")
Back to Journals » Journal of Pain Research » Volume 15
At Least 5-Year Outcomes of Whiplash-Induced Chronic Neck Pain Following Response to Intra-Articular Facet Joint Corticosteroid Injection
Authors Yang S, Boudier-Revéret M , Hsiao MY, Kwak S, Chang MC
Received 26 April 2022
Accepted for publication 19 July 2022
Published 29 July 2022 Volume 2022:15 Pages 2133—2138
DOI https://doi.org/10.2147/JPR.S371263
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael A Ueberall
Seoyon Yang,1 Mathieu Boudier-Revéret,2 Ming-Yen Hsiao,3,4 Soyoung Kwak,5 Min Cheol Chang5
1Department of Rehabilitation Medicine, Ewha Woman’s University Seoul Hospital, Ewha Woman’s University School of Medicine, Seoul, Republic of Korea; 2Department of Physical Medicine and Rehabilitation, Centre Hospitalier de l’Université de Montréal, Montreal, Canada; 3Department of Physical Medicine and Rehabilitation, College of Medicine, National Taiwan University, Taipei, Taiwan; 4Department of Physical Medicine and Rehabilitation, National Taiwan University Hospital, Taipei, Taiwan; 5Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University, Daegu, Republic of Korea
Correspondence: Min Cheol Chang, Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University, 317-1, Daemyungdong, Namku, Daegu, 705-717, Republic of Korea, Tel +82-53-620-4682, Email [email protected]
Objective: To investigate whether the response to intra-articular facet joint corticosteroid injection can determine the long-term prognosis (at least 5 years after injury) of whiplash injury-related neck pain sustained 3– 12 months after injury.
Methods: Of 65 patients who visited a university hospital for persistent whiplash injury-induced axial neck pain sustained 3– 12 months after injury (numeric rating scale score ≥ 3) and had received intra-articular facet joint corticosteroid injection, 40 completed the telephone interview. We divided the patients into “good response group” (≥ 50% pain reduction at 1 month after the injection) and “poor response group” (< 50% pain reduction at 1 month after the injection). We asked participants regarding the presence and degree of neck pain, its impact on work, and the use of oral pain medication or injection treatment.
Results: A follow-up at least 5 years after the injury found that the number of patients with persistent whiplash injury-related neck pain was significantly lower in the good response group than in the poor response group. The number of patients taking oral pain medications prescribed by a medical doctor or receiving injection treatments in a pain clinic or hospital for neck pain was lower in the good response group than in the poor response group. The number of patients who answered that their work was affected by neck pain was lower in the good response group than in the poor response group.
Conclusion: The response to intra-articular corticosteroid injection might be helpful in determining at least 5-year outcomes of chronic whiplash injury-induced pain.
Keywords: whiplash injury, facet joint, corticosteroid, injection, neck pain, chronic pain, outcome, prognosis
Introduction
Whiplash injury occurs when there are sudden forward, backward, or sideway movements of the neck caused by acceleration-Deceleration force transfer to the neck, usually resulting from a motor vehicle collision.1,2 This results in injury to the cervical spine (intervertebral discs, facets, and ligaments) and soft tissues of the neck (muscles and tendons), causing neck pain, headache, stiffness, and loss of neck movement.3 Although approximately 50% of patients with whiplash injury recover completely, the remaining 50% are known to have some degree of persistent symptoms.4 Recovery from whiplash injury mostly occurs within 3 months of the injury, and the recovery rate significantly declines after this period, with only minimal improvement occurring more than 1 year after the injury.1,5,6
Many previous studies have evaluated the outcomes of a whiplash injury and reported that older age, female sex, and high intensity of initial neck pain were risk factors for poor prognosis of whiplash injury-induced neck pain.5,7–10 However, factors that can predict the long-term outcomes of chronic neck pain after whiplash injury have not been investigated.
The cervical facet joint is a common source of chronic whiplash-related neck pain.11,12 During a whiplash injury, overloading of the facet joints via forceful movement can result in the tearing of the joint capsule and the capsular ligament, facet joint hemarthrosis, articular cartilage damage, and synovial fold displacement.11,12 Inflammation within and around the joint capsule causes whiplash injury-related neck pain. However, inflammation can be effectively controlled by corticosteroid injection, and intra-articular facet joint injection is effectively used for managing whiplash induced neck pain.13–17 Furthermore, damage to the joint capsule can be healed by the tissue healing process. However, when neck pain becomes chronic, the treatment also becomes challenging.18 Chronic pain is not a simple extension of acute pain; it can cause neural plasticity or sensitization of the nervous system in the peripheral nerves, spinal cord, and brain.18,19 In other words, it induces alterations to the nervous system.18,19 Because corticosteroids do not play a role in managing neural plasticity or sensitization, the pain-reducing effect of intra-articular corticosteroid injection is usually reduced when it is used to control chronic pain. Sensitized pain is often refractory to many pain-reducing treatments, and its prognosis is frequently poor.18,19
We assume that the lack of response to intra-articular corticosteroid injection in patients with chronic neck pain due to whiplash injury indicates that neck pain is largely associated with plasticity or sensitization of the nervous system. Therefore, the prognosis of whiplash injury-induced chronic neck pain remains poor.
In the current study, we evaluated whether the response to intra-articular facet joint corticosteroid injection can determine the long-term prognosis (at least 5 years after the onset of injury) of whiplash injury-related chronic neck pain.
Methods
Subjects
This study was conducted retrospectively. We recruited patients with chronic axial cervical pain induced by whiplash injury who had visited the pain clinic of a university hospital and received intra-articular facet joint injections between November 2013 and November 2016. The inclusion criteria were as follows: (I) age between 20 and 79 years at the time of whiplash injury; (II) persistent whiplash injury-induced axial neck pain sustained 3–12 months after injury, with a numeric rating scale (NRS) score of ≥3 (NRS 0–10; 0, no pain; 10, worst pain imaginable); (III) failure to respond to oral pain medications; (IV) ≥ 80% temporary pain relief following a diagnostic block with intra-articular injection of 0.3 mL of 2% lidocaine; (V) received intra-articular corticosteroid injection at 3–12 months after onset; and (VI) no radicular symptoms. Patients with a history of neck pain prior to whiplash injury, rheumatic disorders, or psychiatric disorders were excluded. The study has been approved by the Yeungnam university hospital review board (2021–06-021). Informed consent was provided orally by asking participants if they agreed to accept a telephone assessment, which was permitted by the Yeungnam university hospital review board because a face-to-face interview with participants was difficult and the study did not have any risk to harm patients. We followed the Declaration of Helsinki guidelines.
Intra-Articular Facet Joint Corticosteroid Injection
Intra-articular facet joint corticosteroid injections were performed via a posterior approach for C-arm fluoroscopy with the patient in a prone position (Siemens, Munich, Germany). The patients were placed with their thorax rested on two pillows, their neck maximally flexed, and their head turned 60–90° away from the side of the injection. Following neck flexion, the C-arm tube was angled cephalically until it was at a tangent to the cervical facet joint space. A 26-gauge, 90 mm spinal needle was then inserted under fluoroscopy parallel to the C-arm beam. After confirming intraarticular access by injecting 0.3 mL of contrast into the CFJ space, we injected 10 mg (0.25 mL) of triamcinolone acetonide mixed with 0.25 mL of 0.125% bupivacaine. Intraarticular injection was successful in all recruited patients.
Assessment of the 5-Year Outcome of Whiplash Injury-Induced Neck Pain
In total, 65 patients were recruited, and one investigator conducted all the telephone interviews to evaluate the 5-year outcome of whiplash injury-induced neck pain. For the investigation, we asked the following questions: (I) “Are you still experiencing neck pain induced by the accident?”; (II) “Rate the degree of your current neck pain on a scale of 0–10, with 0 being no pain and 10 being the worst pain imaginable”; (III).
Are you taking pain medications prescribed by a medical doctor or receiving injection treatments in a pain clinic or hospital for controlling neck pain due to the accident?; and (IV) “Is your work at your place of employment or home being disturbed by your current neck pain?”
Data Collection by Chart Review and Group Division
Data on age, sex, duration from onset of injury to NRS evaluation prior to corticosteroid injection, duration from onset of injury to the day of the telephone interview, degree of neck pain (NRS) 3–12 months after the whiplash injury (prior to intra-articular facet corticosteroid injection), and degree of neck pain (NRS) at 1 month after intra-articular facet corticosteroid injection were collected from a chart review. We defined a good response to intra-articular steroid injection as ≥50% pain reduction at 1 month after the injection, and a poor response as <50% pain reduction at 1 month after the injection. We divided the patients into “good response group” and “poor response group.”
Statistical Analysis
We compared the demographic data and long-term outcomes (at least 5 years after the onset of whiplash injury) between the two groups using Mann–Whitney U-tests (age, the duration from the onset of the injury to the NRS evaluation prior to injection, the duration from the onset of the injury to the day of the telephone interview, the degree of neck pain at pre-injection as well as at one-month post-injection, and the degree of neck pain at least five years after injury onset), as well as Chi-square tests (sex, the presence of persistent neck pain, taking oral pain medication or receiving injection treatment, and injury-associated disturbances during work at least five years after injury onset). A p-value less than 0.05 was considered statistically significant. The analyses were conducted using the SPSS version 26.0.
Results
Of the 65 recruited patients, 40 (47.6 ± 12.2 years at the time of the injury; M:F = 17:23) participated in the telephone interview (Table 1, Supplementary 1). In all these 40 patients, traffic accidents were the cause of the whiplash injury. Results for the NRS administered at one month after the intra-articular facet corticosteroid injection was presented for all 40 enrolled patients in Table 1. Between the good response and poor response groups, age, sex ratio, duration from onset of injury to NRS evaluation prior to corticosteroid injection, duration from onset of injury to day of telephone interview, and NRS scores of neck pain prior to the injection were not significantly different (age: p = 0.080; sex: p = 0.150; the duration from the onset of the injury to the NRS evaluation conducted prior to injection: p = 0.327; the duration from the onset of the injury to the day of the telephone interview: p = 0.645; NRS scores indicating neck pain prior to injection: p = 0.265) (Table 1). The NRS score of neck pain at 1 month after the injection was significantly lower in the good response group as compared with the poor response group (p < 0.001; good response group = 1.9 ± 1.0 vs poor response group = 4.1 ± 1.5).
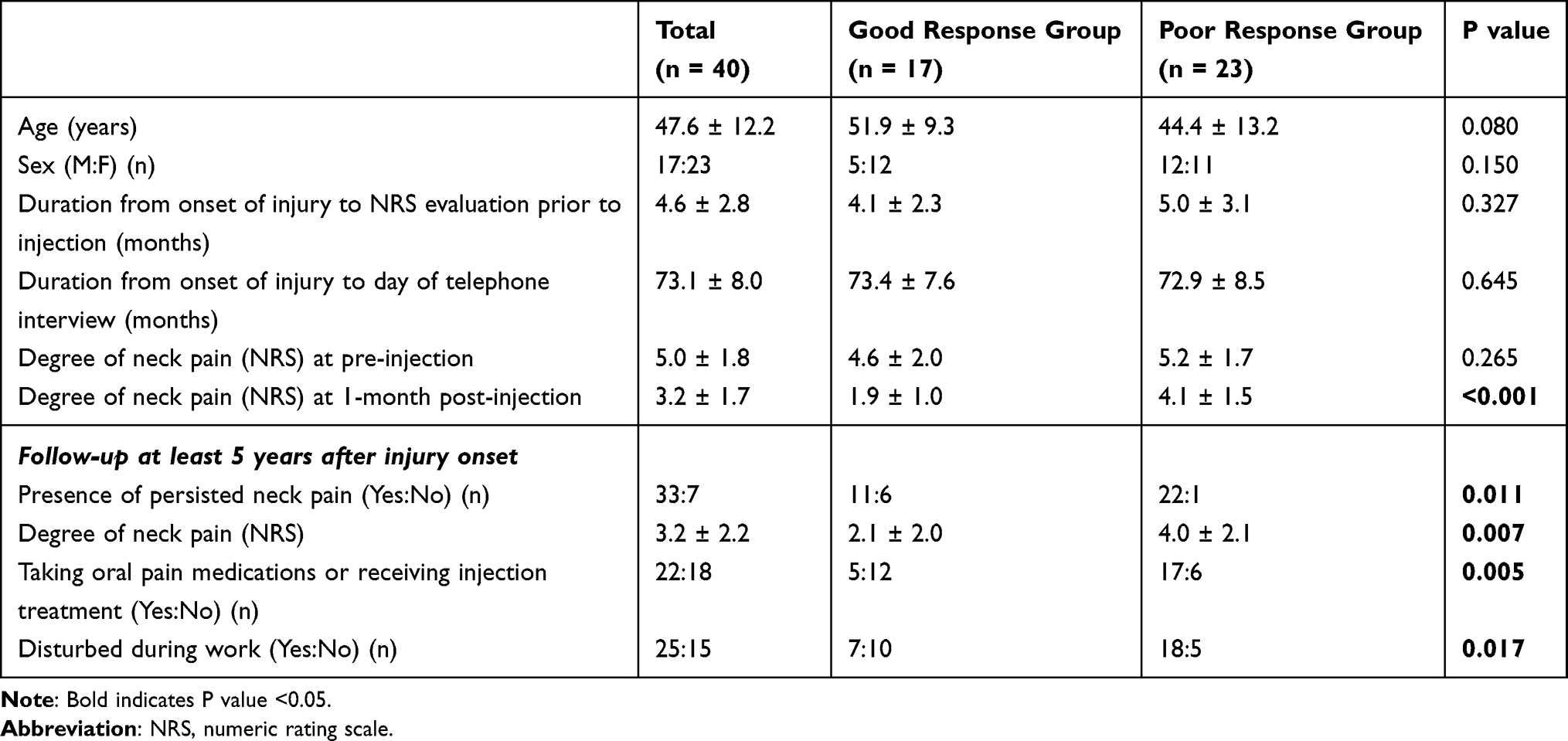 |
Table 1 Comparison of Demographic Data and Long-Term Outcome (at Least 5 Years After the Onset of Whiplash Injury) Between Good Response Group and Poor Response Group |
A follow-up at least 5 years after the whiplash injury found that the number of patients with persistent whiplash injury-related neck pain was significantly lower in the good response group than in the poor response group (p = 0.011; good response group, 64.7% vs poor response group, 95.7%). In addition, the NRS score in the good response group was significantly lower than in the poor response group (p = 0.007; good response group = 2.1 ± 2.0 vs poor response group = 4.0 ± 2.1).
The number of patients taking oral pain medications prescribed by a medical doctor or receiving injection treatments in a pain clinic or hospital for controlling neck pain was lower in the good response group than in the poor response group (p = 0.005; good response group, 29.4% vs poor response group, 73.9%). The number of patients who answered that their work (workplace or home) was affected by the current neck pain was lower in the good response group than in the poor response group (p = 0.017; good response group = 41.2% vs poor response group = 78.3%).
Discussion
In this study, we evaluated the long-term outcomes (at least 5 years after injury) of whiplash injury-related neck pain that was sustained 3–12 months after the onset of the injury following response to intra-articular facet joint corticosteroid injection. In our study, although approximately 35% of patients who showed a good response to corticosteroid injection had no whiplash injury-related pain, the overall prognosis of the included patients was not favorable. Of the 40 patients who answered the survey, 80% still had neck pain induced by whiplash injury even at least 5 years after the onset of the injury. Also, patients who did not have a good response to intra-articular facet joint injection showed a significantly poorer long-term outcome compared with those who showed a good response. Nearly all the patients, except for one patient in the poor response group, had persistent neck pain.
As the recovery of neck pain after whiplash injury is known to be minimal after a year of onset,1 we recruited patients with whiplash injury-related chronic neck pain within 1 year of injury onset. In our study, we found that the prognosis was not favorable even though whiplash injury-related neck pain was continued for 3–12 months after the onset of the injury. Regarding previous studies on prognosis of whiplash injury-related neck pain, Rasmussen et al reported that approximately 55% of patients with whiplash injury experienced some problems at 12–14 years after the onset of injury.20 In addition, Sameh et al reported that approximately 30% of patients received treatment for reducing neck pain approximately 10 years after the onset of injury.6 The reason for the high percentage of persistent neck pain in our study compared to previous studies could be due to the different inclusion criteria between our study and the previous studies. Our study included patients with chronic neck pain due to whiplash injury; however, previous studies investigated the outcomes of patients with acute-stage whiplash injury.
In addition, previously, older age, female sex, and initial severe pain were reported to be associated with delayed recovery from whiplash injury.5,7–10 However, the outcome of whiplash injury according to the response to treatment for pain reduction has not been evaluated. Therefore, to the best of our knowledge, our study is the first to show that the response to intra-articular corticosteroid injection is associated with long-term outcomes of chronic whiplash injury-induced pain.
We think that the poor response to corticosteroid injection into the cervical facet joint indicates that whiplash injury-induced pain might have been centralized.18,19 Additionally, the poor response suggests that the degree of joint injury could be severe and continuous mechanical irritation might exist on the cervical facet joint.
In conclusion, although the overall long-term prognosis of whiplash injury-induced pain is not favorable, if the response to intra-articular corticosteroid injection is good, we can think that there is some possibility that a whiplash injury can be favorably recovered. In contrast, poor response to corticosteroid injection indicates a high possibility of poor long-term outcomes. We believe that the results of our study provide useful clinical information for predicting long-term outcomes of whiplash injury-induced chronic neck pain. However, our study has some limitations. First is the small number of patients. Second, approximately 30% of the initially recruited patients did not answer the telephone interview. However, because the ratio of “good response group” and “poor response group” in 25 patients who did not participate in the telephone interview was not deviated to one side, the non-response would not have had a significant impact on the study results. Third, no control group was recruited. Fourth, various outcomes, such as sleep quality or psychological well-being, were not investigated. Lastly, the intergroup difference in gender ratio was not considered during analyzing the results. Hence, studies that compensate for these limitations are warranted in the future.
Abbreviation
NRS, numeric rating scale.
Data Sharing Statement
Data are available upon reasonable request made to the corresponding author.
Ethics Approval and Consent to Participate
The study has been approved by the Yeungnam University Hospital review board (2021-06-021). Informed consent was provided orally.
Author Contributions
All authors made a significant contribution to the work reported. All authors took part in the conception, study design, execution, acquisition of data, analysis and interpretation, drafting, revising or critically reviewing the article. All authors gave final approval of the version to be published, and have agreed on the journal to which the article has been submitted. Also, they agree to be accountable for all aspects of the work.
Funding
The present study was supported by a National Research Foundation of Korea grant funded by the Korean government (Grant No: NRF-2019M3E5D1A02069399).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Bannister G, Amirfeyz R, Kelley S, Gargan M. Whiplash injury. J Bone Joint Surg Br. 2009;91(7):845–850. doi:10.1302/0301-620X.91B7.22639
2. Godek P. Whiplash injuries. current state of knowledge. Ortop Traumatol Rehabil. 2020;22(5):293–302. doi:10.5604/01.3001.0014.4210
3. Chen HB, Yang KH, Wang ZG. Biomechanics of whiplash injury. Chin J Traumatol. 2009;12(5):305–314.
4. Ritchie C, Sterling M. Recovery pathways and prognosis after whiplash injury. J Orthop Sports Phys Ther. 2016;46(10):851–861. doi:10.2519/jospt.2016.6918
5. Kamper SJ, Rebbeck TJ, Maher CG, McAuley JH, Sterling M. Course and prognostic factors of whiplash: a systematic review and meta-analysis. Pain. 2008;138(3):617–629. doi:10.1016/j.pain.2008.02.019
6. Sameh E-S, Mahmoud E-R, Mohamed MMM, Mifsud Rooney P. Long-term follow-up of whiplash injury of the neck. J Orthop Trauma Rehabil. 2013;17:583.
7. Côté P, Cassidy JD, Carroll L, Frank JW, Bombardier C. A systematic review of the prognosis of acute whiplash and a new conceptual framework to synthesize the literature. Spine. 2001;26(19):E445–E458. doi:10.1097/00007632-200110010-00020
8. Hendriks EJM, Scholten-Peeters GGM, van der Windt DAWM, Neeleman-van der Steen CWM, Oostendorp RAB, Verhagen AP. Prognostic factors for poor recovery in acute whiplash patients. Pain. 2005;114(3):408–416. doi:10.1016/j.pain.2005.01.006
9. Norris SH, Watt I. The prognosis of neck injuries resulting from rear-end vehicle collisions. J Bone Joint Surg Br. 1983;65(5):608–611. doi:10.1302/0301-620X.65B5.6643566
10. Radanov BP, Sturzenegger M, Di Stefano G. Long-term outcome after whiplash injury. A 2-year follow-up considering features of injury mechanism and somatic, radiologic, and psychosocial findings. Medicine. 1995;74(5):281–297. doi:10.1097/00005792-199509000-00005
11. Pearson AM, Ivancic PC, Ito S, Panjabi MM. Facet joint kinematics and injury mechanisms during simulated whiplash. Spine. 2004;29(4):390–397. doi:10.1097/01.BRS.0000090836.50508.F7
12. Quinn KP, Dong L, Golder FJ, Winkelstein BA. Neuronal hyperexcitability in the dorsal horn after painful facet joint injury. Pain. 2010;151(2):414–421. doi:10.1016/j.pain.2010.07.034
13. Dory MA. Arthrography of the cervical facet joints. Radiology. 1983;148(2):379–382. doi:10.1148/radiology.148.2.6867328
14. Dussault RG, Nicolet VM. Cervical facet joint arthrography. J Can Assoc Radiol. 1985;36(1):79–80.
15. Hove B, Gyldensted C. Cervical analgesic facet joint arthrography. Neuroradiology. 1990;32(6):456–459. doi:10.1007/BF02426454
16. Ng A, Wang D. Cervical facet injections in the management of cervicogenic headaches. Curr Pain Headache Rep. 2015;19(5):484. doi:10.1007/s11916-015-0484-1
17. Roy DF, Fleury J, Fontaine SB, Dussault RG. Clinical evaluation of cervical facet joint infiltration. Can Assoc Radiol J. 1988;39(2):118–120.
18. Ji RR, Nackley A, Huh Y, Terrando N, Maixner W. Neuroinflammation and central sensitization in chronic and widespread pain. Anesthesiology. 2018;129(2):343–366. doi:10.1097/ALN.0000000000002130
19. Phillips K, Clauw DJ. Central pain mechanisms in chronic pain states–maybe it is all in their head. Best Pract Res Clin Rheumatol. 2011;25(2):141–154. doi:10.1016/j.berh.2011.02.005
20. Rasmussen MK, Kongsted A, Carstensen T, Jensen TS, Kasch H. Revisiting risk-stratified whiplash-exposed patients 12 to 14 years after injury. Clin J Pain. 2020;36(12):923–931. doi:10.1097/AJP.0000000000000877
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.