")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Associations Between Consumption of Different Vegetable Types and Depressive Symptoms in Japanese Workers: A Cross-Sectional Study
Authors Gong Q, Momma H , Cui Y, Huang C , Niu K , Nagatomi R
Received 30 November 2021
Accepted for publication 1 April 2022
Published 18 May 2022 Volume 2022:15 Pages 1073—1085
DOI https://doi.org/10.2147/RMHP.S350935
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Haiyan Qu
Qiang Gong,1 Haruki Momma,1 Yufei Cui,1,2 Cong Huang,3 Kaijun Niu,4 Ryoichi Nagatomi1,5
1Department of Medicine and Science in Sports and Exercise, Tohoku University Graduate School of Medicine, Sendai, Japan; 2Institute of Exercise Epidemiology and Department of Physical Education, Huaiyin Institute of Technology, Huaian, People’s Republic of China; 3Department of Physical Education, Zhejiang University, Hangzhou, People’s Republic of China; 4Department of Epidemiology, School of Public Health, Tianjin Medical University, Tianjin, People’s Republic of China; 5Division of Biomedical Engineering for Health & Welfare, Tohoku University Graduate School of Biomedical Engineering, Sendai, Japan
Correspondence: Ryoichi Nagatomi, Division of Biomedical Engineering for Health & Welfare, Tohoku University Graduate School of Biomedical Engineering, 2-1 Seiryo-machi, Aoba-ku, Sendai, 980-8575, Japan, Tel/Fax + 81-22-717-8586, Email [email protected]
Purpose: Vegetable intake is an important part of our everyday diet and is associated with many positive health outcomes. Although previous studies have investigated the association between vegetable consumption and depressive symptoms among various populations, no study has examined this association in the adult working population. The present study investigated whether the frequency of consumption of a specific type of vegetable is associated with the prevalence of depressive symptoms in Japanese adult workers.
Participants and Methods: The final participants consisted of 1724 Japanese adults, and a cross-sectional study was conducted to analyze the results. The frequency of vegetable consumption and depressive symptoms was evaluated using a brief-type self-administered diet history questionnaire and the Zung Self-Rating Depression Scale (SDS), respectively. The association between the variables was examined using Poisson regression analysis. Age-stratified analysis was performed, and SDS cut-off values of 45 and 50 were used to perform a sensitivity analysis.
Results: After adjustment for covariates, including age, body mass index, sociodemographic and lifestyle-related variables, health condition, C-reactive protein, and other dietary variables, an inverse association was found between tomato product consumption and the prevalence of depressive symptoms among men (P for trend < 0.01); however, no significant association was found for other vegetable types. For women, there was no association between the frequency of consumption of any of the vegetable types and the prevalence of depressive symptoms. The results were confirmed by the age-stratified analysis for both genders.
Conclusion: Consumption of tomato products may help alleviate depressive symptoms, regardless of differences in dietary culture among men.
Keywords: vegetables, depression, Japan, adults, workers, tomato products
Introduction
The prevalence of depressive symptoms has increased dramatically over the past few decades.1 Previous studies have shown that depressive symptoms are associated with a higher risk of physical disability,2 ischemic heart disease,3 and suicide.4 Moreover, depressive symptoms also adversely affect healthcare costs.5 In Japan, the number of patients with depression has been increasing,6 and approximately 20% of Japanese workers suffer from depressive symptoms.7 Since depressive symptoms are difficult to cure or treat,8 it is necessary to prevent the development of these symptoms among employees, during the early stages of work.
Some factors, such as physical activity9 and sun exposure,10 are considered as protective and alleviating factors for depressive symptoms. However, it may be difficult to obtain adequate time to exercise or receive sun exposure, especially for employees who work indoors, because they usually work more than eight hours a day (from 8 am to 5 pm). Diet, an indispensable part of daily life, is another important aspect in this regard. People gain energy and nutrition from their dietary intake. Vegetable intake is an important part of everyday diet and is directly related to many positive health outcomes, such as lowered risk of hypertension,11 type 2 diabetes,12 and heart failure.13 Vegetables include nutrients such as folate, vitamins, and polyphenol, which are the most effective for reducing anti-oxidative stress.14,15 Since previous studies have reported that oxidative stress may be associated with depressive symptoms,16,17 vegetable consumption can be considered to have beneficial influences on depressive symptoms. A previous study on 1676 Chinese adults aged 45 to 59 years reported that higher consumption of vegetables is significantly associated with a lower risk of depressive symptoms.18 However, this study focused on the association between total vegetable consumption and depressive symptoms and did not examine this association for particular vegetable types. Different vegetables have different nutrients, which may differently influence depressive symptoms. For example, tomato contains large amounts of lycopene, an antioxidant nutrient,19 and green leafy vegetables are great sources of the anti-inflammatory nutrient folate.20 Previous studies have examined the association between consumption of various vegetables, including tomatoes,21 green leafy vegetables,21–23 and yellow vegetables,23–25 and depressive symptoms among various populations, including teenagers, the elderly, and the general population.21–24 However, there is a lack of studies focusing on adult workers, who may be more prone to depressive symptoms in the face of social and family pressures compared to other populations.
Therefore, we designed a cross-sectional study to investigate whether the frequency of consumption of a specific vegetable type is associated with the prevalence of depressive symptoms, focusing on Japanese adult workers. Based on previous studies, we hypothesized that, although the consumption of all vegetables may not be inversely associated with depressive symptoms, a high frequency of consumption of vegetables that have anti-oxidative and anti-inflammatory effects may be associated with a lower prevalence of depressive symptoms in Japanese adult workers.
Methods
Participants
The data used in the present study were obtained from a prospective cohort study investigating the risk factors of non-communicable diseases among adult employees. This study was based on an annual health examination at the Sendai Oroshisho Center, Sendai city, Japan. A total of 1784 participants provided informed consent for data analysis in this study, from 2008 to 2011. The protocol of our study was approved by the Institutional Review Board of the Tohoku University Graduate School of Medicine (2019-1-394) and complies with the Declaration of Helsinki. All methods were performed in accordance with the relevant guidelines and regulations. Participants were excluded if information on dietary habits (n = 50), depressive symptoms (n = 4), or demographics (n = 6) was not available. After these exclusions, the final study sample comprised 1724 participants (men = 1333, women = 391).
Assessment of Frequency of Vegetable Consumption
A dietary survey was conducted using the brief-type self-administered diet history questionnaire (BDHQ) that included questions on 75 food items.26 The BDHQ has been validated in adult Japanese populations.27,28 The frequency of consumption of different vegetables was evaluated using the following questions: During the past month, how frequently did you eat tomato and tomato products/cabbage and Chinese cabbage/green leafy vegetables/root vegetables (including onion, lotus root, and burdock)/turnip/carrot and pumpkin/mushroom? Participants answered by checking one out of seven frequency categories (“almost never,” “<1 time/week,” “1 time/week,” “2−3 times/week,” “4−6 times/week,” “1 time/day,” and “2 or more times/day”). We then divided these responses into the following four categories according to the distribution of consumption of each vegetable type, because of comparable frequency distributions among the vegetable types: “<1 time/week,” “1 time/week,” “2−3 times/week,” and “≥4 times/week.”
Assessment of Depressive Symptoms
Depressive symptoms were assessed using the Zung Self-rating Depression Scale (SDS).29 This is a widely used scale for measuring the severity of depression. It has good internal consistency and validity30,31 and has been used in many Japanese studies.32,33 The SDS comprises 20 questions, and scores range from 20 to 80. Higher scores are indicative of more severe depressive symptoms. Previous studies have used cut-off values of 40,34,35 45,36 and 5037 to define depressive symptoms. In this study, we used the lowest cut-off value of 40 to define depressive symptoms, because this value was established based on the SDS29 and has also widely been used in previous studies including our own.34,35 Other cut-off values (45 and 50) were used for conducting a sensitivity analysis.
Assessment of Covariates
Weight (kg) and height (m) were measured, and body mass index (BMI) was calculated in kg/m2. Physical activity (PA) was evaluated using the International Physical Activity Questionnaire (IPAQ).38 Total daily physical activity was calculated as metabolic equivalents (METs) × hours/week. Based on the Japanese physical activity guidelines, PA was classified into two categories: <23 and ≥23 METs h/week.39 Smoking status was categorized into non, current, and former smoker. Drinking status was classified into three categories: none, 1−6 days/week, and every day. Educational level was classified into two categories: <12 and ≥12 years. Occupation was classified into desk work and other. Living condition was classified into “living alone” and “with others.” Information on age and gender was obtained using a self-reported questionnaire survey. Blood pressure was measured using a blood pressure monitor (Yamasu 605; Kenzmedico Co., Ltd., Saitama, Japan). Hypertension was defined as having a systolic blood pressure ≥140 mmHg or a diastolic blood pressure ≥90 mmHg, or taking an anti-hypertensive drug.40 Fasting blood glucose was measured using enzymatic methods (Eerotec Co., Ltd., Tokyo, Japan). Diabetes was defined as fasting blood glucose ≥126 mg/dL or taking anti-diabetic drugs.41 Dyslipidemia was defined as triglyceride levels ≥150 mg/dl, high-density lipoprotein levels <40 mg/dL or low-density lipoprotein levels ≥140 mg/dL, or taking anti-hyperlipidemia drugs.42 High-sensitivity C-reactive protein concentration (hsCRP) was measured from the blood sample using an immune-technique with a Behring BN II analyzer (Dade Behring, Tokyo, Japan).
Statistical Analysis
Considering that logistic regression is used for the lower range of prevalence of an outcome, the prevalence of depressive symptoms may be overestimated.43,44 Thus, the associations between frequency of consumption of each vegetable type and depressive symptoms were examined using Poisson regression analysis, because the prevalence of the outcome was more than 10%. We calculated prevalence ratios (PRs) with 95% confidence intervals (CIs) stratified by gender. Depressive symptoms were taken as the objective variable, and frequency of consumption of each vegetable type was used as the explanatory variable. PRs were adjusted for age (continuous variable), gender, BMI (continuous variable), educational level, occupation, living condition, smoking status, drinking status, physical activity, hypertension, diabetes, dyslipidemia, hsCRP (continuous variable), intake of total energy (continuous variable), and consumption of milk, seaweed, green tea, soy products, and other vegetables (all continuous variables) except for the explanatory variables. Age-stratified analysis was performed and the median ages (43 years for men and 40 years for women) were used to categorize the participants based on the age distribution. The SDS cut-off values of 45 and 50 were also used for sensitivity analysis. All statistical analyses were performed using the SPSS statistical software version 22.0 for Windows (SPSS, Inc., Chicago, IL). A P-value less than 0.05 was considered statistically significant.
Results
Of the 1724 participants, 1333 (77.3%) were men and 391 (22.7%) were women. Table 1 shows the basic characteristics of the participants. The participants with depressive symptoms had a lower intake of total energy, soy, and seaweed than that of those without depressive symptoms. The percentage of diabetes, nondrinker, educational level (≥ 12 years) in the participants with depressive symptoms was lower in those without depressive symptoms. Table S1 shows the characteristics of men and women according to the prevalence of depressive symptoms. Among men, the number of participants with a high amount of total energy, high food intake, and high educational level were higher in the no depressive symptoms category. In contrast, the proportion of participants who had diabetes was lower in the no depressive symptoms category. Among women, the amount of milk and seaweed intake and the proportion of smokers and drinkers were higher in the no depressive symptoms category.
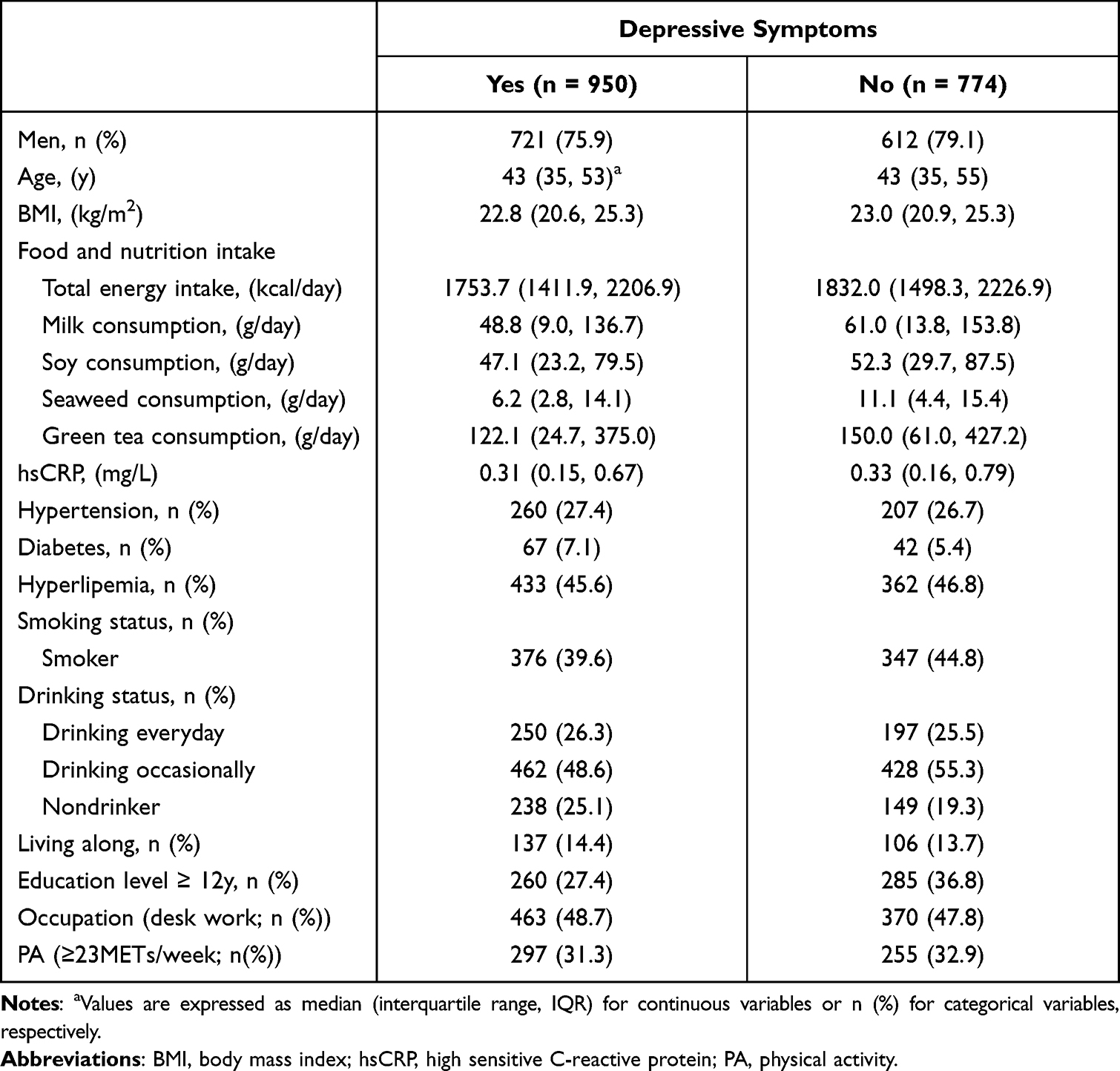 |
Table 1 Characteristics of Participants According to Depressive Symotoms |
Table 2 shows the association between frequency of consumption of each vegetable type and depressive symptoms among both men and women. An inverse association was found between tomato products consumption and prevalence of depressive symptoms in both the unadjusted and adjusted models among men. After adjusting for covariates, compared with the first category of tomato products consumption, the adjusted PRs (95% CIs) for depressive symptoms in the second, third, and fourth categories were 0.91 (0.77, 1.08), 0.83 (0.69, 0.98), and 0.77 (0.61, 0.95), respectively (P for trend <0.01). Moreover, the frequency of green leafy vegetables consumption was inversely, but not significantly, associated with the prevalence of depressive symptoms after adjusting for covariates (P for trend = 0.07). No significant association was found between the frequency of consumption of other vegetables and depressive symptoms in men. For women, the frequency of consumption of none of the vegetable types was associated with the prevalence of depressive symptoms.
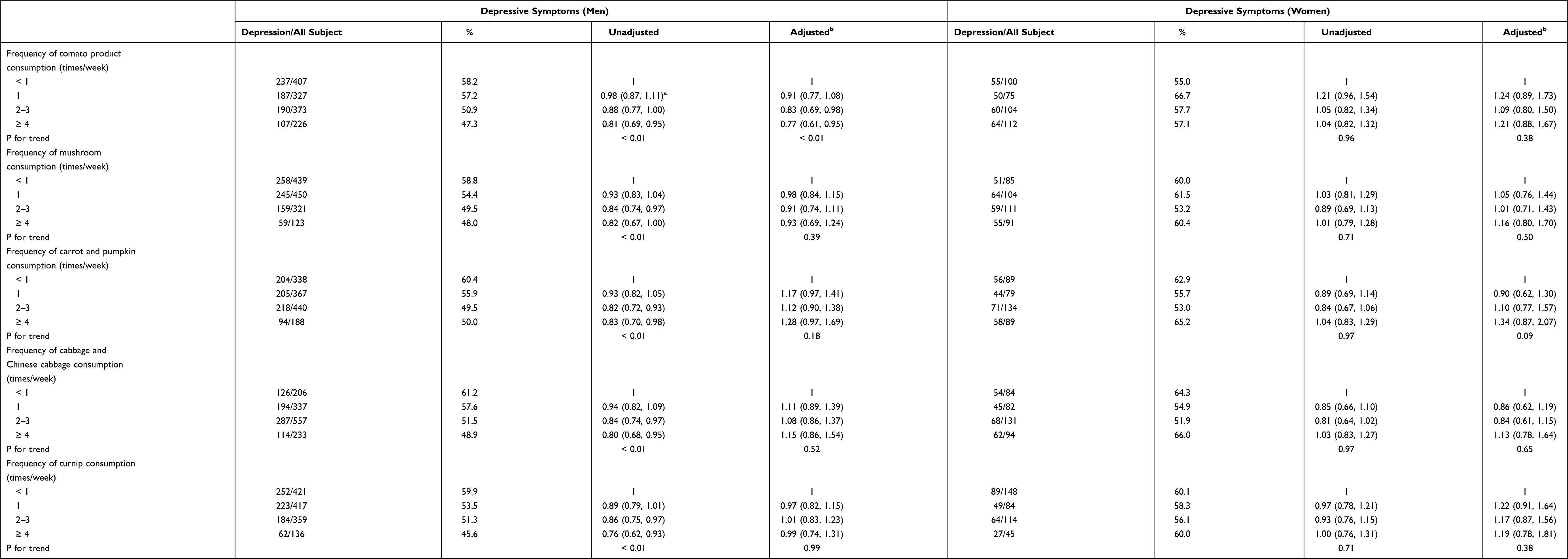 |
Table 2 Associations Between Frequency of Different Vegetable Types Consumption and Depressive Symptoms Among Men and Women |
Table 3 shows the results of the sensitivity analysis using other SDS cut-off points. When the cut-off value was set to ≥45, an inverse association was found between the frequency of tomato products consumption and depressive symptoms in men (P for trend = 0.01). Although this association disappeared when the cut-off value was set to ≥50, the trend was consistent with the results of the main analysis. In women, no association was found for the consumption of any of the vegetable types.
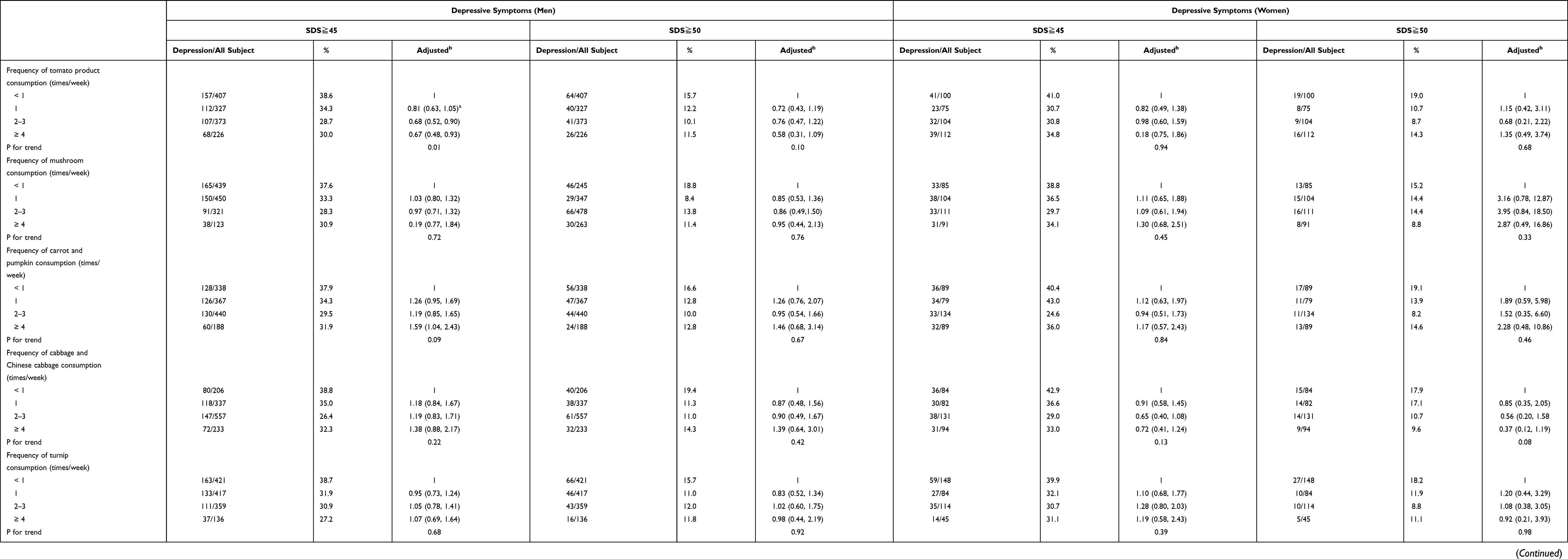 |
Table 3 Sensitive Analysis of Associations Between Frequency of Different Vegetable Types Consumption and Depressive Symptoms Among Men and Women |
Table 4 shows age-stratified associations between the frequency of consumption of each vegetable type and depressive symptoms among men and women. The frequency of tomato products consumption was inversely associated with the prevalence of depressive symptoms, particularly in older men (≥43 years). For green leafy vegetable, an inverse association was obtained in younger men (<43 years). No association was found between any other vegetable type and depressive symptoms among men. In women, no association was found between any vegetable type and depressive symptoms.
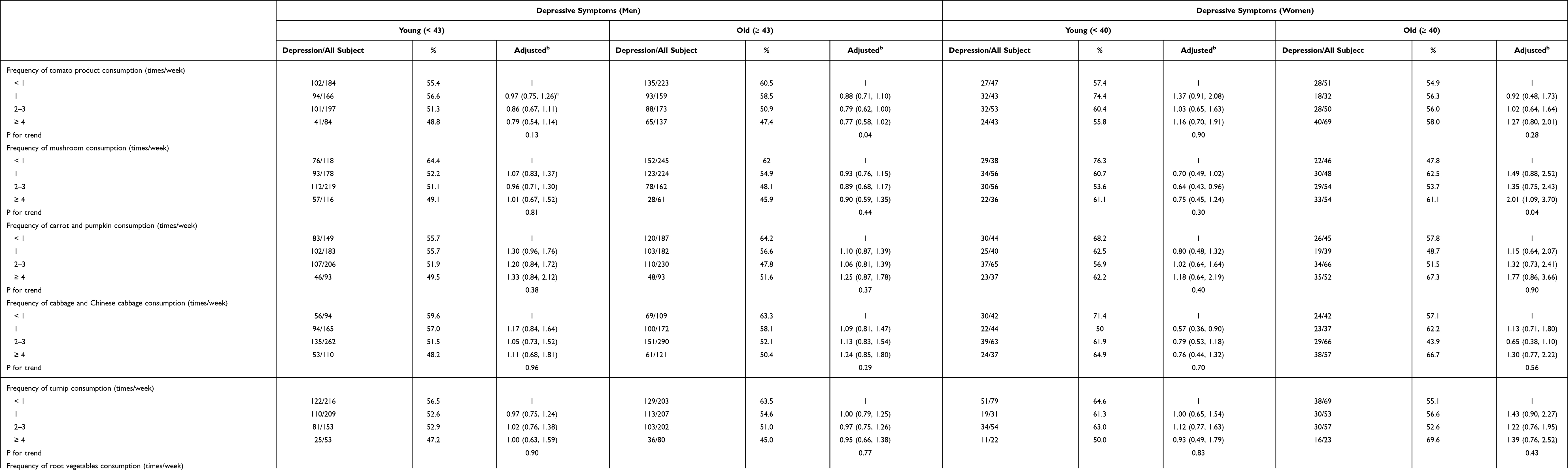 |
Table 4 Age Stratified Associations Between Frequency of Different Vegetable Types Consumption and Depressive Symptoms Among Men and Women Aged |
Discussion
In this study, we investigated the association between the frequency of consumption of different vegetable types and the prevalence of depressive symptoms in Japanese adult workers. As expected, not all types of vegetables were associated with the prevalence of depressive symptoms. Notable, the frequency of tomato products consumption was inversely associated with the prevalence of depressive symptoms in male workers. These results suggest that tomatoes may positively influence the prevention of depressive symptoms among Japanese male workers.
Several previous studies have examined the association between vegetable consumption and depressive symptoms. A Japanese cross-sectional study of 986 retired elderly people, aged 70 years and above, revealed that the intake of tomatoes and a tomato-rich diet was inversely associated with the prevalence of depressive symptoms.21 Consistent with this result, our findings showed that a higher frequency of tomato products consumption was associated with a lower prevalence of depressive symptoms among male workers, particularly those aged 43 years or above. This association was confirmed when a sensitivity analysis using a higher cut-off value was conducted. Our finding is supported by a recent study showing that a higher intake of tomatoes and tomato mixture was inversely associated with depressive symptoms in Americans.23 Therefore, consumption of tomato products may positively influence the alleviation of depressive symptoms regardless of differences in dietary culture or race.
Cross-sectional studies of New Zealanders aged 18–25 years45 and Iranian women aged 20–49 years25 showed that the consumption of dark leafy greens (ie, green leafy vegetables) was inversely associated with depressive symptoms. Moreover, Sun et al showed an inverse association between dark green vegetables and depressive symptoms among American adults.23 However, no clear association was found between green leafy vegetables and the prevalence of depressive symptoms among men in the current study. One of the reasons for this could be the age difference between the study populations. The participants in the previous studies25,45 were younger than the participants in our study (19–83 years). Interestingly, when an age-stratified analysis was performed, the frequency of green leafy vegetable consumption was found to be inversely associated with the prevalence of depressive symptoms among younger men (<43 years) in this study. It is possible that green leafy vegetables may have a beneficial impact for younger people, but not for older people. Considering the trend of older people eating in the traditional Japanese pattern, that is characterized by a larger consumption of vegetables,46 and that consumption of vegetables in general may support anti-oxidative capacities,47 the contribution of green leafy vegetables could have been diluted, whereas tomato and tomato products have a high enough capacity to indicate an independent association. Among the younger participants in our study, the consumption of vegetables in general was lower than that in the older population (data not shown); thus, green leafy vegetable consumption per se could have had a certain impact.
In this study, no association was found between the consumption of any vegetable type and the prevalence of depressive symptoms in women. In addition to the small sample size of women, menopausal status may have affected our findings. A previous study reported that the decline of ovarian function and decreased levels of estrogen during menopause are associated with a higher prevalence of depression.48 However, since the number of post-menopausal women in this study was very small (n = 81), the influence of menopause status does not appear to be notable Since we are unable to provide additional explanations, further research is needed on female workers.
This study has some limitations. First, the study participants were from a single area of Sendai city, Japan. Therefore, selection bias may be present, and our results may not be representative of all Japanese workers. Second, information about food consumption was obtained using a self-reported questionnaire in which participants described their consumption over the last month. This leads to a potential recall bias, although the validity of the BDHQ was verified by comparison with 16 days’ dietary record.27 Third, we did not consider seasonal influences on the frequency of vegetable consumption. Because seasonal influences on the frequency of vegetable intake may not be particularly strong because seasonal vegetables, including tomatoes, are mostly available throughout the year in Japan. Fourth, although several confounding factors were included when analyzing the association between vegetable consumption and depressive symptoms, we cannot exclude the possibility that other factors affected these associations. Finally, because this was a cross-sectional study, the causality of the relationship between vegetable consumption and depressive symptoms cannot be established.
In conclusion, among the selected vegetables, the frequency of tomato products consumption was inversely associated with the prevalence of depressive symptoms in Japanese male workers. Further studies are required to confirm these findings and to clarify causality.
Acknowledgments
This study was supported by a Grant-in-Aid for “Knowledge Cluster Initiative” from the Ministry of Education, Culture, Sports, Science and Technology of Japan, and was partially supported by the Center of Innovation Program from Japan Science and Technology Agency, JST. The funding sources had no role in study design, data collection, analysis and interpretation, the writing of the report, or the decision to submit the paper for publication.
Funding
This study was supported by a Grant-in-Aid for “Knowledge Cluster Initiative” from the Ministry of Education, Culture, Sports, Science and Technology of Japan, and was partially supported by the Center of Innovation Program from the Japan Science and Technology Agency, JST.
Disclosure
All the authors declare that they have no competing interests in this work.
References
1. Moussavi S, Chatterji S, Verdes E, et al. Depression, chronic diseases, and decrements in health: results from the World Health Surveys. Lancet. 2007;370(9590):851–858. doi:10.1016/S0140-6736(07)61415-9
2. Tariq A, Beihai T, Ali S, et al. Mediating effect of cognitive social capital on the relationship between physical disability and depression in elderly people of Rural Pakistan. Int J Environ Res Public Health. 2019;16(21):4232. doi:10.3390/ijerph16214232
3. Charlson FJ, Moran AE, Freedman G, et al. The contribution of major depression to the global burden of ischemic heart disease: a comparative risk assessment. BMC Med. 2013;11(1):250. doi:10.1186/1741-7015-11-250
4. Kasckow J, Golshan S, Zisook S. Does age moderate the relationship between depressive symptoms and suicidal ideation in middle-aged and older patients with schizophrenia and subthreshold depression? Am J Geriatr Psychiatry. 2014;22(5):437–441. doi:10.1016/j.jagp.2013.01.039
5. Bhattarai N, Charlton J, Rudisill C, et al. Prevalence of depression and utilization of health care in single and multiple morbidity: a population-based cohort study. Psychol Med. 2013;43(7):1423–1431. doi:10.1017/S0033291712002498
6. Ministry of Health Labour and Welfare. Health and welfare statistics association; 2019.
7. Tamakoshi A, Ohno Y, Yamada T, et al. Depressive mood and suicide among middle-aged workers: findings from a prospective cohort study in Nagoya, Japan. J Epidemiol. 2000;10(3):173–178. doi:10.2188/jea.10.173
8. Kok RM, Reynolds CF 3rd. Management of depression in older adults: a review. JAMA. 2017;317(20):2114–2122. doi:10.1001/jama.2017.5706
9. Werneck AO, Stubbs B, Szwarcwald CL, et al. Independent relationships between different domains of physical activity and depressive symptoms among 60,202 Brazilian adults. Gen Hosp Psychiatry. 2020;64:26–32. doi:10.1016/j.genhosppsych.2020.01.007
10. Knippenberg S, Damoiseaux J, Bol Y, et al. Higher levels of reported sun exposure, and not vitamin D status, are associated with less depressive symptoms and fatigue in multiple sclerosis. Acta Neurol Scand. 2014;129(2):123–131. doi:10.1111/ane.12155
11. Liu MW, Yu HJ, Yuan S, et al. Association between fruit and vegetable intake and the risk of hypertension among Chinese adults: a longitudinal study. Eur J Nutr. 2018;57(7):2639–2647. doi:10.1007/s00394-018-1687-0
12. Li M, Fan Y, Zhang X, et al. Fruit and vegetable intake and risk of type 2 diabetes mellitus: meta-analysis of prospective cohort studies. BMJ Open. 2014;4(11):e005497. doi:10.1136/bmjopen-2014-005497
13. Rautiainen S, Levitan EB, Mittleman MA, et al. Fruit and vegetable intake and rate of heart failure: a population-based prospective cohort of women. Eur J Heart Fail. 2015;17(1):20–26. doi:10.1002/ejhf.191
14. Urquiaga I, Leighton F. Plant polyphenol antioxidants and oxidative stress. Biol Res. 2000;33(2):55–64. doi:10.4067/S0716-97602000000200004
15. Heber D, Lu QY. Overview of mechanisms of action of lycopene. Exp Biol Med (Maywood). 2002;227(10):920–923. doi:10.1177/153537020222701013
16. Srivastava N, Barthwal MK, Dalal PK, et al. A study on nitric oxide, beta-adrenergic receptors and antioxidant status in the polymorphonuclear leukocytes from the patients of depression. J Affect Disord. 2002;72(1):45–52. doi:10.1016/S0165-0327(01)00421-9
17. Jacka FN, O’Neil A, Opie R, et al. A randomised controlled trial of dietary improvement for adults with major depression (the ‘SMILES’ trial). BMC Med. 2017;15(1):23. doi:10.1186/s12916-017-0791-y
18. Cheng HY, Shi YX, Yu FN, et al. Association between vegetables and fruits consumption and depressive symptoms in a middle-aged Chinese population: an observational study. Medicine. 2019;98(18):e15374. doi:10.1097/MD.0000000000015374
19. Imran M, Ghorat F, Ul-Haq I, et al. Lycopene as a natural antioxidant used to prevent human health disorders. Antioxidants. 2020;9(8). doi:10.3390/antiox9080706.
20. Samblas M, Martinez JA, Milagro F. Folic acid improves the inflammatory response in LPS-activated THP-1 macrophages. Mediators Inflamm. 2018;2018:1312626. doi:10.1155/2018/1312626
21. Niu K, Guo H, Kakizaki M, et al. A tomato-rich diet is related to depressive symptoms among an elderly population aged 70 years and over: a population-based, cross-sectional analysis. J Affect Disord. 2013;144(1–2):165–170. doi:10.1016/j.jad.2012.04.040
22. Ainamani HE, Bamwerinde WM, Rukundo GZ, et al. Fruit and vegetable intake and mental health among family caregivers of people with dementia in Uganda. Ment Health Prev. 2021;24:200223. doi:10.1016/j.mhp.2021.200223
23. Sun J, Li Z, Li Y, et al. Intakes of specific categories of vegetables and fruits are inversely associated with depressive symptoms among adults. J Epidemiol. 2020;31(3):210–219. doi:10.2188/jea.JE20200003
24. Tanaka M, Hashimoto K. Impact of consuming green and yellow vegetables on the depressive symptoms of junior and senior high school students in Japan. PLoS One. 2019;14(2):e0211323. doi:10.1371/journal.pone.0211323
25. Baharzadeh E, Siassi F, Qorbani M, et al. Fruits and vegetables intake and its subgroups are related to depression: a cross-sectional study from a developing country. Ann Gen Psychiatry. 2018;17(1):46. doi:10.1186/s12991-018-0216-0
26. Sasaki S, Ushio F, Amano K, et al. Serum biomarker-based validation of a self-administered diet history questionnaire for Japanese subjects. J Nutr Sci Vitaminol. 2000;46(6):285–296. doi:10.3177/jnsv.46.285
27. Kobayashi S, Murakami K, Sasaki S, et al. Comparison of relative validity of food group intakes estimated by comprehensive and brief-type self-administered diet history questionnaires against 16 d dietary records in Japanese adults. Public Health Nutr. 2011;14(7):1200–1211. doi:10.1017/S1368980011000504
28. Kobayashi S, Honda S, Murakami K, et al. Both comprehensive and brief self-administered diet history questionnaires satisfactorily rank nutrient intakes in Japanese adults. J Epidemiol. 2012;22(2):151–159. doi:10.2188/jea.JE20110075
29. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12(1):63–70. doi:10.1001/archpsyc.1965.01720310065008
30. Zung WW. A cross-cultural survey of symptoms in depression. Am J Psychiatry. 1969;126(1):116–121. doi:10.1176/ajp.126.1.116
31. Zung WW, Richards CB, Short MJ. Self-rating depression scale in an outpatient clinic. Further validation of the SDS. Arch Gen Psychiatry. 1965;13(6):508–515. doi:10.1001/archpsyc.1965.01730060026004
32. Nitta T, Deguchi Y, Iwasaki S, et al. Depression and occupational stress in Japanese school principals and vice-principals. Occup Med. 2019;69(1):39–46. doi:10.1093/occmed/kqy149
33. Nishi N, Kurosawa M, Nohara M, et al. Knowledge of and attitudes toward suicide and depression among Japanese in municipalities with high suicide rates. J Epidemiol. 2005;15(2):48–55. doi:10.2188/jea.15.48
34. Hamano T, Takeda M, Sundquist K, et al. Geographic elevation, car driving, and depression among elderly residents in rural areas: the Shimane CoHRE Study. Int J Environ Res Public Health. 2016;13(5):738. doi:10.3390/ijerph13070738
35. Tan M, Chen M, Li J, et al. Depressive symptoms and associated factors among left-behind children in China: a cross-sectional study. BMC Public Health. 2018;18(1):1059. doi:10.1186/s12889-018-5963-y
36. Cui Y, Huang C, Momma H, et al. Consumption of low-fat dairy, but not whole-fat dairy, is inversely associated with depressive symptoms in Japanese adults. Soc Psychiatry Psychiatr Epidemiol. 2017;52(7):847–853. doi:10.1007/s00127-016-1333-1
37. Guo F, Huang C, Cui Y, et al. Dietary seaweed intake and depressive symptoms in Japanese adults: a prospective cohort study. Nutr J. 2019;18(1):58. doi:10.1186/s12937-019-0486-7
38. Craig CL, Marshall AL, Sjostrom M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381–1395. doi:10.1249/01.MSS.0000078924.61453.FB
39. Ministry of Health Labour and Welfare. Exercise and physical activity references for health promotion 2013; 2013. in Japanese.
40. Morita E, Naito M, Hishida A, et al. No association between the frequency of forest walking and blood pressure levels or the prevalence of hypertension in a cross-sectional study of a Japanese population. Environ Health Prev Med. 2011;16(5):299–306. doi:10.1007/s12199-010-0197-3
41. Wu H, Jackson CA, Wild SH, et al. Socioeconomic status and self-reported, screen-detected and total diabetes prevalence in Chinese men and women in 2011–2012: a nationwide cross-sectional study. J Glob Health. 2018;8(2):020501. doi:10.7189/jogh.08.020501
42. Sugai T, Suzuki Y, Yamazaki M, et al. High prevalence of obesity, hypertension, hyperlipidemia, and diabetes mellitus in Japanese outpatients with schizophrenia: a nationwide survey. PLoS One. 2016;11(11):e0166429. doi:10.1371/journal.pone.0166429
43. Barros AJ, Hirakata VN. Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol. 2003;3(1):21. doi:10.1186/1471-2288-3-21
44. Zhang J, Yu KF. What’s the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. JAMA. 1998;280(19):1690–1691. doi:10.1001/jama.280.19.1690
45. Brookie KL, Best GI, Conner TS. Intake of raw fruits and vegetables is associated with better mental health than intake of processed fruits and vegetables. Front Psychol. 2018;9:487. doi:10.3389/fpsyg.2018.00487
46. Guo H, Niu K, Monma H, et al. Association of Japanese dietary pattern with serum adiponectin concentration in Japanese adult men. Nutr Metab Cardiovasc Dis. 2012;22(3):277–284. doi:10.1016/j.numecd.2010.06.006
47. Bacchetti T, Turco I, Urbano A, et al. Relationship of fruit and vegetable intake to dietary antioxidant capacity and markers of oxidative stress: a sex-related study. Nutrition. 2019;61:164–172. doi:10.1016/j.nut.2018.10.034
48. Zeng LN, Yang Y, Feng Y, et al. The prevalence of depression in menopausal women in China: a meta-analysis of observational studies. J Affect Disord. 2019;256:337–343. doi:10.1016/j.jad.2019.06.017
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.