")
Back to Journals » OncoTargets and Therapy » Volume 10
Associations of NQO1 C609T and NQO1 C465T polymorphisms with acute leukemia risk: a PRISMA-compliant meta-analysis
Authors He H, Zhai X, Liu X, Zheng J, Zhai Y, Gao F, Chen Y, Lu J
Received 18 January 2017
Accepted for publication 3 March 2017
Published 23 March 2017 Volume 2017:10 Pages 1793—1801
DOI https://doi.org/10.2147/OTT.S132503
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr William C. Cho
Hairong He,1 Xiaoyu Zhai,1,2 Xiaomin Liu,3 Jie Zheng,1 Yajing Zhai,4 Fan Gao,1 Yonghua Chen,5 Jun Lu1
1Clinical Research Center, 2College of Pharmacy, Xi’an Medical University, 3Dialysis Department of Nephrology Hospital, 4Department of Pharmacy, The First Affiliated Hospital of Xi’an Jiaotong University, 5School of Public Health, Xi’an Jiaotong University, Xi’an, China
Objective: The NAD(P)H:quinone oxidoreductase (NQO1) C609T and C465T polymorphisms have been widely thought to be associated with the risk of acute leukemia (AL) in recent years, but the correlations are still unclear. A meta-analysis is generally acknowledged as one of the best methods for secondary research, and so it was applied in this study with the aim of elucidating how the NQO1 C609T and C465T polymorphisms are related to the risk of AL.
Methods: Relevant studies were searched in the PubMed, EMBASE, CNKI, and Wanfang databases, and the obtained data were analyzed using Stata (version 12.1). The allele-contrast model was applied, and odds ratios (ORs) with 95% confidence intervals (CIs) were used to evaluate relationship strengths. Meta-regression was used to identify sources of heterogeneity, and subgroup analyses were conducted. Publication bias was analyzed using funnel plots, with the trim-and-fill method used to analyze the effect of publication bias on pooled results. In addition, sensitivity analysis, the fail-safe number method, and cumulative analysis by publication year were performed to measure the stability of the obtained results.
Results: This meta-analysis included 28 relevant studies involving 5,953 patients and 8,667 controls. Overall, the C609T polymorphism was associated with the risk of acute lymphoblastic leukemia (ALL; OR =1.18, 95% CI =1.00–1.39, P=0.05). Meanwhile, race was found to be a potential source of heterogeneity for the relationship between the C609T polymorphism and acute myeloid leukemia (AML) risk, and the subgroup analysis identified the C609T polymorphism as a risk factor for AML in Asians (OR =1.34, 95% CI =1.03–1.74, P=0.03). The number of studies about C465T polymorphism was too small to pool the data.
Conclusion: There are increased risks of ALL in all subjects and of AML in Asians for carriers of the NQO1 C609T polymorphism. Further studies are needed to verify the associations of the C465T polymorphism with the risk of AL.
Keywords: NQO1, polymorphism, AML, ALL
Introduction
Leukemia is a clonal disorder of hematopoietic cells that is mostly associated with genetic mutation along with a diversity of chromosomal and molecular changes.1 It is one of top ten malignant tumors in China, and the number of leukemia patients has increased markedly in recent years.2 Acute lymphoblastic leukemia (ALL) and acute myeloid leukemia (AML) are the most common types of acute leukemia (AL) in both adults and children. Although there are well-documented studies of the clinical and biological aspects of leukemia, little is known about the predisposing factors of leukemia.3 Smoking, obesity, and exposure to radiation and chemical carcinogens are putative or actual risk factors for AL. However, AL only develops in a small proportion of individuals who have been exposed to these environmental and lifestyle risk factors, and so the genetic background may also be a possible etiology in AL.4
NAD(P)H:quinone oxidoreductase (NQO1), which was originally called DT-diaphorase, is a flavoenzyme that can detoxify quinines derived from the oxidation of phenolic metabolites of benzene by catalyzing two or four electron reductions of these substrates. It can protect cells against oxidative damage by preventing redox cycling and the generation of free radicals.5 Single-nucleotide polymorphisms (SNPs) are the most common type of variant in the human genome.6 A widely researched SNP in NQO1 is C609T. A C/T change at nucleotide 609 causes a proline-to-serine substitution and therefore destabilizes and inactivates the enzyme. Individuals with TT genotype completely lack NQO1 activity, and CT genotype carriers present about threefold decreased enzyme activity compared with wild-type carriers.7 The frequency of the NQO1 C609T polymorphism exhibits ethnic variation. The prevalence of the homozygous variant genotype (TT) was ~20% in Asian populations and 4% in Caucasians.8 Another common SNP was C465T: a C/T change at nucleotide 465. This SNP can also diminish the activity of NQO1.9 So the ability to detoxify carcinogens is reduced when these two polymorphisms are present, which may increase the probability of malignant changes in susceptible individuals.10 These observations support the hypothesis that the TT genotypes for C609T or C465T polymorphisms are likely to be related to the high risk of AL.
It is possibly more meaningful to analyze the effects of genotype–environment interactions on chronic leukemia, and the genetic background may play a more important role in the etiology of AL. Since 2000, the NQO1 C609T and NQO1 C465T polymorphisms have been widely thought to be associated with the risk of AL, but the correlations are still unclear, possibly due to insufficient studies with complete data, diverse study designs and methods, differences in race and geography, and publication bias.
A meta-analysis of published case–control studies was therefore undertaken to precisely evaluate whether the NQO1 C609T and NQO1 C465T polymorphisms are associated with the risk of AL. Potential sources of heterogeneity, subgroups, stability of results, and publication bias were carefully analyzed in this study.
Methods
This meta-analysis was designed and written according to the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-analyses.
Search strategy
The medical literature on associations between the AL risk and the NQO1 C609T and NQO1 C465T polymorphisms that was published before February 2016 was searched in the PubMed, EMBASE, CNKI, and Wanfang electronic databases. The following combination of keywords was used: [AL OR (acute leukemia) OR (AML) OR (acute myeloid leukemia) OR (acute myelocytic leukemia) OR (acute myeloblastic leukemia) OR (ALL) OR (acute lymphocytic leukemia) OR (acute lymphoblastic leukemia)] AND [NQO1 OR (quinone reductase 1) OR (quinone oxidoreductase 1)] AND [polymorphism OR allele OR variant OR variation OR genotype]. The research subjects were limited to humans, and the language was limited to English or Chinese. The references in identified publications were also browsed in order to identify any other relevant studies.
Eligibility criteria
The following inclusion criteria were applied to the studies: 1) must focus on associations of the NQO1 C609T and NQO1 C465T polymorphisms with the AL risk; 2) must have a case–control design; and 3) the reported genotype distribution data must be sufficient to allow the odds ratios (ORs) with 95% confidence intervals (CIs) to be calculated. Studies involving larger samples or published more recently were selected in cases of repeated studies or overlapping data. If the reported data were incomplete, the corresponding author was contacted to obtain complete data.
Data extraction
The following details were extracted from all eligible studies: first author, publication year, race of included subjects, sample sizes of cases and controls, age group, genotyping method, source of controls, mutational location in NQO1, quality score, and results of the Hardy–Weinberg equilibrium (HWE) test for the controls.
Quality assessment
The quality of the included studies was assessed using the quality scoring criteria employed in a previous meta-analysis.11 The representativeness of cases, source of controls, genotyping examination (whether or not genotyping was performed under a blinded condition), the association assessment method, and the HWE test for controls were included as quality assessment indicators. The quality score was calculated by summing the scores for all of these indicators, with the total score ranging from 0 to 10 points. Studies with a score of <6 points were considered to be of low quality.
Statistical analysis
An allele-contrast model was used to investigate the associations of the NQO1 C609T and NQO1 C465T polymorphisms with the risk of AL, and relationship strengths were assessed by ORs with 95% CIs. The statistical random-effects model was used to evaluate different underlying influences and consider variations within or among studies, which provided the advantages of accommodating diversity among studies and offering more conservative evaluations.
Heterogeneity among the studies was analyzed by the chi-square test based on the Q statistic, with significant heterogeneity considered to be present when the P-value was <0.1. The heterogeneity was quantified by the I2 value, with a value >50% indicating higher heterogeneity among the studies. The potential sources of heterogeneity were explored by meta-regression based on the following covariates: race, age, and source of controls. A subgroup analysis was also performed using these covariates.
The publication bias was analyzed by using funnel plots, where an asymmetric funnel plot indicates the presence of such bias. The symmetry of a funnel plot was quantified using Egger’s linear regression test, where a P-value of <0.05 was considered to indicate significant asymmetry and significant publication bias existence. Then the trim-and-fill method was used to assess the effect of publication bias on pooled results.
A cumulative analysis by publication year was performed to observe the trend of pooled results over time. The influence analysis of single study was applied to assess the robustness of the obtained results. Meanwhile, sensitivity analyses were also applied to studies of low quality or that did not conform to HWE to evaluate the effect of these studies on the overall results. In addition, the fail-safe number of negative studies that would be required to nullify (ie, make P>0.05) the effect size was calculated, and a bigger number indicated a more stable pooled result. Stata (version 12.1) was used for all of the statistical tests.
Results
Study characteristics
In total, 893 articles were searched in electronic databases, which resulted in the inclusion of 28 studies. Among the articles, 18 and 18 were about the associations of the NQO1 C609T polymorphism with the risks of AML and ALL, respectively, two were about the association between the NQO1 C465T polymorphism and the AML risk, and three were about the association between the NQO1 C465T polymorphism and the ALL risk. Among these studies, 11 focused on Caucasians,1,3,12–20 10 on Asians,2,9,10,21–27 four on mixed populations,5,28–30 two on Africans,31,32 and one on Javanese.33 In terms of the genotype distribution of controls, 20 of the studies about the association between the NQO1 C609T polymorphism and the AL risk conformed with HWE,1,3,5,9,12,14–20,22–24,28,30–33 while seven did not,2,10,21,25–27,29 and the HWE test could not be applied to one study13 because of insufficient data. Two studies of the association between the NQO1 C465T polymorphism and the AL risk conformed with HWE,16,9 while two did not.23,24 Moreover, there were two studies of low quality.2,13 A flow diagram of the study selection procedure is shown in Figure 1, and the main characteristics of the included studies are presented in Table 1.
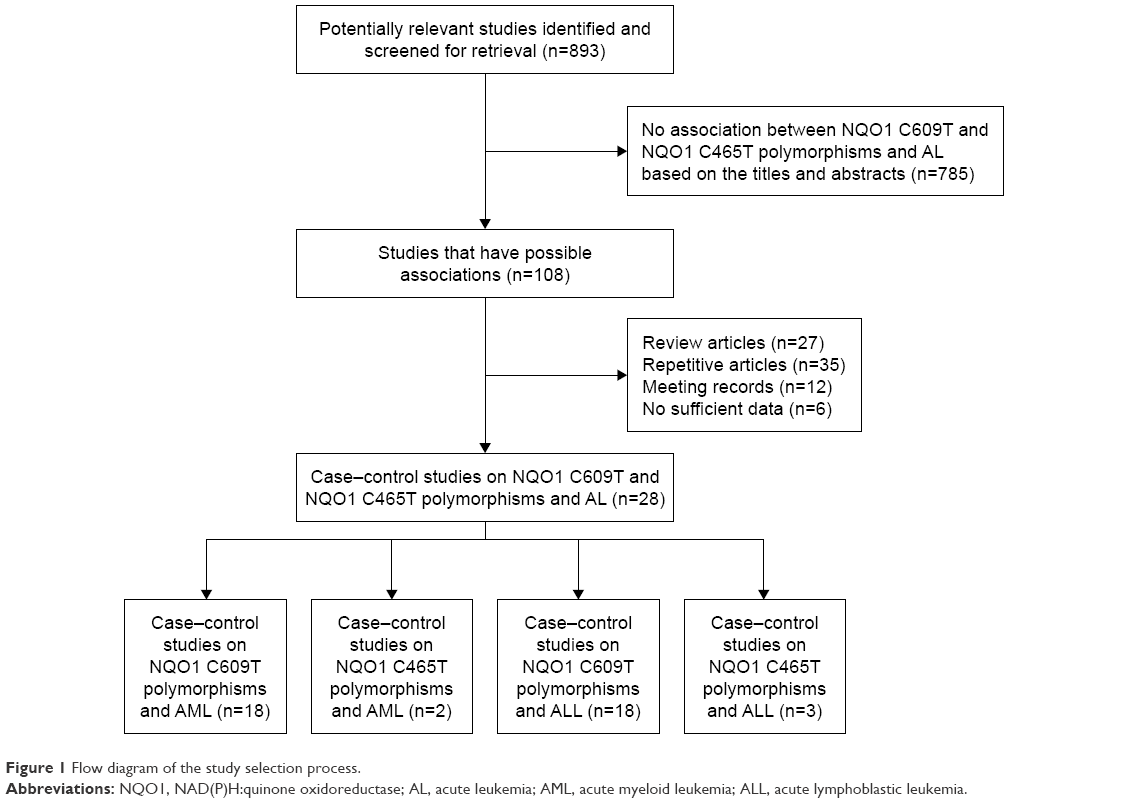 | Figure 1 Flow diagram of the study selection process. |
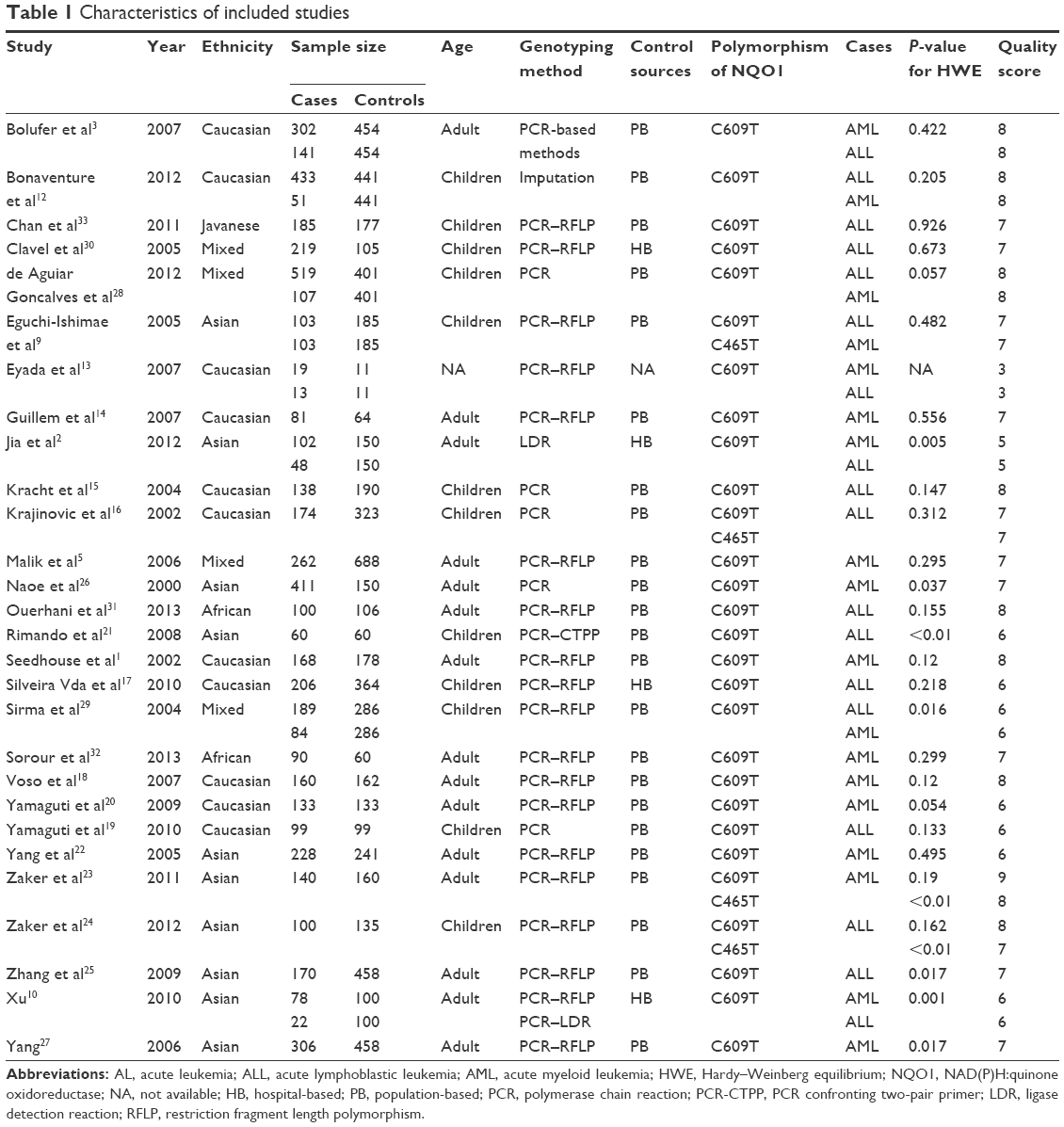 | Table 1 Characteristics of included studies |
NQO1 C609T polymorphism and the ALL risk
Eighteen relevant studies were used to assess the association between the NQO1 C609T polymorphism and the ALL risk. The pooled result revealed a marginally increased risk of ALL for the NQO1 C609T polymorphism (OR =1.18, 95% CI =1.00–1.39, P=0.05; Figure 2A). The fail-safe number was 77.03. The heterogeneity was high (I2=73.0%), but meta-regression did not reveal the potential source of this heterogeneity. In addition, an increased ALL risk for adults was found in the subgroup analysis (OR =1.71, 95% CI =1.20–2.43, P=0.003). The results of the subgroup analysis are presented in Table 2.
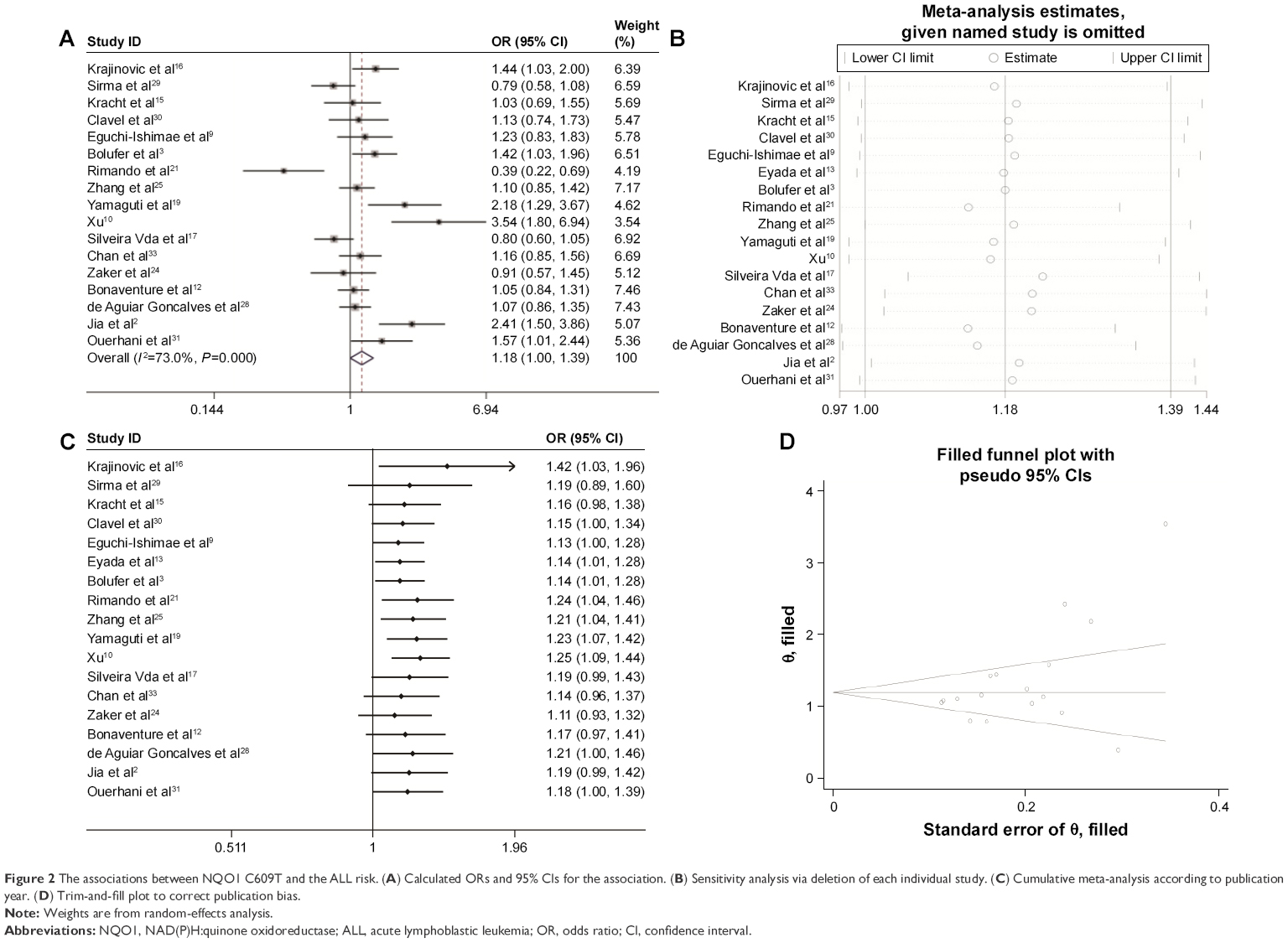 | Figure 2 The associations between NQO1 C609T and the ALL risk. (A) Calculated ORs and 95% CIs for the association. (B) Sensitivity analysis via deletion of each individual study. (C) Cumulative meta-analysis according to publication year. (D) Trim-and-fill plot to correct publication bias. |
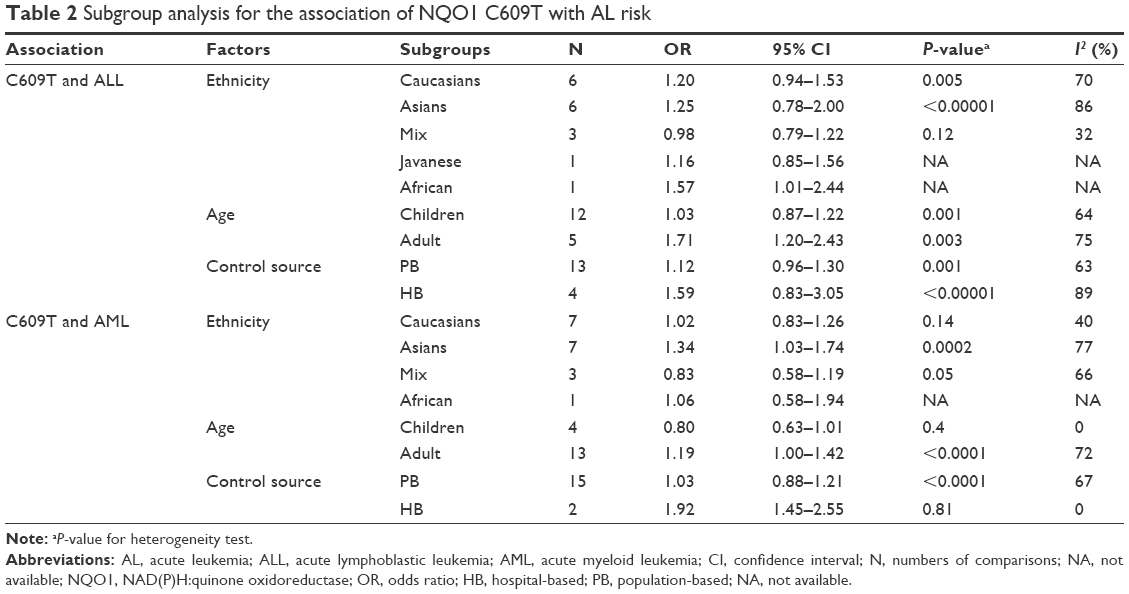 | Table 2 Subgroup analysis for the association of NQO1 C609T with AL risk |
When attempting to identify the presence of publication bias, it is difficult to assess whether a funnel plot is symmetric merely by visual examination. Egger’s linear regression test provided evidence of asymmetry (P=0.031). The publication bias was adjusted by the trim-and-fill method; after that, the pooled result did not change (ie, the effect size from 1.322, 95% CI =1.091–1.554, to 3.752, 95% CI =2.977–4.730; Figure 2D), meaning that the analyses were stable, and moreover that future new research might not change the pooled results. In addition, the influence analysis of single study showed that the total pooled result was greatly affected by the 15 studies (Figure 2B).2,3,9,10,12,13,15,16,19,21,25,28–31 Excluding any of these studies resulted in the statistically significant loss of pooled OR values. Meanwhile, the sensitivity analysis revealed that deleting two studies of low quality,2,13 five studies that did not conform to HWE,2,10,21,25,29 or one study for which the HWE test was not applied did not change the pooled ORs,13 showing that these factors did not affect the stability of the pooled results. No stable tendency was found in the cumulative analysis by publication year (Figure 2C).
NQO1 C609T polymorphism and the AML risk
Eighteen relevant studies were used to assess the association between the NQO1 C609T polymorphism and the AML risk. The pooled result was not statistically significant (OR =1.11, 95% CI =0.94–1.30, P=0.23; Figure 3A). The heterogeneity was high (I2=71.5%), and meta-regression revealed that race and the source of controls were potential sources of this heterogeneity. In addition, an increased AML risk for Asians, adults, and hospital-based control groups was found in the subgroup analysis. The results of the subgroup analysis are presented in Table 2. Egger’s linear regression test provided evidence of symmetry (P=0.338, Figure 3B).
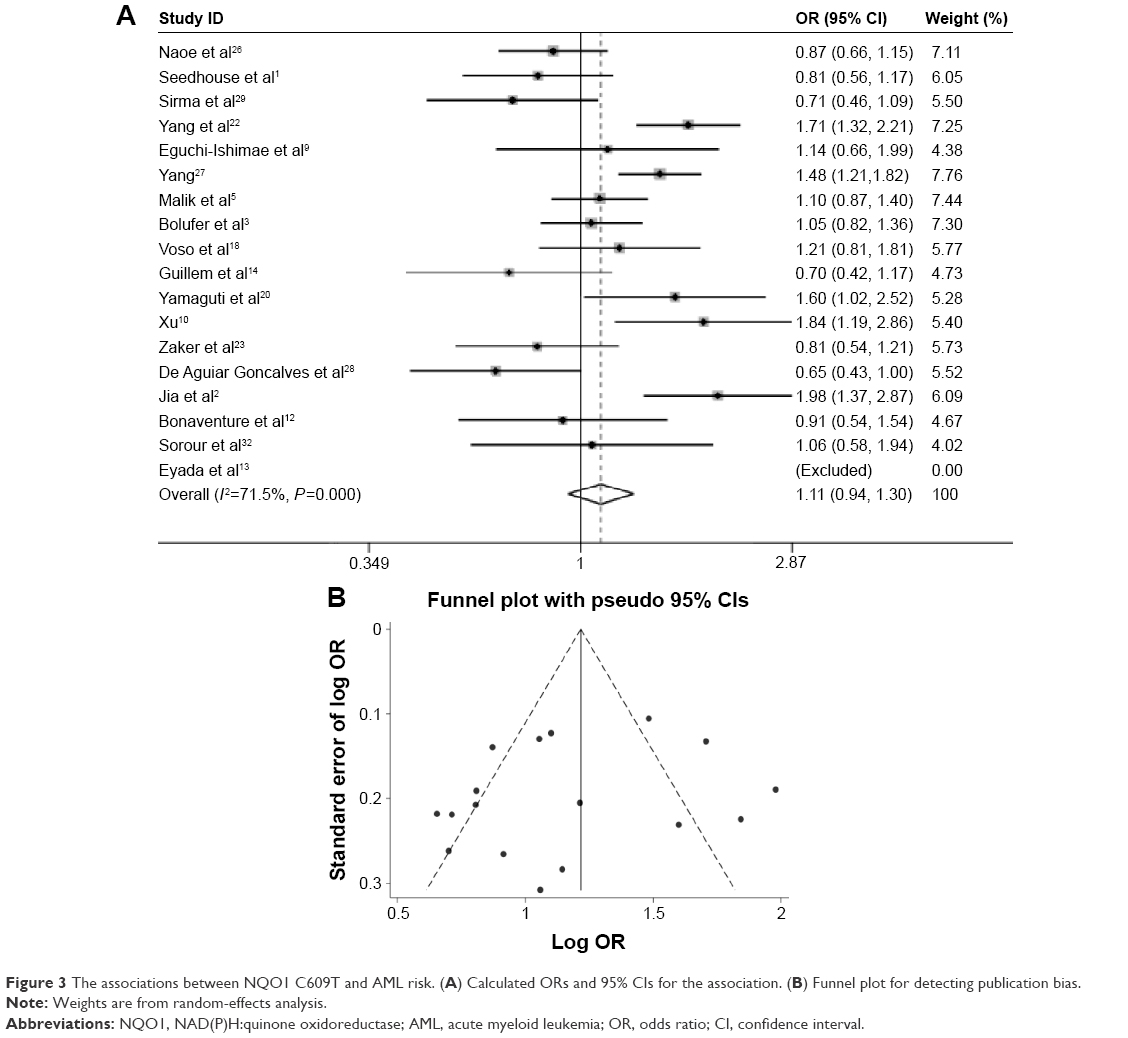 | Figure 3 The associations between NQO1 C609T and AML risk. (A) Calculated ORs and 95% CIs for the association. (B) Funnel plot for detecting publication bias. |
NQO1 C465T polymorphism and risks of AML and ALL
Three relevant studies assessed the association between the NQO1 C465T polymorphism and the ALL risk, of which two did not find a significant association9,16 and one found an increased risk of ALL for the NQO1 C465T polymorphism.24 Two relevant studies researched the association between the NQO1 C465T polymorphism and the AML risk, and both of them did not a find significant association.9,23
Discussion
The method of meta-analysis was used in this study to integrate the published evidence on the associations of the NQO1 C609T and NQO1 C465T polymorphisms with the risk of AL. A heterogeneity evaluation, source searching, sensitivity analysis, publication bias analysis, and analysis of the stability of results were also conducted.
The NQO1 C609T polymorphism was found to be a risk factor for ALL. However, the P-value was only marginally significant, which may have been related to the sample size, and so a more precise result will need to be obtained in the future by using a larger sample. This polymorphism was associated with an increased ALL risk for adults. The different results for children and adults may have been due to the AL etiology differing between these two populations.34 Children are generally more susceptible to environmental toxins because of their immature metabolism and their faster cell division and growth compared with adults.35 This result also suggests the presence of age stratification for the AL risk, and so age-stratification studies are needed to clarify this. Moreover, this research result was very sensitive, which may be due to the number of raw studies being too small, and so more relevant studies are needed to verify the association between the NQO1 C609T polymorphism and the ALL risk in the future.
The association between the NQO1 C609T polymorphism and the ALL risk was analyzed by Li and Zhou36 in four models. They found that this polymorphism increased the ALL risk in a recessive model and a model of T/T versus C/C, while no statistical significance was seen in a dominant model or a model of C/T versus C/C. Their subgroup analysis found that the NQO1 C609T polymorphism increased the ALL risk for adults in a dominant model and a model of T/T versus C/C. The allele-comparison model was used in this study, and it was found that the NQO1 C609T polymorphism increased the ALL risk, with the effect size of an increased ALL risk for adults still being significant in the subgroup analysis. Only the allele-contrast model was selected for this meta-analysis, which could avoid the reuse of data and thus reduce false positive results.
No statistically significant results were found for AML in this study. Meta-regression revealed race to be a potential source of heterogeneity. The subgroup analysis showed that the NQO1 C609T polymorphism is a risk factor for AML in Asians. The meta-analysis showed that the NQO1 C609T polymorphism is a risk factor for bladder and bowel cancer in Caucasians, but a protective factor in Asians;12 these differences indicate that genetic mechanisms may differ between Asians and Caucasians. In addition, the NQO1 C609T polymorphism was a risk factor for AML when the controls were from hospitals, but there were only two raw studies involving hospital-based controls, which suggests that caution is required when interpreting this result owing to the small number of samples and the corresponding low statistical power.
The association between the NQO1 C609T polymorphism and the AML risk was analyzed by Li et al4 in four models. They found that the NQO1 C609T polymorphism increased the AML risk using the recessive fixed-effects model and the model of TT versus CC. However, no statistical significance was seen in the dominant random-effects model or the model of CT versus CC. In addition, the NQO1 C609T polymorphism increased the risks of AML in adults and Asians in the subgroup analysis in the recessive random-effects model in their study. In this study, no statistically significant association was found between this SNP and the AML risk under the allele-comparison model, but significant associations were found for Asians, adults, and hospital-based control groups, which was consistent with the study by Li et al.4 The main differences between this study and the two articles by Li et al4,36 were mainly reflected in the following two aspects: 1) this sample was larger because several raw studies were newly added and 2) the stability of pooled results was also analyzed to provide a more objective evaluation.
Only a small amount of the literature focuses on the relationships of the NQO1 C465T polymorphism with the risks of ALL and AML, which was definitely not enough the meta-analysis in this study. So the results of original articles were described.
This study was subject to three main limitations. First, leukemia is associated with several risk factors including age, previous blood disease, genetic variants, occupational hazards, chemotherapy, and exposure to viruses, X-rays, and chemicals. However, only gene polymorphisms were considered in this study. The effects of gene–environment interactions on the initiation and development of leukemia need to be analyzed further in individual patients. Second, only relevant studies published in English or Chinese were included in this study, and so there is a possibility of language bias. Third, the number of raw studies was small in some of the subgroup analyses, which could have led to overestimations of real relationships.
Conclusion
The NQO1 C609T polymorphism may be associated with an increased risk of AL. T allele carriers might be more susceptible to AL and thus should pay more attention to away from environmental and lifestyle risk factors. In order to provide better guidance for clinical practice, future studies need to verify the relationships of the NQO1 C609T polymorphism with the risks of ALL and AML.
Acknowledgments
This work was supported by the Natural Science Foundation of Shaanxi Province (number 2015JM8415) and the Fundamental Research Funds for the Central Universities of China (number 2011jdhz55).
Disclosure
The authors report no conflicts of interest in this work.
References
Seedhouse C, Bainton R, Lewis M, Harding A, Russell N, Das-Gupta E. The genotype distribution of the XRCC1 gene indicates a role for base excision repair in the development of therapy-related acute myeloblastic leukemia. Blood. 2002;100(10):3761–3766. | ||
Jia MF, Xi YM, Shi XE, et al. Relationship of MPO and NQO1 gene polymorphisms with susceptibility to acute leukemia. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2012;20(6):1336–1340. Chinese. | ||
Bolufer P, Collado M, Barragán E, et al. The potential effect of gender in combination with common genetic polymorphisms of drug-metabolizing enzymes on the risk of developing acute leukemia. Haematologica. 2007;92(3):308–314. | ||
Li C, Liu Y, Wei S, Zhou Y. A meta-analysis of the association between NQO1 C609T variation and acute myeloid leukemia risk. Pediatr Blood Cancer. 2014;61(5):771–777. | ||
Malik E, Cohen SB, Sahar D, Dann EJ, Rund D. The frequencies of NAD(P)H quinone oxidoreductase (NQO1) variant allele in Israeli ethnic groups and the relationship of NQO1*2 to adult acute myeloid leukemia in Israeli patients. Haematologica. 2006;91(7):956–959. | ||
Yuan L, Zhang TT, Ren Y. miR-27a rs895819 polymorphism and risk of cancer in Chinese population: a meta-analysis. J Evid Based Med. 2015;8(2):75–83. | ||
Zachaki S, Stavropoulou C, Koromila T, et al. High frequency of NAD(P)H:quinone oxidoreductase 1 (NQO1) C(609)T germline polymorphism in MDS/AML with trisomy 8. Leuk Res. 2013;37(7):742–746. | ||
Kelsey KT, Ross D, Traver RD, et al. Ethnic variation in the prevalence of a common NAD(P)H quinone oxidoreductase polymorphism and its implications for anti-cancer chemotherapy. Br J Cancer. 1997;76(7):852–854. | ||
Eguchi-Ishimae M, Eguchi M, Ishii E, et al. The association of a distinctive allele of NAD(P)H:quinone oxidoreductase with pediatric acute lymphoblastic leukemias with MLL fusion genes in Japan. Haematologica. 2005;90(11):1511–1515. | ||
Xu JW. A Study between Genetic Polymorphisms of MPO and NQO1 and Susceptibility of Acute Leukemia [dissertation]. Lanzhou: Lanzhou University; 2010. | ||
Niu YM, Du XY, Cai HX, et al. Increased risks between Interleukin-10 gene polymorphisms and haplotype and head and neck cancer: a meta-analysis. Sci Rep. 2015;5:17149. | ||
Bonaventure A, Goujon-Bellec S, Rudant J, et al. Maternal smoking during pregnancy, genetic polymorphisms of metabolic enzymes, and childhood acute leukemia: the ESCALE study (SFCE). Cancer Causes Control. 2012;23(2):329–345. | ||
Eyada TK, El Ghonemy EG, El Ghoroury EA, El Bassyouni SO, El Masry MK. Study of genetic polymorphism of xenobiotic enzymes in acute leukemia. Blood Coagul Fibrinolysis. 2007;18(5):489–495. | ||
Guillem VM, Collado M, Terol MJ, et al. Role of MTHFR (677, 1298) haplotype in the risk of developing secondary leukemia after treatment of breast cancer and hematological malignancies. Leukemia. 2007;21(7):1413–1422. | ||
Kracht T, Schrappe M, Strehl S, et al. NQO1 C609T polymorphism in distinct entities of pediatric hematologic neoplasms. Haematologica. 2004;89(12):1492–1497. | ||
Krajinovic M, Sinnett H, Richer C, Labuda D, Sinnett D. Role of NQO1, MPO and CYP2E1 genetic polymorphisms in the susceptibility to childhood acute lymphoblastic leukemia. Int J Cancer. 2002;97(2):230–236. | ||
Silveira Vda S, Canalle R, Scrideli CA, Queiroz RG, Tone LG. Role of the CYP2D6, EPHX1, MPO, and NQO1 genes in the susceptibility to acute lymphoblastic leukemia in Brazilian children. Environ Mol Mutagen. 2010;51(1):48–56. | ||
Voso MT, Fabiani E, D’Alo’ F, et al. Increased risk of acute myeloid leukaemia due to polymorphisms in detoxification and DNA repair enzymes. Ann Oncol. 2007;18(9):1523–1528. | ||
Yamaguti GG, Lourenco GJ, Silveira VS, et al. Increased risk for acute lymphoblastic leukemia in children with cytochrome P450A1 (CYP1A1)- and NAD(P)H:quinone oxidoreductase 1 (NQO1)-inherited gene variants. Acta Haematol. 2010;124(3):182–184. | ||
Yamaguti GG, Lourenco GJ, Costa FF, Lima CS. High risk of “de novo” acute myeloid leukaemia in individuals with cytochrome P450 A1 (CYP1A1) and NAD(P)H:quinone oxidoreductase 1 (NQO1) gene defects. Eur J Haematol. 2009;83(3):270–272. | ||
Rimando MG, Chua MN, Yuson E, de Castro-Bernas G, Okamoto T. Prevalence of GSTT1, GSTM1 and NQO1 (609C>T) in Filipino children with ALL (acute lymphoblastic leukaemia). Biosci Rep. 2008;28(3):117–124. | ||
Yang L, Zhang Y, Zhang MR, Xiao ZJ. Relationship between GSTT1, GSTM1 and NQO1 gene polymorphism and acute myeloid leukemia and recurrent chromosome translocations. Zhonghua Yi Xue Za Zhi. 2005;85(33):2312–2316. Chinese. | ||
Zaker F, Safaei A, Hashemi M, Pazhakh V. The frequency and association of C609T and C465T polymorphisms of NAD(P)H:quinone oxidoreductase gene with adult acute myeloid leukemia. Lab Med. 2011;42(11):674–677. | ||
Zaker F, Safaei A, Nasiri N, Abdollahzadeh M, Pazhakh V. The association of NAD(P) H:quinine oxidoreductase gene polymorphisms with pediatric acute lymphoblastic leukemia. Lab Med. 2012;43(6):256–261. | ||
Zhang ZQ, Yang L, Zhang Y, et al. Relationship between NQO1C(609T), RAD51(G135C), XRCC3(C241T) single nucleotide polymorphisms and acute lymphoblastic leukemia. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2009;17(3):523–528. Chinese. | ||
Naoe T, Takeyama K, Yokozawa T, et al. Analysis of genetic polymorphism in NQO1, GST-M1, GST-T1, and CYP3A4 in 469 Japanese patients with therapy-related leukemia/myelodysplastic syndrome and de novo acute myeloid leukemia. Clin Cancer Res. 2000;6(10):4091–4095. | ||
Yang L. Relationship between Genetic Polymorphisms and Acute Myeloid Leukemia and Recurrent Chromosome Translocations [dissertation]. Beijing: Peking Union Medical College; 2006. | ||
de Aguiar Goncalves BA, Vasconcelos GM, Thuler LC, et al. NQO1 rs1800566 (C609T), PON1 rs662 (Q192R), and PON1 rs854560 (L55M) polymorphisms segregate the risk of childhood acute leukemias according to age range distribution. Cancer Causes Control. 2012;23(11):1811–1819. | ||
Sirma S, Agaoglu L, Yildiz I, et al. NAD(P)H:quinone oxidoreductase 1 null genotype is not associated with pediatric de novo acute leukemia. Pediatr Blood Cancer. 2004;43(5):568–570. | ||
Clavel J, Bellec S, Rebouissou S, et al. Childhood leukaemia, polymorphisms of metabolism enzyme genes, and interactions with maternal tobacco, coffee and alcohol consumption during pregnancy. Eur J Cancer Prev. 2005;14(6):531–540. | ||
Ouerhani S, Cherif N, Bahri I, Safra I, Menif S, Abbes S. Genetic polymorphisms of NQO1, CYP1A1 and TPMT and susceptibility to acute lymphoblastic leukemia in a Tunisian population. Mol Biol Rep. 2013;40(2):1307–1314. | ||
Sorour A, Ayad MW, Kassem H. The genotype distribution of the XRCC1, XRCC3, and XPD DNA repair genes and their role for the development of acute myeloblastic leukemia. Genet Test Mol Biomarkers. 2013;17(3):195–201. | ||
Chan JYS, Ugrasena DG, Lum DWK, Lu Y, Yeoh AEJ. Xenobiotic and folate pathway gene polymorphisms and risk of childhood acute lymphoblastic leukaemia in Javanese children. Hematol Oncol. 2011;29(3):116–123. | ||
Larfors G, Hallböök H, Simonsson B. Parental age, family size, and offspring’s risk of childhood and adult acute leukemia. Cancer Epidemiol Biomarkers Prev. 2012;21(7):1185–1190. | ||
Perera FP. Environment and cancer: who are susceptible? Science. 1997;278(5340):1068–1073. | ||
Li C, Zhou Y. Association between NQO1 C609T polymorphism and acute lymphoblastic leukemia risk: evidence from an updated meta-analysis based on 17 case-control studies. J Cancer Res Clin Oncol. 2014;140(6):873–881. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.