")
Back to Journals » Patient Preference and Adherence » Volume 9
Associations of quality of life, pain, and self-reported arthritis with age, employment, bleed rate, and utilization of hemophilia treatment center and health care provider services: results in adults with hemophilia in the HERO study
Authors Forsyth A, Witkop M , Lambing A, Garrido C, Dunn S , Cooper DL , Nugent D
Received 30 April 2015
Accepted for publication 3 September 2015
Published 29 October 2015 Volume 2015:9 Pages 1549—1560
DOI https://doi.org/10.2147/PPA.S87659
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Angela L Forsyth,1 Michelle Witkop,2 Angela Lambing,3 Cesar Garrido,4 Spencer Dunn,5 David L Cooper,6 Diane J Nugent7
1BioRx, Cincinnati, OH, USA; 2Munson Medical Center, Traverse City, MI, USA; 3Henry Ford Hospital, Detroit, MI, USA; 4Asociacion Venezolana para la Hemofilia, Caracas, Venezuela; 5Center for Inherited Blood Disorders, Orange, CA, USA; 6Novo Nordisk Inc., Plainsboro, NJ, USA; 7Children’s Hospital of Orange County, Center for Inherited Blood Disorders, Orange, CA, USA
Introduction: Severe hemophilia and subsequent hemophilic arthropathy result in joint pain and impaired health-related quality of life (HRQoL). Assessment of HRQoL in persons with hemophilia (PWH), including underlying factors that drive HRQoL differences, is important in determining health care resource allocation and in making individualized clinical decisions.
Aim: To examine potential associations between HRQoL, pain interference, and self-reported arthritis and age, employment, activity, bleed frequency, and hemophilia treatment center and health care professional utilization.
Methods: PWH (age ≥18 years) from ten countries completed a 5-point Likert scale on pain interference over the previous 4 weeks, the EQ-5D-3L scale (mobility, usual activities, self-care, pain/discomfort, anxiety/depression) including a health-related visual analog scale (0–100, coded as an 11-point categorical response).
Results: Pain interference (extreme/a lot) was higher in PWH aged >40 years (31%) compared to those aged 31–40 years (27%) or ≤30 years (21%). In an analysis of eight countries with home treatment, PWH who reported EQ-5D mobility issues were less likely to be employed (53% vs 79%, with no mobility issues). Median annual bleed frequency increased with worsening EQ-5D pain or discomfort. The percentage of PWH with inhibitors reporting visual analog scale scores of 80–90–100 was lower (20%) than those without inhibitors (34%). Median bleed frequency increased with pain. Globally, nurse and social worker involvement increased with disability and pain; physiotherapist utilization was moderate regardless of the extent of disability or pain.
Conclusion: Increased disability and pain were associated with increased age, lower employment, higher reported bleed frequency, and lower HRQoL.
Keywords: hemophilia, quality of life, HERO, pain
Introduction
Severe congenital hemophilia A (HA) and hemophilia B (HB) are associated with various types of bleeding, of which 70%–80% of bleeds are hemarthroses (joint bleeds).1 According to a retrospective data analysis of patients with severe hemophilia in the UK, the most common joints affected in adult persons with hemophilia (PWH) were the ankle (60.0%), knee (12.9%), and elbow (14.3%), although bleeding also occurred in the hips, shoulders, wrist, hands, and feet.2 Recurrent joint bleeding can result in acute and subsequent chronic hemophilic synovitis, leading to irreversible damage to joint cartilage and bone.1,3 Hemarthrosis, synovitis, and hemophilic arthropathy ultimately result in acute and persistent joint pain1,3 as well as progressive limitations in range of motion.4 Pain and functional impairment impact the patient’s employment, relationships, daily activities, and perceived quality of life.1
Measuring the health-related quality of life (HRQoL) of PWH, as well as assessing what affects a patient’s HRQoL, is important to inform policy decisions regarding health care resource utilization and in individual clinical decision-making.5 As treatment strategies evolve, interest has grown in measuring the HRQoL in PWH.5–7 Strategies to measure HRQoL have included standardized (eg, EQ-5D-3L, SF-36) and novel disease-specific instruments (Haemo-A-QoL, HaemoQoL, Hemophilia Activities List).8–10 The standard of care in developed countries is the comprehensive care model at hemophilia treatment centers (HTCs), and as part of that model, nurses, social workers, and physiotherapists, in part, spend time addressing psychosocial issues impacting HRQoL, including pain and functional impairment.
The Hemophilia Experiences, Results and Opportunities (HERO) study aimed to provide a large-scale global assessment of psychosocial issues (including employment, comorbidities, pain, functional impairment, relationships, HRQoL) affecting adults and children with hemophilia and their families in ten countries, as well as to assess treatment parameters and HTC/health care practitioner (HCP) utilization. The demographics and impact on employment and recreational activities have been described by Forsyth et al11 and issues relating to treatment and impact on relationships have also been discussed by Nugent et al12 and Cassis et al13 respectively.
The aim of this analysis is to describe the overall quality of life in adult respondents based on covariates identified in the primary analysis of HERO and to focus on patient HRQoL assessed by EQ-5D-3L, EQ-5D health-related visual analog scale (VAS), and categorical measure of pain interference in the previous 4 weeks. Additional post hoc analysis of covariates, including associations between EQ-5D and pain interference with employment, bleed frequency, and HTC/HCP utilization, included the eight countries (excludes Algeria and People’s Republic of China) that predominantly reported home infusion treatment. This study adds to the current understanding of HRQoL in adult PWH by providing a large multinational assessment of how multiple patient variables may affect overall quality of life. These results may be important for informing health policy decisions and may suggest opportunities to improve comprehensive patient care.
Methods
A detailed methodology of HERO has been described elsewhere.11 Briefly, the study used two online Web-based questionnaires (one for PWH and one for parents of affected children), each consisting of more than 100 items that included multiple choice questions and rating scales. In general, participants were recruited through national hemophilia organizations via email and Web pages. To address country-specific needs in Algeria, where access to the Internet is limited, participants were allowed to complete a paper version of the survey that was circulated by mail. In addition, an agency panel was used to collect the data in France. The original design of HERO was to evaluate a total of ~600 PWH (≥18 years old) and 600 parents responding on behalf of their oldest affected child (<18 years old) from 12 countries, with the goal of having 50 PWH and 50 parents from each country. Ethical approvals were secured in ten participating countries (Algeria, Argentina, Canada, People’s Republic of China, France, Germany, Italy, Spain, the UK, and the US), and informed consent was obtained where required. To ensure that the global enrollment targets were met, the 200 subjects from Japan and Brazil, and other unmet recruitment targets, were reallocated to larger countries (specifically the US and People’s Republic of China).11 The final number of survey respondents for each country were as follows: Algeria (n=50), Argentina (n=50), Canada (n=30), People’s Republic of China (n=110), France (n=50), Germany (n=60), Italy (n=43), Spain (n=41), the UK (n=52), and the US (n=189).
The current analyses reported here include adult males ≥18 years of age with HA or HB, with or without inhibitors. To define a population with moderate-to-severe hemophilia, adult PWH were required to have either 1) received regular replacement therapy or 2) had at least one spontaneous bleed into one or more joints within the previous 12 months. Inclusion criteria did not differ between countries. All adult PWH were asked to report comorbidities, including self-reported arthritis, and to complete an EQ-5D-3L (mobility, usual activities, self-care, pain/discomfort, anxiety/depression)14 and an EQ-5D VAS (0–100, coded electronically as an 11-point categorical response based upon the nearest value). Based on EQ-5D-3L responses, an EQ-5D index was derived using the methodology of Shaw et al.15 Treatment regimen (on-demand, prophylaxis, or on-demand with situational prophylaxis) was provided by each PWH/parent; however, the type (primary, secondary, situational), duration, and timing of current prophylaxis treatment were not collected.
Statistical analyses were primarily descriptive and correlative in nature, as the study was not powered for determinations of statistical significance. Primary analysis of HERO data was based on all adult PWH in the ten participating countries with cross tabulations by individual country. Subsequent post hoc analyses that included HTC utilization and HCP involvement in management were based on the results of eight countries. To minimize the impact of additional utilization around acute bleed treatment (eg, factor infusions) at the HTC reported by most of the respondents from Algeria and People’s Republic of China, the eight countries analyzed were those that employed predominantly home infusion treatment. The same post hoc analysis was completed separately for PWH respondents from the US, who accounted for a large percentage (37%) of patients in the eight-country analysis. In addition, there are published values for HRQoL (specifically EQ-5D index) for the general US population, which allows for comparison to the HERO hemophilia population.
Results
Patient demographics
Detailed patient demographics, including cross tabulations by country, have been published previously.11 Among the 675 adult PWH from ten countries who completed the survey, the median (interquartile range, IQR) age was 36 (28–45) years with an overall range of 18–86 years. For all adult PWH, the majority (74%) reported HA, with 13% reporting HB and 13% reporting hemophilia with inhibitors. Of the 91 patients reporting hemophilia with inhibitors (median age, 34 years), 45 were from the US (median age, 33 years). The most common reported comorbidities associated with hemophilia were self-reported arthritis (49%), hepatitis C virus (43%), and/or human immunodeficiency virus (18%). Excluding patients from Algeria and People’s Republic of China, the median (IQR) age for the eight-country subset was 38 (30–48) years, and for the US, it was 35 (28–41) years. Other demographic parameters were similar to those reported above for the subset of eight countries included in post hoc analyses, including the US (Table S1).
Pain interference
Overall, 89% of adult PWH reported that they experienced pain that interfered with activities in the previous 4 weeks; 26% of adult PWH reported that in the past 4 weeks, pain interfered with their daily life “extremely” or “quite a lot”. The percentage of adults >40 years old (31%) reporting “extreme” or “quite a lot” of pain interference was higher than that of adults aged 31–40 years (27%) or ≤30 years (21%). The percentage of adults reporting “extreme” or “quite a lot” of pain interference was also higher in those with self-reported arthritis (35% vs 15% without) (Figure 1A). Similar results were seen in patients from the US, with a slightly higher percentage (41%) aged >40 years and a lower percentage (9%) aged ≤30 years, reporting “extreme” or “quite a lot” of pain interference (Figure 1B).
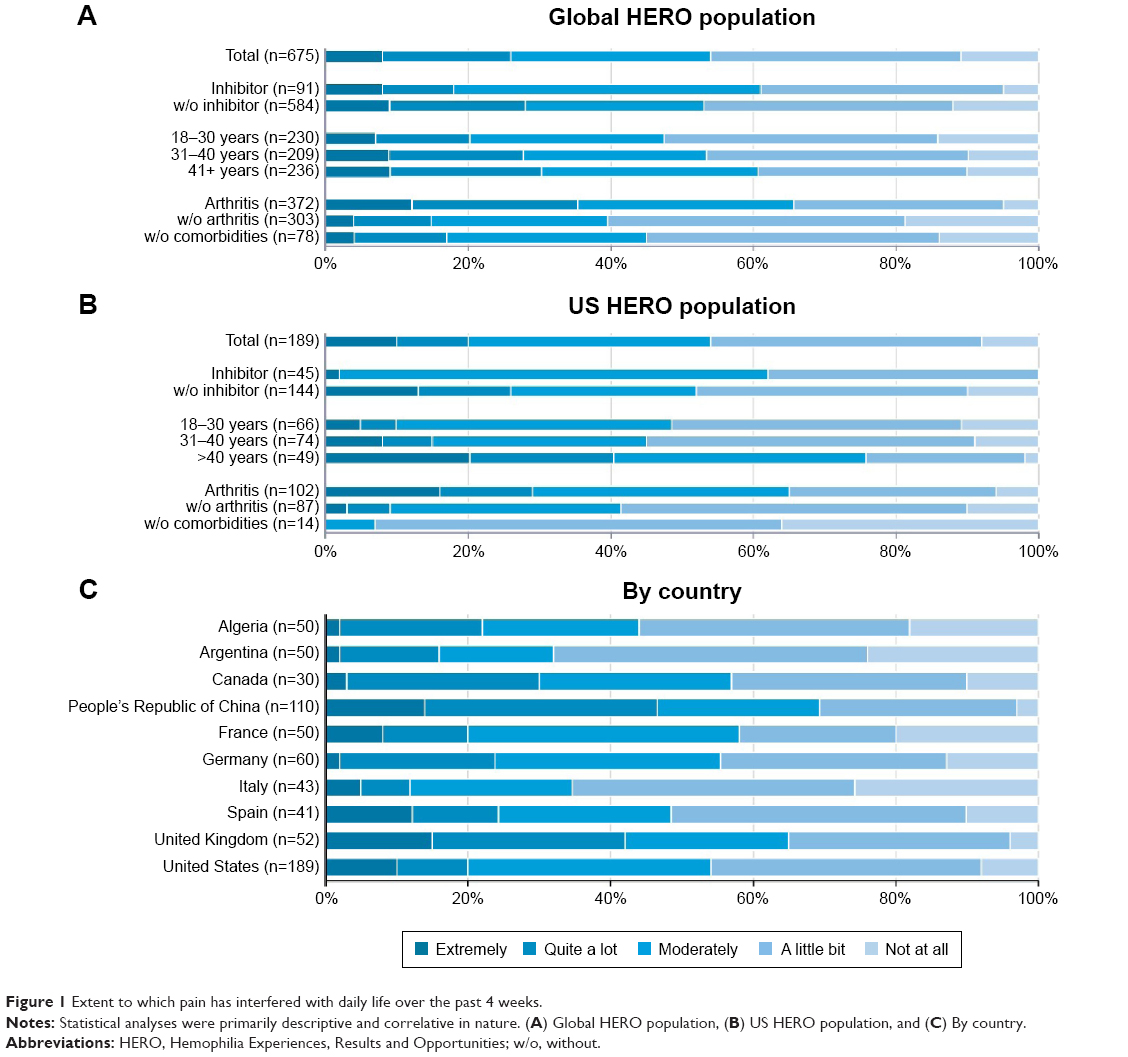 | Figure 1 Extent to which pain has interfered with daily life over the past 4 weeks. |
Of patients with inhibitors, 18% reported “extreme” or “quite a lot” of pain interference compared to 27% of patients with HA and 29% of patients with HB. This may be driven by the fact that half (45/91, 49%) of the patients with inhibitors were from the US,12 were younger, and reported a high frequency of prophylactic use (22/45 [49%]); only 2% of US patients with inhibitors reported “extreme” or “quite a lot” of pain interference, compared to 27% of patients with HA and 18% of patients with HB. In addition, the global inhibitor population was slightly younger (median age, 34 years) than patients with HA or HB (median age, 36 years for each; Table 1). The extent of pain interference by country is shown in Figure 1C.
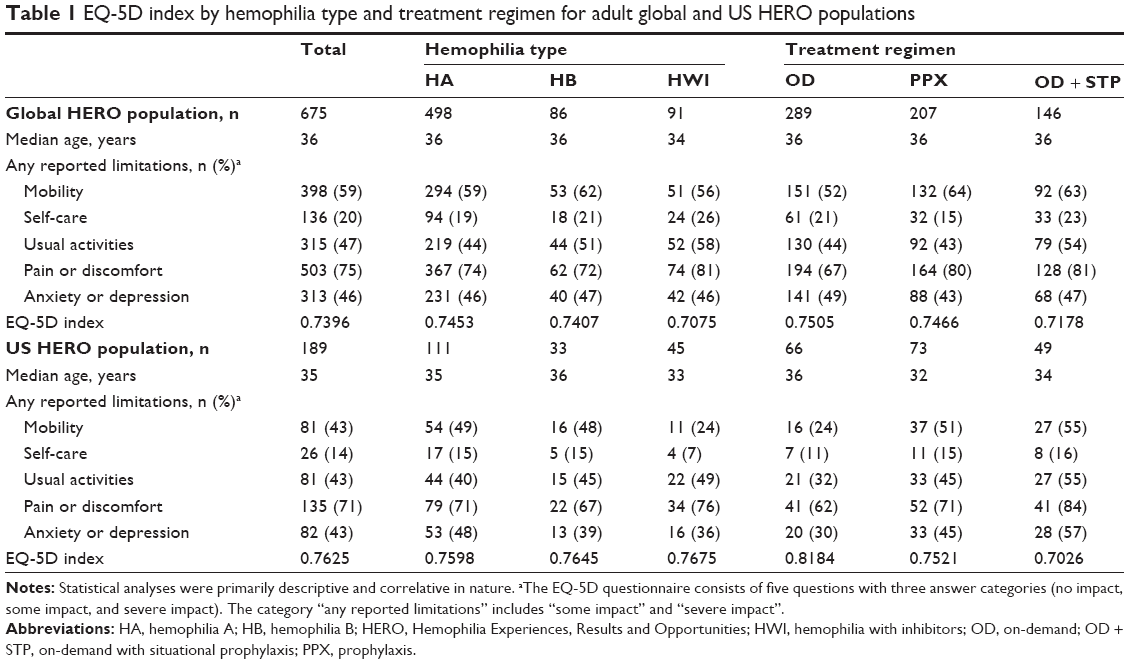 | Table 1 EQ-5D index by hemophilia type and treatment regimen for adult global and US HERO populations |
Adults were most likely to report that they experience pain only when a bleed occurs (42%), while 21% reported persistent pain and 29% reported persistent pain that worsens when they have a bleed; 8% reported they did not know when their pain occurred. Those who were employed were more likely to report pain only when a bleed occurs (eg, no persistent pain) than those who were not employed (48% vs 31%). PWH with self-reported arthritis were more likely to report persistent pain (pain all the time or pain all the time that worsens when they have a bleed) than those without (62% vs 34%).
EQ-5D components, index, and VAS
More than half (59%) the adult patients reported problems with mobility (Table 1). Adults on prophylaxis (type, duration, timing, and extent during lifetime not documented) reported more issues with mobility (64% vs 52% on-demand). Most patients (75%) reported moderate or extreme pain or discomfort (Tables 1 and 2). Adults currently on prophylaxis reported more pain or discomfort (80%) than those treated on-demand (67%). Adults with inhibitors reported slightly more pain or discomfort (81%) than those with HA (74%) or HB (72%). EQ-5D component scores varied between countries (Table 2).
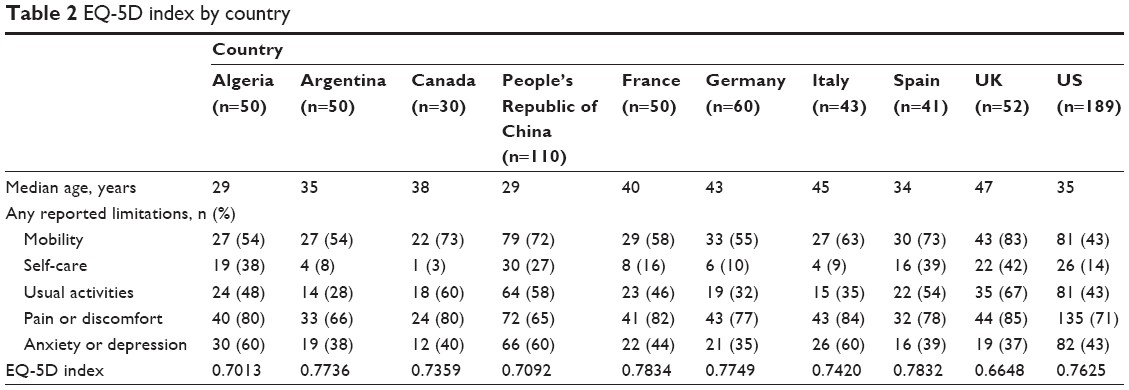 | Table 2 EQ-5D index by country |
The EQ-5D index for all adult patients who participated in HERO, tabulated by hemophilia type and treatment regimen, is shown in Table 1. Treatment was categorized based on current treatment and may not be reflective of any/all prior treatment since diagnosis or the extent to which the patients received prophylaxis during their life. In the global population, the mean EQ-5D index was higher (which reflects a better health state) in adults treated on-demand (0.7505) or on prophylaxis (0.7466) than those treated on-demand plus short-term prophylaxis (0.7178). In the US, adult respondents currently treated on-demand had a higher EQ-5D index (0.8184) than those who were on prophylaxis (0.7521) or treated on-demand plus short-term prophylaxis (0.7026). In the global population, EQ-5D index was similar for those with HA and HB (0.7453 and 0.7407), but lower in PWH with inhibitors (0.7075). In the slightly younger US respondent population with a greater percentage of inhibitor patients on prophylaxis and without pain interference, EQ-5D index was similar in patients with HA, HB, or hemophilia with inhibitors (0.7598, 0.7645, and 0.7675, respectively). EQ-5D index is also shown by country in Table 2. Compared to the normative US population, patients with hemophilia (both globally and in the US) have a lower EQ-5D index score for all age groups and exhibit a decrease in index with advancing age (Table 3).
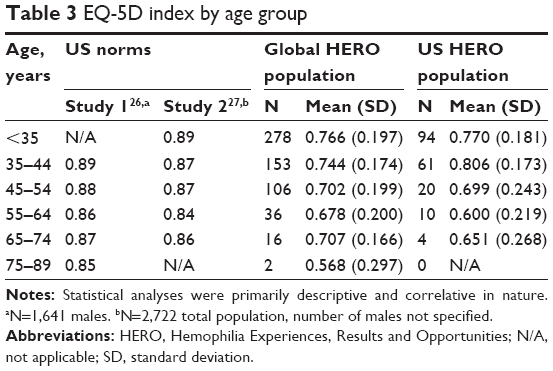 | Table 3 EQ-5D index by age group |
In total, 32% of adults reported “good” VAS health scores (reported categorically as 80–90–100). The percentage of adults with inhibitors reporting “good” VAS health scores was lower, compared to those without inhibitors, for both the global (20% vs 34% without) (Figure 2A) and US (24% vs 48% without) populations (Figure 2B). Those who were employed were more likely to report good scores than those who were not employed (36% vs 20%). PWH without self-reported arthritis also more often reported good scores than those with self-reported arthritis (44% vs 23%).
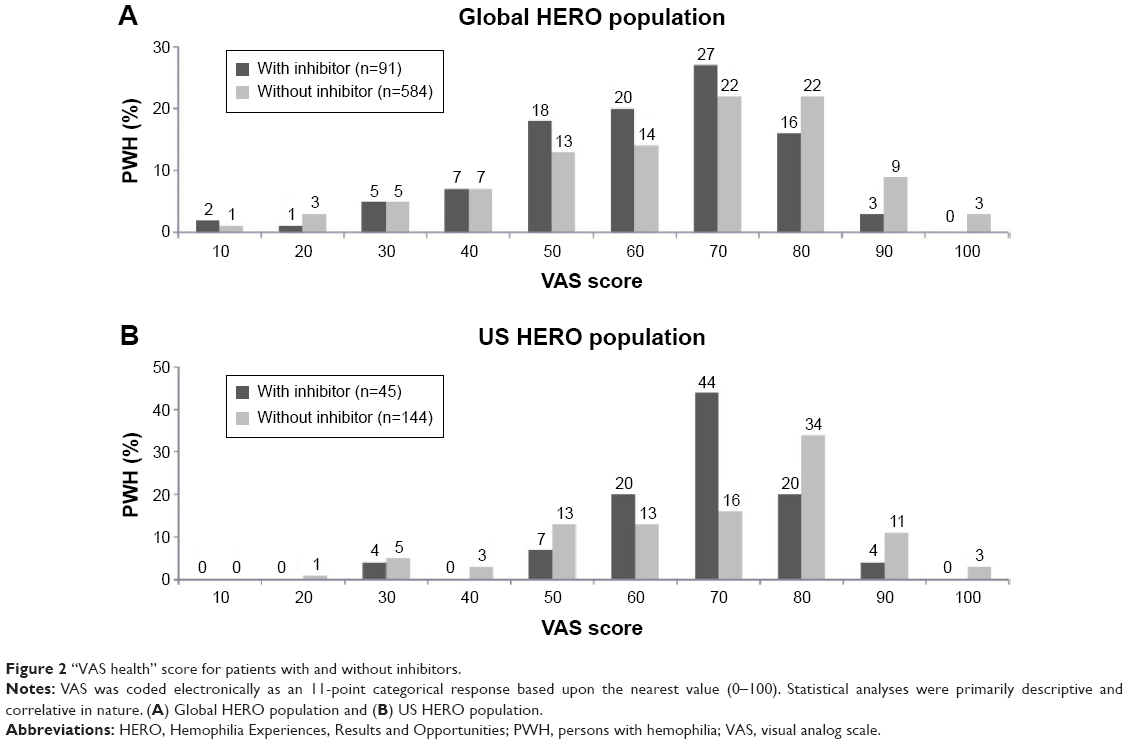 | Figure 2 “VAS health” score for patients with and without inhibitors. |
Associations with employment
Overall, 80% reported that hemophilia had a negative impact on employment. Fewer PWH with inhibitors reported no negative impact (5% vs 21% without).11 Most adults were employed full- or part-time or self-employed (60%), with few unemployed and looking for a job (8%); 13% were unable to work due to long-term disability.11
In the post hoc analysis of eight countries (included only those with predominantly home infusion treatment), adult PWH who reported EQ-5D mobility issues were less likely to be employed full- or part-time or self-employed (53% vs 79% with no mobility issues) (Figure 3A); this was true of adult PWH in the US analysis (55% vs 85% with no mobility issues) (Figure 3A). Adults who reported extreme EQ-5D pain/discomfort were less likely to be employed (31% vs 84% with no pain/discomfort; 35% vs 93%, respectively in US adults) (Figure 3A). Adults who reported a pain interference rating of a lot/extreme pain or discomfort were less likely to be employed (41% employed) compared to those reporting none/a little bit (73%) or moderate (67%) pain interference. US adults also reported lower employment with increasing pain interference (a lot/extreme, 38%; moderate, 73%; and none/a little bit, 88%) (Figure 3A).
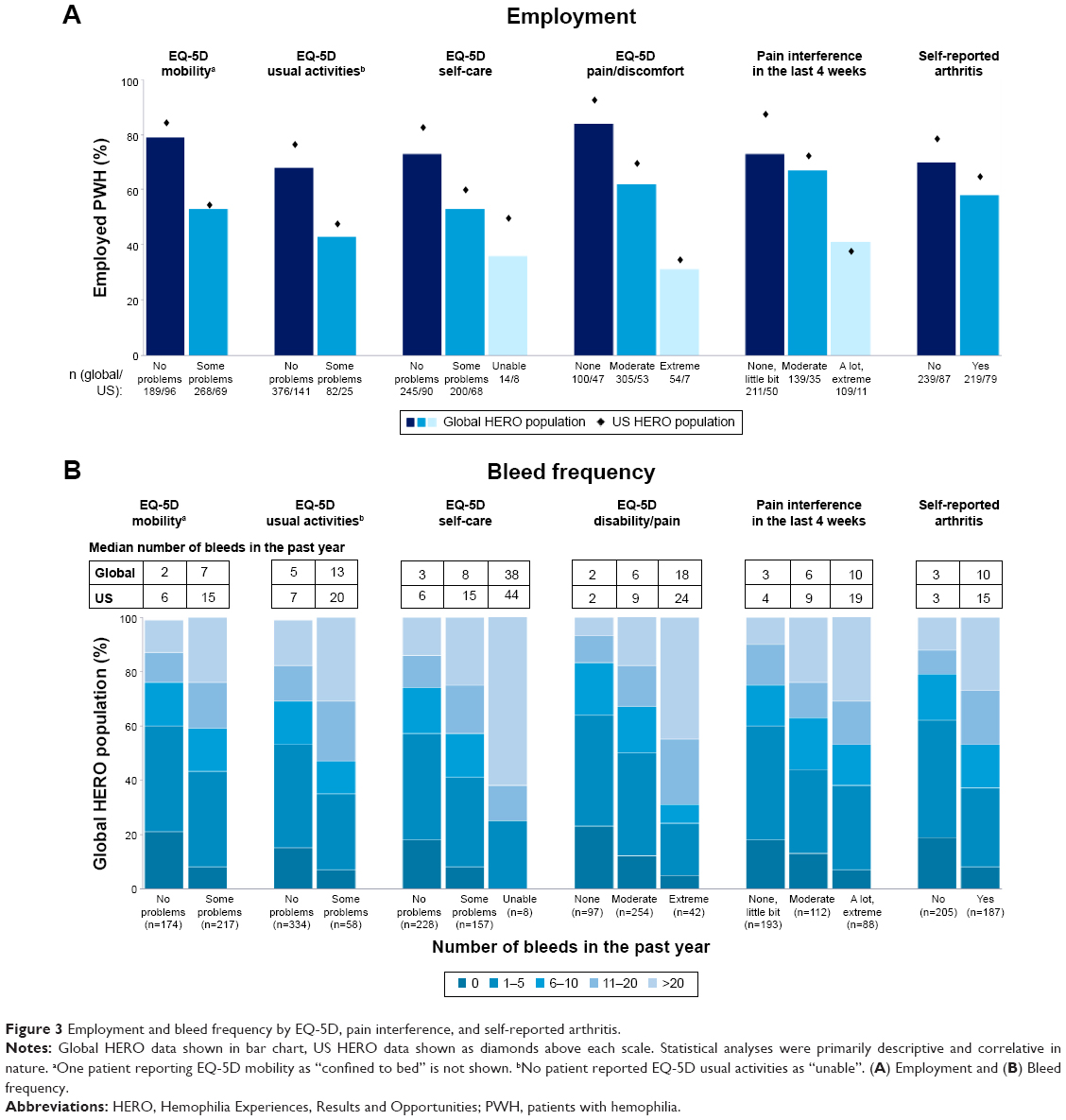 | Figure 3 Employment and bleed frequency by EQ-5D, pain interference, and self-reported arthritis. |
Associations with bleeding frequency
Spontaneous bleeding was reported by most PWH with HA (76%) or HB (67%) and was higher in those with inhibitors (93%).11 Median (IQR) number of bleeds in the past year was 7 (2–20) with a nonnormal distribution due to outliers with higher bleeding rates.11 In the eight countries with home treatment, adults who reported any EQ-5D mobility issues reported a higher median bleed frequency (7) in the past year compared to those with no issues (2) (Figure 3B). This was also seen in US patients (15 with issues vs 6 with no issues) (Figure 3B).
Median bleed frequency in the past year increased with worsening EQ-5D pain or discomfort for both those countries with home treatment (extreme, 18; moderate, 6; none, 2; Figure 3B) and US (a lot/extreme, 24; moderate, 9; none, 2; Figure 3B) respondents. Adults who self-reported arthritis and those with increased pain interference also reported higher bleed frequencies (Figure 3B).
Associations with HCP utilization
Adults from all ten countries were most likely to report that a hematologist (89%) or hemophilia nurse (51%) was involved in the management of their hemophilia. Fewer adult PWH reported involvement of a physiotherapist (35%), general practitioner (22%), social worker (16%), counselor or psychologist (12%), or complementary therapist (eg, acupuncture, massage; 5%). Availability of each of these HCP specialists at the HTC level was not documented, and the term “management” was left to the patient’s interpretation.
In the eight-country analysis, adults who reported moderate EQ-5D mobility issues were slightly more likely than those with no mobility issues to report nurse involvement (56% vs 48%) and social worker involvement (22% vs 17%) in their hemophilia management; physiotherapist involvement did not vary (38% vs 36%; Figure 4). In the US respondents, those reporting moderate EQ-5D mobility issues reported less frequent involvement of physiotherapists in management (33%) than those without mobility issues (45%). US adults who reported any EQ-5D mobility issues were more likely than those with no mobility issues to report nurse involvement (83% vs 69%) and social worker involvement (56% vs 33%) in their hemophilia management.
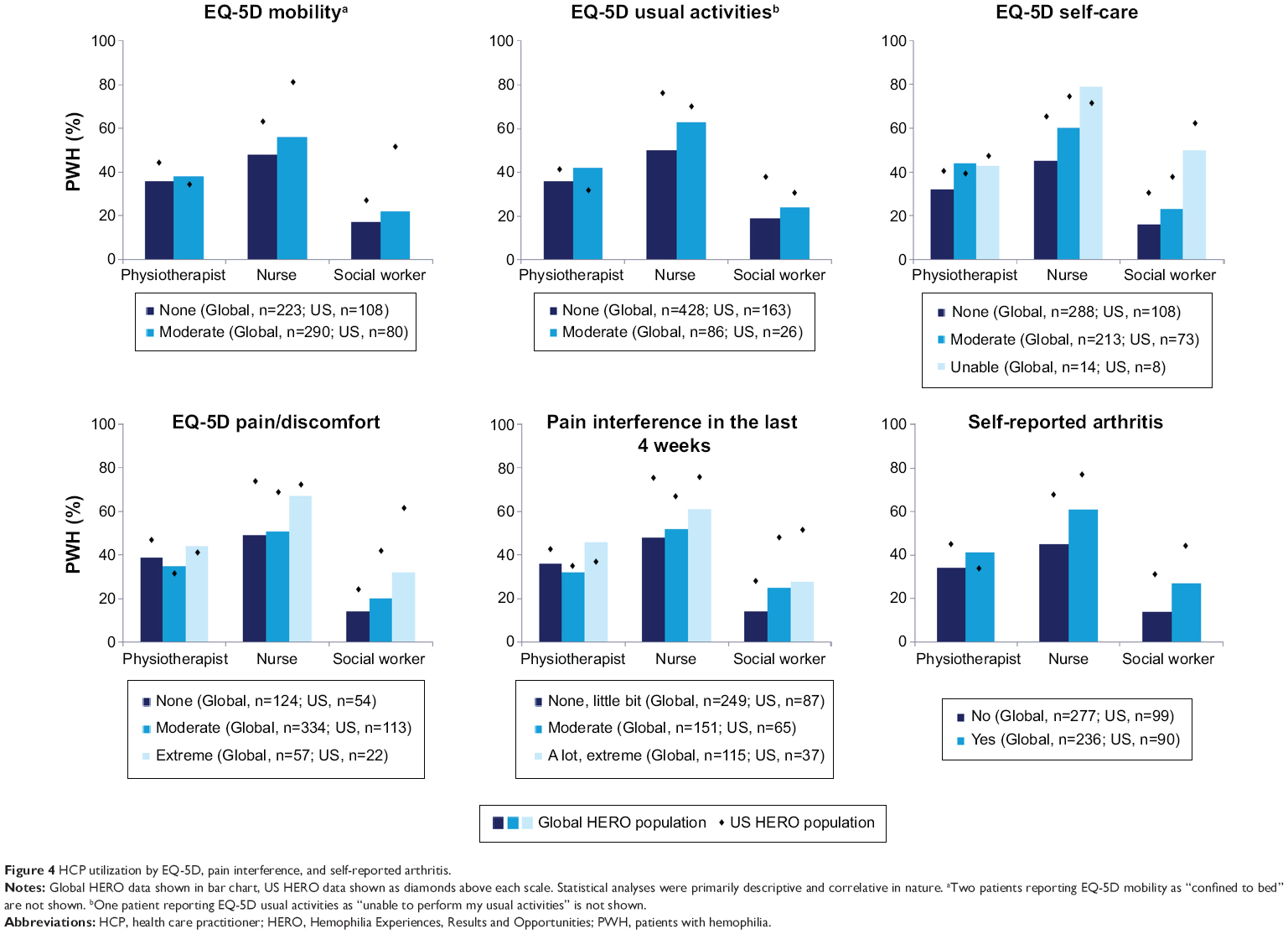 | Figure 4 HCP utilization by EQ-5D, pain interference, and self-reported arthritis. |
Similarly, adults who reported EQ-5D extreme pain or discomfort were more likely than those with no pain or discomfort to report nurse involvement (67% vs 49%, respectively) and social worker involvement (32% vs 14%, respectively); this did not change as much for physiotherapist involvement (44% vs 39%, respectively; Figure 4). Adult PWH who self-reported arthritis were more likely than those who did not report to identify nurse involvement (61% vs 45%, respectively), social worker involvement (27% vs 14%, respectively), and physiotherapist involvement (41% vs 34%, respectively; Figure 4). For US respondents, those with extreme EQ-5D pain and discomfort reported lower physiotherapist involvement (41%) than those without pain and discomfort (54%); adults who reported extreme EQ-5D pain or discomfort were no more likely than those with no pain or discomfort to report nurse involvement (77% vs 78%, respectively) and were more likely to report social worker involvement (64% vs 26%) in their hemophilia management. US adults with self-reported arthritis reported lower physiotherapist involvement (30%) than those without arthritis (48%) but identified more nurse involvement (80% vs 70%, respectively) and social worker involvement (52% vs 34%, respectively; Figure 4).
Discussion
This analysis of the HERO study data identifies important associations between HRQoL and various patient- and disease-related characteristics. It has previously been reported that patients with hemophilia complicated by inhibitors experience a lower HRQoL.16,17 This finding is supported by the current analysis of the global (ten-country) population of adult PWH respondents in HERO, in which patients with inhibitors reported a lower EQ-5D index (0.7075) than those with HA (0.7453) or HB (0.7407) and greater pain interference compared to patients without inhibitors. Other studies have also found the severity of disease to affect HRQoL and EQ-5D index. In a UK study, 67 PWH with severe hemophilia were shown to exhibit a lower median EQ-5D index score than 101 PWH with moderate/mild hemophilia (0.66 and 0.85, respectively);18 the low HRQoL of patients with severe hemophilia is also supported by a similar study of 72 adults with severe HA or HB, which reported a mean EQ-5D utility of 0.64.18 Furthermore, the Hemophilia Utilization Group Study Va (HUGS-Va) found physical component scores (PCS-12, component of the Short Form-12 Health Survey) to be decreased with increasing severity of disease.19 EQ-5D index values reported in the current study, which included patients with moderate-to-severe hemophilia (mean, 0.7396; 0.7625 in the US), are therefore expected to be lower than for patients with mild/moderate hemophilia.
Consideration must be given to the home country of each participant when assessing patient-reported HRQoL. The perceptions, descriptions, open discussions, and control of pain are culture and country specific;20 therefore, PWH from one country may have a different perception of their pain than PWH from other countries. Ethnicity and culture also affect the expression or verbal description of pain and may influence the way in which patients respond to pain assessment questions.21 This may account for some of the variability in pain interference between countries participating in HERO.
An additional patient variable that may influence HRQoL is history of a prophylactic treatment regimen, as suggested by multiple published studies.22–24 Significant differences in HRQoL have been found between Swedish patients, who have had access to prophylaxis since the 1970s, and patients from Ireland, the UK, and France, where prophylaxis was not routine until the 1990s; patients from Sweden spent more of their life on prophylaxis (P≤0.05) and had the lowest annual bleed rates, a lower presence of target joints (P≤0.001), and the highest EQ-5D utility value (0.93) compared with those from the other countries (0.68–0.76).22 Furthermore, when pooled across countries, those on lifetime prophylaxis (100%) had higher mean EQ-5D utility values (0.88) compared with those treated only in part with prophylaxis (0.77–0.79) or treated exclusively on-demand (0.72).22 Important effects of prophylaxis on HRQoL are also supported by a recent multinational survey of 116 adults, which found EQ-5D index scores to increase with time spent on prophylaxis; patients always treated on-demand had a lower EQ-5D index (0.619) than those who spent <50% of their life on prophylaxis (0.755), those who spent ≥50% of their life on prophylaxis (0.812), and those who were always on prophylaxis (0.866).23 Prophylaxis with recombinant activated factor VII (rFVIIa) has also been shown to improve HRQoL in patients with inhibitors; patients who participated in a prospective trial and received rFVIIa prophylactically for 3 months followed by 3 months of postprophylaxis (treated on-demand) showed improvements in EQ-5D index (mean, 0.68) compared to the preprophylaxis period (mean, 0.65).24
Bleed type and the number of bleeding episodes may also affect EQ-5D index and pain. In the current analysis, increased bleed frequency was associated with worsening EQ-5D and more pain interference. PWH treated with on-demand plus short-term prophylaxis had the lowest EQ-5D index and, as indicated in previous reports of HERO study data, had the highest median annual bleed frequency (20) compared to those treated on-demand (5) or with prophylaxis (5).12 Important effects of bleeds on HRQoL are also supported by data from the Dosing Observational Study in Hemophilia (DOSE), a diary study that evaluated the use of bypassing agents, with a focus on the use of rFVIIa in the home setting, and captured EQ-5D on a daily basis.25 PWH with inhibitors in DOSE reported significantly lower EQ-5D index scores on bleed days (mean ± standard deviation: 0.64±0.23) compared to nonbleed days (0.84±0.16, P<0.001 vs nonbleeding days), indicating significantly reduced HRQoL associated with each bleeding episode.25 Additionally, results from an international survey of adult PWH found that those treated on-demand had a worse EQ-5D index and were more likely to report more than 30 bleeds in the past year (61%) compared to those who spent <50% of their life on prophylaxis (3%) or ≥50% of their life on prophylaxis (0%) or were always on prophylaxis (0%).23 HRQoL may also be considerably worse in PWH who experience more pain; results from the international survey showed that PWH with the least exposure to prophylactic treatment (associated with the worst reported HRQoL) were most likely to report daily pain.23 Furthermore, results from the HUGS-Va study showed HRQoL to be worse in patients who reported more pain, as assessed by PCS-12 scores.19
Previous analysis of the HERO study data indicated that adult PWH reported a median of 2 HTC visits in the past year; this was lower in the US population (median, 1).12 Even though US PWH are visiting HTCs less, they reported more nurse (75% vs 51%) and social worker (43% vs 16%) involvement in the management of their hemophilia than the global population.12 In the current analysis of the global population, nurse and social worker involvement was more commonly reported in association with worsening EQ-5D and increased pain interference. Nurse involvement in the US varied by EQ-5D disability and pain interference. Social worker involvement in the US was associated with worsening EQ-5D and increased pain interference, as also seen in the global population. Across all adult PWH respondents, the amount of physiotherapist involvement was similar in the US (40%) compared to the global population (35%).12 Globally, physiotherapist involvement increased with worsening EQ-5D and increased pain interference. In the US respondents, physiotherapist involvement was more frequently reported in association with better EQ-5D and less pain interference. Physiotherapist involvement in management of hemophilia may be lower than nurse involvement in PWH for a variety of reasons. One reason may be a lack of availability and utilization of physiotherapists at an individual HTC or the distance of the HTC from the PWH’s home, as PWH/parents may not want to travel a great distance for physiotherapist appointments. In the US, it may be due to lack of insurance coverage for physiotherapists (for both comprehensive care visits and subsequent therapy) or the lack of full-time physiotherapists at each HTC. However, the HERO study did not specifically ask PWH which HCPs were readily available or they had seen at their HTC, but rather those who were involved in the management of hemophilia. Therefore, the overall low involvement of social workers and physiotherapists may be variably due to either narrow perceptions of what constitutes management (eg, doctor who prescribes treatment) or a true lack of availability at individual HTCs within each country.
Conclusion
As a patient-reported study, HERO gives a unique perspective on life with hemophilia for adult PWH. Increased disability and pain were associated with increased age, lower employment, higher reported bleed frequency, and lower HRQoL. Adults who reported experiencing more pain were more likely to report suffering from what they self-reported as arthritis and to have more issues with mobility. Results suggest that more can be done to achieve the standard of true comprehensive care, including greater participation of physiotherapists, social workers, and counselors across HTCs with varied resources.
Acknowledgments
AL Forsyth, C Garrido, DL Cooper, D Nugent performed/designed the research; AL Forsyth, C Garrido, DL Cooper, D Nugent provided clinical insights to the study design and results; and all authors (AL Forsyth, M Witkop, A Lambing, C Garrido, S Dunn, DL Cooper, D Nugent) contributed to the writing/review of the manuscript. The authors acknowledge the assistance of Kantar Health (Surrey, UK), who managed the study and provided primary statistical analysis under funding by Novo Nordisk Inc. Secondary statistical analysis (US-specific data and eight-country data) was provided by Novo Nordisk A/S. Editorial assistance was provided by Amanda Tricarico, PhD, ETHOS Health Communications, Newtown, Pennsylvania, with financial assistance from Novo Nordisk Inc., in compliance with international guidelines on Good Publication Practice.
Disclosure
Dr David Cooper is an employee of Novo Nordisk Inc. All other authors for this manuscript were involved as part of their institution’s participation as a study site and have otherwise no direct or indirect financial relationships with the sponsor and received no remuneration for authorship. Angela Forsyth has been a paid consultant and speaker for Novo Nordisk along with all other major Pharma companies. There was no fee paid for participating in writing and submitting this paper for publication. Michelle Witkop has received grant funding from Pfizer, Inc., is on advisory boards with Baxter BioScience, Novo Nordisk, and Pfizer, and is on the speakers bureau at Novo Nordisk. Angela Lambing is currently employed with Bayer Health Care. At the time of this research, she was employed at the Henry Ford Hemophilia Treatment Center. There are no competing interests at this time. Cesar Garrido stated that he had no interests that might be perceived as posing a conflict or bias. David Cooper, MD, MBA, is an employee of Novo Nordisk Inc., the company that sponsored the HERO study. Diane Nugent stated that she had no interests that might be perceived as posing a conflict or bias.
Data in the manuscript have been presented, in part, as a poster at the following congress meetings: NHF’s 65th Annual Meeting, October 3–5, 2013, Anaheim, CA, USA; XXIV Congress of the International Society on Thrombosis and Haemostasis, June 29–July 4, 2013, Amsterdam, the Netherlands; World Federation of Hemophilia, WFH 13th International Musculoskeletal Congress 2013, April 18–21, 2013, Chicago, IL, USA; NHF’s 64th Annual Meeting, November 8–10, 2012, Orlando, FL, USA. The authors report no other conflicts of interest in this work.
References
World Federation of Hemophilia. Guidelines for the Management of Hemophilia. 2nd ed. Montreal, Quebec, Canada: World Federation of Hemophilia; 2013. | ||
Stephensen D, Tait RC, Brodie N, et al. Changing patterns of bleeding in patients with severe haemophilia A. Haemophilia. 2009;15(6):1210–1214. | ||
Rodriguez-Merchan EC. Musculoskeletal complications of hemophilia. HSS J. 2010;6(1):37–42. | ||
Soucie JM, Cianfrini C, Janco RL, et al. Joint range-of-motion limitations among young males with hemophilia: prevalence and risk factors. Blood. 2004;103(7):2467–2473. | ||
Aledort L, Bullinger M, von Mackensen S, Wasserman J, Young NL, Globe D. Why should we care about quality of life in persons with haemophilia? Haemophilia. 2012;18(3):e154–e157. | ||
Globe D, Young NL, Von Mackensen S, Bullinger M, Wasserman J. Measuring patient-reported outcomes in haemophilia clinical research. Haemophilia. 2009;15(4):843–852. | ||
Gringeri A, Von Mackensen S. Quality of life in haemophilia. Haemophilia. 2008;14(Suppl 3):19–25. | ||
Fischer K, van der Bom JG, van den Berg HM. Health-related quality of life as outcome parameter in haemophilia treatment. Haemophilia. 2003;9(Suppl 1):75–81; discussion 82. | ||
Pollak E, Muhlan H, von Mackensen S, Bullinger M; Haemo-QoL Group. The Haemo-QoL index: developing a short measure for health-related quality of life assessment in children and adolescents with haemophilia. Haemophilia. 2006;12(4):384–392. | ||
von Mackensen S, Gringeri A. Quality of life in hemophilia. In: Handbook of Disease Burdens and Quality of Life Measures. Vol 3. Heidelberg, Germany: Springer; 2009:1895–1920. | ||
Forsyth AL, Gregory M, Nugent D, et al. Haemophilia Experiences, Results and Opportunities (HERO) study: survey methodology and population demographics. Haemophilia. 2014;20(1):44–51. | ||
Nugent D, Kalnins W, Querol F, et al. Haemophilia Experiences, Results and Opportunities (HERO) study: treatment-related characteristics of the population. Haemophilia. 2015;21(1):e26–e38. | ||
Cassis FR, Buzzi A, Forsyth A, et al. Haemophilia Experiences, Results and Opportunities (HERO) study: influence of haemophilia on interpersonal relationships as reported by adults with haemophilia and parents of children with haemophilia. Haemophilia. 2014;20(4):e287–e295. | ||
EuroQol Group. EuroQol – a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199–208. | ||
Shaw JW, Johnson JA, Coons SJ. US valuation of the EQ-5D health states: development and testing of the D1 valuation model. Med Care. 2005;43(3):203–220. | ||
Gringeri A, Mantovani LG, Scalone L, Mannucci PM. Cost of care and quality of life for patients with hemophilia complicated by inhibitors: the COCIS Study Group. Blood. 2003;102(7):2358–2363. | ||
Bastani P, Pourmohamadi K, Karimi M. Quality of life in hemophilia complicated by inhibitors. Iran Red Crescent Med J. 2012;14(4):250–251. | ||
Miners AH, Sabin CA, Tolley KH, Jenkinson C, Kind P, Lee CA. Assessing health-related quality-of-life in individuals with haemophilia. Haemophilia. 1999;5(6):378–385. | ||
Poon JL, Zhou ZY, Doctor JN, et al. Quality of life in haemophilia A: Hemophilia Utilization Group Study Va (HUGS-Va). Haemophilia. 2012;18(5):699–707. | ||
Free MM. Cross-cultural conceptions of pain and pain control. Proc (Bayl Univ Med Cent). 2002;15(2):143–145. | ||
Lasch KE. Culture and pain. Int Assoc Study Pain. 2002;10(5). | ||
Noone D, O’Mahony B, Prihodova L. A survey of the outcome of prophylaxis, on-demand or combined treatment in 20–35 year old men with severe haemophilia in four European countries. Haemophilia. 2011;17(5):e842–e843. | ||
Noone D, O’Mahony B, van Dijk JP, Prihodova L. A survey of the outcome of prophylaxis, on-demand treatment or combined treatment in 18–35-year old men with severe haemophilia in six countries. Haemophilia. 2013;19(1):44–50. | ||
Hoots WK, Ebbesen LS, Konkle BA, et al. Secondary prophylaxis with recombinant activated factor VII improves health-related quality of life of haemophilia patients with inhibitors. Haemophilia. 2008;14(3):466–475. | ||
Neufeld EJ, Recht M, Sabio H, et al. Effect of acute bleeding on daily quality of life assessments in patients with congenital hemophilia with inhibitors and their families: observations from the dosing observational study in hemophilia. Value Health. 2012;15(6):916–925. | ||
Fryback DG, Dunham NC, Palta M, et al. US norms for six generic health-related quality-of-life indexes from the National Health Measurement study. Med Care. 2007;45(12):1162–1170. | ||
Revicki DA, Kawata AK, Harnam N, Chen WH, Hays RD, Cella D. Predicting EuroQol (EQ-5D) scores from the patient-reported outcomes measurement information system (PROMIS) global items and domain item banks in a United States sample. Qual Life Res. 2009;18(6):783–791. |
Supplementary material
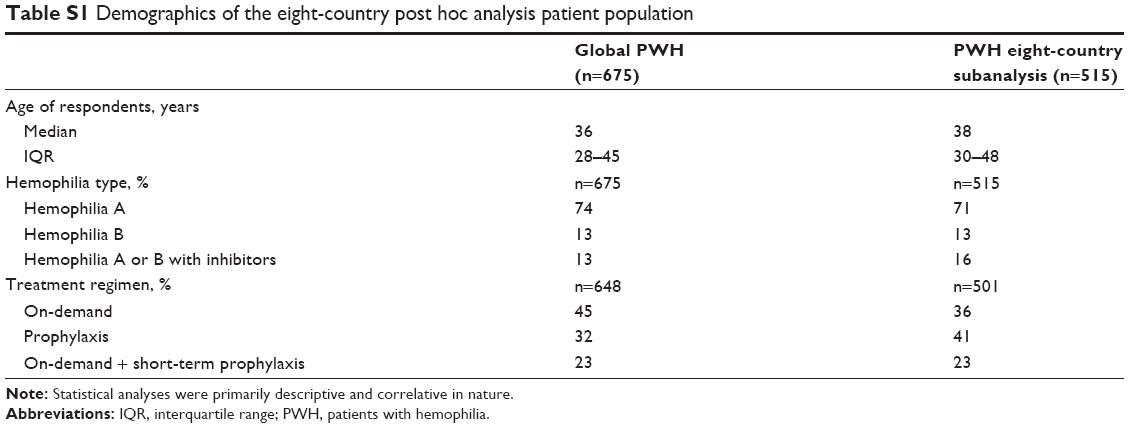 | Table S1 Demographics of the eight-country post hoc analysis patient population |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.