondary analysis of the 13 patients who had stroke, using the CHADS2 stroke risk stratification, showed that ten (76.9%) patients had a high stroke risk while three (23.1%) had a moderate risk.
Discussion
To our knowledge, this is the first study to describe the clinical profile and complications of patients presenting with AF in Uganda, a country with a rising burden of cardiovascular diseases.
In regards to the mean age of the study participants, the findings of our descriptive survey were similar to what was noted in studies done in Cote d’Ivoire, South Africa, and India.7,8,15 The mean age of the study participants was comparable to what was documented in the above studies (52±21.3 years), reflecting a younger patient population with AF in SSA. Studies from Cameroon and Kenya documented a higher mean age of 65.8±13 years and 67.8±17.1 years, respectively.9,10
A female predominance was noted in our study (56.9%) similar to studies performed in South Africa (61%), Cameroon (56.4%), and India (55.5%).8, 9,15 Studies from Cote d’Ivoire and Kenya had more males presenting with AF (56% and 52%, respectively).7,10 This female predominance in our study could probably be explained by the sex-based differences in underlying etiologies of AF in our study. Rheumatic heart disease and mitral stenosis were more prevalent among female patients.
Clinical presentations of the study participants
Palpitations, dyspnea, and chest pain were the most prominent symptoms reported, occurring in 84.3%, 68.6%, and 49% of the patients, respectively. A high frequency of symptoms related to a rapid heart rate, ie palpitations, syncope, dizziness, and fatigue (32%), was reported in the study participants in Kenya.10 Among the 158 (92%) patients with AF who reported with symptoms of heart failure in the study done in Cameroon, dyspnea was the most prevalent occurring in 72.1% of the patients.9 Other symptoms were palpitations in 46.5% and malaise in 20.9% of the patients. Dyspnea was also the commonest reported symptom in the study done in Cote d’Ivoire.7
The most prominent documented clinical signs in the study participants (50%) were congruent with heart failure. This noted high frequency of heart failure is similar to what was documented in Cote d’Ivoire (62.6%), South Africa (56%), and Cameroon (49.4%).7–9 Studies from Kenya and People’s Republic of China on patients presenting with AF reported relatively low frequency of heart failure of 38% and 33.1%, respectively.10,16
Coexisting medical conditions or risk factors
Hypertension in our study was the most prevalent coexisting medical condition, noted in 43 (42%) study participants. This is consistent with findings from majority of the recent studies on AF in developing countries that have also documented hypertension as the most prevalent coexisting medical condition. This is in contrast to the past notion that rheumatic heart disease is the commonest.7,9,10,16–19
However, rheumatic heart disease was noted to be the commonest coexisting medical condition in a similar study done in North India, reported in 61.3% of the patients.15 Only 14.6% of the patients were documented to have hypertension with 10.2% having hypertensive heart disease on ECHO. With the exception of heart failure in the study from South Africa, a significant proportion of patients with AF had rheumatic heart disease (21%) compared to those with hypertensive heart disease (19%).8
Other coexisting medical conditions reported among the study participants in our study were rheumatic heart failure (32%), diabetes mellitus, and myocardial infarction (both in 9.8% of the patients). Lung disease of any form and preexisting thyroid dysfunction were very infrequent, reported in only 2% and 4.9% of the patients, respectively.
Thyroid dysfunction has been noted to be very uncommon among patients with AF in most studies done in developing countries. Studies reported from Kenya, People’s Republic of China, Pakistan, and Brazil have reported prevalence of 3.7%, 2.5%, 7.5%, and 14.3%, respectively.10,16,20,21
It is worth noting that coronary artery disease is also very infrequent among African patients presenting with AF. Prevalence of 6.5%, 6.4%, 19%, and 6.6% have been documented in studies done in South Africa, Cameroon, Kenya, and Ethiopia, respectively.8–10,19 The probable explanations are lower mean total cholesterol or low-density lipoprotein cholesterol concentrations and lower frequencies of smoking among the African patients compared to their contemporaries in developed countries. We did not assess lipid profiles in our study. Only 3.9% of the study participants gave a history of smoking and all were male.
The intimate relationship between hypertension and AF has been extensively described in medical literature. Long standing uncontrolled hypertension is often associated with left ventricular diastolic and systolic dysfunction. This subsequently results in increased left atrial pressure and left atrial enlargement. The latter is a precursor of AF. Hypertension is also associated with renin–angiotensin–aldosterone system activation which increases oxidative stress and inflammation. This collectively augments atrial fibrosis and cellular hypertrophy increasing the risk of AF.22
Complications attributed to AF
Regarding complications associated with AF, heart failure of any form (50%) and recurrent hospital admissions (40.2%) were the most prevalent. Thromboembolic stroke was noted in 13 (12.8%) patients. Stroke risk stratification of these patients using the CHADS score revealed that majority (10 [76.9%]) had a high stroke risk. This high frequency of thromboembolic stroke was similar to what was documented in the Cameroonian (17.4%), Chinese (17.5%), and Ethiopian (15.4%) studies.9,16,19 This magnitude of stroke among patients with AF is outstandingly higher than what has been documented in the developed countries. In one prospective study reported from Geneva, Switzerland, stroke was prevalent in only 2.6% of the patients.23 This disparity could be explained by the probable suboptimal use of oral anticoagulant therapy among patients with AF in the developing countries.5,16,24 This calls for policies and guidelines aimed at improving treatment of AF in these countries.
In our study, ten (9.8%) patients with AF died within 3 days of admission. Although no postmortem examinations were done, we presume the causes of death were of cardiovascular nature because all the patients who died had severe heart failure (New York Heart Failure class III and IV). Another probable documented cause of death was severe hypostatic pneumonia.
A high mortality rate in patients with AF has also been revealed in the Cameroonian study compared to low rates in European countries (<4%), Switzerland (2.6%), and France (ALPHA study in France [1.8%]).9,23,25 This signifies that AF in African patients is more severe and is associated with more adverse outcomes. This high rate of mortality in Africa could also be explained by the suboptimal use of oral anticoagulant therapy due to economic reasons, difficulties in performing international normalized ratio (INR) to assess adequate anticoagulation, and presence of uncontrolled hypertension, a documented relative contraindication. Other factors that could explain the higher rate of mortality are the higher prevalence of rheumatic heart disease and increased severity of comorbidities like uncontrolled hypertension.
In a study done in Cameroon, out of 88 patients who were followed up for a mean period of 318±124 days, 26 (29.5%) died. This proportion was higher than what was registered in our study, probably because of our shorter period of assessment for mortality (3 days vs 318±124 days). A low rate of use of oral anticoagulant therapy was noted in the study from Cameroon. Only three (11.5%) of the 26 patients who died were on oral anticoagulant therapy.9
In the Kenyan study, despite 64.7% of patients having a CHADS score ≥2, 21.2% of these patients did not receive any form of anticoagulant therapy.10 We however noted a moderately good prescription rate of oral anticoagulant therapy in our study. Approximately, 53% of patients with at least one stroke risk factor received therapy. These rates of use of the recommended therapy are, nevertheless, still lower than what is reported from studies from some developed countries (88% in Switzerland).23
Combined left ventricular diastolic and systolic dysfunction was also frequent in the study participants, noted in 20 (19.6%) cases. Diastolic and systolic dysfunction in isolation occurred in 19.6% and 6.9% of the patients, respectively. Similar studies from South Africa, Cameroon, and People’s Republic of China have reported a higher proportion of patients with systolic dysfunction (22.7%, 30%, and 35% respectively) compared to our study.8,9,16
Study limitations
This cross-sectional study was designed to assess the clinical characteristics and complications of patients with AF with out a follow-up component; hence, we were unable to classify AF into paroxysmal, persistent, and permanent AF.
It was difficult to verify the precise cause of death because no autopsy studies were done; therefore, causes of death were determined based only on clinical grounds. Due to economic constraints, we did not perform neuroimaging to document the type of stroke and infarct size.
Because Mulago hospital is the only national referral hospital in Uganda where a full-scale cardiology approach is practiced, a selection bias was certainly present because only very sick patients are referred to a cardiologist. This study, hence, excluded those suffering from milder forms of cardiovascular disease or asymptomatic AF in the community as well as noncardiac cases in the hospital. This is particularly relevant when interpreting the estimated rate of case presentations.
We used the CHADS score which is less sensitive compared to the congestive heart failure-hypertension-age ≥75 years-diabetes mellitus-prior stroke or transient ischemic attack-vascular disease-age of 65–74 years and sex category (CHADS2VASC) score for the lower risk group.
Conclusion
In this study, we have demonstrated that the clinical presentation of Ugandan patients with AF is more common, severe (more prevalent advanced congestive heart failure, palpitations, recurrent hospital admissions, and incidence of thromboembolic stroke), and occurs at a younger age than in developed countries. It also illustrates the rising prevalence of noncommunicable diseases like hypertension as the commonest risk factor of AF with an already existing high prevalence of rheumatic heart disease, hence a dual epidemic. AF in Ugandan patients is a predictive factor for both severe stroke and early mortality.
Recommendations
A meticulous cardiac evaluation for AF should be executed especially in patients with hypertension, rheumatic heart disease, and diabetes mellitus in Uganda. Local guidelines on management of AF should be developed to improve the outcome in patients with AF and reduce adverse outcomes.
Acknowledgments
We would like to thank the following people for their invaluable contribution toward this study: Dr Peter Mudiope for the statistical input, Drs Stephen Bavewo, Robert Kalyesubula, Emmy Okello, Barbra Kakande, and Bruce Kirenga. We would also like to thank all the study participants. This study was funded by the Medical Educational Partnership Initiative-Cardiovascular Diseases Linked award (MEPI-CVD) in collaboration with the Fogarty International Centre, the National Heart Lung and Blood Institute, and the Common Fund of the National Institutes of Health under Award Number R24TW008861.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Lloyd-Jones D, Wang T, Leip E, et al. Lifetime risk for development of atrial fibrillation: the Framingham Heart Study. Circulation. 2004;110(9):1042–1046. | |
Nieuwlaat R, Prins M, Le-Heuzey J, et al. Prognosis, disease progression, and treatment of atrial fibrillation patients during 1 year: follow-up of the Euro Heart Survey on atrial fibrillation. Eur Heart J. 2008;29:1181–1189. | |
Sala D, Stigliano R, Stella A, Genovesi S. The epidemiological transition in developing countries: estimated prevalence of non-communicable chronic diseases in a population of sub-Saharan Africa. High Blood Press Cardiovasc Prev. 2010;17:140. | |
Anakwue R, Ocheni S, Madu J. The pattern and challenges of anticoagulation in a resource-constrained setting in Nigeria. J Clin Pharmacol. 2011;51:1352. | |
Aalbers J. South Africa’s poor warfarin control raises questions of benefit above other anticoagulant therapies in atrial fibrillation. Cardiovasc J Afr. 2011;22:220. | |
Mbaye A, Pessinaba S, Bodian M, et al. Atrial fibrillation, frequency, etiologic factors, evolution and treatment in a cardiology department in Dakar, Senegal. Pan Afr Med J. 2010;6:16. | |
Coulibaly I, Anzouan-Kacou J, Konin K, Kouadio S, Abouo-N’Dori R. Atrial fibrillation: epidemiological data from the Cardiology Institute in Abidjan, Cote d’Ivoire. Med Trop. 2010;70:371–374. | |
Sliwa K, Carrington M, Klug E, et al. Predisposing factors and incidence of newly diagnosed atrial fibrillation in an urban African community: insights from the Heart of Soweto Study. Heart. 2010; 96(23):1878–1882. | |
Ntep-Gweth M, Zimmermann M, Meiltz A, et al. Atrial fibrillation in Africa: clinical characteristics, prognosis, and adherence to guidelines in Cameroon. Europace. 2010;12(4):482–487. | |
Shavadia J, Yonga G, Mwanzi S, Jinah A, Moriasi A, Otieno H. Clinical characteristics and outcomes of atrial fibrillation and flutter at the Aga Khan University Hospital, Nairobi. Cardiovasc J Afr. 2013;24:6–9. | |
Foppa M, Duncan B, Rohde L. Echocardiography-based left ventricular mass estimation. How should we define hypertrophy? Cardiovascular Ultrasound. 2005;3:17. | |
Hancock E, Deal B, Mirvis D, Okin P, Kligfield P, Gettes L. AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part V: Electrocardiogram Changes Associated With Cardiac Chamber Hypertrophy: A Scientific Statement From the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society: Endorsed by the International Society for Computerized Electrocardiology. Circulation. 2009;119:e251–e261. | |
Gage B, Waterman A, Shannon W, et al. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001;285:2864–2870. | |
Fuster V1, Rydén LE, Cannom DS, et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation-executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients with Atrial Fibrillation). Eur Heart J. 2006;27:1979–2030. | |
Bhardwaj R. Atrial fibrillation in a tertiary care institute: a prospective study. Indian Heart J. 2012;64:476–478. | |
Wen-Hang Q. Retrospective investigation of hospitalised patients with atrial fibrillation in mainland China. Int J Cardiol. 2005;105:283–287. | |
Bulanova N, Stazhadze L, Alekseeva L, Dubrovina E, Dorofeeva E. Prevalence of atrial fibrillation among patients under observation by an outpatient clinic. Kardiologiia. 2011;51(12):29–35. | |
Haq U, Lip G. A prospective survey of acute hospital admissions with atrial fibrillation in Karachi, Pakistan. J R Coll Physicians Edinb. 2009;39:200–203. | |
Maru M. Atrial fibrillation and embolic complications. East Afr Med J. 1997;74:3–5. | |
Randhawa M. Antithrombotic therapy in patients with non-rheumatic atrial fibrillation. Specialist. 1998;14:281–284. | |
De-Carvalho E, Miotta S, Alves A, Curiati J, De-Alencar Y. Chronic atrial fibrillation in the elderly. Arq Bras Cardiol. 1991;57:109–114. | |
Lau Y, Yiu K, Siu C, Tse H. Hypertension and atrial fibrillation: epidemiology, pathophysiology and therapeutic implications. J Hum Hypertens. 2012;26:563–9. | |
Meiltz A, Zimmermann M, Urban P, et al. Atrial fibrillation management by practice cardiologists: a prospective survey on the adherence to guidelines in the real world. Europace. 2008;10:674–680. | |
Bhagat K, Tisocki K. Prescribing patterns for the use of antithrombotics in the management of atrial fibrillation in Zimbabwe. Cent Afr J Med. 1999;45:287–290. | |
Levy S, Maarek M, Coumel P, et al. The ALPHA study: on behalf of the College of French Cardiologists. Characterization of different subsets of atrial fibrillation in general practice in France. Circulation. 1999;99:3028–3035. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.