")
Back to Journals » Patient Preference and Adherence » Volume 14
Associations Between Health Literacy and Medication Self-Management Among Community Health Center Patients with Uncontrolled Hypertension
Authors Persell SD , Karmali KN, Lee JY, Lazar D, Brown T, Friesema EM , Wolf MS
Received 9 August 2019
Accepted for publication 13 December 2019
Published 15 January 2020 Volume 2020:14 Pages 87—95
DOI https://doi.org/10.2147/PPA.S226619
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Stephen D Persell, 1, 2 Kunal N Karmali, 3 Ji Young Lee, 1 Danielle Lazar, 4 Tiffany Brown, 1 Elisha M Friesema, 1, 2, 5 Michael S Wolf 1
1Division of General Internal Medicine and Geriatrics, Department of Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA; 2Center for Primary Care Innovation, Institute for Public Health and Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA; 3Division of Cardiology, Department of Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA; 4Access Community Health Network and the ACCESS Center for Discovery and Learning, Chicago, IL, USA; 5Carlson School of Management, University of Minnesota, Minneapolis, MN, USA
Correspondence: Stephen D Persell
Division of General Internal Medicine and Geriatrics, Department of Medicine Feinberg School of Medicine, Northwestern University, 750 North Lake Shore Drive, 10th Floor, Chicago, IL 60611, USA
Tel +1 312 503 6464
Fax +1 312 503 2755
Email [email protected]
Purpose: Examine associations between health literacy and several medication self-management constructs among a population of adults with uncontrolled hypertension.
Patients and Methods: Cross-sectional study of health center patients from the Chicago area with uncontrolled hypertension enrolled between April 2012 and February 2015. Medication self-management constructs—applied to hypertension medications, chronic condition medications and all medications—included: 1) medication reconciliation, 2) knowledge of drug indications, 3) understanding instructions and dosing, and 4) self-reported adherence over 4 days (no missed doses). We determined associations between health literacy and self-management outcomes using multivariable generalized linear regression.
Results: There were 1460 patients who completed screening interviews; 62.9% enrolled and had complete baseline data collected, and were included in the analysis. Of 919 participants, 47.4% had likely limited (low), 33.2% possibly limited, and 19.4% likely adequate health literacy. Compared to participants with likely adequate health literacy, participants with low health literacy were less likely to have chronic medications reconciled (18.0% versus 29.6%, p=0.007), know indications for chronic medications (64.1% versus 83.1%, p< 0.001), and demonstrate understanding of instructions and dosing (68.1% versus 82.9%, p=0.001). Self-reported adherence to hypertension medications was higher among the low health literacy group (65.6% versus 56.0%, p=0.010). In multivariable models, health literacy was strongly associated with knowledge of drug indications, and understanding of instructions and dosing.
Conclusion: Low health literacy was associated with worse medication self-management in several domains. However, non-adherence was greatest in the most health literate in unadjusted analysis. Among a population of patients with uncontrolled hypertension, the drivers of poor control may vary by health literacy.
Keywords: health literacy, hypertension, medication reconciliation, community health centers
Introduction
Individuals with chronic health conditions like hypertension are often advised by clinicians to take multiple medications. Complex drug regimens can raise the risk of medication self-administration errors. This risk may be greatest for people with low health literacy.1 Low health literacy has been shown in a systematic review to be associated with poorer health outcomes.2 A potential causal pathway connecting low health literacy to worse health outcomes may be through its effects on medication self-management. For example, low health literacy is associated with worse medication self-administration skills,3–5 generally lower medical knowledge,6 and with worse medication reconciliation.7 The relationship between medication adherence and health literacy has been inconsistent.8,9 Some studies have shown low health literacy to be associated with worse medication adherence.10−13 While others showed higher adherence among individuals with low health literacy,14,15 or no association.16–19
Individuals with low health literacy may also be less likely to have a shared understanding with clinicians of which medications have been prescribed to control their health condition. In other words, patients’ and clinicians’ active medication lists may not be reconciled. This can occur when patients and their treating clinicians are inadvertently in disagreement about the intended prescription plan, patients choose not to adhere to medication independent of their clinicians, or the healthcare team has made errors.6,7,20
In this study, our objectives were to examine the relationships between health literacy and several aspects of medication self-management: medication reconciliation, knowledge of drug indications, understanding of medication instructions and dosing, and self-reported medication adherence among community health center patients enrolling in a clinical study with uncontrolled hypertension. A conceptual schema connecting the self-management and medication reconciliation concepts addressed here with chronic illness outcomes was published previously.21 We hypothesized that these constructs would be associated with health literacy. We examined these relationships by performing a cross-sectional analysis of baseline data collected from adults with uncontrolled hypertension receiving care at community health centers who enrolled in a randomized trial of two medication self-management support strategies.21,22
Methods
We performed this study using baseline data from the Northwestern and Access Community Health Network Medication Education Study (NAMES). The design and outcomes of this trial were previously reported.21,22 Northwestern University’s institutional review board approved the study. Participants provided written informed consent.
Setting
The study was conducted at 12 community health centers in the Access Community Health Network (ACCESS) in the Chicago, IL area. The study intervention materials were in English, therefore, health centers with largely non-English speaking patient populations were not included.
Participants
We recruited participants from February 2012 through February 2015. Full eligibility criteria have been previously published.21,22 In short age, participants were eligible if they were 18 years of age or older, said they used three or more medications used for any purpose, had an enrollment visit blood pressure ≥130 mm Hg systolic or ≥80 mm Hg diastolic with diabetes or ≥135 mm Hg systolic or ≥85 mm Hg diastolic without diabetes, were responsible for administering their own medications, and were able to communicate in English. We recruited patients with a hypertension diagnosis identified from electronic health record (EHR)-generated lists who had three or more medications (clinicians could indicate who should not be contacted). We also recruited participants from health center waiting rooms. Of the 1460 patients who participated in the screening assessment, 124 (8.5%) did not meet eligibility criteria based on their survey responses, 347 (27.5%) did not meet blood pressure criteria, 69 (4.7%) were eligible but declined to enroll, and 1 enrolled but had missing data. The remaining 919 (62.9%) patients had complete baseline data collected, and were included in this analysis.
Outcomes and Measures
Research assistants administered in-person assessments at the health centers. Questions assessed socio-demographic characteristics, medical conditions and participant-reported outcomes. We used the Newest Vital Sign to assess health literacy. We grouped participants into 3 categories based on a score of 0 to 6: likely limited (0 or 1), possibly limited (2 or 3) and likely adequate (4 or greater).23
We assessed medication reconciliation by making direct comparisons of the medications reported by participants with the active medication list in the EHR (EpicCare, Epic Systems Corporation, Verona, WI) from the same date.7,22 The physicians who performed these comparisons were blinded to patient identity and characteristics. We classified the patient-reported and EHR medication lists as reconciled or not reconciled for three categories of medications: 1) antihypertensive medications, 2) all not-as-needed chronic prescription medications (not including non-systemic medications and including daily aspirin), and 3) all medications (chronic, as-needed and over-the-counter medications). We examined medication outcomes in these three categories because the first is most directly tied to the clinical reason participants were included (uncontrolled hypertension); the second represents chronic disease management overall including related chronic illnesses like hypercholesterolemia, diabetes and other chronic conditions; and the third provides insight into patients’ and clinicians’ understanding of all medications used including important as-needed medications that may impact chronic illness care (such as non-steroidal anti-inflammatory drugs).
Blinded physicians assessed participants’ knowledge of medication indication. Participants were considered to not know the indication for a medication if they said they did not know the reason why they took a medication or provided a reason that was classified as probably or definitely incorrect.24 General answers (e.g., “Hydrochlorothiazide is for my heart”) that referred to the correct organ system or disease process (e.g., “Metformin is for blood sugar”) were classified as correct whereas statements like, “Amlodipine is a blood thinner” or “Atorvastatin is to help with sleep” were classified as incorrect.
We assessed understanding of medication instructions and dosing by comparing prescription instructions to participants’ mock demonstration of the way they use each medication including the dosing quantity and dosing frequency.22 We used binary classifications (full understanding of all medications in that category vs not) with the above three medication categories. For each medication, we asked participants to demonstrate the times of day and the number of pills taken using beads that they placed onto a tray with boxes representing each hour of the day. This objective assessment of patients’ understanding and proper dosing of prescribed regimens has been validated and used extensively in prior health literacy research studies.1,25,26 In addition, poorer performance on this task has been found to be significantly associated with more inadequate medication adherence and adverse healthcare outcomes.5,27
We measured medication adherence for the prescription medications participants indicated that they were taking by using a 4-day assessment of pills taken divided by pills prescribed (always including at least one weekend day) from the Patient Medication Adherence Questionnaire (PMAQ),28,29 and classified each participant as having full adherence or not full adherence for each of the three study medication categories.
For each medication self-management measure, we used a binary classification (perfect performance vs not perfect performance). We did this because: 1) lack of understanding or lack of knowledge for any medication in the category may be indicative of important self-management limitations, and 2) this classification approach enabled us to make straightforward comparisons across individuals using different numbers of medications.
Statistical Analysis
We used descriptive statistics to compare characteristics of participants with likely limited, possibly limited and likely adequate health literacy (χ2 test for categorical variables, and parametric and non-parametric tests for normal and non-normally distributed continuous variables as appropriate). We used multivariable generalized linear regression with a logit link to assess the independent relationships between health literacy and medication self-management outcomes. Models included age, sex and number of medications within an examined category as fixed effects and health center as random effects. We did not include educational attainment or income in the primary models because they were highly correlated with health literacy, their inclusion might represent over-adjustment, and could lead to an underestimation of the relationships between health literacy and the factors we examined.2 Addition of education and income categories to the models was tested in a sensitivity analysis. P values of <0.05 were used to assess statistical significance. All analyses utilized SAS v 9.4 (SAS Institute Inc., Cary, NC).
Results
Among the 919 included participants, 436 (47.4%) had likely limited health literacy, 305 (33.2%) had possibly limited health literacy, and 178 (19.4%) had adequate health literacy. Mean age was 52.3 years, 67.9% were female, and 87.1% were black. Approximately two-thirds completed a high school education or less and 74.6% reported annual household income of less than $20,000. Age, race/ethnicity, educational attainment, and income varied by health literacy category. Blood pressures, the number of medications used, and diabetes prevalence were similar in each health literacy group (Table 1).
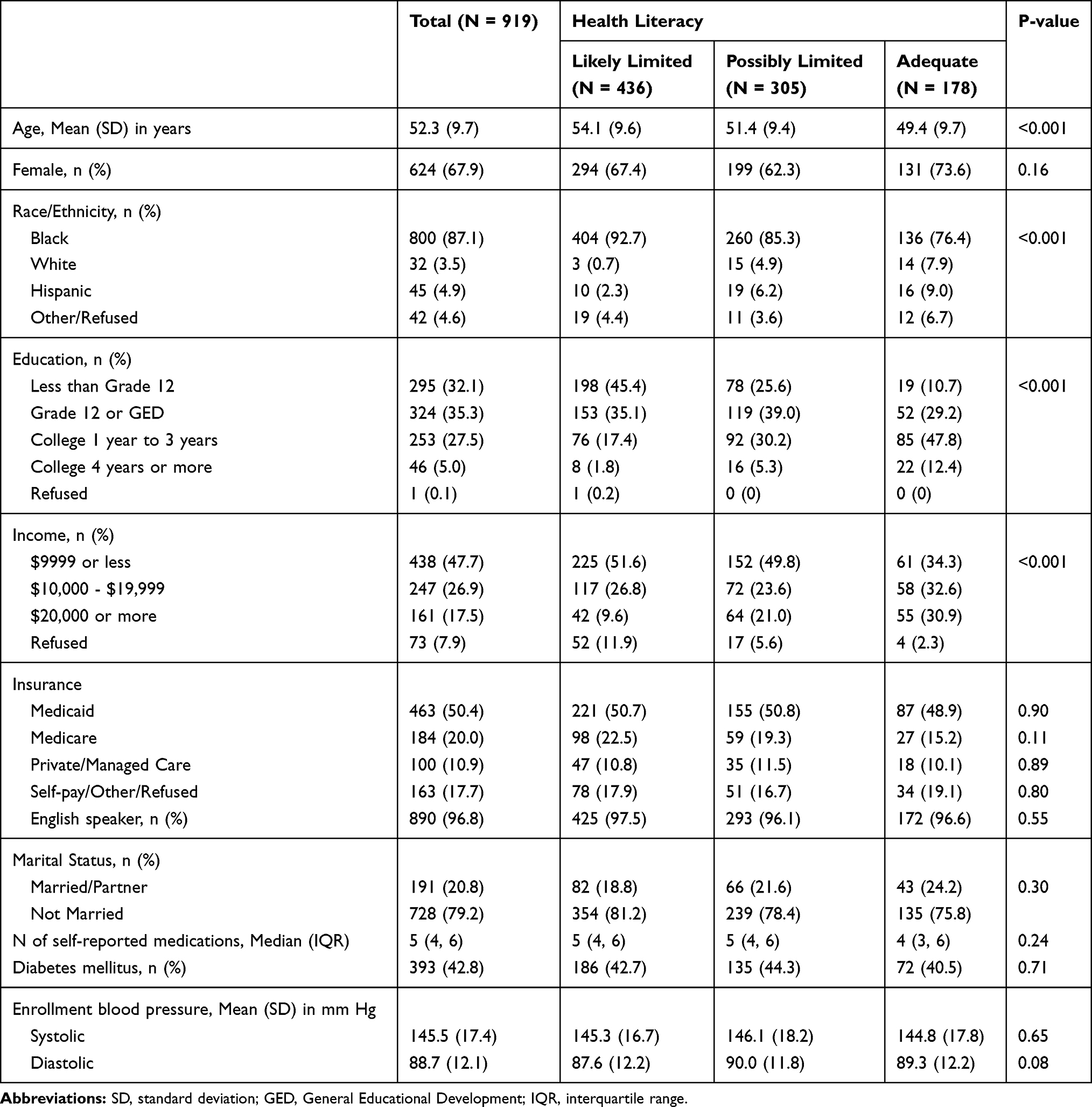 |
Table 1 Participant Characteristics Overall and Stratified by Health Literacy |
In bivariate comparisons, participants with limited health literacy had the lowest rates and those with adequate health literacy had the highest rates of medication reconciliation, knowledge of medication indications, and demonstrated understanding of medication instructions and dosing for each of the three medication categories examined—hypertension medications, all chronic condition medications, and all medications (Table 2). Self-reported medication adherence for hypertension medications was also associated with health literacy category but was highest in the group with limited health literacy (65.6% full adherence) and lowest in the group with adequate health literacy (56.0% full adherence, P = 0.01) (Table 2).
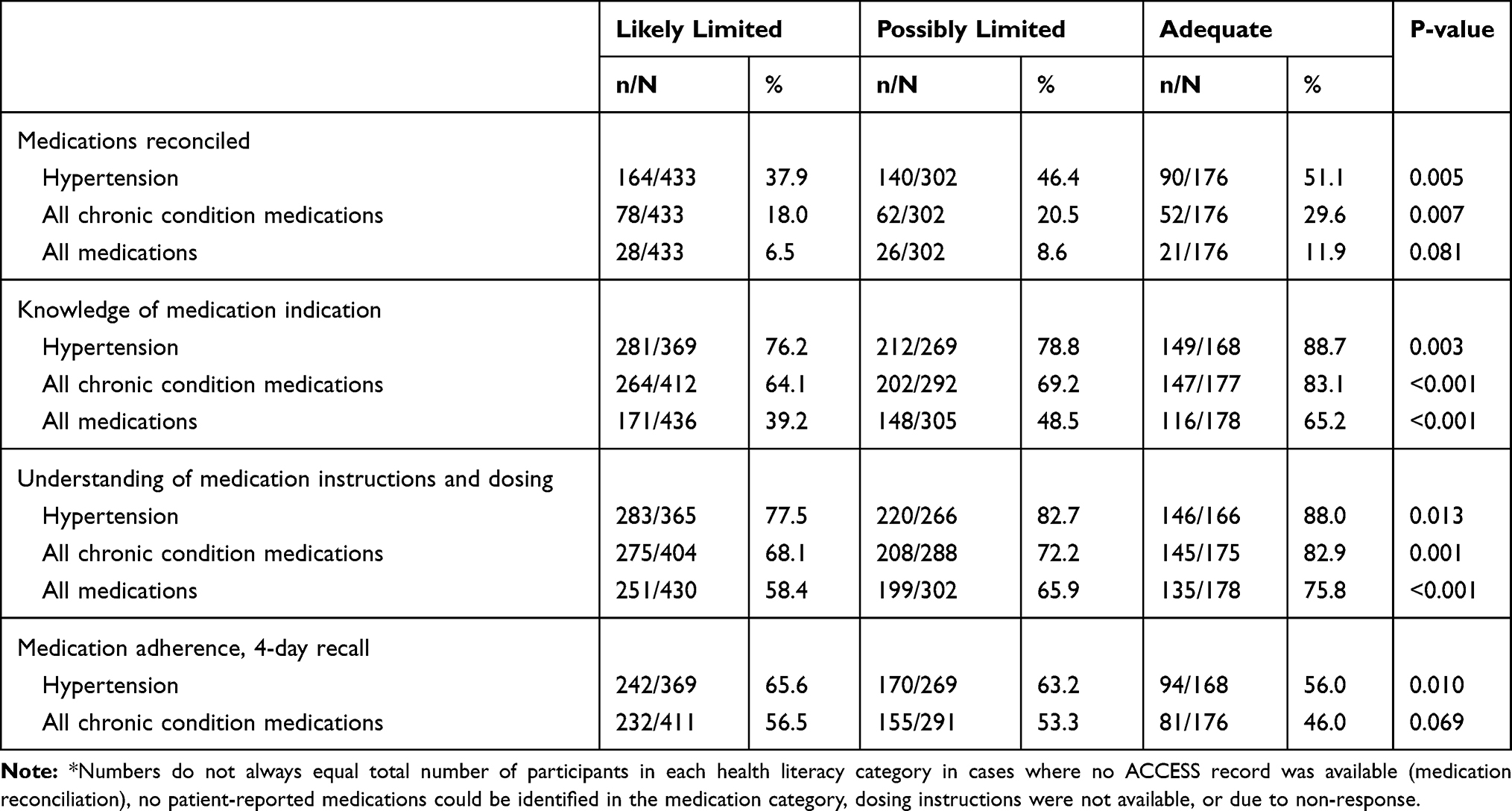 |
Table 2 Medication Self-Management Outcomes by Health Literacy* |
In multivariable adjusted models (Table 3), likely limited health literacy was associated with lower odds of knowing medication indications, and demonstrating correct understanding of medication instructions and dosing for each of the three medication categories compared to adequate health literacy (P ≤ 0.02 for each). The group with possibly limited health literacy was less likely to know medication indications (all three comparisons, P ≤ 0.04 for each), and less likely to demonstrate correct understanding of instructions and dosage (all chronic disease medications and all medications) compared to adequate health literacy (P < 0.04). In the multivariable models, the relationships between health literacy and medication reconciliation were attenuated and not statistically significant. Compared to adequate health literacy, the group with limited health literacy had higher self-reported adherence for hypertension medications (OR 1.38, 95% CI 0.93 to 2.05) and all chronic condition medications (OR 1.47, 95% CI 1.00 to 2.16), but these differences were not statistically significant at the pre-specified level.
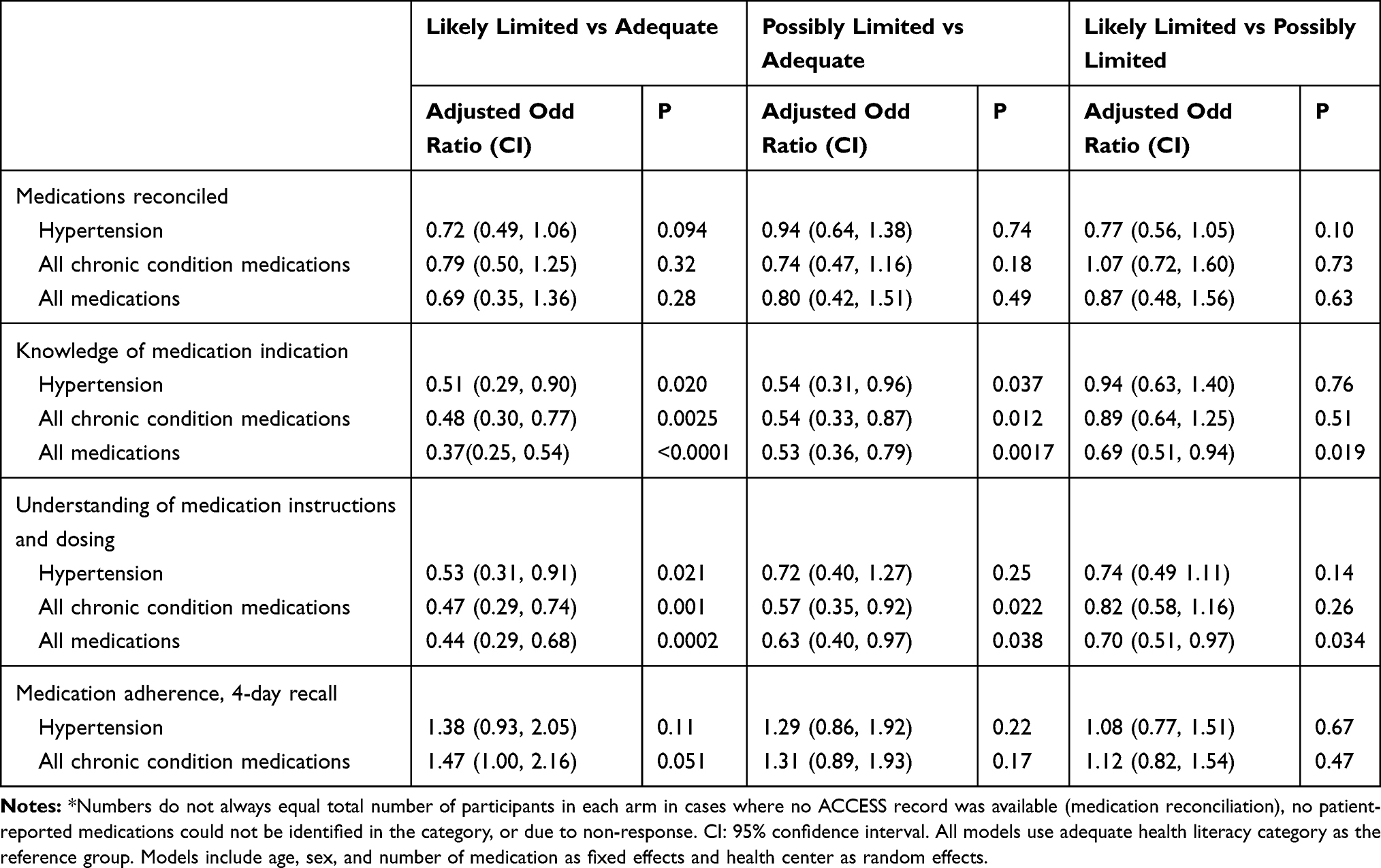 |
Table 3 Adjusted Relationships of Medication Self-Management Outcomes by Health Literacy* |
Intra-class correlation coefficients (ICC) (representing the degree to which there was similarity of outcomes within clinics) was low for most medication management outcomes (Supplemental Table 1) except for medication reconciliation of all chronic condition medications (ICC = 0.12) and reconciliation of all medications (ICC 0.16).
In the sensitivity analyses that included education and income in the models, the associations between health literacy and medication self-management outcomes changed little (Supplemental Table 2). In this model, likely limited health literacy was associated with reduced likelihood of having hypertension medications reconciled compared to adequate health literacy, and several comparisons of the possibly limited health literacy group to other groups were no longer statistically significant (Supplemental Table 2).
Discussion
Among this group of uncontrolled hypertension patients at Chicago-area community health centers who self-reported the use of at least three medications, there were several notable findings. First, the prevalence of limited health literacy was very high (only a fifth of participants had adequate health literacy and almost half had likely limited health literacy as assessed by the Newest Vital Sign). This prevalence is substantially higher than what has been reported in several other populations and is similar to prior studies conducted in safety net clinical settings.3,7,30 These high prevalences support the notion that health literacy best practices should be widely and routinely adopted, particularly in safety-net settings.
Second, there were large differences in several medication self-management outcomes by health literacy, particularly knowledge of drug indications, and understanding of medication instructions and dosage. Our findings are consistent with the associations between health literacy and of knowledge of drug indications, ability to identify one’s own medications, and to demonstrate proper usage of medications that have been observed in prior studies.3,5,7
In contrast, medication adherence based on self-reported recall of recent use of the chronic medications patients’ currently report taking in this population of community health center patients with uncontrolled hypertension was lowest in the group with adequate health literacy. This finding may be due to several factors. This study included only uncontrolled hypertensive patients so all patients had some reason for being uncontrolled. It seems plausible that those with lower health literacy may have had inadequate disease control due to inadvertent errors in following prescribed regimens (inadvertently omitting medications intended by their clinicians or not taking medications at the prescribed frequency) but believed they were taking their medications correctly. Errors of this nature would more readily identified in the measures of medication reconciliation or demonstrated understanding of medication instructions and dosing that were used in this study, or in measures of refill adherence used in some prior studies that used pharmacy fill data or objective medication monitoring systems. Several prior studies have distinguished between intentional and unintentional nonadherence. Lindquist and colleagues found in older adults following discharge, those with low health literacy were less likely to intentionally not adhere to discharge medications but had had more unintentional non-adherence due to medication discrepancies resulting from errors.15 More recently Fan and colleagues observed among adults with type 2 diabetes that low health literacy was associated with unintentional non-adherence, but was not significantly associated with intentional non-adherence (though the ability of this study to detect such an association was limited by the study’s size).13 An alternative explanation of this finding is that health literacy may be negatively associated with the likelihood of providing socially desirable survey responses about medication use. Nevertheless, the observed differences in the examined aspects of medication self-management examined here suggest that drivers of inadequate chronic disease control may differ across the health literacy spectrum.
A third notable finding is the very low level of medication reconciliation in this population across the health literacy spectrum. Chronic disease medications reported by patients with adequate health literacy matched the medical record less than a third of the time. The entire medication list almost never matched. Feasible strategies to improve medication reconciliation are needed. There was a graded relationship between medication reconciliation and health literacy in unadjusted analyses that was attenuated after adjustment and accounting for site-level effects. This, along with the high ICCs for the medication reconciliation measures at the site level suggest that practice variations among participating health centers may be a more important driver of this medication management construct than the other constructs we examined.
Fourth, about half of this population could not provide an accurate indication for all of their prescription medications. While this was lowest among those with low health literacy, a third of individuals with adequate health literacy could not provide even a basic indication for each prescription medication. The lack of knowledge of drug indications for one or more medications in this population is much greater than the rate of 13.5% found in a population assessed using similar methods that was of higher socioeconomic status, and used an average of 3.8 medications per person.12 This suggests that there is a need for clinicians and health systems to find better ways to help ensure that patients understand why they use their medications.
This study has several important strengths. First, we studied a large number of individuals, including many with low health literacy and drew from 12 different health centers from across a large greater metropolitan area. Second, we measured multiple constructs related to medication self-management. These two factors enabled us to observe differences in potential drivers of poor hypertension control that appear to vary across the health literacy spectrum.
There are also several limitations that should be noted. Since all participants came from one network of health centers in a single metropolitan area, and were selected based on the clinical trial entry criteria, these findings may not be generalizable to other settings, to patients with well-controlled hypertension, or to patients using fewer medications. Because this study did not include individuals whose hypertension was well controlled, we are not able to examine relationships between health literacy, medication self-management and blood pressure outcomes. We cannot exclude the possibility that health literacy was associated with individuals’ willingness to report medication non-adherence. The measure of adherence did not distinguish intentional from unintentional non-adherence, and, to our knowledge, its reliability has not been assessed in the same population as the one studied here. Lastly, participants with lower health literacy were less likely to be able to identify the name or indication of the medications they used. Therefore, some measures of hypertension medication self-management likely had a higher proportion of missing data in the lower health literacy groups.
Conclusion
Among community health center patients with uncontrolled hypertension, limited health literacy was highly prevalent and strongly associated with worse medication self-management in several domains. In the unadjusted analysis, non-adherence based on self-report of skipped doses appeared greatest in the most health literate suggesting that principle drivers of inadequate chronic disease control (among a population who all have uncontrolled hypertension) may differ across the health literacy spectrum. Medication reconciliation—agreement between patients’ self-reported medication list and the medication list in the EHR—in this population was low.
Although much remaining work is needed to determine how to best support chronic disease care across the health literacy spectrum, there are important implications for current practice. Care processes that meet the information needs of all patients should be routinely applied. Methods that may be employed might include use of information technology, the use of verbal or pictographic information exchange, education of family members or caregivers, or the use of other educational resources or healthcare team members.31,32 Clinicians and healthcare staff need to have a high level of awareness to detect and address low health literacy, medication errors and reconciliation problems.
Acknowledgments
The authors thank Milton “Mickey” Eder, PhD for his contribution to this study. The authors also acknowledge and thank staff members of the participating health centers and Northwestern University. This study was presented in part at the Society of General Internal Medicine’s Annual Meeting, April 21, 2017, Washington D.C.
Disclosure
Dr. Persell receives unrelated research support from Omron Healthcare, Ltd. and has previously received unrelated research support from Pfizer, Inc. He reports grants from National Institutes of Health, during the conduct of the study; grants from Omron Healthcare Co. Ltd., and Pfizer, Inc., including personal fees from CVS Health, outside the submitted work. Dr Michael Wolf reports grants from Amgen, Merck, and Eli Lilly; personal fees from Pfizer, outside the submitted work. Dr Wolf is an advisor on usability testing for medical products for Luto UK. The authors report no other conflicts of interest in this work.
References
1. Davis TC, Wolf MS, Bass PF
2. Berkman ND, Sheridan SL, Donahue KE, et al. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155:97–107. doi:10.7326/0003-4819-155-2-201107190-00005
3. Kripalani S, Henderson LE, Chiu EY, et al. Predictors of medication self-management skill in a low-literacy population. J Gen Intern Med. 2006;21:852–856. doi:10.1111/j.1525-1497.2006.00536.x
4. Raehl CL, Bond CA, Woods TJ, et al. Screening tests for intended medication adherence among the elderly. Ann Pharmacother. 2006;40:888–893. doi:10.1345/aph.1G478
5. Patzer RE, Serper M, Reese PP, et al. Medication understanding, non-adherence, and clinical outcomes among adult kidney transplant recipients. Clin Transplant. 2016;30:1294–1305. doi:10.1111/ctr.2016.30.issue-10
6. Mackey LM, Doody C, Werner EL, et al. Self-management skills in chronic disease management: what role does health literacy have? Med Decis Making. 2016;36:741–759. doi:10.1177/0272989X16638330
7. Persell SD, Osborn CY, Richard R, et al. Limited health literacy is a barrier to medication reconciliation in ambulatory care. J Gen Intern Med. 2007;22:1523–1526. doi:10.1007/s11606-007-0334-x
8. Zhang NJ, Terry A, McHorney CA. Impact of health literacy on medication adherence: a systematic review and meta-analysis. Ann Pharmacother. 2014;48:741–751. doi:10.1177/1060028014526562
9. Loke YK, Hinz I, Wang X, Salter C. Systematic review of consistency between adherence to cardiovascular or diabetes medication and health literacy in older adults. Ann Pharmacother. 2012;46:863–872. doi:10.1345/aph.1Q718
10. Kripalani S, Gatti ME, Jacobson TA. Association of age, health literacy, and medication management strategies with cardiovascular medication adherence. Patient Educ Couns. 2010;81:177–181. doi:10.1016/j.pec.2010.04.030
11. Freedman RB, Jones SK, Lin A, Robin AL, Muir KW. Influence of parental health literacy and dosing responsibility on pediatric glaucoma medication adherence. Arch Ophthalmol. 2012;130:306–311. doi:10.1001/archopthalmol.2011.1788
12. Bauer AM, Schillinger D, Parker MM, et al. Health literacy and antidepressant medication adherence among adults with diabetes: the diabetes study of Northern California (DISTANCE). J Gen Intern Med. 2013;28:1181–1187. doi:10.1007/s11606-013-2402-8
13. Fan JH, Lyons SA, Goodman MS, Blanchard MS, Kaphingst KA. Relationship between health literacy and unintentional and intentional medication nonadherence in medically underserved patients with type 2 diabetes. Diabetes Educ. 2016;42:199–208. doi:10.1177/0145721715624969
14. Hironaka LK, Paasche-Orlow MK, Young RL, Bauchner H, Geltman PL. Caregiver health literacy and adherence to a daily multi-vitamin with iron regimen in infants. Patient Educ Couns. 2009;75:376–380. doi:10.1016/j.pec.2009.03.016
15. Lindquist LA, Go L, Fleisher J, Jain N, Friesema E, Baker DW. Relationship of health literacy to intentional and unintentional non-adherence of hospital discharge medications. J Gen Intern Med. 2012;27:173–178. doi:10.1007/s11606-011-1886-3
16. Gazmararian JA, Kripalani S, Miller MJ, et al. Factors associated with medication refill adherence in cardiovascular-related diseases: a focus on health literacy. J Gen Intern Med. 2006;21:1215–1221. doi:10.1111/j.1525-1497.2006.00591.x
17. Bains SS, Egede LE. Associations between health literacy, diabetes knowledge, self-care behaviors, and glycemic control in a low income population with type 2 diabetes. Diabetes Technol Ther. 2011;13:335–341. doi:10.1089/dia.2010.0160
18. Mosher HJ, Lund BC, Kripalani S, Kaboli PJ. Association of health literacy with medication knowledge, adherence, and adverse drug events among elderly veterans. J Health Commun. 2012;17(Suppl 3):241–251. doi:10.1080/10810730.2012.712611
19. Thurston MM, Bourg CA, Phillips BB, Huston SA. Impact of health literacy level on aspects of medication nonadherence reported by underserved patients with type 2 diabetes. Diabetes Technol Ther. 2015;17:187–193. doi:10.1089/dia.2014.0220
20. Nassaralla CL, Naessens JM, Chaudhry R, et al. Implementation of a medication reconciliation process in an ambulatory internal medicine clinic. Qual Saf Health Care. 2007;16:90–94. doi:10.1136/qshc.2006.021113
21. Persell SD, Eder M, Friesema E, et al. EHR-based medication support and nurse-led medication therapy management: rationale and design for a three-arm clinic randomized trial. J Am Heart Assoc. 2013;2:e000311. doi:10.1161/JAHA.113.000311
22. Persell SD, Karmali KN, Lazar D, et al. Effect of electronic health record-based medication support and nurse-led medication therapy management on hypertension and medication self-management: a randomized clinical trial. JAMA Intern Med. 2018;178:1069–1077. doi:10.1001/jamainternmed.2018.2372
23. Weiss BD, Mays MZ, Martz W, et al. Quick assessment of literacy in primary care: the newest vital sign. Ann Fam Med. 2005;3:514–522. doi:10.1370/afm.405
24. Persell SD, Heiman HL, Weingart SN, et al. Understanding of drug indications by ambulatory care patients. Am J Health Syst Pharm. 2004;61:2523–2527. doi:10.1093/ajhp/61.23.2523
25. Wolf MS, Curtis LM, Waite K, et al. Helping patients simplify and safely use complex prescription regimens. Arch Intern Med. 2011;171:300–305. doi:10.1001/archinternmed.2011.39
26. Wolf MS, Davis TC, Curtis LM, et al. Effect of standardized, patient-centered label instructions to improve comprehension of prescription drug use. Med Care. 2011;49:96–100. doi:10.1097/MLR.0b013e3181f38174
27. Serper M, Patzer RE, Reese PP, et al. Medication misuse, nonadherence, and clinical outcomes among liver transplant recipients. Liver Transpl. 2015;21:22–28. doi:10.1002/lt.v21.1
28. DeMasi RA, Graham NM, Tolson JM, et al. Correlation between self-reported adherence to highly active antiretroviral therapy (HAART) and virologic outcome. Adv Ther. 2001;18:163–173. doi:10.1007/BF02850110
29. Waite KR, Paasche-Orlow M, Rintamaki LS, et al. Literacy, social stigma, and HIV medication adherence. J Gen Intern Med. 2008;23:1367–1372. doi:10.1007/s11606-008-0662-5
30. Paasche-Orlow MK, Parker RM, Gazmararian JA, et al. The prevalence of limited health literacy. J Gen Intern Med. 2005;20:175–184. doi:10.1111/j.1525-1497.2005.40245.x
31. Poureslami I, Nimmon L, Rootman I, Fitzgerald MJ. Priorities for action: recommendations from an international roundtable on health literacy and chronic disease management. Health Promot Int. 2017;32:743–754. doi:10.1093/heapro/daw003
32. Champion HM, Loosen JA, Kennelty KA. Pharmacy students and pharmacy technicians in medication reconciliation: a review of the current literature. J Pharm Pract. 2019;32:207–218. doi:10.1177/0897190017738916
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.